1. Introduction
With the rapid advancements in neonatal care, the
survival rates of very-low-birth-weight infants (VLBWIs) and
critical preterm infants have significantly improved. However,
bronchopulmonary dysplasia (BPD) is still associated with high
annual morbidity among preterm infants (1,2).
Northway et al first described BPD in 1967(3). It is a common respiratory system
disease in premature infants whose birth weight is less than 1,000
g. It is characterized by high fatality rates, and the surviving
premature infants have a high possibility of other sequelae
(4-6).
Due to different diagnostic methods and medical levels, the
prevalence rate of BPD varies greatly between 11 and 50% in
different countries (7). The USA
witnesses an annual of over 10,000 births with BPD (8). In preterm infants born before the
32nd gestational week, BPD is associated with an incidence of 12 to
32% (9). The incidence of BPD in
infants with birth weight less than 1,000 g is 30 to 50% (10). The causes of death in children
include recurrent respiratory tract infections (RTIs), pulmonary
heart diseases, and persistent pulmonary hypertension (PH). For
those who survive, the readmission rate is as high as 50% in the
first year of survival (11,12).
The main cause of readmission is recurrent lower RTI. The effect of
lung tissue damage in children can persist from the neonatal period
to adulthood (13-15).
Currently, the drugs used to treat BPD have several side effects
and poor efficacy (16-20).
Therefore, finding new therapeutic targets and drugs is a great
challenge faced by researchers and pediatricians.
Insulin-like growth factor-1 (IGF-1), which belongs
to the insulin family, plays a key role in body development,
vascular differentiation, and metabolism (21). IGF-1 plays a pivotal function in
treating chronic obstructive pulmonary disease (COPD), asthma,
idiopathic fibrosis, and acute respiratory distress syndrome (ARDS)
(22). Recently, studies have
shown a close association between IGF-1 and the occurrence and
development of BPD in preterm infants. Immunohistochemistry of the
lung tissues of children with BPD has revealed increased IGF-1
staining in alveolar epithelium, airway, and mesenchymal cells
(23). Hyperoxia can interfere
with the binding of IGF-1 and its receptor, IGF-1R, affect the
development of lung tissues, and subsequently hamper the normal
alveolar and microvascular development, causing pathological
changes similar to those seen in BPD (22,24).
In addition, studies have shown that the serum levels of IGF-1 are
associated with the risk of developing BPD (25,26).
These studies have highlighted that IGF-1 could be used as a novel
anti-BPD therapeutic target. The present review is a PubMed
(https://pubmed.ncbi.nlm.nih.gov/)-based
literature review, starting from several key words in different
combinations as mentioned in the specific ‘Key words’ section. Case
reports, case series and literature review-type articles were
included in the present research. A total number of 91 references
are included from 2003 to 2021. Inclusion criteria included English
language and full-length articles that were recently published with
the majority of the articles published within the last five
years.
2. Definition and naming of BPD
‘Classic’ BPD, also called ‘old’ BPD, refers to 32
cases of BPD initially described by Northway et al in
1967(3). ‘Old’ BPD was associated
with a higher fatality rate. The average gestational age of
children was 34 weeks. Children with old BPD developed severe
respiratory distress syndrome (RDS) after birth accompanied by
respiratory failure; therefore, mechanical ventilation with high
airway pressure was required for more than 28 days. The
pathological characteristics of ‘old’ BPD include chronic
inflammation of lung parenchyma, localized emphysema, and alveolar
septal fibrosis. With the continuous evolution of neonatal
intensive care and perinatal medical management, coupled with the
prenatal preventive use of glucocorticoids, the application of
exogenous pulmonary surfactants, and the implementation of
protective ventilation techniques (27), the incidence of ‘classic’ BPD has
been greatly reduced. Now, a more common form, called ‘light’ or
‘new’ BPD is used (28,29). The pathology of ‘new’ BPD is
characterized by a simplified alveolar structure, increased
alveolar volume, reduced numbers, and abnormal pulmonary vascular
morphology. ‘New’ BPD usually occurs in VLBWIs born before the 26th
gestational week or infants with birth weight <1,000 g. For
nearly half a century, there existed no agreement in the naming and
definition of BPD (30,31). In the 1990s, most of the experts
believed that BPD with abnormal chest X-ray changes was
collectively referred to as chronic lung disease (CLD), which
required continuous oxygen consumption after 36 weeks of
gestational age, or oxygen or mechanical ventilation at 28 days
after birth (32). At a workshop
organized by the National Heart, Lung and Blood Disorders Office
(NHLBI) and the National Institute of Child Health and Human
Development (NICHD) in 2000, BPD was redefined as: newborns who are
oxygen dependent (>21%) for more than 28 days (33). According to the new definition,
there are three types of BPD: mild, no oxygen required; moderate,
FiO2 less than 30%; severe, FiO2 greater than or equal to 30% or
requiring mechanical ventilation (33,34).
3. Pathogenesis and current situation of
BPD
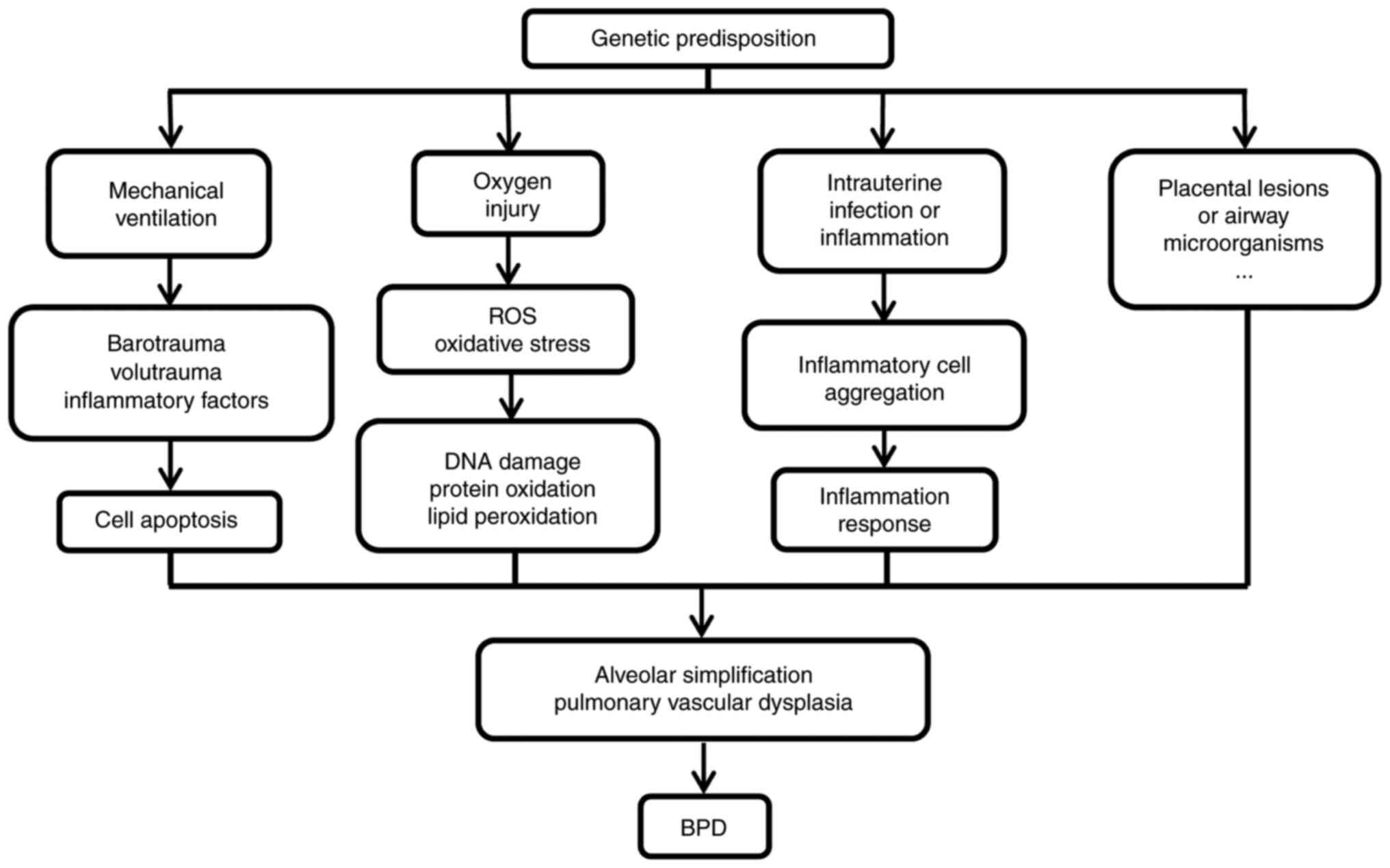
The factors that contribute to the development of
BPD are numerous, and the mechanisms are complex (35). It is now generally accepted that
BPD is based on genetic susceptibility and adverse factors such as
infection, mechanical ventilation and hyperoxia, damage to the
developing lung, and abnormal repair after injury (Fig. 1).
High oxygen concentrations and prolonged mechanical
ventilation therapy are the main reasons for the development of
‘classical’ BPD (36). Premature
infants of gestational age <28 weeks are at the advanced lung
development stage, which is caused by premature pulmonary
development, high oxygen level exposure after birth, or damage to
the airway, lung vessels, and parenchyma aggravated by mechanical
ventilation, ultimately resulting in BPD. In animal experiments,
newborn rats were placed in a hyperoxic environment to investigate
morphological changes in their lung tissue from 0 to 28 days. They
showed simple alveolar structures, fibrosis at the alveolar septum,
and reduced pulmonary microvasculature with prolonged oxygen
exposure (37,38). In addition, preterm infants have
weak resistance to oxidative stress. Under hyperoxic conditions,
the production of large amounts of reactive oxygen species (ROS)
exceeds the body's antioxidant capacity causing oxidative stress
damage and inhibiting the growth and differentiation of the
alveolar epithelium, hindering the development of lung septa and
alveolar formation after birth and eventually developing BPD
(39). Furthermore, hyperoxia can
induce lung injury through the cyclooxygenase-2 (Cox-2) and
endoplasmic reticulum stress pathways, leading to impaired
alveolarization of lung tissue (40). Teng et al demonstrated that
hyperoxia increased the expression of endoplasmic reticulum stress
pathways and downstream markers (41), whereas endoplasmic reticulum stress
led to impaired vascular endothelialization through oxidative
stress mechanisms and p38MAPK (42). These animal studies established
that significant lung injury occurs in preterm infants even when
ventilated at very low ventilator pressures because the lungs of
preterm infants are immature, and the collagen in the alveoli and
interstitium does not limit the expansion of the lungs leading to
hyperinflation. Overall, hyperoxia and mechanical ventilation play
an important role in the development of BPD.
Inflammatory response or intrauterine infection is
an important cause of ‘mild’ BPD development (43-45).
Over 90% of premature infants born before the 28th gestational week
have an intrauterine infection, whereas co-morbid BPD shows a
higher prevalence (46).
Intrauterine infections cause the inflammatory cells to be
accumulated within the fetal lungs, resulting in the release of
abundant pro-inflammatory cells, which can impair fetal lung
development and lead to preterm delivery (47). Postnatal high levels of oxygen
therapy, mechanical ventilation, and certain infections may cause a
pulmonary inflammatory response (48,49).
When the alveolar-capillary barrier becomes impaired, the injured
alveolar tissue promptly releases inflammatory factors resulting in
the dysregulated levels of pro- and anti-inflammatory factors,
increased apoptosis, and decreased proliferation of lung epithelial
cells, thereby affecting the differentiation of endothelial cells,
lung epithelial cells, and mesenchymal cells and further hindering
the alveolar development. Kumar et al, in their study on
bronchoalveolar development in children with BPD, found that
interleukin (IL)-1β, IL-6, IL-8, IL-10, and tumor necrosis factor
(TNF)-α expression was significantly increased by lavage tests
(50). In addition, blood and
urine tests on children with BPD can also reveal the above
biomarkers (51,52). The above results suggest that an
intrauterine or postnatal inflammatory response is involved in the
development of BPD in infants.
Several recent studies have hypothesized that
placental lesions have an important function in BPD etiology, which
is related to moderate-to-severe BPD among the VLBWIs (53,54).
In addition, the association between microorganisms in the airway
and BPD has drawn researchers' attention, with studies evidencing
astounding differences in airway microorganisms between children
with BPD, preterm infants, and full-term infants (55). Airway microorganisms among
premature infants who require mechanical ventilation are
potentially related to BPD severity (56).
Surviving children with BPD develop proliferation of
airway smooth muscle cells and epithelial cells, airway remodeling,
and combined inflammatory infiltration of the lungs, resulting in
airway hyperresponsiveness, impaired lung function, and increased
chances of respiratory viral infections in the first year of life
(38,57). Based on the follow-up of children
with BPD, this impairment of lung function lasts until adolescence
or even an adult stage and may be accompanied by long-range
respiratory disorders such as chronic obstructive pulmonary disease
(COPD) or asthma (58,59). Saarenpää et al, in their
age-matched study on 29 adults (age group, 18-27 years) with a
previous diagnosis of BPD with age-matched healthy adults,
documented that first-second exertional expiratory volume and
first-second exertional expiratory volume/exertional lung capacity
were significantly lower than those in healthy adults (60). According to Kotecha et al
(61), a 20% decrease in first
and/or second exhalation exertion among BPD cases in comparison
with controls suggested that the adulthood COPD risk elevated among
BPD children. This was related to the simplification of alveolar
structure and increased and decreased alveolar volumes and numbers
in patients with BPD.
4. Biological characteristics and activity
of IGF-1
IGF-1 belongs to a class of polypeptides of the
insulin family (tyrosine kinase) and was discovered by Salmanh and
Daughudy in 1957(62). Somatic
growth hormone is mediated by a substance in serum that exerts a
growth-promoting effect and is termed sulfation-activated factor
(SFA) because it acts through sulfation. Later, Dulak and Temin
discovered (63) that certain
cells secrete a substance that promotes cell growth; hence the name
multiplication-stimulating activity (MSA) was coined. Until 1978,
these two substances were successfully isolated from the plasma and
named insulin-like growth factor because of their structural and
functional similarity to insulin (64). To date, only two members, IGF-1 and
IGF-2, have been identified. IGF-1 is a 7.5 kDa polypeptide formed
by 70 amino acids, four domains, and three pairs of disulfide
bonds, which is highly homologous (about 49%) to insulin (65). The biological effects of IGF-1 are
predominantly 2-fold (66). First,
it stimulates the synthesis of DNA and RNA, mediates cell
proliferation and differentiation, and helps in promoting mitosis.
Second, it promotes fat and protein synthesis, regulates glycolysis
and glucose isogenesis, and has insulin-like metabolic effects.
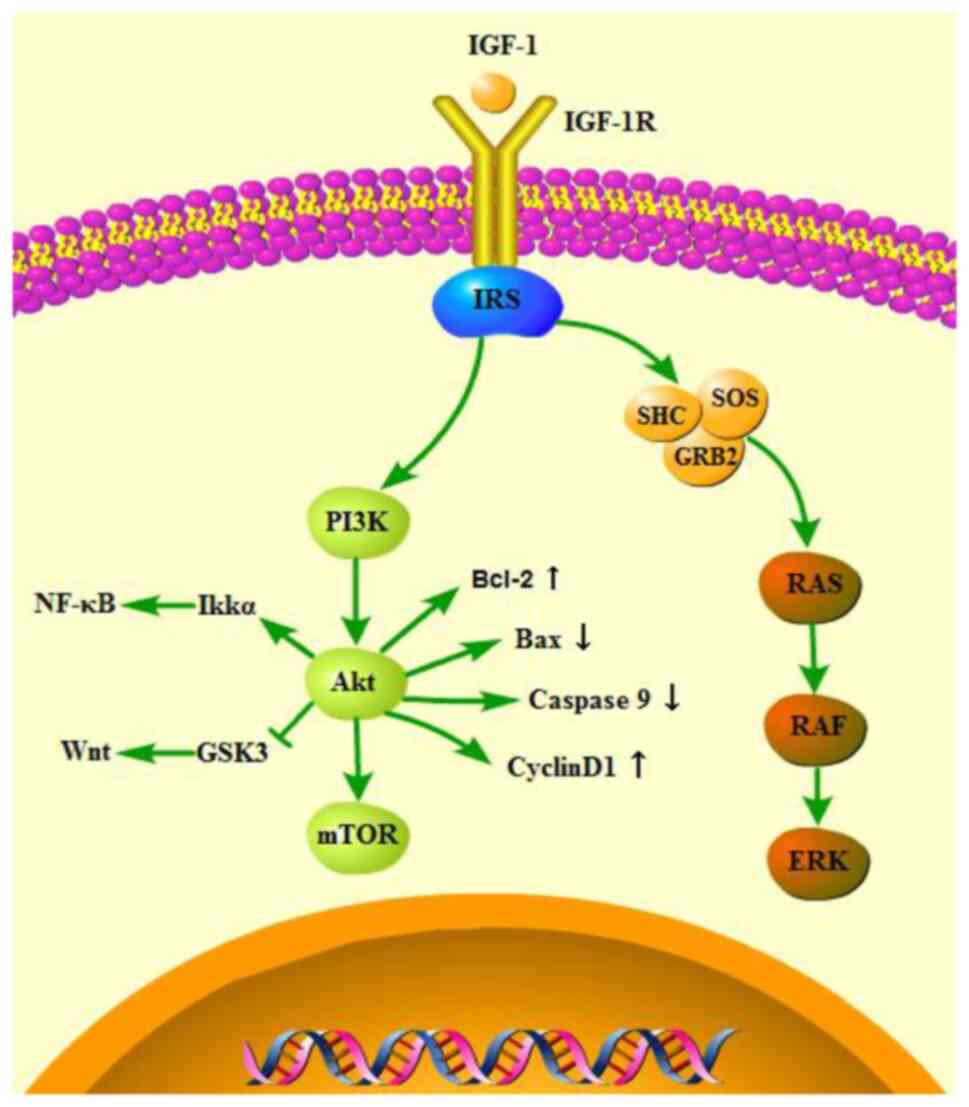
Several tissues supply IGF-1 to cells through autocrine or
paracrine forms/modes; however, in the circulation, IGF-1 is mostly
produced from the liver under the regulation of growth hormone,
which acts on target tissues through endocrine, autocrine, or
paracrine manner, exerts biological effects, and plays a vital
function in regulating different cell growth and differentiation
processes (21) (Fig. 2).
5. IGF-1 in lung development
IGF-1 is required for lung development processes.
IGF-1 is widely distributed in the lungs of newborn rodents
(67), and IGF-1 deletion is
suggested to greatly affect the development of the lungs. The
concentration of IGF-1 in the cord blood of newborns is associated
with the development of the fetal lung. ATII cells play a pivotal
role in lung tissue development. When ATII cells are transformed to
type I alveolar (ATI) cells, the expression of IGF-1 is
significantly increased (68). The
exogenous application of recombinant IGF-1 promoted the conversion
of ATII to ATI. However, the addition of the IGF-1 antibody
inhibited the proliferation and differentiation of ATII (69). Moreover, ATII cells showed a high
percentage in IGF-1-deficient mice (70), indicating that the IGF-1 deficiency
affected the differentiation of ATII cells. In addition, IGF-1
promotes lung tissue development by modulating alveolar epithelial
and airway basal cells. The mechanism has not yet been elucidated
but could be related to the interaction between IGF-1 and its
downstream factors, or maybe via a paracrine or autocrine manner. A
similar finding was observed in certain in vivo and in
vitro studies. IGF-1-/- mutant mice are born with
poor lung development, which is characterized by thickening of the
alveolar interstitium, thinning of smooth muscles, dilatation of
blood vessels, diffuse deposition of the extracellular matrix
(ECM), delayed long-term lung development, susceptibility to
respiratory distress syndrome, and elevated mortality (71).
6. IGF-1 and lung injury
When lung injury response occurs, lung epithelial
cells, type II alveolar (ATII) cells, and inflammatory cells
activate and release IGF-1(72),
which is involved in the proliferation and migration of lung tissue
fibroblasts and stimulates collagen production, ultimately causing
ECM remodeling and aggregation. IGF-1 modulates
epithelial-mesenchymal transition (EMT) in ATII cells during lung
damage (73), greatly affecting
ECM production. The airway basal cells play a vital function in the
injury to the airway as well as its repair, and IGF-1 may regulate
basal cell differentiation and proliferation through FOXO-mediated
p63(74). Thus, IGF-1 may be an
important factor in lung injury repair.
7. Possible underlying mechanisms of IGF-1
in BPD development
The level of IGF-1 was found to be markedly elevated
in myofibroblasts, alveolar epithelial cells, and mesenchymal cells
when the lungs of patients who died from BPD were studied (23). Significantly increased levels of
IGF-1 were found in bronchoalveolar lavage fluid (BALF) obtained
from BPD premature infants (28).
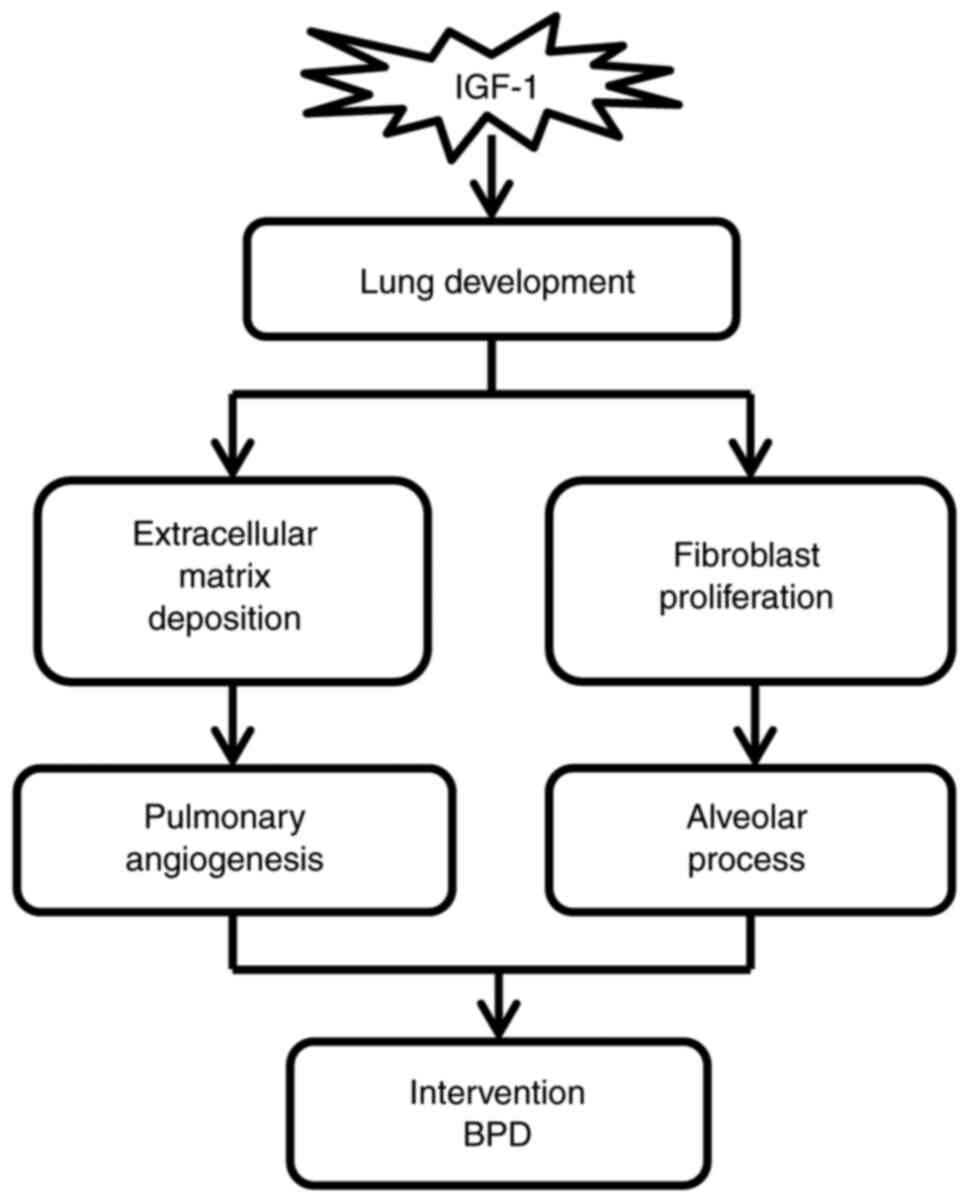
In animal studies, IGF-1 expression was significantly elevated in
the lungs during hyperoxia exposure and recovery (69). These studies indicate the
involvement of IGF-1 in BPD development (Fig. 3).
In IGF-1-knockout mice, lung development is
characterized by severe lung dysplasia with increased apoptosis,
decreased airway volume, and collapsed alveoli (70), which is similar to the pathology of
BPD. According to a study (75),
the ventilation and breathing patterns of IGF-1Rneo/-
mice were significantly better than those of IGF-1R+/+
mice under hyperoxic conditions, and they could better survive
under hyperoxic conditions. IGF-1R+/+ group mice were
more likely to present with abnormal breathing patterns due to
hyperoxia and increased probability of respiratory failure. In
addition, the lung tissues in IGF-1R+/+ mice showed
significant pulmonary edema, intra-alveolar hemorrhage along the
formation of the hyaline membrane relative to those observed in
IGF-1Rneo/- mice. This indicates that interference or
destruction of the IGF-1 signaling pathway plays an important role
in hyperoxia-induced BPD.
Stagnation of lung development, decreased alveolus
number and elevated size, and reduced pulmonary vascular production
are some of the characteristics of BPD. Echocardiography during
pregnancy found that fetal pulmonary vascular disease is closely
related to the occurrence of BPD at 36 weeks of corrected
gestational age (76). The
mechanisms affecting alveolar development and angiogenic alveolar
development during this process have not been elucidated. In the
fetus, alveolarization is initiated at about the 36th gestational
week, and most children who develop BPD are born before 32 weeks of
gestation and have not yet developed alveoli at birth (24). Studies conducted in animal models
have shown that alveoli are initially formed by inward growth of
secondary cristae and septum, a process regulated by multiple
cytokines. IGF-1 regulates the generation of secondary cristae
during alveolar formation. Studies have shown that loss of IGF-1
reduced the synthesis of elastin fibers, type I pre-collagen, and
secondary cristae cell DNA, severely affecting alveolar development
and even causing lethal respiratory distress (77). Findings from several studies have
revealed that hyperoxia affects the affinity of IGF-1 and its
receptors, interfers with the formation of secondary cristae, and
hinders the formation of alveoli (24). Most organs, including the vascular
system, depend on IGF-1 for their growth and differentiation
(21,78). In the vascular and alveolar
epithelial development process, IGF-1 and leukemia inhibitory
factor (LIF) exert synergistic effects (70). LIF and IGF-1 double knockout mice
exhibit severe alveolar collapse and pulmonary vascular
malformations. Previous studies have shown that vascular
endothelial growth factor (VEGF) plays an essential function during
lung vascular development. VEGF signals can hinder the
alveolarization process and participate in the occurrence and
development of BPD (79). It has
been shown that IGF-1 can activate VEGF signaling through the MAPK
and Akt pathways and can play a protective role in angiogenesis,
endothelial differentiation, and regeneration (80). In addition, IGF-1 may upregulate
VEGF protein expression by increasing the rate of transcription of
the VEGF gene (81). In a
recent study, intraperitoneal injection of rhIGF-1/BP3 promoted the
formation of alveoli and microvessels, thereby improving lung
function (82). Alveolar
development and angiogenesis are important processes in lung
development. IGF-1 treatment may affect alveolar development and
angiogenesis, and thus restores lung injury in children with
BPD.
The aggregation of inflammatory cells, such as
neutrophils, greatly affects lung damage among BPD cases (45). IGF-1 participates in the regulation
of T-helper cell subset 1/2 (Th-1)/Th-2 balance in the body
(83). Clinical studies (84) indicate that when serum IGF-1 is
<20 mg/l, symptoms of infection occurred nine times (out of a
total of 16) higher, suggesting the involvement of IGF-1 in the
inflammatory response of lung tissues. These studies indicate that
lower levels of IGF-1 in the circulation and the destruction of the
IGF-1 signaling pathway may be related to the pathogenesis of
BPD.
8. IGF-1 as a new option for BPD
treatment
Experiments concerning IGF-1 have been carried out.
Several in vitro and in vivo studies suggest the
vital role of IGF-1 in BPD genesis and development. As demonstrated
in animal research (85), exposure
to hyperoxia for a long time induced alveolar cell apoptosis and
suppressed Clara cell secretory protein (CCSP) expression.
Intraperitoneal injection of IGF-1 was found to increase the
secretion of CCSP, reduce the inflammatory response in the lung,
and inhibit the apoptosis of lung tissue cells. In addition, CC10
is the main secreted protein of Clara cells and plays a protective
role in lung injury due to its anti-inflammatory properties.
Previous studies have shown that the lower the expression of CC10,
the higher the risk of BPD development. In an animal model of BPD
(86), exogenous injection of
recombinant IGF-1 was found to increase the number of Clara cells,
which indirectly acted as an anti-inflammatory agent and reduced
the risk of BPD. In clinical studies, IGF-1 in fetal serum was
found to be elevated in mid and late gestational periods. The
levels of IGF-1 in preterm infants are significantly lower than
intrauterine levels at the same gestational age. The lack of IGF-1
in the serum of preterm infants in the early postnatal period
suggests an increased risk of developing BPD. Recombinant
rhIGF-1/IGFBP-3 is currently in clinical trials as a therapy for
preterm infants. A phase I and II Randomized Controlled Trial (RCT)
on the pharmacokinetics and safety of rhIGF-1/IGFBP-3 did not
reveal any significant adverse effects at this time, and the safety
variables were within normal limits (87-89).
In addition, in a study of rhIGF-1/IGFBP-3 for the prevention of
retinopathy of prematurity (ROP), secondary findings found a
significant reduction in the incidence of severe BPD in the full
analysis set group (53%) (90). A
recent study found that rhIGF-1/IGFBP-3 treatment improved lung
function in 2 prenatal BPD models of intrauterine infection and
pre-eclampsia, as well as in a hyperoxia-induced postpartum BPD
model (82). An RCT (Identifier:
NCT03253263) containing the clinical efficacy of rhIGF-1/IGFBP-3 in
the treatment of BPD in very preterm infants is underway, and it is
believed that the results of this study will provide strong
evidence for the future clinical treatment of BPD with IGF-1.
9. Challenges and prospects of IGF-1
To the best of our knowledge, IGF-1 is involved in
both BPD induced by prolonged hyperoxia exposure and BPD mediated
by inflammation of intrauterine infection. In addition, the
exogenous supplementation of IGF-1 can reduce BPD symptoms.
Although extensive research has been conducted on IGF-1, there are
still numerous issues that require elucidation. First, there are
contradictory reports on the expression of IGF-1, which may be
related to its biological characteristics. Further studies are
required to explore the ability of IGF-1 to promote both
proliferation and differentiation, as well as insulin-like
metabolism. In addition, most of the current data are derived from
animal models, and adequate clinical data are lacking. Thus,
results from a large number of multicenter randomized controlled
trials are still required to support this hypothesis. Further
studies can incorporate the knowledge and findings of the present
review to integrate basic experimental and clinical studies for the
early use of IGF-1 to prevent and treat BPD among premature
infants.
10. Conclusion
The current review discusses the association between
IGF-1 and BPD. IGF-1 is an important chemical in the human body
that is associated with over 100 diseases and even the early onset
of aging. We believe this review will enlighten the community and
prove helpful in reducing morbidity and mortality in preterm and
postnatal children affected with BPD. However, more clinical trials
are warranted to establish conclusive and convincing associations
in humans.
Acknowledgements
Not applicable.
Funding
Funding: The present study was funded by the National Natural
Science Foundation of China (no. 81860279).
Availability of data and materials
Not applicable.
Authors' contributions
SZ contributed to the investigation and wrote the
original draft of the manuscript. XL and SZ performed the relevant
literature research and revised the manuscript. HL and XL
contributed to the literature search and processing of the
findings. ZJ contributed to the conceptualization of the review.
Data authentication is not applicable. All authors read and
approved the final manuscript for publication.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hwang JS and Rehan VK: Recent advances in
bronchopulmonary dysplasia: Pathophysiology, prevention, and
treatment. Lung. 196:129–138. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bancalari E and Jain D: Bronchopulmonary
dysplasia: 50 Years after the original description. Neonatology.
115:384–391. 2019.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Northway WH Jr, Rosan RC and Porter DY:
Pulmonary disease following respirator therapy of hyaline-membrane
disease. Bronchopulmonary dysplasia. N Engl J Med. 276:357–368.
1967.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Chen S, Wu Q, Zhong D, Li C and Du L:
Caffeine prevents hyperoxia-induced lung injury in neonatal mice
through NLRP3 inflammasome and NF-κB pathway. Respir Res.
21(140)2020.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Principi N, Di Pietro GM and Esposito S:
Bronchopulmonary dysplasia: Clinical aspects and preventive and
therapeutic strategies. J Transl Med. 16(36)2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sahni M and Bhandari V: Recent advances in
understanding and management of bronchopulmonary dysplasia.
F1000Res 9: F1000 Faculty Rev-703, 2020.
|
|
7
|
Thébaud B, Goss KN, Laughon M, Whitsett
JA, Abman SH, Steinhorn RH, Aschner JL, Davis PG, McGrath-Morrow
SA, Soll RF and Jobe AH: Bronchopulmonary dysplasia. Nat Rev Dis
Primers. 5(78)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Lavoie PM and Dubé MP: Genetics of
bronchopulmonary dysplasia in the age of genomics. Curr Opin
Pediatr. 22:134–138. 2010.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Trembath A and Laughon MM: Predictors of
bronchopulmonary dysplasia. Clin Perinatol. 39:585–601.
2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Collaco JM, Romer LH, Stuart BD, Coulson
JD, Everett AD, Lawson EE, Brenner JI, Brown AT, Nies MK, Sekar P,
et al: Frontiers in pulmonary hypertension in infants and children
with bronchopulmonary dysplasia. Pediatr Pulmonol. 47:1042–1053.
2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Liu Y and Dong WB: Preventive effect of
caffeine on bronchopulmonary dysplasia in preterm infants. Zhongguo
Dang Dai Er Ke Za Zhi. 20:598–602. 2018.PubMed/NCBI View Article : Google Scholar : (In Chinese).
|
|
12
|
Bhandari A and Panitch HB: Pulmonary
outcomes in bronchopulmonary dysplasia. Semin Perinatol.
30:219–226. 2006.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Davidson LM and Berkelhamer SK:
Bronchopulmonary dysplasia: Chronic lung disease of infancy and
Long-Term pulmonary outcomes. J Clin Med. 6(4)2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Postma DS, Bush A and van den Berge M:
Risk factors and early origins of chronic obstructive pulmonary
disease. Lancet. 385:899–909. 2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sucre J, Haist L, Bolton CE and
Hilgendorff A: Early changes and indicators characterizing lung
aging in neonatal chronic lung disease. Front Med (Lausanne).
8(665152)2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Pakvasa MA, Saroha V and Patel RM:
Optimizing caffeine use and risk of bronchopulmonary dysplasia in
preterm infants: A systematic review, Meta-analysis, and
application of grading of recommendations assessment, development,
and evaluation methodology. Clin Perinatol. 45:273–291.
2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Baud O and Watterberg KL: Prophylactic
postnatal corticosteroids: Early hydrocortisone. Semin Fetal
Neonatal Med. 24:202–206. 2019.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Askie LM, Davies LC, Schreiber MD, Hibbs
AM, Ballard PL and Ballard RA: Race effects of inhaled nitric oxide
in preterm infants: An individual participant data Meta-Analysis. J
Pediatr. 193:34–39.e2. 2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Thompson EJ, Greenberg RG, Kumar K,
Laughon M, Smith PB, Clark RH, Crowell A, Shaw L, Harrison L,
Scales G, et al: Association between furosemide exposure and patent
ductus arteriosus in hospitalized infants of very low birth weight.
J Pediatr. 199:231–236. 2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Augustine S, Cheng W, Avey MT, Chan ML,
Lingappa SM, Hutton B and Thébaud B: Are all stem cells equal?
Systematic review, evidence map, and meta-analyses of preclinical
stem cell-based therapies for bronchopulmonary dysplasia. Stem
Cells Transl Med. 9:158–168. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Hellstrom A, Ley D, Hallberg B, Lofqvist
C, Hansen-Pupp I, Ramenghi LA, Borg J, Smith LE and Hard AL: IGF-1
as a drug for preterm infants: A Step-Wise clinical development.
Curr Pharm Des. 23:5964–5970. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Wang Z, Li W, Guo Q, Wang Y, Ma L and
Zhang X: Insulin-Like Growth Factor-1 Signaling in lung development
and inflammatory lung diseases. Biomed Res Int.
2018(6057589)2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Chetty A, Andersson S, Lassus P and
Nielsen HC: Insulin-like growth factor-1 (IGF-1) and IGF-1 receptor
(IGF-1R) expression in human lung in RDS and BPD. Pediatr Pulmonol.
37:128–136. 2004.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Belcastro R, Lopez L, Li J, Masood A and
Tanswell AK: Chronic lung injury in the neonatal rat: Up-regulation
of TGFβ1 and nitration of IGF-R1 by peroxynitrite as likely
contributors to impaired alveologenesis. Free Radic Biol Med.
80:1–11. 2015.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Banjac L, Kotur-Stevuljević J, Gojković T,
Bokan-Mirković V and Banjac G and Banjac G: Relationship between
insulin-like growth factor type 1 and intrauterine growth. Acta
Clin Croat. 59:91–96. 2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Salaets T, Aertgeerts M, Gie A, Vignero J,
de Winter D, Regin Y, Jimenez J, Vande Velde G, Allegaert K,
Deprest J and Toelen J: Preterm birth impairs postnatal lung
development in the neonatal rabbit model. Respir Res.
21(59)2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Dumpa V and Bhandari V: Surfactant,
steroids and non-invasive ventilation in the prevention of BPD.
Semin Perinatol. 42:444–452. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Day CL and Ryan RM: Bronchopulmonary
dysplasia: New becomes old again! Pediatr Res. 81:210–213.
2017.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Collaco JM and McGrath-Morrow SA:
Respiratory phenotypes for preterm infants, children, and adults:
Bronchopulmonary dysplasia and more. Ann Am Thorac Soc. 15:530–538.
2018.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Bancalari E and Jain D: Bronchopulmonary
dysplasia: Can we agree on a definition? Am J Perinatol.
35:537–540. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Jensen EA and Wright CJ: Bronchopulmonary
dysplasia: The ongoing search for one definition to rule them all.
J Pediatr. 197:8–10. 2018.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Philip AG: Chronic lung disease of
prematurity: A short history. Semin Fetal Neonatal Med. 14:333–338.
2009.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Jobe AH and Bancalari E: Bronchopulmonary
dysplasia. Am J Respir Crit Care Med. 163:1723–1729.
2001.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Jensen EA, Dysart K, Gantz MG, McDonald S,
Bamat NA, Keszler M, Kirpalani H, Laughon MM, Poindexter BB, Duncan
AF, et al: The diagnosis of bronchopulmonary dysplasia in very
preterm infants. An Evidence-based approach. Am J Respir Crit Care
Med. 200:751–759. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Islam JY, Keller RL, Aschner JL, Hartert
TV and Moore PE: Understanding the Short- and Long-Term respiratory
outcomes of prematurity and bronchopulmonary dysplasia. Am J Respir
Crit Care Med. 192:134–156. 2015.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Haggie S, Robinson P, Selvadurai H and
Fitzgerald DA: Bronchopulmonary dysplasia: A review of the
pulmonary sequelae in the post-surfactant era. J Paediatr Child
Health. 56:680–689. 2020.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Cox AM, Gao Y, Perl AT, Tepper RS and
Ahlfeld SK: Cumulative effects of neonatal hyperoxia on murine
alveolar structure and function. Pediatr Pulmonol. 52:616–624.
2017.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Niedermaier S and Hilgendorff A:
Bronchopulmonary dysplasia-an overview about pathophysiologic
concepts. Mol Cell Pediatr. 2(2)2015.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Balaji S, Dong X, Li H, Zhang Y, Steen E
and Lingappan K: Sex-specific differences in primary neonatal
murine lung fibroblasts exposed to hyperoxia in vitro: Implications
for bronchopulmonary dysplasia. Physiol Genomics. 50:940–946.
2018.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Choo-Wing R, Syed MA, Harijith A, Bowen B,
Pryhuber G, Janér C, Andersson S, Homer RJ and Bhandari V:
Hyperoxia and interferon-γ-induced injury in developing lungs occur
via cyclooxygenase-2 and the endoplasmic reticulum stress-dependent
pathway. Am J Respir Cell Mol Biol. 48:749–757. 2013.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Teng RJ, Jing X, Michalkiewicz T, Afolayan
AJ, Wu TJ and Konduri GG: Attenuation of endoplasmic reticulum
stress by caffeine ameliorates hyperoxia-induced lung injury. Am J
Physiol Lung Cell Mol Physiol. 312:L586–L598. 2017.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Galán M, Kassan M, Kadowitz PJ, Trebak M,
Belmadani S and Matrougui K: Mechanism of endoplasmic reticulum
stress-induced vascular endothelial dysfunction. Biochim Biophys
Acta. 1843:1063–1075. 2014.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Pan J, Zhan C, Yuan T, Wang W, Shen Y, Sun
Y, Wu T, Gu W, Chen L and Yu H: Effects and molecular mechanisms of
intrauterine infection/inflammation on lung development. Respir
Res. 19(93)2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Laube M, Amann E, Uhlig U, Yang Y, Fuchs
HW, Zemlin M, Mercier JC, Maier RF, Hummler HD, Uhlig S and Thome
UH: Inflammatory mediators in tracheal aspirates of preterm infants
participating in a randomized trial of inhaled nitric oxide. PLoS
One. 12(e0169352)2017.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Savani RC: Modulators of inflammation in
bronchopulmonary dysplasia. Semin Perinatol. 42:459–470.
2018.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Ghosh C and Wojtowycz M: Effect of
gestational disorders on preterm birth, low birthweight, and NICU
admission. Arch Gynecol Obstet. 303:419–426. 2021.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Papagianis PC, Pillow JJ and Moss TJ:
Bronchopulmonary dysplasia: Pathophysiology and potential
anti-inflammatory therapies. Paediatr Respir Rev. 30:34–41.
2019.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Cui TX, Brady AE, Fulton CT, Zhang YJ,
Rosenbloom LM, Goldsmith AM, Moore BB and Popova AP: CCR2 Mediates
Chronic LPS-Induced pulmonary inflammation and hypoalveolarization
in a murine model of bronchopulmonary dysplasia. Front Immunol.
11(579628)2020.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Kalikkot Thekkeveedu R, Guaman MC and
Shivanna B: Bronchopulmonary dysplasia: A review of pathogenesis
and pathophysiology. Respir Med. 132:170–177. 2017.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Kumar VH, Lakshminrusimha S, Kishkurno S,
Paturi BS, Gugino SF, Nielsen L, Wang H and Ryan RM: Neonatal
hyperoxia increases airway reactivity and inflammation in adult
mice. Pediatr Pulmonol. 51:1131–1141. 2016.PubMed/NCBI View Article : Google Scholar
|
|
51
|
D'Angio CT, Ambalavanan N, Carlo WA,
McDonald SA, Skogstrand K, Hougaard DM, Shankaran S, Goldberg RN,
Ehrenkranz RA, Tyson JE, et al: Blood cytokine profiles associated
with distinct patterns of bronchopulmonary dysplasia among
extremely low birth weight infants. J Pediatr. 174:45–51.e5.
2016.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Balany J and Bhandari V: Understanding the
impact of infection, inflammation, and their persistence in the
pathogenesis of bronchopulmonary dysplasia. Front Med (Lausanne).
2(90)2015.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Torchin H, Ancel PY, Goffinet F, Hascoët
JM, Truffert P, Tran D, Lebeaux C and Jarreau PH: Placental
complications and bronchopulmonary dysplasia: EPIPAGE-2 Cohort
Study. Pediatrics. 137(e20152163)2016.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Bhandari V and Lodha A: Is
bronchopulmonary dysplasia decided before birth? Pediatr Res.
87:809–810. 2020.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Pammi M, Lal CV, Wagner BD, Mourani PM,
Lohmann P, Luna RA, Sisson A, Shivanna B, Hollister EB, Abman SH,
et al: Airway microbiome and development of bronchopulmonary
dysplasia in preterm infants: A systematic review. J Pediatr.
204:126–133.e2. 2019.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Surate Solaligue DE, Rodríguez-Castillo
JA, Ahlbrecht K and Morty RE: Recent advances in our understanding
of the mechanisms of late lung development and bronchopulmonary
dysplasia. Am J Physiol Lung Cell Mol Physiol. 313:L1101–L1153.
2017.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Lewin G and Hurtt ME: Pre- and Postnatal
lung development: An updated species comparison. Birth Defects Res.
109:1519–1539. 2017.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Segerer FJ and Speer CP: Lung function in
childhood and adolescence: Influence of prematurity and
bronchopulmonary dysplasia. Z Geburtshilfe Neonatol. 220:147–154.
2016.PubMed/NCBI View Article : Google Scholar : (In German).
|
|
59
|
Landry JS, Tremblay GM, Li PZ, Wong C,
Benedetti A and Taivassalo T: Lung function and bronchial
hyperresponsiveness in adults born prematurely. A Cohort study. Ann
Am Thorac Soc. 13:17–24. 2016.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Saarenpää HK, Tikanmäki M, Sipola-Leppänen
M, Hovi P, Wehkalampi K, Siltanen M, Vääräsmäki M, Järvenpää AL,
Eriksson JG, Andersson S and Kajantie E: Lung function in very low
birth weight adults. Pediatrics. 136:642–650. 2015.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Kotecha SJ, Edwards MO, Watkins WJ,
Henderson AJ, Paranjothy S, Dunstan FD and Kotecha S: Effect of
preterm birth on later FEV1: A systematic review and meta-analysis.
Thorax. 68:760–766. 2013.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Salmon WD Jr and Daughaday WH: A
hormonally controlled serum factor which stimulates sulfate
incorporation by cartilage in vitro. J Lab Clin Med. 49:825–836.
1957.PubMed/NCBI
|
|
63
|
Dulak NC and Temin HM: A partially
purified polypeptide fraction from rat liver cell conditioned
medium with multiplication-stimulating activity for embryo
fibroblasts. J Cell Physiol. 81:153–160. 1973.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Rinderknecht E and Humbel RE: The amino
acid sequence of human insulin-like growth factor I and its
structural homology with proinsulin. J Biol Chem. 253:2769–2776.
1978.PubMed/NCBI
|
|
65
|
Bortvedt SF and Lund PK: Insulin-like
growth factor 1: Common mediator of multiple enterotrophic hormones
and growth factors. Curr Opin Gastroenterol. 28:89–98.
2012.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Piñeiro-Hermida S, López IP, Alfaro-Arnedo
E, Torrens R, Iñiguez M, Alvarez-Erviti L, Ruíz-Martínez C and
Pichel JG: IGF1R deficiency attenuates acute inflammatory response
in a bleomycin-induced lung injury mouse model. Sci Rep.
7(4290)2017.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Vitale G, Pellegrino G, Vollery M and
Hofland LJ: ROLE of IGF-1 system in the modulation of Longevity:
Controversies and new insights from a Centenarians' Perspective.
Front Endocrinol (Lausanne). 10(27)2019.PubMed/NCBI View Article : Google Scholar
|
|
68
|
López IP, Piñeiro-Hermida S, Pais RS,
Torrens R, Hoeflich A and Pichel JG: Involvement of Igf1r in
bronchiolar epithelial regeneration: Role during repair kinetics
after selective club cell ablation. PLoS One.
11(e0166388)2016.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Narasaraju TA, Chen H, Weng T, Bhaskaran
M, Jin N, Chen J, Chen Z, Chinoy MR and Liu L: Expression profile
of IGF system during lung injury and recovery in rats exposed to
hyperoxia: A possible role of IGF-1 in alveolar epithelial cell
proliferation and differentiation. J Cell Biochem. 97:984–998.
2006.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Moreno-Barriuso N, López-Malpartida AV, de
Pablo F and Pichel JG: Alterations in alveolar epithelium
differentiation and vasculogenesis in lungs of LIF/IGF-I double
deficient embryos. Dev Dyn. 235:2040–2050. 2006.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Liu JP, Baker J, Perkins AS, Robertson EJ
and Efstratiadis A: Mice carrying null mutations of the genes
encoding insulin-like growth factor I (Igf-1) and type 1 IGF
receptor (Igf1r). Cell. 75:59–72. 1993.PubMed/NCBI
|
|
72
|
Clement A and Eber E: Interstitial lung
diseases in infants and children. Eur Respir J. 31:658–666.
2008.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Li H, Batth IS, Qu X, Xu L, Song N, Wang R
and Liu Y: IGF-IR signaling in epithelial to mesenchymal transition
and targeting IGF-IR therapy: Overview and new insights. Mol
Cancer. 16(6)2017.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Günschmann C, Stachelscheid H, Akyüz MD,
Schmitz A, Missero C, Brüning JC and Niessen CM: Insulin/IGF-1
controls epidermal morphogenesis via regulation of FoxO-mediated
p63 inhibition. Dev Cell. 26:176–187. 2013.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Ahamed K, Epaud R, Holzenberger M, Bonora
M, Flejou JF, Puard J, Clement A and Henrion-Caude A: Deficiency in
type 1 insulin-like growth factor receptor in mice protects against
oxygen-induced lung injury. Respir Res. 6(31)2005.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Mourani PM, Mandell EW, Meier M, Younoszai
A, Brinton JT, Wagner BD, Arjaans S, Poindexter BB and Abman SH:
Early pulmonary vascular disease in preterm infants is associated
with late respiratory outcomes in childhood. Am J Respir Crit Care
Med. 199:1020–1027. 2019.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Li J, Masood A, Yi M, Lau M, Belcastro R,
Ivanovska J, Jankov RP and Tanswell AK: The IGF-I/IGF-R1 pathway
regulates postnatal lung growth and is a nonspecific regulator of
alveologenesis in the neonatal rat. Am J Physiol Lung Cell Mol
Physiol. 304:L626–L637. 2013.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Hellström A, Ley D, Hansen-Pupp I,
Hallberg B, Löfqvist C, van Marter L, van Weissenbruch M, Ramenghi
LA, Beardsall K, Dunger D, et al: Insulin-like growth factor 1 has
multisystem effects on foetal and preterm infant development. Acta
Paediatr. 105:576–586. 2016.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Hirsch K, Taglauer E, Seedorf G, Callahan
C, Mandell E, White CW, Kourembanas S and Abman SH: Perinatal
Hypoxia-Inducible factor stabilization preserves lung alveolar and
vascular growth in experimental bronchopulmonary dysplasia. Am J
Respir Crit Care Med. 202:1146–1158. 2020.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Higashi Y, Gautam S, Delafontaine P and
Sukhanov S: IGF-1 and cardiovascular disease. Growth Horm IGF Res.
45:6–16. 2019.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Stahl A, Connor KM, Sapieha P, Chen J,
Dennison RJ, Krah NM, Seaward MR, Willett KL, Aderman CM, Guerin
KI, et al: The mouse retina as an angiogenesis model. Invest
Ophthalmol Vis Sci. 51:2813–2826. 2010.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Seedorf G, Kim C, Wallace B, Mandell EW,
Nowlin T, Shepherd D and Abman SH: rhIGF-1/BP3 preserves lung
growth and prevents pulmonary hypertension in experimental
bronchopulmonary dysplasia. Am J Respir Crit Care Med.
201:1120–1134. 2020.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Capoluongo E, Vento G, Ameglio F, Lulli P,
Matassa PG, Carrozza C, Santini SA, Antenucci M, Castagnola M,
Giardina B, et al: Increased levels of IGF-1 and
beta2-microglobulin in epithelial lining fluid of preterm newborns
developing chronic lung disease effects of rhG-CSF. Int J
Immunopathol Pharmacol. 19:57–66. 2006.PubMed/NCBI
|
|
84
|
Klevebro S, Hellgren G, Hansen-Pupp I,
Wackernagel D, Hallberg B, Borg J, Pivodic A, Smith L, Ley D and
Hellström A: Elevated levels of IL-6 and IGFBP-1 predict low serum
IGF-1 levels during continuous infusion of rhIGF-1/rhIGFBP-3 in
extremely preterm infants. Growth Horm IGF Res. 50:1–8.
2020.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Jin ZA, Jin ZY, Chi YX and Lu JR: Effects
of recombinant human insulin-like growth factor-1 on the expression
of Clara cell secretory protein in lung of hyperoxia-exposed
newborn rats. Zhonghua Er Ke Za Zhi. 45:369–373. 2007.PubMed/NCBI(In Chinese).
|
|
86
|
Guzmán-Bárcenas J, Calderón-Moore A,
Baptista-González H and Irles C: Clara cell protein expression in
mechanically ventilated term and preterm infants with respiratory
distress syndrome and at risk of bronchopulmonary dysplasia: A
Pilot study. Can Respir J. 2017(8074678)2017.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Löfqvist C, Niklasson A, Engström E,
Friberg LE, Camacho-Hübner C, Ley D, Borg J, Smith LE and Hellström
A: A pharmacokinetic and dosing study of intravenous insulin-like
growth factor-I and IGF-binding protein-3 complex to preterm
infants. Pediatr Res. 65:574–579. 2009.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Ley D, Hansen-Pupp I, Niklasson A,
Domellöf M, Friberg LE, Borg J, Löfqvist C, Hellgren G, Smith LE,
Hård AL and Hellström A: Longitudinal infusion of a complex of
insulin-like growth factor-I and IGF-binding protein-3 in five
preterm infants: Pharmacokinetics and short-term safety. Pediatr
Res. 73:68–74. 2013.PubMed/NCBI View Article : Google Scholar
|
|
89
|
Chung JK, Hallberg B, Hansen-Pupp I,
Graham MA, Fetterly G, Sharma J, Tocoian A, Kreher NC, Barton N,
Hellström A and Ley D: Development and verification of a
pharmacokinetic model to optimize physiologic replacement of
rhIGF-1/rhIGFBP-3 in preterm infants. Pediatr Res. 81:504–510.
2017.PubMed/NCBI View Article : Google Scholar
|
|
90
|
Ley D, Hallberg B, Hansen-Pupp I, Dani C,
Ramenghi LA, Marlow N, Beardsall K, Bhatti F, Dunger D, Higginson
JD, et al: rhIGF-1/rhIGFBP-3 in preterm infants: A Phase 2
Randomized Controlled Trial. J Pediatr. 206:56–65.e8.
2019.PubMed/NCBI View Article : Google Scholar
|