Introduction
Best vitelliform macular dystrophy (BVMD) is a
hereditary retinal disease characterized by the accumulation of
lipofuscin in the central macula of both eyes (1-3).
Adult-onset BVMD was first described by Gass (4) more than four decades ago and is
usually diagnosed after the age of 40 years (1,4-6).
Compared to juvenile-onset BVMD, adult-onset BVMD is associated
with a wider spectrum of fundus abnormalities. The descriptions of
the first nine cases by Gass (4)
reflected the difficulty in differentiating adult-onset BVMD from
the full spectrum of age-related macular degeneration (AMD)
(4,5,7). Thus,
the lack of strict diagnostic criteria for adult-onset BVMD is
challenging for clinicians and researchers.
Overall, eyes affected by VMD exhibit various
patterns of progressive retinal pigment epithelium (RPE)
alterations involving the macula, making it difficult to obtain a
correct diagnosis according to the features of the imaging results.
Peripherin-2, bestrophin-1 (BEST1), inter photoreceptor matrix
proteoglycan-1(IMPG1) and IMPG2 are the genes detected in
adult-onset BVMD (5,8). These genes may be used as markers for
the diagnosis of adult-onset BVMD if it manifests with adulthood
macular degeneration, a variable degree of electrooculography (EOG)
suppression. The present study aimed to address the clinical,
histological, genetic, imaging and functional characteristics of
adult-onset BVMD and further aimed to provide a comprehensive
overview of the current understanding of adult-onset BVMD and its
putative causes.
To this end, multimodal imaging and genetic analysis
were combined to determine the clinical manifestations and genetic
characteristics of four advanced-age Chinese patients with
adult-onset BVMD.
Patients and methods
Study subjects and clinical
examinations
All experimental protocols and methods were approved
by the Ethics Committee of Zhongshan Ophthalmic Center of Sun
Yat-sen University (Guangzhou, China). Written informed consent was
obtained from all of the participants who were treated according to
the Declaration of Helsinki.
A total of four older patients >50 years with
suspected adult-onset BVMD were encountered at the Zhongshan
Ophthalmic Center (Guangzhou, China; between March 2017 and March
2021). Ophthalmic examinations were performed as follows: Visual
acuity was examined using an Early Treatment Diabetic Retinopathy
Study chart (Precision Vision). Optical coherence tomography (OCT)
was performed using a Cirrus HD-OCT (Carl Zeiss Meditec). Three
patients (Patients no. 1, 2 and 4) underwent OCT. Fundus
photography and fundus fluorescein angiography (FFA) imaging were
performed using a Heidelberg Retina Angiograph (Heidelberg
Engineering). EOG was recorded in all patients and these tests were
performed in conformity with the guidelines of the International
Society for Clinical Electrophysiology of Vision standards
(9). Physical examination was
performed to exclude any systemic diseases.
Sample collection and mutation
screening
Venous blood samples were collected from these four
patients, their family members and 200 subjects without BVMD from
the same region (Guangdong, China). The normal control presented in
the Results section is a 50-year-old male, recruited by
volunteering in November 2017. Genomic DNA was extracted from
peripheral blood leukocytes using standard protocols. Exons of the
BEST1 gene were amplified by PCR using primers (Table I) as previously described (8,10). PCR
was performed in 50-µl reactions. Amplification included a single
5-min step at 94˚C, followed by 40 cycles of 94˚C for 45 sec,
58-61˚C for 45 sec and 72˚C for 45 sec, and a final 10-min step at
72˚C. The PCR products were sequenced in both directions using an
ABI3730 Automated Sequencer (Thermo Fisher Scientific, Inc.). The
sequencing results were analyzed using Seqman (version 2.3;
Technelysium Pty., Ltd.) and compared with the reference sequences
in the database of the National Center for Biotechnology
Information (NCBI; NC_000011.10).
 | Table IPrimers used for the amplification of
the exons of bestrophin-1and product sizes. |
Table I
Primers used for the amplification of
the exons of bestrophin-1and product sizes.
| Exon | Forward
(5'-3') | Reverse
(5'-3') | Product size,
bp | Annealing
temperature, ˚C |
|---|
| 2 |
AGTCTCAGCCATCTCCTCGC |
TGGCCTGTCTGGAGCCTG | 212 | 61 |
| 3 |
GGGACAGTCTCAGCCATCTC |
CAGCTCCTCGTGATCCTCC | 238 | 58 |
| 4 |
AGAAAGCTGGAGGAGCCG |
GCGGCAGCCCTGTCTGTAC | 1408 | 59 |
| 5 |
GGGGCAGGTGGTGTTCAGA |
GGCAGCCTCACCAGCCTAG | 150 | 59 |
| 6 |
GGGCAGGTGGTGTTCAGA |
CCTTGGTCCTTCTAGCCTCAG | 181 | 59 |
| 7 |
CATCCTGATTTCAGGGTTCC |
CTCTGGCCATGCCTCCAG | 257 | 59 |
| 8 |
AGCTGAGGTTTAAAGGGGGA |
TCTCTTTGGGTCCACTTTGG | 215 | 59 |
| 9 |
ACATACAAGGTCCTGCCTGG |
GCATTAACTAGTGCTATTCTAAGTTCC | 298 | 59 |
| 10A |
GGTGTTGGTCCTTTGTCCAC |
CTCTGGCATATCCGTCAGGT | 591 | 59 |
| 10B |
CTTCAAGTCTGCCCCACTGT |
TAGGCTCAGAGCAAGGGAAG | 457 | 59 |
| 11 |
CATTTTGGTATTTGAAATGAAGG |
CCATTTGATTCAGGCTGTTG | 216 | 59 |
To analyze the effect of missense variants,
polymorphism phenotyping (PolyPhen; http://genetics.bwh.harvard.edu/pph2/) and sorting
intolerant from tolerant (SIFT; http://sift.jcvi.org/) were used to predict the
possible impact of an amino acid substitution on the structure and
function of the protein using straight forward physical and
comparative considerations. Variants were considered to be
pathogenic when at least one of the two programs predicted a
deleterious effect of amino acid substitution on protein structure
and function. The Human Gene Mutation Database (http://www.hgmd.org/) was used to screen for mutations
reported in published studies. HomoloGene (https://www.ncbi.nlm.nih.gov/homologene) was used to
check whether the mutated amino acid residues were conserved across
different species.
Results
Clinical findings
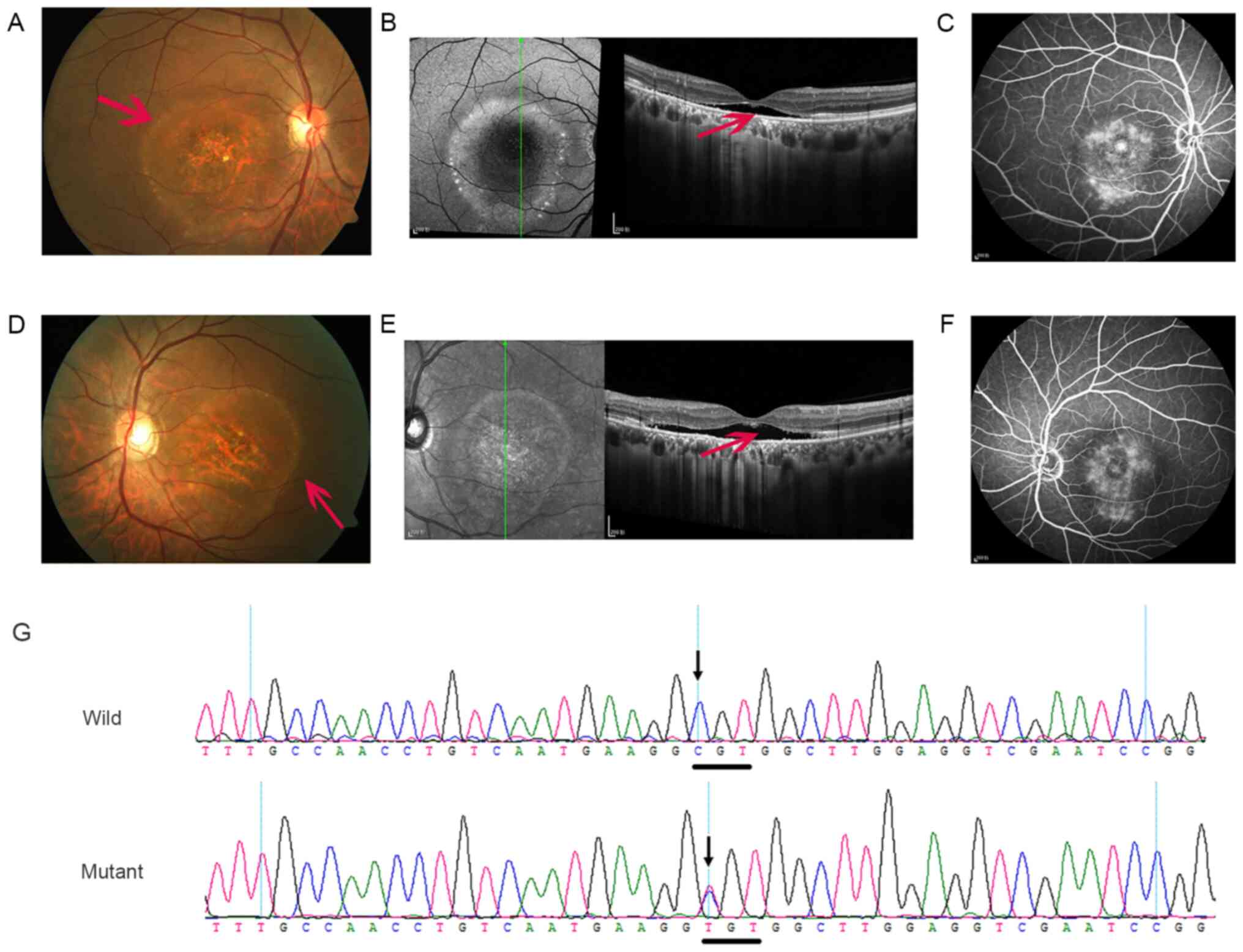
All patients were from southern China. A 62-year-old
female patient (Patient no. 1; Fig.
1) had no known familial history of ocular diseases. Her
best-corrected visual acuity (BCVA) was 20/100 in both eyes, which
was not possible to be corrected. The cornea was transparent and
there were certain opacities in the lens. Fundus examination
indicated that certain pigments in the macular area and the fovea
reflex were negative (Fig. 1A and
D) compared to anormal control
subject (Fig. 1H). OCT scans
revealed that the foveal region was abnormally thick in both eyes
due to neuroretinal detachment from the retinal pigment epithelium
(RPE; Fig. 1B and E), which was likely triggered by the
abnormal accumulation of subretinal fluid compared to the normal
control (Fig. 1I). FFA indicated
pooling of fluorescein dye in the cystoid spaces in the late phase
of fluorescein angiography, which may have been caused by the RPE
defect (Fig. 1C and F). The Arden ratio (light peak/dark
trough) was markedly reduced to <1.6. Chronic central serous
chorioretinopathy (CSC) was initially diagnosed and the patient was
treated with photodynamic therapy (PDT) with no clinical
response.
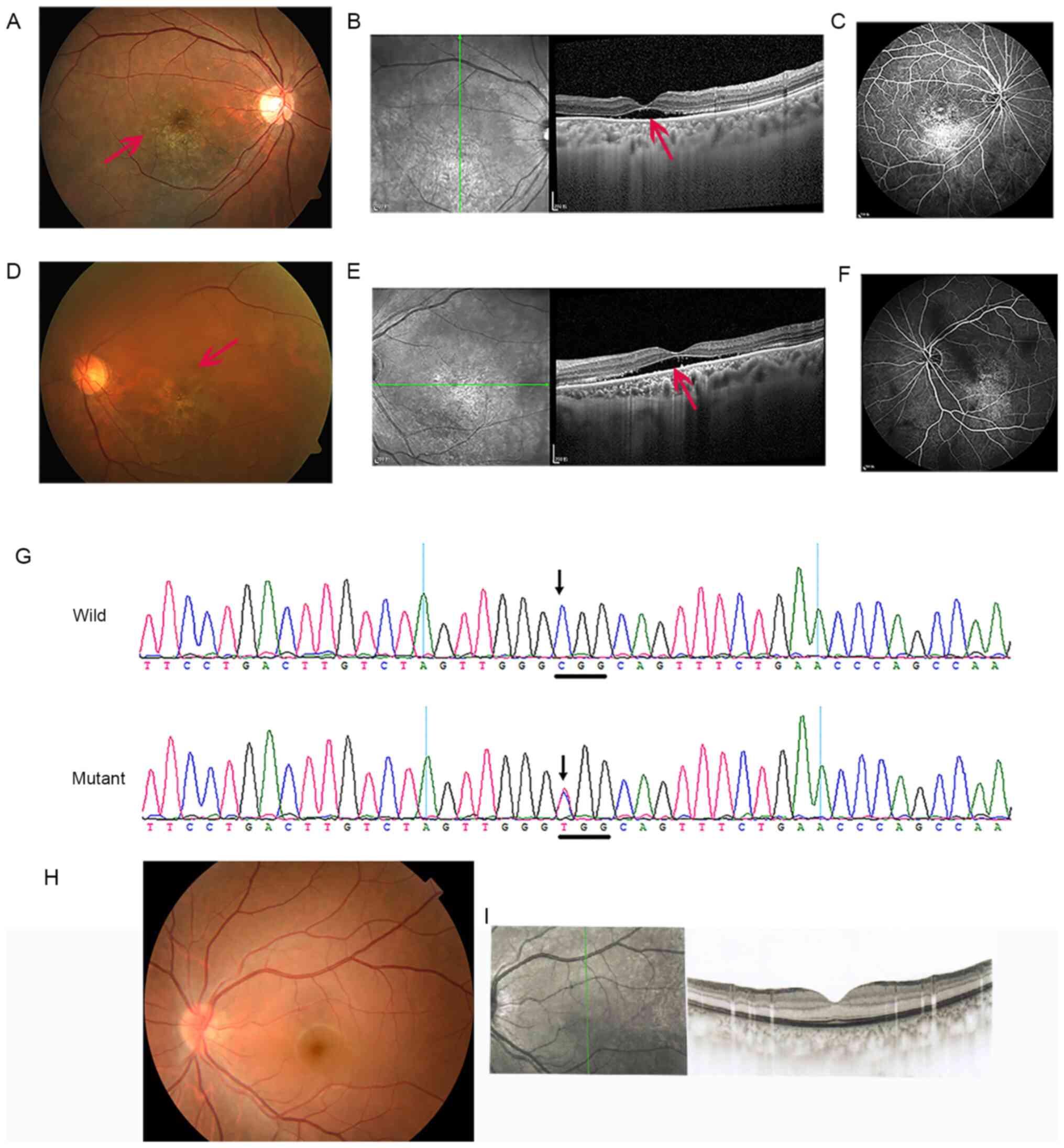 | Figure 1Clinical features and genetic results
of Patient no. 1, a 62-year-old female. (A-C) Right eye and (D-F)
left eye. (A and D) Fundus examination indicated that certain
pigments in the macular area and the fovea reflex were negative
(red arrows). (B and E) OCT scans revealed that the foveal regions
of both eyes were abnormally thick due to neuroretinal detachment
from the RPE, which was likely triggered by the abnormal
accumulation of subretinal fluid (red arrows). (C and F) FFA
indicates pooling of fluorescein dye in the cystoid spaces in the
late phase of FFA, which may have been caused by the RPE defect.
(G) In Patient no. 1, a heterozygous mutation, c.763C>T (p.
Arg255Trp, p.R255W), was identified in exon 7 of the
bestrophin-1gene. (H) Fundus photo of normal control (a 50-year-old
male). (I) OCT scan of normal control (the same as in H). RPE,
retinal pigment epithelium; OCT, optical coherence tomography; RPE,
retinal pigment epithelium; FFA, fundus fluorescein angiography;
wild, wild-type. |
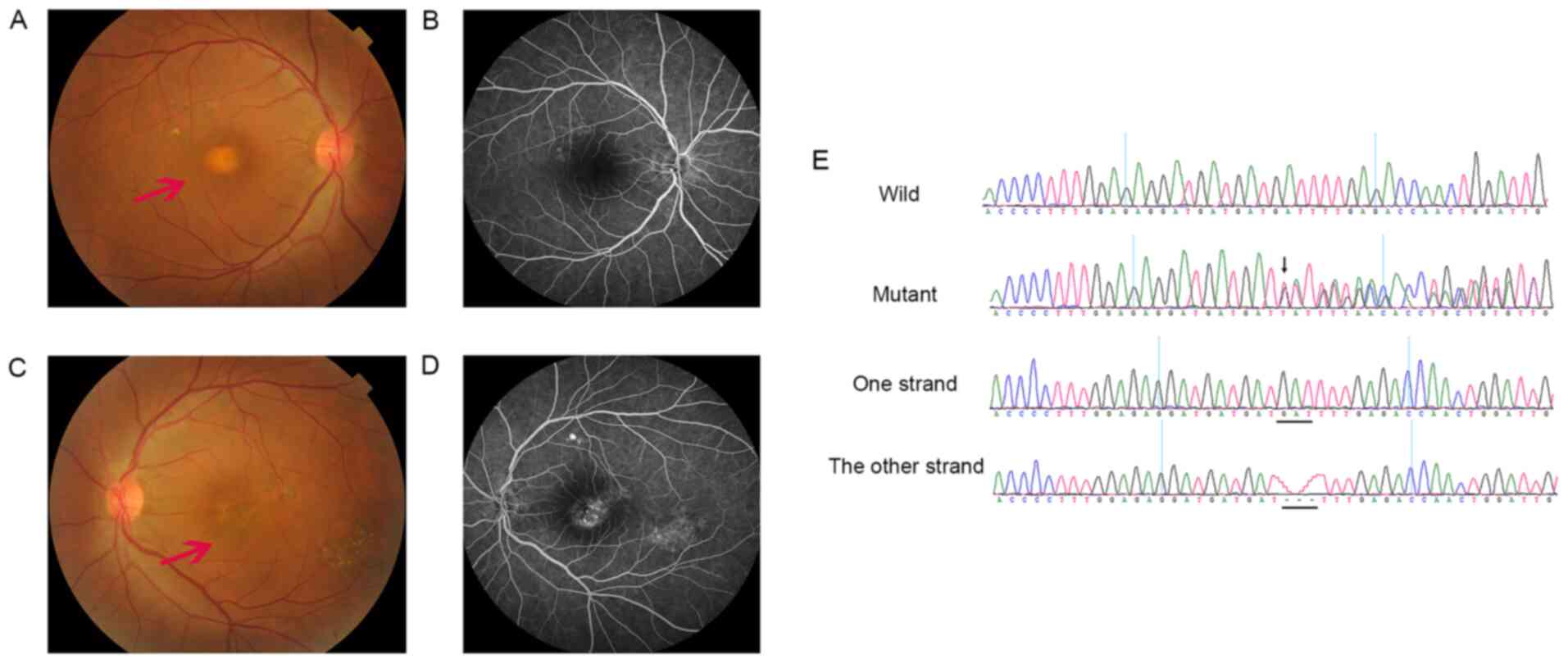
A 50-year-old male patient's (Patient no. 2;
Fig. 2) BVCA was 20/80 in both
eyes. The cornea and lens were transparent. Fundus photographs
revealed round lesions in the macular area (Fig. 2A and D). OCT indicated serous retinal detachment
(Fig. 2B and E). A fluorescein angiogram displayed
hyperfluorescence in the macular area (Fig. 2C and F). The Arden ratio was reduced to <1.6.
Chronic CSC was initially diagnosed and treated with PDT with no
improvement in vision.
A 60-year-old male patient's (patient no. 3;
Fig. 3) BCVA was 20/200 in the
right eye and counting fingers (CF) at 30 cm (CF/30 cm) in the left
eye. The cornea was transparent and there were certain opacities in
the lens. Fundus examination indicated a yolk-like lesion in the
macula of the right eye and an atrophic lesion in the left eye
(Fig. 3A and C). FFA revealed a small amount of
hyperfluorescence in the right eye, which may have been caused by
the RPE defect, and certain hyperfluorescence in the macular area
of the left eye corresponding to the region containing the atrophic
lesion detected on color fundus photography (Fig. 3B and D). The Arden ratio was reduced to
<1.8.
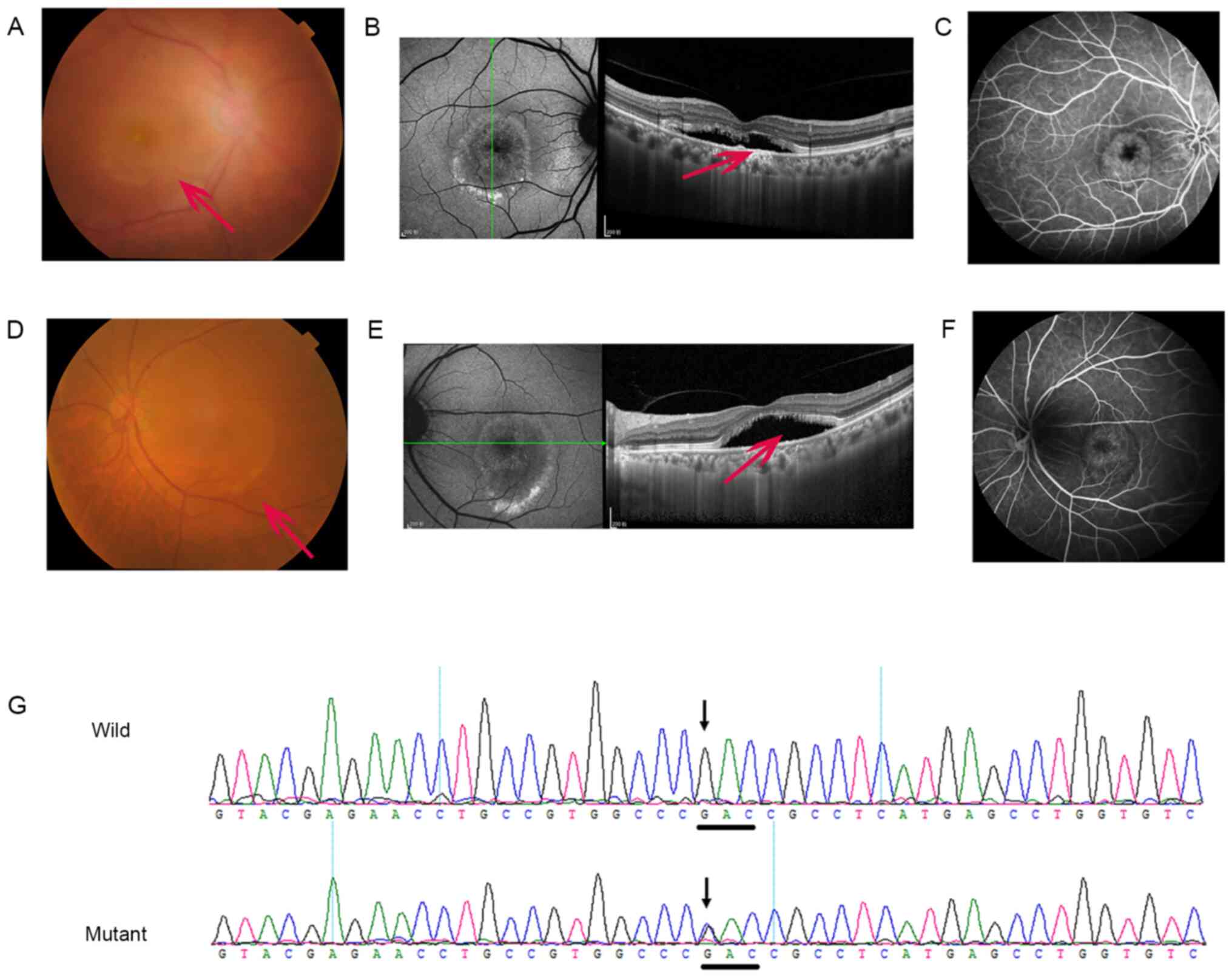
A 78-year-old male patient's (Patient no. 4;
Fig. 4) BVCA was CF/20 cm in the
right eye and CF/30 cm in the left eye. The cornea was transparent.
Severe opacities in the left lens and an intraocular lens in the
right eye with certain opacity in the posterior capsule were
observed and the fundus photographs were therefore not very clear.
Fundus photography indicated round lesions in the macular area and
a venous loop in the inferior part of the optic nerve head
(Fig. 4A and D). OCT scans revealed that serous retinal
detachments with elongated photoreceptor outer segments were
correlated with the size of the yellowish elevated lesion (Fig. 4B and E). A fluorescein angiogram revealed a
region of blocked fluorescence in the foveal center surrounded by a
transmission defect in the FFA (Fig.
4C and F). The Arden ratio was
severely reduced to <1.4. Chronic CSC was diagnosed at first and
the patient was treated with PDT with no improvement in vision.
One characteristic that was similar in all of the
four patients was that it was difficult to obtain an accurate
diagnosis due to the onset age of the disease and its atypical
clinical manifestations. Hence, the genetic analysis results have
an important role in adult-onset BVMD.
Mutation screening and bioinformatics
analysis
In Patient no. 1, a heterozygous mutation,
c.763C>T (p. Arg255Trp, p.R255W), was identified in exon 7 of
BEST1 (Fig. 1G). In Patient no. 2,
the mutation c.584C>T (p.Ala195Val, p.A195V) was identified in
exon 5 of BEST1 (Fig. 2G). In
Patient no. 3, the mutation c.910_912del GAT (p.Asp304del,
p.D304del) was identified in exon 8 of BEST1 (Fig. 3E). In Patient no. 4, the mutation
c.310G>C (p.Asp104His, p.D104H) was identified in exon 4 of the
BEST1 gene (Fig. 4G). No equivalent
mutations were detected in the family members of these subjects or
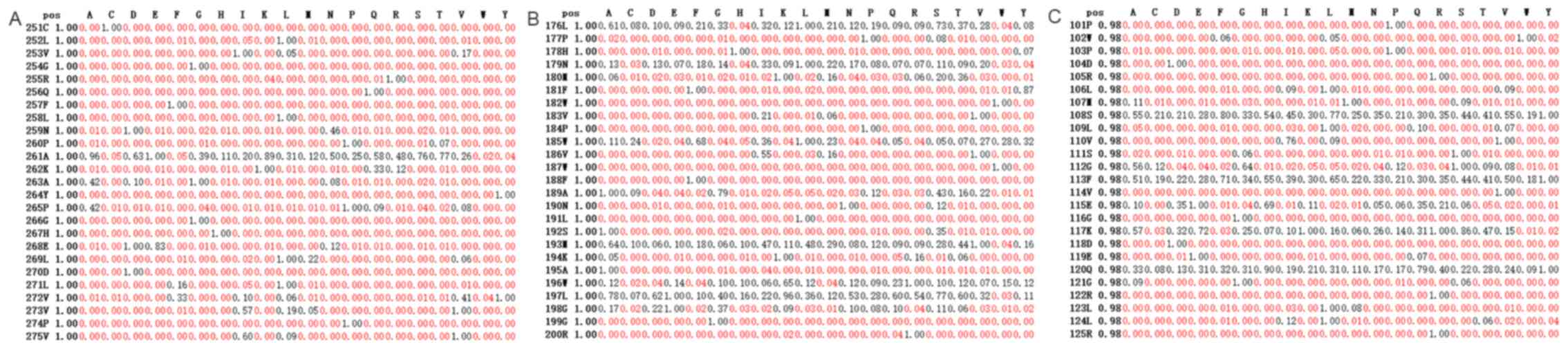
the control subjects. SIFT predicted that the amino acid
substitutions Arg255Trp, Ala195Val, and Asp104His in the BEST1
protein were damaging to its function (Fig. 5A-C). PolyPhen was not able to
predict the effects of these four mutations.
Discussion
Adult-onset BVMD is one of the most prevalent forms
of macular degeneration and was first described by Gass in
1974(4). Compared to juvenile-onset
BVMD, adult-onset BVMD is less characterized and lacks strict
diagnostic criteria. It was suggested that adult-onset BVMD
typically occurs between 30 and 50 years of age (5). The patients in the present study were
older than 50 years, similar to those in previous studies (7), indicating that adult-onset BVMD cannot
be excluded in older patients with macular lesions.
The clinical symptoms of adult-onset BVMD are highly
variable, but patients tend to remain asymptomatic until the 5th
decade or may even remain asymptomatic throughout life (11). Atypical presentations, such as
multifocal vitelliform lesions and the occurrence of choroidal
neovascularization (CNV) in various stages of the disease, may
confound the diagnosis (8,12,13).
In previous studies, the majority of cases had a negative family
history of the disease (5), similar
to the four cases in the present study. Furthermore, adult-onset
BVMD-like lesions have been suggested to be associated with several
additional phenotypes and pathologies, such as AMD (7) and chronic CSC (5,14). A
study by Spaide et al (15)
reported vitelliform lesions in three patients who were diagnosed
with typical CSC. In this study, three patients were misdiagnosed
with CSC, as the vitelliform lesions caused mechanical separation
between the photoreceptors and RPE. Therefore, for patients with
adult-onset BVMD, combining multimodal imaging and genetic
examination is helpful for confirming the diagnosis when other
causes of macular atrophy may be excluded (7,16-18).
BVMD is highly causally associated with mutations in
the gene BEST1(19) which encodes
BEST1. Human BEST1, identified in 1998, is a calcium-activated
chloride channel in the RPE (11).
In addition to evaluating clinical and genetic
manifestations of BVMD, the present study sought to investigate the
correlations between genotypes and phenotypes in order to provide
additional criteria for this disease for ophthalmologists to avoid
an incorrect diagnosis. A study performed in Japan identified one
patient with heterozygous variants of V239VfsX2/p.R255W, who
presented mainly with macular edema and low amounts of subretinal
fluid (Table II) (20) unlike what was detected in Patient
no. 1 of the present study. First, the phenotypes of compound
heterozygous mutations and those associated with this one mutation
maybe different. Furthermore, the patients in the Japanese study
had juvenile-onset BVMD, which may differ from adult-onset BVMD,
which was the focus of the present study. Furthermore, the p.R255W
mutation may not be related to subretinal fluid, which is
reasonable because BVMD involves 4-5 stages. Wong et al
(21) reported another patient, an
8-year-old male with BVMD and CNV (Table II). Tian et al (22) and another study (23) from the glaucoma division of our
hospital also identified that certain patients with p.R255W had
angle-closure glaucoma in addition to macular lesions (Table II). Thus, these results may confirm
that addressing the role of p.R255Win BVMD is important in both
juvenile-onset and adult-onset BVMD and may present with numerous
clinical features, which makes it a hot topic in the field.
According to the protein structure of BEST1, amino acid 255 is
positioned at the margin of the cell membrane (19); p.R255W therefore deserves further
research regarding the mechanism by which it contributes to BVMD
(24).
| Table IIComparison of clinical features of
the same mutation between the present study and other studies. |
Table II
Comparison of clinical features of
the same mutation between the present study and other studies.
| Study (year) | Mutation | Region | Sex | Age (years) | Visual acuity | Fundus
appearance | (Refs.) |
|---|
| Present study | p.R255W
(heterozygous) Patient no. 1 | Asia (China) | F | 62 | OU: 20/100 | Pigmentation in the
macular area | - |
| Kubota et
al, 2016 | V239VfsX2/p.R255W
(heterozygous) | Asia (Japan) | M | 25 | OD: 0.9 OS: 0.3
(decimal) | Cystoid macular
lesions and multiple yellowish deposits | (20) |
| Wong et al,
2010 | p.R255W
(heterozygous) | Asia (China) | M | 8 | OD: 20/200 OS:
20/30 | OD: CNV OS:
Vitelliruptive | (21) |
| Tian et al,
2017 | p.R255W
(heterozygous) | Asia (China) | NS | NS | NS | Diffuse yellowish
lesion in the macula; the C/D ratio was 0.8 | (22) |
| Luo et al,
2019 | p.R255W
(homozygous, heterozygous) | Asia (China) | NS | NS | NS | Angle-closure
glaucoma and macular lesion | (23) |
| Present study | p.A195V
(heterozygous) Patient no. 2 | Asia (China) | M | 50 | OU: 20/80 | Round lesions in
the macular area | - |
| Katagiri et
al, 2015 | p.A195V
(heterozygous) | Asia (Japan) | M | 50 | OD:1.2 OS:1.0
(decimal) | OD: Vitelliruptive
stage OS: Vitelliruptive stage | (25) |
| Tian et al,
2014 | p.A195V/p.R255W
(heterozygous) | Asia (China) | NS | 25 | OD: 20/50 OS:
20/40 | OD: Pseudohypopyon
OS: Vitelliform lesion | (27) |
| Present study | p.D304del
(heterozygous) Patient no. 3 | Asia (China) | M | 60 | OD: 20/200 OS:CF/30
cm | OD: Yolk-like
lesion in the macula OS: Atrophic lesion | - |
| Katagiri et
al, 2015 | p.D304del
(heterozygous) | Asia (Japan) | M | 56 | OD:0.15 OS:1.2
(decimal) | OD: Atrophic stage
OS: Vitelliform stage | (25) |
| Present study | p.D104H
(heterozygous) Patient no. 4 | Asia (China) | M | 78 | CF/20 cm OD CF/30
cm OS | Round lesions in
the macular area | - |
| Krämer et
al, 2003 | p.D104H
(heterozygous) | Germany | | NS | NS | NS | (31) |
The variant p.A195V had been previously reported in
a 50-year-old Japanese male with adult-onset BVMD (Table II) (25), whose vision was much better than
that of Patient no. 2 in the present study, although both patients
were 50-year-old males. Lee et al (26) determined that 293T cells transfected
with a p.A195V mutant produced significantly smaller currents than
cells transfected with the wild-type gene. Tian et al
(27) also reported a case of the
compound mutation p.A195V/p.R255W in a young patient with good
vision, which may indicate that the compound mutation is not as
severe as the single mutation, similar to the results of a previous
study (28). It may be suggested
that the reason is that certain mutations increase
Cl-currents but that others decrease
Cl-currents.
To the best of our knowledge, as for Patient no. 3
of the present study, only one previous study by Katagiri et
al (25) detected the
c.910_912del GAT mutation in a 56-year-old Japanese male. Although
c.910G>A (p.Asp304Asn) was identified by another investigator,
no detailed description was provided (https://www.ncbi.nlm.nih.gov/clinvar/variation/496689/).
These results indicated that Asp in this position is important for
the function of the whole protein. According to the structure of
the BEST1 protein (8,29,30),
the amino acids in positions 301-304 are all Asp and all mutations
at these sites cause BVMD, which may indicate that the structure of
several continuous residues of the same amino acid is easily
damaged.
The c.310G>C (p.Asp104His, p.D104H) mutation in
exon 4 is also a recurrent mutation, as reported by Krämer et
al (31) (Table II). The Asp104 residue is highly
conserved among other species, including nematodes and fruit flies.
Finally, codon 104 has previously been indicated to be affected by
a mutational change that altered the asparagine residue to a
glutamic residue (Asp104Glu) (32).
Taken together, these data indicate that Asp104 is likely to be the
causative agent of BVMD.
Currently, no validated therapy is available for
restoration of the normal contact between the photoreceptors and
the RPE and/or for facilitating safe lesion absorption (5). Ergun et al (33) reported that PDT had no beneficial
effect on the vision of patients with BVMD, suggesting that severe
adverse effects were associated with this treatment. In the present
study, Patients no. 1, 2 and 4 were treated with PDT without any
favorable outcomes. The prognosis of adult-onset BVMD is poor, as
visual impairment and legal blindness may occur, as was observed in
the present study. Gene therapy is the most promising option for
treating monogenic forms of BVMD prior to fluid-induced rod cell
death (11,34).
Certain limitations of the present study should be
noted. First, the sample size of the included subjects was limited
because of the rarity of adult-onset BVMD. Furthermore, no
longitudinal study was performed and therefore, it was not possible
to assess the temporal trends of these changes during aging.
In summary, by combining multimodal imaging and
genetic examination, adult-onset BVMD was confirmed in four
patients. These results expand the mutation spectrum of BEST1and
may be helpful in genetic and clinical counseling to correctly
diagnose patients with adult-onset BVMD. In addition, the
characterization of these patients with adult-onset BVMD in the
present study provides a basis for future investigations of the
mechanisms underlying the pathogenesis and for the development of
therapeutic interventions.
Acknowledgements
Not applicable.
Funding
Funding: This study was supported by the National Natural
Science Foundation of China (grant no. 82070972).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YLin, TL, BL, CJ and LL analyzed and interpreted the
patient data. CL, YLian, YH, QW, HL and JL examined the patients
and performed PCR and gene sequence analysis. YLin, JL and HL
interpreted the sequencing data, drafted the manuscript and revised
it critically. YLin and LL confirm the authenticity of all the raw
data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All experimental protocols were approved by the
Ethics Committee of Zhongshan Ophthalmic Center (Guangzhou, China).
Written informed consent was obtained from all subjects.
Patient consent for publication
Written informed consent for publication was
obtained from all participants.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
MacDonald IM and Lee T: Best vitelliform
macular dystrophy. In: GeneReviews((R)). Adam MP, Ardinger HH and
Pagon RA (eds). University of Washington, Seattle, WA, 1993.
|
|
2
|
Katz MS, Walsh EK and Medow NB:
Vitelliform macular dystrophy. JAMA Ophthalmol.
132(1098)2014.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Tsang SH and Sharma T: Best vitelliform
macular dystrophy. Adv Exp Med Biol. 1085:157–158. 2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Gass JD: A clinicopathologic study of a
peculiar foveomacular dystrophy. Trans Am Ophthalmol Soc.
72:139–156. 1974.PubMed/NCBI
|
|
5
|
Chowers I, Tiosano L, Audo I, Grunin M and
Boon CJ: Adult-onset foveomacular vitelliform dystrophy: A fresh
perspective. Prog Retin Eye Res. 47:64–85. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Jun I, Lee JS, Lee JH, Lee CS, Choi SI,
Gee HY, Lee MG and Kim EK: Adult-onset vitelliform macular
dystrophy caused by BEST1 p.Ile38Ser mutation is a mild form of
best vitelliform macular dystrophy. Sci Rep. 7(9146)2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Toto L, Borrelli E, Mastropasqua R, Di
Antonio L, Mattei PA, Carpineto P and Mastropasqua L: Adult-onset
foveomacular vitelliform dystrophy evaluated by means of optical
coherence tomography angiography: A comparison with dry age-related
macular degeneration and healthy eyes. Retina. 38:731–738.
2018.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lin Y, Li T, Ma C, Gao H, Chen C, Zhu Y,
Liu B, Lian Y, Huang Y, Li H, et al: Genetic variations in
bestrophin-1 and associated clinical findings in two Chinese
patients with juvenile-onset and adult-onset best vitelliform
macular dystrophy. Mol Med Rep. 17:225–233. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Constable PA, Bach M, Frishman LJ, Jeffrey
BG and Robson AG: International Society for Clinical
Electrophysiology of Vision. ISCEV standard for clinical
electro-oculography (2017 update). Doc Ophthalmol. 134:1–9.
2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lin Y, Li T, Gao H, Lian Y, Chen C, Zhu Y,
Li Y, Liu B, Zhou W, Jiang H, et al: Bestrophin 1 gene analysis and
associated clinical findings in a Chinese patient with best
vitelliform macular dystrophy. Mol Med Rep. 16:4751–4755.
2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Yang T, Justus S, Li Y and Tsang SH:
BEST1: The best target for gene and cell therapies. Mol Ther.
23:1805–1809. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Shahzad R and Siddiqui MA: Choroidal
neovascularization secondary to best vitelliform macular dystrophy
detected by optical coherence tomography angiography. J AAPOS.
21:68–70. 2017.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Stattin M, Ahmed D, Glittenberg C, Krebs I
and Ansari-Shahrezaei S: Optical coherence tomography angiography
for the detection of secondary choroidal neovascularization in
vitelliform macular dystrophy. Retin Cases Brief Rep. 14:49–52.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Giuffrè C, Miserocchi E, Modorati G,
Carnevali A, Marchese A, Querques L, Querques G and Bandello F:
Central serous chorioretinopathylike mimicking multifocal
vitelliform macular dystrophy: An ocular side effect of
mitogen/extracellular signal-regulated kinase inhibitors. Retin
Cases Brief Rep. 12:172–176. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Spaide RF, Noble K, Morgan A and Freund
KB: Vitelliform macular dystrophy. Ophthalmology. 113:1392–1400.
2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Lima de Carvalho JR Jr, Paavo M, Chen L,
Chiang J, Tsang SH and Sparrow JR: Multimodal imaging in best
vitelliform macular dystrophy. Invest Ophthalmol Vis Sci.
60:2012–2022. 2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Querques G, Bux AV, Prato R, Iaculli C,
Souied EH and Noci ND: Correlation of visual function impairment
and optical coherence tomography findings in patients with
adult-onset foveomacular vitelliform macular dystrophy. Am J
Ophthalmol. 146:135–142. 2008.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bitner H, Schatz P, Mizrahi-Meissonnier L,
Sharon D and Rosenberg T: Frequency, genotype, and clinical
spectrum of best vitelliform macular dystrophy: Data from a
national center in Denmark. Am J Ophthalmol. 154:403–412.e4.
2012.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Boon CJ, Klevering BJ, Leroy BP, Hoyng CB,
Keunen JE and den Hollander AI: The spectrum of ocular phenotypes
caused by mutations in the BEST1 gene. Prog Retin Eye Res.
28:187–205. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kubota D, Gocho K, Akeo K, Kikuchi S,
Sugahara M, Matsumoto CS, Shinoda K, Mizota A, Yamaki K, Takahashi
H and Kameya S: Detailed analysis of family with autosomal
recessive bestrophinopathy associated with new BEST1 mutation. Doc
Ophthalmol. 132:233–243. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wong RL, Hou P, Choy KW, Chiang SW, Tam
PO, Li H, Chan WM, Lam DS, Pang CP and Lai TY: Novel and homozygous
BEST1 mutations in Chinese patients with best vitelliform macular
dystrophy. Retina. 30:820–827. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Tian L, Sun T, Xu K, Zhang X, Peng X and
Li Y: Screening of BEST1 gene in a Chinese cohort with best
vitelliform macular dystrophy or autosomal recessive
bestrophinopathy. Invest Ophthalmol Vis Sci. 58:3366–3375.
2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Luo J, Lin M, Guo X, Xiao X, Li J, Hu H,
Xiao H, Xu X, Zhong Y, Long S, et al: Novel BEST1 mutations and
special clinical characteristics of autosomal recessive
bestrophinopathy in Chinese patients. Acta Ophthalmol. 97:247–259.
2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Milenkovic VM, Rivera A, Horling F and
Weber BH: Insertion and topology of normal and mutant bestrophin-1
in the endoplasmic reticulum membrane. J Biol Chem. 282:1313–1321.
2007.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Katagiri S, Hayashi T, Ohkuma Y, Sekiryu
T, Takeuchi T, Gekka T, Kondo M, Iwata T and Tsuneoka H: Mutation
analysis of BEST1 in Japanese patients with Best's vitelliform
macular dystrophy. Br J Ophthalmol. 99:1577–1582. 2015.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Lee CS, Jun I, Choi SI, Lee JH, Lee MG,
Lee SC and Kim EK: A novel BEST1 mutation in autosomal recessive
bestrophinopathy. Invest Ophthalmol Vis Sci. 56:8141–8150.
2015.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Tian R, Yang G, Wang J and Chen Y:
Screening for BEST1 gene mutations in Chinese patients with
bestrophinopathy. Mol Vis. 20:1594–1604. 2014.PubMed/NCBI
|
|
28
|
Johnson AA, Bachman LA, Gilles BJ, Cross
SD, Stelzig KE, Resch ZT, Marmorstein LY, Pulido JS and Marmorstein
AD: Autosomal recessive bestrophinopathy is not associated with the
loss of bestrophin-1 anion channel function in a patient with a
novel BEST1 mutation. Invest Ophthalmol Vis Sci. 56:4619–4630.
2015.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Hartzell HC, Qu Z, Yu K, Xiao Q and Chien
LT: Molecular physiology of bestrophins: Multifunctional membrane
proteins linked to best disease and other retinopathies. Physiol
Rev. 88:639–672. 2008.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tsunenari T, Sun H, Williams J, Cahill H,
Smallwood P, Yau KW and Nathans J: Structure-function analysis of
the bestrophin family of anion channels. J Biol Chem.
278:41114–41125. 2003.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Krämer F, Mohr N, Kellner U, Rudolph G and
Weber BH: Ten novel mutations in VMD2 associated with best macular
dystrophy (BMD). Hum Mutat. 22(418)2003.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Petrukhin K, Koisti MJ, Bakall B, Li W,
Xie G, Marknell T, Sandgren O, Forsman K, Holmgren G, Andreasson S,
et al: Identification of the gene responsible for best macular
dystrophy. Nat Genet. 19:241–247. 1998.PubMed/NCBI View
Article : Google Scholar
|
|
33
|
Ergun E, Costa D, Slakter J, Yannuzzi LA
and Stur M: Photodynamic therapy and vitelliform lesions. Retina.
24:399–406. 2004.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Guziewicz KE, Zangerl B, Komaromy AM,
Iwabe S, Chiodo VA, Boye SL, Hauswirth WW, Beltran WA and Aguirre
GD: Recombinant AAV-mediated BEST1 transfer to the retinal pigment
epithelium: Analysis of serotype-dependent retinal effects. PLoS
One. 8(e75666)2013.PubMed/NCBI View Article : Google Scholar
|