Introduction
Globally, as of June 7, 2021, there have been
173,005,553 confirmed cases of COVID-19, including 3,727,605
associated deaths, reported to the World Health Organization
(https://covid19.who.int). Even though mass
vaccination started early in December 2020 and nearly 2 billion
vaccine doses have been administered across the world (1), (https://covid19.who.int), we are standing on the verge
of the fourth wave of the COVID-19 pandemic.
From the pathophysiological point of view, in later
stages of the infection when viral replication accelerates,
epithelial-endothelial barrier integrity is compromised. The severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus infects
epithelial cells and, in addition, infects pulmonary capillary
endothelial cells, emphasizing the inflammatory response, and
triggering an influx of monocytes and neutrophils (2). The interstitial mononuclear
inflammatory infiltrates and edema that develop appear as
ground-glass opacities on computed tomography imaging. Early phase
acute respiratory distress syndrome (ARDS) sets in, as pulmonary
edema fills the alveolar spaces, with hyaline membrane formation
(3).
COVID-19 has proved to be one of the most
challenging diseases mankind has ever faced, with an extremely
intricate symptom pattern ranging from a dysregulated host response
to infection, which causes severe inflammation and cytokine storms,
to ARDS, coagulopathy, multi-organ failure and ultimately death
(2,4). Siddiqi and Mehra (5) proposed dividing the evolution of the
disease into three stages: Stage I (early infection); stage II
(moderate), pulmonary involvement (IIa) without hypoxia and (IIb)
with hypoxia; and stage III (severe), systemic hyperinflammation.
Stage I occurs at the inoculation and early stages of the disease.
Most people present with mild, non-specific symptoms such as fever,
dry cough and malaise. During stage II of the disease, a viral
pneumonia develops, possibly with hypoxia. If hypoxia occurs, it is
likely that patients will progress to requiring mechanical
ventilation. Stage III is an extrapulmonary systemic
hyperinflammation syndrome, where systemic inflammation markers are
elevated. COVID-19 infection results in a decrease in helper,
suppressor and regulatory T cell counts (5). The ‘Guidelines for the Diagnosis and
Treatment of Novel Coronavirus (2019-nCoV) Infection by the
[Chinese] National Health Commission (Trial Version 5)’ clinically
distinguishes four levels of severity: Mild, common, severe and
critical (6).
While the global medical community has worked around
the clock to find the best treatment for this disease, few
therapeutic options (corticosteroids: Dexamethasone, high level of
recommendation and rating of evidence; remdesivir, baricitinib,
tociliziumab, tofacitinib and sarilumab, lower level of
recommendation and rating of evidence) have proved to be successful
so far (4,7).
The aim of the present study was to determine
whether combining therapeutic plasma exchange (TPE) (a specific
therapeutic apheresis procedure with the goal of the rapid removal
of the patient's plasma and its ‘exchange’ with a replacement
solution) with convalescent plasma (CVP) transfusion (CVP therapy
uses blood from people who have recovered from an illness to help
others recover) early in the intensive care unit (ICU) stay
improves survival among severe and critically ill COVID-19
patients, and to evaluate the effects of this combined treatment on
patient outcomes and on other parameters, such as the partial
pressure of arterial oxygen to fractional inspired oxygen
(FiO2) ratio (P/F ratio), and C reactive protein (CRP),
lactate dehydrogenase (LDH) and ferritin levels.
Patients and methods
Study design, setting and
population
A total of 38 Caucasian patients were included in
the present single centre non-randomized controlled trial. The
patients were admitted to the ICU of the ‘Dr Teodor Andrei’
Municipal Hospital (Lugoj, Romania), a tertiary care hospital,
subordinated to ‘Pius Brinzeu’ Emergency Clinical County Hospital
(Timisoara, Romania), between August 8, 2020, and January 9, 2021.
All patients included in the study were adults (>18 years) who
presented with acute respiratory failure and ARDS, and had positive
reverse transcriptase-polymerase chain reaction (RT-PCR) test
results for SARS-CoV-2 virus upon hospital admission. ARDS was
defined as acute-onset hypoxemia (P/F ratio <300) with >50%
bilateral pulmonary opacities on chest imaging within 24-48 h that
were not fully explained by congestive heart failure and that
required ICU treatment and monitoring (8). Exclusion criteria were represented by
any of the following: Pregnancy, patients with suspected or
confirmed pulmonary embolisms and patients with terminal disease.
Patients enrolled in the study were divided equally,
non-randomized, into two groups as follows: A treatment group
administered sequential TPE and CVP transfusion in addition to the
standard treatment for COVID-19, and a control group administered
only standard treatment for COVID-19 (antiretrovirals,
corticosteroids, anticoagulants and antibiotics if deemed
necessary) according to hospital protocols.
All patients provided written informed consent
immediately after admission into the ICU regarding all the
procedures performed during hospitalization, including the
treatment scheme applied in the present study and the use of the
resulting data in scientific research publications, with the
assurance that they would remain anonymous. In cases where
obtaining informed consent from the patients was not possible due
to their critical medical condition, a legal representative was
informed and provided written consent. The trial was approved by
the Ethics Committee of ‘Pius Brinzeu’ Emergency Clinical County
Hospital Timisoara (approval no. 91/03.08.2020).
Study protocol
The blood type of the patients was determined
immediately upon being admitted to the ICU. In the treatment group,
a dual lumen, 14 French, dialysis catheter was used for vascular
access, by placing it in the femoral vein under echographic
guidance. A single TPE session was performed on the Infomed HF 440
machine (Infomed SA), with a plasma/blood separation ratio of 20%,
using 40 ml/kg fresh frozen plasma as the substitute. The circuit
was anticoagulated with unfractioned heparin during the procedure.
Upon completion of the TPE session, each patient from the treatment
group was transfused with 500 ml of ABO compatible CVP. Patients
were carefully monitored during both the TPE session and the CVP
transfusion, and also after the procedures, in order to treat
emerging complications.
Patients from the treatment and control groups
received standard treatment for COVID-19 according to hospital
protocols, consisting of corticosteroids, antiretrovirals,
anticoagulants and antibiotics if deemed necessary. Patients from
both groups were anticoagulated with subcutaneous nadroparine
(Fraxiparine; Aspen Pharma Trading) in therapeutic dosage, once
every 12 h, adjusted according to bodyweight (≤70 kg: 3,800 Anti-Xa
IU; >70 kg: 5,700 Anti-Xa IU). Patients from the treatment and
control groups received corticosteroids in the form of 16 mg
dexamethasone (Dexamethason; Krka) divided into 2 doses, daily.
Antiretrovirals used were lopinavir/ritonavir (Kaletra; Hetero
Labs, Ltd.), 300 mg b.i.d. and remdesivir (Veklury; Gilead
Sciences), 200 mg loading dose, then 100 mg o.d. for 5 days.
Antimalarial drugs were also used, in the form of
hydroxychloroquine (Plaquenil; Sanofi-Aventis), 400 mg b.i.d.
loading dose, then 200 mg b.i.d. Upon clinical (fever, chills,
sweats or aspect/quantity of bronchial secretions) and paraclinical
(leucocytosis, CRP or cultures) findings of infection, empiric
antibiotics were started, consisting of piperacilin/tazobactam
(Fresenius Kabi) 4.5 g q.i.d., until de-escalation following
culture results was possible. Patients were intensively monitored,
and daily clinical and laboratory data were collected during the
ICU stay. Outcomes monitored were survival at 30 days, oxygenation
(P/F ratio) (normal ratio >300) and inflammatory markers [CRP
(normal range 0-5 mg/l), LDH (normal range 135-225 U/l) and
ferritin (normal range 30-400 µg/l)] at the 7-day follow-up, as
assessed using ASTRUP analyses and blood tests.
Statistical analysis
Statistical data were analysed using GraphPad Prism
8 (GraphPad Software, Inc.) and IBM SPSS Statistics 20 (IBM Corp.).
The category variables are characterized by value and percentage.
Continuous variables are presented as mean (± standard deviation)
and median (interquartile range). Data distribution testing was
performed using the Shapiro-Wilk test. The numerical variables were
compared with the t-test for independent samples or the
Mann-Whitney U test, depending on the type of distribution of the
variables. The χ2 test (or Fisher's exact test) was used
for the nominal variables. The Kaplan-Meyer method with the
log-rank (Mantel-Cox) test was applied to evaluate the primary
endpoint. Cox regression was utilized to determine hazard ratio of
the treatment group. All statistical tests were calculated with 2
tails and P<0.05 was considered to indicate a statistically
significant difference.
Results
Baseline characteristics of patients
in the treatment and control groups
The present study cohort of 38 patients included 24
(63.16%) males and 14 (36.84%) females, with a median age of 63
years (range, 51-70 years). The patients were mainly overweight
[median body mass index (BMI), 26 kg/m2 (range,
24.15-32.83 kg/m2)] and 35 (92.11%) of them had
comorbidities (mostly arterial hypertension, type 2 diabetes
mellitus, chronic kidney disease and obesity). According to the
clinical and radiological correlations mentioned in the COVID-19
guidelines (6,9), 22 (57.89%) patients had a severe form
of the disease while 16 (42.11%) were considered critical.
Considering the proposal made by Siddiqi and Mehra (5) to divide patients according to the
evolution of the disease, patients from the present study were
classified as stage IIb (22 patients) and stage III (16 patients).
Time interval from symptom onset to treatment was a median of 8
days (range, 6.75-9.00 days) for the entire study group.
A total of 19 (50.00%) of the 38 patients enrolled
in the study received TPE and subsequent transfusion of CVP, in
addition to the standard treatment, while 19 patients (50.00%)
received only standard treatment. Baseline characteristics were
balanced between the treatment group and the control group. There
were no significant differences with regard to age, sex,
comorbidities, time from symptom onset to treatment, severity of
disease, APACHE II score (10) and
antiviral drug use between the groups, except for BMI, which was
higher in the treatment group (Table
I).
 | Table IBaseline characteristics of patients
in the treatment and control groups. |
Table I
Baseline characteristics of patients
in the treatment and control groups.
| Characteristic | Treatment group | Control group | P-value |
|---|
| Age | | | 0.271 |
|
Mean (± SD),
years | 58.74 (±7.76) | 62 (±12) | |
|
Median
(IQR) | 57(13) | 68(21) | |
| Sex, n (%) | | | 0.737 |
|
Male | 13 (68.42) | 11 (57.89) | |
|
Female | 6 (31.58) | 8 (42.11) | |
| BMI | | | 0.034 |
|
Mean (± SD),
kg/m² | 29.75 (±5.02) | 27.16 (±6.92) | |
|
Median
(IQR) | 29.20 (9.30) | 24.70 (4.80) | |
| Comorbidities, n
(%) | | | 0.547 |
|
Yes | 18 (94.74) | 17 (89.47) | |
|
No | 1 (5.26) | 2 (10.53) | |
| Symptoms onset to
treatment | | | 0.385 |
|
Mean (± SD),
days | 7.68 (±2.49) | 8.58 (±2.14) | |
|
Median
(IQR) | 8.00 (5.00) | 8.00 (2.00) | |
| Severity of the
disease, n (%) | | | 0.743 |
|
Severe | 12 (63.16) | 10 (52.63) | |
|
Critical | 7 (36.84) | 9 (47.37) | |
| APACHE II | | | 0.339 |
|
Mean (±
SD) | 5.74 (±3.16) | 7.58 (±6.48) | |
|
Median
(IQR) | 5.00 (3.00) | 6.00 (5.00) | |
| Antiviral drug, n
(%) | | | 0.406 |
|
Lopinavir/ritonavira
and HCQb | 6 (31.58) | 10 (52.63) | |
|
Lopinavir/ritonavira | 5 (26.32) | 4 (21.05) | |
|
Remdesivirc | 8 (42.11) | 5 (26.32) | |
Primary and secondary outcomes
Since all patients admitted to the ICU presented
with acute respiratory failure, they received 1 h of high-flow
nasal oxygen, 30 l/min (FiO2=100%), combined with a
non-rebreathing mask, 15 l/min, and then had a median P/F ratio of
61.50 (range, 54.00-71.25).
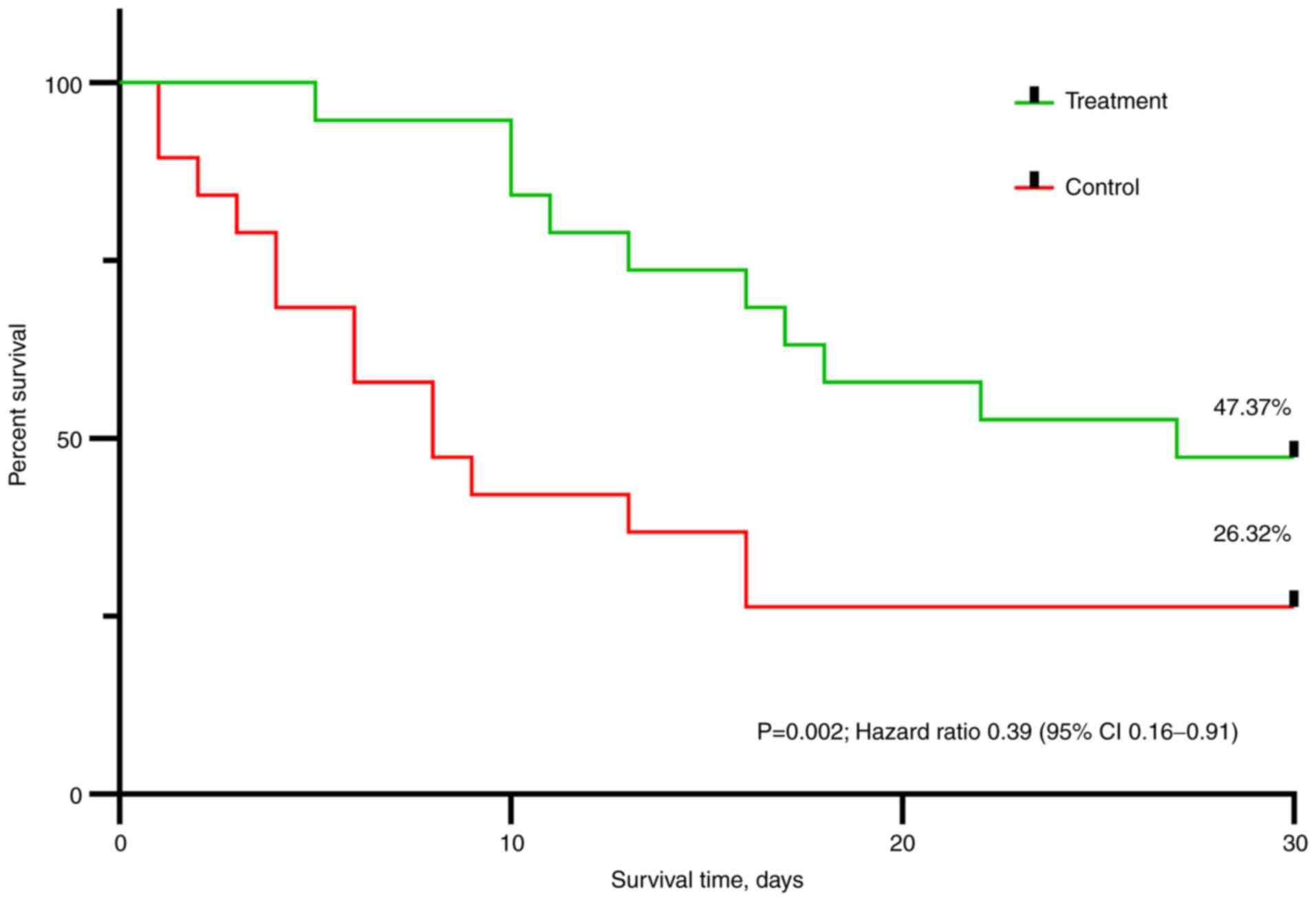
At day 30, 9 (47.37%) patients in the treatment
group and only 5 (26.32%) patients in the control group had
survived. The distribution of survival between the 2 groups was
statistically significant (log rank test: P=0.002) (Fig. 1). Using the Cox regression analysis
of outcome, the treatment showed a statistically significant
positive effect on survival (hazard ratio, 0.39; 95% confidence
interval, 0.16-0.91; P=0.007).
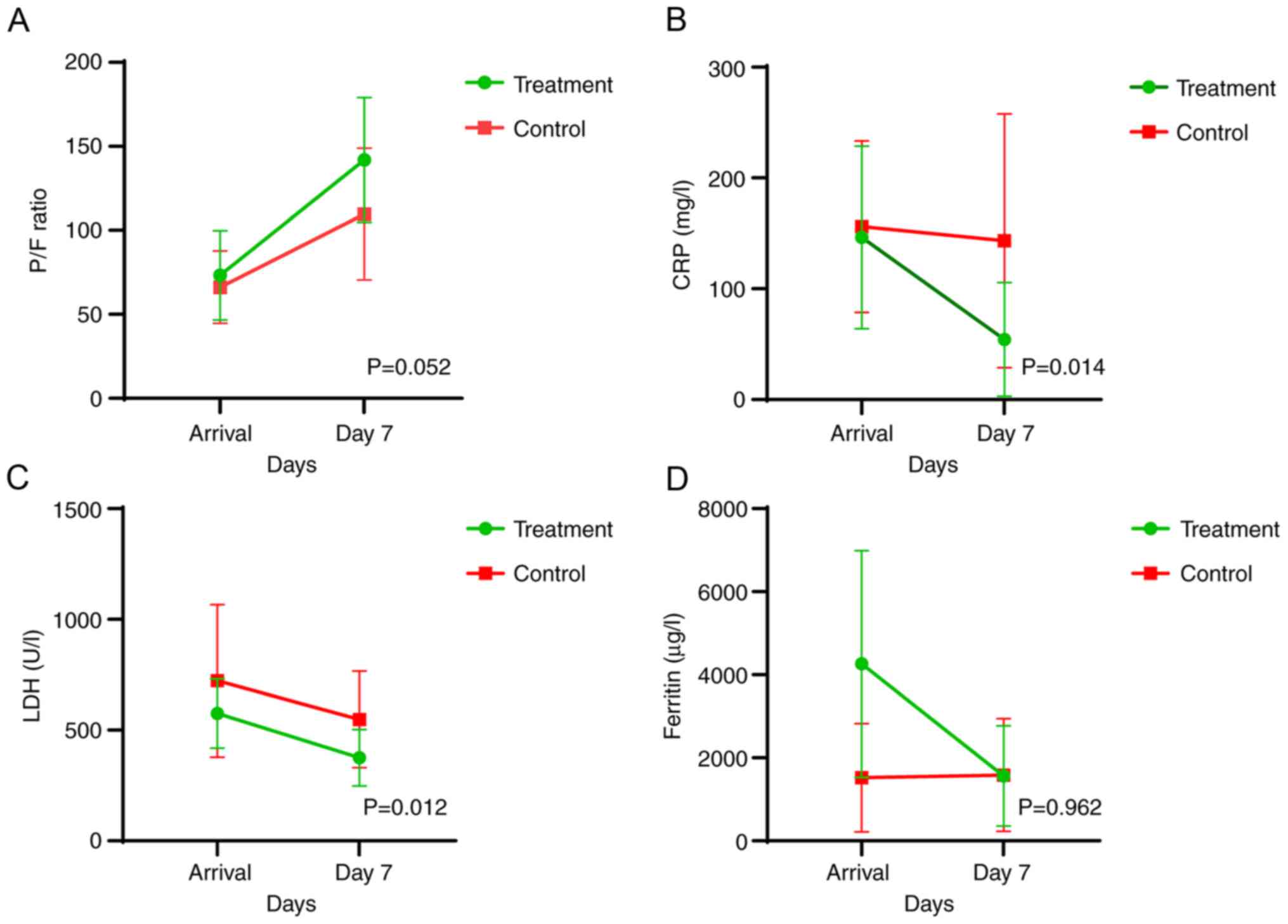
The variation in parameters representing the
secondary endpoints [oxygenation (P/F ratio), and CRP, LDH and
ferritin levels at day 7] between the two groups is presented in
Table II. The CRP and LDH values
exhibited a statistically significant decrease in the treatment
group compared with those in the control group, while the P/F ratio
increased markedly right on the verge of being statistically
significant (P=0.052). Although patients in the treatment group
presented with higher ferritin levels at admission, survival time
at 30 days was better than that in the control group, where
ferritin levels were constant throughout the 7-day monitoring
period. The variation in ferritin levels between the 2 groups was
not statistically significant (P=0.962). An overall improvement of
the assessed parameters in favour of the treatment group is also
illustrated in Fig. 2.
| Table IISecondary objectives assessed at day
7. |
Table II
Secondary objectives assessed at day
7.
| Objective | Treatment
groupa | Control
groupa | P-value |
|---|
| P/F ratio | 141.88±37.19 | 109.61±39.25 | 0.052 |
| CRP, mg/l | 46.17±60.89 | 144.00±115.3 | 0.014 |
| LDH, U/l | 375.11±127.41 | 548.41±218.03 | 0.012 |
| Ferritin, µg/l |
1,563.23±1,206.05 |
1,586.27±1,356.42 | 0.962 |
Complications of the treatment
Complications related to the studied treatment were
minimal, with 1 (5.26%) patient in the treatment group presenting
with transient hypotension (systolic blood pressure <90 mmHg)
after the transfusion of CVP, which responded to crystalloid bolus.
One of the ICU-related complications in the cohort was
superinfection. In total, 14 (73.68%) patients in the treatment
group and 10 (52.63%) patients in the control group acquired an
infection during their stay.
Particularities
Mean ICU length of stay (LOS) was 16.84 (±7.25) days
in the treatment group vs. 8.58 (±6.13) days in the control group
(P=0.001) (Table III). The reason
behind some of the unusual results when comparing the treatment
group and the control group, such as that for ICU LOS, invasive
mechanical ventilation duration and non-invasive ventilation
duration (Table III) was the fact
that 7 (36.84%) patients in the control group had died by day 7
(thus markedly decreasing ICU LOS, invasive mechanical ventilation
duration and non-invasive ventilation duration).
| Table IIIMechanical ventilation duration and
length of stay. |
Table III
Mechanical ventilation duration and
length of stay.
| Parameter | Treatment
group | Control group | P-value |
|---|
| ICU LOS, days | | | 0.001 |
|
Mean (±
SD) | 16.84 (±7.25) | 8.58 (±6.13) | |
|
Median
(IQR) | 17.00 (12.00) | 7.00 (8.00) | |
| IMV duration,
days | | | 0.172 |
|
Mean (±
SD) | 7.10 (±7.33) | 2.32 (±3.99) | |
|
Median
(IQR) | 5.00 (13.00) | 1.00 (16.00) | |
| NIV duration,
days | | | 0.665 |
|
Mean (±
SD) | 3.11 (±4.03) | 2.68 (±2.73) | |
|
Median
(IQR) | 1.00 (6.00) | 2.00 (2.00) | |
Discussion
Numerous studies regarding both CVP transfusion and
TPE in COVID-19 were available at the time of patient enrolment in
the present study, yet none were available that combined the two
methods (11-16).
After reviewing the available literature, Balagholi
et al (17) concluded that
immunopathogenesis and coagulopathy induced by SARS-CoV2 in
susceptible patients lead to cytokine storms and aberrant
coagulation responses, which can lead to high mortality due to the
occurrence of ARDS and multi-organ dysfunction. The main factor in
the success of TPE is starting the procedure in the early stage of
inflammation, in which there is a high concentration of
inflammatory cytokines, in order to reduce their burden and
abnormal coagulation agents. Khamis et al (14) demonstrated similar findings in a
case series in which the early use of TPE was associated with lower
28-day mortality rate, and improved laboratory and ventilator
parameters were observed in the TPE group when compared with those
in the control group. Another study also found superior survival
rates following the early use of TPE (18).
Liu et al (19) found that CVP recipients were more
likely to remain at the same level or show improvements in their
supplemental oxygen requirements by post-transfusion day 14
compared with control patients. Plasma recipients also showed
improved survival rate when compared with control patients. In a
large cohort of patients with COVID-19 who received CVP in Wuhan,
it was shown that CVP transfused even 2 weeks after the onset of
symptoms [compared with a median of 8 days (range, 6.75-9.00 days)
in the present cohort] could improve the symptoms and level of
mortality in patients with severe or critical cases of
COVID-19(20).
The improved outcomes concerning survival,
oxygenation and inflammation in the present treatment group are in
line with the results of these aforementioned studies. However, it
is difficult to decide whether the combined effect of these
therapies shows superiority over the single use of each one of
them.
The present study results are similar to those
obtained in the study by Jaiswal et al (21), which was the first study on the
sequential use of TPE and CVP transfusion in which inflammation was
decreased and oxygenation improved. After applying the TPE plus CVP
treatment to the present study group, 3 (15.79%) patients improved
without the need for escalation to non-invasive mechanical
ventilation and 4 (21.05%) were able to be weaned off non-invasive
mechanical ventilation. A total of 7 (36.84%) patients in the
treatment group were, thus, prevented from escalating to invasive
mechanical ventilation. A further 2 (10.53%) patients requiring
invasive mechanical ventilation were liberated from the machines,
and subsequently improved and were discharged. In total, 9 patients
(47.37%) in the treatment group had survived at the end of the
study period.
Certain issues have been raised about the use of
TPE; more specifically that the ‘artificial’ reduction of plasma
levels of inflammatory mediators via the use of TPE is not
necessarily consistent with the status improvement of the patient,
and that the removal of immunoglobulins and complement components
C3 and C4 has the potential of diluting or attenuating the adaptive
response of the patient to infection (22). Honore et al (23) discussed the possibility that the
exchange of plasma may also replace consumed protective factors
that are critical to maintain microcirculatory flow (e.g.,
ADAMTS-13 and protein C) and prevent vascular leaks (e.g.,
angiopoietin-1), and that specific IgG and IgA antibodies can be
detected in the waste bag plasma while the circulating number of
antibodies are reduced. Fresh frozen plasma as a replacement fluid
for TPE may help in modulating the circulating inflammatory
cytokines and hypercoagulable state by replacing the ADAMTS-13
enzyme (23).
In a recent study, Focosi et al (24) emphasised that neutralizing
antibodies correlate with the severity of disease. Also, SARS-COV-2
replication may still be driving the pathology in advanced stages
of the disease. In a screening for autoantibodies against 2,770
secreted proteins (the ‘exoproteome’), it was concluded that
patients with COVID-19 exhibit marked increases in autoantibody
reactivity compared with uninfected controls, with a high
prevalence of autoantibodies against immunomodulatory proteins,
including cytokines, chemokines, complement components and cell
surface proteins (25).
The key in controlling dysregulated inflammation in
severe forms of COVID-19 in patients requiring ICU monitoring and
therapy may be the early initiation of TPE and transfusion of CVP
in order to improve oxygenation, reduce inflammation, prevent
cytokine storms, and eliminate viral load and autoantibodies, which
increase in the later more severe stages of the infection (2,26), as
well as to shift the antigen-antibody ratio in favour of the latter
(27).
Median duration from symptom onset to TPE and CVP
transfusion in the present study was 8 days (range, 6.75-9.00
days). Antibody titre of the CVP transfused ranged from 1:80 to
1:160, values considered acceptable at the time the trial started,
if high titre units were not available (https://www.uptodate.com/contents/covid-19-convalescent-plasma-and-hyperimmune-globulin).
A major advantage of this study is that it was
controlled; it is also the first study performed on COVID-19
patients in Romania and the second in the world that evaluates TPE
followed by CVP transfusion, a unique approach (21), in severe and critically ill COVID-19
patients. All in all, it can be concluded that the early initiation
of TPE followed by transfusion of CVP in severe and critical ICU
patients reduces the risk of progression of the disease and
ultimately, reduces the risk of negative outcomes.
Limitations of the study include the small number of
patients enrolled, the non-randomized nature of the study and the
low neutralizing antibody titre ratio of the CVP (1:80-1:160). Last
but not least, the use of corticosteroids and different antiviral
agents may have interfered with the outcome.
The present study showed that the early use of TPE
followed by transfusion of CVP resulted in improved survival rates
and a reduction in inflammation in a small number of severe and
critical COVID-19 patients treated in the ICU. More research
consisting of large randomized controlled trials should be
conducted to further explore this innovative treatment.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analysed in the current
study are available from the corresponding author on request.
Authors' contributions
ANN and ML had a major role in the conception,
investigation and design of the current study. The acquisition of
data was performed by ANN, GD, BB, OB, MP, DS and DV. LMB, ANN and
TS analysed and interpreted the data. Resources were provided by
LMB, DV, GD, BB. ANN, GD, BB, OB, MP and DV wrote the original
draft, while DS, TS, ML and LMB critically revised the content for
important intellectual content. DS validated the results of the
study. ML managed the project and coordinated responsibility for
the research planning and execution, and supervised the research
activity. AAN, ML and DS confirm the authenticity of all the raw
data. All authors have read and approved the final version for
publication.
Ethics approval and consent to
participate
The trial was approved by the Ethics Committee of
‘Pius Brinzeu’ Emergency Clinical County Hospital Timisoara
(91/03.08.2020). Written informed consent was obtained from each
patient or their legal representative.
Patient consent for publication
The patients consented to the publication of their
data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Calina D, Docea AO, Petrakis D, Egorov AM,
Ishmukhametov AA, Gabibov AG, Shtilman MI, Kostoff R, Carvalho F,
Vinceti M, et al: Towards effective COVID-19 vaccines: Updates,
perspectives and challenges (Review). Int J Mol Med. 46:3–16.
2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Wiersinga WJ, Rhodes A, Cheng AC, Peacock
SJ and Prescott HC: Pathophysiology, transmission, diagnosis, and
treatment of coronavirus disease 2019 (COVID-19): A review. JAMA.
324:782–793. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Xu Z, Shi L, Wang Y, Zhang J, Huang L,
Zhang C, Liu S, Zhao P, Liu H, Zhu L, et al: Pathological findings
of COVID-19 associated with acute respiratory distress syndrome.
Lancet Respir Med. 8:420–422. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Docea AO, Tsatsakis A, Albulescu D,
Cristea O, Zlatian O, Vinceti M, Moschos SA, Tsoukalas D, Goumenou
M, Drakoulis N, et al: A new threat from an old enemy: Re-emergence
of coronavirus (Review). Int J Mol Med. 45:1631–1643.
2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Siddiqi HK and Mehra MR: COVID-19 illness
in native and immunosuppressed states: A clinical-therapeutic
staging proposal. J Hear Lung Transplant. 39:405–407.
2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lin L and Li TS: Interpretation of
‘guidelines for the diagnosis and treatment of novel coronavirus
(2019-nCoV) infection by the national health commission (trial
version 5)’. Zhonghua Yi Xue Za Zhi. 100:805–807. 2020.PubMed/NCBI View Article : Google Scholar : (In Chinese),
(Online ahead of print).
|
|
7
|
COVID-19 Treatment Guidelines Panel:
Coronavirus disease 2019 (COVID-19) treatment guidelines. National
Institutes of Health. Available at: https://www.covid19treatmentguidelines.nih.gov/.
Accessed June 15, 2021.
|
|
8
|
ARDS Definition Task Force. Ranieri VM,
Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E,
Camporota L and Slutsky AS: Acute respiratory distress syndrome:
The Berlin definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Martínez Chamorro E, Díez Tascón A, Ibáñez
Sanz L, Ossaba Vélez S and Borruel Nacenta S: Radiologic diagnosis
of patients with COVID-19. Radiologia (Engl Ed). 63:56–73.
2021.PubMed/NCBI View Article : Google Scholar : (In English,
Spanish).
|
|
10
|
Knaus WA, Draper EA, Wagner DP and
Zimmerman JE: Apache II. A severity of disease classification
system. Crit Care Med. 13:818–829. 1985.PubMed/NCBI
|
|
11
|
Franchini M and Liumbruno GM: Convalescent
plasma for the treatment of severe COVID-19. Biologics. 15:31–38.
2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Li L, Zhang W, Hu Y, Tong X, Zheng S, Yang
J, Kong Y, Ren L, Wei Q, Mei H, et al: Effect of convalescent
plasma therapy on time to clinical improvement in patients with
severe and life-threatening COVID-19: A randomized clinical trial.
JAMA. 324:460–470. 2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Keith P, Day M, Perkins L, Moyer L, Hewitt
K and Wells A: A novel treatment approach to the novel coronavirus:
An argument for the use of therapeutic plasma exchange for
fulminant COVID-19. Crit Care. 24(128)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Khamis F, Al-Zakwani I, Al Hashmi S, Al
Dowaiki S, Al Bahrani M, Pandak N, Al Khalili H and Memish Z:
Therapeutic plasma exchange in adults with severe COVID-19
infection. Int J Infect Dis. 99:214–218. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Gucyetmez B, Atalan HK, Sertdemir I, Cakir
U and Telci L: COVID-19 Study Group. Therapeutic plasma exchange in
patients with COVID-19 pneumonia in intensive care unit: A
retrospective study. Crit Care. 24(492)2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Sarfraz A, Makkar SS, Sarfraz Z, Hathaway
III D, Paul T, Sana MK, Talalaev M, Perez-Fernandez J and Yatzkan
G: Therapeutic plasma exchange and COVID-19: A rapid review. J Clin
Immunol Immunother. 6(041)2020.
|
|
17
|
Balagholi S, Dabbaghi R, Eshghi P, Mousavi
SA, Heshmati F and Mohammadi S: Potential of therapeutic
plasmapheresis in treatment of COVID-19 patients:
Immunopathogenesis and coagulopathy. Transfus Apher Sci.
59(102993)2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kamran SM, Mirza ZE, Naseem A, Liaqat J,
Fazal I, Alamgir W, Saeed F, Saleem S, Nisar S, Yousaf MA, et al:
Therapeutic plasma exchange for coronavirus disease-2019 triggered
cytokine release syndrome; a retrospective propensity matched
control study. PLoS One. 16(e0244853)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Liu STH, Lin HM, Baine I, Wajnberg A,
Gumprecht JP, Rahman F, Rodriguez D, Tandon P, Bassily-Marcus A,
Bander J, et al: Convalescent plasma treatment of severe COVID-19:
A matched control study. Nat Med. 26:1708–1713. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Xia X, Li K, Wu L, Wang Z, Zhu M, Huang B,
Li J, Wang Z, Wu W, Wu M, et al: Improved clinical symptoms and
mortality among patients with severe or critical COVID-19 after
convalescent plasma transfusion. Blood. 136:755–759.
2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jaiswal V, Nasa P, Raouf M, Gupta M,
Dewedar H, Mohammad H, Al Rais Z, Ali Baqer M, Alsabbah A, Ibrahim
Y, et al: Therapeutic plasma exchange followed by convalescent
plasma transfusion in critical COVID-19-an exploratory study. Int J
Infect Dis. 102:332–334. 2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Stahl K, Bode C and David S: First do no
harm-beware the risk of therapeutic plasma exchange in severe
COVID-19. Crit Care. 24(363)2020.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Honore PM, Barreto Gutierrez L, Kugener L,
Redant S, Attou R, Gallerani A and De Bels D: Plasma exchange in
critically ill COVID-19 patients improved inflammation,
microcirculatory clot formation, and hypotension, thereby improving
clinical outcomes: Fact or fiction? Crit Care.
24(551)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Focosi D, Maggi F, Franchini M, Aguzzi A,
Lanza M, Mazzoni A and Menichetti F: Patient-blood management for
COVID19 convalescent plasma therapy: Relevance of affinity and
donor-recipient differences in concentration of neutralizing
antibodies. Clin Microbiol Infect. 27:987–992. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Wang EY, Mao T, Klein J, Dai Y, Huck JD,
Jaycox JR, Liu F, Zhou T, Israelow B, Wong P, et al: Diverse
functional autoantibodies in patients with COVID-19. Nature.
595:283–288. 2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Fajnzylber J, Regan J, Coxen K, Corry H,
Wong C, Rosenthal A, Worrall D, Giguel F, Piechocka-Trocha A, Atyeo
C, et al: SARS-CoV-2 viral load is associated with increased
disease severity and mortality. Nat Commun. 11(5493)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Vuitton DA, Vuitton L, Seillès E and
Galanaud P: A plea for the pathogenic role of immune complexes in
severe Covid-19. Clin Immunol. 217(108493)2020.PubMed/NCBI View Article : Google Scholar
|