Introduction
Calcaneus fractures represent >2% of all
fractures, and 90% of these fractures are found in men aged 21-45
years (1). After high-energy
trauma, intra-articular calcaneus fractures are common, and there
are a range of treatments for anatomic reduction and surgical
fixation. The most effective method to treat displaced
intra-articular calcaneus fractures is a hotly debated topic that
has piqued researchers' interest for the past two decades (2-4).
Only a few studies have proven that surgical treatment of
intra-articular calcaneus fractures improves functional results and
patient satisfaction when compared to non-surgical treatment
(5,6).
The extended lateral side approach is a common
technique in the surgical treatment of calcaneal fractures with
thalamic collapse, offering a good exposure of the fractured site.
However, it can be burdened by complications due to soft tissue
trauma (7). The most common
complications include dehiscence of the incision, calcaneus
osteomyelitis and sural nerve damage in 15% of the cases (8). Restoring the local anatomy, preventing
the appearance of the subtalar arthrosis and restoring the joint
function are the main objectives of the surgical treatment
(9). As a result, less invasive
procedures, such as limited-incision sinus tarsi open reduction and
internal fixation, percutaneous fixation, and arthroscopic-assisted
fixation have been developed in recent years (10,11).
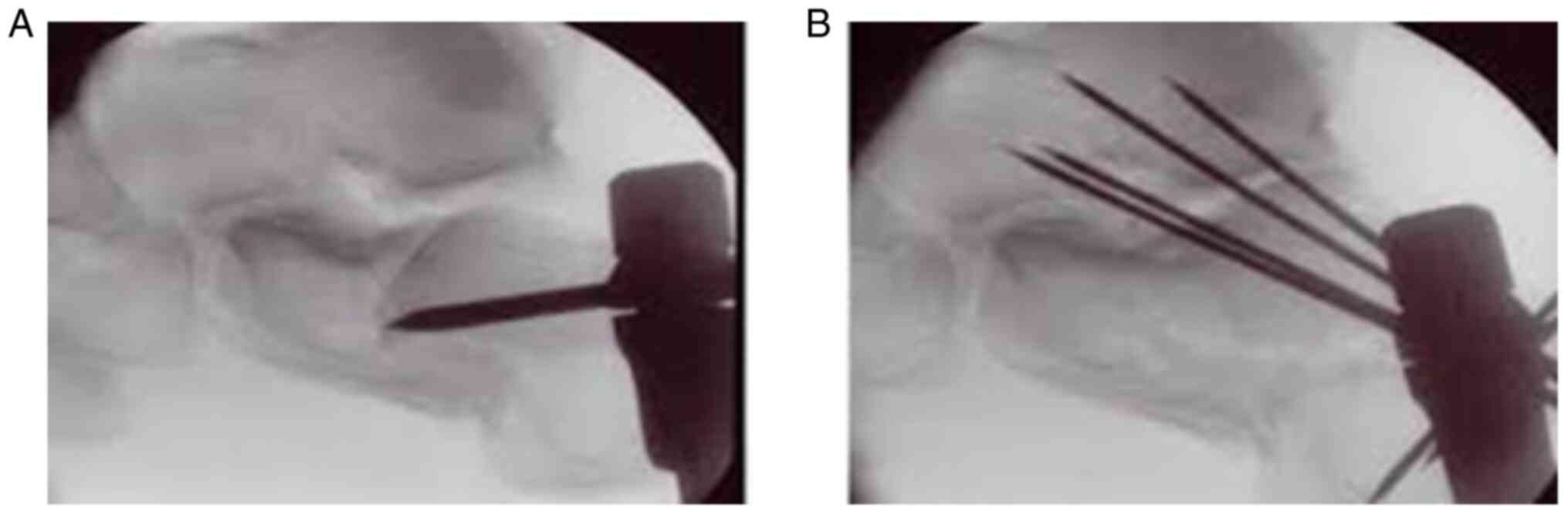
The minimally invasive technique consists of
positioning the patient in lateral decubitus, with the knee at 90˚
of flexion (12). The minimum
calcaneal lateral approach is 5 cm proximal and in line with the
base of the fifth metatarsal to provide lifting the collapsed
thalamic surface, followed by introduction of percutaneous K. wires
and screws under roentgenographic guidance (Fig. 1) (13). Stabilization of the fracture is
achieved following restoration of the thalamic surface with a
steinmann nail, K. brooches or percutaneous screws. To prevent
migration of the wires, as well as to give an additional stability
to the fracture, the K. brooches are stabilized in the cuboid or
talus bone (14).
The present study aimed to compare patients who were
treated with minimally invasive osteosynthesis through a minimum
lateral approach and internal fixation with patients who were
treated using internal fixation, with an extended lateral side
approach in cases of intra-articular calcaneal fractures with
thalamic collapse. A total of 68 calcaneal fractures were
retrospectively analyzed with respect to surgical technique and
minimally invasive technique when compared with the classic
technique, and showed effective results regarding the reduction and
postoperative complication rates.
Patients and methods
This retrospective cohort study included 60 patients
(68 calcaneal fractures) for a period of 3 years (between January
2017 and December 2020). All patients were admitted and treated at
the Division of Trauma and Orthopedic Surgery of the Bucharest
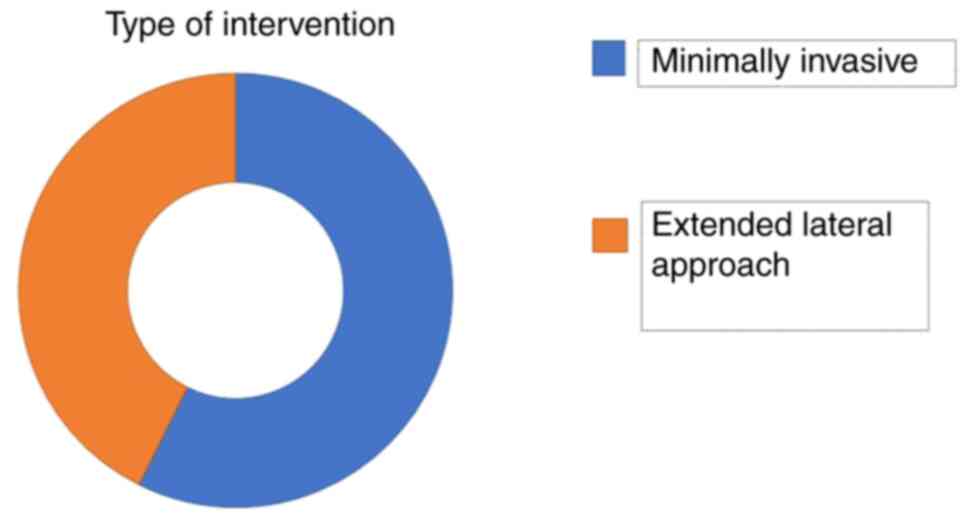
Emergency University Hospital. A total of 39 calcaneal fractures
were treated with minimally invasive osteosynthesis through a
minimum lateral approach and internal fixation with Kirschner
brooches and screws (group 1), while 29 calcaneal fractures were
treated with internal fixation, with the extended lateral side
approach (group 2) (Fig. 2). The
inclusion criteria were as follows: Heel fractures with
displacement involving the thalamic surface and closed fractures
without post-traumatic skin injuries (closed fractures). The
exclusion criteria were as follows: Patients with fractures without
displacement, extra-articular fractures and open fractures of the
calcaneus. Patients who failed to regularly attend the clinical
evaluations were also excluded from the present study.
Group 1 consisted of 36 patients (39 calcaneal
fractures), while group 2 consisted of 24 patients (29 calcaneal
fractures). There were seven women and 29 men in group 1, while in
group 2, there were four women and 25 men. The patients included in
the present study were aged 19-71 years, with an average age of
46.8 years.
Patients were evaluated preoperatively and
postoperatively by performing clinical and imagistic examinations,
with radiography scans of the anterior-posterior calcaneal profile
and computer tomography (CT). CT scans are performed prior to
surgery to decide the type of procedure used (15). The present study performed
preoperative and postoperative analyses of the Böhler angle on the
radiological profile for a good quantification of the reduction
control of the thalamic surface. During the evaluations at the
hospital and at the periodic examinations, local complications were
assessed in both groups. All patients were evaluated at 6 weeks, 3
and 6 months after surgery between January 2017 and December 2020.
Functional results were measured with The American Orthopedic Foot
and Ankle Society (AOFAS) score at 3 months after surgery for both
groups.
Results
There were 36 patients in group 1 (39 calcaneus
fractures) and 24 patients in group 2 (29 calcaneus fractures). The
early surgery intervention was the main option in choosing the
right time for the surgical procedure. In most cases, the early
surgical procedure was chosen (in 24 cases the early surgical
intervention was performed in the first 48 h); therefore, the
chances for local complications, such as blisters, were reduced
(16). The average time from
hospitalization to surgery was 2-3 days, and the associated lesions
were similar in both groups.
The most common injuries (7 cases, 11.6%) were
associated with fractures of the lower limb, followed by injuries
involving the head and spine (5 cases, 8.3%). These results were
consistent with previous findings (17). Patients were evaluated
preoperatively and postoperatively using clinical examinations and
radiology examinations, including x-rays in antero-posterior and
profile incidence and CT scans.
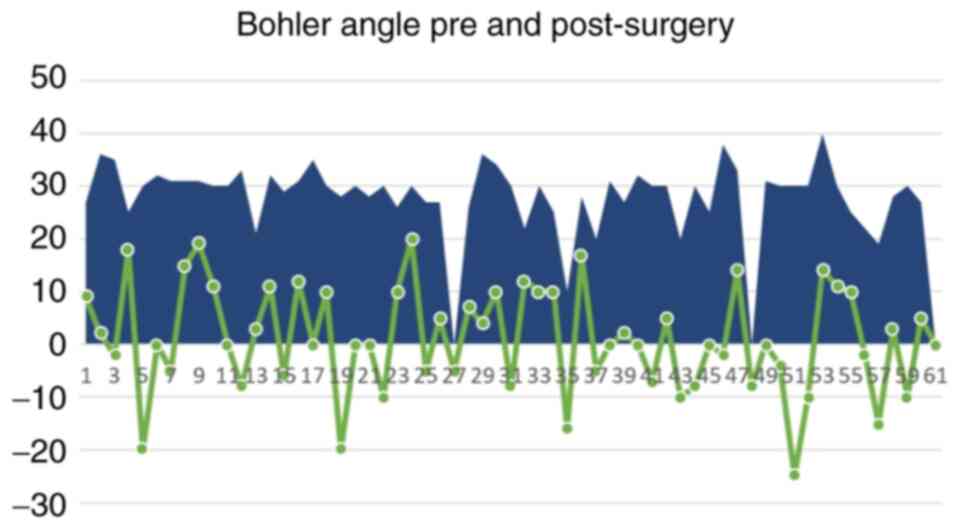
The most frequent investigation was the measurement
of the Böhler angle on the profile incidence of the x-ray,
preoperatively and postoperatively, which was used for reduction
control (Fig. 3). For a good
functional quantification, the AOFAS score at 3 months after
surgery was used in both groups. The average score was 82.95,
indicating good and excellent results. There were no significant
differences from a functional point of view between the two groups.
The average AOFAS score was 83.25 for group 1 and 85.65 for group 2
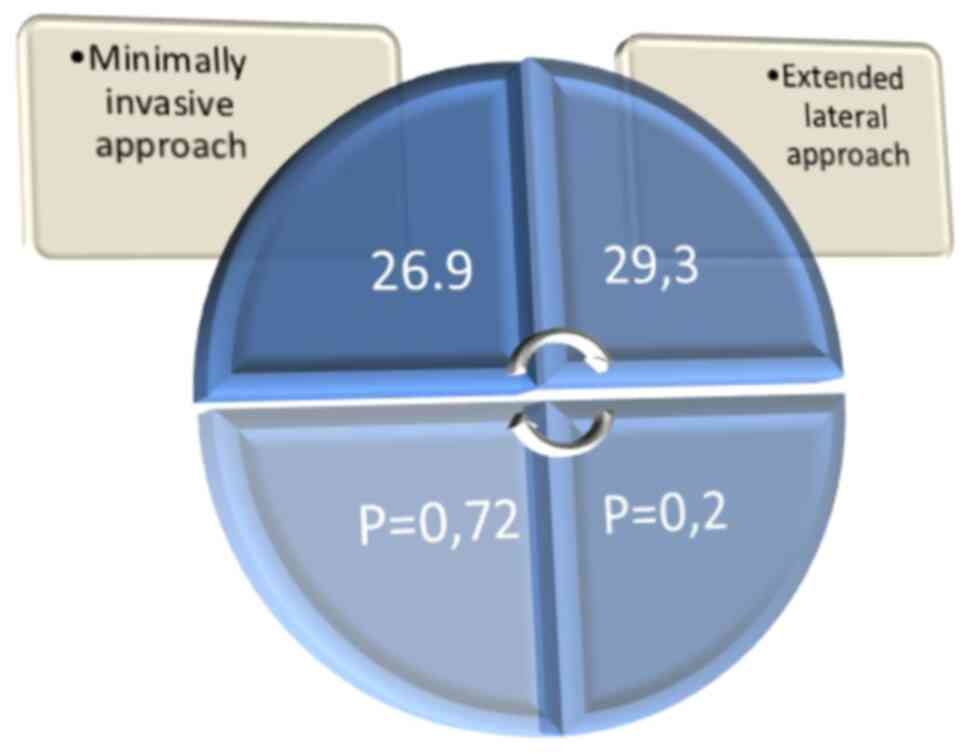
(P=0.179). The postoperative average values of the Böhler angle
were 26.9 degrees in group 1 and 29.3 degrees for group 2.
Patient distribution within both groups exhibited a
relatively symmetrical distribution, and there were no
statistically significant differences in the preoperative Böhler
angle and the applied techniques (Fig.
4). The period of antibiotic therapy after surgery was shorter
in group 1 compared with group 2 (2.6 days vs. 3.2 days; P=0.02)
(18). Furthermore, no septic
complications were recorded in group 1, while one case was recorded
in group 2. In the studied groups, bone grafts were used in only 7
cases (Fig. 5). The type of bone
graft used was autograft from the iliac crest due to better
integration (19). No differences
were observed from a statistical point of view for the post-surgery
restoration of the thalamic height (restoration of the Böhler
angle) and the collapse of the thalamic surface in the post-surgery
controls. A total of 11 patients were treated with Kirschner
brooches inserted only in the calcaneus and, in two cases,
migration of a brooch occurred. Notably, stabilization of the
fracture on the level of the cuboid and talus prevented early
migration of the osteosynthesis material. There were no cases of
migration of the osteosynthesis material in the fractures that were
stabilized by introducing Kirschner brooches to the talus or
cuboid.
Discussion
The results of the present study demonstrated that
preoperative evaluation using CT scans assisted with the
determination of the type of treatment used. Furthermore, early
surgery procedure (surgical treatment in the first 24 h) decreased
the rate of local complications. The most frequent lesions
associated in the two groups, considering the high energy trauma,
were found at the lower limbs and the spine. No statistically
significant difference was observed in the AOFAS functional score
at 3 months between patients treated with closed reductions
compared with those treated by extended lateral approach. The
satisfaction rates and functional scores when an extensile approach
is used are optimal at 3 months, but only after following strict
inclusion criteria (20). For
patients with Sander's type IV, peripheral vascular disease, prior
foot surgery, skin infections, patients with diabetes and known
smokers an extensive lateral approach may lead to important local
complications.
Notably, no significant difference was observed in
the Böhler angle between the minimally invasive technique and the
open reduction procedure (G1=26.9; P=0.72 and G2=29.3; P=0.20).
Taken together, the results of the present study suggest that the
minimally invasive technique is a reliable method, with good
functional postoperative results, which decreases the rate of local
complications.
Current literature presents similar results with the
current study when minimally invasive techniques are used for the
treatment of calcaneal fractures, with low local complication rates
and good functional results. One study compared these two
approaches in a group of 125 intra-articular calcaneal fractures
and found that the minimally invasive approach minimized
complications, and achieved and maintained extra-articular
reductions, as well as the standard extensile open reduction and
internal fixation compared with that for open reduction (21). Another important study, that
included a large number of fractures (112), found that the
minimally invasive approach had a significantly lower incidence
rate of wound complications and secondary surgeries compared with
that with the extensile approach (22).
In selected cases the minimally invasive approach is
a valuable method for the treatment of intra-articular calcaneal
fractures, with low complication rates and the results are
comparable to those treated with an extensile approach (23). These results are similar to those
obtained in the present study
Compared to other publications, the present study
has an important limitation, the small number of patients
recruited. Analyzing a larger group of patients will provide clear
results as to which technique is effective with respect to proper
reduction and lower complication rates.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in the published article.
Authors' contributions
AC, BC and CC were responsible for conceiving and
designing the study. AC, SI, BS and CC acquired the data and
performed the analysis. BC, CGS, MP and CO interpreted the data,
and wrote and revised the manuscript. BC and CO reviewed and edited
the manuscript. AC, BC and BS confirm the authenticity of all the
raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Schepers T, Ginai AZ, Van Lieshout EMM and
Patka P: Demographics of extra-articular calcaneal fractures:
Including a review of the literature on treatment and outcome. Arch
Orthop Trauma Surg. 128:1099–1106. 2008.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Gardner MJ, Nork SE, Barei DP, Kramer PA,
Sangeorzan BJ and Benirschke SK: Secondary soft tissue compromise
in tongue-type calcaneus fractures. J Orthop Trauma. 22:439–445.
2008.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sanders R, Fortin P, DiPasquale T and
Walling A: Operative treatment in 120 displaced intraarticular
calcaneal fractures. Results using a prognostic computed tomography
scan classification. Clin Orthop Relat Res. 290:87–95.
1993.PubMed/NCBI
|
|
4
|
Swanson SA, Clare MP and Sanders RW:
Management of intra-articular fractures of the calcaneus. Foot
Ankle Clin. 13:659–678. 2008.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Randle JA, Kreder HJ, Stephen D, Williams
J, Jaglal S and Hu R: Should calcaneal fractures be treated
surgically? A meta-analysis. Clin Orthop Relat Res. 377:217–227.
2000.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Thordarson DB and Krieger LE: Operative
vs. nonoperative treatment of intra-articular fractures of the
calcaneus: A prospective randomized trial. Foot Ankle Int. 17:2–9.
1996.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kiewiet NJ and Sangeorzan BJ: Calcaneal
fracture management: Extensile lateral approach versus small
incision technique. Foot Ankle Clin. 22:77–91. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Haugsdal J, Dawson J and Phisitkul P:
Nerve injury and pain after operative repair of calcaneal
fractures: A literature review. Iowa Orthop J. 33:202–207.
2013.PubMed/NCBI
|
|
9
|
Schenker ML, Mauck RL, Ahn J and Mehta S:
Pathogenesis and prevention of posttraumatic osteoarthritis after
intra-articular fracture. J Am Acad Orthop Surg. 22:20–28.
2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Weng QH, Dai GL, Tu QM, Liu Y, Lutchooman
V, Hong JJ and Yu Y: Comparison between percutaneous screw fixation
and plate fixation via sinus tarsi approach for calcaneal
fractures: An 8-10-year follow-up study. Orthop Surg. 12:124–132.
2020.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Sivakumar BS, Wong P, Dick CG, Steer RA
and Tetsworth K: Arthroscopic reduction and percutaneous fixation
of selected calcaneus fractures: Surgical technique and early
results. J Orthop Trauma. 28:569–576. 2014.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Hsu AR, Anderson RB and Cohen BE: MD
Advances in surgical management of intra-articular calcaneus
fractures. J Am Acad Orthop Surg. 23:399–407. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Rodemund C, Krenn R, Kihm C, Leister I,
Ortmaier R, Litzlbauer W, Schwarz AM and Mattiassich G: Minimally
invasive surgery for intra-articular calcaneus fractures: A 9-year,
single-center, retrospective study of a standardized technique
using a 2-point distractor. BMC Musculoskelet Disord.
21(753)2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Macey LR, Benirschke SK, Sangeorzan BJ and
Hansen ST: Acute calcaneal fractures: Treatment options and
results. J Am Acad Orthop Surg. 2:36–43. 1994.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Swords MP, Alton TB, Holt S, Sangeorzan
BJ, Shank JR and Benirschke SK: Prognostic value of computed
tomography classification systems for intra-articular calcaneus
fractures. Foot Ankle Int. 35:975–980. 2014.PubMed/NCBI View Article : Google Scholar
|
|
16
|
de Boer AS, van Lieshout EMM, Land FV,
Misselyn D, Schepers T, Hartog DD and Verhofstad MHJ: Soft tissue
complications and timing of surgery in patients with a tongue-type
displaced intra-articular calcaneal fracture: An international
retrospective cohort study. Injury. 49:425–429. 2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Galluzzo M, Greco F, Pietragalla M, De
Renzis A, Carbone M, Zappia M, Maggialetti N, D'andrea A,
Caracchini G and Miele V: Calcaneal fractures: Radiological and CT
evaluation and classification systems. Acta Biomed. 89
(1-S):138–150. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Modha MR, Morriss-Roberts C, Smither M,
Larholt J and Reilly I: Antibiotic prophylaxis in foot and ankle
surgery: A systematic review of the literature. J Foot Ankle Res.
11(61)2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Shaw KA, Griffith MS, Shaw VM, Devine JG
and Gloystein DM: Harvestingautogenous cancellous bone graft from
the anterior iliac crest. JBJS Essent Surg Tech.
8(e20)2018.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kavin K, Vijay S, Devendra L and Kamran F:
Patient satisfaction after open reduction and internal fixation
through lateral extensile approach in displaced intraarticular
calcaneal fractures (Sander's type II and III). J Clin Orthop
Trauma. 7:296–301. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
DeWall M, Henderson CE, McKinley TO,
Phelps T, Dolan L and Marsh JL: Percutaneous reduction and fixation
of displaced intra-articular calcaneus fractures. J Orthop Trauma.
24:466–472. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Kline AJ, Anderson RB, Davis WH, Jones CP
and Cohen BE: Minimally invasive technique versus an extensile
lateral approach for intra-articular calcaneal fractures. Foot
Ankle Int. 34:773–780. 2013.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Tomesen T, Biert J and Frölke JP:
Treatment of displaced intra-articular calcaneal fractures with
closed reduction and percutaneous screw fixation. J Bone Joint Surg
Am. 93:920–928. 2011.PubMed/NCBI View Article : Google Scholar
|