Introduction
Hypoxic-ischemic encephalopathy (HIE) is a major
cause of neurologic disabilities in neonates despite the recent
widespread use of hypothermia therapy. The incidence of HIE ranges
from 1 to 8 per 1,000 live births in developed countries and is as
high as 26 per 1,000 live births in underdeveloped countries
(1). Hypoxia-ischemia (HI) is a
contributing factor to neonatal morbidity and mortality, often
leading to chronic neurological disorders and disabilities, such as
mental retardation, motor and behavioral developmental issues,
cerebral palsy, seizure, and epilepsy. Newborns with mild HIE
(grade I) have a favorable evolution. Approximately 80% of the
patients with grade II encephalopathy recover; however, the
mortality rate is 3 and 20-45% have neurological sequelae. Patients
with severe HIE (grade III) have a mortality rate of 50% and
survivors present severe neurological consequences (2).
Manifestations of HIE involve heart rhythm
disorders, basic acid balance disorders (pH<7.0 or basic
deficiency ≥12 mmol/l), low Apgar index, amniotic fluid impregnated
with meconium or the need for respiratory support in the first few
minutes of postnatal life (3).
The redistribution of cerebral blood flow induced by
asphyxia is the main post-asphyxiation change. Brain injury results
from hypoxia and ischemia. As a result of asphyxia, cardiac output
is compensated by redistribution, thus increasing cerebral blood
flow. If hypoxia persists, this self-regulatory mechanism is no
longer effective, resulting in decreased heart rate, with systemic
hypotension and decreased cerebral flow leading to brain damage. At
the cellular level, oxygen depletion blocks oxidative
phosphorylation resulting in an anaerobic metabolism, which is
energy inefficient, resulting in: i) Rapid depletion of phosphate
reserves, including adenosine triphosphate, ii) accumulation of
lactic acid and iii) inability to maintain cellular functions.
Oxidative stress, which is basically an alteration
in the balance between antioxidants and prooxidants, needs to be
considered, particularly in view of the existence of certain
microcirculation deficits and endothelial dysfunction related to
excess production of free radicals, which results in increased
oxidative stress status (4).
In the first phase, an initial healing process
begins in the first 60 min after the acute injury. In the latent
phase (between the first and the sixth hour), oxidative metabolism
inflammation and the continuation of apoptotic cascades take place.
Six to 48 h after the hypoxic-ischemic incident, phosphate reserves
are depleted, excitatory neurotransmitters and free radicals are
released. In the third phase, a few months after acute ischemia,
late cell death, remodeling of brain tissue and astrogliosis occur
(4,5). Multiorgan dysfunction represents a
natural consequence of the redistribution of blood flow mechanism.
Affected cells release intracellular enzymes, some of which are
easy to measure, such as lactate dehydrogenase (LDH), which is
present in most body tissues. Elevated levels of this enzyme have
been reported after neonatal asphyxia. These aspects make this
enzyme a potential predictor of the severity of hypoxic-ischemic
injury in the postnatal period (6).
In clinical practice, biochemical evidence of
multiorgan dysfunction is evident in over 70% of the cases of acute
intrapartum asphyxia leading to neonatal encephalopathy (7). The measurement of LDH at 72 h may
differentiate between neonatal asphyxia and other non-asphyxiating
etiologies, especially in newborns with nonspecific signs of
disease. In a study of 45 newborns, Reddy et al showed that
LDH sensitivity was 100% and specificity was 89% (8). However, in another study of 61
newborns, it was shown that the sensitivity of LDH was 94% and the
specificity was 67% (9).
In most organs, including the brain, neutrophils are
the first cells to accumulate and infiltrate the tissue at
reperfusion followed by monocytes and then T lymphocytes (10). Leukocyte recruitment into inflamed
tissue proceeds in a cascade-like fashion. The first contact of
neutrophils with the endothelium is mediated by selectins and their
counterreceptors, followed by rolling of neutrophils along the
endothelial wall of postcapillary venules and integrin-mediated
arrest (11).
Cerebral ischemia induces an inflammatory response
in both the parenchyma and the systemic circulation. Within hours
after an insult to the brain, cytokines are produced in large
amounts, and leukocytes are activated and migrate into the injured
brain. There are few studies investigating the role of lymphocytes
in HIE. A lymphocyte response is likely to be involved in the
activation and exacerbation of chronic immuno-inflammatory after
HIE. It is not clear yet whether this lymphocyte response improves,
or, conversely, worsens healing after cerebral ischemia (12). In newborns with asphyxia at birth, a
low number of lymphocytes have been found to be associated with a
high risk of death (13).
Cytokines induce leukocyte proliferation, increase
the number of circulating neutrophils and help endothelial
transmigration and chemotaxis in damaged areas. It has been
observed that the increased number of peripheral neutrophils in the
first 96 h of life in newborns with HIE may contribute to the
abnormal outcome of neurological development (14). However, in a study performed on 316
newborns, no associations were observed between changes in
hematological values and brain damage due to post or intrapartum
asphyxia (15).
This study was designed to investigate whether there
is a relationship between serum cellular enzymes (LDH) with
hematologic changes in red and white blood cells (lymphocytes and
neutrophils) and the systemic inflammatory response revealed by
procalcitonin (PCT) and C-reactive protein (CRP) values.
The first objective was to determine the evolution
over time of hematological and biochemical changes in the newborn
with HIE.
The second objective was to determine whether there
was a relationship between the observed changes and the prognosis
of newborns. The time to determine the blood tests varied between 6
and 96 h. If blood tests were repeated, the maximum values in the
first 96 h were recorded.
Materials and methods
Newborns
This is a retrospective, cross-sectional cohort
study. This study was performed at the Neonatology Department at
the Emergency Hospital for Children ‘Louis Turcanu’ Timisoara. This
study was conducted over a period of 3 years, from January 1, 2016
to December 31, 2018. The study included 78 newborns weighing
between 1 kg and 3.8 kg at birth.
The exclusion criteria from the study were:
Incomplete patient data, information unavailable in the hospital's
computer system, gestational age less than 35 weeks, newborns who
suffered or had signs of infection/sepsis that could have
influenced these investigations, the presence of a major congenital
anomaly or any primary cause of encephalopathy other than
ischemia/hypoxia.
Demographic, gestational, and perinatal data for the
newborns included in the study were reviewed, including the
presence of antenatal risk factors for both HIE, congenital
anomalies and infections of any kind.
All newborns were identified by computer search of
medical documents in the online database of the medical unit.
Hemotological investigation
Hematological investigations were performed with a
Sysmex XS800i analyzer using impedance spectroscopy, flow
cytometry, Hydro Dynamic Focusing (DC Detection method) and the
reagents were provided by Sysmex Corp. (Kobe, Japan). The cell
blood count (CBC) was collected from peripheral venous blood, 1 ml
of blood, and the sample was taken in a test tube with EDTA (sodium
calcium edetate). The unit of measurement for Hb was g/dl and for
the leukocyte formula it was µl for biochemical investigations 1 ml
of peripheral venous blood was collected, using a normal test tube.
The biochemical investigations were performed with a Cobas Integra
400 Plus analyzer and the reagents were provided by Roche
Diagnostics GmbH. The methods used were turbidimetry for CRP and
spectrophotometry for LDH. For PCT test, 1 ml of peripheral venous
blood was collected using an anticoagulant-free tube with separator
gel. This investigation was performed on a Cobas e411 device and
the reagents were provided by Roche Diagnostics GmbH. The method
used was ECLIA (immunochemistry with electrochemiluminescence
detection). The units of measurement for CRP was mg/l, for PCT
ng/ml and for LDH U/l.
Analyzed biological markers were harvested at
time-point 1 (t1) which means blood tests were collected in the
first hours after birth; and time-point 2 (t2) wich means blood
tests were collected during the 96 h of follow-up.
Statistical analysis
Data analyses were performed using the statistical
package (SPSS), version 23.0 (IBM, Corp.). Comparisons between
group means were analyzed using the ANOVA test. Pearson's
Chi-squared test was used for each separate variable. If Pearson's
Chi-squared test could not be used, the Fisher test was used. A
P-value of <0.05 was considered to indicate a statistically
significant difference.
Results
During the 3 years in which the study was performed
at the Neonatology Department of the ‘Louis Turcanu’ Emergency
Hospital for Children Timisoara, 2,191 newborns were admitted, of
which 78 met the inclusion criteria. Of these, 52.6% (n=41) were
female and 47.4% (n=37) were male. Regarding origin, 65.4% were
from urban areas and 34.6% from rural areas. 60.2% were premature
and 39.8% were full-term newborns. The average birth weight was
2,311 g. The average number of hospitalization days in the Neonatal
Intensive Care Unit was 23.8 days. The average number of
hospitalization days in the case of patients with a favorable
prognosis was 26.8 days, and in the case of patients with an
unfavorable prognosis was 9.7 days, these evolving to worse and
then to death in a relatively short period of time (Table I).
 | Table IBaseline characteristics of the
neonates (N=78). |
Table I
Baseline characteristics of the
neonates (N=78).
| Variables | Percentage % | |
|---|
| Sex |
|
Male | 47.4 | |
|
Female | 52.6 | |
| Origin |
|
Urban | 65.4 | |
|
Rural | 34.6 | |
| Birth status |
|
Full-term | 39.8 | |
|
Premature | 60.2 | |
| Average birth
weight | | 2,311 g |
| Average number of
hospitalization days for the entire group | | 23.8 days |
| Average number of
hospitalization days for favorable prognosis group | | 26.8 days |
| Average number of
hospitalization days for unfavorable prognosis group | | 9.7 days |
The classification of patients was made according to
prognosis. The prognosis was based on the following criteria: Birth
weight, biological markers obtained, the patient's evolution during
hospitalization and also the days of hospitalization in which they
needed therapy. Depending on these 4 criteria, patients were
considered to have a good or unfavorable prognosis. Patients with a
negative prognosis had a lower average birth weight of 2,192 g
compared to patients with a good prognosis, whose average was 2,338
g.
Therefore, at discharge from the hospital, the
patients status was as follows: 78.2% of patients were improved,
3.8% stationary, 1.3% aggravated and 16.7% were deceased. Depending
on this status, we divided the patients into two groups: 82.1% with
a favorable prognosis and 17.9% with an unfavorable prognosis.
Table II shows the
average values of the results of the biological investigations
gathered in the two groups under study and it can be seen that in
the case of patients with unfavorable evolution, hematological
parameters were lower and the average inflammatory sample was
higher than that recorded in the patients with a favorable
evolution.
| Table IIPrognosis according to the average
values of biological markers at t1. |
Table II
Prognosis according to the average
values of biological markers at t1.
| Favorable
prognosis |
|---|
| | Hb (g/dl) | LE (µl) | NE (µl) | LY (µl) | CRP (mg/l) | PCT (ng/ml) | LDH (U/l) |
|---|
| Mean | 17.09 | 18,955.00 | 10,046.17 | 4,565.10 | 2.71 | 5.35 | 754.43 |
| Std. error of
mean | 0.299 | 1,447.89 | 690.54 | 283.11 | 0.91 | 1.96 | 38.05 |
| Std. deviation | 2.39 | 11,583.14 | 4,734.12 | 1,981.80 | 7.23 | 13.34 | 304.40 |
| Unfavorable
prognosis |
| | Hb (g/dl) | LE (µl) | NE (µl) | LY (µl) | CRP (mg/l) | PCT (ng/ml) | LDH (U/l) |
| Mean | 14.90 | 15,947.85 | 10,823.64 | 4,208.33 | 8.10 | 9.1 | 1,235.42 |
| Std. error of
mean | 0.8224 | 1,719.48 | 1,382.61 | 508.46 | 4.62 | 3.8 | 255.32 |
| Std. deviation | 3.0771 | 6,433.71 | 4,585.60 | 1,761.37 | 17.29 | 13.8 | 955.33 |
Statistically significant differences were observed
between the average hemoglobin (Hb) values both at birth and in the
first 96 h between the two groups studied; patients with an
unfavorable prognosis having on average lower Hb values or a more
pronounced decrease in the first days of life (P<0.01) (Fig. 1).
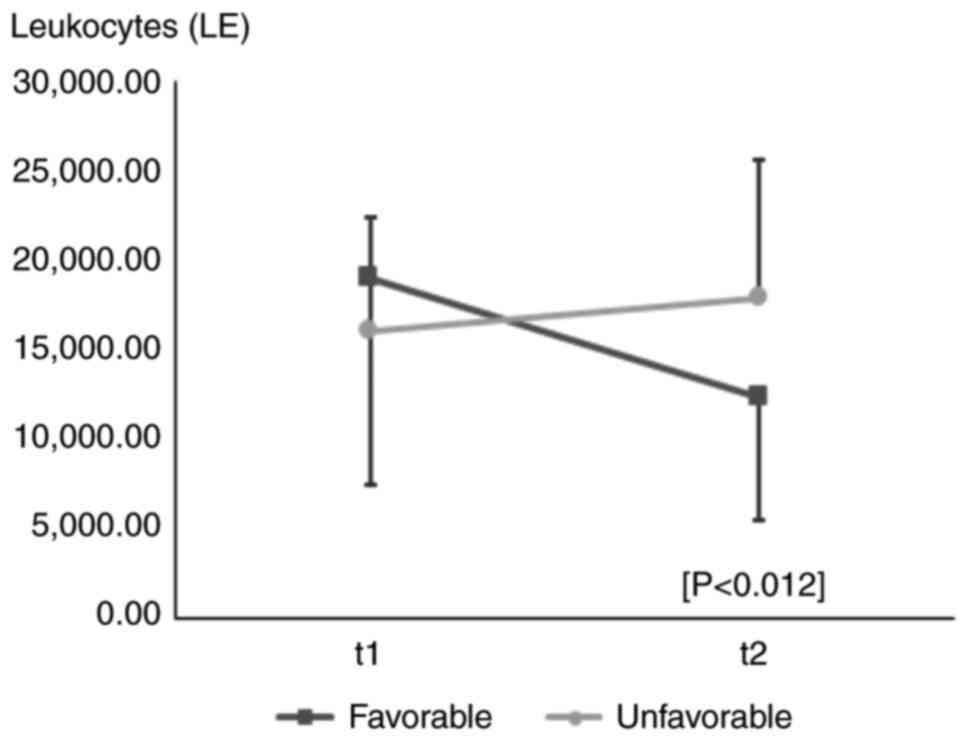
In the evolution of leukocytes (LE t2) (P<0.012),
it was observed that in the case of patients with a unfavorable
prognosis, LE values increased compared to birth values. The
average variation of the values in the evolution of LE shows that
in the case of patients with a favorable prognosis, LE values
decreased by an average of 6,688 µl and in the case of patients
with an unfavorable prognosis, LE values increased on average by
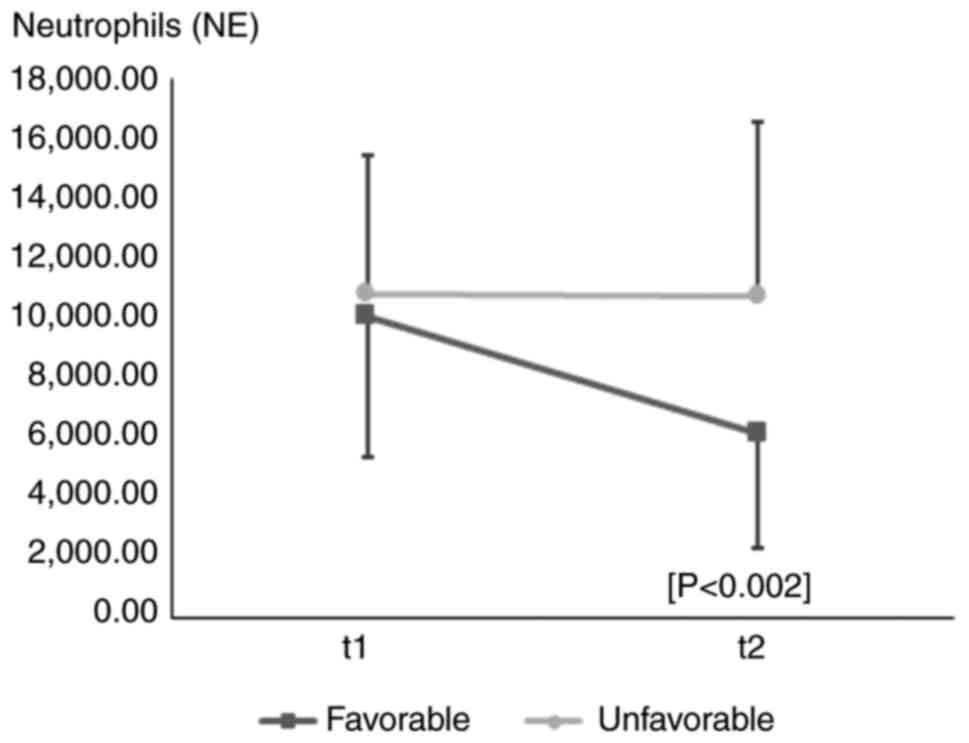
2,139 µl (Fig. 2). Regarding the
evolution of NE values (t2), it was observed that patients with a
favorable prognosis had a decreased evolution of NE compared to the
value determined in the first hours of life (t1), unlike patients
with an unfavorable prognosis, whose value had a slightly upward
trend (P<0.002) (Fig. 3).
No statistically high values or variations were
observed in LY values. In our study, the average LY values in the
two groups of patients was approximately equal in the first 24 h
and in evolution during the 96 h there was a slight decrease in
values in patients with favorable evolution and a stagnation of
values in the case of patients with unfavorable evolution (Table III).
| Table IIIEvolution of biological
parameters. |
Table III
Evolution of biological
parameters.
| Time | Prognosis | Mean Hb (g/dl) | Mean LY (µl) | Mean PCT (ng/ml) | Mean LDH (U/l) |
|---|
| t1 | Good | 17.09 | P<0.004 | 4,565.10 | 5.35 | 754.43 | P<0.001 |
| | Unfavorable | 14.90 | | 4,208.33 | 9.1 | 1,235.42 | |
| t2 | Good | 15.91 | P<0.001 | 3,345.00 | 6.8 | | |
| | Unfavorable | 12.93 | | 4,358.00 | 10.7 | | |
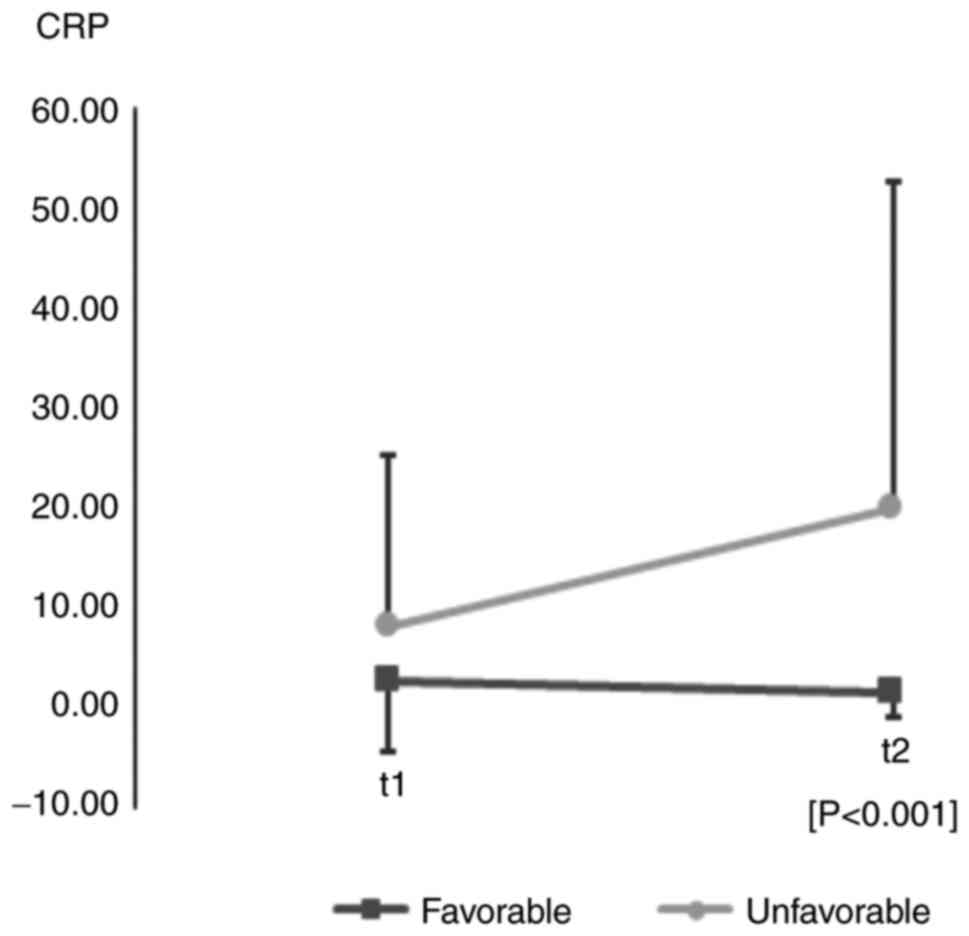
In the evolution of inflammatory parameters of the
CRP type (t2), variations with significant values (P<0.001) were
observed between the two groups studied; therefore, patients with a
favorable prognosis had an average CRP values of 1.5 mg/l and those
with an unfavorable prognosis-a value average of 19.82 mg/l
(Fig. 4).
Statistically significant differences were not
obtained in the case of PCT parameters. The average values (t1) in
the case of patients with a favorable prognosis was 5.3 ng/ml and
in the case of newborns with an unfavorable prognosis, it was 9.1
ng/ml. In t2 the average values of patients with a favorable
prognosis was 6.8 ng/ml and in the case of newborns with an
unfavorable prognosis, it was 10.7 ng/ml (Table III). However, it was observed that
72.8% of patients had PCT values above normal. Making an analysis
by risk groups, we observed that 71.7% of newborns with favorable
prognosis had values of PCT above normal and 84.6% of newborns with
unfavorable prognosis had PCT values above normal values.
In the newborns included in this study, it was
observed that 76.9% of them had LDH values higher than the upper
limit of normal values. With statistical significance (P<0.01),
we can say that in the group with favorable prognosis, 73.4% of the
newborns with HIE had LDH values above the maximum limit of normal,
their average being around 754.43 U/l. In the group with an
unfavorable prognosis, 92.8% of the newborns with HIE had high
values, the average value being 1,235.42 U/l (Table III).
Discussion
Oxygen delivery to the brain is directly
proportional to cerebral blood flow and arterial oxygen content
and, therefore, also to hemoglobin (Hb) levels. According to this
equation, a significant reduction in Hb may lead to decreased brain
oxygen delivery and eventually tissue hypoxia, if the compensatory
mechanisms aiming to keep a constant tissue oxygenation fail or are
overtaken (15). One of the causes
of moderate to severe perinatal asphyxia is perinatal anemia.
Earlier research demonstrated that a lower level of initial Hb was
a significant prognostic factor for abnormal neurodevelopmental
outcome in severely anemic asphyxiated infants (16).
Cerebral hypoxia-ischemia enhances rapid expression
of brain inflammatory cytokines and leads to an inflammatory cell
response to injury that includes neutrophils, lymphocytes, and
microglia (17). HIE was found not
to be correlated with an increase in inflammatory samples, such as
CRP, in all cases (18), which
corresponds to the findings of our study, where only 15.8% of
patients had elevated CRP values.
The observed hematological changes are attributable
to asphyxiation injury, not brain damage, which was also noted in
another study (19). It is possible
that increased nucleated red blood cell production in the immediate
neonatal state primarily reflects hypoxic injury (20).
Lymphocyte values in newborns have been shown to be
dependent on the duration of fetal bradycardia. Fetal bradycardia
exceeding 25 min resulted in an increase in the number of
lymphocytes, the values being relatively transient with rapid
normalization occurring between 18 and 24 h limiting its use as a
marker for asphyxia. This variation in lymphocyte count has been
attributed to a stress response that may originate in the thymus
(21).
One study conducted in term infants with HIE found
no correlation between lymphocyte number and outcome. Findings from
another study revealed that elevated peripheral neutrophils were
associated with worsened neurological outcome (22).
According to previous research as well as the
present study it was also observed that lactate dehydrogenase (LDH)
is a good predictor of HIE in the first 12/24 h after birth
(23). In a retrospective study,
serum LDH successfully predicted an abnormal mental or psychomotor
development index at 18 months of age in neonates with HIE
(24). This result is of clinical
interest providing a potential prognostic marker, inexpensive and
safe, in newborns with perinatal asphyxia. In addition, in a
previously study, Karlsson et al obtained 100% sensitivity
and 97% specificity in patients with HIE at a cut off level of 1049
U/l for LDH in the first 12 h after birth (6).
This retrospective study has several limitations.
Firstly, infant blood tests were collected in the first hours after
birth (t1), then during the 96 h of follow-up (t2), but were not
harvested at the same time in all patients.
Larger groups of patients are needed in order to be
able to say that the analysis of serum LDH has a high sensitivity
and specificity for nerve cell and brain damage, because we know
that LDH can be detectable in the cytoplasm of almost every cell in
the human body and it becomes extracellular upon cell death.
Considering its widespread presence in different types of tissues,
increased LDH levels have been reported in many pathological
conditions. LDH could be used as a biomarker of neuronal damage in
the first hours of life, but perhaps for greater accuracy, it would
be necessary to correlate with salivary LDH, which was not
performed in our study.
The etiology of neonatal anemia could not be
determined or well defined in some cases, here referring to
maternal causes that could induce neonatal anemia because not all
pregnancies were monitored by a gynecologist.
In conclusion, in patients with an unfavorable
prognosis, the mean hemoglobin values were lower or had a more
pronounced decrease in the first days of life. The values of
leukocytes and neutrophils increased in the first 96 h. A high
sensitivity of PCT was observed in newborns with hypoxic distress
and HIE. We can also conclude that LDH is a good predictor of HIE
in the first 12/24 h after birth.
Acknowledgements
Professional editing, linguistic and technical
assistance was performed by Irina Radu.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AIM and MB conceived and designed the study; AIM and
AMM collected the data. AMM and CMJ analyzed the data; AIM and CMJ
edited the figures and AIM, AMM and CMJ drafted the manuscript. MB
revised the manuscript critically for important intellectual
content. All authors contributed to the data interpretation and
approved the submitted version.
Ethics approval and consent to
participate
Approval of the local ethics committee (Ethics
Committee for Scientific Research of the Emergency Hospital for
Children ‘Louis Turcanu’/approval no. 76/2020) was obtained prior
to starting the study. Parental or caregiver consent was obtained
where applicable. This publication and the database does not
contain personal data, does not compromise anonymity or
confidentiality or breach local data protection laws.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Douglas-Escobar M and Weiss MD:
Hypoxic-Ischemic Encephalopathy A review for the Clinician. JAMA
Pediatr. 169:397–403. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Chaparro-Huerta V, Flores-Soto ME, Merin
Sigala ME, Barrera de León JC, Lemus-Varela M de L, Torres-Mendoza
BM de G and Beas-Zárate C: Proinflammatory cytokines, enolase and
S-100 as early biochemical indicators of hypoxic-ischemic
encephalopathy following perinatal asphyxia in newborns. Pediatr
Neonatol. 58:70–76. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Allen KA and Brandon DH: Hypoxic ischemic
encephalopathy: Pathophysiology and experimental treatments.
Newborn Infant Nurs Rev. 11:125–133. 2011.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Serban D, Anton E, Chirita R, Bild V,
Ciobica A, Alexinschi O, Arcan O, Popescu R, Paduraru L and Timofte
D: Current aspects of the interactions between dementia, the brain
renin-angiotensin system and oxidative stress. Arch Biol Sci.
67:903–907. 2015.
|
|
5
|
Yıldız EP, Ekici B and Tatlı B: Neonatal
hypoxic ischemic encephalopathy: An update on disease pathogenesis
and treatment. Expert Rev Neurother. 17:449–459. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Karlsson M, Wiberg-Itzel E, Chakkarapani
E, Blennow M, Winbladh B and Thoresen M: Lactate dehydrogenase
predicts hypoxic ischaemic encephalopathy in newborn infants: A
preliminary study. Acta Paediatr. 99:1139–1144. 2010.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hayes BC, Doherty E, Grehan A, Madigan C,
McGarvey C, Mulavany S, Geary M, Matthews TG and King MD: Are serum
markers of liver and muscle injury useful in neonatal
hypoxic-ischemic encephalopathy? J Neonatal Perinatal Med.
5:305–310. 2012.
|
|
8
|
Reddy S, Dutta S and Narang A: Evaluation
of lactate dehydrogenase, creatine kinase and hepatic enzymes for
the retrospective diagnosis of perinatal asphyxia among sick
neonates. Indian Pediatr. 45:144–147. 2008.PubMed/NCBI
|
|
9
|
Jahan R, Khanam A, Masood A and Rehman R:
Diagnostic accuracy of lactate dehydrogenase for diagnosis of
perinatal asphyxia in neonates with non-reactive CTG. Pak J Med
Heal Sci. 13:458–460. 2019.
|
|
10
|
Yilmaz G, Arumugam TV, Stokes KY and
Granger DN: Role of T lymphocytes and interferon-gamma in ischemic
stroke. Circulation. 113:2105–2112. 2006.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zarbock A and Ley K: Mechanisms and
consequences of neutrophil interaction with the endothelium. Am J
Pathol. 172:1–7. 2008.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Liu F and Mccullough LD: Inflammatory
responses in hypoxic ischemic encephalopathy. Acta Pharmacol Sin.
34:1121–1130. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Christensen RD, Baer VL, Gordon PV, Henry
E, Whitaker C, Andres RL and Bennett ST: Reference ranges for
lymphocyte counts of neonates: Associations between abnormal counts
and outcomes. Pediatrics. 129:e1165–e1172. 2012.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Morkos AA, Hopper AO, Deming DD, Yellon
SM, Wycliffe N, Ashwal S, Sowers LC, Peverini RL and Angeles DM:
Elevated total peripheral leukocyte count may identify risk for
neurological disability in asphyxiated term neonates. J Perinatol.
27:365–370. 2007.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Lelubre C, Bouzat P, Crippa IA and Taccone
FS: Anemia management after acute brain injury. Crit Care.
20(152)2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kalteren WS, Ter Horst HJ, den Heijer AE,
de Vetten L, Kooi EMW and Bos AF: Perinatal anemia is associated
with neonatal and neurodevelopmental outcomes in infants with
moderate to severe perinatal asphyxia. Neonatology. 114:315–322.
2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Alsulaimani AA, Abuelsaad AS and Mohamed
NM: Inflammatory cytokines in neonatal hypoxic ischemic
encephalopathy and their correlation with brain marker S100
protein: A case control study in Saudi Arabia. J Clin Cell Immunol.
6:1–8. 2015.
|
|
18
|
Saito J, Shibasaki J, Shimokaze T,
Kishigami M, Ohyama M, Hoshino R, Toyoshima K and Itani Y: Temporal
relationship between serum levels of interleukin-6 and C-reactive
protein in therapeutic hypothermia for neonatal hypoxic-ischemic
encephalopathy. Am J Perinatol. 33:1401–1406. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Shah V, Beyene J, Shah P and Perlman M:
Association between hematologic findings and brain injury due to
neonatal hypoxic-ischemic encephalopathy. Am J Perinatol.
26:295–302. 2009.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Vandana V, Amit V, Meena V, Anuradha B,
Vivek B, Deepak V and Salone MR: Study of basic biochemical and
haematological parameters in perinatal asphyxia and its correlation
with hypoxic ischemic encephalopathy (HIE) Staging. J Adv Res Biol
Sci. 3:79–85. 2011.
|
|
21
|
Dina P and Muraskas JK: Hematologic
changes in newborns with neonatal encephalopathy. Neoreviews.
19:e29–e33. 2018.
|
|
22
|
Povroznik JM, Engler-Chiurazzi EB,
Nanavati T and Pergami P: Absolute lymphocyte and neutrophil counts
in neonatal ischemic brain injury. SAGE Open Med.
6(2050312117752613)2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Yum SK, Moon CJ, Youn YA and Sung IK:
Changes in lactate dehydrogenase are associated with central gray
matter lesions in newborns with hypoxic-ischemic encephalopathy. J
Matern Neonatal Med. 30:1177–1181. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Mehta A, Chawla D, Kaur J, Mahajan V and
Guglani V: Salivary lactate dehydrogenase levels can provide early
diagnosis of hypoxic-ischaemic encephalopathy in neonates with
birth asphyxia. Acta Paediatr. 104:e236–e240. 2015.PubMed/NCBI View Article : Google Scholar
|