Introduction
Diagnosing patients with primary hyperparathyroidism
is a challenge. They are often clinically asymptomatic with various
biochemical changes in serum levels for calcium (Ca), parathyroid
hormone (PTH), vitamin D, and urinary Ca (1). Increased serum levels of PTH and Ca in
primary hyperparathyroidism may be associated with clinical
manifestations such as osteoporosis, bone demineralization,
nephrolithiasis, dehydration, hypertension, gastrointestinal
manifestations (peptic ulcer, pancreatitis) and may even be
associated with neuropsychiatric diseases (1,2).
Single or multiple adenomas or multiglandular hyperplasia or
parathyroid carcinoma can be found in the parathyroid gland.
Hyperparathyroidism can be associated with multiple endocrine
tumors (genetic syndromes MEN 1 and type 2a) (2). The literature states that asymptomatic
hyperparathyroidism has been the most common clinical phenotype in
the last 40 years (3).
The etiopathogenesis of hyperparathyroidism is
defined by the histopathological diagnosis of surgical resection
tissues (adenomas, hyperplasia, cancer) (4). There is also a lack of evidence for
personalized molecular diagnosis (4,5), as
well as a lack of details on surgical means for a complete
resection of pseudotumor and/or parathyroid formations (6,7).
Surgical interventions for pseudotumor or tumor
parathyroid formation removal are adapted depending on the
anatomical localization of the parathyroid glands (classical or
ectopic): classic or minimally invasive cervical parathyroidectomy
and mediastinal parathyroidectomy by classical approach
(cervicosternotomy), or by mediastinoscopy (6). Guided parathyroidectomy by ultrasound
imaging, jugular venous sampling-intraoperative PTH dosing, probe
localization, and frozen sections are well known standard
procedures (1). These
intraoperative adjuvant techniques confirm the efficient removal of
the pathological glands (8,9). When parathyroid cancer is suspected,
resection is performed with the parathyroid capsule, which is the
standard of operation (10).
The complete removal of the parathyroid pseudotumors
regardless of localization and anatomical relationships, with
decompression of adjacent anatomical formations, requires different
surgical approaches. Partial cervicosternotomy is required for
mediastinal parathyroid large formations or fixated to the
anatomical structures of the mediastinum (11-13).
In some cases, we used modified classical cervicotomy and modified
Kocher cervicotomy (14,15).
We conducted this retrospective study to reveal the
diagnostic attitude and surgical approaches applied by our team;
the advantages of Kocher modified incision. We consulted
international protocols for hyperparathyroidism in pseudotumor
lesions: hyperplasias or parathyroid adenomas. We underline the
role of the thoracic surgeon for the surgical interventions of
these formations with the typical and ectopic location.
Patients and methods
This study was reported according to STROBE
(Strengthening the Reporting of Observational Studies in
Epidemiology) guidelines (16).
This is a retrospective study. The study was approved by the
Research Ethics Committee carried out through the collaboration of
the ‘Carol Davila’ University of Medicine and Pharmacy from
Bucharest and the Central Military Emergency University Hospital
‘Dr. Carol Davila’ Bucharest (no. 388/09 June 2020). We
retrospectively studied the records of the patients who underwent
surgery against pseudotumor formations with hyperparathyroidism in
SUUMC, between 2014 and 2019. The interventions were performed in a
single surgical center.
Participants
With these guides as a benchmark, we analyzed the
surgical treatment of hyperparathyroidism and the inclusion
criteria for surgery (increased values of serum Ca; levels of PTH
compared to reference values; biochemical analysis of renal
function; the presence of renal lithiasis; the presence of
osteoporosis on X-rays; the age of each patient). We evaluated the
therapeutic efficacy by comparing preoperative to postoperative
values. A database of clinical and paraclinical signs was created
from observation sheets, operatory protocols, and histopathological
reports.
The study group comprised 41 women and 14 men with a
mean age of 54 years and ages between 21 and 87 years. Initially,
the patients were selected by the endocrinologist based on clinical
diagnosis, laboratory, and imaging criteria. Blood samples for
serum Ca and PTH were analyzed for all patients. A total of 51
patients were diagnosed with primary hyperparathyroidism, 3
patients were diagnosed with secondary hyperparathyroidism and one
patient was diagnosed with tertiary hyperparathyroidism.
The selection of patients for surgical interventions
was made based on international protocols for diagnostic
management.
Clinical analysis
Clinical analysis included: fatigue in 42 patients,
bone pain in 49 patients, myalgia in 36 patients, polyuria in 22
patients, polydipsia in 26 patients, renal lithiasis in 37
patients, hypertension in 32 patients, osteoporosis in 48 patients,
and depression in 34 patients.
Laboratory analysis
Preoperative and postoperative blood samples were
analyzed immediately after collection. Preoperative blood sample
investigations in patients detected serum Ca levels >8.40-10.2
mg/dl (considered to be normal in the reference values). A total of
51 patients presented equivalent values for primary
hyperparathyroidism, 3 secondary and one tertiary; an increased
serum level of PTH >15-65 pg/ml (considered to be the normal
reference range) was detected in all patients in the group and an
increased serum level of total proteins >6.5-8.1 g/dl (normal
reference range) was also detected in all patients. Postoperative
serum levels of these analytes were normal or close to normal
values.
Imaging diagnosis
All patients underwent an X-ray for bone conditions
(48 patients had osteoporosis), and ultrasound evaluations of soft
parts of the cervical region were performed for all patients. Renal
ultrasounds were performed for all patients (37 patients were
diagnosed with renal lithiasis), 99mTc-sestamibi scintigraphy, and
computed tomography (CT). Patients who received intraoperative
ultrasound cervical examination aided the surgical team approach to
target the pseudotumor formation.
Histopathological diagnosis
The confirmation of the diagnosis of the excised
parts was established by the pathological anatomy service. Twelve
specimens with parathyroid hyperplasia were found and 43 were
parathyroid adenomas.
The therapeutic attitude complied with the
international treatment management protocols for
hyperparathyroidism (11). Thus,
depending on the typical anatomical (cervical) or ectopic
(intramediastinal) localization of the pseudotumor formations, 36
parathyroidectomies surgical approaches through minimal incisions
centered on formations under ultrasound guidance, 11 classical
parathyroidectomies, 3 partial cervical sternotomies and 8
excisions by mediastinoscopy were performed. A total of 6 patients
benefited from autotransplantation of a parathyroid gland, in the
deltoid muscle or the sternocleidomastoid muscles.
Results
High therapeutic efficacy is achieved by curing the
hyperparathyroidism, decreasing morbidities related to the disease,
increasing the quality of life of the patient, decreasing
hospitalization days for severe correction of hypercalcemia or
acute renal failure, and reducing direct costs of treatment and
hospitalization time.
Characteristics of the patients
The endocrinologist selected the patients with
hyperparathyroidism who required surgery. Only patients who had
undergone surgery were studied. The symptomatology was specific for
hyperparathyroidism: fatigue in 42 patients, bone pain in 49
patients, myalgia in 36 patients, polyuria in 22 patients,
polydipsia in 26 patients, renal lithiasis in 37 patients,
hypertension in 32 patients, osteoporosis in 48 patients, and
depression in 34 patients. Examinations of the blood for calcemia,
PTH, and proteinemia were carried out preoperatively as well as
postoperatively. Preoperative PTH values 73 and 210 pg/ml decreased
after surgery to 48-65 pg/ml.
Localization of the tumors
Imaging investigations established the following
localizations of the pseudotumoral parathyroid formations: Right
upper parathyroid in 6 cases, right lower parathyroid in 26 cases,
left upper parathyroid in 7 cases, left lower parathyroid in 10
cases, right retrothyroidian parathyroid in 3 cases, left
retrothyroidian parathyroid in 5 cases, right paratracheal
mediastinal parathyroid in 3 cases, parathyroid in the anterior
mediastinum in 5 cases, right mediastinal cervical parathyroid in 4
cases, parathyroid adherence of the brachiocephalic artery trunk in
1 case. It should be mentioned that 43 patients had a single
pseudotumoral formation of parathyroid disease, 9 patients were
detected with two formations, and 3 patients with 3 formations.
After the classification of Perrier parathyroid
adenomas, the locations of the pseudotumors were: type A in 24
formations, type B in 11 formations, type C in 13 cases, type D in
3 cases, type E in no cases, type F in 14 cases, and type G in 5
cases.
Surgical approach
Typical or ectopic anatomical localizations
indicated the type of surgical approach. We performed classical
parathyroidectomy for bilateral or multiple parathyroid lesions
(classic Kocher incision), parathyroidectomy through Kocher
modified incision (for the superior parathyroid lesions), minimally
invasive parathyroidectomy (for the inferior parathyroid lesions),
and mediastinal parathyroidectomy (through upper cervicosternotomy
or by mediastinoscopy). We also performed 6 associated parathyroid
autotransplantations in some cases. For successful operative
management, parathyroid pseudotumoral formations were spotted both
preoperatively and intraoperatively (38 formations) by
ultrasound.
For patients who had upper right parathyroid
pseudotumoral formations (6 cases) and for 7 cases of upper left
localized parathyroid lesions, a modified Kocher incision was
performed, approximately 3 cm in length, to allow for an efficient
surgical approach of the area containing the lesion. After a
thorough dissection of the anatomical planes, with the
identification of the ipsilateral recurrent laryngeal nerve and its
preservation, as well as the control of the upper thyroid artery,
the posterior face of the thyroid gland was reached where the
pseudotumoral formations were found. Aspects of the parathyroid
pseudotumoral formations included: A yellowish-brown color,
encapsulated, and the vast majority were relatively easily
delineated from the tissue of the thyroid gland, but 4 formations
were difficult to delineate from the adjacent thyroidal
peri-glandular tissues, with diameters between 1 and 2 cm. No
partial or total thyroidectomy was required in any patient.
There were 26 cases of lower right parathyroid
pseudotumoral formations, and 10 cases of lower left parathyroid
gland, for which incisions centered on the pseudotumoral formation
were made. Preoperatively, the tegument was marked under ultrasound
guidance, then a minimal incision was made in the marked area. In
the dissection of the anatomical layers, special attention was paid
to the inferior thyroid arteries and the ipsilateral recurrent
laryngeal nerve respectively, but some 4 formations were difficult
to delineate from the thyroid peri-glandular tissues.
Modified Kocher type incision was carried out in the
lower right retro-thyroid pseudotumoral formations (3 cases) and
for the lower-left one (1 case). Increased attention was paid to
vasculonervous formations, especially the recurrent laryngeal
nerve, upper and lower thyroid arterial branches.
Carlen's type cervical mediastinoscopy was performed
in 8 cases of mediastinal parathyroid pseudotumoral formations.
After the incision, the cervical anatomical planes were carefully
dissected and soft dissection was performed at the level of the
upper mediastinum, below the arterial vascular plane represented by
the brachiocephalic artery trunk and aorta. Paratracheal
pseudotumoral formations were removed under the mediastinoscopy, 3
cases from the right (adjacent to the remaining thymic tissue), and
5 cases from the left (in the mediastinal fat).
A minimal suprasternal cervicotomy was performed in
1 case of parathyroid adenoma adherent to the brachiocephalic
artery trunk. After dissection of the anatomical layers, a
pseudotumoral formation with a diameter of 2.5 cm was found,
located at the level of the brachiocephalic artery trunk. In this
case, the experience of the operative team was necessary to perform
an excision of this pathological formation without complications. A
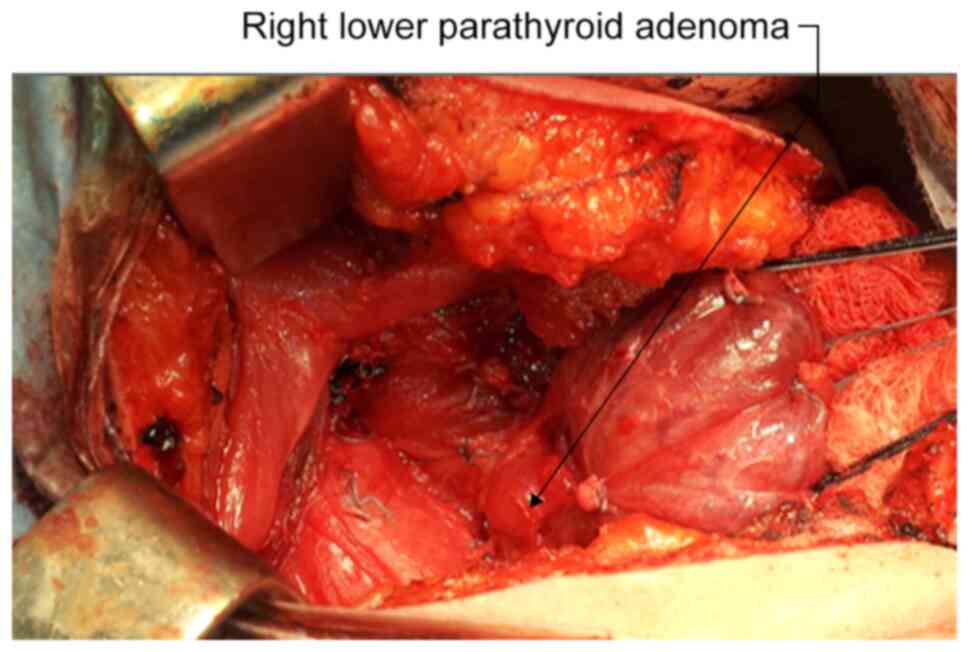
total of 6 patients required parathyroid autotransplantation. In
this context, parathyroid pseudotumoral (hyperplasia) formation was
detected. Excision of the gland was performed, 1/3 was sent for
histopathological examination and 2/3 was re-implanted at the level
of the right deltoid muscle and sternocleidomastoid muscles. Also
in these cases, the experience of the surgical team was necessary
for this attitude of preservation of the parathyroid tissue, aimed
to maintain the parathyroid function (Fig. 1).
Partially parathyroid autotransplantation in the
deltoid muscle after parathyroidectomy was made for PTH level
adjustment. Tissue samples were subsequently sent for evaluation to
the pathology department of the same hospital. The specimen samples
were fixated with 10% buffered formalin and were processed by
conventional histopathological methods using paraffin-embedding,
2-micron sectioning, and hematoxylin and eosin (H&E) staining.
Histopathological examination of the standard H&E-stained
slides revealed in most cases typical forms of parathyroid adenomas
and a few cases of parathyroid hyperplasia. The tumoral masses were
composed of chief cells, oncocytes (including transitional
oncocytes), or an admixture of these cell types. Pathological
anatomy examinations were analyzed for all of the surgically
operated patients. In 6 cases (11%) parathyroid hyperplasias were
found and in 49 cases (89%) parathyroid adenomas.
Primary result
The results of the laboratory analyses carried out
immediately postoperatively showed values close to the reference
ranges considered normal. No expanding hematoma was found in the
pretracheal space in any patient, neither laryngeal edema nor
dysphonia or phony.
Secondary results
At the check-up carried out 30 days after surgery,
all patients presented normal values of the reference serological
analyses provided in the protocols.
Discussion
Surgical treatment is necessary in the cases of
primary hyperparathyroidism and parathyroidectomy as a therapeutic
strategy is realized through numerous approaches (1,8,17). The
thoracic surgeon plays a very important role in the application of
the surgical treatment. The approaches for parathyroid surgery are
similar to the approaches for the thyroid (18-20).
Typical and ectopic anatomical localization of the pathological
parathyroid glands requires an experienced team in the surgery of
parathyroid and thyroid glands (21,22).
These localizations may often require surgery performed at the
anatomical border between the cervical and thoracic regions,
requiring several surgical specialties (otorhinolaryngology,
oromaxillofacial surgery, thoracic surgery). The localization of
these pseudotumoral formations at the level of the lower neck,
upper thorax, anterior mediastinum, paratracheal mediastinal
region, requires the experience of a thoracic surgeon (23). Our team of surgeons has developed
modified surgical approaches to the classical ones, as follows.
The modified Kocher cervical incision was used in
the situation of preoperative suspicion of parathyroid glandular
hyperplasia as a cause of primary hyperparathyroidism. This
incision, which the medical literature (24-26)
does not mention as such, consists of a suprasternal, symmetric
cervical incision, up to 3 cm long, centered on the midline of the
neck. We have successfully used it in surgeries performed for
parathyroid glandular hyperplasia because it has some advantages
over standard Kocher cervicotomy. Thus, in addition to the
aesthetic advantage, this incision allows better visualization and
dissection of the posterior face of the thyroid lobes to identify
the parathyroid gland quite difficult to observe and isolate in
rich perithyroidal fat. It also allows the bilateral approach of
the parathyroid glands. This incision is more important as we are
in the situation of lower parathyroid glandular hyperplasia. The
approach of the upper parathyroid hyperplasia was more difficult to
perform on this path. Another advantage of this incision is the
possibility to extend it bilaterally in the shape of the classical
Kocher cervical incision, in the situation required by the too-high
localization of glandular hyperplasia and in the case of
hyperplastic parathyroid glands inclavated intrathyroidal, which
may require the bulk removal of the parathyroid gland and the
thyroid lobe.
Mediastinoscopy allows easier visual identification
(by magnifying the video image) (27-29)
of parathyroid adenomas localized either peritracheal and
retro-vascular or at the level of the anterosuperior mediastinum
and permitted complete removal of parathyroid ectopic tumor
formations (30-32).
For the patients with a positive diagnosis of
hyperparathyroidism, we made a personalized surgical approach, with
a histopathological profile of excised parathyroid formations,
followed by endocrinological reassessment. The other patients were
referred to the endocrinology service.
In conclusion, the attitude of the diagnosis and the
surgical approach in hyperparathyroidism made by our team resulted
in the cure of patients with hyperparathyroidism associated with
parathyroid hyperplasia and parathyroid adenoma. The surgical
approaches aimed at total excision of the pathological formations
with minimal lesions, rapid healing, decrease in the number of days
of hospitalization, and early social reintegration.
Acknowledgements
Many thanks to ‘Dr. Carol Davila’ Central Military
Emergency University Hospital Bucharest, Romania and ‘Carol Davila’
University of Medicine and Pharmacy Bucharest for supporting our
study.
Funding
Funding: No funding was received.
Availability of data and materials
The data that support the findings of this study are
available from the corresponding author (CEN), upon reasonable
request.
Authors' contributions
CEN and AC recruited and carried out the patient
surgery. CSG was part of the operating team and performed data
collection and statistical analysis. FV and AVD processed the
biological samples collected by CEN and AC performed the
anatomopathological examination. All authors designed, read and
agreed to the published version of the manuscript.
Ethics approval and consent to
participate
The study was approved by the Research Ethics
Commission from ‘Dr. Carol Davila’ Central Military Emergency
University Hospital Bucharest (no. 388/3.06.2020).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Parnell KE and Oltmann SC: The surgical
management of primary hyperparathyroidism: An updated review. Int J
Endocr Oncol. 5(IJE07)2018.
|
|
2
|
DeLellis RA, Mazzaglia P and Mangray S:
Primary hyperparathyroidism: A current perspective. Arch Pathol Lab
Med. 132:1251–1262. 2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Silverberg SJ, Clarke BL, Peacock M,
Bandeira F, Boutroy S, Cusano NE, Dempster D, Lewiecki EM, Liu JM,
Minisola S, et al: Current issues in the presentation of
asymptomatic primary hyperparathyroidism: Proceedings of the fourth
international workshop. J Clin Endocrinol Metab. 99:3580–3594.
2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mizamtsidi M, Nastos C, Mastorakos G, Dina
R, Vassiliou I, Gazouli M and Palazzo F: Diagnosis, management,
histology and genetics of sporadic primary hyperparathyroidism: Old
knowledge with new tricks. Endocr Connect. 7:R56–R68.
2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Mamedova E, Mokrysheva N, Vasilyev E,
Petrov V, Pigarova E, Kuznetsov S, Kuznetsov N, Rozhinskaya L,
Melnichenko G, Dedov I and Tiulpakov A: Primary hyperparathyroidism
in young patients in Russia: High frequency of
hyperparathyroidism-jaw tumor syndrome. Endocr Connect. 6:557–565.
2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pappachan JM, Sodi R, Viswanath AK and
Lahart IM: Parathyroidectomy for adults with primary
hyperparathyroidism (Protocol). Cochrane Database Syst Rev.
2018(CD013035)2018.
|
|
7
|
National Institute for Health and Care
Excellence (NICE): Hyperparathyroidism (primary): Diagnosis,
assessment and initial management. NICE guideline [NG132].
https://www.nice.org.uk/guidance/ng132/chapter/Recommendations.
Accessed May 23, 2019.
|
|
8
|
Udelsman R, Åkerström G, Biagini C, Duh
QY, Miccoli P, Niederle B and Tonelli F: The surgical management of
asymptomatic primary hyperparathyroidism: Proceedings of the fourth
international workshop. J Clin Endocrinol Metab. 99:3595–3606.
2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Udelsman R, Lin Z and Donovan P: The
superiority of minimally invasive parathyroidectomy based on 1650
consecutive patients with primary hyperparathyroidism. Ann Surg.
253:585–591. 2011.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Wilhelm SM, Wang TS, Rua DT, Lee JA, Asa
SL, Duh QY, Doherty GM, Herrera MF, Pasieka JL, Perrier ND, et al:
The American association of endocrine surgeons guidelines for
definitive management of primary hyperparathyroidism. JAMA Surg.
151:959–968. 2016.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Nistor Cl, Ciuche A and Horvat T: Thoracic
Surgery. Vol IV. Mediastinal pseudotumors. Treaty of Surgery. 1st
edition. Romanian Academy Publishing House, Bucharest, pp701-704,
2008.
|
|
12
|
Spiroiu C, Ranetti AE and Nistor C: Giant
parathyroid adenoma with severe hypercalcaemia: Case report.
Endocrine Abstracts. 37(EP296)2015.
|
|
13
|
Nistor C, Davidescu M, Ciuche A, Rus O,
Tudose A, Vasilescu F and Horvat T: Giant multifocal thyroid tumor.
Maedica-a Journal of Clinical Medicine. 4:346–352. 2009.
|
|
14
|
Nistor C, Ciuche A, Motaş C, Motaş N,
Bluoss C, Pantile D, Davidescu M and Horvat T: Cervico-mediastinal
thyroid masses-our experience. Chirurgia (Bucur). 109:34–43.
2014.PubMed/NCBI
|
|
15
|
Nistor C, Ciuche A and Constantinescu I:
Emergency surgical tracheal decompression in a huge retrosternal
goiter. Acta Endocrinol (Buchar). 13:370–374. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
von Elm E, Altman DG, Egger M, Pocock SJ,
Gøtzsche PC and Vandenbroucke JP: STROBE Initiative. The
Strengthening the reporting of observational studies in
epidemiology (STROBE) statement: Guidelines for reporting
observational studies. Ann Intern Med. 147:573–577. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Song CM, Ji YB, Kim IS, Lee JY, Kim DS and
Tae K: Low transverse incision for lateral neck dissection in
patients with papillary thyroid cancer: Improved cosmesis. World J
Surg Oncol. 15(97)2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Noureldine SI, Gooi Z and Tufano RP:
Minimally invasive parathyroid surgery (Review). Gland Surg.
4:410–419. 2015.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Henry JF: Minimally invasive thyroid and
parathyroid surgery is not a question of length of the incision.
Langenbecks Arch Surg. 393:621–626. 2008.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Duke WS and Terris DJ: Alternative
approaches to the thyroid gland. Endocrinol Metab Clin North Am.
43:459–474. 2014.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mazeh H, Stoll SJ, Robbins JB, Sippel RS
and Chen H: Validation of the ‘Perrier’ parathyroid adenoma
location nomenclature. World J Surg. 36:612–616. 2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Simo R, Nixon I, Tysome JR, Balfour A and
Jeannon JP: Modified extended Kocher incision for total
thyroidectomy with lateral compartment neck dissection-a critical
appraisal of surgical access and cosmesis in 31 patients. Clin
Otolaryngol. 37:395–398. 2012.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Irvin GL III, Carneiro DM and Solorzano
CC: Progress in the operative management of sporadic primary
hyperparathyroidism over 34 years. Ann Surg. 239:704–708;
discussion 708-711. 2004.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Runge T, Inglin R, Riss P, Selberherr A,
Kaderli RM, Candinas D and Seiler CA: The advantages of extended
subplatysmal dissection in thyroid surgery-the ‘mobile window’
technique. Langenbecks Arch Surg. 402:257–263. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Lin N, Yu L, Ma J and Wang Y: Minimally
invasive non-endoscopic thyroidectomy with a low anterior cervical
incision. Clin Oncol. 6(Article 1776)2021.
|
|
26
|
Elkanovich T, Hajouj M and Ronen O: The
natural neck crease as an anatomic landmark for thyroid surgery
incision. Surgeon. 30:S1479–S1666. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Spear C, Geraci T, Bizekis C and Zervos M:
Resection of an ectopic parathyroid adenoma via video-assisted
mediastinoscopy. Semin Thorac Cardiovasc Surg. 31:323–325.
2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Liman ST, Topcu S, Dervisoglu E, Gorur GD,
Elicora A, Burc K and Akgul AG: Excision of ectopic mediastinal
parathyroid adenoma via parasternal videomediastinoscopy. Ann
Thorac Cardiovasc Surg. 20:67–69. 2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Röösli C, Bortoluzzi L, Linder TE and
Müller W: Role of minimal invasive surgery for primary and
secondary hyperparathyroidism. Laryngorhinootologie. 88:460–464.
2009.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
30
|
Razzak R, McMullen T and Bédard ELR:
Excision of middle mediastinal parathyroid adenoma by videoscopic
assisted mediastinoscopy (VAM). J Thorac Dis. 8:2651–2653.
2016.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Tcherveniakov P, Menon A, Milton R,
Papagiannopoulos K, Lansdown M and Thorpe JA: Video-assisted
mediastinoscopy (VAM) for surgical resection of ectopic parathyroid
adenoma. J Cardiothorac Surg. 2(41)2007.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Toktaş O, İliklerden Ü, Yerlikaya B, Kotan
Ç and Batur A: Transcervical resection of two parathyroid adenomas
located on the anterior mediastinum. Turk J Surg. 34:247–249.
2018.PubMed/NCBI View Article : Google Scholar
|