Introduction
Osteomyelitis induced by a Salmonella strain
is rarely reported in the literature (1). Staphylococcus aureus is the
most common causative agent of osteomyelitis and osteomyelitis
caused by Mycobacterium tuberculosis is also found in
endemic areas (2). Primary sternal
osteomyelitis (PSO) caused by Salmonella is rare and has
typically been associated with sickle cell disease, systemic lupus
erythematosus, lymphoma and liver disease, occurring at the
extremes of age (1,3). To date, only one case of Salmonella
osteomyelitis infection of the sternum has been reported in an
infant under 1 year of age (4);
therefore, clinical experience in the timely diagnosis and
management of such cases is lacking. Meanwhile, there is no
consensus on the best treatment options for PSO in the pediatric
population with respect to long-term outcomes (5). The present study reported on two cases
of complicated PSO in infants caused by Salmonella in the
absence of any hematological diseases. These two cases may be the
youngest cases of sternal instability or abscess formation
attributed to PSO and treated with surgical debridement reported to
date. In addition, the study provided a preliminary discussion on
the relationship between the pathogenesis of this rare infectious
disease and the physiological and anatomical characteristics of
infants. CT multiplanar reconstruction combined with ultrasound
(US) is advantageous for the early diagnosis and surgical
localization of PSO. Of note, the outcomes achieved with surgical
debridement and prolonged antibiotic therapy (6) were satisfactory in the two
infants.
Case reports
Case descriptions Case A
A 12-month-old male infant suffered from fever
(maximum temperature, 40.3˚C) and excessive irritability for 2
days. His symptoms did not improve after treatment with an
alexipyretic at another clinic prior to admission to the First
People's Hospital of Honghe Prefecture in Mengzi, China in August
2018. On physical examination, the patient had a body temperature
of 40.0˚C, a heart rate of 150 beats/min, a respiratory rate of 46
breaths/min and a soft lump on the lower end of the sternum
measuring 2.5 cm in diameter. The unclearly defined swelling was
tender and warm with reddening of the local skin. The infant had
leukocytosis (8.69x109/l) with neutrophilia (48.2%,
4.2x109/l) and an elevated level of C-reactive protein
(67.8 mg/l). X-ray examination did not indicate any obvious sternal
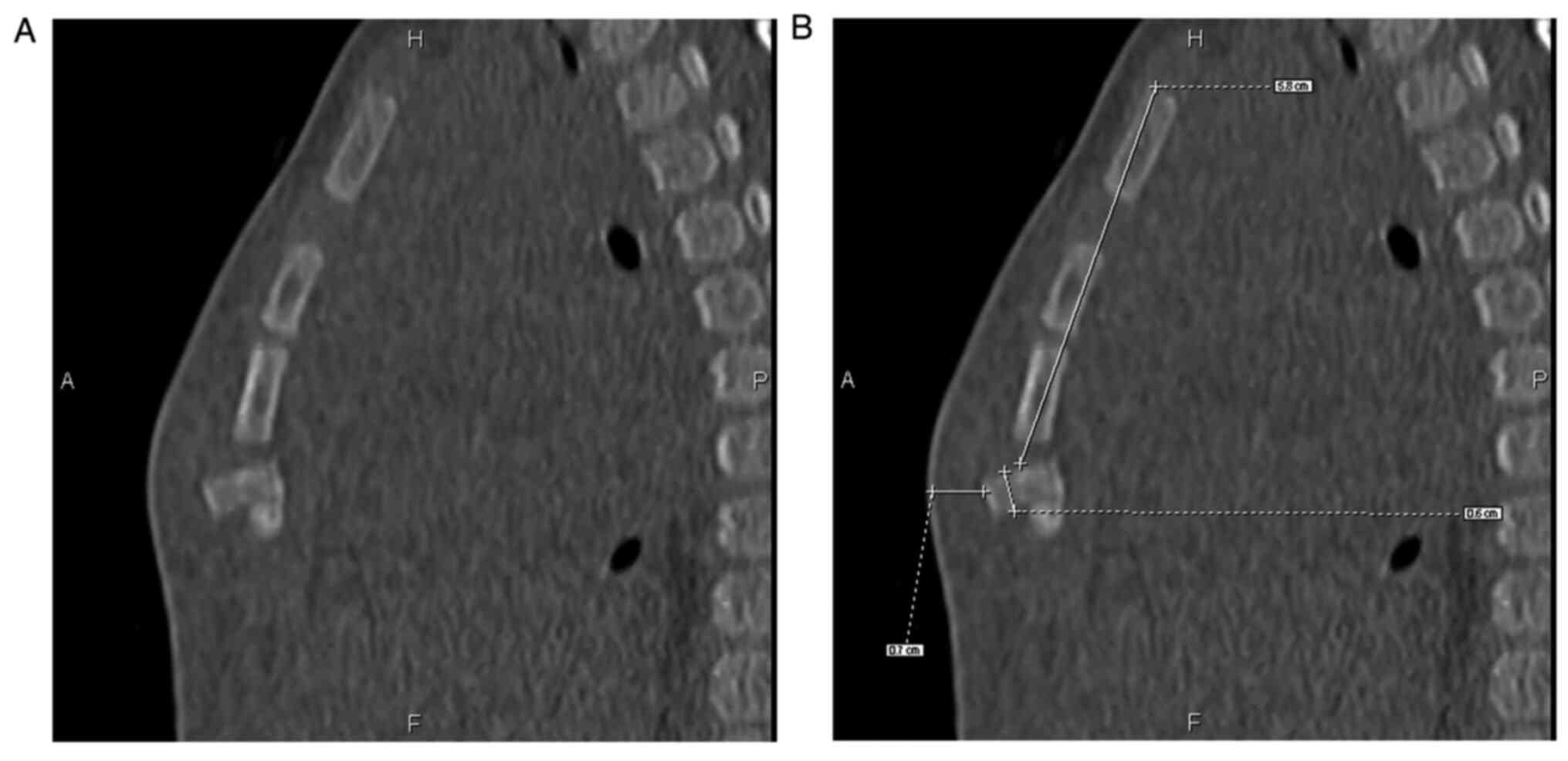
abnormalities. On CT imaging, the 4th sternebra exhibited angular
forward dislocation and a decrease in the density of the bone
cortex with overlying peripherally enhancing soft tissue was
observed (Fig. 1). US suggested
that the position of the lower sternum was abnormal and peripheral
echo enhancement was observed due to periosteal elevation (Fig. 2). Blood culture was positive for
Salmonella enteritidis sensitive to cefoperazone-sulbactam
sodium and the infant immediately received an intravenous regimen
of cefoperazone sodium and sulbactam sodium (40 mg/kg b.i.d).
Case B
A 10-month-old male infant had received
anti-infection therapy at another clinic due to fever for 1 week.
On admission to the First People's Hospital of Honghe Prefecture
(Mengzi, China) in December 2018, the patient had a body
temperature of 38.1˚C, a heart rate of 144 beats/min and a
respiratory rate of 38 breaths/min. A 2-cm firm but tender mass was
detected on the right side of the lower sternum. Laboratory
analysis revealed that the complete blood cell count was remarkable
for leukocytosis (19.2x109/l) with 52.5% neutrophils and
thrombocytosis (384x109/l), and C-reactive protein
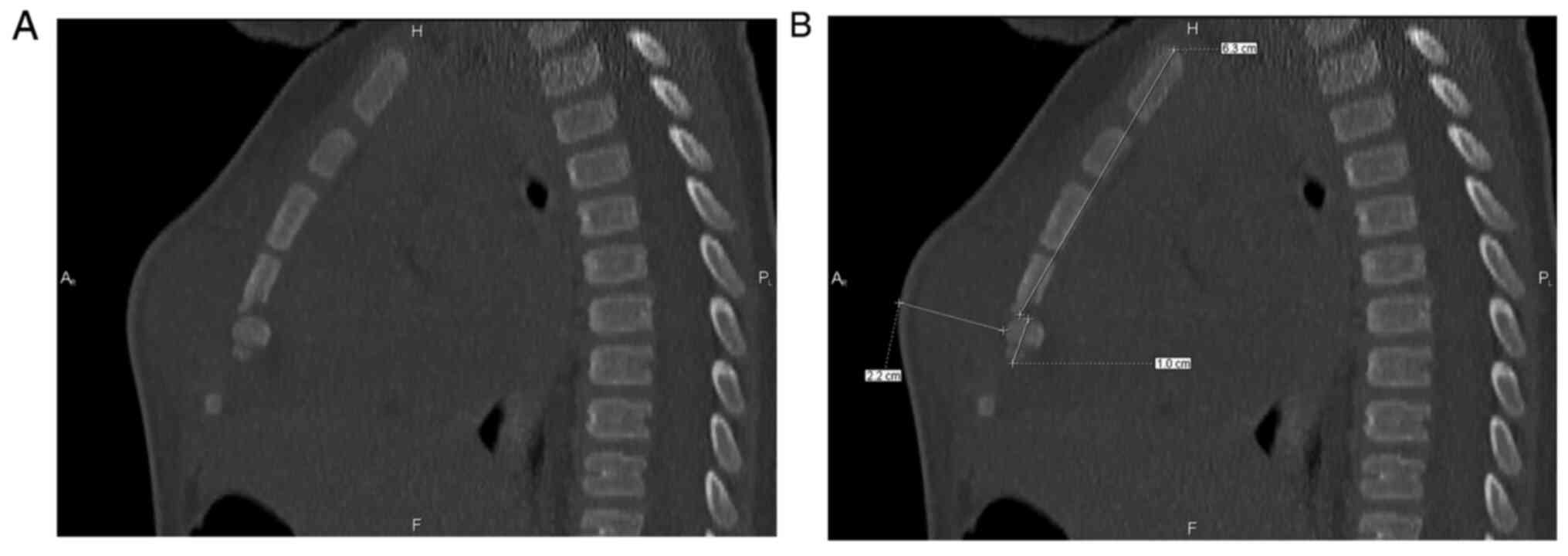
levels were elevated to >81.6 mg/l. CT scans indicated an
obviously angled 5th sternebra, lytic destruction of the 4-5th
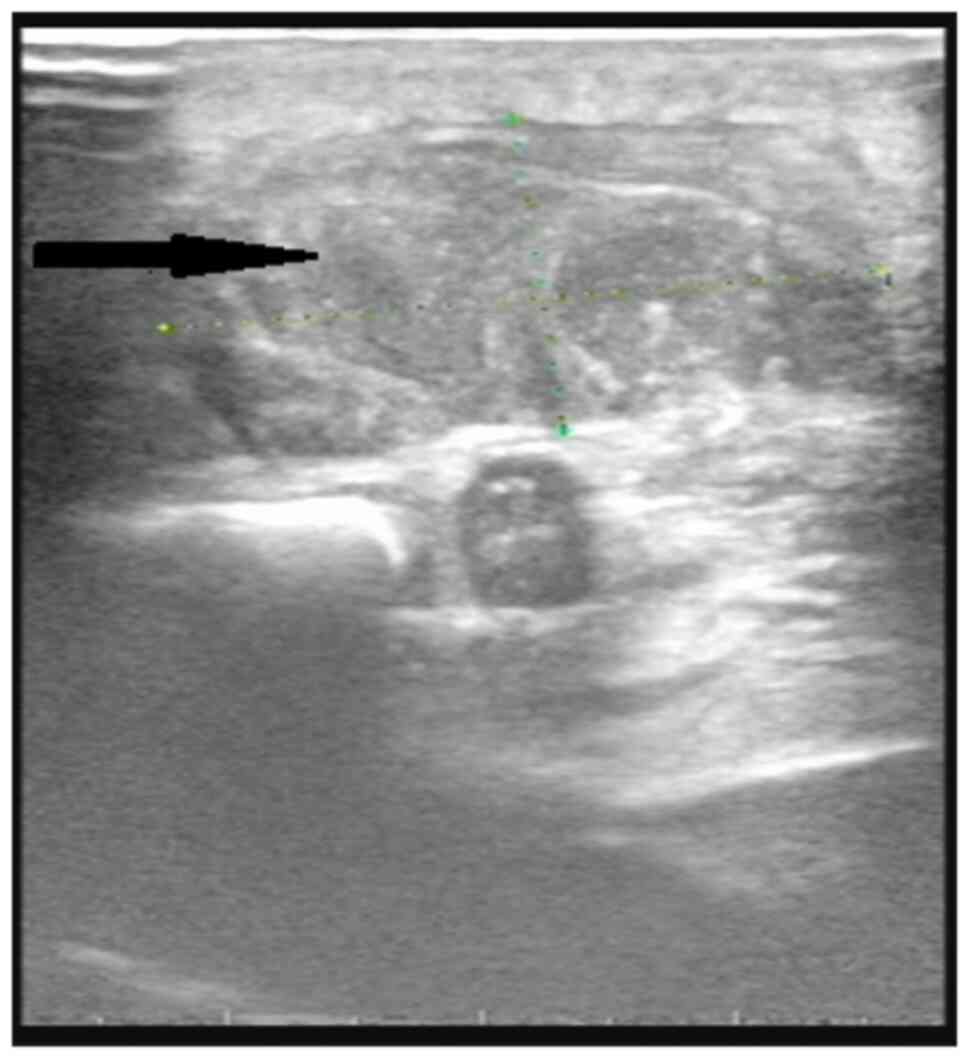
sternebrae and adjacent soft-tissue swelling (Fig. 3). US indicated that the periosteum
of the lower sternum was thickened and a 1.6x0.6 cm subcutaneous
heterogeneous hypoechoic mass was present (Fig. 4), suggestive of osteomyelitis of the
sternum with abscess formation in the adjacent tissue. Although the
blood and stool cultures were negative, the infant was treated
empirically with intravenous cefoperazone-sulbactam sodium, as
described above.
Interventions and outcomes
At ~1 week after antibiotic therapy, decreases in
the inflammatory indexes and clinical improvement were observed,
and the two patients underwent surgical debridement at this time
point. Both cases were assessed by CT multiplanar reconstruction;
based on the assessment, a minimally-invasive vertical incision was
made close to the site of dislocation on the basis of the distance
from the suprasternal fossa to the site of dislocation, and the
incision length was also based on the thickness and depth of the
sternal lesion (Figs. 1 and
3). The surgical procedures were
similar in the two cases. After perforation of the subcutaneous
tissue, purulent flow was noted. The portion of the sternum was
destroyed due to dissolution. Once the pus was drained from the
wound, bony sequestra were detected in the pleural cavity in both
cases. Only one oval-shaped bony sequestrum, with an approximate
size of 1x1 cm, was detected and removed in case A (Fig. S1). Two sequestra were removed
during the debridement process in case B, and both sequestra were
irregular in shape and ~0.5x0.5 cm in size.
The upper and lower ends of the sternum were
resected until healthy osseous tissue was reached. After
sequestrectomy was performed, the wound was flushed with saline and
hydrogen peroxide solution. Bilateral muscles around the pus cavity
were detached from the adjacent 4-5th costal cartilages with
preservation of the primary blood supply. After extension of ~2 cm
to both sides, partial flaps of bilateral pectoralis major muscles
were neatly created to cover the defect and the wound was closed
primarily with a drain.
Intraoperative purulent material cultures were
positive for Salmonella in both cases and the preoperative
antimicrobial therapy was continued according to the results of the
drug sensitivity test (minimum inhibitory concentration=16 µg/ml).
Simultaneous culture tests for Mycobacterium in both cases
provided no evidence of co-infection with other bacteria, including
Mycobacterium tuberculosis. The same preoperative
antimicrobial prescription was administered for 14 days. Once the
leukocyte count, C-reactive protein level and neutrophil
granulocyte count returned to normal ranges (Table I), the infants were discharged, and
oral trimethoprim/sulfamethoxazole was continued for 2 months
(1,5). The patients remained symptom-free and
local recurrence of PSO was not detected at the one-year follow-up.
Follow-up CT scan was performed regularly from 3-6 months, which
indicated a local sternal defect without any bony sequestrum or
abscess formation in both cases. At the time of publications, no
signs of spontaneous closure of the sternal defect had been
identified.
 | Table IRelevant laboratory data at baseline
and at significant time-points for the two cases. |
Table I
Relevant laboratory data at baseline
and at significant time-points for the two cases.
| | Case A | Case B |
|---|
| Variable | Normal range | Admission | Pre-operation | Discharge | Admission | Pre-operation | Discharge |
|---|
| Leukocyte count
(109/l) | 1.0-3.0 | 8.69 | 4.7 | 4.2 | 19.2 | 8.3 | 3.5 |
| C-reactive protein
level (mg/l) | 0-5.0 | 67.8 | 10.6 | 2.3 | 81.6 | 10.8 | 4.8 |
| Neutrophil
granulocyte count (109/l) | 1.8-7.8 | 4.2 | 3.8 | 3.5 | 10.1 | 2.5 | 3.3 |
Final diagnoses
CT multiplanar reconstruction and US provided
evidence of PSO and microbial cultivation revealed that
Salmonella was the causative agent. Based on these results,
a diagnosis of PSO caused by Salmonella was established in
each case.
Discussion
Kingella kingae, Streptococcus pneumonia and
coagulase-negative Staphylococci have been frequently
reported to be pathogenic bacteria isolated from pediatric patients
with PSO (4). However, two
consecutive cases of PSO caused by Salmonella were
encountered within 6 months and the ages of these two patients were
10 and 12 months. At this stage of life, infants start receiving
supplementary food daily in addition to breastfeeding. With respect
to the 10-month-old infant, his parents recalled that the baby had
been fed a small amount of shellfish only 1 month prior to the
occurrence of fever. The other 1-year-old infant, who lived in a
remote mountainous area, may have consumed unsterilized water as a
result of poor sanitation and living conditions. Infants and young
children are susceptible to Salmonella infection through the
ingestion of contaminated food or water (7). However, not all infants with
Salmonella infection develop a clinical manifestation of
PSO. It may be associated with non-identification of the etiology
of the infection and nonreceipt of effective anti-infective therapy
in the early stages of infection, as parents of the infants in the
present case report recalled that there was an absence of common
symptoms of Salmonella infection, including gastrointestinal
complaints and diarrhea (8).
However, whether this condition occurs as a result of a particular
Salmonella strain requires further study and observation. Of
note, extensive Volkmann canals and a Haversian system are present
in the infant sternum (3). As a
result, as pathogens are transmitted through the gastrointestinal
tract into the blood and bacteremia occurs in an infant, the porous
nature of the sternum and abundant bone marrow in the sternum may
make it susceptible to hematogenous spread of Salmonella
enteritidis, particularly in subjects with a weak immune system
(4).
The literature review comprised all reported cases
of PSO, as it is a rare condition. Its presentation may be
nonspecific and the diagnostic value of plain radiography is not
reliable (4). MRI, positron
emission tomography and single-photon emission CT are reliable
modalities for establishing the diagnosis of osteomyelitis, but
further research on their diagnostic accuracy in children is
required (9,10). In the present cases, these imaging
methods were not used due to the disadvantages of harmful ionizing
radiation, lack of cooperation by infants, long nursing time and
other considerable uncertainties in infants (age, ≤1 year).
Although US is only able to reveal outer changes in the bone
cortex, cortical destruction and periosteal elevation are visible
within a few days after the onset of clinical symptoms of
osteomyelitis and osteomyelitis is more obvious on US in the
immature bones of children (11,12).
CT scanning is also able to clearly visualize the pathological
changes of osteomyelitis, such as cortical destruction,
heterogeneous bone density and bony sequestration (12). CT with multiplanar reconstruction is
suitable for the sternum and is able to display the anatomy in
great detail (12). Therefore, US
and CT with multiplanar reconstruction were used as the diagnostic
means and for the precise surgical localization of the sequestrum
or angular displacement in the present cases. Soft-tissue swelling
on the anterior chest wall was extensive in these infants and
accurate determination of the location of the site of infection was
performed to reduce the amount of unnecessary surgical injury.
Although PSO has been managed with antibiotics only
in most cases in the pediatric population, the long-term outcomes
of this treatment regimen remain undetermined (3,5).
Numerous scholars hold the opinion that an aggressive approach
should be adopted to decrease the morbidity of indolent
osteomyelitis and mediastinitis in complicated PSO (3,5). As a
subcutaneous abscess over the anterior chest wall and sternal
instability were detected in the present cases, it was decided to
proceed with the aggressive approach. Considering the uninvolved
anterior mediastinum and the adjacent costal cartilage, the
surgical debridement procedures preserved the posterior periosteum
(5) and the wounds were closed by
using the medial margin of the pectoralis muscle flaps. Based on
the identification and sensitivity of purulent material cultures,
Salmonella was the causative agent in the two infants. A
therapeutic regimen involving sequential intravenous and oral
antibiotics was adopted (13);
parenteral cefoperazone sulbactam sodium was administered for 2
weeks, followed by oral trimethoprim/sulfamethoxazole for 2 months.
At the follow-up, the patients' wounds had healed without any
recurrence and CT imaging of the sternum indicated no
instability.
Due to the rarity of this disease, most
pediatricians have not had the opportunity to attend to and treat
such cases (14). Unfamiliarity
with PSO may contribute to a delay in diagnosis (4), and the consequences of such a delay
may be hazardous due to the seriousness of potential complications,
such as fistula formation, indolent osteomyelitis and
mediastinitis, as well as erosion of large vessels (5,15). The
present study reported on two cases of PSO along with a brief
overview of the characteristics and management modalities of this
disease, which may serve as a guide for pediatricians regarding
this rare disease caused by Salmonella, particularly in
infants.
In infants who present with fever, elevated
inflammatory indices and a chest wall mass, PSO should be highly
suspected. If the patient has a history of an unhygienic diet, the
possibility of Salmonella infection should not be
overlooked. CT multiplanar reconstruction combined with US has the
practicability and maneuverability to establish an early diagnosis
and to achieve surgical localization of PSO in infants. Surgical
debridement and prolonged therapy with antibiotics (6) is key to achieving satisfactory
outcomes for cases of complicated PSO.
Supplementary Material
Intraoperative photographs of a
sequestrum moved in the pleural cavity around the mesosternum for
case A. (A) Black arrow indicates the sequestrum. (B) Black arrow
indicates the pleural cavity.
Acknowledgements
The authors wish to thank Dr Xin Cao (Division of
Pediatric Cardiothoracic Surgery, The Children's Hospital of
Kunming, Yunnan, China) for his critical reading of the manuscript
and helpful discussion.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
MQ and YL conceived the study, participated in its
design and coordination, and drafted the manuscript. JW, XC, and XP
performed the clinical diagnosis and treatment of the patients. SW,
ZW, JL, and HO were responsible for the collection and analysis of
the experimental data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was approved by the ethics committee of
The First People's Hospital of Honghe Prefecture (Mengzi, China).
All procedures performed in the study involving human participants
were in accordance with the ethical standards of the institutional
and/or national research committee and with the 1964 Declaration of
Helsinki and its later amendments or comparable ethical
standards.
Patient consent for publication
Informed written consent was obtained from the
infants' guardians for publication of their data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Araiza-Garaygordobil D, Soto-Nieto GI,
Aguilar-Rojas LA and Catrip J: Primary sternal osteomyelitis caused
by Salmonella enteritidis. Enferm Infecc Microbiol Clin.
35:60–62. 2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Pettas NS, Apostolopoulos AP, Flieger I
and Leonidou O: Primary sternal osteomyelitis in a 40 days old
infant: A case report and review of the literature. Cases J.
2(7504)2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sayed S, Prabhu S, Thomas M, McBride CA
and Alphonso N: Primary sternal osteomyelitis with extensive
mediastinal abscess in a neonate. Ann Thorac Surg. 100:e85–e87.
2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Schweitzer A, Della Beffa C, Akmatov MK,
Narchi H, Abaev YK, Sherry DD and Pessler F: Primary osteomyelitis
of the sternum in the pediatric age group: Report of a new case and
comprehensive analysis of seventy-four cases. Pediatr Infect Dis J.
34:e92–e101. 2015.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bryant R III, Morales DL and Phalak K:
Multimodality therapy for primary sternal osteomyelitis. Pediatr
Infect Dis J. 28:73–74. 2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Muesse JL, Blackmon SH, Ellsworth WA IV
and Kim MP: Treatment of sternoclavicular joint osteomyelitis with
debridement and delayed resection with muscle flap coverage
improves outcomes. Surg Res Pract. 2014(747315)2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Thomson RM, Henderson HJ and Smith-Palmer
A: An outbreak of Salmonella Saintpaul in a Scottish
childcare facility: The influence of parental under-reporting. BMC
Infect Dis. 19(847)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ngogo FA, Joachim A, Abade AM, Rumisha SF,
Mizinduko MM and Majigo MV: Factors associated with
Salmonella infection in patients with gastrointestinal
complaints seeking health care at Regional Hospital in Southern
Highland of Tanzania. BMC Infect Dis. 20(135)2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Crone AM, Wanner MR, Cooper ML, Fox TG,
Jennings SG and Karmazyn B: Osteomyelitis of the ribs in children:
A rare and potentially challenging diagnosis. Pediatr Radiol.
50:68–74. 2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Llewellyn A, Jones-Diette J, Kraft J,
Holton C, Harden M and Simmonds M: Imaging tests for the detection
of osteomyelitis: A systematic review. Health Technol Assess.
23:1–128. 2019.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Lu CH, Hsiao YF, Hsu HC, Ko YL, Lin TS,
Chen LF, Hsieh SC and Li KJ: Can ultrasound differentiate acute
erosive arthritis associated with osteomyelitis, rheumatoid
arthritis, or gouty arthritis? Int J Rheum Dis. 22:1972–1977.
2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Sammak B, Abd El Bagi M, Al Shahed M,
Hamilton D, Al Nabulsi J, Youssef B and Al Thagafi M:
Osteomyelitis: A review of currently used imaging techniques. Eur
Radiol. 9:894–900. 1999.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ecury-Goosssen GM, Huysman MA,
Verhallen-Dantuma JC and Man P: Sequential intravenous-oral
antibiotic therapy for neonatal osteomyelitis. Pediatr Infect Dis
J. 28:72–73. 2009.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Joshi P, Bavdekar SB and Save SU: A
swelling over sternum in a child: Reminder of an uncommon
diagnosis. Case Rep Pediatr. 2016(3765786)2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Singal R, Singh P, Mittal A, Gupta S,
Singla S and Kenwar DB: Primary sternal tuberculous ulcer with
dissemination to the bone marrow: A clinical rarity. Ann Saudi Med.
31:542–545. 2011.PubMed/NCBI View Article : Google Scholar
|