Introduction
Although lipoma is the most commonly encountered
benign mesenchymal tumor (1),
chondroid lipoma is a rare entity originating from soft tissues
that was initially described by Meis and Enzinger in 1993(1). Due to the presence of certain
similarities with extra-skeletal chondrosarcoma and round cell
liposarcoma, the diagnosis of this pathological entity may become
challenging especially in cases presenting large lesions (2,3).
Histopathological and immunohistochemical studies demonstrating the
presence of an association between adipose tissue, cartilaginous
tissues, mature adipocytes, chondroblasts and hyaline matrix as
well as the absence of aberrant proliferation suggesting malignant
transformation seems to play a crucial role in order to provide a
differential diagnosis with malignant lesions such as
chondrosarcoma and liposarcoma (4).
Providing a correct diagnosis is crucial in the prevention of the
overtreatment of these lesions which otherwise may be treated as
malignant lesions.
In the present study, the case of a 61-year-old
patient who self-referred for the development of a large tumor at
the level of the left breast is reported.
Case report
Patient data
A 61-year-old patient with no significant medical
history self-presented for the appearance of a large tumor which
was observed within the last eight months and which presented a
rapid growth within the last three months.
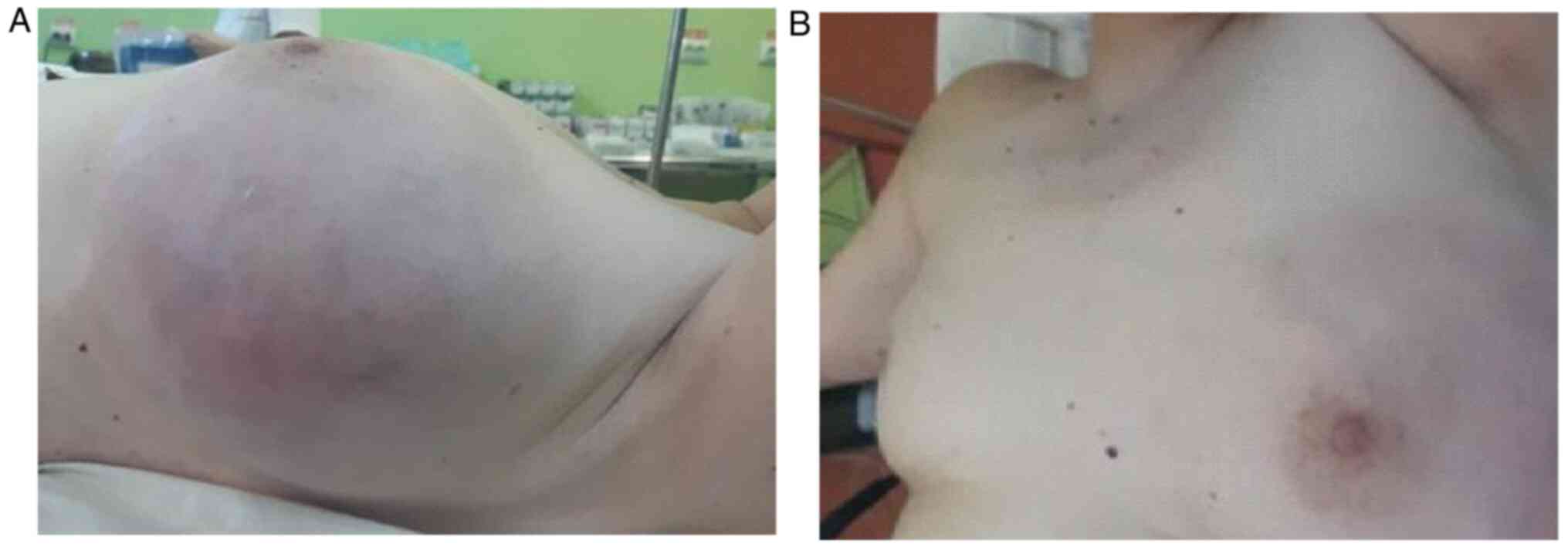
The clinical examination revealed the presence of a
large tumoral mass having developed at the level of the left breast
measuring 20/15 cm, deforming the entire breast. Additionally,
signs of collateral circulation were observed at the level of the
adjacent skin (Fig. 1). The mass
seemed to keep its mobility in the surrounding skin and to the
prepectoral fascia while the nipple presented no pathological
aspects and no discharge. Local examination of the left axilla
failed to demonstrate the presence of suspect adenopathies;
furthermore, the contralateral breast and axilla presented no
pathological modifications (Fig. 1A
and B).
Methods
The patient was further submitted to a mammography
which confirmed the presence of a 22/18 cm lesion with regular
margins and intra-tumoral calcifications. The lesion was classified
as a Breast Imaging-Reporting and Data System (BIRDAS) grade 2
tumor, and normal breast parenchyma was almost absent (Fig. 2). The patient underwent breast
ultrasound which confirmed the presence of a heterogeneous mass
measuring 20/18/15 cm with peripheral positive Doppler signal and
minimal areas of normal breast parenchyma; the ultrasound-guided
biopsy raised the suspicion of a chondroid lipoma, with no signs of
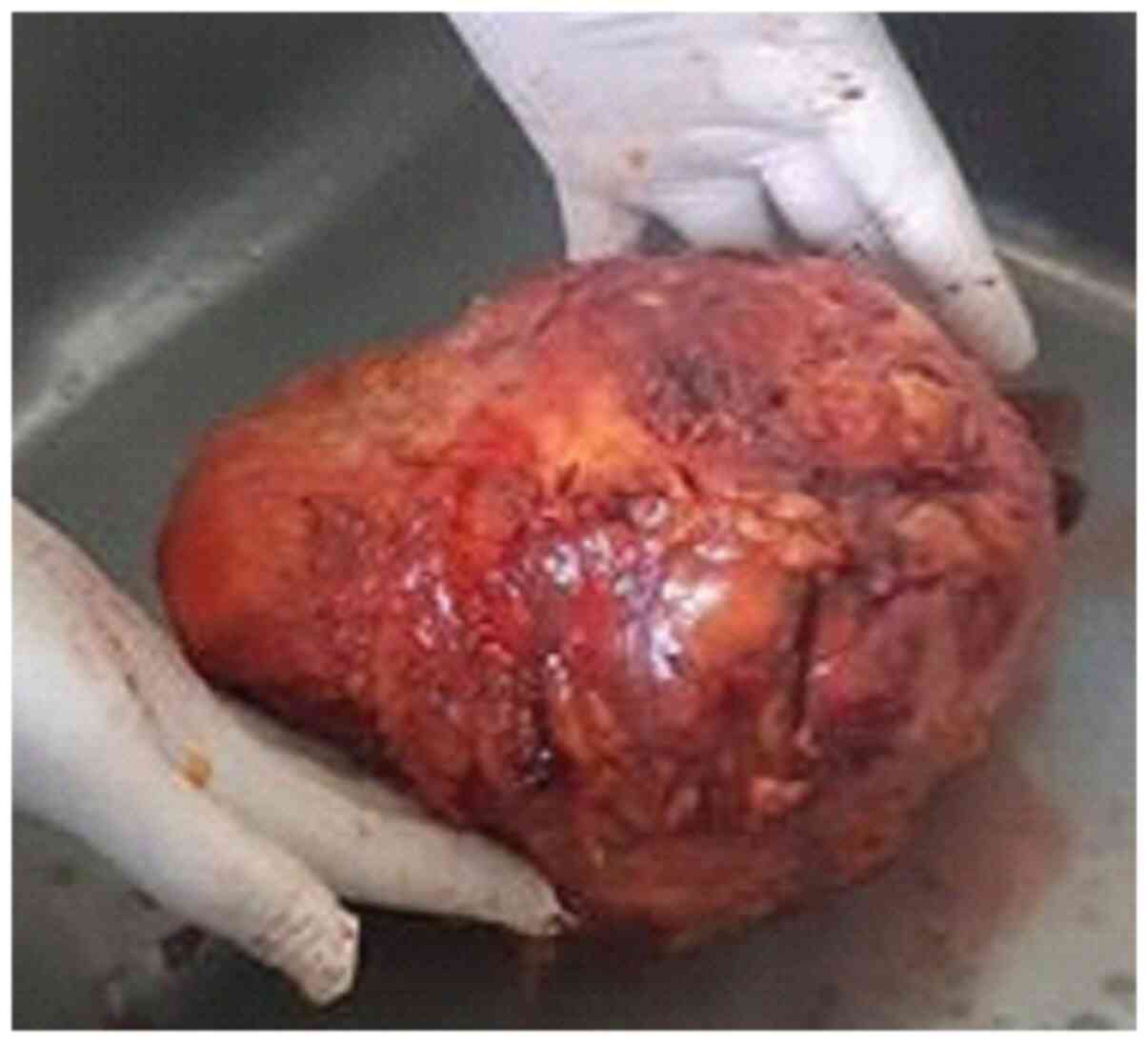
malignancy being encountered. The patient then underwent surgery
with conservative intent; however, after excision of the
encapsulated tumor, no remnant breast parenchyma was found.
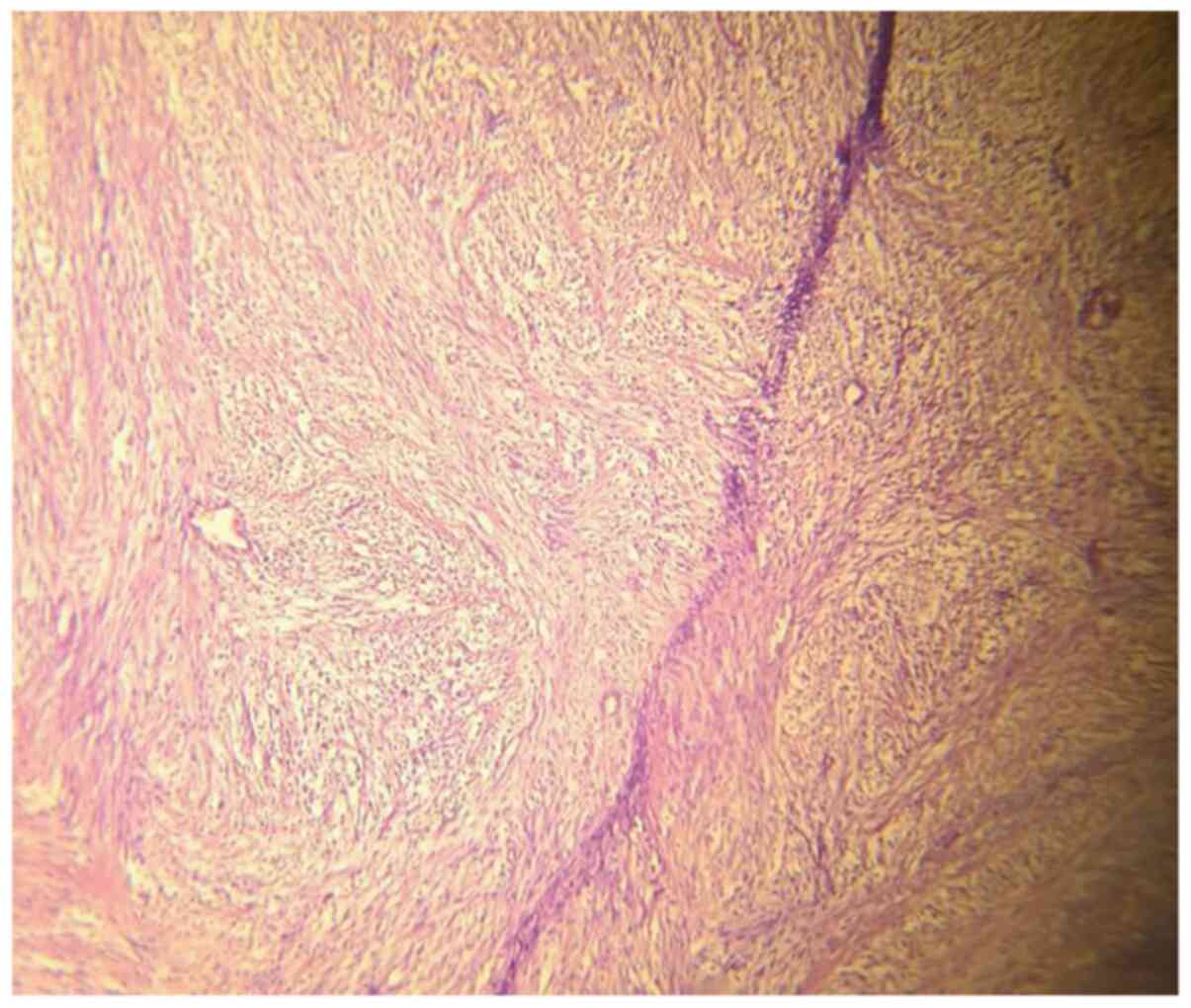
Therefore, total mastectomy was performed (Fig. 3). The histopathological studies,
which included hematoxylin and eosin staining, demonstrated the
presence of a 20/18/10 cm encapsulated lesion presenting
mesenchymal proliferation formed by chondroid myxoid matrix with
lipoblast areas and blood vessels and no mitotic activity (Fig. 4). In addition, a 1.5 cm fibroadenoma
was also found in the close proximity of the giant chondroid
lipoma. The postoperative outcome was uneventful. The patient then
underwent breast reconstruction with an implant two months later.
At 24 months, the patient is free of local or distant recurrent
disease.
Discussion
The structure of breast lipomas is usually modified
by the presence of other mesenchymal elements leading to the
development of fibrolipoma, angiolipoma, osteolipoma, myxolipoma,
or chondrolipoma (5). Most often
cartilaginous transformation inside a lipomatous lesion leading to
the development of a chondrolipoma is related to a prolonged
evolution and to larger dimensions of a lipoma (6). Although the exact process of
chondrolipoma histogenesis is not well understood, there are three
theories which have been considered. The first one considers that
in cases in which glandular components are found inside the tumor,
they act like choristoma; the second theory considers that immature
mesenchymal cells develop towards both adipocytes and chondrocytes;
while the third theory considers that these tumors originate from
cartilaginous metaplasia of the adipose tissue in lipomas (7-13).
Chondroid lipomas are delimited, asymptomatic
lesions developed in the subcutaneous tissues or at the level of
the skeletal muscles, more commonly at the level of the arms, neck
and head. Breast chondroid lipomas represent a scarce eventuality,
being more frequently encountered in young women (during the third
decade of life) and present as small volume lesions (2). Their histopathological particularity
is represented by the presence of cartilaginous tissue among mature
fat and glandular mammary parenchyma and their dimensions usually
range between 2 and 6 cm (4). Giant
lesions are those >5 cm in one dimension, with a weight of
>500 g (14), but rarely
surpassing 10 cm (15). The tumor
is characterized by the presence of peripheral compressed mammary
parenchyma which is transformed into a true capsule for the tumor
while at the level of the tumor ductal structures and mammary
stroma may not be present (4,16). In
order to achieve proper diagnosis, imagistic studies such as breast
ultrasound, mammography, and MRI followed by biopsy is mandatory.
When it comes to the mammographic aspect of the lesion, it usually
presents as a radiolucent mass due to the presence of an increased
amount of fatty tissue in the absence of mammary stroma or ducts in
association with focal opacities induced by the presence of islets
of cartilaginous structures. However, the presence of
calcifications is rather scarce, with few such cases being reported
thus far (5,7,17).
Therefore, preoperatively, in the absence of a biopsy, the
differential diagnosis with a malignant lesion is rather difficult
to be established (5,18). The most common entities which should
be taken into consideration when performing a differential
diagnosis are represented by fat necrosis, giant fibroadenoma,
supernumerary breast as well as malignant lesions such as
chondrosarcoma or liposarcoma (15-28);
in this respect, ultrasound-guided biopsy is mandatory.
Thus, appropriate diagnosis of benignity can be
established and therefore, the patient can be submitted to local
excision of the lesion, and overtreatment can be prevented
(4,14,29-36).
However, in certain cases, due to the high volume of the lesion,
retrieving the tumor can consist in fact in performing a total
mastectomy (as presented in our case) although surgery is not
intended to be a radical one as long as the biopsy has confirmed
the absence of atypical mitoses (3). In order to prevent the risk of local
recurrence, complete excision of the lesion en bloc with the
adjacent capsule is mandatory (4,15).
Another important aspect which should be taken into
consideration when it comes to chondroid lipoma of the breast is
the one regarding the differential diagnostic with malignant
chondroid tumors such as primary chondroid sarcoma (19-24).
Therefore, in cases in which malignant transformation is suspected,
immunohistochemical studies aiming to investigate the presence of
cytokeratin expression are mandatory (25-28).
In summary, giant breast chondroid lipoma represent
scarce situations affecting women worldwide. Preoperative biopsy is
mandatory in order to demonstrate the absence of any sign of
malignant disease and to further allow the surgeon to perform
tumoral enucleation without radical breast surgery. However, in
certain cases the absence of normal breast parenchyma will
transform the enucleation procedure into a total mastectomy
followed by breast reconstructive surgery.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Further information regarding the case study is
available from the corresponding author on reasonable request.
Authors' contributions
AAA and SS performed the surgical procedures. NB, MD
and IB prepared the draft of the article in light of the literature
data and case findings. NB was advisor of the surgical procedures.
CD, CS and OS preoperatively investigated the patient. AAA and NB
revised the final draft of the manuscript. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The Ethics Committee of Ramnicu Sarat County
Hospital approved the study (no. 21/2018).
Patient consent for publication
Written informed consent was obtained from the
patient on 11.04.2018.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Meis JM and Enzinger FM: Chondroid lipoma.
A unique tumor simulating liposarcoma and myxoid chondrosarcoma. Am
J Surg Pathol. 17:1103–1112. 1993.PubMed/NCBI
|
|
2
|
Vandeweyer E and Scagnol I: Axillary giant
lipoma: A case report. Acta Chir Belg. 105:656–657. 2005.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Aljarrah A, Malik KA, Al Jarraha A,
Sawhney S and Lakhtakia R: Chondroid lipoma of breast: A rare
pathology. J Liaquat Univ Med Health Sci. 12:131–132. 2013.
|
|
4
|
Banev SG and Filipovski VA: Chondrolipoma
of the breast-case report and a review of literature. Breast.
15:425–426. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Sudhamani S, Pandit AA and Kiri VM:
Chondrolipoma of breast: A case report with the review of the
literature. J Sci Soc. 39:147–148. 2012.
|
|
6
|
Weiss SW and Goldblum JR: Cartilaginous
soft tissue tumors. In: Enzinger and Weiss's Soft tissue tumors.
4th edition. Strauss M (ed).St. Louis, Mosby, p1361, 2001.
|
|
7
|
Kaplan L and Walts AE: Benign
chondrolipomatous tumor of the human female breast. Arch Pathol Lab
Med. 101:149–151. 1977.PubMed/NCBI
|
|
8
|
Benisch B, Peison B and Sarno J: Benign
mesenchymoma of the breast. Mt Sinai J Med. 43:530–533.
1976.PubMed/NCBI
|
|
9
|
Fushimi H, Kotoh K, Nishihara K, Fujinaka
H and Takao T: Chondrolipoma of the breast: A case report with
cytological and histological examination. Histopathology.
35:478–479. 1999.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Fujimura N and Enomoto S: Lipoma of the
tongue with cartilaginous change: A case report and review of the
literature. J Oral Maxillofac Surg. 50:1015–1017. 1992.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lugo M, Reyes JM and Putong PB: Benign
chondrolipomatous tumors of the breast. Arch Pathol Lab Med.
106:691–692. 1982.PubMed/NCBI
|
|
12
|
Katzer B: Histopathology of rare
chondroosteoblastic metaplasia in benign lipomas. Pathol Res Pract.
184:437–445. 1989.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Shintaku M, Yamamoto Y, Kono F, Kitai T,
Tsuji W, Yotsumoto F and Kushima R: Chondrolipoma of the breast as
a rare variant of myofibroblastoma: An immunohistochemical study of
two cases. Virchows Arch. 471:531–535. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ricardo CR, Renato S, Luiz F and Espana Q:
Breast reconstruction with parenchymal cross after giant lipoma
removal. Aesth Plast Surg. 32:695–697. 2008.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Jorwekar GJ, Baviskar PK, Sathe PM and
Dandekar KN: Giant chondroid lipoma of breast. Indian J Surg.
74:342–343. 2012.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Marsh WL Jr, Lucas JG and Olsen J:
Chondrolipoma of the breast. Arch Pathol Lab Med. 113:369–371.
1989.PubMed/NCBI
|
|
17
|
Perez MT and Alexis JB: Chondrolipoma of
the breast presenting as calcifications in a routine mammogram.
Histopathology. 35:189–191. 1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Stark AM and Sunter JP: Benign
chondrolipomatous tumour of the breast. Clin Radiol. 39:328–329.
1988.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Errarhay S, Fetohi M, Mahmoud S, Saadi H,
Bouchikhi C and Banani A: Primary chondrosarcoma of the breast: A
case presentation and review of the literature. World J Surg Oncol.
11(208)2013.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Nakanishi G, Lin SN, Asagoe K, Suzuki N,
Matsuo A, Tanaka R, Makino E, Fujimoto W and Iwatsuki K: A novel
fusion gene of collagen type 1 alpha 1 (exon 31) and platelet
derived growth factor B-chain (exon 2) in dermato fibrosarcome
protuberans. Eur J Dermatol. 17:217–219. 2007.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Montgomery E, Goldblum JR and Fisher C:
Myofibrosarcoma: A clinicopathologic study. Am J Surg Pathol.
25:219–228. 2001.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Morgan PB, Chundra S, Hatch SS, Hawkins
HK, Adegboyega PA and Eltorky MA: Uncommon malignancies: Case 1.
Low grade myofibroblastic sarcoma of the breast. J Clin Oncol.
23:6249–6251. 2005.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Stark M, Hoffman A and Xiong Z: Mammary
myofibrosarcoma: Case report and literature review. Breast J.
17:300–304. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Brenn T and Fletcher CD:
Radiation-associated cutaneous atypical vascular lesions and
angiosarcoma: Clinicopathologic analysis of 42 cases. Am J Surg
Pathol. 29:983–996. 2005.PubMed/NCBI
|
|
25
|
Cooper R, Rajak R, Valentine K and
Bhargava V: Metaplastic carcinoma of the breast. Diagnostic
Histopathol. 24:83–85. 2018.
|
|
26
|
Ginter PS, Mosquera JM, MacDonald TY,
D'Alfonso TM, Rubin MA and Shin SJ: Diagnostic utility of MYC
amplification and anti-MYC immunohistochemistry in atypical
vascular lesions, primar yor radiation induced mammary angiosarcoma
and primary angiosarcomas of other sites. Hum Pathol. 45:709–716.
2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Cornejo KM, Deng A, Wu H, Cosar EF, Khan
A, Cyr MS, Tomaszewicz K, Dresser K, O'Donnell P and Hutchinson L:
The utility of MYC and FLT4 in the diagnosis and treatment of post
radiation atypical vascular lesion and angiosarcoma. Hum Pathol.
46:868–875. 2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Maggiano F, Debiec-Rychter M, Vanbockrijck
M and Sciot R: Cellular angiofibroma: Another mesenchymal tumour
with 13q14 involvement, suggesting a link with spindle cell lipoma
and (extra)-mammary myofibroblastoma. Histopathology. 51:410–412.
2007.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Pasta V, Sottile D, Urciouli P, Del
Vecchio L, Custureri F and D'Orazi V: Rare chondrosarcoma of the
breast treated with quadrantectomy instead of mastectomy: A case
report. Oncol Lett. 9:1116–1120. 2015.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Pasta V, Monti M, Cialini M, Vergine M,
Urciuoli P, Iacovelli A, Rea S and D'Orazi V: Primitive sarcoma of
the breast: New insight on the proper surgical management. J Exp
Clin Cancer Res. 34(72)2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Thilagavath G, Subramanian S, Samuel AV,
Rani U and Somasundaram C: Primary chondrosarcoma of the breast. J
Indian Med Assoc. 90:16–17. 1992.PubMed/NCBI
|
|
32
|
Vandenhaute B, Validire P, Veillex C,
Voelh P and Zafrani B: Breast carcinoma with chondroid metaplasia.
Ann Pathol. 15:53–58. 1995.PubMed/NCBI
|
|
33
|
Pencavel TD and Hayes A: Breast sarcoma-a
review of diagnosis and management. Int J Surg. 7:20–23.
2009.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Pasta V, Monti M, Antonucci D, Di Matteo
FM, Boccaccini F and Brescia A: Primary sarcoma of the breast:
Criteria for radical surgery. G Chir. 18:703–706. 1997.PubMed/NCBI
|
|
35
|
Stojadinovic A, Leung DH, Hoos A, Jaques
DP, Lewis JJ and Brennan MF: Analysis of the prognostic
significance of microscopic margins in 2,084 localized primary
adult soft tissue sarcomas. Ann Surg. 235:424–434. 2002.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zelek L, Llombart-Cussac A, Terrier P,
Pivot X, Guinebretiere JM, Le Pechoux C, Tursz T, Rochard F,
Spielmann M and Le Cesne A: Prognostic factors in primary breast
sarcomas: A series of patients with long-term follow-up. J Clin
Oncol. 21:2583–2588. 2003.PubMed/NCBI View Article : Google Scholar
|