Introduction
Combined esophageal atresia/tracheoesophageal
fistula (EA/TEF) and duodenal obstruction is very rare, and is
accompanied with high morbidity and mortality rates (1-3).
The combined anomalies always pose challenges for disease
management. At present, management protocols for these combined
anomalies have not yet been clearly defined, and it remains a
controversial issue whether the anomalies occur together or are
staged (3-6).
Esophageal anastomotic stricture is a frequent complication
following EA repair (7). In some
cases, stricture may be recalcitrant in spite of dilatation
procedures (8). For these patients,
a variety of treatment methods have been tried and employed,
including steroids (9), mitomycin C
(10), bougie and balloon
dilatation, and esophageal stenting (11,12),
with varying efficiencies and success rates. However, these
conventional treatment options are not useful in treating recurring
hypertrophic scar tissue, and some of these patients require
repeated thoracotomy with segmental esophageal resection and
reanastomosis or esophageal replacement (13-14).
Therefore, there is an urgent need for a treatment option for
esophageal stricture in children that can effectively remove the
hyperplastic scar tissues formed in the esophagus without causing
trauma. In the last decade, magnetic compression anastomosis has
been used to treat anastomotic stenosis following
esophagoesophagostomy for EA (15-17).
The present case report describes our first
experience with simultaneous repair of a combination of
gastrointestinal anomalies and magnetic compression stricturoplasty
treating refractory stricture after EA repair in two male neonates.
The clinical experience and data concerning the diagnosis and
treatment of complex multiple digestive tract obstructions in
infants with combined EA/TEF and severe duodenal obstruction were
recorded and analyzed. Moreover, important properties of magnetic
compression stricturoplasty while treating refractory stricture
following EA repair are discussed.
Case report
Patient 1
The first case was a 2 years and 2 months old male
infant, who was born at 38 weeks of gestation via cesarean section
due to a uterine scar and premature rupture of the membranes, with
the umbilical cord wrapping around the neck by 360˚. An excessive
amount of amniotic fluid was noted on a prenatal ultrasound. His
Apgar score (14) were 10 at 1 min,
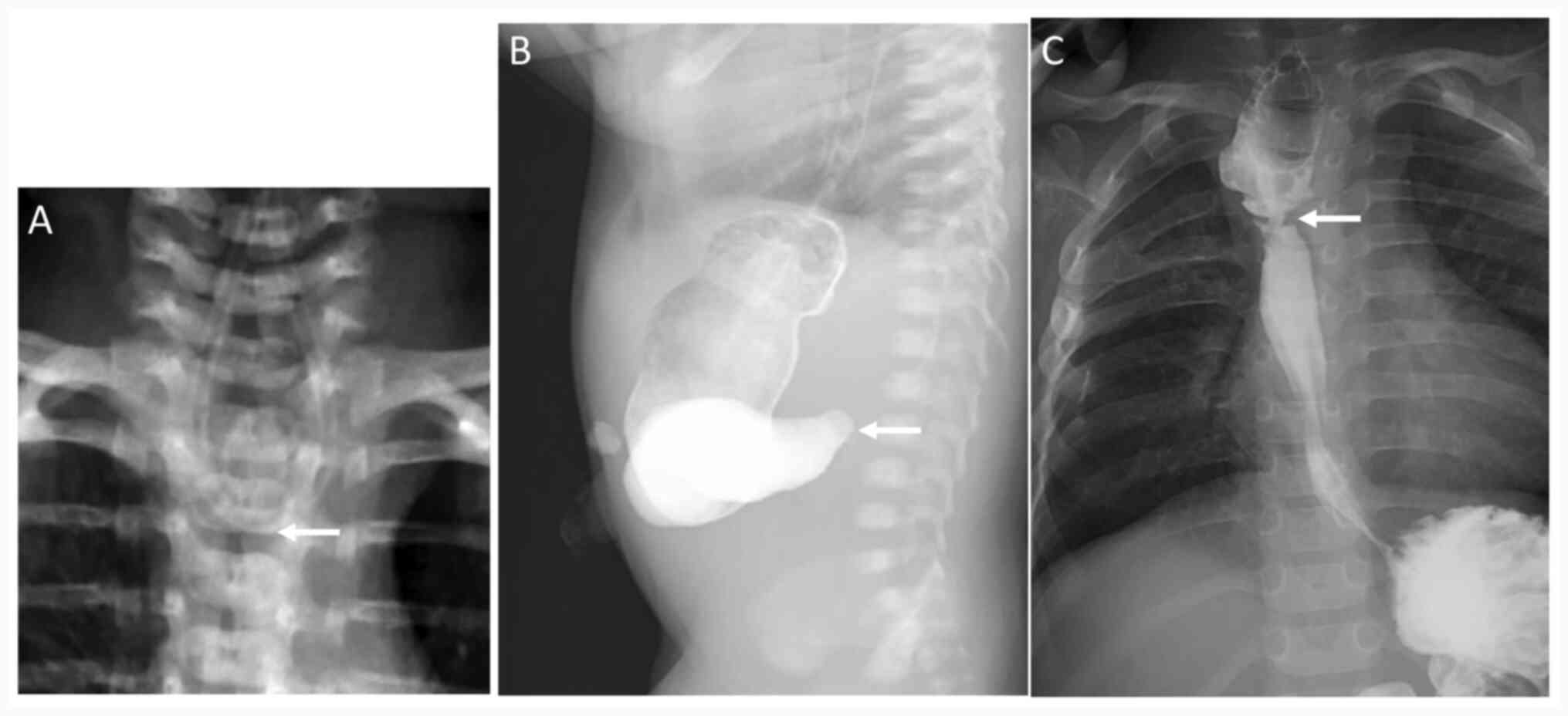
10 at 5 min, and 10 at 10 min. Chest X-rays showed that the
nasogastric tube (NGT) was located in the upper esophagus,
suggesting EA (Fig. 1A). On the
subsequent day after birth, the patient underwent the first urgent
surgery, comprising right posterolateral thoracotomy and
extrapleural separation for EA with proximal TEF (Gross type C) and
malformation repair. On day 16 after the first operation, repeated
upper gastrography verified patency of the esophageal anastomosis
and a delayed diagnosis of duodenal obstruction (Fig. 1B). The patient therefore underwent
an emergency exploratory laparotomy and duodenoduodenostomy for the
duodenal obstruction repair. On day 4 after the second operation,
enteral feeding was started after a swallow test. The infant was
able to take full volume oral feeding by day 12, indicating the
absence of esophageal or duodenal leakage. The infant was in good
health at the 14-month follow-up. Over the next 12 months, the
narrowing progressed to a refractory stricture in spite of multiple
endoscopic dilatation procedures. On the 4th attempt at wire-guided
balloon dilatation, it was observed that the stricture had
essentially caused a severe (nearly complete) esophageal
obstruction (<3 mm; Fig. 1C). As
a result, the patient was a candidate for stent placement or
segmental resection/anastomosis. A detailed discussion on stent
placement or thoracotomy with attempted segmental resection and
anastomosis was conducted with the parents of the patient, who
refused the procedure due to the risk of complications such as
restenosis. Ultimately, according to medical opinion, the patient
received an endoscopy-guided magnetic esophageal compression
stricturoplasty.
Patient 2
The second case was another 1 years and 11 months
old male infant who was born at 39 weeks of gestation through
vaginal delivery, weighing 2,540 g. The Apgar scores were 8, 9 and
9 at 1, 5 and 10 min after birth, respectively. The prenatal
ultrasound showed polyhydramnios. Spontaneous breathing was good
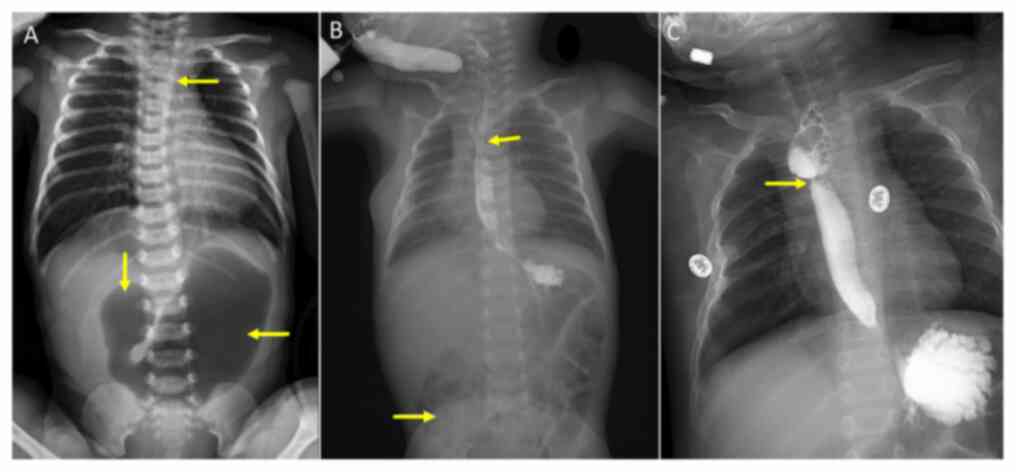
and vital signs were normal, without hypoxia. An NGT could not be
successfully advanced. A combined chest and abdominal X-ray film
showed that the NGT was located in the upper esophageal pouch
(Fig. 2A). Moreover, vertebral
abnormalities, mediastinal shift and a large gastric bubble without
any distal bowel gas were noted. These findings suggested that the
infant exhibited EA/TEF complicated with duodenal obstruction and
hypoplasia of the right lung. Emergency surgery was performed on
the day after birth, confirming the duodenal obstruction due to an
annular pancreas (AP). The intra-operative pathological anatomy
showed EA with proximal TEF (Gross type C). An extrapleural
operation for repair of EA/TEF, and laparotomy and
duodenoduodenostomy for repair of AP (EA repair followed by AP
repair) were synchronously performed in 2.5 h without gastrostomy.
On day 9, enteral feeding was started, and the infant was able to
receive full volume oral feeding by day 14. The NGT was removed on
day 8, and oral feeding was initiated on day 9 after the swallow
test, which indicated no esophageal or duodenal leakage. Repeated
upper gastrointestinal imaging confirmed good patency of the
esophageal and duodenal anastomosis (Fig. 2B).
The patient was in good health at the 10-month
follow-up. An angiogram revealed only mild narrowing at the site of
the anastomosis. During the next 15 months, the narrowing
progressed into a recalcitrant stricture in spite of multiple
endoscopic dilatation procedures. Due to near-complete esophageal
obstruction (<2 mm; Fig. 2C),
the parents of the patient refused stent placement. Therefore, the
patient was a candidate for segmental resection/anastomosis. A
detailed discussion on thoracotomy with attempted segmental
resection and anastomosis was conducted with the parents; however,
they refused the procedures due to the risk of restenosis.
Ultimately, following medical evaluation, the patient received an
endoscopy-guided magnetic esophageal compression
stricturoplasty.
Ethical approval
The two infants received treatment at the Department
of Pediatric Surgery of The Northwest Women's and Children's
Hospital (Xi'an, China). All clinical application protocols for the
techniques performed were approved by the Ethics Committee of The
Northwest Women's and Children's Hospital, and were in accordance
with the relevant guidelines and regulations. Written informed
consent was obtained from the parents of each infant with regard to
use of the novel technique. Retrospective Institutional Review
Board approval of The Northwest Women's and Children's Hospital was
obtained for the purposes of publication.
Treatment of the refractory stricture
Deployment of magnetic ring device
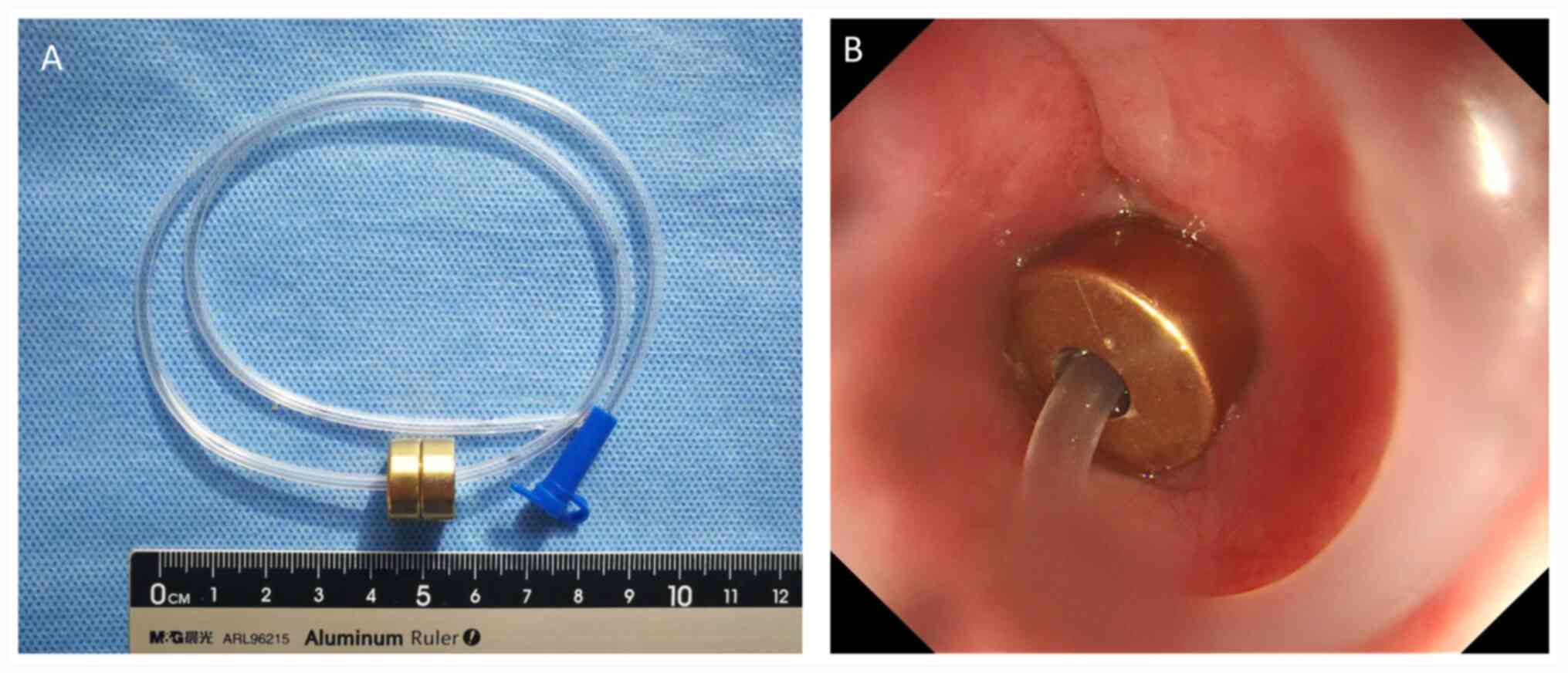
Magnetic rings prepared from a neodymium-iron-boron
(Nd-Fe-B) alloy were obtained from the Northwest Institute for
Nonferrous Metal Research and airbrush coated with titanium oxide
(5-6-µm thick; Fig. 3A). The rings
were developed such that they had an outer diameter of 10 mm and a
height of 5 mm, with strength of 0.25 T force, and they were placed
with suction power between the esophageal compression
stricturoplasty.
Endoscopy-guided magnetic esophageal
compression stricturoplasty
Sterilized magnets were placed through the transoral
approach and via gastrostomy under fluoroscopic and endoscopic
guidance (16,17). One magnet ring (mother ring) with an
8F gastric tube was placed in the proximal esophagus using a
transoral approach, which reached the stomach cavity through the
stenotic segment under endoscopic guidance (Fig. 3B). Subsequently, the gastric tube
was placed through the central hole of the daughter ring by
gastrostomy. Next, the daughter ring was fixed onto the tube, which
was positioned in the stenotic distal esophageal lumen. Magnets
were kept in place for 18 days to allow for gradual compression
stricturoplasty/anastomosis. Then, under the effect of the magnetic
force, the two magnet rings were pulled along the gastric tube to
ensure the adequacy of esophageal stricturoplasty. The patient was
fed via a gastric tube after the operation.
Outcomes
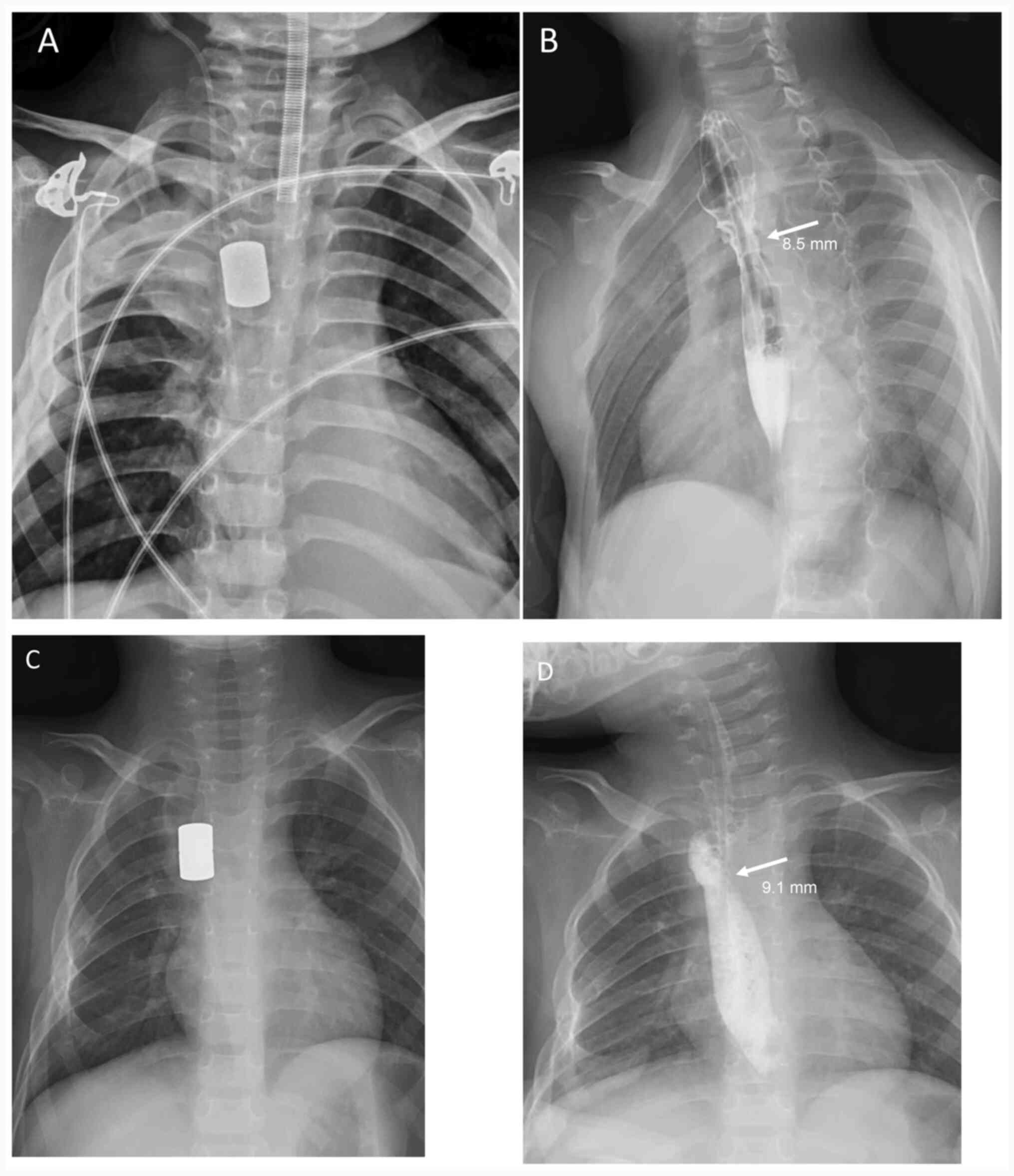
The placement of magnets was successful in both
patients. After the operation, the infants were kept and observed
in the Pediatric Intensive Care Unit until the magnets were
removed. The magnets achieved full approximation in these two
cases, as visualized by a chest radiograph on day 1 (Fig. 4A and C). Attempts were made to move the magnets
by gently pulling the tube fixed to the magnets. This process was
attempted daily, starting within 1 week post-operation. When the
pair of rings could slide up and down, the patients were
transferred to the Department of Radiology to confirm the direct
apposition of the magnets, and then the magnets were removed under
fluoroscopic guidance (Fig. 4B and
D). On removal, an upper
gastroenterography demonstrated a substantially increased luminal
diameter. Furthermore, 8.5- and 9.1-mm anastomotic stomas were
formed without esophageal perforation in patients 1 and 2,
respectively, with no other early complications. There was no
requirement for balloon dilatation and temporary stent placement
after magnetic compression stricturoplasty. At 10 and 15 months
after magnetic compression stricturoplasty, no further signs of
esophageal stricture were observed. Routine examination showed very
good growth and development without any further symptoms of
dysphagia or reflux. The follow-up esophagram showed no evidence of
residual stricture.
Discussion
Duodenal obstruction is associated with EA/TEF, with
a prevalence of ~6% (18). This
combined abnormality is associated with high morbidity and
mortality rates (1,19). Varying treatment protocols for
combined EA/TEF and duodenal obstruction have been reported in the
published literature (18,20,21),
with high overall prevalence of gastrointestinal morbidity. This
may have been due to the concurrent and synergistic effects of
various functional and anatomical upper gastrointestinal defects
characterizing the two malformations (22).
Due to the rarity of combined EA/TEF and duodenal
obstruction, there is a lack of consensus concerning the optimal
treatment strategy for these combined abnormalities. Based on the
first case reported in the present study, an early combined chest
and abdominal X-ray investigation is helpful in avoiding a missed
diagnosis of duodenal obstruction in patients with EA/TEF.
In cases similar to the second case reported in the
present study, initial thoracotomy with ligation of the fistula and
esophageal repair via extrapleural separation should be performed.
This may prevent the risk of aspiration and permit the continuation
of the laparotomy under stable ventilatory status.
Based on the cases reported in the present study, we
propose that in an infant with stable vital signs, a primary
simultaneous EA and duodenal obstruction repair should be attempted
(4). Surgical treatment of EA/TEF
is still maturing, and thoracoscopic ligation has been increasingly
performed over the past years (20). The greatest efforts have been made
to perform operative treatments of several malformations with the
combination of thoracoscope and laparoscope.
A recalcitrant esophageal anastomotic stricture
following EA repair in infants presents a surgical challenge, and
supportive therapies in combination with balloon or bougie
dilatation have been used. However, in a few cases, severe
anastomotic stricture may be recalcitrant in spite of several
dilatation procedures. The techniques used to treat recalcitrant
stricture include intralesional steroid injection and local
application of mitomycin C over the stricture site to prevent
stricture reformation after dilatation via inhibition of fibroblast
proliferation and collagen synthesis (23-25).
Additionally, there are reports of using self-expanding stents to
prevent stricture recurrence after sufficient dilatation and
esophageal stenting (11,12,26).
Unfortunately, these traditional methods are not able to
effectively remove scar tissues. If bougie or balloon dilatation
and these supportive treatments fail, therapeutic options are
limited to operative resection of the strictured segment along with
reanastomosis or esophageal replacement (13). In past decades, it has been reported
that magnetic compression anastomosis (MCA) can be used for benign
biliary strictures (27-29),
magnetic connectors for coronary surgery (30), functional undiversion of ileostomy
(31) and rectal anastomosis
(28) in pediatric patients. In
pediatric surgery, Russell et al (32) determined the effectiveness of MCA in
animal models. Zaritzky et al (33) first proposed the application of
magnets in treating patients with long-gap EA. Takamizawa et
al (16) reported the
application of magnetic compression revision anastomosis in a
31-month-old child who had an anastomotic stenosis following
esophagoesophagostomy for long-gap EA without any fistula. Zaritzky
et al (15,33) reported successful application of MCA
in infants who had EA without airway fistula and a gap no broader
than 3 cm. Anastomotic stenosis developed in 8 out of 14 patients;
among them, two cases needed stent placement and one case needed
surgical reanastomosis. Additionally, 5 out of 14 infants received
surgical correction of EA, but developed severe recurrent
postoperative esophageal stenosis, with no response to dilatation.
The patients subsequently underwent MCA, and esophageal
reanastomosis was attained within a mean duration of 6 days. In the
present study, Nd-Fe-B alloy magnetic rings were prepared with
airbrush coating using titanium oxide to enhance their ability to
resist gastric acid corrosion, in contrast with previous reports
(15,16,33).
In the two cases reported in the present study,
discussions were conducted with the parents of each patient
regarding alternative treatment options over a time period of weeks
before trying the magnetic compression stricturoplasty. These
infants had failed standard treatment with endoscopic balloon
dilatation, while their parents refused alternative treatments,
such as topical injection, stent placement or thoracotomy combined
with attempted segmental resection and anastomosis, due to the risk
of restenosis. It was hypothesized that, for these two patients,
the potential risks associated with surgery were highest for
magnetic compression stricturoplasty, in comparison with the other
surgical alternatives, which would be less invasive than segmental
resection or esophageal replacement. In comparison with the other
studies, these two patients did not undergo immediate expansion
after magnetic anastomosis. Additionally, it was considered that
attempting a magnetic compression stricturoplasty would not
preclude future attempts at performing segmental resection or
esophageal replacement.
A combination of radio-opaque markers, wires,
endoscopy and fluoroscopy were used to achieve the correct
orientation of the magnets in the present study. Due to the
‘on/off’ behavior of magnets through a gap, the surgeon needed to
take meticulous care in maintaining the magnet polarity and
orientation. Another important property of magnetism is related to
the association between attractive force and magnet separation.
Importantly, the attractive force between two magnets rises
exponentially with reduced separation distance. Considering this
property of magnetism, magnetic compression would be well suited
for patients who have strictures due to the intrinsic resistance
induced by scar tissue. Therefore, it is hypothesized that the
interposed resistance caused by scar tissue may delay magnetic
coupling, which would lead to a slower/longer process, allowing for
stretching of the healthy esophageal segments. In clinical
practice, it was observed that magnetic coupling occurred faster
than expected. The patients did not develop any leakage and
perforation, most probably due to the protection provided by the
adjoining scar tissue due to previous surgery.
Esophageal continuity was attained after magnetic
compression stricturoplasty for recalcitrant esophageal anastomotic
stricture after EA with AP repair. No short-term complications were
noted. These findings suggested that this technique is feasible for
selected patients. However, there are some limitations of the
present study. Firstly, the case number was limited, and additional
clinical cases and experience are required to ascertain the
necessity and optimal duration of magnetic compression
stricturoplasty. Moreover, following the magnetic compression
stricturoplasty, the two patients attained esophageal continuity.
However, restenosis was a continuing problem, and the patients
needed several interventions, including balloon dilatation and
temporary stent placement. At 10 and 15 months during the follow-up
period, the patients showed durable esophageal patency without
dysphagia upon esophagram and clinical examination.
The present case report shows that the early
combination of chest and abdominal X-ray investigations can be
helpful for treating EA, and may avoid delayed diagnosis of DA. A
synchronous operation for repairing EA/TEF and performing
duodenoduodenostomy in a single surgery without gastrostomy is
recommended for treating the combination of EA/TEF and duodenal
obstruction. Magnetic compression stricturoplasty successfully
established the patency of the esophagus in these two patients with
refractory EA stricture. These two cases required multiple
additional procedures, but durable esophageal patency with absence
of dysphagia was achieved at 15 or 10 months after magnetic
compression stricturoplasty. Further in-depth investigation and
follow-up will determine the long-term success of this method. In
addition, knowledge of primary magnetic principles will allow for
the future customization of magnet arrays for the presentation of
individual patients.
Acknowledgements
The authors would like to thank Dr Rui Yan
(Department of Radiology, Northwest Women's and Children's
Hospital, Xi'an, China) for performing the imaging examination.
Funding
Funding: This study was supported by a grant from the Natural
Science Foundation of Shaanxi Provincial Key Industries Innovation
Chain (Cluster)-Social Development Project (grant no.
2020ZDLSF02-03) and the Special Fund for High-level talents of
Xijing University (grant no. XJ20B04).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
SL conducted the operation, collected data,
performed data analysis and interpretation, and drafted the
manuscript. YL and JZ designed operation procedures and revised the
manuscript. RXL assisted in magnetic ring processing. YF and HY
contributed to the endoscopic procedures. RGL and AZ provided
assistance in the operation and analyzed and interpreted the
patient data regarding the hematological disease. JC and YS
contributed to the analysis of the test data in the Intensive Care
Unit. NJ contributed to the acquisition and analysis of data
regarding the localization of magnets in the esophagus during the
anesthetic management of the patient. YL, JZ and SL confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
All clinical application protocols for the
techniques performed were approved by the Ethics Committee of the
Northwest Women's and Children's Hospital, and were in accordance
with the relevant guidelines and regulations. Written informed
consent was obtained from the parents of each infant with regard to
use of the novel technique.
Patient consent for publication
Patient consent forms were obtained from the
parents/guardians of the patients, giving their consent for the
images and other clinical information to be reported in the
journal. The parents/guardians understand that the names and
initials of the patients will not be published and due efforts will
be made to conceal their identities.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Spitz L, Ali M and Brereton RJ: Combined
esophageal and duodenal atresia: Experience of 18 patients. J
Pediatr Surg. 16:4–7. 1981.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Andrassy RJ and Mahour GH:
Gastrointestinal anomalies associated with esophageal atresia or
tracheoesophageal fistula. Arch Surg. 114:1125–1128.
1979.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ein SH, Palder SB and Filler RM: Babies
with esophageal and duodenal atresia: A 30-year review of a
multifaceted problem. J Pediatr Surg. 41:530–532. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Cao ZP, Li QF, Liu SQ, Niu JH, Zhao JR,
Chen YJ, Wang DY and Li XS: Surgical management of newborns with
combined tracheoesophageal fistula, esophageal atresia, and
duodenal obstruction. Chin Med J (Engl). 132:726–730.
2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Dave S and Shi EC: The management of
combined oesophageal and duodenal atresia. Pediatr Surg Int.
20:689–691. 2004.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nabzdyk CS, Chiu B, Jackson CC and Chwals
WJ: Management of patients with combined tracheoesophageal fistula,
esophageal atresia, and duodenal atresia. Int J Surg Case Rep.
5:1288–1291. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Catalano P, Di Pace MR, Caruso AM, Salerno
S, Cimador M and De Grazia E: A simple technique of oblique
anastomosis can prevent stricture formation in primary repair of
esophageal atresia. J Pediatr Surg. 47:1767–1771. 2012.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Alberca de Las Parras F, Navalón Rubio M
and Egea Valenzuela J: Management of refractory esophageal stenosis
in the pediatric age. Rev Esp Enferm Dig. 108:627–636.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hishiki T, Kouchi K, Saito T, Terui K,
Sato Y, Mitsunaga T, Nakata M and Yoshida H: Successful treatment
of severe refractory anastomotic stricture in an infant after
esophageal atresia repair by endoscopic balloon dilation combined
with systemic administration of dexamethasone. Pediatr Surg Int.
25:531–533. 2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Heran MKS, Pham TH, Butterworth S and
Robinson A: Use of a microporous polytetrafluoroethylene catheter
balloon to treat refractory esophageal stricture: A novel technique
for delivery of mitomycin C. J Pediatr Surg. 46:776–779.
2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Foschia F, De Angelis P, Torroni F, Romeo
E, Caldaro T, di Abriola GF, Pane A, Fiorenza MS, De Peppo F and
Dall'Oglio L: Custom dynamic stent for esophageal strictures in
children. J Pediatr Surg. 46:848–853. 2011.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Rollins MD and Barnhart DC: Treatment of
persistent esophageal leaks in children with removable, covered
stents. J Pediatr Surg. 47:1843–1847. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Garritano S, Irino T, Scandavini CM,
Tsekrekos A, Lundell L and Rouvelas I: Long-term functional
outcomes after replacement of the esophagus in pediatric patients:
A systematic literature review. J Pediatr Surg. 52:1398–1408.
2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Milickovic M, Savic D, Grujic B, Vlahovic
A, Vukadin M, Stajevic M and Kojovic V: Gastric tube esophageal
reconstruction in children with esophageal atresia and caustic
stricture study of clinical value based on 25 single-center. Centre
experience. Ann Ital Chir. 87:589–594. 2016.PubMed/NCBI
|
|
15
|
Zaritzky M, Ben R and Johnston K: Magnetic
gastrointestinal anastomosis in pediatric patients. J Pediatr Surg.
49:1131–1137. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Takamizawa S, Yamanouchi E, Muraji T,
Nishijima E, Satoh S and Tsugawa J: MCRA of an anastomotic stenosis
after esophagoesophagostomy for long gap esophageal atresia: A case
report. J Pediatr Surg. 42:769–772. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Woo R, Wong CM, Trimble Z, Puapong D,
Koehler S, Miller S and Johnson S: Magnetic compression
stricturoplasty for treatment of refractory esophageal strictures
in children: Technique and lessons learned. Surg Innov. 24:432–439.
2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Stark Z, Patel N, Clarnette T and Moody A:
Triad of tracheoesophageal fistula-esophageal atresia, pulmonary
hypoplasia, and duodenal atresia. J Pediatr Surg. 42:1146–1148.
2007.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Saing H, Mya GH and Cheng W: The
involvement of two or more systems and the severity of associated
anomalies significantly influence mortality in esophageal atresia.
J Pediatr Surg. 33:1596–1598. 1998.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Holder TM, Ashcraft KW, Sharp RJ and
Amoury RA: Care of infants with esophageal atresia,
tracheoesophageal fistula, and associated anomalies. J Thorac
Cardiovasc Surg. 94:828–835. 1987.PubMed/NCBI
|
|
21
|
Mollitt DL and Golladay ES: Management of
the newborn with gastrointestinal anomalies and tracheoesophageal
fistula. Am J Surg. 146:792–795. 1983.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Fragoso AC, Ortiz R, Hernandez F, Olivares
P, Martinez L and Tovar JA: Defective upper gastrointestinal
function after repair of combined esophageal and duodenal atresia.
J Pediatr Surg. 50:531–534. 2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Antoniou D, Soutis M and
Christopoulos-Geroulanos G: Anastomotic strictures following
esophageal atresia repair: A 20-year experience with endoscopic
balloon dilatation. J Pediatr Gastroenterol Nutr. 51:464–467.
2010.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Alshammari J, Quesnel S, Pierrot S and
Couloigner V: Endoscopic balloon dilatation of esophageal
strictures in children. Int J Pediatr Otorhinolaryngol.
75:1376–1379. 2011.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Michaud L and Gottrand F: Anastomotic
strictures: Conservative treatment. J Pediatr Gastroenterol Nutr.
52 (Suppl 1):S18–S19. 2011.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Rico FR, Panzer AM, Kooros K, Rossi TM and
Pegoli W Jr: Use of Polyflex Airway stent in the treatment of
perforated esophageal stricture in an infant: A case report. J
Pediatr Surg. 42:E5–E8. 2007.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Jang SI, Lee KH, Yoon HJ and Lee DK:
Treatment of completely obstructed benign biliary strictures with
magnetic compression anastomosis: Follow-up results after
recanalization. Gastrointest Endosc. 85:1057–1066. 2017.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Rivas H, Robles I, Riquelme F, Vivanco M,
Jiménez J, Marinkovic B and Uribe M: Magnetic surgery: Results from
first prospective clinical trial in 50 patients. Ann Surg.
267:88–93. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Parlak E, Koksal AS, Kucukay F, Eminler
AT, Toka B and Uslan MI: A novel technique for the endoscopic
treatment of complete biliary anastomosis obstructions after liver
transplantation: Through-the-scope magnetic compression
anastomosis. Gastrointest Endosc. 85:841–847. 2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Tossios P, Triantafillopoulou K, Sianos G,
Karapanayiotides T and Foroulis CN: Magnetic connectors for
coronary surgery: What do we know a decade later? Minim Invasive
Ther Allied Technol. 23:313–316. 2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Toselli L, Martinez-Ferro M, Cervio G,
Kwiat D, Imamura-Ching J, Graves CE, Gaston B and Harrison M:
Magnetic compression anastomosis (magnamosis) for functional
undiversion of ileostomy in pediatric patients. J Laparoendosc Adv
Surg Tech A. 27:1314–1317. 2017.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Russell KW, Rollins MD, Feola GP and
Scaife ER: Magnamosis: A novel technique for the management of
rectal atresia. BMJ Case Rep. 2014(bcr2013201330)2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Zaritzky M, Ben R, Zylberg GI and
Yampolsky B: Magnetic compression anastomosis as a nonsurgical
treatment for esophageal atresia. Pediatr Radiol. 39:945–949.
2009.PubMed/NCBI View Article : Google Scholar
|