1. Introduction
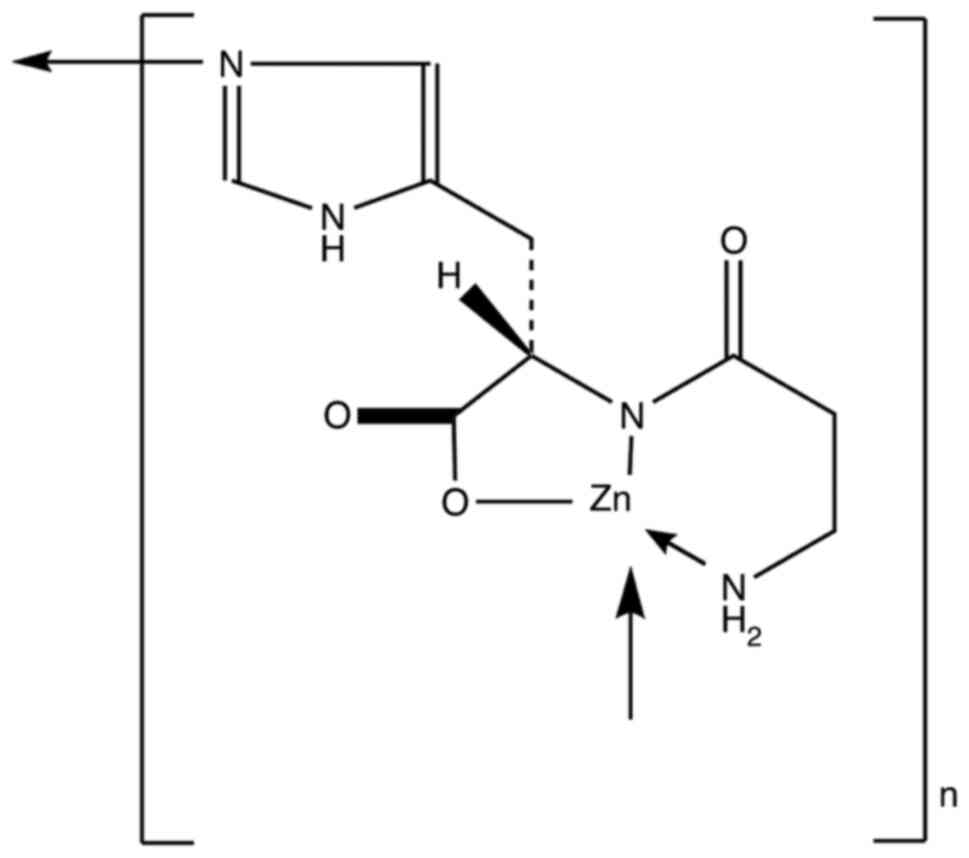
Polaprezinc, a chelated form of zinc (Zn) and
L-carnosine, is a new generation gastric mucosal protective agent
that has been used in clinical for more than 20 years in Japan
(1). The structural formula is
presented in Fig. 1. Polaprezinc
can improve the eradication rates of Helicobacter pylori,
which has been verified in clinical practice (2). Polaprezinc also provides mucosal
protection by increasing heat shock protein expression (3-5)
and presenting antioxidant (6) and
antiapoptotic (7) effects. It can
also inhibit the expression of inflammatory factors (8-10),
as well as stimulate the proliferation and migration of granulation
tissue in injured epithelial cells (11). Polaprezinc can therefore promote
the healing of peptic ulcers and improve the quality of ulcer
healing (12,13). Polaprezinc might have a broad
clinical application prospect.
2. Patents and preparations
Patents
Japan applied to the first world patent for
polaprezinc in 1989 (patent no. WO9015616), which is an application
patent for gastric ulcer, followed by a patent application for
liver fibrosis in 2004 (patent no. JP4802470B2) (14) and a patent application for an
orally disintegrating tablet in 2016 (patent no. JP2017002045A)
(15). However, the patent
application for the core compound of polaprezinc was not covered in
China. In 2012, China produced its first generic drug indicated for
gastric ulcer, which was approved for listing by the State Food and
Drug Administration (Jilin Broadwell Pharmaceutical Co., Ltd.). In
2016, a related patent was applied for in China. The subjects of
the application and authorization were relatively similar, in terms
of compounds, preparation methods and application patents (16-18).
Preparations
Polaprezinc preparations in Japan include granules,
tablets and orally disintegrating tablets, whereas those in China
mainly come in the form of granules. To improve the dissolution of
polaprezinc, the granular formulation contains polaprezinc,
ethanol, mannitol, povidone K-30, cyclodextrin, trehalose, maltitol
and pregelatinized starch prepared dispersion. This formula can
also enhance the stability and bioavailability of polaprezinc. The
combination preparation of polaprezinc and other active ingredients
also represents an effective research and development strategy. An
in vitro pharmacological study demonstrated that, combined
with the conventional antibiotics levofloxacin, doxycycline,
ceftazidime and clarithromycin, polaprezinc exhibits an
antibacterial activity superior to that of the antibiotic-alone
group, indicating a significant synergistic effect (19). Furthermore, the combination of
polaprezinc and proton pump inhibitors (PPIs) can significantly
accelerate the rate of ulcer healing following endoscopic
submucosal dissection (ESD), leading to improved quality of healing
and reduced incidence of postoperative complications (20).
3. Synthetic route and pharmacokinetics of
polaprezinc
Synthesis route
Polaprezinc is a complex of L-carnosine and Zn.
Thus, the synthesis of polaprezinc can be decomposed into
L-carnosine synthesis and L-carnosine-Zn salt complexation.
b-Dihydro-1,3-thiazol-2,4-dione was synthesized from alanine and
methyl o-ethyl xanthate, then acylated with L-histidine to obtain
L-carnosine and finally complexed with zinc acetate to obtain
polaprezinc.
Pharmacokinetics
The intestinal absorption of L-CAZ was studied in
rats by Matsukura and Tanaka (21)
using 14C- and 65Zn-labeled compounds. L-CAZ
was suggested to dissociate to its components, L-carnosine and Zn,
during intestinal absorption. After a single administration of
14C-labeled L-CAZ to rats, the accumulated excretion
rates of L-CAZ were 4.1% in urine, 13.3% in feces, and 38.8% in
exhalation. For 65Zn-labeled L-CAZ, the excretion rates
were 0.3% in urine and 85.0% in feces. The absorption rate of Zn
was estimated to be 11%.
In another study, seven healthy subjects received
polaprezinc (75 mg) in a single oral administration (22). The highest plasma Zn concentration
was reached 1.6 h after the drug was ingested and was 1.9
µg/ml.
Evaluation of the rat model of acetic acid-induced
ulcer showed that the Zn concentration at the ulcer site was still
higher compared with that before administration and 12 h after
polaprezinc (50 mg/kg) was administered. During absorption, the
product dissociates into carnosine, which is metabolized into
L-histidine and aminoacrylic acid. The amino acids and absorbed Zn
are then metabolized according to the endogenous metabolic system
(23). Zn is mainly excreted in
the feces, with excretion rates of 0.47% when taking polaprezinc
(150 mg) on an empty stomach and of 0.12% after a meal. If
polaprezinc is taken orally for 7 consecutive days, the excretion
rate of Zn in urine for one day is 0.21-0.46%. If 300 mg of
polaprezinc is taken on an empty stomach, the excretion rates of Zn
in feces in 24 and 48 h are 41.4 and 58.8%, respectively. The Zn
content in feces is twice that before taking the drug because the
accumulation rate of Zn is relatively low.
4. Pharmacological study of polaprezinc
Anti-ulcer effect
Polaprezinc is effective in all experimental models,
including emergency gastric injury, aspirin hydrochloride gastric
injury, histamine gastric injury and ethanol hydrochloric acid
gastric injury (24), and presents
a dose-dependent efficiency, particularly for ethanol hydrochloride
gastric injury and duodenal ulcer. An in vitro experiment
demonstrated that polaprezinc can inhibit the secretion of pepsin
in rat gastric epithelial cell line RGM1 and therefore
significantly reduce the damage to gastric mucosa. Polaprezinc is
therefore an anti-ulcer drug with enhanced defensive factors
(25).
Anti-Helicobacter pylori (H. pylori)
effect
Previous in vivo and in vitro studies
have confirmed that polaprezinc exerts an anti-H. pylori
effect (19), which is mainly
attributed to Zn ions. Polaprezinc can significantly increase
antibacterial activity in the stomach due to its chelating
structure and because it can effectively adhere to damaged gastric
mucosa. The results indicated that the eradication rate of H.
pylori in polaprezinc (150 mg/d) combined with conventional
triple therapy (omeprazole 40 mg/d, amoxicillin 2 g/d and
clarithromycin 1 g/d) was significantly higher compared with that
of conventional triple therapy (ITT 77 vs. 58.6%, PP 81.1 vs.
61.4%) (2). H. pylori
produces a large amount of active urease, which is an important
pathogenic factor for H. pylori infection. Zn and
L-carnosine, two important components of polaprezinc, can
significantly inhibit urease activity. Urease is a nickel
metalloenzyme, which activity is determined by the nickel content
of the active site. The urease gene cluster ureABIEFGH contains at
least seven essential genes, including ureA and ureB, which are
structural genes, ureEFGH, which is an auxiliary gene and ureI,
which is a gene unique to Hp urease. Urease helper genes
facilitate the insertion of nickel into ureA/ureB protein active
sites to form active proteins. Urease activation requires the
insertion of two nickels in the six active sites of the whole
enzyme. The protein encoded by the helper gene plays therefore an
important role in the polymerization of nickel ions to the active
site of the enzyme. Zn can induce the substitution reaction of
nickel ions in the urease molecule and change the conformation of
the urease, significantly inhibiting its enzyme activity (26). In addition, carnosine is composed
of alanine and histidine, and histidine can effectively adjust the
Zn ion and accurately insert it into the structural site of the
enzyme, significantly inhibiting urease activity. Carnosine can
also regulate the accurate insertion of Zn ions into the active
site of the zymogen and replace the nickel ion (27).
Promotion of healing
Polaprezinc promotes healing in the rat model of
chronic ulcer (28). A study
selected numerous acetate ulcer models (AAUs) and iron-ascorbic
acid models (FAUs) to determine the ulcer area, and hydroxyproline
(HYP) and DNA contents at the ulcer site were used as indicators
(29). Following oral
administration of polaprezinc at the concentrations of 1, 3 and 10
mg/kg, the ulcer areas of the models of AAUs and FAUs decreased on
day 4 of ulceration, but the ulcer did not heal completely on Day
14. The lysine content of the polaprezinc group increased on Days 4
(4.3±0.8 µg/mg) and 7 (10.7±1.2 µg/mg) of ulceration compared with
the control group, and significantly increased on day 11. The DNA
content of the FAU model was significantly lower than that of the
non-ulcer site on Day 7 of ulceration. However, the DNA content of
the AAU model was not reduced, although the DNA content of the two
model ulcer sites on Day 11 was significantly higher than that of
the non-ulcer site. The contents returned to their normal levels
after 14 days. For both models, the HYP content in the ulcer site
was increased in a dose-dependent manner when a polaprezinc dose of
1-10 mg/g was given (29). When a
polaprezinc dose of 3 mg/kg was administered to the AAUs on Day 4
of ulceration and to FAUs on Day 7 of ulceration, the DNA contents
returned to normal levels faster, compared with the control group
(30). Furthermore, the healing
effect of polaprezinc on ulcers is attributed to its antioxidative
property. A previous study reported that polaprezinc significantly
reduces the gastric ulcer area in a dose-dependent manner, with a
concomitant reduction in the activities of xanthine oxidase and
myeloperoxidase; meanwhile, it also reduces the malondialdehyde
level in the ulcerated mucosa. Polaprezinc can restore the
glutathione level in the mucosa. It can also consistently
downregulate the protein expression of tumor necrosis factor-α,
interleukin-1β, macrophage inflammatory protein-2 and
cytokine-induced neutrophil chemoattractant-2a, which are all
activated in the ulcerated tissues to promote the healing of ulcer
mucosa (31).
Anti-liver fibrosis
Hepatic fibrosis is caused by fibrocytes stimulated
by certain infections, such as hepatitis B and hepatitis C
infections, producing therefore a large amount of extracellular
matrix (ECM). Up to 90% of patients with liver cancer present with
advanced liver fibrosis or cirrhosis. Static hepatic stellate cells
in the space around the liver sinusoids are the main producers of
liver ECM and are considered as key factors for liver fibrosis
(14,32). The study by Ye et al
(33) reported that polaprezinc
can inhibit the proliferation and migration of hepatic stellate
cells. Furthermore, the expression of liver fibrosis markers,
including type I collagen, fibronectin, and α-smooth muscle actin,
is downregulated following treatment with polaprezinc. Gene chip
analysis through microarray analysis was performed using OneArray,
which contains 31,741 mRNA probes, detecting 20,672 genes in the
human genome. It was found that 202 differentially expressed genes
were altered by >1.5 times after polaprezinc treatment, Changes
in these genes were associated with tumor cell proliferation,
migration and cytoskeletal structure. In the animal model of
hepatic fibrosis induced by thioacetamide, 200 mg/day polaprezinc
significantly inhibits the expression of matrix metalloproteinase
(MMP)-2 and MMP-9 while reducing the area of liver fibrosis. A
Japanese clinical study reported that patients with hepatitis C and
cirrhosis that were treated with 150 mg/day polaprezinc for 3
years, had significantly decreased levels of alanine
aminotransferase and aspartate aminotransferase after those 3 years
compared with patients in the control group (P=0.0293). Taken
together, these findings suggested that polaprezinc can be
considered as a novel treatment method for patients with liver
cirrhosis (34).
5. Clinical uses of polaprezinc
H. pylori eradication
A previous study reported that polaprezinc can
significantly reduce urease activity and inhibit the levels of
inflammation and oxidative stress caused by H. pylori
infection (35). Kashimura et
al (19) demonstrated that
polaprezinc has a potential role in H. pylori eradication
therapy. This study included 66 patients with H. pylori
infection, and dyspepsia was studied for 7 days. The quadruple
therapy group of patients (lansoprazole, amoxycillin,
clarithromycin and polaprezinc) who received polaprezinc had a 17%
higher H. pylori eradication rate than patients in the
triple therapy group (lansoprazole, amoxycillin and clarithromycin)
(P<0.05). To further compare the efficacy and safety of
polaprezinc-containing quadruple therapy and triple therapy for the
eradication of H. pylori, a prospective, multicenter,
randomized, parallel, open-label, controlled and multicenter
clinical study was conducted by the Department of Gastroenterology
of Peking Union Medical College Hospital in 11 cities across the
country. This study found a significant increase in the H.
pylori eradication rate in the polaprezinc quadruple therapy
compared with that in the standard triple therapy. The difference
in rate reached 19.7% (per protocol analysis, 81.1 vs. 61.4%)
(2), suggesting that polaprezinc
can also enhance resistance of the gastric mucosa to H.
pylori infection and that polaprezinc could be used for H.
pylori eradication treatment.
Application after ESD
With the introduction of ESD in the late 1990s, the
indications for early gastric cancer endoscopic treatment have
further expanded (36). Minimally
invasive and exhibiting good efficacy, ESD is currently the
standard method for endoscopic treatment of early gastric cancer
and precancerous lesions (20). At
present, patients following upper gastrointestinal ESD routinely
use PPIs to stimulate ulcer healing. A meta-analysis conducted by
Nishizawa et al (20)
reported that PPI combined with gastric mucosal protective agents
is significantly more effective than PPI alone. Furthermore, a
study by Inaba et al (37)
included 163 patients after ESD surgery, who were randomly assigned
to take either lansoprazole daily (30 mg) or lansoprazole (30 mg)
combined with polaprezinc (150 mg) daily. After 2 months, the ulcer
healing scores of patients who received the lansoprazole combined
with polaprezinc treatment were significantly increased
(P<0.0001) compared with the lansoprazole group, while the ulcer
base protrusion rate was significantly decreased (P<0.0001).
Polaprezinc therefore provides more choices for postoperative ESD
drug applications.
Drug-related gastrointestinal mucosal
injury
In a randomized controlled study (n=20) conducted by
Watari et al (38),
patients with small-bowel mucosal injuries that had been treated
with low-dose aspirin for an extended time were orally administered
polaprezinc (150 mg) daily. After 4 weeks, the number of lower
lesions (including erythema and ulcers) was significantly reduced
in the polaprezinc treatment group compared with the control group,
as revealed by capsule endoscopy (P<0.05). These results
indicate that polaprezinc effectively protects the mucosa against
low-dose aspirin-induced small-bowel injuries. The underlying
mechanisms remain unknown and require further investigation.
Mucosal damage caused by radiotherapy
Oral mucositis
A prospective Japanese study reported that patients
with head and neck tumors who received radiotherapy and
chemotherapy combined with polaprezinc treatment had a lower
incidence of severe oral mucositis compared with the control group
who did not received polaprezinc (39.3 vs. 60.7%) (39). In patients with leukemia who
received chemotherapy and radiotherapy and an allogeneic bone
marrow stem cell transplant (40),
the incidence of moderate to severe oral mucositis is significantly
reduced in the polaprezinc-treated group compared with the control
group (20 vs. 82%; P<0.01). Ishihama et al (41) reported that a polaprezinc mouth
rinse effectively improves oral mucosal injury in 423 patients with
symptoms of oral mucosal injury as a result of cancer treatment.
The effects of the polaprezinc rinse were evaluated according to
the cancer treatment method. The stomatitis prevention success
rate, symptom improvement rate, pain prevention success rate and
symptom improvement rate were 68.5, 84.4, 75.4 and 76.7%,
respectively, for patients who received chemotherapy (n=280), 32.7,
64.5, 45.5 and 73.5%, respectively, for patients who received
chemoradiation therapy (n=95), and 29.6, 60.0, 40.7 and 68.6%,
respectively, for patients who received radiotherapy alone.
Radioactive esophagitis
Hayashi et al (42) conducted a randomized controlled
study on patients with non-small cell lung cancer treated with
radiotherapy and chemotherapy at Gifu University Hospital between
2011 and 2015. The results demonstrated that the polaprezinc group
can prevent patients from developing grade 2 or higher radiation
esophagitis compared with the group not treated with polaprezinc
(hazard ratio=0.397; 95% confidence interval=0.160-0.990;
P=0.047).
Radioactive gastroenteritis
Patients with hematological malignancies often
require systemic radiotherapy before stem cell transplantation. One
of the common adverse reactions is radiation gastritis. Masayuki
et al (43) reported that
oral administration of polaprezinc before oral systemic
radiotherapy leads to a lower incidence of radiation gastritis
(P=0.046). Furthermore, in another study, female Wister rats aged 5
weeks were treated with polaprezinc enema for 10 days following
rectal radiation. Endoscopic and histological analyses demonstrated
that mucosal inflammation is significantly reduced in theses rats
compared with control group (44).
Another study also reported that administration of 100 mg/kg
polaprezinc 2 h before experiment can reduce the apoptosis of
intestinal epithelial cells in the duodenum, jejunum and ileum
during ion beam injury, protecting the normal epithelial cells in
the intestine (45).
Treatment of ulcerative colitis
The pathogenesis of ulcerative colitis is currently
unclear. It is a chronic, recurrent intestinal inflammatory disease
characterized by diffuse inflammation and ulcers. A previous study
demonstrated that serum zinc concentration is reduced in patients
with inflammatory bowel disease (IBD), and that severe IBD patients
have serum zinc deficiency. After the polaprezinc treatment, the
serum zinc level can be increased and maintained in the normal
range (46). A study of
2,4,6-trinitrobenzenesulphonic acid-induced colitis in rats,
demonstrated that, compared with the control group, the polaprezinc
(60 mg/kg/d) group could significantly inhibit the activation of
calcineurin and the expression of proinflammatory cytokines in the
mucosa, thus improving the symptoms of ulcerative colitis (47). Moreover, an in vitro study
demonstrated that the viability of T cells was not affected by
polaprezinc (47).
6. Other clinical applications
Taste disorders
Taste disorders are often associated with oral
mucositis and can be additional side effects of chemotherapy and
radiotherapy (48). Cancer
patients undergoing chemotherapy often experience changes in taste
perception. Multiple evidence suggests that taste disorders are
associated with zinc deficiency, since enzymes that require zinc
are found in the taste buds and that they play an important role in
the function of taste (49). A
study was performed to evaluate the presence of taste alteration
and the effectiveness of polaprezinc administration in 136 female
patients with breast cancer who underwent FE100 therapy. Of 58
patients with taste alteration, 20 received polaprezinc, with the
following outcomes: Taste alteration improved in 70.0% of the
patients, no change was observed in 25.0% and the condition
decreased in 5.0%. Multivariate regression analysis indicated that
the body surface area and low hemoglobin levels were independent
factors that caused changes in taste (P=0.003 and P=0.021,
respectively) (50). Another
multicenter, randomized, double-blind and placebo-controlled
clinical study revealed that treatment with 68 mg of polaprezinc
daily for 12 weeks is also effective for patients with idiopathic
taste disorders (51).
Treatment of chronic obstructive
pulmonary disease
Kimura et al (52) used the human cancer lung epithelial
cell line A549 to evaluate the effect of polaprezinc on
cadmium-induced apoptosis. Polaprezinc was found to inhibit
CdCl2-induced apoptosis of human lung epithelial cells.
This inhibition suppressed the production of cadmium-dependent
reactive oxygen species, significantly inhibiting the
cadmium-induced apoptosis of lung epithelial cells. The study also
demonstrated that the anti-oxidative effect of polaprezinc is
mediated via the induction of metallothionein. Therefore, it is
hypothesized that Polaprezinc might also be used to treat
respiratory diseases such as chronic obstructive pulmonary
disease.
7. Safety
In a previous study from our laboratory, specific
adverse events that have been reported to be associated with
high-dose zinc (120 mg/kg) daily were not observed (16); however, if required, zinc
concentration may be kept under monitoring while treating patients
with polaprezinc. Polaprezinc granules are a gastric mucosal
protective drug, which can prevent acute injury of rat gastric and
duodenal ulcer models and have a healing effect of chronic gastric
ulcers in rat models. In the long-term toxicity test, rats present
with salivation after oral administration of polaprezinc at a dose
of 300 mg/kg or more for 13 weeks. Oral administration of
polaprezinc at a dose of 600 mg/kg or more will cause a decrease in
hemoglobin concentration, a decrease in hematocrit value and
reticulocyte count, elevated glutamic-pyruvic transaminase,
pathological examination of pancreatic fibrosis and erosions. A
high dose of polaprezinc (1,200 mg/kg) causes side effects of
sedation, erect hair, abdominal enlargement and diarrhea, in
addition to a mortality rate of 40% in rats. The dead rats all
presented with pancreatic fibrosis, thymus atrophy, adrenal cortex
fatty degeneration and bone marrow suppression. The aforementioned
adverse reactions caused by drugs can return to normal after drug
withdrawal. In clinic, the main side effects of polaprezinc are
nausea, vomiting, constipation or diarrhea. Some patients may have
abnormal liver function, but these side effects are generally
temporary and will eventually disappear. If the side effects are
serious, other types of gastric drugs can be used for treatment. In
addition, polaprezinc may interact with some other drugs. For
example, when this product is taken simultaneously with
penicillamine and levothyroxine sodium, it can form a chelate to
reduce the absorption level of polaprezinc and reduce its curative
effect. Therefore, taking these drugs together should be avoided.
It is therefore crucial to inform the clinician of additional
medications taken by the patient. The use of polaprezinc granules
should be carried out under the guidance of the doctor (53).
The specific adherence of polaprezinc at the ulcer
lesion is attributed to the formation of a new chemical bond
between zinc and body components, such as albumin or other proteins
to form mixed ligand complexes. L-carnosine still binds with Zn at
this stage. These body components emerging from the ulcer site can
bind strongly to zinc ions with functional groups such as
sulfhydryl or imidazole. L-carnosine, which possesses wound healing
properties owing to its free radical-scavenging properties, is
released on the ulcer lesion via a complete ligand exchange
reaction with a body component such as albumin or other proteins to
form mixed ligand complexes capable of forming a complex of a
larger stability constant than that of the complex formed from
L-carnosine (21). Simultaneously,
zinc with a protective effect on membranes is captured completely
by the body component (such as albumin) and penetrates into the
ulcer to ease inflammation (21).
However, a typical composition of polaprezinc particles is 22% zinc
and 78% L-carnosine (excipient is starch), which typically delivers
~15-16 mg of zinc, which should not be a concern. In addition,
polaprezinc has a long-established safety profile based on
long-term use in humans and several preclinical and human clinical
studies (2,19,20,46)
with no adverse events reported.
8. Conclusions
Apart from those in Japan, the number of patent
applications for polaprezinc in China has increased. However,
recent preparation routes and crystal-type inventions still show
significant effects. Combined with other active ingredients,
polaprezinc exerts evident synergistic effects and can therefore
serves as a guide for the preparation of similar compositions with
potentially improved synergy. Polaprezinc has multiple mechanisms
of action, which vary from those of other mucosal protective
agents. Comprehensive research on polaprezinc will help to expand
the clinical application of polaprezinc.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
ML and ZS designed the concept, wrote the
manuscript, collected and sorted the literature and revised the
article. HZ and ZL analyzed, interpreted the information and
participated in the modification and revision. All authors have
read and approved the final manuscript. Data sharing is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Seiki M, Ueki S, Tanaka Y, Soeda M, Hori
Y, Aita H, Yoneta T, Morita H, Tagashira E and Okabe S: Studies on
anti-ulcer effects of a new compound, zinc l-carnosine (z-103).
Nihon Yakurigaku Zasshi. 95:257–269. 1990.PubMed/NCBI View Article : Google Scholar : (In Japanese).
|
|
2
|
Tan B, Luo HQ, Xu H, Lv NH, Shi RH, Luo
HS, Li JS, Ren JL, Zou YY, Li YQ, et al: Polaprezinc combined with
clarithromycin-based triple therapy for Helicobacter
pylori-associated gastritis: A prospective, multicenter, randomized
clinical trial. PLoS One. 12(e0175625)2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Wada I, Otaka M, Jin M, Odashima M,
Komatsu K, Konishi N, Matsuhashi T, Horikawa Y, Ohba R, Itoh H and
Watanabe S: Expression of HSP72 in the gastric mucosa is regulated
by gastric acid in rats-Correlation of HSP72 expression with
mucosal protection. Biochem Biophys Res Commun. 349:611–618.
2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Qin Y, Naito Y, Handa O, Hayashi N, Kuki
A, Mizushima K, Omatsu T, Tanimura Y, Morita M, Adachi S, et al:
Heat shock protein 70-dependent protective effect of polaprezinc on
acetylsalicylic acid-induced apoptosis of rat intestinal epithelial
cells. J Clin Biochem Nutr. 49:174–181. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ohkawara T, Nishihira J, Nagashima R,
Takeda H and Asaka M: Polaprezinc protects human colon cells from
oxidative injury induced by hydrogen peroxide: Relevant to
cytoprotective heat shock proteins. World J Gastroenterol.
12:6178–6181. 2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Ueda K, Ueyama T, Oka M, Ito T, Tsuruo Y
and Ichinose M: Polaprezinc (Zinc L-Carnosine) is a potent inducer
of anti-oxidative stress enzyme, Heme Oxygenase (HO)-1-a new
mechanism of gastric mucosal protection. Pharmacol Sci.
110:285–294. 2009.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Omatsu T, Naito Y, Handa O, Mizushima K,
Hayashi N, Qin Y, Harusato A, Hirata I, Kishimoto E, Okada H, et
al: Reactive oxygen species-quenching and anti-apoptotic effect of
polaprezinc on indomethacin-induced small intestinal epithelial
cell injury. J Gastroenterol. 45:692–702. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Shimada T, Watanabe N, Ohtsuka Y, Endoh M,
Kojima K, Hiraishi H and Terano A: Polaprezinc Down-regulates
proinflammatory cytokine-induced nuclear Factor-kappaB activation
and Interleukin-8 expression in gastric epithelial cells. J
Pharmacol Exp Ther. 291:345–352. 1999.PubMed/NCBI
|
|
9
|
Handa O, Yoshida N, Tanaka Y, Ueda M and
Yoshikawa T: Inhibitory effect of polaprezinc on the inflammatory
response to Helicobacter pylori. Can J Gastroenterol. 16:785–789.
2002.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Ohata S, Moriyama C, Yamashita A, Nishida
T, Kusumoto C, Mochida S, Minami Y, Nakada J, Shomori K, Inagaki Y,
et al: Polaprezinc protects mice against endotoxin shock. J Clin
Biochem Nutr. 46:234–243. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Watanabe S, Wang XE, Hirose M, Kivilioto
T, Osada T, Miwa H, Oide H, Kitamura T, Yoneta T and Seto K:
Insulin-like growth factor I Plays a role in gastric wound healing:
Evidence using a zinc derivative, polaprezinc, and an in vitro
rabbit wound repair model. Aliment Pharmacol Ther. 12:1131–1138.
1998.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Seto K, Yoneta T, Suda H and Tamaki H:
Effect of polaprezinc (N-(3-aminopropionyl)-L-histidinato zinc), a
novel antiulcer agent containing zinc, on cellular proliferation:
Role of insulin-like growth factor I. Biochem Pharmacol.
58:245–250. 1999.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Jung DH, Park JC, Lee YC, Lee SK, Shin SK,
Chung H, Park JJ, Kim JH, Youn YH and Park H: Comparison of the
efficacy of Polaprezinc plus proton pump inhibitor and rebamipide
plus proton pump inhibitor treatments for endoscopic submucosal
dissection-induced ulcers. Clin Gastroenterol. 55:233–238.
2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kono T, Asama T, Chisato N, Ebisawa Y,
Okayama T, Imai K, Karasaki H, Furukawa H and Yoneda M: Polaprezinc
prevents ongoing thioacetamide-induced liver fibrosis in rats. Life
Sci. 90:122–130. 2012.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Katayama S, Nishizawa K, Hirano M,
Yamamura S and Momose Y: Effect of polaprezinc on healing of acetic
acid-induced stomatitis in hamsters. J Pharm Pharm Sci. 3:114–117.
2000.PubMed/NCBI
|
|
16
|
Liu Z, Xie W, Li M, Teng N, Liang X, Zhang
Z, Yang Z and Wang X: Oral administration of polaprezinc attenuates
fluorouracil induced intestinal mucositis in a mouse model. Basic
Clin Pharmacol Toxicol. 121:480–486. 2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Liu ZY, Xie WB, Li MR, Teng N, Liang X and
Zhang ZQ: Effects of polaprezinc on gastric mucosal damage and
neurotransmitters in a rat model of chemotherapy-induced vomiting.
Int Med Res. 46:2436–2444. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Liu ZY, Xie WB, Li MR, Liu J, Liang X and
Li T: Intrarectally administered polaprezinc attenuates the
development of dextran sodium sulfate-induced ulcerative colitis in
mice. Exp Ther Med. 18:4927–4934. 2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kashimura H, Suzuki K, Hassan M, Ikezawa
K, Sawahata T, Watanabe T, Nakahara A, Mutoh H and Tanaka N:
Polaprezinc, a mucosal protective agent, in combination with
lansoprazole, amoxicillin and clarithromycin increases the cure
rate of Helicobacter pylori infection. Aliment Pharmacol Ther.
13:483–487. 1999.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Nishizawa T, Suzuki H, Kanai T and Yahagi
N: Proton pump inhibitor alone vs proton pump inhibitor plus
mucosal protective agents for endoscopic submucosal
dissection-induced ulcer: A systematic review and meta-analysis. J
Clin Biochem Nutr. 56:85–90. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Matsukura T and Tanaka H: Applicability of
zinc complex of L-carnosine for medical use. Biochemistry (Mosc).
65:817–823. 2000.PubMed/NCBI
|
|
22
|
Matsuda K, Mera Y, Wada H, Aruga H, Saik Y
and Taniguchi Y: Repeated dose toxicity studies on
catena-(S)-[mu-[N alpha-(3-aminopropionyl)
histidinato(2-)-N1,N2,O:N tau]-zinc] in rats.
Arzneimittelforschung. 41(1036)1991.PubMed/NCBI
|
|
23
|
Furuta S, Toyama S, Miwa M and Sano H:
Disposition of polaprezinc (zinc L-carnosine complex) in rat
gastrointestinal tract and effect of cimetidine on its adhesion to
gastric tissues. J Pharm Pharmacol. 47:632–636. 1995.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Choi HS, Lim JY, Chun HJ, Lee M, Kim ES,
Keum B, Seo YS, Jeen YT, Um SH, Lee HS, et al: The effect of
polaprezinc on gastric mucosal protection in rats with ethanol
induced gastric mucosal damage: Comparison study with rebamipide.
Life Sci. 93:69–77. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Fujii Y, Matsura T, Kai M, Kawasaki H and
Yamada K: Protection by polaprezinc, an anti-ulcer drug, against
indomethacin-induced apoptosis in rat gastric mucosal cells. Jpn J
Pharmacol. 84:63–70. 2000.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Yakoob J, Abbas Z, Jafri W, Usman MW and
Awan S: Zinc chloride inhibits Helicobacter pylori growth and
reduces expression of interleukin-1beta by gastric epithelial
cells. Br J Biomed Sci. 71:43–45. 2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ishihara R, Iishi H, Sakai N, Yano H, Uedo
N, Narahara H, Iseki K, Mikuni T, Ishiguro S and Tatsuta M:
Polaprezinc attenuates Helicobacter pylori-associated gastritis in
Mongolian gerbils. Helicobacter. 7:384–389. 2010.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Naito Y, Yoshikawa T, Yagi N, Matsuyama K,
Yoshida N, Seto K and Yoneta T: Effects of polaprezinc on lipid
peroxidation, neutrophil accumulation, and TNF-alpha expression in
rats with aspirin-induced gastric mucosal injury. Dig Dis Sci.
46:845–851. 2001.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Aita H, Yoneta T, Seto K, Morit H, Hori Y,
Takemasa T, Chaki K, Yamada H, Seiki M and Tagashira E: Studies on
the healing promoting action of Z-103 in chronic gastric ulcer
models of rats. Nihon Yakurigaku Zasshi. 99:345–352.
1992.PubMed/NCBI View Article : Google Scholar : (In Japanese).
|
|
30
|
Odashima M, Otaka M, Jin M, Wada I,
Horikawa Y, Matsuhashi T, Ohba R, Hatakeyama N, Oyake J and
Watanabe S: Zinc L-carnosine protects colonic mucosal injury
through induction of heat shock protein 72 and suppression of
NF-kappaB activation. Life Sci. 79:2245–2250. 2006.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Ko JK and Leung CC: Ginger extract and
polaprezinc exert gastroprotective actions by anti-oxidant and
growth factor modulating effects in rats. J Gastroenterol Hepatol.
25:1861–1869. 2010.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Matsuoka S, Matsumura H, Nakamura H,
Oshiro S, Arakawa Y, Hayashi J, Sekine N, Nirei K, Yamagami H,
Ogawa M, et al: Zinc supplementation improves the outcome of
chronic hepatitis C and liver cirrhosis. J Clin Biochem Nutr.
45:292–303. 2009.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Ye J, Zhang ZS, Zhu L, Lu FM, Li Y, Zhou
JJ, Lu XL and Du Q: Polaprezinc inhibits liver fibrosis and
proliferation in hepatocellular carcinoma. Mol Med Rep.
16:5523–5528. 2017.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Matsumura H, Nirei K, Nakamura H, Arakawa
Y, Higuchi T, Hayashi J, Yamagami H, Matsuoka S, Ogawa M, Nakajima
N, et al: Zinc supplementation therapy improves the outcome of
patients with chronic hepatitis C. J Clin Biochem Nutr. 51:178–184.
2012.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Amin M, Iqbal MS, Hughes RW, Khan SA,
Reynolds PA, Enne VI, Sajjad-ur-Rahman and Mirza AS:
Mechanochemical synthesis and in vitro anti-Helicobacter pylori and
uresase inhibitory activities of novel zinc(II)-famotidine complex.
J Enzyme Inhib Med Chem. 25:383–390. 2010.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Nishizawa T and Yahagi N: Endoscopic
mucosal resection and endoscopic submucosal dissection: Technique
and new directions. Curr Opin Gastroenterol. 33:315–319.
2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Inaba T, Ishikawa S, Toyokawa T, Ishikawa
H, Miyahara K, Wato M, Kawai K, Okada H and Yamamoto K: Basal
protrusion of ulcers induced by endoscopic submucosal dissection
(ESD) during treatment with proton pump inhibitors, and the
suppressive effects of polaprezinc. Hepatogastroenterology.
57:678–684. 2010.PubMed/NCBI
|
|
38
|
Watari I, Oka S, Tanaka S, Aoyama T,
Imagawa H, Shishido T, Yoshida S and Chayama K: Effectiveness of
polaprezinc for low-dose aspirin-induced small-bowel mucosal
injuries as evaluated by capsule endoscopy: A pilot randomized
controlled study. Gastroenterology. 13(108)2013.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Doi H, Fujiwara M, Suzuki H, Niwa Y,
Nakayama M, Shikata T, Odawara S, Takada Y, Kimura T, Kamikonya N
and Hirota S: Polaprezinc reduces the severity of radiation-induced
mucositis in head and neck cancer patients. Mol Clin Oncol.
3:381–386. 2015.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Hayashi H, Kobayashi R, Suzuki A, Ishihara
M, Nakamura N, Kitagawa J, Kanemura N, Kasahara S, Kitaichi K, Hara
T, et al: Polaprezinc prevents oral mucositis in patients treated
with high-dose chemotherapy followed by hematopoietic stem cell
transplantation. Anticancer Res. 34:7271–7277. 2014.PubMed/NCBI
|
|
41
|
Ishihama H, Sayo S, Yokoyama T, Ueno M,
Ebihara N, Doi Y, Asano K, Kawamata H, Imai H and Ueki K:
P1-032preventive and therapeutic effects of Polaprezinc suspension
on oral mucosal injury. Ann Oncol. 24:ix66–ix99. 2013.
|
|
42
|
Hayashi H, Kobayashi R, Suzuki A, Yamada
Y, Ishida M, Shakui T, Kitagawa J, Hayashi H, Sugiyama T, Takeuchi
H, et al: Preparation and clinical evaluation of a novel lozenge
containing polaprezinc, a zinc-L-carnosine, for prevention of oral
mucositis in patients with hematological cancer who received
high-dose chemotherapy. Med Oncol. 33(91)2016.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Masayuki F, Norihiko K, Keita T, Miwa I,
Masayuki I, Toshihiko I, Hiromi F, Chikaaki M and Norio N: Efficacy
and safety of polaprezinc as a preventive drug for
radiation-induced stomatitis. Nihon Igaku Hoshasen Gakkai Zasshi.
62:144–150. 2002.PubMed/NCBI(In Japanese).
|
|
44
|
Doi H, Kamikonya N, Takada Y, Fujiwara M,
Tsuboi K, Inoue H, Tanooka M, Nakamura T, Shikata T, Tsujimura T
and Hirota S: Efficacy of Polaprezinc for acute radiation Proctitis
in a rat model. Int J Radiat Oncol Biol Phys. 80:877–884.
2011.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Odawara S, Doi H, Shikata T, Kitajima K,
Suzuki H, Niwa Y, Kosaka K, Tarutani K, Tsujimura T, Kamikonya N
and Hirota S: Polaprezinc protects normal intestinal epithelium
against exposure to ionizing radiation in mice. Mol Clin Oncol.
5:337–381. 2016.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Itagaki M, Saruta M, Saijo H, Mitobe J,
Arihiro S, Matsuoka M, Kato T, Ikegami M and Tajiri H: Efficacy of
zinc-carnosine chelate compound, Polaprezinc, enemas in patients
with ulcerative colitis. Scand J Gastroenterol. 49:164–172.
2014.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Zhang Y, Okamura S, Kudo T, Masuo T and
Mori M: Calcineurin inhibition by polaprezinc in rats with
experimentally-induced colitis. Life Sci. 88:432–439.
2011.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Hewlings S and Kalman D: A review of
Zinc-L-Carnosine and its positive effects on oral Mucositis, taste
disorders, and gastrointestinal disorders. Nutrients.
12(665)2020.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Takaoka T, Sarukura N, Ueda C, Kitamura Y,
Kalubi B, Toda N, Abe K, Yamamoto S and Takeda N: Effects of zinc
supplementation on serum zinc concentration and ratio of
apo/holo-activities of angiotensin converting enzyme in patients
with taste impairment. Auris Nasus Larynx. 37:190–194.
2010.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Mizukami Y, Sato J, Nihei S, Kashiwaba M,
Kudo K, Okuyama H and Tamura K: The effectiveness of Polaprezinc
preparation for taste alteration in cancer chemotherapy. Gan To
Kagaku Ryoho. 43:979–983. 2016.PubMed/NCBI(In Japanese).
|
|
51
|
Sakagami M, Ikeda M, Tomita H, Ikui A,
Aiba T, Takeda N, Inokuchi A, Kurono Y, Nakashima M, Shibasaki Y
and Yotsuya O: A zinc-containing compound, Polaprezinc, is
effective for patients with taste disorders: Randomized,
double-blind, placebo-controlled, multi-center study. Acta
Otolaryngol. 129:1115–1120. 2009.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Kimura K, Nakano Y, Sugizaki T, Shimoda M,
Kobayashi N, Kawahara M and Tanaka KI: Protective effect of
polaprezinc on cadmium-induced injury of lung epithelium.
Metallomics. 11:1310–1320. 2019.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Japan standard commodity classification
No. 872329: 11, 2009. https://www.pmda.go.jp/PmdaSearch/iyakuDetail/GeneralList/2329027.
|