1. Introduction
In a clinically-based consensus report, pelvic organ
prolapse (POP) was defined as 'the downward descent of the anterior
or posterior vaginal wall, the uterus and the vaginal vault into or
through the vagina' (1). In total,
30-76% of females present with POP during routine gynecological
examinations, even in the absence of specific alarming symptoms
(2). This condition may have a
negative impact on sexual life, body image and quality of life
(2). According to a study performed
by Wu et al (3), the number
of females with POP is expected to increase to 46% and is estimated
to reach 4.9 million by 2050. Aging increases the incidence of POP,
which requires significant costs and causes a financial burden to
the healthcare system.
POP is a multifactorial disease and pregnancy is the
most common risk factor for its development. Labor directly damages
the pelvic floor muscles and connective tissues (4). A prospective ultrasound study
indicated that the incidence of pelvic floor muscle injury was
associated with POP and its incidence ranged from 21-36% following
vaginal delivery (5). In addition,
prior to hysterectomy, estrogen levels, parity, age, body mass
index (BMI) and sustained elevated intra-abdominal pressure,
including obesity, chronic cough, constipation and repeated
weight-bearing, may also contribute to prolapse (6).
It is worth noting that the aforementioned
macroscopic factors cannot fully clarify the pathogenesis of POP,
which may not occur in all females exposed to these risk factors.
Therefore, prolapse may also affect females who do not present with
these conditions. Therefore, it is imperative to fully investigate
the mechanisms of action of POP. The molecular mechanism of POP and
the key genes involved in its development have been studied
in-depth using bioinformatic approaches, such as genetic
engineering and gene expression profiling chips. In the present
review article, a summary of the latest advances of the molecular
mechanisms of POP is provided, with a view to provide novel
perspectives in elucidating the pathogenesis, identifying
prevention methods and improving the means of diagnosis and
treatment.
2. Methods
A comprehensive search of relevant systematic
reviews and articles was performed using the PubMed and Google
Scholar databases. This review adheres to Preferred Reporting Items
for Systematic reviews and Meta-Analyses guidelines (7). The publication years ranged between
2005 and 2020. To expand the retrieval scope, the 'pelvic floor
dysfunction' (PFD) concept was introduced. The search strategies
included the following Mesh terms: ‘Pelvic organ prolapse’ and
‘pelvic floor dysfunction’; ‘PFD’ and ‘POP’; ‘etiology’ and
‘mechanism’. Furthermore, citation tracking of the studies
retrieved was used to identify additional relevant articles, which
were obtained using Google Scholar. Table I illustrates the general idea of the
study and the cited references, correspondingly.
 | Table IMolecular mechanisms of pelvic organ
prolapse. |
Table I
Molecular mechanisms of pelvic organ
prolapse.
| Category | Factors | (Refs.) |
|---|
| Reduction of
ECM | | |
|
Reduced
anabolism | TGF-β1 | (9-13,18) |
| | HOXA11 | (14-18) |
| | FBLN5 | (20,21) |
| | LOXL1 | (22-25,68) |
|
Increased
catabolism | MMPs/TIMPs,
elastases | (10,11,16,18,20,27-30) |
| Activation of
oxidative stress | NAa | (32-38) |
| Genetic
susceptibility | NA | Table
IIb |
| Reduction of
neurotransmitters | VIP | (63,64) |
| | NPY | (63,64,68) |
| Reduction of
estrogen infiltration | NA | (65-67) |
3. Mechanisms underlying POP
The molecular mechanisms of POP are complex and have
remained to be fully elucidated. They may be divided into the
following aspects: i) Reduction of the extracellular matrix (ECM)
in pelvic floor connective tissue; ii) activation of oxidative
stress (OS); iii) genetic susceptibility; iv) denervation of the
pelvic floor; and v) reduction of estrogen infiltration (Fig. 1).
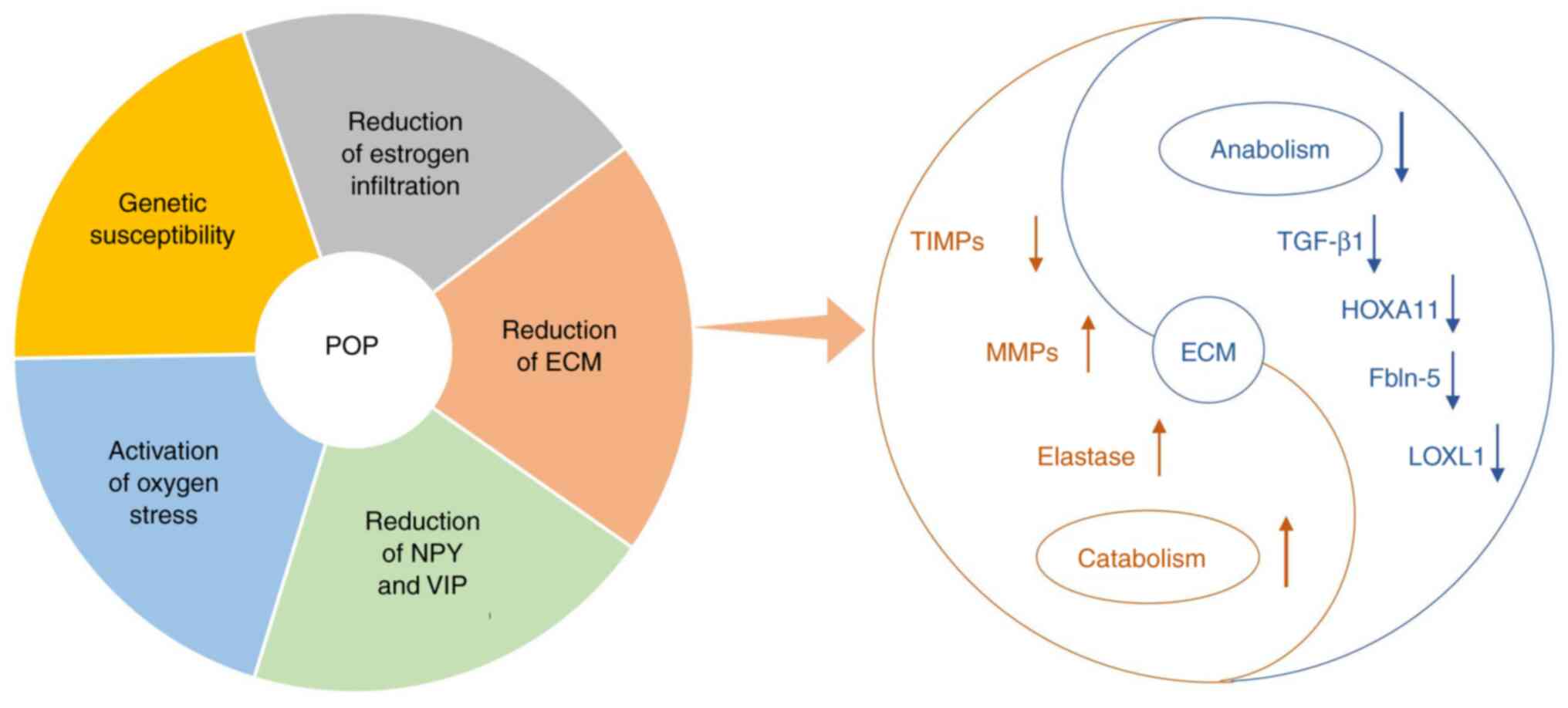 | Figure 1Overview diagram of the article. (A)
Pie chart of the five core factors of POP. (B) Specific molecular
mechanisms involved in the reduction of ECM. POP, pelvic organ
prolapse; ECM, extracellular matrix; TGF-β1, transforming growth
factor-β1; HOXA11, homeobox A11; FBLN5, fibulin-5; LOXL1, lysyl
oxidases-like protein 1; MMPs, matrix metalloproteinases; TIMPs,
tissue inhibitors of MMP; NPY, neuropeptide; VIP, vasoactive
intestinal peptide. |
Reduced ECM and POP
The connective tissue of the pelvic floor is
composed of nerves, muscles, ligaments and fascia, and supports the
female pelvic organs. The fibroblasts secrete collagen and elastin,
which are the essential components of the ECM that provide strength
and flexibility to the pelvic floor (8). To the best of our knowledge, reduced
ECM metabolism in pelvic floor connective tissue, including reduced
anabolism and increased catabolism, is the predominant pathogenic
mechanism of POP.
Reduced anabolism of ECM
The research hotspot in the field of collagen
synthesis is transforming growth factor-β1 (TGF-β1), a typical
multifunctional cytokine, which broadly regulates various
biological functions and has been indicated to be involved in the
synthesis of connective tissue (9).
It has been confirmed that decreased mRNA and protein expression
levels of TGF-β1 are associated with the severity of POP (10). Pretreatment with TGF-β1 activates
the TGF-β1/Smad signaling pathway, thereby attenuating the loss of
ECM (11). Investigation of its
mechanistic involvement in chronic kidney diseases and idiopathic
pulmonary fibrosis has resulted in the conclusion that TGF-β1
promotes collagen synthesis via the following methods: i)
Activation of downstream signaling pathways, such as the
TGF-β1/Smad pathway; ii) increased de novo synthesis of
serine; and iii) increased expression of protease inhibitors
(12,13). It is reasonable to hypothesize that
downregulation of TGF-β1 hinders collagen synthesis, interferes
with ECM metabolism and ultimately affects the occurrence and
development of POP.
In addition, a previous study published in 2008
reported that the homeobox A11 (HOXA11) gene, which is a
transcriptional regulator, is key to the balance of collagen
metabolism and its deficiency was associated with a decrease in
collagen content (14). Another
study had indicated that HOXA11 inhibits the expression of p53, a
tumor suppressor gene, which controls the progression of the cell
cycle (15). This may be a
mechanism via which HOXA11 regulates collagen synthesis. In
addition, it has been demonstrated that the expression levels of
matrix metalloproteinase (MMP) enzymes are increased, while those
of tissue inhibitors of MMP (TIMPs) are decreased following
knockdown of HOXA11 expression, which in turn increases the
degradation of ECM, suggesting that a deficiency in HOXA11 disrupts
the balance of collagen metabolism and eventually contributes to
POP (16). A study indicated that
the expression levels of microRNA (miRNA/miR)-30D and miR-181A in
patients with POP were negatively correlated with HOXA11 mRNA
levels; it was hypothesized that these miRNAs regulate the
expression of HOXA11 and may be used as therapeutic targets for POP
(17).
The above findings suggest that HOXA11 and TGF-β1
exert a synergistic effect on the expression of collagen and MMP
enzymes. These two signaling mediators have important roles in the
development of ECM, as demonstrated by a recent study (18). The balanced turnover of collagen is
necessary for maintaining the mechanical strength of pelvic
supportive connective tissues.
The major components of ECM are elastic fibers and
collagen. Elastic fibers are able to maintain the integrity of
pelvic organs and vaginal structures to resist mechanical strain
due to its elasticity and recoil properties (18). Patients with POP exhibit weakened
flexibility of elastin and increased flexibility of elastase, which
disrupts the mechanical balance of the pelvic floor (19). Fibulin-5 (FBLN5) and lysyl
oxidase-like protein 1 (LOXL1) have attracted considerable
attention due to their major roles in the synthesis of elastic
fibers (20-25).
FBLN5 is an integrin-bound matricellular protein
required for elastic fiber assembly; it exerts dual effects by
ensuring normal assembly of elastic fibers and inhibiting the
activity of MMP9 to maintain the biomechanical integrity of the
pelvic floor and prevent the development of POP (20). An additional study indicated that
FBLN5 inhibits upregulation of MMP9 by inhibiting β1
integrin-dependent and fibronectin-mediated pathways (21).
LOXL1 is involved in the cross-linking of
tropoelastin monomers and interacts with FBLN5(22). It serves both as a cross-linking
enzyme and as an element of the scaffold, having an essential role
in the synthesis and assembly of elastic fibers (23). Previous studies have clarified that
defect in the synthesis of elastic fibers caused by decreased
expression of FBLN5 and LOXL1 contribute to POP (24,25).
It was recently determined that the coexpression of LOXL1 and bone
morphogenetic protein has a significant impact on the regulation of
postpartum connective tissue metabolism in mice (22).
In summary, the disordered elastic fiber homeostasis
may weaken the function of the stent, which is one of the primary
events in the pathogenesis of POP.
Increased catabolism of ECM
MMPs mainly include MMP1, -2, -3 and -9. These
enzymes are capable of degrading collagen and other ECM components
(26). A previous study indicated
that overexpression of MMP2 is a harmful factor for POP (27). In patients with POP, the expression
levels of MMP2/9 in the pelvic floor tissue were increased, while
those of TIMPs, which antagonize MMP action, were decreased
(16). Therefore, MMPs and TIMPs
are considered the key factors of regulating ECM degradation. In
addition, it has been reported that TGF-β1 stimulates the synthesis
of TIMP-2 and inhibits the activity of MMP2/9 via the TGF-β1/Smad3
signaling pathway, thereby reducing the loss of ECM (10,11).
However, an additional study that utilized a rainbow trout heart
fibrosis model indicated that following 24 h of TGF-β1 treatment,
the transcription levels of TIMP-2 and MMP9 were increased
(28). Heterogeneity among studies,
such as differences in research methods, sample sizes, research
subjects, locations of biopsy materials and genetic background, may
lead to such distinct outcomes.
A previous study compared the expression levels of
various elastases in vaginal tissues of female patients with pelvic
floor dysfunction and confirmed that increased elastin metabolism
may alter the mechanical properties of supporting tissues (29). A subsequent study indicated that
increased expression of elastase causes rupture of elastic fibers,
leading to the destruction of the structural integrity of the
pelvic floor and increased risk of prolapse (30).
In summary, MMP and TIMP functions are balanced in
order to regulate ECM anabolism. HOXA11, TGF-β1 and FBLN5 influence
the expression of MMPs (16,18,20).
It may be considered that the anabolism and catabolism of ECM are
inseparable and intricate. Decreased anabolism and increased
catabolism are key factors for the onset of POP.
4. OS and POP
OS may cause increased oxidative modification of
DNA, lipids and proteins, and induce mitochondrial apoptosis
(31). Its role in the pathogenesis
of POP has received increased attention. OS is indicated to be able
to interfere with key points of elastic fiber assembly and reduce
the quality of elastin (32). A
previous study published in 2013 indicated that the balance of
oxidation and antioxidation in females with POP was disrupted,
which increased the levels of reactive oxygen species (ROS) and
downregulated the TGF-β1 signaling pathway. This caused inhibition
of collagen synthesis and damage to the pelvic support structure
(33). In addition, it has been
reported that the levels of 8-hydroxy-2-deoxyguanosine and
4-hydroxynonenal, which are biomarkers of oxidative damage and may
be used to determine OS and mitochondrial apoptosis, are involved
in the pathological process of POP (34). Another study determined that the
levels of ROS and the apoptotic rate of fibroblasts were enhanced
following an increase in mechanical stress, which indicates that
mechanical strain promotes the development of POP by activating ROS
(35). A further study concluded
that mechanical strain may activate the PI3K/AKT-mediated OS
signaling pathway, thereby promoting the apoptosis and senescence
of pelvic fibroblasts, and reducing the production of collagen
(36). A subsequent study also
confirmed this notion (37).
Furthermore, reduced OS has been indicated to promote collagen
synthesis, while its overexpression may interfere with the
homeostasis and metabolism of ECM by affecting the levels of
MMPs/TIMPs and the activation of the TGF-β1/Smad signaling pathway,
which in turn results in induction of POP (38).
Based on these results, it is hypothesized OS
hinders the balance of MMPs/TIMPs and interferes with the
TGF-β1/Smad pathway, which negatively affects the production of
elastic fibers, thereby destroying the pelvic floor support network
and ultimately leading to the occurrence of POP.
5. Genetic susceptibility and POP
It is becoming increasingly accepted that
fertility-associated factors are the most common pathogenic driving
factors of POP. However, this cannot fully explain the development
of POP in nulliparous females without any known risk factors. In
addition, the notable medical history of POP is not only based on
the obstetric and gynecological history, but also on the family
history. In the case of a positive family history, the risk of POP
is increased. Table II displays
the evidence that indicates that genetic factors may be involved in
the development of POP. The majority of the gene mutations
currently known to be associated with POP are located in the coding
regions of the genes encoding for the aforementioned proteins, such
as TGF-β1, FBLN5 and LOXL1. These mutations may lead to changes in
the functions of those molecules and to the development of POP with
the combined action of environmental factors.
| Table IISusceptibility genes of POP. |
Table II
Susceptibility genes of POP.
| Genetic entity | Proven
susceptibilitya,
yes/no | (Refs.) |
|---|
| COL3A1
rs1800255 | Yes | (39,40,42,45) |
| | No | (41,43,44,46) |
| COL1A1
rs1800012 | Yes | (46) |
| | No | (49,51) |
| LAMC1
rs10911193 | No | (46,48,52) |
| ESR1 rs2228480 | Yes | (47,48) |
| | No | (49) |
| PGR rs484389 | Yes | (53) |
| MMP1 | Yes | (51) |
| | No | (46) |
| HOXA11 | No | (49) |
| LOXL1 | Yes | (54) |
| FBLN5 | Yes | (55) |
| | No | (56) |
| Chromosomes
9q21/10q24-26/17q25 | Yes | (57-59) |
The genetic polymorphism of the collagen type III α
1 (COL3A1) gene leads to amino acid changes in the cy1 (III) chain,
which may interfere with the mechanical properties of type III
collagen and affect the supporting structure of the pelvic floor.
The single nucleotide polymorphism (SNP) G/A rs1800255 is located
in the coding region of COL3A1 and has been evaluated as a possible
risk factor for POP (39-45).
The conclusions of research on this aspect are conflicting. A
systematic review has summarized pedigree studies on POP published
in 2005-2013 and concluded that only the presence of the rs1800012
polymorphism of COL1A1 was associated with the incidence of POP,
while the rs1800255 polymorphism of COL3A1 did not exhibit any
significant association with the development of this disease
(46). However, a previous study
published in 2014 performed a genetic epidemiological assessment on
POP and demonstrated that the probability of developing the disease
increased to 4.79-fold in the presence of the COL3A1 rs1800255
genotype (45). This study further
demonstrated that the polymorphic site rs2228480 of the estrogen
receptor α, which is encoded by estrogen receptor 1 (ESR1), was a
susceptibility factor for the development of POP, which was
subsequently confirmed by additional studies (47,48),
although conflicting results have also been reported (49). A previous study indicated that
miR-221 and miR-222, two regulatory factors of ESR1, negatively
regulate the expression of ESR1 in patients with POP (50). The aforementioned results
demonstrated that the ESR1 genotype may be a predisposing factor
for POP and that it may be used as a potential therapeutic target
for this disease. Apart from the aforementioned genes (COL3A1
rs1800255; COL1A1 rs1800012; ESR1 rs2228480), other genes involved
in the occurrence and development of POP have been discovered,
including MMP1, laminin γ-1 rs10911193, progesterone receptor
rs484389, LOXL1 and common SNPs of the FBLN5 gene (rs2018736,
rs12589592) (48,51-56).
In addition, genome-wide association studies have determined that
the presence of chromosomes 9q21, 10q24-26 and 17q25 is associated
with the susceptibility of European patients with POP (57-59).
However, the susceptibility loci on these chromosomes remain to be
identified (60).
From aforementioned research, it is important to
note that several research results are contradictory, as indicated
in Table II. As stated by
Cartwright ‘many studies were at high risk of bias from genotyping
error or population stratification’ (46), which may contribute the
contradictory results. In addition, the heterogeneity among studies
in terms of differences in the genetic background of participants
and gene sequencing methods may also led to inconsistent results.
The rapid development of gene expression analysis and
high-throughput sequencing technology has enabled the successful
identification of genes and pathways that may provide detailed
information on the molecular mechanisms underlying POP (61,62).
These genes may be used as potential biomarkers of POP.
6. Reduction in the levels of
neurotransmitters of the pelvic floor
It is well accepted that vaginal delivery and
multiple pregnancies lead to overstretching of the pelvic floor
nerves and muscles. During this process, the nerves suffer more
damage due to their weaker ability to withstand traction compared
with that of the muscles (63).
Abnormalities in peptide neurotransmitters, notably vasoactive
intestinal peptide (VIP) and neuropeptide (NPY), reflect the degree
of denervation of the pelvic floor structure, promote pelvic and
vaginal blood flow and serve as a critical marker for evaluating
pelvic floor nerve injury (64).
Accumulating evidence has demonstrated that the expression levels
of VIP and NPY in patients with POP are decreased (63,64).
Their absence results in changes in blood flow, muscle atrophy,
local nutritional insufficiency and ultimately dysfunction in the
pelvic floor of females. Furthermore, the decreased expression
levels are associated with the severity of the symptoms (63,64).
To date, only a small number of studies have been performed to
assess the levels of neuropeptides in the pelvic floor, and the
scope to explore the underlying mechanisms of chemical transmitter
loss following nerve damage remains limited.
7. Reduced content of estrogen
It has been indicated that increased risk of pelvic
floor disease following menopause may be associated with estrogen
deficiency, whereas changes in the expression of estrogen receptors
also affect the risk to females of developing POP (65). A previous study demonstrated that
estrogen may increase collagen turnover and positively affect
pelvic floor tissue (66).
Furthermore, estrogen has been indicated to stimulate and increase
collagen content, thereby enhancing the resistance of the pelvic
floor network structure (67). It
is now widely accepted that following menopause, the secretion of
estrogen in females decreases rapidly and the connective tissue
cannot be repaired effectively, which weakens the function of the
supporting network. Furthermore, it has been indicated that
estrogen affects the content of LOXL1 and the distribution of NPY
(68).
Consequently, exogenous estrogen has long been
suggested for the treatment or prevention of POP. It is able to
improve the homeostasis of the pelvic floor; however, it has been
noted to have certain side effects, such as dizziness, endometrial
disease, uterine fibroids and endocrine disorders (69). Although its therapeutic effects have
been reported, there is still insufficient evidence to prove its
effectiveness. According to a 2017 retrospective observational
study, the use of exogenous estrogen and its substitutes has
limited benefits for genitourinary syndrome in menopausal females
(70). Therefore, the effectiveness
and safety of this treatment should be reviewed comprehensively and
systematically.
8. Discussion
Although POP is not life-threatening, it may be
painful, embarrassing and uncomfortable. Its incidence and
prevalence increase with age. The risk factors for POP are
considered to include age, parity, vaginal delivery, obesity,
diabetes, previous hysterectomy and connective tissue diseases. To
prevent POP, the BMI is the only risk factor that may be
controlled. Generally speaking, parity and delivery methods may be
changed, whereas in practice, POP is rarely taken into
consideration. Therefore, it is crucial to further explore its
underlying molecular mechanisms, unravel the complex causal network
composed of factors such as heredity, reproductive factors and
lifestyle, and seek improved prevention and treatment targets.
Since the technology on bioinformatics and gene microarray had made
great progress in in recent years, the revision and supplementation
of previous data is required.
The present review summarized the molecular
mechanisms of POP into five aspects, including the metabolism of
ECM, OS activation, genetic susceptibility, pelvic floor
denervation and reduction of estrogen infiltration. In addition,
the following strategies are proposed with regard to prevention: i)
High-risk groups should attempt to avoid pathological conditions
with increased abdominal pressure, such as chronic cough; and ii)
females with a family history should undergo genetic testing and
POP screening as soon as possible. Furthermore, the following
strategies were adopted with regard to treatment: i) Although the
use of estrogen following menopause may be promising, further
investigation is required to confirm its efficacy; ii) the choice
of treatment method (conservative or surgery) should rely on the
collaboration between specialized teams and shared decision-making
with patients; and iii) in addition to improving the symptoms of
the patients, attention should be paid to their quality of life and
mental health. Investing additional manpower and resources to
systematically evaluate the mechanisms of POP is beneficial to both
prevention and treatment. Comprehensive utilization of
multidisciplinary approaches may provide breakthroughs and novel
ideas for studying the pathogenesis of POP.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by the Key Research and
Development Program of Hubei Province (grant no. 2020BCB023), the
China Graduate School of Graduate Education Fund Project (grant no.
B2-YX20180302-19), the Renmin Hospital of Wuhan University Guidance
Fund Project (grant no. RMYD2018M05) and the Education and Teaching
Reform Research Project of Wuhan University (grant no.
413200095).
Availability of data and materials
Not applicable.
Authors' contributions
ZMD conceived and designed the study. FFD, MQY, DYY
and YJZ performed the literature search. ZMD drafted the manuscript
and prepared the tables. YXC revised the manuscript and acquired
funding. All authors read and approved the final manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Haylen BT, Maher CF, Barber MD, Camargo S,
Dandolu V, Digesu A, Goldman HB, Huser M, Milani AL, Moran PA, et
al: An International Urogynecological Association (IUGA) /
International Continence Society (ICS) joint report on the
terminology for female pelvic organ prolapse (POP). Int Urogynecol
J Pelvic Floor Dysfunct. 27:165–194. 2016.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Barber MD: Pelvic organ prolapse. BMJ.
354(i3853)2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wu JM, Hundley AF, Fulton RG and Myers ER:
Forecasting the prevalence of pelvic floor disorders in U.S. Women:
2010 to 2050. Obstet Gynecol. 114:1278–1283. 2009.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Iglesia CB and Smithling KR: Pelvic Organ
Prolapse. Am Fam Physician. 96:179–185. 2017.PubMed/NCBI
|
|
5
|
van Delft K, Sultan AH, Thakar R,
Schwertner-Tiepelmann N and Kluivers K: The relationship between
postpartum levator ani muscle avulsion and signs and symptoms of
pelvic floor dysfunction. BJOG. 121:1164–1172. 2014.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Friedman T, Eslick GD and Dietz HP: Risk
factors for prolapse recurrence: Systematic review and
meta-analysis. Int Urogynecol J Pelvic Floor Dysfunct. 29:13–21.
2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Moher D, Liberati A, Tetzlaff J and Altman
DG: PRISMA Group. Preferred reporting items for systematic reviews
and meta-analyses: the PRISMA statement. BMJ.
339(b2535)2009.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Chen B and Yeh J: Alterations in
connective tissue metabolism in stress incontinence and prolapse. J
Urol. 186:1768–1772. 2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yang L, Pang Y and Moses HL: TGF-beta and
immune cells: An important regulatory axis in the tumor
microenvironment and progression. Trends Immunol. 31:220–227.
2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Liu C, Wang Y, Li BS, Yang Q, Tang JM, Min
J, Hong SS, Guo WJ and Hong L: Role of transforming growth factor β
1 in the pathogenesis of pelvic organ prolapse: A potential
therapeutic target. Int J Mol Med. 40:347–356. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Min J, Li B, Liu C, Guo W, Hong S, Tang J
and Hong L: Extracellular matrix metabolism disorder induced by
mechanical strain on human parametrial ligament fibroblasts. Mol
Med Rep. 15:3278–3284. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Meng XM, Nikolic-Paterson DJ and Lan HY:
TGF-β: The master regulator of fibrosis. Nat Rev Nephrol.
12:325–338. 2016.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Nigdelioglu R, Hamanaka RB, Meliton AY,
O'Leary E, Witt LJ, Cho T, Sun K, Bonham C, Wu D, Woods PS, et al:
Transforming Growth Factor (TGF)-β Promotes De Novo Serine
Synthesis for Collagen Production. J Biol Chem. 291:27239–27251.
2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Connell KA, Guess MK, Chen H, Andikyan V,
Bercik R and Taylor HS: HOXA11 is critical for development and
maintenance of uterosacral ligaments and deficient in pelvic
prolapse. J Clin Invest. 118:1050–1055. 2008.PubMed/NCBI View
Article : Google Scholar
|
|
15
|
Connell KA, Guess MK, Chen HW, Lynch T,
Bercik R and Taylor HS: HOXA11 promotes fibroblast proliferation
and regulates p53 in uterosacral ligaments. Reprod Sci. 16:694–700.
2009.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ma Y, Guess M, Datar A, Hennessey A,
Cardenas I, Johnson J and Connell KA: Knockdown of Hoxa11 in vivo
in the uterosacral ligament and uterus of mice results in altered
collagen and matrix metalloproteinase activity. Biol Reprod.
86(100)2012.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Jeon MJ, Kim EJ, Lee M, Kim H, Choi JR,
Chae HD, Moon YJ, Kim SK and Bai SW: MicroRNA-30d and microRNA-181a
regulate HOXA11 expression in the uterosacral ligaments and are
overexpressed in pelvic organ prolapse. J Cell Mol Med. 19:501–509.
2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhang L, Dai F, Chen G, Wang Y, Liu S,
Zhang L, Xian S, Yuan M, Yang D, Zheng Y, et al: Molecular
mechanism of extracellular matrix disorder in pelvic organ
prolapses. Mol Med Rep. 22:4611–4618. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Chin K, Wieslander C, Shi H, Balgobin S,
Montoya TI, Yanagisawa H and Word RA: Pelvic Organ Support in
Animals with Partial Loss of Fibulin-5 in the Vaginal Wall. PLoS
One. 11(e0152793)2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Northington GM: Fibulin-5: Two for the
price of one maintaining pelvic support. J Clin Invest.
121:1688–1691. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Budatha M, Roshanravan S, Zheng Q,
Weislander C, Chapman SL, Davis EC, Starcher B, Word RA and
Yanagisawa H: Extracellular matrix proteases contribute to
progression of pelvic organ prolapse in mice and humans. J Clin
Invest. 121:2048–2059. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
22
|
Borazjani A, Couri BM, Kuang M, Balog BM
and Damaser MS: Role of lysyl oxidase like 1 in regulation of
postpartum connective tissue metabolism in the mouse vagina. Biol
Reprod. 101:916–927. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Liu X, Zhao Y, Gao J, Pawlyk B, Starcher
B, Spencer JA, Yanagisawa H, Zuo J and Li T: Elastic fiber
homeostasis requires lysyl oxidase-like 1 protein. Nat Genet.
36:178–182. 2004.PubMed/NCBI View
Article : Google Scholar
|
|
24
|
Zhao BH and Zhou JH: Decreased expression
of elastin, fibulin-5 and lysyl oxidase-like 1 in the uterosacral
ligaments of postmenopausal women with pelvic organ prolapse. J
Obstet Gynaecol Res. 38:925–931. 2012.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kufaishi H, Alarab M, Drutz H, Lye S and
Shynlova O: Comparative Characterization of Vaginal Cells Derived
From Premenopausal Women With and Without Severe Pelvic Organ
Prolapse. Reprod Sci. 23:931–943. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Cui N, Hu M and Khalil RA: Biochemical and
Biological Attributes of Matrix Metalloproteinases. Prog Mol Biol
Transl Sci. 147:1–73. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Phillips CH, Anthony F, Benyon C and Monga
AK: Collagen metabolism in the uterosacral ligaments and vaginal
skin of women with uterine prolapse. BJOG. 113:39–46.
2006.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Johnston EF and Gillis TE: Transforming
growth factor beta-1 (TGF-β1) stimulates collagen synthesis in
cultured rainbow trout cardiac fibroblasts. J Exp Biol.
220:2645–2653. 2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Chen B, Wen Y and Polan ML: Elastolytic
activity in women with stress urinary incontinence and pelvic organ
prolapse. Neurourol Urodyn. 23:119–126. 2004.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Akintunde A, Robison KM, Capone D,
Desrosiers L, Knoepp LR and Miller KS: Effects of elastase
digestion on the murine vaginal wall biaxial mechanical response. J
Biomech Eng. 141:0210111–02101111. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sosa V, Moliné T, Somoza R, Paciucci R,
Kondoh H and LLeonart ME: Oxidative stress and cancer: an overview.
Ageing Res Rev. 12:376–990. 2013.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Akhtar K, Broekelmann TJ, Miao M, Keeley
FW, Starcher BC, Pierce RA, Mecham RP and Adair-Kirk TL: Oxidative
and nitrosative modifications of tropoelastin prevent elastic fiber
assembly in vitro. J Biol Chem. 285:37396–37404. 2010.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Li BS, Hong L, Min J, Wu DB, Hu M and Guo
WJ: The expression of glutathione peroxidase-1 and the anabolism of
collagen regulation pathway transforming growth
factor-beta1-connective tissue growth factor in women with uterine
prolapse and the clinic significance. Clin Exp Obstet Gynecol.
40:586–590. 2013.PubMed/NCBI
|
|
34
|
Kim EJ, Chung N, Park SH, Lee KH, Kim SW,
Kim JY, Bai SW and Jeon MJ: Involvement of oxidative stress and
mitochondrial apoptosis in the pathogenesis of pelvic organ
prolapse. J Urol. 189:588–594. 2013.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Hong S, Li H, Wu D, Li B, Liu C, Guo W,
Min J, Hu M, Zhao Y and Yang Q: Oxidative damage to human
parametrial ligament fibroblasts induced by mechanical stress. Mol
Med Rep. 12:5342–5348. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Li BS, Guo WJ, Hong L, Liu YD, Liu C, Hong
SS, Wu DB and Min J: Role of mechanical strain-activated PI3K/Akt
signaling pathway in pelvic organ prolapse. Mol Med Rep.
14:243–253. 2016.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Fang G, Hong L, Liu C, Yang Q, Zhang Q, Li
Y, Li B, Wu D, Wu W and Shi H: Oxidative status of cardinal
ligament in pelvic organ prolapse. Exp Ther Med. 16:3293–3302.
2018.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Stewart AG, Thomas B and Koff J: TGF-β:
Master regulator of inflammation and fibrosis. Respirology.
23:1096–1097. 2018.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Chen HY, Chung YW, Lin WY, Wang JC, Tsai
FJ and Tsai CH: Collagen type 3 alpha 1 polymorphism and risk of
pelvic organ prolapse. Int J Gynaecol Obstet. 103:55–58.
2008.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Jeon MJ, Chung SM, Choi JR, Jung HJ, Kim
SK and Bai SW: The relationship between COL3A1 exon 31 polymorphism
and pelvic organ prolapse. J Urol. 181:1213–1216. 2009.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Martins KF, de Jármy-DiBella ZI, da
Fonseca AM, Castro RA, da Silva ID, Girão MJ and Sartori MG:
Evaluation of demographic, clinical characteristics, and genetic
polymorphism as risk factors for pelvic organ prolapse in Brazilian
women. Neurourol Urodyn. 30:1325–1328. 2011.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Ricard-Blum S: The collagen family. Cold
Spring Harb Perspect Biol. 3(a004978)2011.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Lince SL, van Kempen LC, Dijkstra JR,
IntHout J, Vierhout ME and Kluivers KB: Collagen type III alpha 1
polymorphism (rs1800255, COL3A1 2209 G>A) assessed with
high-resolution melting analysis is not associated with pelvic
organ prolapse in the Dutch population. Int Urogynecol J Pelvic
Floor Dysfunct. 25:1237–1242. 2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Teixeira FH, Fernandes CE, do Souto RP and
de Oliveira E: Polymorphism rs1800255 from COL3A1 gene and the risk
for pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct.
31:73–78. 2020.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Ward RM, Velez Edwards DR, Edwards T, Giri
A, Jerome RN and Wu JM: Genetic epidemiology of pelvic organ
prolapse: A systematic review. Am J Obstet Gynecol. 211:326–335.
2014.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Cartwright R, Kirby AC, Tikkinen KA,
Mangera A, Thiagamoorthy G, Rajan P, Pesonen J, Ambrose C,
Gonzalez-Maffe J, Bennett P, et al: Systematic review and
metaanalysis of genetic association studies of urinary symptoms and
prolapse in women. Am J Obstet Gynecol. 212:199. e191–124.
2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Moon YJ, Bai SW, Jung CY and Kim CH:
Estrogen-related genome-based expression profiling study of
uterosacral ligaments in women with pelvic organ prolapse. Int
Urogynecol J Pelvic Floor Dysfunct. 24:1961–1967. 2013.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Nakad B, Fares F, Azzam N, Feiner B,
Zilberlicht A and Abramov Y: Estrogen receptor and laminin genetic
polymorphism among women with pelvic organ prolapse. Taiwan J
Obstet Gynecol. 56:750–754. 2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Dökmeci F, Tekşen F, Çetinkaya SE, Özkan
T, Kaplan F and Köse K: Expressions of homeobox, collagen and
estrogen genes in women with uterine prolapse. Eur J Obstet Gynecol
Reprod Biol. 233:26–29. 2019.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Shi Z, Zhang T, Zhang L, Zhao J, Gong J
and Zhao C: Increased microRNA-221/222 and decreased estrogen
receptor α in the cervical portion of the uterosacral ligaments
from women with pelvic organ prolapse. Int Urogynecol J Pelvic
Floor Dysfunct. 23:929–934. 2012.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Ferrari MM, Rossi G, Biondi ML, Viganò P,
Dell'utri C and Meschia M: Type I collagen and matrix
metalloproteinase 1, 3 and 9 gene polymorphisms in the
predisposition to pelvic organ prolapse. Arch Gynecol Obstet.
285:1581–1586. 2012.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Wu JM, Visco AG, Grass EA, Craig DM,
Fulton RG, Haynes C, Amundsen CL and Shah SH: Comprehensive
analysis of LAMC1 genetic variants in advanced pelvic organ
prolapse. Am J Obstet Gynecol. 206:447.e1–6. 2012.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Chen HY, Chung YW, Lin WY, Chen WC, Tsai
FJ and Tsai CH: Progesterone receptor polymorphism is associated
with pelvic organ prolapse risk. Acta Obstet Gynecol Scand.
88:835–838. 2009.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Khadzhieva MB, Kamoeva SV, Ivanova AV,
Abilev SK and Salnikova LE: Elastogenesis-Related Gene
Polymorphisms and the Risk of Pelvic Organ Prolapse Development.
Genetika. 51:1191–1198. 2015.PubMed/NCBI(In Russian).
|
|
55
|
Khadzhieva MB, Kamoeva SV, Chumachenko AG,
Ivanova AV, Volodin IV, Vladimirov IS, Abilev SK and Salnikova LE:
Fibulin-5 (FBLN5) gene polymorphism is associated with pelvic organ
prolapse. Maturitas. 78:287–292. 2014.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Paula MVB, Lira Junior MAF, Monteiro
VCESC, Souto RP, Fernandes CE and Oliveira E: Evaluation of the
fibulin 5 gene polymorphism as a factor related to the occurrence
of pelvic organ prolapse. Rev Assoc Med Bras. 66:680–686.
2020.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Allen-Brady K, Norton PA, Farnham JM,
Teerlink C and Cannon-Albright LA: Significant linkage evidence for
a predisposition gene for pelvic floor disorders on chromosome
9q21. Am J Hum Genet. 84:678–682. 2009.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Allen-Brady K, Cannon-Albright LA, Farnham
JM and Norton PA: Evidence for pelvic organ prolapse predisposition
genes on chromosomes 10 and 17. Am J Obstet Gynecol. 212:771.
e771–777. 2015.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Khadzhieva MB, Kolobkov DS, Kamoeva SV,
Ivanova AV, Abilev SK and Salnikova LE: Verification of the
Chromosome Region 9q21 Association with Pelvic Organ Prolapse Using
RegulomeDB Annotations. BioMed Res Int. 2015(837904)2015.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Zhou Q, Hong L and Wang J: Identification
of key genes and pathways in pelvic organ prolapse based on gene
expression profiling by bioinformatics analysis. Arch Gynecol
Obstet. 297:1323–1332. 2018.PubMed/NCBI View Article : Google Scholar
|
|
61
|
McDermaid A, Monier B, Zhao J, Liu B and
Ma Q: Interpretation of differential gene expression results of
RNA-seq data: Review and integration. Brief Bioinform.
20:2044–2054. 2019.PubMed/NCBI View Article : Google Scholar
|
|
62
|
van Dijk EL, Jaszczyszyn Y, Naquin D and
Thermes C: The Third Revolution in Sequencing Technology. Trends
Genet. 34:666–681. 2018.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Hu JM, Wang L, Cheng X, Zhou LH and Li ZG:
Neuropeptide Y innervation in the vaginal mucosa among patients
with pelvic organ prolapse. Mol Med Rep. 5:444–448. 2012.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Hu JM, Cheng X, Wang L, Zhu JN and Zhou
LH: Vasoactive intestinal peptide expression in the vaginal
anterior wall of patients with pelvic organ prolapse. Taiwan J
Obstet Gynecol. 52:233–240. 2013.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Rahn DD, Ward RM, Sanses TV, Carberry C,
Mamik MM, Meriwether KV, Olivera CK, Abed H, Balk EM and Murphy M:
Society of Gynecologic Surgeons Systematic Review Group. Vaginal
estrogen use in postmenopausal women with pelvic floor disorders:
Systematic review and practice guidelines. Int Urogynecol J Pelvic
Floor Dysfunct. 26:3–13. 2015.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Edwall L, Carlström K and Jonasson AF:
Endocrine status and markers of collagen synthesis and degradation
in serum and urogenital tissue from women with and without stress
urinary incontinence. Neurourol Urodyn. 26:410–415. 2007.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Tomaszewski J, Adamiak-Godlewska A,
Bogusiewicz M, Brzana W, Juszczak M, Rzeski W and Rechberger T:
Collagen type III biosynthesis by cultured pubocervical fascia
fibroblasts surrounding mono and multifilament polypropylene mesh
after estrogens and tamoxifen treatment. Ginekol Pol. 81:493–500.
2010.PubMed/NCBI(In Polish).
|
|
68
|
Tanaka T, Saito Y, Matsuda K, Kamio K, Abe
S, Kubota K, Azuma A and Gemma A: Cyclic mechanical stretch-induced
oxidative stress occurs via a NOX-dependent mechanism in type II
alveolar epithelial cells. Respir Physiol Neurobiol. 242:108–116.
2017.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Rahn DD, Carberry C, Sanses TV, Mamik MM,
Ward RM, Meriwether KV, Olivera CK, Abed H, Balk EM and Murphy M:
Society of Gynecologic Surgeons Systematic Review Group. Vaginal
estrogen for genitourinary syndrome of menopause: A systematic
review. Obstet Gynecol. 124:1147–1156. 2014.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Wasenda EJ, Kamisan Atan I, Subramaniam N
and Dietz HP: Pelvic organ prolapse: Does hormone therapy use
matter? Menopause. 24:1185–1189. 2017.PubMed/NCBI View Article : Google Scholar
|














