Introduction
Uremia, also known as end-stage renal failure in the
clinic, is particularly common in nephrology. In such patients,
uremia is frequently complicated with myocardial damage, leading to
cardiac insufficiency (1). The most
common causes of cardiac insufficiency in uremic patients are
hemodynamic changes and metabolic abnormalities, leading to
increased mortality (2). In
patients with uremia, significant hemodynamic changes and
accumulation of toxins are present, and myocardial tissue cells
frequently have systolic and diastolic dysfunction (3). More than half of the patients with
uremia succumb to cardiac insufficiency (4). Uremic patients frequently have varying
degrees of anemia and decreased production of erythropoietin
(5). Uremia is not only a
pathological reaction of the body's response to renal dysfunction
but also an inflammatory reaction associated with chronic oxidation
(6). A previous study has defined
this as a uremia-associated inflammatory response and the degree of
anemia is aggravated due to reduced production of erythropoietin
and impaired iron mobilization caused by an excessive inflammatory
response (7). The occurrence of
cardiac dysfunction in patients with uremia is significantly
associated with oxidative stress in the body and oxidative stress
is also an important contributing factor to the occurrence of
cardiac dysfunction (8).
Significantly increased oxidative stress levels in patients with
uremia are caused by increased production of toxins and impaired
excretion function in end-stage renal failure. Excessive oxidative
stress mainly leads to damage of the patient's vascular endothelial
cells, thereby promoting the occurrence of cardiac insufficiency
(9). However, the exact association
of cardiac function with inflammatory cytokines, oxidative stress
and anemia in patients with uremia remains to be fully elucidated.
The aim of the present study was to assess the association of
cardiac function with inflammatory cytokines, oxidative stress and
anemia in patients with uremia.
Patients and methods
Patients
A total of 79 patients diagnosed with uremia at the
Department of Nephrology of the Affiliated Hospital of North
Sichuan Medical College (Nanchong, China) between May 2016 and June
2017 were recruited. Among them, 43 patients had cardiac
insufficiency (observation group) and 36 patients had no cardiac
insufficiency (control group). The cohort comprised 49 males and 30
females aged 40-72 years with an average age of 57.78±12.09 years.
The diagnostic criteria for uremia were as follows: Glomerular
filtration rate (GFR) <10 ml/min or serum creatinine >707
µmol/l. The exclusion criteria were as follows: patients with
systemic multiple organ failure, those complicated with serious
infections, rheumatoid arthritis and other autoimmune diseases,
those taking topical steroids or receiving blood purification or
peritoneal dialysis treatment prior to diagnosis, or those with
mental illness, with incomplete clinical data or refusing to
provide informed consent. The present study was approved by the
ethics committee of the Affiliated Hospital of North Sichuan
Medical College (Nanchong, China; no. 20160102AHNSMCE) and informed
consent from the subjects was obtained prior to the study.
Measurement of blood biochemical
parameters
After fasting for solids and liquids for 10 h
overnight, fasting peripheral blood was collected from all patients
enrolled and centrifuged to obtain serum, which was used to measure
total cholesterol (TC), triglyceride (TG), low-density lipoprotein
cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C),
hemoglobin (Hb), platelets (PLT) and mean corpuscular volume (MCV)
using an automatic biochemical analyzer (Hitachi; model no.
HTCA3060).
Detection of the levels of
inflammatory cytokines
The levels of inflammatory cytokines [C-reactive
protein (CRP), interleukin-6 (IL-6) and IL-10] were measured
through immunoturbidimetry (BK-400; Shandong Boke CNC equipment
Co., Ltd.) following the manufacturer's protocol. The reagents were
provided by Shenzhen Genrui Biological Technology Co., Ltd. The
levels of malondialdehyde (MDA; cat. no. ab238537; Abcam), oxidized
low-density lipoprotein (OX-LDL; cat. no. ab242302; Abcam) and
advanced oxidation protein products (AOPP; cat. no. ab242295;
Abcam) were determined by ELISA according to the manufacturer's
protocol.
Assessment of cardiac function
Cardiac function was determined through measuring
the cardiac output (CO), cardiac stroke volume (SV), left
ventricular ejection fraction (LVEF), left ventricular
end-diastolic diameter (LVEDd) and left ventricular end-systolic
diameter (LVESd) by a full-time technician using a Vivid
6-dimension ultrasound instrument (GE Healthcare).
Statistical analysis
SPSS 19.0 software (IBM Corp.) was used for data
processing. The results were expressed as the mean ± standard
deviation. Student's t-test was performed for comparison of
differences between two groups and the Chi-square test was adopted
for comparisons of enumeration data. Pearson correlation was
applied for correlation analysis. P<0.05 was considered to
indicate a statistically significant difference.
Results
Comparisons of clinical
characteristics
There were no statistically significant differences
in age, sex, body mass index, TC, LDL-C and HDL-C levels between
the observation group and the control group (P>0.05). However,
the observation group had significantly higher TG and blood
pressure levels, as well as a longer duration of uremia compared
with the control group (P<0.05; Table I).
 | Table IComparison of general characteristics
between the observation group and control group. |
Table I
Comparison of general characteristics
between the observation group and control group.
| General data | Observation group
(n=43) | Control group
(n=36) | P-value |
|---|
| Age, years (mean ±
SD) | 58.53±6.98 | 57.03±9.61 | 0.619 |
| Sex, male/female
(n) | 29/14 | 20/16 | 0.145 |
| Disease course, years
(mean ± SD) | 11.78±2.05 | 6.79±3.83 | 0.018 |
| BMI, kg/m² (mean ±
SD) | 18.88±2.93 | 18.79±3.29 | 0.475 |
| TC, mmol/l (mean ±
SD) | 5.83±1.05 | 5.45±1.02 | 0.068 |
| TG, mmol/l (mean ±
SD) | 2.94±1.05 | 2.07±0.79 | 0.042 |
| LDL-C, mmol/l (mean ±
SD) | 3.43±0.97 | 3.08±0.76 | 0.588 |
| HDL-C, mmol/l (mean ±
SD) | 1.53±0.54 | 1.45±0.33 | 0.081 |
| SBP, mmHg (mean ±
SD) | 165±28 | 147±24 | 0.039 |
| DBP, mmHg (mean ±
SD) | 99±18 | 83±16 | 0.041 |
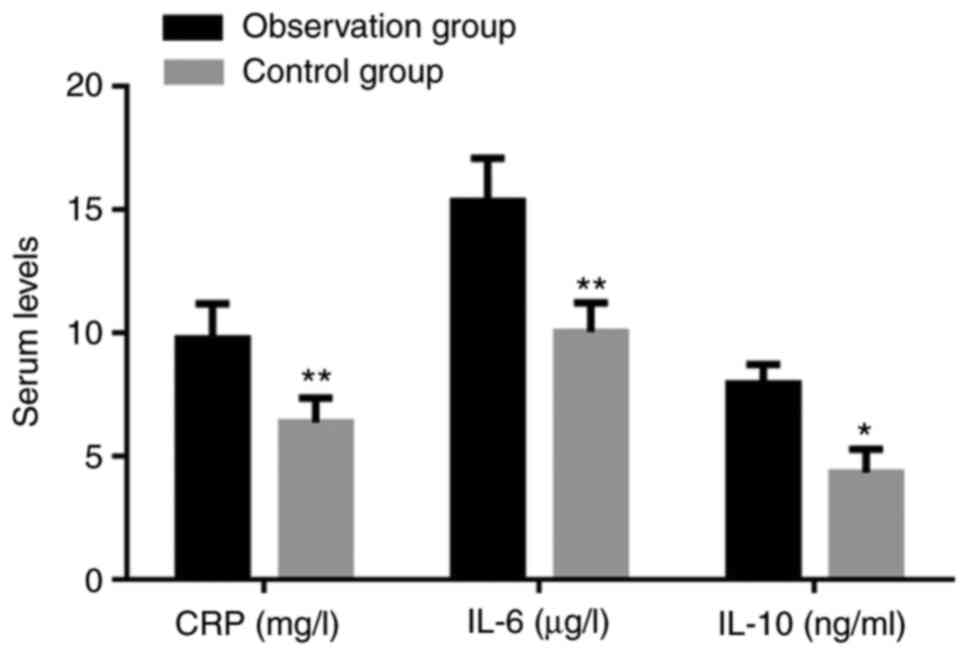
Increased levels of inflammatory
cytokines in patients with cardiac dysfunction
The peripheral serum levels of CRP, IL-6 and IL-10
in the observation group were all significantly higher than those
in the control group (P<0.05; Fig.
1).
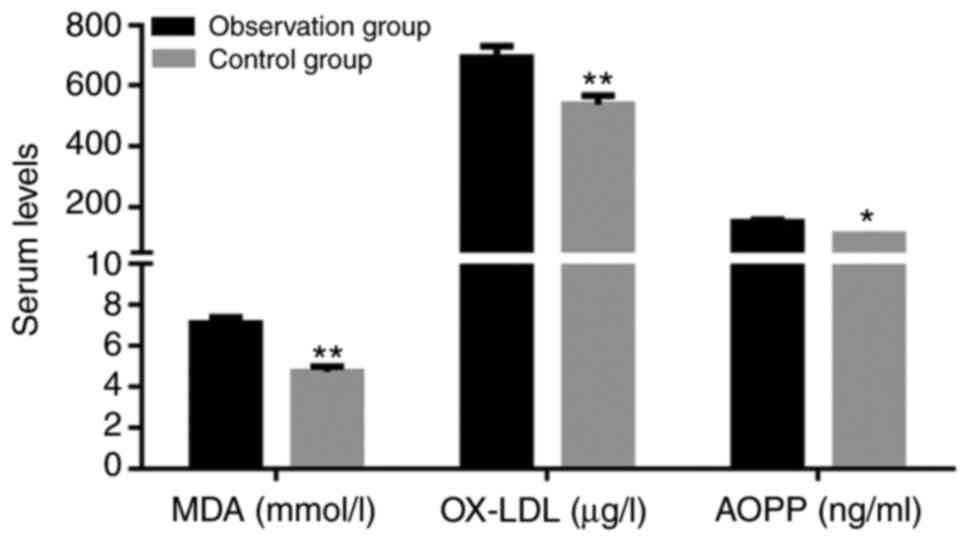
Elevated oxidative stress in patients
with cardiac dysfunction
The levels of MDA, OX-LDL and AOPP in the
observation group were significantly increased compared with those
in the control group (P<0.05; Fig.
2).
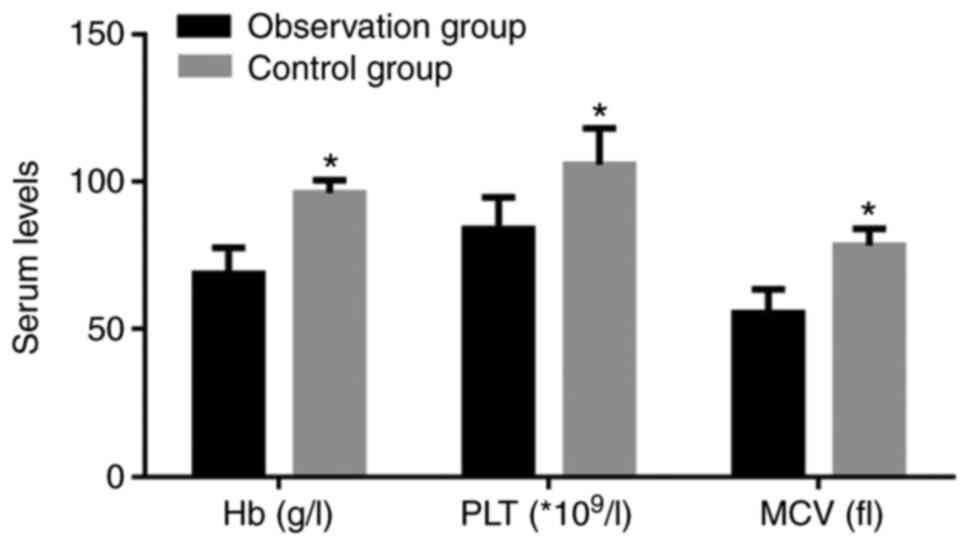
Comparison of anemia
Comparison of anemia-associated parameters between
the two groups of patients indicated that the observation group had
significantly lower Hb, PLT and MCV compared with the control group
(P<0.05; Fig. 3).
Comparison of cardiac function
indicators
In terms of cardiac function, the observation group
had a significantly lower CO, SV and LVEF and higher LVEDd and
LVESd compared with the control group (P<0.05; Table II).
| Table IIComparison of cardiac function
indicators. |
Table II
Comparison of cardiac function
indicators.
| Relevant
indicator | Observation group
(n=43) | Control group
(n=36) | P-value |
|---|
| CO, l/min (mean ±
SD) | 3.73±0.82 | 4.39±0.88 | 0.025 |
| SV, ml (mean ±
SD) | 40.78±6.15 | 51.90±5.69 | 0.003 |
| LVEF, % (n) | 32±7 | 43±5 | 0.039 |
| LVEDd, mm (mean ±
SD) | 73.39±7.42 | 69.58±8.03 | 0.040 |
| LVESd, mm (mean ±
SD) | 59.29±3.05 | 48.75±4.28 | 0.035 |
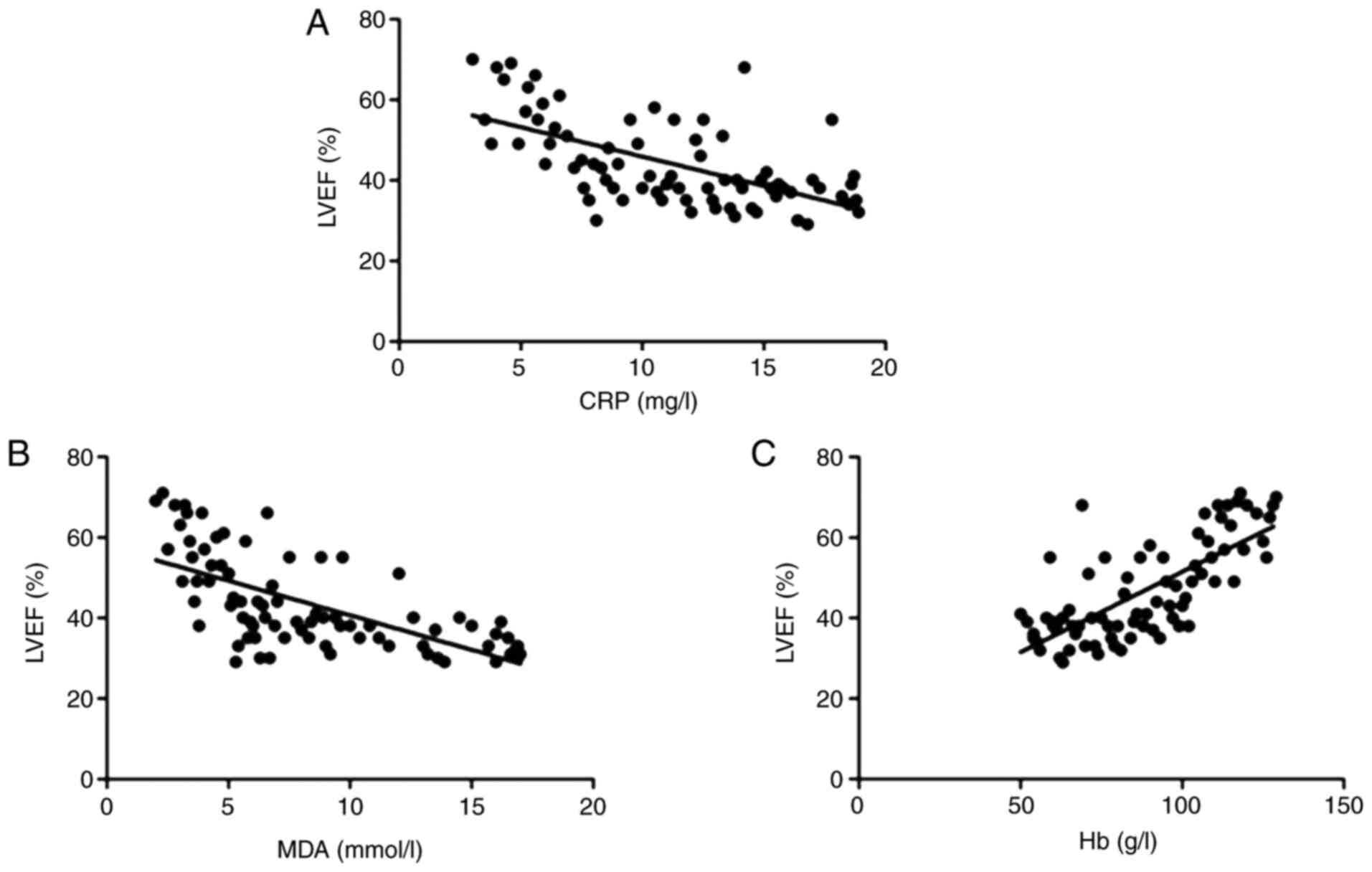
Correlations of cardiac function with
serum inflammatory cytokines, oxidative stress and anemia
To analyze the association of cardiac dysfunction
with inflammatory cytokines, oxidative stress or anemia, a
correlation analysis was performed. It was indicated that the LVEF
was negatively correlated with CRP (r=-0.636, P<0.01; Fig. 4A) and MDA (r=-0.705, P<0.01;
Fig. 4B), but positively correlated
with Hb levels (r=0.732, P<0.001; Fig. 4C).
Discussion
Uremia, a chronic inflammatory disease, is generally
considered as a reaction (in cellular, biochemical and other
aspects) of the patient's body in response to renal failure, the
major driving factors of which are a series of inflammatory
cytokines and the most striking feature is chronic oxidation
(10). Uremic patients frequently
exhibit excessive inflammatory response and different degrees of
anemia. Iron mobilization declines due to a markedly reduced
production of erythropoietin. Furthermore, there is a certain
degree of resistance to erythropoietin in uremic patients (11). The major causes of death in patients
with uremia are cardiovascular disease-associated complications, as
demonstrated by impaired myocardial cell systolic or diastolic
function in uremic patients, which are caused by myocardial cell
tissue fibrosis, ventricular enlargement and hypertrophy,
pericarditis and impairment of various valve areas (12). Numerous studies have indicated that
cardiac insufficiency in patients with uremia is mainly caused by
non-specific pathological changes in various aspects rather than
uremia alone (13). The most common
causes of cardiac insufficiency in uremic patients include an
elevation in blood pressure, increased heart volume and load,
anemia of various severities, release of a large number of
inflammatory cytokines and uremic toxins, as well as long-term
oxidative stress (3). A recent
study has suggested that CRP and IL may effectively reflect the
degree of inflammation in uremic patients (14). It has been indicated that
inflammation is a common cause of renal impairment and a major
cause of morbidity and mortality of patients with kidney disease,
and overactivation of the inflammatory response in uremic patients
is closely linked to infection, toxin release and malnutrition
(15). Consistent with these
results, the present study indicated that inflammatory cytokines in
uremic patients complicated with cardiac insufficiency were
significantly higher than those in uremic patients without cardiac
insufficiency. Furthermore, inflammatory cytokines were also
negatively correlated with the LVEF, suggesting that the
inflammation triggered by increased secretions of inflammatory
cytokines may be a contributing factor in the development of
cardiac insufficiency, implying that anti-inflammatories may be
beneficial to improve cardiac function in uremic patients with
cardiac insufficiency.
Oxidative stress, which causes lipid peroxidation,
may contribute to increase the risk of atherosclerosis. Oxidative
stress in patients with uremia refers to increased reactive oxygen
species in the body. Recent study indicates that levels of lipid
peroxidation products (malonaldehyde and 4-hydroxyalkenals) are
significantly raised in the plasma of renal patients before
dialysis and, although reduced after this treatment, the levels
still remained above the normal range (16). Once there is a dynamic imbalance
between oxidation and anti-oxidative processes in the body, the
internal environment becomes unstable. Uremic patients suffer from
disorder of the internal environment (i.e., oxidative stress) for a
long time, causing damage to endothelial cell tissues (17). In general, disorder of lipid and
calcium-phosphorus metabolism occurs in uremic patients, resulting
in activated oxidation of fat and protein, and increased levels of
oxidation products, including MDA in the patients' body (18). Oxidation products, including MDA and
AOPP, are closely linked to atherosclerosis. Furthermore, increased
levels of oxidation products in vivo may lead to impaired
cardiovascular endothelial function (19). In accordance with these previous
results, the present study indicated that uremic patients with
cardiac insufficiency had significantly higher levels of oxidation
products in comparison with those without cardiac insufficiency. On
the other hand, patients with uremia suffer from anemia due to the
reduction of erythropoietin, which is aggravated, as red blood
cells have increased fragility and are more susceptible to rupture
due to decreased levocarnitine and other substances in the body.
Furthermore, anemia leads to insufficient blood supply to the
myocardium, resulting in impaired cardiac function (19). The present study indicated that the
degree of anemia in uremic patients with cardiac insufficiency was
higher than in patients without cardiac insufficiency, and Hb was
positively correlated with LVEF. A previous study evaluated the
effect of left ventricular hypertrophy and deformation on cardiac
function in patients with uremic cardiomyopathy by using the
technology of two-dimensional speckle tracking imaging and the
result indicated that the LVEF was decreased as cardiac function
was reduced (20), which was
consistent with the present study. However, limitations with this
study are that the current data is based on a single-center study
with a relatively small cohort. The correlation between cardiac
insufficiency in uremic patients and inflammatory cytokines,
oxidative stress and anemia requires to be further validated in a
large number of samples from different regions in order to decrease
the bias.
In conclusion, the present study indicated that
cardiac insufficiency in patients with uremia is closely associated
with inflammatory cytokines, oxidative stress and the degree of
anemia, suggesting that inhibition of inflammation and oxidative
stress or amelioration of anemia may improve cardiac function in
uremic patients with cardiac insufficiency.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HZ substantially contributed to the experimentation
and acquisition of data. LF designed experiments, performed data
analysis and wrote the manuscript. HL and LT contributed to the
conception of the study. JZ and DX helped perform the analysis with
constructive discussions. JF contributed significantly to the data
analysis and manuscript preparation. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of the Affiliated Hospital of North Sichuan Medical
College (Nanchong, China; no. 20160102AHNSMCE) and informed consent
from the subjects was obtained prior to the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Foley RN, Parfrey PS and Sarnak MJ:
Clinical epidemiology of cardiovascular disease in chronic renal
disease. Am J Kidney Dis. 32 (Suppl 3):S112–S119. 1998.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Usberti M, Gerardi GM, Gazzotti RM,
Benedini S, Archetti S, Sugherini L, Valentini M, Tira P, Bufano G,
Albertini A, et al: Oxidative stress and cardiovascular disease in
dialyzed patients. Nephron. 91:25–33. 2002.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Himmelfarb J, Stenvinkel P, Ikizler TA and
Hakim RM: The elephant in uremia: Oxidant stress as a unifying
concept of cardiovascular disease in uremia. Kidney Int.
62:1524–1538. 2002.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Witko-Sarsat V, Friedlander M,
Capeillère-Blandin C, Nguyen-Khoa T, Nguyen AT, Zingraff J, Jungers
P and Descamps-Latscha B: Advanced oxidation protein products as a
novel marker of oxidative stress in uremia. Kidney Int.
49:1304–1313. 1996.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Morena M, Cristol JP and Canaud B: Why
hemodialysis patients are in a prooxidant state? What could be done
to correct the pro/antioxidant imbalance. Blood Purif. 18:191–199.
2000.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hirayama A, Nagase S, Gotoh M, Takemura K,
Tomida C, Ueda A, Aoyagi K, Terao J and Koyama A: Hemodialysis does
not influence the peroxidative state already present in uremia.
Nephron. 86:436–440. 2000.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Miyata T, Ueda Y, Yamada Y, Izuhara Y,
Wada T, Jadoul M, Saito A, Kurokawa K and van Ypersele de Strihou
C: Accumulation of carbonyls accelerates the formation of
pentosidine, an advanced glycation end product: Carbonyl stress in
uremia. J Am Soc Nephrol. 9:2349–2356. 1998.PubMed/NCBI
|
|
8
|
Zimmermann J, Herrlinger S, Pruy A,
Metzger T and Wanner C: Inflammation enhances cardiovascular risk
and mortality in hemodialysis patients. Kidney Int. 55:648–658.
1999.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Riella MC: Malnutrition in dialysis:
Malnourishment or uremic inflammatory response? Kidney Int.
57:1211–1232. 2000.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Steinberg D, Parthasarathy S, Carew TE,
Khoo JC and Witztum JL: Beyond cholesterol. Modifications of
low-density lipoprotein that increase its atherogenicity. N Engl J
Med. 320:915–924. 1989.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Mak S, Lehotay DC, Yazdanpanah M, Azevedo
ER, Liu PP and Newton GE: Unsaturated aldehydes including
4-OH-nonenal are elevated in patients with congestive heart
failure. J Card Fail. 6:108–114. 2000.PubMed/NCBI
|
|
12
|
Cracowski JL, Devillier P, Durand T,
Stanke-Labesque F and Bessard G: Vascular biology of the
isoprostanes. J Vasc Res. 38:93–103. 2001.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Schettler V, Wieland E, Methe H,
Schuff-Werner P and Müller GA: Oxidative stress during dialysis:
Effect on free radical scavenging enzyme (FRSE) activities and
glutathione (GSH) concentration in granulocytes. Nephrol Dial
Transplant. 13:2588–2593. 1998.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Uchida K: Role of reactive aldehyde in
cardiovascular diseases. Free Radic Biol Med. 28:1685–1696.
2000.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Helmke A and von Vietinghoff S:
Extracellular vesicles as mediators of vascular inflammation in
kidney disease. World J Nephrol. 5:125–138. 2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Fiorillo C, Oliviero C, Rizzuti G, Nediani
C, Pacini A and Nassi P: Oxidative stress and antioxidant defenses
in renal patients receiving regular haemodialysis. Clin Chem Lab
Med. 36:149–153. 1998.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Canaud B, Cristol J, Morena M,
Leray-Moragues H, Bosc J and Vaussenat F: Imbalance of oxidants and
antioxidants in haemodialysis patients. Blood Purif. 17:99–106.
1999.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Siems WG, Sommerburg O and Grune T:
Erythrocyte free radical and energy metabolism. Clin Nephrol. 53
(Suppl):S9–S17. 2000.PubMed/NCBI
|
|
19
|
Siems W, Carluccio F, Grune T, Jakstadt M,
Quast S, Hampl H and Sommerburg O: Elevated serum concentration of
cardiotoxic lipid peroxidation products in chronic renal failure in
relation to severity of renal anemia. Clin Nephrol. 58 (Suppl
1):S20–S25. 2002.PubMed/NCBI
|
|
20
|
Zheng Y, Yang X, Zhou Q, Huang Y, Zhang F
and Wang L: Effect of left ventricular hypertrophy and deformation
on cardiac function in patients with uremia cardiomyopathy by using
quantitative speckle tracking technology. Zhong Nan Da Xue Xue Bao
Yi Xue Ban. 42:400–405. 2017.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|