1. Introduction
Breast cancer remains the most common cause of
morbidity and mortality by cancer in females worldwide (1,2).
During the last decade (2005-2015), the number of cases of breast
cancer increased by 35% worldwide, and approximately one-fifth of
this increase was due to an increase in incidence rates (2). Notably, the breast cancer incidence
(age standardized rate) decreased only in countries with a high
social development index (SDI), while it increased in all the other
countries (2). In regard to
mortality, the worldwide number of deaths increased by 21%, but the
age-standardized death rate declined globally by 6% (3). The decline in mortality was seen
especially in high SDI and high middle SDI countries (3-6).
Worldwide, 2,088,849 new cases and 626,679 deaths
due to breast cancer were estimated as occurring in 2018 by the
International Agency for Research on Cancer and World Health
Organization, with this disease accounting for 24% of all new cases
of cancer and 15% of all cancer-related deaths in females (7). In Europe, for the same year, same
source, 522,513 new cases and 137,707 deaths due to breast cancer
were estimated to occur in females, these representing 26.4% of all
cancers and 16% of cancer-related deaths in this region (7). Thus, in 2018, Europe possessed 23% of
all breast cancer cases in the world and 21% of deaths, although it
has only 10% of the world female population.
Despite its extensive impact on public health
worldwide, breast cancer is largely preventable through healthy
lifestyle, specific high-risk strategies for non-modifiable risks
and early detection (8-11).
Breast cancer screening through mammography is largely recommended
worldwide, and contributions of 20-40% to a reduction in mortality
were revealed by different studies (10,12-16).
In the European Union (EU), high quality population
screening through mammography in women aged 50-69 years has been
recognized as a priority for action (together with screening for
cervix and colon cancer) since 2003(17). Two assessments of the implementation
for this recommendation have been performed. The first (2008)
revealed that 11 countries had population-based screening programs
for cancer screening (18). The
second assessment found a notable progress in improving access to
breast cancer screening, with 79% of the eligible women covered by
invitation to screening and 49% covered by examination (19). However, wide variations in access to
screening for breast cancer, as well as in incidence and mortality
for this disease still persist in the EU, and generally, women in
more socio-economically deprived areas have lower access to
screening, lower breast cancer incidence, but higher mortality
rates (19-22).
This statistical review aimed to investigate the
breast cancer-related health gaps in Romanian women compared to the
average EU female population after 10 years of accession. We
focused on breast cancer mortality indicators: Breast cancer
deaths, age standardized mortality rates, life expectancy at birth
and contribution of breast cancer to life expectancy.
2. Statistical collection methods
The study interval was 2007-2016, 2007 being the
year of accession of Romania to the EU. The study populations were
represented by the female population of Romania and EU 27 (the 27
EU countries excluding the UK since 2020), respectively.
Breast cancer-related deaths were considered
following the code C50 of the International Classification of
Diseases Revision 10 (ICD-10), which is used in the country at
present (23). They were analyzed
as percentage change compared to deaths from 2007 for both Romania
and EU. We also compared changes in breast cancer deaths with
changes in deaths for all cancer (C00-C97) and all causes of deaths
(A00-Y89, excluding S00-T98) (24).
The annual standardized mortality rates were
compared as trend and percentage change over 10 years among the two
populations. For understanding the breast cancer situation, we
followed also the deaths for all causes and all cancer-related
deaths.
Life expectancy at birth was compared as trend and
percentage change. Contribution of breast cancer to life expectancy
was calculated only for Romania.
All the data were extracted from Eurostat database
(deaths by different ICD codes, age standardized mortality rates,
life expectancy, population by age-group) (24). The contribution of breast cancer to
life expectancy was calculated using the abridged life table for
five-year age groups (24,25).
Morbidity indicators (incident cases/rates) were not
considered due to the fact that routine reporting of morbidity is
fragmentary, and the country does not have a national functional
registry for breast cancer.
3. Results of the statistical analysis
Country context
Romania experienced a delay in implementing an
organized population screening for breast cancer compared to other
EU members. The country accessed the EU in 2007 and at that moment,
a breast cancer screening was under planning (18). In 2017, a breast cancer screening
was under piloting as a small-scale project (19). Some attempts to provide free access
to mammography screening for women of eligible age were envisaged,
either as service included in the basic health package of services,
or in the framework of some projects, but the impact of these
measures was very low, once that 79% of the Romanian women report
they never had a breast X-ray examination (20).
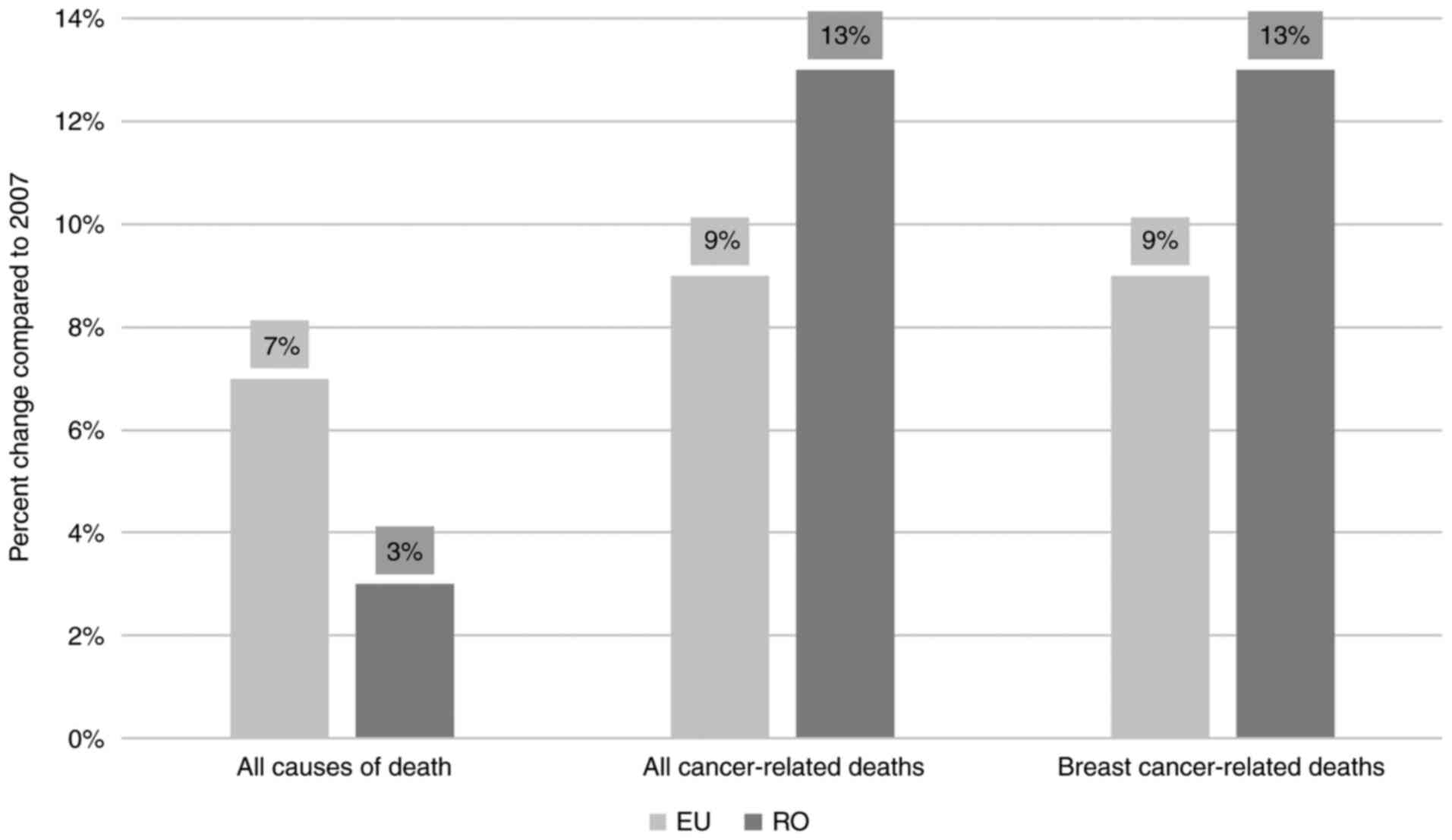
Changes in the number of deaths
In 2007, in the EU 27 female population, there were
a registered 2,121,906 deaths of all causes, 468,044 deaths due to
all cancers and 77,743 deaths due to breast cancer. In Romania, in
the same year, 118,560 deaths from all causes, 18,491 deaths due to
all cancers and 3,049 deaths due to breast cancer were registered.
After 10 years, the annual deaths from all causes in the EU
increased by 7%; meanwhile the number of deaths due to all cancers
and the number of deaths due to breast cancer increased by 9% each
(Fig. 1). Romania had only 3%
increase of the annual deaths of all causes in 2016 compared to
2007, but the deaths due to all cancers and the breast
cancer-related deaths increased by 13%, compared to 2007 (Fig. 1).
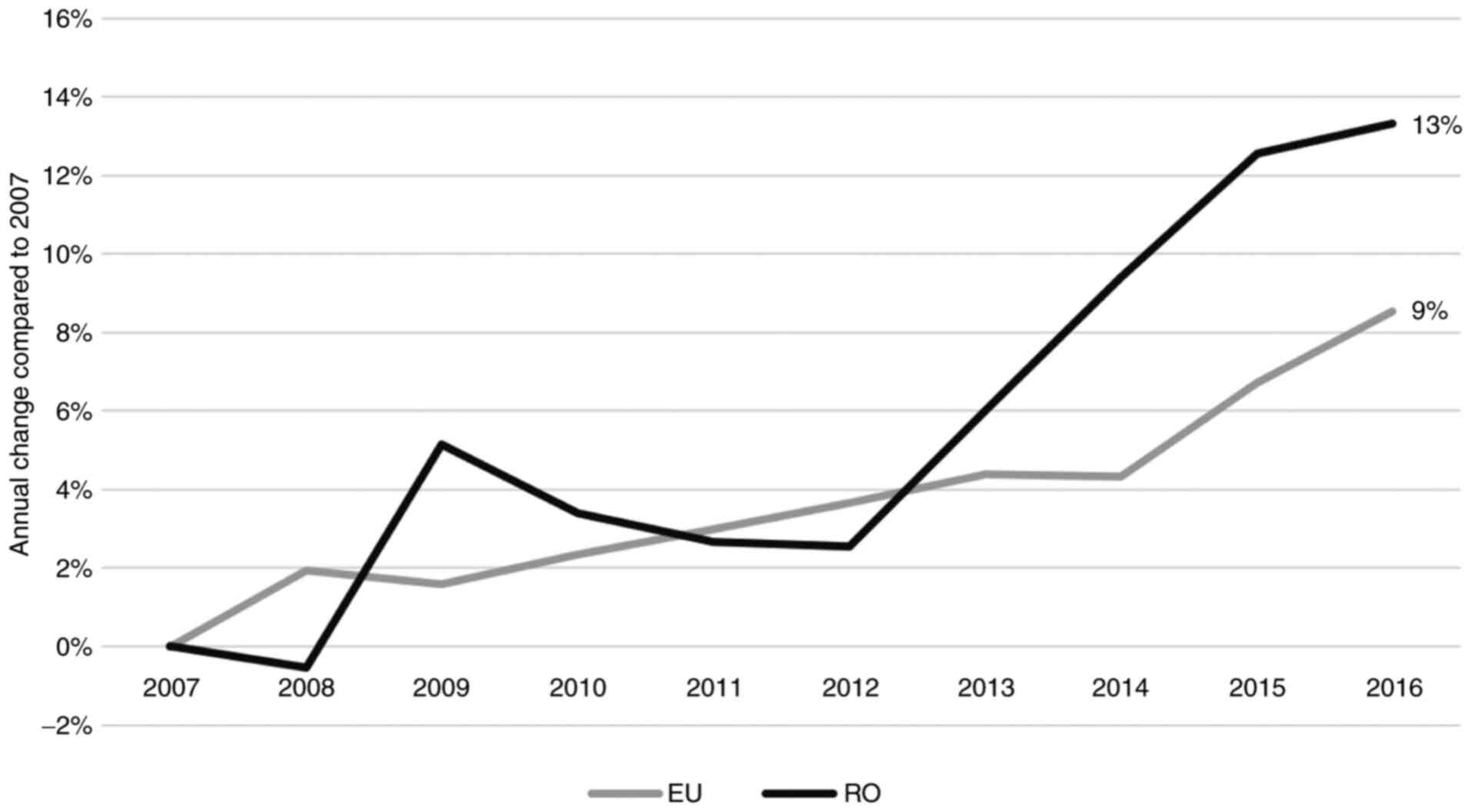
The annual change in breast cancer-related deaths in
EU was slightly upward, reaching 9% in 2016; meanwhile in Romania
there were higher variations and an obvious worsening after 2012
(Fig. 2).
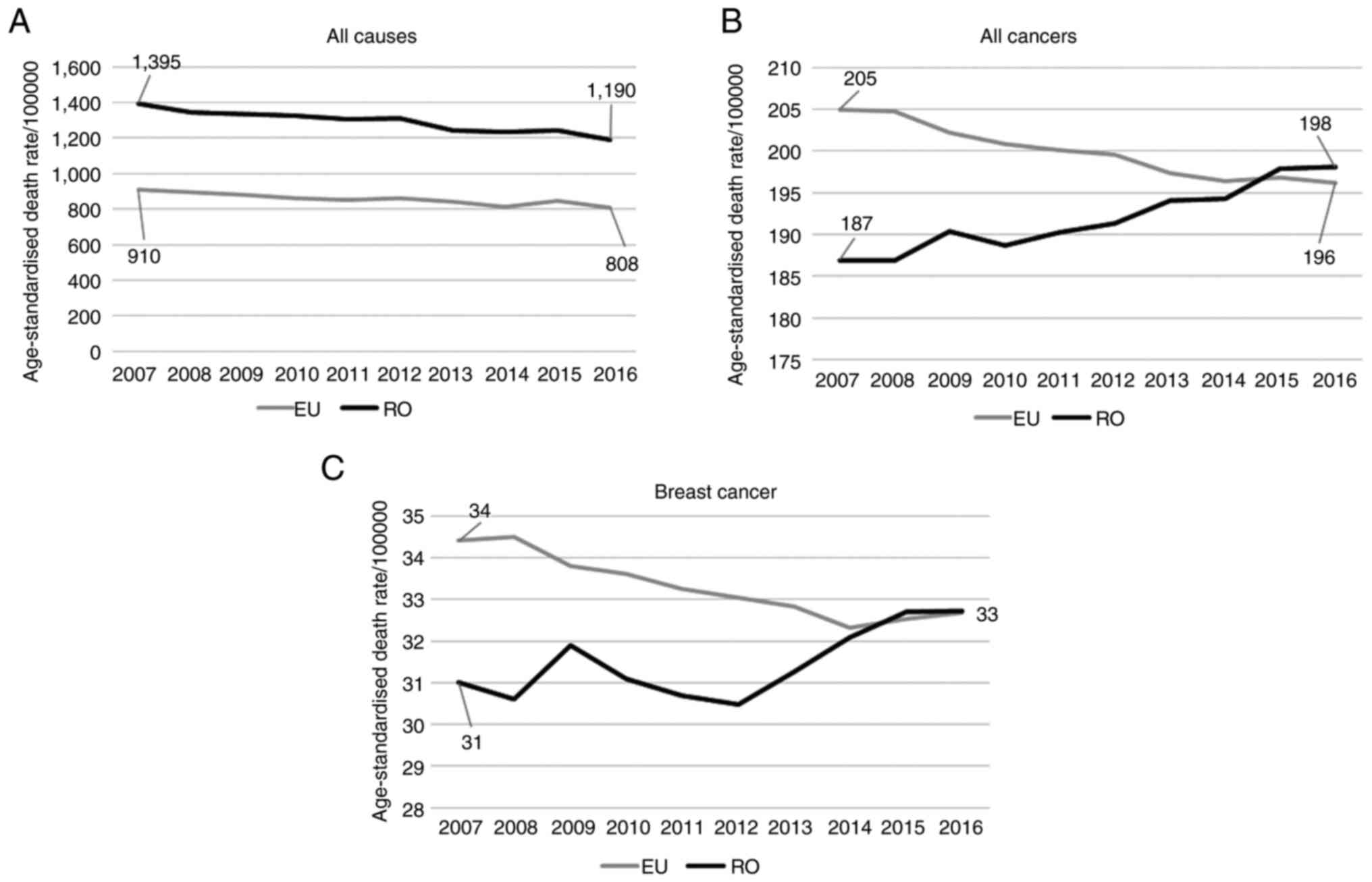
Changes in the age-standardized
mortality rate
The age-standardized mortality rates for all causes
had similar, slightly decreasing and almost parallel trends in the
EU and Romania, with Romania starting the beginning of the interval
with a much higher value compared to the EU (1,395 deaths/100,000
inhabitants, compared to 910 in the EU) (Fig. 3A). At the end of the study interval,
the mortality in Romania decreased by 15% while mortality in the EU
decreased by 11%. In 2016, mortality due to all causes in Romania
was 47% higher compared to the EU.
The mortality of all cancers had divergent trends in
Romania and EU (Fig. 3B). Romania
started at the beginning of the study period with a 9% lower
mortality of all cancers compared to EU, but it had an increasing
trend, while the mortality due to all cancers in the EU decreased
progressively in the interval. Overall, the all cancer mortality
rate in Romania increased by 6% and that of EU decreased by 4%. In
2016, the mortality in Romania was 1% higher compared to the
EU.
Breast cancer-related mortality had also divergent
trends, with a constant decline in the EU, but an irregular,
increasing course for Romania (Fig.
3C). In 2007, the mortality in Romania was 9% lower compared
than the EU, but in 2016, all the advantage that Romania apparently
had at the beginning of the interval was lost, both populations
reaching the same mortality rate. Overall, we found an increase of
6% in Romania and a decrease by 5% in EU. The increasing trend of
breast cancer mortality in Romania has been underlined also in the
precedent decade (26). It is
assumed that it will continue in the future and this will widen the
health gap compared to the EU.
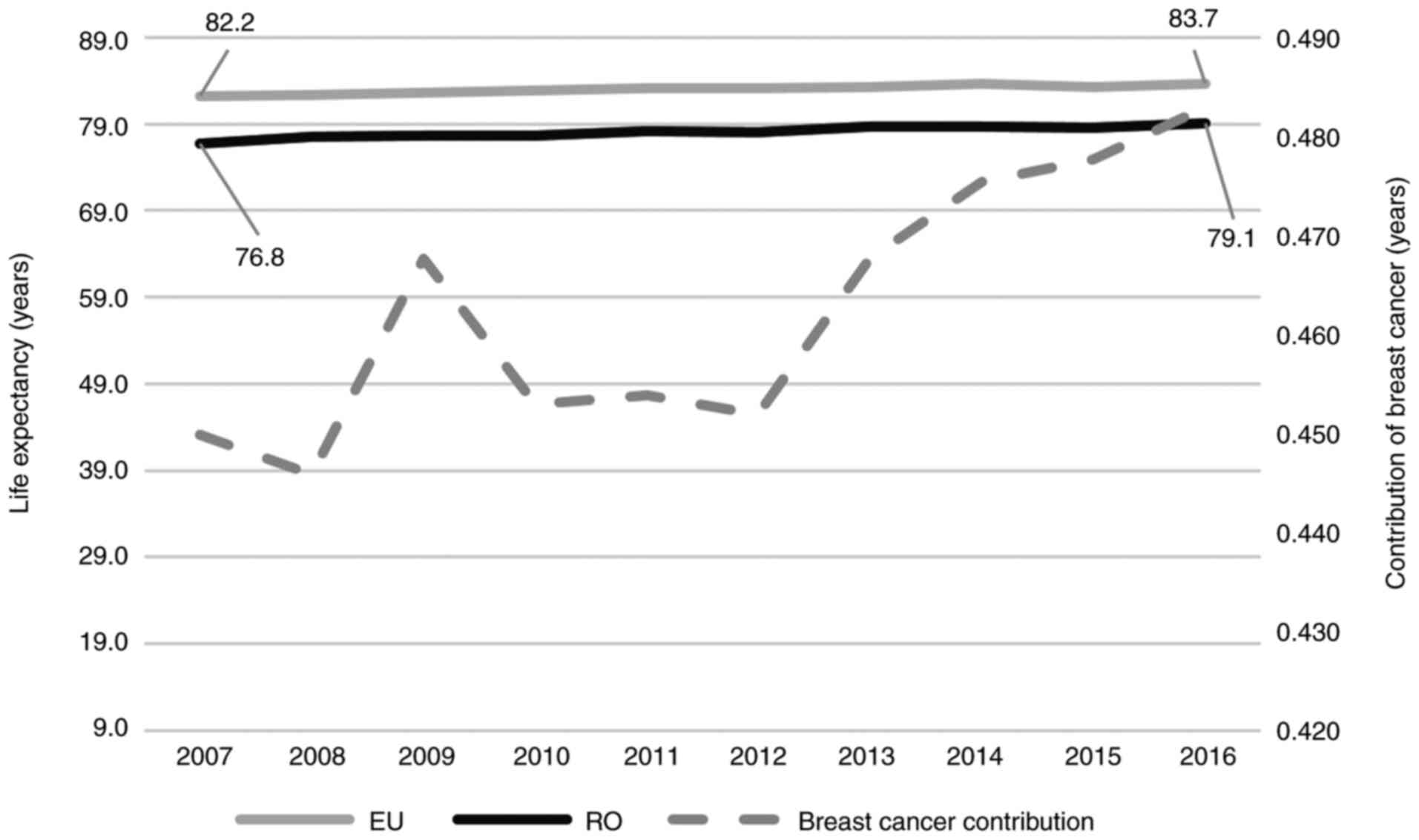
Changes in life expectancy at
birth
In 2007, Romanian females had one of the lowest life
expectancies at birth of 76.8 years among all EU members, with 5.4
year gap compared to the EU average. A slight increasing trend was
found for both Romania and EU, with a small reduction in the gap
(Fig. 4). Thus, at the end of the
interval, life expectancy at birth increased by 3 and 2% in Romania
and the EU, respectively, and the gap reached 4.8 years.
The contribution of breast cancer to the reduction
in life expectancy at birth reached 0.45 years in 2007 and
increased slowly to 0.48 years in 2016.
4. Discussion
At present, the access to breast screening
mammography in Romanian women is fragmentary, often imposing
out-of-pocket payment for the investigation. No population
screening has been organized to date, despite some attempts to
include mammography screening in the national health programs or to
some pilot projects that have been implemented, in conformity of
Order of the Health Minister and of the president of the National
Health Insurance House no 574/269/2008 regarding the implementing
norms for the national health programs (27-36).
Therefore, a small section of the female population in Romania
regularly undergoes clinical and imaging examinations, in the
context of which in Romania breast cancer is the first cause of
cancer-related death in females, with a long gap to colon or lung
cancer.
The situation in Romania is not particular, as
evidence suggests that access to organized screening programs for
breast cancer is more restricted in Eastern Europe, compared to the
rest of the continent, despite the fact that organized mammography
screening reduces the mortality due to breast cancer (20,37,38).
Moreover, countries from Eastern Europe have more limited
capacities for organizing population screening and usually lack the
high-quality data for measuring the occurrence of breast cancer
(38).
In Romania, breast cancer represents the main cause
of cancer-related mortality in females, presenting an increased
number over the years and a constant proportion of 16% of all
cancer-related deaths. The mortality model is worsening, and this
increased the health gap compared to the EU female population. All
of these facts represent urgent reasons for acting for planning and
implementing an organized, population-based screening.
As an EU member, Romania has been concerned in the
last decade about the need for implementing a population-based
breast cancer screening. Opportunities for developing such a
program have been prioritized in the Partnership Agreement with EU
for 2014-2020(39). Under this
framework, an important project for developing breast cancer
screening is planned: ‘Operational Program Human Capital (project
no. 120799) (40). Increasing the
institutional capacity and professional competencies of health
system specialists is needed in order to implement the National
Breast Cancer Screening Program. In its first phase, this project
aims to build capacity in the country by creating a reference
center for regional breast cancer screening programs, by developing
a national standardized methodology for prevention, early
detection, diagnosis and early treatment of breast cancer, in
accordance with European guidelines, and by providing training for
the medical workforce (40).
Increase in awareness of the general population and vulnerable
groups for attending the breast cancer screening is also a priority
objective, in the context in which information campaigns for
screening programs lacking in Romania are up to date (38). The second phase of the project is
under preparation and there is expected to provide breast screening
in four regions of the country, targeting a minimum of 30,000 women
aged 50-69 years, with a focus on vulnerable groups: Operational
Program Human Capital Applicants Guideline ‘Be responsible for your
health-regional programs for prevention, early detection, diagnosis
and early treatment for breast cancer-phase 2’ (41).
This project is essential in the existing country
context and there is expected that, after its successful
implementation (planned to end in 2023), breast screening will be
provided throughout the country. However, about three million women
aged 50-69 years live in Romania at present according to Eurostat
database (24). If we consider only
this age-group for mammography screening, and only one examination
every three years for each woman, which is below the European
Guideline, the project will cover around 1% of the eligible
population. This means that more efforts and resources should be
concentrated to organize a population breast cancer screening in
Romania in the next years, in order to speed up the process of
ensuring proper access for all eligible women, on ethical premises,
and also to slow the upward trend of breast cancer-related
mortality.
5. Conclusions
Breast cancer represents an important public health
issue in Romania, through the trend in the increasing number of
deaths and mortality in the last decade and through its
contribution to lower life expectancy. The absence of an organized
population screening in the country will aggravate the gap in
breast cancer mortality between Romania and the EU in the near
future.
Romania has concrete and consistent opportunities to
develop a population screening for breast cancer in the upcoming
years. These opportunities seem to be relevant, but far from
sufficient for covering the eligible population on short-term
basis. More efforts and resources should be concentrated in the
next years in order to ensure universal access to breast screening
for eligible women, and to control the gap in health status between
Romania and the EU.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from Eurostat and the National Institute of
Statistics, Bucharest, Romania, on reasonable request.
Authors' contributions
FF, REB and CSP collected and analyzed the data
regarding the breast cancer mortality in Romania compared with the
EU. FF, REB, CSP, TAG and OM made substantial contribution to the
conception of the work and interpretation of data; in addition,
they drafted the manuscript and were major contributors in writing
the manuscript. SV and AN made substantial contributed to the
design of the work, further drafts and comments. FF and REB
performed statistical analysis and study description. All authors
read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not required due to the statistical analysis nature
of the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Azamjah N, Soltan-Zadeh Y and Zayeri F:
Global trend of breast cancer mortality rate: A 25-year study.
Asian Pac J Cancer Prev. 20:2015–2020. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Global Burden of Disease Cancer
Collaboration. Fitzmaurice C, Allen C, Barber RM, Barregard L,
Bhutta ZA, Brenner H, Dicker DJ, Chimed-Orchir O, Dandona R, et al:
Global, regional, and national cancer incidence, mortality, years
of life lost, years lived with disability, and disability-adjusted
life-years for 32 cancer groups, 1990 to 2015: A systematic
analysis for the global burden of disease study. JAMA Oncol.
3:524–548. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
GBD 2015 Disease and Injury Incidence and
Prevalence Collaborators. Global, regional, and national incidence,
prevalence, and years lived with disability for 310 diseases and
injuries, 1990-2015: A systematic analysis for the Global Burden of
Disease Study 2015. Lancet. 388:1545–1602. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Ying W, Yi Z, Zhen Z, Qian H, Dingli S,
Dai Z, Huafeng K and Zhijun D: Global burden of breast cancer and
attributable risk factors in 195 countries and territories, from
1990 to 2017: Results from the Global Burden of Disease Study 2017.
J Hematol Oncol. 12(140)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Longfei L, Lei Y, Yuling L, Fang Y, Hui Li
and Jian N: Incidence and death in 29 cancer groups in 2017 and
trend analysis from 1990 to 2017 from the Global Burden of Disease
Study. J Hematol Oncol. 12(96)2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sharma R: Breast cancer incidence,
mortality and mortality-to-incidence ratio (MIR) are associated
with human development, 1990-2016: Evidence from Global burden of
disease study 2016. Breast Cancer. 26:428–445. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
International Agency for Research on
Cancer and World Health Organization. Global Cancer Observatory.
Cancer today. Available from: https://gco.iarc.fr// (accessed on 23 Oct, 2020).
|
|
8
|
Lacey JV Jr, Kreimer AR, Buys SS, Marcus
PM, Chang SC, Leitzmann MF, Hoover RN, Prorok PC, Berg CD and
Hartge P: Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer
Screening Trial Project Team. Breast cancer epidemiology according
to recognized breast cancer risk factors in the Prostate, Lung,
Colorectal and Ovarian (PLCO) Cancer Screening Trial Cohort. BMC
Cancer. 9(84)2009.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Marmot MG, Altman DG, Cameron DA, Dewar
JA, Thompson SG and Wilcox M: The benefits and harms of breast
cancer screening: An independent review. Br J Cancer.
108:2205–2240. 2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
International Agency for Research on
Cancer: IARC Handbooks of Cancer Prevention. Volume 15: Breast
Cancer Screening. IARC Press, Lyon, 2015.
|
|
11
|
Dimitrova N, Saz PZE, Bramesfeld A,
Ulutürk A, Bocchi G, López-Alcalde J, Pylkkanen L, Neamțiu L,
Ambrosio M, Deandrea S and Lerda D: European guidelines for breast
cancer screening and diagnosis-the European Breast Guidelines. EUR
28360 EN doi:10.2788/503032. 2016.
|
|
12
|
Independent UK Panel on Breast Cancer
Screening. The benefits and harms of breast cancer screening: An
independent review. Lancet. 380:1778–1786. 2012.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Monticciolo DL: Current guidelines and
gaps in breast cancer screening. J Am Coll Radiol. 17:1269–1275.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Beau AB, Andersen PK, Vejborg I and Lynge
E: Limitations in the effect of screening on breast cancer
mortality. J Clin Oncol. 36:2988–2994. 2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Olsen AH, Lynge E, Njor SH, Merethe K,
Marit W, Tonje B and Eiliv L: Breast cancer mortality in Norway
after the introduction of mammography screening. Int J Cancer.
132:208–214. 2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Peintinger F: National breast screening
programs across Europe. Breast Care (Basel). 14:354–358.
2019.PubMed/NCBI View Article : Google Scholar
|
|
17
|
European Council. Council recommendation
of 2 December 2003 on cancer screening (2003/878/EC). Off J Eur
Union. 327:34–38. 2003.
|
|
18
|
Von Karsa L, Anttila A, Ronco GL, Ponti A,
Malila N, Arbyn M, Segnan N, Castillo-Beltran M, Boniol M, Ferlay
J, et al: Cancer screening in the European Union. Report on the
implementation of the Council Recommendation on cancer screening.
First report. Brussels: European Commission; 2008. https://eur-lex.europa.eu/legal-content/en/ALL/?uri=CELEX%3A52008DC0882.
|
|
19
|
Ponti A, Anttila A, Ronco G and Senore C:
Cancer Screening in the European Union. Report on the
implementation of Council Recommendation on Cancer Screening.
Brussels: European Commission; 2017. https://screening.iarc.fr/EUreport.php.
|
|
20
|
Smith D, Thomson K, Bambra C and Todd A:
The breast cancer paradox: A systematic review of the association
between area-level deprivation and breast cancer screening uptake
in Europe. Cancer Epidemiol. 60:77–85. 2019.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Levi F, Lucchini E, Negri C and Vecchia L:
Trends in mortality from major cancers in the European Union,
including acceding countries, in 2004. Cancer. 101:2843–2850.
2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Deandrea S, Molina-Barceló A, Uluturk A,
Moreno J, Neamtiu L, Peiró-Pérez R, Saz-Parkinson Z, Lopez-Alcalde
J, Lerda D and Salas D: Presence, characteristics and equity of
access to breast cancer screening programmes in 27 European
countries in 2010 and 2014. Results from an international survey.
Prev Med. 91:250–263. 2016.PubMed/NCBI View Article : Google Scholar
|
|
23
|
World Health Organization. International
Statistical Classification of Diseases and Related Health Problems.
10th Revision. Volume 2. Instruction manual, 1-174, 2010.
|
|
24
|
Eurostat database. Population and social
condition. Health status. https://ec.europa.eu/eurostat/data/database//
(accessed on 23 Oct, 20).
|
|
25
|
Chiang Chin Long: Life Table and mortality
analysis. World Health Organization Geneva. 1978. https://apps.who.int/iris/bitstream/handle/10665/62916/15736_eng.pdf.
|
|
26
|
Tereanu C, Baili P, Berrino F, Micheli A,
Furtunescu FL, Minca DG and Sant M: Recent trends of cancer
mortality in Romanian adults: Mortality is still increasing,
although young adults do better than the middle-aged and elderly
population. Eur J Cancer Prev. 22:199–209. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Bohîlțea RE, Turcan G, Cîrstoiu MM,
Ionescu C, Nemescu D, Turcan N and Vladareanu R: Clinical
implementation of ultrasound gynecological examination report
(software REGU) based on international consensuses of tumor study
groups. Filodiritto editore-proceedings. 5th Romanian congress of
the Romanian society of ultrasound in obstetrics And Gynecology:
99-104, 2017.
|
|
28
|
Badea M, Baros A, Bohiltea RE, Julea IE,
Furtunescu F, Istrate-Ofiteru AM, Iovan L, Cirstoiu MM, Burcin MR,
Turcan N, et al: Modern interdisciplinary monitoring of cervical
cancer risk. Rom J Morphol Embryol. 60:469–478. 2019.PubMed/NCBI
|
|
29
|
Tataru AL, Furau G, Afilon J, Ionescu C,
Dimitriu M, Bratu OG, Tit DM, Bungau S and Furau C: The situation
of cervical cancers in the context of female genital cancer
clustering and burden of disease in Arad County, Romania. J Clin
Med. 8(96)2019.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Iorga RA, Bratu OG, Marcu RD, Constantin
T, Mischianu DLD, Socea B, Gaman MA and Diaconu CC: Venous
thromboembolism in cancer patients: Still looking for answers
(Review). Exp Ther Med. 18:5026–5032. 2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Miricescu D, Diaconu CC, Stefani C,
Stanescu AMA, Totan A, Rusu IR, Bratu OG, Spinu D and Greabu M: The
serine/threonine protein kinase (Akt)/protein kinase B (PkB)
signaling pathway in breast cancer. J Mind Med Sci. 7:34–39.
2020.
|
|
32
|
Ionescu CA, Matei A, Navolan D, Dimitriu
M, Bohîltea R, Neacsu A, Ilinca C and Ples L: Correlation of
ultrasound features and the risk of ovarian malignancy algorithm
score for different histopathological subtypes of benign adnexal
masses. Medicine. 97(e11762)2018.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bohîlțea RE, Ancăr V, Cîrstoiu M, Rădoi V,
Bohiltea LC and Furtunescu F: Project for the National program of
early diagnosis of endometrial cancer part I. J Med Life.
8:305–314. 2015.PubMed/NCBI
|
|
34
|
Bohîlțea RE, Ancăr V, Rădoi V, Furtunescu
F and Bohiltea LC: Project for the National program of early
diagnosis of endometrial cancer part II. J Med Life. 8:423–431.
2015.PubMed/NCBI
|
|
35
|
Bohîlțea RE, Furtunescu F, Dosius M,
Cîrstoiu M, Radoi V, Baros A and Bohiltea LC: Evaluation of
endometrial cancer epidemiology in Romania. J Med Life. 8:218–225.
2015.PubMed/NCBI
|
|
36
|
Bohîlțea RE, Sajin M, Furtunescu F,
Bohiltea LC, Mihart A, Baros A and Anca AF: Clinical and
pathological correlations in endometrial pathology. J Med Life.
8:552–562. 2015.PubMed/NCBI
|
|
37
|
Zielonke N, Gini A, Jansen EEL, Anttila A,
Segnan N, Ponti A, Veerus P, de Koning HJ, van Ravesteyn NT and
Heijnsdijka EAM: EU-TOPIA consortium. Evidence for reducing
cancer-specific mortality due to screening for breast cancer in
Europe: A systematic review. Eur J Cancer. 127:191–206.
2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Altobelli E, Rapacchietta L, Angeletti PM,
Barbante L, Profeta FV and Fagnano R: Breast cancer screening
programmes across the WHO European Region: Differences among
countries based on national income level. Int J Environ Res Public
Health. 14(452)2017.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Partnership Agreement Romania
2014RO16M8PA001.1.2. https://www.fonduri-ue.ro/acord-parteneriat#varianta-%C3%AEn-englez%C4%83.
|
|
40
|
Oncologic Institute ‘Prof Dr I Chiricuta’
Cluj Napoca. Project 120799 ‘Increasing the institutional capacity
and professional competencies of health system specialists in order
to implement the National Breast Cancer Screening Program.
http://www.iocn.ro/Noutati/-Publicatii-proiect-POCU-Etapa-I-Cresterea-capacitatii-institutionale-si-a-competentelor-profesionale-ale-specialistilor-din-sistemul-de-sanatate-in-scopul-implementarii-Programului-National-de-screening-pentru-cancerul-de-san-120799-eID967.html.
|
|
41
|
Ministry of the European Funds. Project
Fische ‘Breast cancer screening-stage 2’. https://www.fonduri-structurale.ro/fisa-proiect/2/programul-operational-capital-uman/275/pocu-4-9-screening-cancer-de-san-etapa-ii.
|