1. Introduction
In heart disease, medical imaging may provide an
objective basis for the diagnosis and suitable treatment of changes
in cardiac structure and minor pathological changes. The imaging
examination techniques of the coronary arterial lumen mainly
include coronary angiography (CAG), intravascular ultrasound
(IVUS), optical coherence tomography (OCT), angioscopy and
near-infrared spectroscopy (NIRS), which are able to clearly
display the internal structure and pathological changes of blood
vessels (1). These provide
clinicians with real-time dynamic observations, help reach the
correct diagnosis of the disease in a timely manner and provide
reasonable treatment strategies (Table
I).
 | Table IComparison of several catheter
technologies. |
Table I
Comparison of several catheter
technologies.
| Item | CAG | OCT | IVUS | Angioscopy | NIRS |
|---|
| Plaque volume | - | - | ++ | + | - |
| Calcification | ++ | ++ | +++ | - | - |
| Fiber cap | - | +++ | + | + | + |
| Lipid core | - | +++ | ++ | + | ++ |
| Inflammation | - | + | - | - | - |
| Thrombus | + | ++ | + | +++ | + |
| Vascular
remodeling | - | - | ++ | - | - |
| Stent
expansion | - | ++ | ++ | + | - |
| Intimal
hyperplasia | + | ++ | + | + | - |
CAG is a routine method used to assess the extent
and severity of coronary artery disease. Intracoronary imaging
methods, such as IVUS and OCT, may provide helpful information on
the morphology of the coronary arteries and may help evaluate the
size of the lumen, plaque load and composition in detail, which are
helpful for treatment planning (1). As presented in Table II, accumulating evidence suggests
that both IVUS and OCT are able to optimize the deployment and
outcome of the stent while improving patient prognosis,
particularly regarding the prognostic significance of the disease
(the left main disease) and anatomical structures that are
difficult to assess on imaging (2,3).
| Table IIComparison of the characteristics of
OCT and IVUS. |
Table II
Comparison of the characteristics of
OCT and IVUS.
| A, IVUS
modality |
|---|
| Advantages | Limitations |
|---|
| The development of
IVUS and the recognition of images are relatively mature | The currently
developed IVUS imaging catheter has poor passing ability for more
severe stenosis or twisted angular lesions |
| IVUS is able to
clearly display the intravascular structure and evaluate the plaque
composition | As different
tissues may have the same acoustic properties, the same density
value may be reflected in IVUS images |
| It may optimize and
guide the treatment of coronary intervention | The current IVUS on
the market has a low resolution and is not able to make accurate
judgments for small structures and lesions in blood vessels, and
corresponding changes in the lumen after stent implantation |
| It may be used to
study the mechanism of plaque progression or regression prior to
and after treatment, vascular remodeling and restenosis after stent
implantation | |
| B, OCT
modality |
| Advantages | Limitations |
| It has an
ultra-high resolution comparable to histology, allowing real-time
observation of small structures and lesions in blood vessels | The OCT imaging
process requires blocking or removal of the blood in the
corresponding detection vessel, which increases the difficulty of
the operation and limits its application in severe coronary
ischemic diseases |
| It is able to
accurately measure coronary luminal parameters, observe the
morphological characteristics of arterial intima and plaques, and
identify vulnerable plaques and macrophage infiltration prior to
surgery | OCT has a weak
penetrating ability and is not able to accurately analyze the whole
picture of the lesion. It is also difficult to measure the diameter
of larger blood vessels and evaluate vascular remodeling |
| It is able to make
the percutaneous coronary intervention process more refined and
optimize the immediate effect after stent implantation. It may
accurately observe the postoperative situation of various types of
stent implantation at the cross-sectional level | OCT is not able to
clearly identify the internal tissue covered by the thrombus
(particularly red thrombus) inside the blood vessel |
| | In the detection
after stent implantation, although OCT may clearly detect the stent
intima, it is still unable to distinguish the histological
characteristics of the stent surface covering the intima |
2. OCT evaluation of atherosclerotic
plaque-related factors
Atherosclerotic plaque is a term used to describe a
space-occupying lesion (thickening lesion) or loss of a three-layer
structure in the blood vessel wall on OCT images. The OCT
diagnostic criteria stated below refer to the internationally
recognized OCT consensus (4-6).
Types of plaques on OCT images
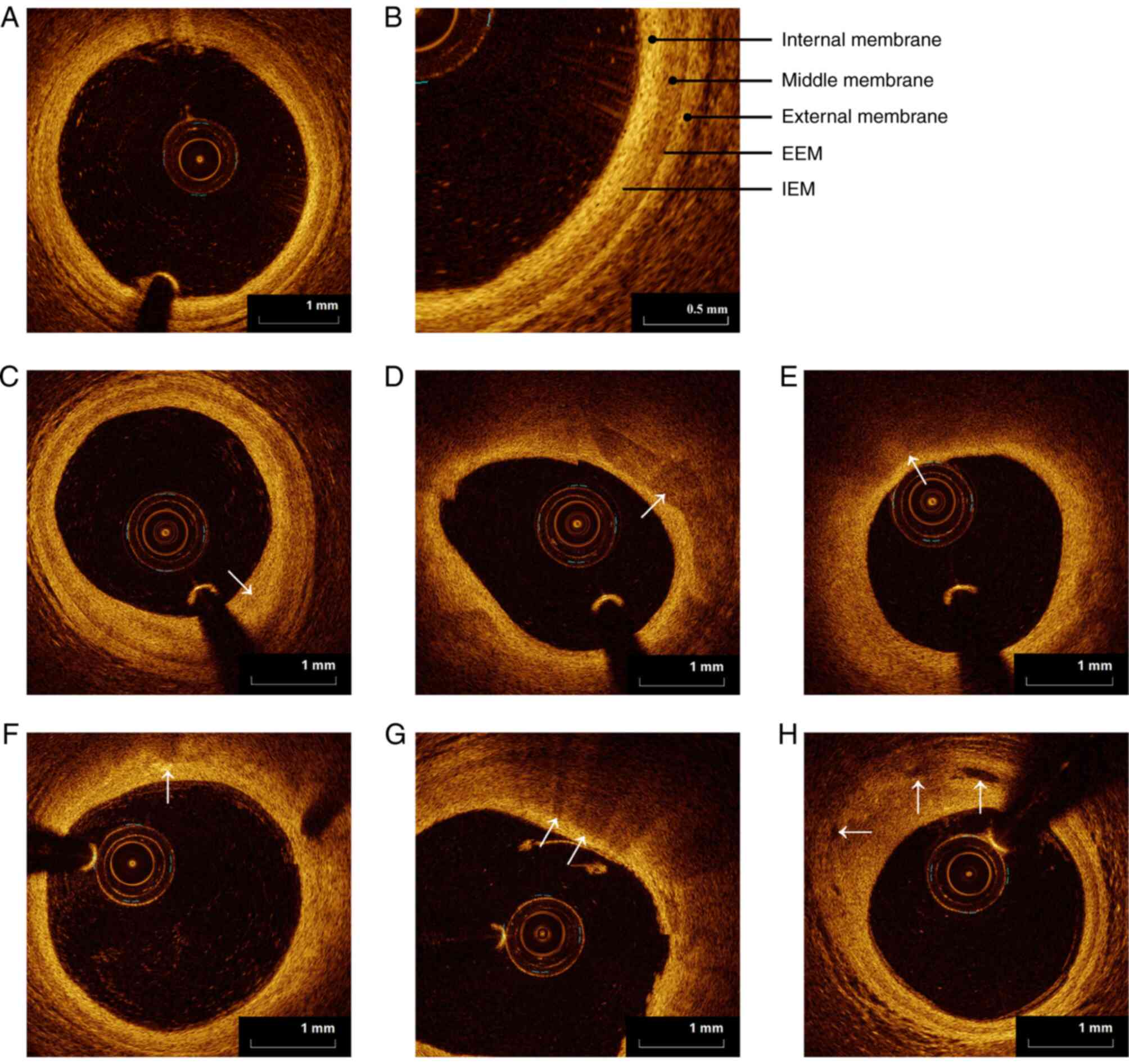
In the OCT image, the normal coronary artery wall is
characterized by a typical three-layer structure (Fig. 1A), which is composed of blood
intima, media and adventitia (Fig.
1B). The intima of the blood vessel has a high reflection
signal, the reflection signal of the media is usually low or weak
and the adventitia frequently exhibits an uneven high-reflection
signal. In OCT, the internal elastic membrane (IEM) is defined as
the boundary between arterial intima and media, while the external
elastic membrane (EEM) is defined as the boundary between arterial
media and adventitia (Fig. 1B).
Compared with traditional coronary angiography, OCT has marked
high-resolution characteristics. OCT is able to accurately identify
certain atherosclerotic plaques, adventitia, EEM and IEM, and may
accurately identify different tissue characteristics of plaques,
including fibers (Fig. 1C),
calcification components (Fig. 1D)
and lipids (Fig. 1E). At the same
time, the evaluation of the microstructure in the plaque by OCT is
unmatched by other imaging techniques, including cholesterol
crystals (Fig. 1F), macrophages
(Fig. 1G), microvessels (Fig. 1H) and microcalcifications. These
types of plaques have differences in scattering characteristics
(intensity of the reflected signal) and attenuation characteristics
(as the signal penetrates deeper into the tissue layer, the
intensity of the light signal gradually decreases through
scattering and absorption). Therefore, these plaques with different
properties will have corresponding characteristic changes on the
OCT image. As is presented in Fig.
1 and Table III, the plaques
displayed in OCT images include fibrous, calcified and lipid
plaques; microstructures within the plaques may also be observed
(5-7).
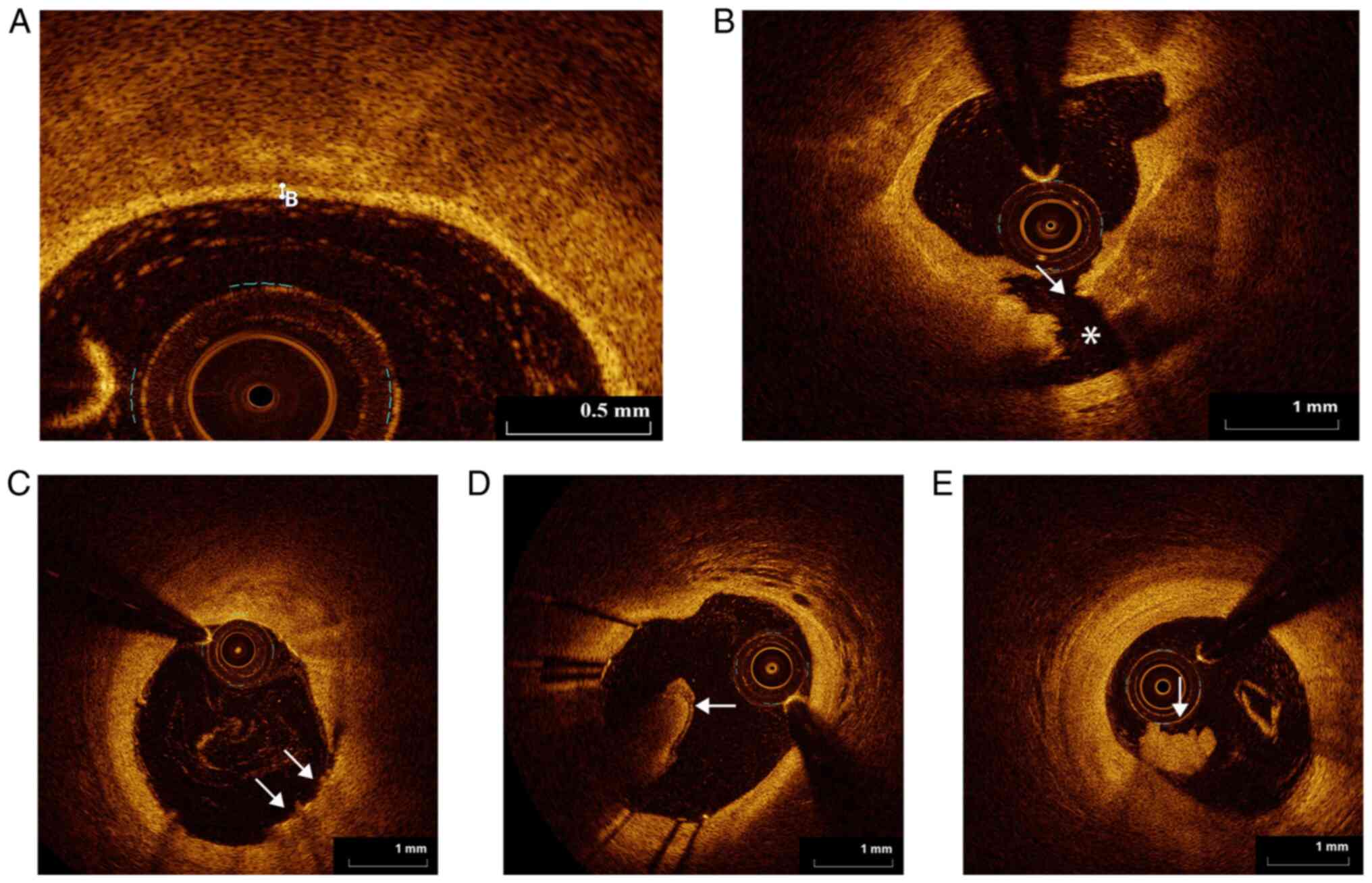
 | Figure 1Types of plaques in optical coherence
tomography images. (A) Diagram of normal coronary arteries (scale
bar, 1 mm). (B) Magnified image of normal coronary artery wall
(scale bar, 0.5 mm). Representative images of (C) fibrous plaque,
(D) calcified plaque, (E) lipid plaque, (F) cholesterol crystal,
(G) macrophage infiltration and (H) microchannel (arrows, scale
bar, 1 mm). EEM, external elastic membrane; IEM, internal elastic
membrane. |
| Table IIITypes of plaques in OCT images. |
Table III
Types of plaques in OCT images.
| Type of plaque | Feature | OCT image
performance | Sensitivity and
specificity (%) |
|---|
| Fibrous plaque | The pathological
feature is the pathological thickening of the intima, and an
intimal thickness of 600 µm is regarded as the limit value between
normal and pathological intimal thickening. In OCT, it is
characterized by low attenuation, homogeneity and fine texture | It has a relatively
uniform and highly reflective optical signal. If the inner elastic
membrane and outer elastic membrane cannot be seen in the lesion,
the lesion should be carefully considered as a fibrous plaque | 79, 97 |
| Calcified
plaquea | The pathological
feature is that calcium salt is deposited in the necrosis and the
fibrous cap, and the arterial wall becomes hard and brittle. In
OCT, it is characterized by low back reflection and low
attenuation, with sharp edges | It is manifested as
a sharp-edged low signal or uneven signal area. This definition is
suitable for large calcifications. It has not been determined
whether the above OCT definition is suitable for
micro-calcification | 95-96, 97 |
| Lipid plaque | Pathological
characteristics: Lipid deposition in the fat streak, smooth muscle
cells in the middle membrane migrate into the inner membrane, part
of the proliferation forms a fibrous cap, part of the phagocytosis
of lipids forms smooth muscle-derived foam cells, which evolve into
lipid plaques. In OCT, the edges are blurred or features are
illegible | The edge contour is
blurred in the weak optical signal area and there is a high signal
fiber cap on the surface of the low signal area. When diagnosing
lipid plaques deep in tissues, caution is warranted, as the
attenuation of OCT signal may also lead to the appearance of weak
signal areas. Therefore, OCT is more accurate at identifying lipid
plaques and lipid pools near the surface of the lumen. It is
generally thought that when the external elastic membrane cannot be
identified, OCT cannot measure the thickness, area or volume of the
lipid pool. In OCT images, the angle of the lipid pool is
frequently used to evaluate the size of the lipid pool | 90-94, 90-92 |
| Microstructure
within plaque | | | |
| Macrophage
infiltration | The rich lipid
components in macrophages may cause significant attenuation or
blocking of OCT signals | Highly reflective,
strongly attenuated dot or stripe structure, frequently forming
radial shadows behind high-signal dotted areas. At present, OCT
images mainly evaluate macrophages in fibrous plaques and lipid
plaques | - |
| Microchannel | From the adventitia
of the blood vessel to the intima, it communicates with the blood
vessels around the adventitia and finally extends to the coronary
artery lumen | A hole with a
diameter of 50-300 µm, weak signal and sharp edges, and may usually
be tracked in multiple consecutive frames. It has not yet been
determined whether these blood vessels are connected to the surface
of the lumen or originate from nourishing blood vessels | - |
| Cholesterol
crystals | It is usually
located in the fibrous cap and the core of lipid. necrosis | Thin linear regions
with higher signal strength and lower. attenuation | - |
Vulnerable plaque
As early as 1989, Muller et al (8) put forward the concept of ‘vulnerable
plaque’ to study acute cardiovascular disease. According to that
study, the leading cause of acute coronary syndrome (ACS) is the
rupture of an unstable plaque and secondary thrombosis. Kolodgie
et al (9) renamed the
‘vulnerable plaque’ to ‘thin-cap fibroatheroma’ (TCFA) after
combining the autopsy results of patients who died from cardiac
causes. This term refers explicitly to an atherosclerotic plaque
with macrophage infiltration and a necrotic center covered by a
fibrous cap with a thickness of ≤65 µm (Fig. 2). As presented in Table IV, Naghavi et al (10) provided the histopathological
definition and diagnostic criteria of vulnerable plaque (10-12).
| Table IVHistopathological definition and
criteria of vulnerable plaque (10-12).
A positive diagnosis was made when one of the main criteria and at
least two of the secondary criteria were met. |
Table IV
Histopathological definition and
criteria of vulnerable plaque (10-12).
A positive diagnosis was made when one of the main criteria and at
least two of the secondary criteria were met.
| A, Main
criteria |
|---|
| Histopathological
feature | Definition and
characterisation |
|---|
| Active
inflammation | Plaques with active
inflammation frequently have a large number of monocytes,
macrophages and T lymphocytes infiltrated and aggregated |
| Thin fiber cap and
large lipid core | The thickness of
the fibrous cap of these plaques is <100 µm and the lipid core
accounts for more than 40% of the total plaque volume |
| Exfoliation of
endothelium with platelet aggregation | These plaques are
characterized by superficial erosion with platelet aggregation or
cellulose deposition |
| Damaged or cracked
plaque | Most of them are
recent ruptures, which may be the cause of subacute thrombosis |
| Severe stenosis
(>90%) | The surface shear
force at severely narrowed areas has a vital role in the formation
of thrombus and occlusion |
| B, Secondary
criteria |
| Histopathological
feature | Definition and
characterisation |
| Superficial
calcified nodules | There are calcified
nodules in or near the fiber cap of the plaque. These nodules will
highlight the plaque and cause the plaque to rupture. This may not
be related to the severity of the calcification |
| Yellow shiny
patches | The yellow plaques
under angioscopy suggest large lipid cores and thin fibrous caps,
which are easier to rupture, but this indicator lacks sufficient
specificity |
| Bleeding in the
plaque | Red blood cell
overflow or iron deposits in the plaque may reflect the instability
of the plaque |
| Endothelial
dysfunction | Occurring in a
variety of acute and chronic disease states, active inflammation
and oxidative stress in vulnerable plaques are thought to be
related to endothelial dysfunction |
| Positive remodeling
of blood vessels | Studies have
indicated that positive vascular remodeling is an important sign of
vulnerable plaque |
A previous study used OCT to perform imaging
analysis on 26 cases with ST-segment elevation myocardial
infarction (STEMI) and 16 patients with stable angina pectoris. The
results indicated that patients with STEMI had a higher proportion
of TCFAs observed in the ‘culprit lesions’ (85 vs. 13%,
respectively; P<0.001), while the fibrous cap was thinner (57±12
vs. 180±65 µm, respectively; P<0.001) (13). In addition to TCFA, plaque rupture,
plaque erosion, calcified nodules, macrophage infiltration and
formation of nutrient blood vessels are all associated with the
occurrence of ACS. Thus, the evaluation and quantitative analysis
of vulnerable plaques may guide the risk stratification of clinical
conditions, as well as the protection and treatment of vulnerable
plaques, and help evaluate treatment efficacy.
Advantages and disadvantages of
methods used for evaluating vulnerable plaques
In the clinic, the coronary angiography results of
numerous patients are not able to display the underlying coronary
artery lesions, particularly culprit lesions that are not able to
identify thrombosis, whether they are caused by unstable plaque
rupture, plaque erosion or calcified nodules. As presented in
Table V, although several methods
may be used to detect vulnerable plaques, various detection methods
have their advantages and disadvantages (14,15).
The major factor that determines the vulnerability of plaques is
abnormal plaque structure and OCT is able to accurately identify
plaque components and microstructure within the plaque due to its
high resolution. The superficial calcification and
neovascularization of the five main and secondary criteria for
vulnerable plaques may be accurately analyzed qualitatively or
quantitatively, making it the most ideal imaging technique for
identifying vulnerable plaques.
| Table VAdvantages and disadvantages of
several methods for evaluating vulnerable plaques (14-15). |
Table V
Advantages and disadvantages of
several methods for evaluating vulnerable plaques (14-15).
| Modality | Advantages | Disadvantages |
|---|
| CAG | The method of CAG
is simple, it requires a short time, has fewer complications and
high diagnostic value. To a certain extent, the smoothness and
stenosis of the lumen may be observed | The effect of
foreshortening leads to underestimation of the length of the
stenosis of the lesion and there are large errors in the
measurement of the vascular structure at the bifurcation and the
eccentric plaque, and it is impossible to clearly determine whether
the plaque is a vulnerable plaque |
| Angioscopy | The surface of the
thrombus and plaque may be directly observed and the fibrous cap
rupture and thrombosis may be detected. At the same time, the color
of the plaque may be observed (white indicates mostly a stable
plaque and yellow mostly a vulnerable plaque) | The size of the
device is large. It may only be used to observe limited blood
vessels and is not able to observe the inside of the plaque and the
blood vessel wall. In addition, the blood flow requires to be
blocked, which may cause remote ischemia |
| IVUS | It is able to
clearly distinguish the structure of each layer of the blood vessel
wall, determine the diameter of the lumen, plaque volume, load and
vascular remodeling, and may distinguish the properties of plaque
such as lipid core, calcification and fibrous tissue | IVUS may only
display image information of plaque subcomponents and not able to
provide any quantitative detection. Only the calcified surface
structure may be observed and the display effect is not
optimal |
| | With strong
penetrating power, it may provide overall and comprehensive imaging
information for plaque assessment | The thickness of
the fiber cap cannot be accurately determined and the detection of
thrombus is not sufficiently sensitive |
| OCT | It has a high
resolution, may accurately evaluate the microstructure close to the
lumen, particularly in the unstable components of plaque, such as
the thickness of the fiber cap, macrophage infiltration, lipid
plaque size or plaque rupture. The fibrous cap thickness
measurement is in good agreement with histology | The penetration
ability is weak (1-2 mm) and its penetration depth is far less than
that of IVUS (8-10 mm). OCT is not able to provide an accurate
analysis of the full picture of the lesion. The lesion area covered
by the thrombus may not be used for an accurate assessment |
Identification of vulnerable plaques
by OCT OCT measures the thickness of the fibrous cap and may
identify the thin fibrous cap
The thickness of the fibrous cap is the decisive
factor for vulnerable plaques (16). The fibrous cap appears as a
high-density, low-reflection image on OCT. OCT may clearly
distinguish vulnerable plaques with thin fibrous caps (Fig. 2A). The thickness of the fragile
cap, which is widely accepted and recognized in clinical practice,
is 65 µm (17). TCFA, in the
context of OCT, is defined as a lipid-rich plaque with a thin
fibrous cap (the thinnest part is ≤65 µm), and the lipid component
in a plaque occupies ≥2 quadrants (17). A previous study performed a
histomorphological analysis of 295 coronary plaques (105 fibrous
plaques, 88 TCFAs and 102 ruptured plaques) in patients who
suffered sudden cardiac death. That study indicated that fibrous
cap thickness distinguishes these types of plaques. The critical
feature of the TCFA is that the plaque volume increases and the
stenosis of the coronary arterial lumen becomes increasingly
severe, which may lead to plaque rupture, causing an acute coronary
event (18).
Microchannels
A microchannel on OCT imaging is defined as a
non-signal luminal structure image of >3 frames that does not
communicate with the lumen (19).
The greater the number of microchannels (≥2), the higher the
proportion of TCFAs and the plaques with microchannels are more
likely to rupture (20). On the
one hand, microchannels may provide nutrients and oxygen to the
heart muscle; on the other hand, they may promote the influx of
lipids and inflammatory cell infiltration in coronary plaques. The
newly formed microchannels are fragile and easy to rupture, leading
to hemorrhage in the plaque, which eventually leads to a rapid
increase in plaque volume and narrowing of the lumen (20).
Rupture and erosion of the
plaques
On OCT, plaque rupture (Fig. 2B) manifests as intimal tearing,
destruction or plaque fibrous cap dissection. Erosion (Fig. 2C) refers to an irregular or
discontinuous vascular intimal surface with a tiny thrombus;
however, there is no fibrous cap damage or void formation (21). An OCT study systematically
classified and defined ACS culprit plaques and indicated that
plaque rupture, plaque erosion and calcified nodules under the OCT
definition accounted for 43.7, 31.0 and 7.9% of culprit lesions in
ACS (22).
Macrophages
Macrophage activity is a crucial feature for
evaluating plaque stability. Macrophages appear as dot-shaped areas
with abundant, apparent or fused signals on OCT and the noise
intensity of this area is stronger than the noise intensity of
background spots (21). It has
been confirmed that macrophages are associated with the severity of
clinical symptoms. A study used OCT to image culprit and
non-culprit lesions in a group of patients with stable angina
pectoris, unstable angina pectoris (UAP) and STEMI and
quantitatively analyzed macrophages in the plaques. The results
suggested that the cell density in patients with STEMI and UAP was
increased, the density of macrophages in the culprit plaque lesion
was higher compared with that of the non-culprit lesion and the
macrophage density in the ruptured plaque was greater compared with
that of the non-ruptured plaque (23).
Calcified nodules
Calcified nodules appear as low-density areas with
distinct edges, distinguished from the fuzzy edges of the fat
nucleus (21). Among them,
punctate calcification (calcification angle <90˚, length <10
mm) is considered to be one of the characteristics that affect
plaque stability. A study using OCT to observe the association
between punctate calcification and plaque vulnerability suggested
that plaques containing punctate calcifications have more
vulnerable plaque characteristics in patients with coronary heart
disease. The number of punctate calcifications in the plaque is
significantly correlated with the thickness of the fibrous cap;
furthermore, the number of punctate calcifications in the plaque is
also positively correlated with the incidence of microchannels
(24).
Positive vascular remodeling
A study by Vink et al (25) confirmed that positive remodeling of
the vascular lumen is related to the instability of the plaque;
however, due to the low penetration of OCT, relevant studies are
sparse.
Recognition of thrombus
OCT is able to recognize all types of thrombus and
it is more sensitive and specific compared with IVUS (Fig. 2). OCT may also clearly distinguish
between red and white thrombi in the lesion (21). The red thrombus is a strong
backscatter and appears as a radially shaded area with a high
signal on the surface and low or no signal posteriorly (Fig. 2D). The white thrombus is a low
backscatter, showing a homogeneous region of high or normal signal
with an irregular shape (Fig.
2E).
3. OCT guides interventional coronary artery
treatment
OCT has significant advantages in evaluating acute
lesions, guiding PCI and evaluating the mechanisms underlying
treatment failure.
Assessment of borderline lesions
Regarding the diagnostic threshold of OCT for
evaluating the degree of coronary artery stenosis and the treatment
strategy under the corresponding threshold, there is still no
consensus. A previous study compared the diagnostic efficacy of OCT
and IVUS for coronary artery disease with fractional flow reserve
(FFR) ≤0.8(26). The results
suggested that, with a minimal luminal area (MLA) of 1.95 mm² as
the cutoff value, OCT has moderate diagnostic power, with a
sensitivity of 82% and a specificity of 63%. With an MLA of 2.63
mm² as the cutoff value, the sensitivity decreases to 67% and the
specificity is 65%, and there is no statistically significant
difference between OCT and IVUS in terms of diagnostic performance
[area under the curve (AUC): 0.70, 95% confidence interval (CI):
0.55-0.83 to AUC: 0.63, 95% CI: 0.47-0.77; P=0.19]. In the subgroup
of small blood vessels (reference diameter <3 mm), OCT provided
significant advantages (AUC: 0.77, 95% CI: 0.60-0.89 vs. AUC: 0.63,
95% CI: 0.46-0.78; P=0.04). However, although OCT has higher
diagnostic power compared with IVUS in this subgroup, its
specificity for evaluating functional stenosis is low.
Furthermore, it is not sufficient to formulate a
treatment strategy solely based on the degree of stenosis or the
length of the lesion (27). The
nature of the plaque frequently provides important information and
it is also of far-reaching significance for guiding clinical
treatment. The advantage of OCT lies in the accurate identification
of thrombi, vulnerable plaques and minor lesions, such as intimal
erosions and tears. A number of coronary angiograms may indicate
borderline lesions with moderate stenosis. OCT examination may
uncover the presence of unstable lesions with a high possibility of
acute events. Therefore, the study of borderline lesions should
shift the focus to screening for high-risk vulnerable plaques and
ensure early intervention to reduce ACS events. The new generation
of OCT integrates the detection function of FFR and obtains
morphological and functional information at the same time. This
achieves the guiding effect of optimizing the treatment of critical
lesions (28,29).
OCT assists in guiding PCI
treatment
For patients requiring PCI treatment, surgeons may
use OCT to analyze the composition and characteristics of the
plaque in order to guide the pre-treatment or pre-dilation of the
diseased vessel and to help the interventionist select the length,
size and type of the stent or balloon.
Selection of the stent diameter
The principle of selecting the diameter of the stent
to guide CAG is that the ratio of the diameter of the stent to the
vessel diameter is 1.1:1. However, only the size of the stent is
selected based on the results of the angiography and the opinions
of different surgeons may vary. Since OCT may display the exact
blood vessel contour and vascular wall structure, the selection of
the diameter of the stent is more accurate compared with CAG
(28). In addition, OCT may
indicate the reference blood vessel diameter according to the
severity and stability of the vascular disease at both ends of the
lesion. The ILUMIEN III study selected different stent schemes
according to whether the media may be detected in the reference
segment of the OCT image (26). If
the media are visible, the minor media layer diameter (usually the
distal end) is measured as the reference value of the stent
diameter. If the media is not visible, the minimum diameter of the
reference segment automatically measured by the machine is selected
as the reference value of the stent diameter. In the era of
bioabsorbable stents, in theory, it may be more appropriate to
select the diameter of the stent based on the media to prevent the
thicker surface of the stent rod from protruding into the lumen and
affecting blood flow (30).
Determination of the requirement for
stent post-expansion
The requirement for post-expansion following stent
implantation is mainly determined by the attachment and expansion
of the stent. In principle, the expansion rate of the metal stent
should reach >80% and the expansion rate of the absorbable stent
should reach >90%. Poor stent expansion is closely associated
with stent restenosis and thrombosis in the stent. The ILUMIEN II
study confirmed that OCT and IVUS have comparable efficacies in
evaluating stent expansion (30,31).
If the stent displays poor expansion, a non-compliant balloon of
the same caliber should be used to apply high pressure and fully
expand the stent. The determination of poor stent adhesion by using
OCT is more sensitive compared with IVUS. In the OCT image, the
‘expansion rate’ may be used to evaluate stent expansion. In
general, the expansion rate is 90% critical for evaluating the
immediate underexpansion. The ILUMIEN I study determined that the
OCT detection underexpansion ratio may be as high as 41.3%
(28). The stent expansion rate is
calculated as follows:
Selection of the landing point of the
support
IVUS and OCT studies have indicated that, if the
stent is placed on an unstable plaque, it is prone to long-term
restenosis or edge dissection after implantation (30-32).
Of note, in theory, the stent should be placed on the regular blood
vessel segment, where angiography appears normal, OCT and IVUS
examinations still have specific load plaques (even TCFA), so OCT
examinations should be used and the selection is relatively stable.
The normal blood vessel segment is used as a reference to
accurately measure the diameter of the blood vessel, which not only
ensures the efficacy of stent implantation but also avoids
excessive damage to the blood vessel wall at the edges of the
stent.
OCT evaluation of the immediate effect
of stent PCI
The optimal stent implantation effect is that the
stent adheres to the wall and expands well. Furthermore, it is not
accompanied by dissection of the stent edge, tissue prolapse or
thrombosis in the stent. OCT may identify a higher rate of
complications after stent implantation, such as stent edge
dissection, tissue prolapse and stent thrombosis.
Stent expansion
In the drug-eluting stent (DES) era, poor stent
expansion is one of the fundamental reasons for in-stent restenosis
and thrombosis. A previous study indicated that, whether it is a
first-generation or second-generation drug stent, the minimum stent
area (MSA) is >5.0 mm2 (28). If the stent does not expand
properly, the incidence of thrombosis in the stent will increase
significantly within 1 year (33).
Particularly in cases with left main disease, the MSA goal is to
achieve circumflex branch opening >5.0 mm2, anterior
descending branch opening >6.0 mm2, left main trunk
end >7.0 mm2 and left main trunk body >8.0
mm2 (33). In general,
calcified lesions and plaques form on a background of heavier
eccentric fibrous lesions, prone to poor stent expansion.
Therefore, adequate pretreatment should be performed for such
lesions. For instance, eccentric fibrous plaques should be fully
pre-dilated and severely calcified lesions should be treated with
rotational atherectomy or balloon incision (34). After PCI, poor stent expansion
should be actively treated. Non-compliant balloons may be used to
expand the stent by applying high pressure and OCT should be
performed again after expansion to determine the adequacy of
expansion.
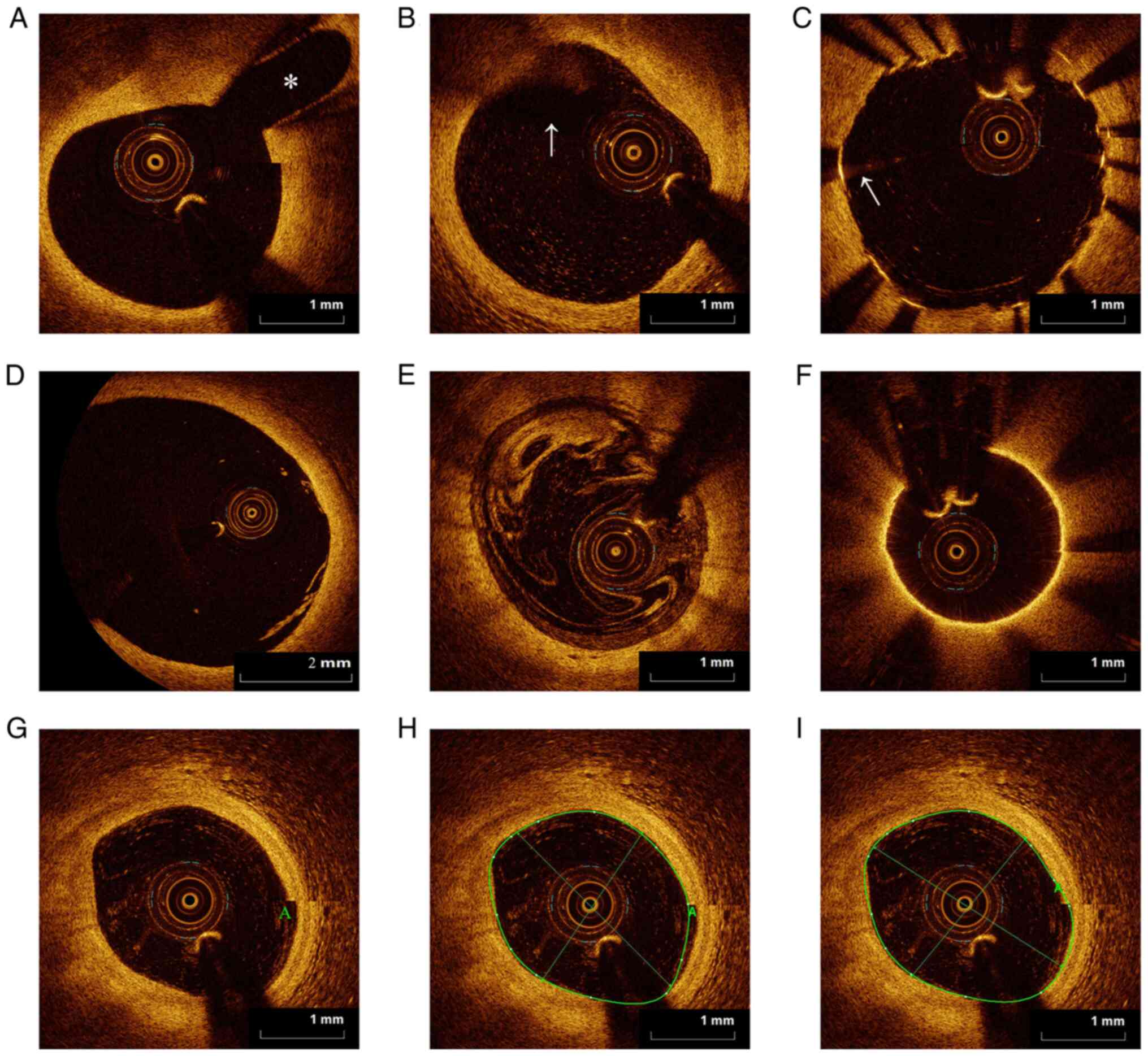
Stent malapposition (SM)
SM on OCT images means that the longitudinal
distance from the stent trabecular surface to the lumen surface is
greater than the thickness of the stent trabecula (if there is a
polymer on the stent trabecula, it should also be included in the
measurement). When the distance between the two is >200 µm, this
is defined as significant adhesion failure (Fig. 3A and B). Clinically, if the stent area poorly
adhered to the wall is small and is not accompanied by poor stent
expansion, no treatment is required (34). However, in the presence of SM and
poor stent expansion, MSA <5.0 mm2 post-expansion is
recommended to ensure adequate stent expansion and adherence. In a
follow-up study of OCT, poorly adhered stent filaments may also
gradually be covered by endothelial cells and completely fuse with
the vessel wall (35). Previous
studies have performed OCT serial detection on 78 blood vessel
segments where the stent wire was poorly attached immediately after
surgery. The 6-month follow-up after the operation suggested that
the volume of poorly adhered stents immediately after the operation
decreased significantly and 75% of the stents that were poorly
adhered immediately after the operation were completely fused with
the vessel wall. This indicates that SM may delay the healing
process of damaged blood vessels. When the distance between the
stent wire and the vessel wall is narrow, the proliferating
neointimal tissue may frequently cover the distance to the poorly
adhered stent wire (35,36).
Dissection of the stent edge and
tissue prolapse
Following stent implantation, damage to the blood
vessel wall often occurs at the edge of the stent. OCT is able to
detect 37.8% of stent edge dissections (37). The edge dissection of the stent may
be divided into intimal tear and media dissection. Intimal tear
refers to the sheet-like lifting of the intima after stent
implantation, without any obvious rupture of the plaque fibrous
cap. Media dissection refers to the intimal tear extending to the
media of the coronary artery, which may lead to intracoronary
hematoma. In general, the severity of interlayer dissection, the
angle at which the interlayer occurs and the length measured on the
vertical axis images are taken into consideration. Stent edge
dissection is closely associated with in-stent thrombosis and poor
prognosis. Compared with superficial layer dissection, stent edge
dissection involving the deep layer of the coronary artery wall
significantly reduces the survival rate of patients without
clinical events (38).
On OCT imaging, tissue prolapse is defined as tissue
protruding from the lumen between the trabeculae of the stent after
the stent is implanted. Tissue prolapse may be divided into plaque
prolapse (Fig. 3C) and thrombosis
(Fig. 3D). Plaque prolapse usually
has a smooth surface without apparent signal attenuation, while
thrombosis usually has an irregular surface with solid attenuation.
The incidence of tissue prolapse after stent implantation is high.
It was reported that 95% of stents may be detected by OCT
immediately after implantation (30). The occurrence of tissue prolapse
after PCI is associated with the nature of the plaque. When the
stent is located on the TCFA or necrotic nucleus defined by OCT,
tissue prolapse is likely to occur (39). Irregular tissue prolapse is an
independent predictor of adverse clinical events after PCI
(Table VI).
| Table VITreatment principles for vascular
dissection after stent implantation and the main treatment
principles for tissue prolapse in the stent after stent
implantation. |
Table VI
Treatment principles for vascular
dissection after stent implantation and the main treatment
principles for tissue prolapse in the stent after stent
implantation.
| A, Principles of
treatment of vascular dissection after stent implantation |
|---|
| Type of vascular
dissection | Processing
principle |
|---|
| For intimal
dissection with no clinical symptoms, no ischemic ECG changes, TIMI
blood flow grade III | No special
treatment |
| For dissection
involving the vascular media, even intra-vascular hematoma or
vascular rupture | Implant the stent
immediately |
| The severity lies
between the above two | If the edge of the
stent dissection is >60˚, the length of the dissection is >3
mm, the distal TIMI blood flow is affected, and the MLA is <5.0
mm2, the stent should be further implanted to avoid
serious clinical consequences |
| B, Major treatment
principles of tissue prolapse in the stent after stent
implantation |
| Type of tissue
prolapse | Processing
principle |
| The amount of
tissue prolapse in the stent is small, the protruding lumen is
<200 µm, prolapsed area is <10% of the area in the stent, the
stent expands well and the TIMI blood flow is grade III | Should not
intervene temporarily, postoperative antiplatelet therapy should be
strengthened |
| The amount of
tissue prolapse in the stent is large, the protruding lumen >200
µm, the prolapsed area is ≥10% of the internal area of the stent
and the stent is poorly expanded | Use of a balloon
with the same diameter as the stent for high-pressure
expansion |
| The effect of the
above two methods is still not obvious | It may be
considered to implant a stent in the prolapsed tissue to cover the
prolapsed tissue to increase the effective lumen area |
Immediate stent thrombosis
Immediate stent thrombosis on OCT appears as an
irregular mass that protrudes into the lumen immediately after
stent implantation. Although stent thrombosis is rare, it
frequently leads to PCI complications with severe clinical events.
At present, OCT is the only imaging technique other than angioscopy
that may identify ~100% of thrombi. For stent thrombosis detected
by OCT, corresponding treatment measures should be taken according
to the severity, the patient's clinical manifestations and the
hemodynamic impact. First, for immediate stent thrombosis with low
thrombus volume, no clinical symptoms, no ischemic ECG changes and
no severe hemodynamic disorders, anticoagulation and dual
antiplatelet therapy should be administered. If the volume of the
thrombus in the stent is larger, the patient has obvious ischemic
symptoms and severe hemodynamic disorders, a suction catheter may
be used for thrombus aspiration to reduce the load of the thrombus
in the stent. If there is no apparent improvement after aspiration,
following intracoronary administration of a dose of tirofiban, a
balloon with the same diameter as the stent should be used for
low-pressure expansion. If the effect of the aforementioned method
is still not sufficient, re-implanting a stent at the thrombus
should be considered. The immediate causes of thrombosis in the
stent (such as poor expansion, immediate SM and dissection of the
stent edge) identified on OCT should be dealt with accordingly as
described above (40).
4. OCT guides complex lesion management
Left main disease
Left main coronary artery lesions refer to lesions
with stenosis of the left main coronary artery by ≥50% on CAG. This
is one of the common clinically complex lesions. In recent years,
with the advances in technology, left main bifurcation lesions are
no longer considered to be a contraindication for PCI treatment
(Table VII) (27,41).
| Table VIISeveral features used in the
examination of left main lesions (4,27,41). |
Table VII
Several features used in the
examination of left main lesions (4,27,41).
| A, CAG |
|---|
| Consideration | Comments |
|---|
| Judement of the
degree of stenosis | Surgeons have
different judgments on the degree of stenosis of coronary
angiography and they frequently underestimate the degree of
stenosis of coronary artery disease |
| Diffuse left main
disease | When the left main
disease is diffuse, it is difficult for angiography to accurately
reflect the diameter of the blood vessel, which affects the choice
of stent diameter and ultimately affects the effect of PCI |
| Left main ostium
imaging | During the left
main ostium imaging, the contrast agent flows back to the aorta,
resulting in unclear visualization of the coronary ostium |
| Left main artery
emergence | When the left main
artery emerges from the aorta with an acute angle or the left main
body is curved, the severe stenosis is easily missed by coronary
angiography |
| Coronary
angiography | Coronary
angiography is not able to provide any detailed information on
plaque composition and immediate effects after PCI |
| B, IVUS |
| Consideration | Comments |
| Preoperative IVUS
examination | Preoperative IVUS
examination may confirm stenosis of the left main lesion, the
length of the lesion and the characteristics of the plaque |
| Intraoperative
IVUS | Intraoperative IVUS
may determine the position and accuracy of the reset side
guidewire, exclude the guidewire from passing outside the stent and
avoid serious deformation of the stent |
| Postoperative
IVUS | Postoperative IVUS
examination may clarify the immediate effect of the stent and
postoperative complications, and reduce the occurrence of
postoperative cardiovascular adverse events |
| IVUS in combination
with FFR | IVUS combined with
FFR may guide the choice of treatment strategies for borderline
left main lesions |
| C, OCT |
| Consideration | Comments |
| OCT scanning
speed | The scanning speed
of the left main disease is faster (25 mm/sec), which may reduce
the inter ference of the cardiac cycle on coronary artery
imaging |
| Accuracy of area
and diameter measurement | Measurement of the
smallest lumen area and diameter and the evaluation of the
composition are more accurate (4) |
| OCT evaluation of
effects and OCT sensitivity | OCT may clearly
evaluate the immediate effects, vascular wall damage and
complications after PCI, and is more sensitive than IVUS |
|
ILUMIEN™OPTIS™
system real-time three-dimensional imaging | The
ILUMIEN™OPTIS™ system may perform real-time
three-dimensional imaging of the left main lesion, which may finely
determine the extent, length, stenosis and reference blood vessel
diameter of the lesion, and it is convenient for the surgeon to
observe and analyze the blood vessel from multiple angles to make a
correct assessment |
|
ILUMIEN™OPTIS™
system integration of FFR | The
ILUMIEN™OPTIS™ system integrates the FFR
function, so that it has both morphological and functional
evaluation functions, so as to more comprehensively evaluate the
coronary artery function |
| OCT transmission
depth | OCT transmission
depth is small and the remodeling changes of the blood vessels and
the surrounding conditions of the blood vessels cannot be
evaluated. This is the drawback in guiding PCI treatment of the
left main disease |
Bifurcation lesions
A bifurcation lesion of the coronary artery refers
to a >50% stenosis of the opening of the main vessel and branch
vessel. This is a complex type of lesion with a high failure rate
of coronary stent implantation (42). Atherosclerosis readily develops at
the bifurcation of the blood vessels due to the high shear stress
of blood flow.
Preoperative OCT examination may accurately measure
the stenosis of the main branch and branch opening, the length of
the lesion and the distribution and the nature of the plaque, and
it may help the surgeon select the appropriate interventional
device and branch stent treatment strategy. It should be determined
whether single-stent or multi-stent technology may be used or
whether branch vessels require to be protected. OCT indicates that,
for the proximal wall of the branch in which TCFA frequently
occurs, the double-stent technology (such as crush T-stenting) is
required. The multi-layer stent trabecular attachment site may
easily lead to poor stent adhesion, uneven drug distribution and
vulnerable plaques. Rupture of the stent may lead to embolism of
the distal branch and the occurrence of the ‘no-flow’ phenomenon
(43). In terms of imaging, it may
prevent the implantation of the stent on the TCFA. OCT may be used
to guide the branch guidewire to enter the branch from the middle
or distal mesh to achieve a satisfactory balloon anastomosis and
expansion of the stent to adhere to the vascular wall.
OCT examination after surgery may be performed to
observe the adhesion and endothelialization of the stent at the
bifurcation, thereby reducing the occurrence of thrombosis in the
stent. In addition, the real-time 3D imaging function of the
ILUMIEN™ OPTIS™ OCT system may also reveal
the spatial distribution and structure of blood vessels, analyze
the blood vessels at all angles freely in space and guide the
re-entry of the guidewire (44).
It was reported that 3D-OCT-guided stent implantation for
bifurcation lesions is feasible and may reduce the occurrence of
stent malapposition (45).
Therefore, this application should be considered as a guidance in
the clinical treatment of bifurcation lesions.
Chronic occlusive disease
In recent years, with the development of
interventional devices, considerable progress has been made in the
treatment of chronic total occlusion (CTO), but the success rate of
CTO intervention remains relatively low and faces several
challenges (46). In this complex
disease, the information provided by OCT may affect successful
completion of the operation.
There have been reports of in vitro
experiments using the forward-looking OCT system to perform
multi-axis imaging of occluded blood vessels to construct
cross-sectional images of the affected vessels (47). OCT is able to distinguish between
different levels of the occluded lumen and vessel wall, and it is
possible to identify microchannels. This information may be used to
guide the wire through the lesion. Once the guidewire has passed
through the occluded segment, OCT may detect the plaque component
that caused the occlusion.
In addition, an OCT study indicated that the intimal
repair of CTO lesions is delayed after stent implantation; thus,
OCT may help determine the time limit of dual antiplatelet therapy
following stent implantation in CTO lesions (48). It should be pointed out that the
currently available evidence on OCT as a method for guiding the
treatment of CTO lesions is insufficient and further research is
required.
Calcified lesions
When severe annular calcification is detected on
OCT, direct implantation of stents should be avoided and
pre-dilation or experimental expansion strategies should be
considered first (49). Balloon
cutting or coronary atherectomy may be used in short calcification
rings. It should be noted that there is currently no clear cutoff
value (calcification angle, length or thickness) that may be used
as an indication for balloon incision or coronary atherectomy
(50).
Calcified lesions limit the expansion of blood
vessels and balloons; therefore, calcified lesions frequently lead
to poor stent expansion (49). OCT
may accurately assess the expansion of the stent, thereby guiding
the selection of a suitable post-expansion balloon. It was
indicated that the calcification angle and calcification area
measured by OCT are negatively correlated with the MSA and the
minimal stent diameter after DES expansion (49).
5. Application of OCT in the post-stent
implantation follow-up
OCT has significant advantages in assessing the
repair of blood vessels after stenting and the mechanisms
underlying treatment failure.
OCT assessment of intimal
coverage
The thickness of the stent intima measured by OCT
has been indicated to be highly correlated with the thickness of
the tissue (r=0.85, P<0.01), with excellent repeatability of the
thickness measurement between individuals or the same intima
(51). OCT has a sensitivity of
80% and a specificity of 95% for detecting incomplete stent intimal
coverage. For stent neointima (Fig.
3E) with a thickness of >100 µm, it may be divided into
three categories according to OCT image characteristics: The first
is characterized by homogeneity, high reflection and a relatively
uniform signal, with no local attenuation signal. The second
involves layered, centripetal, double-layer or multi-layer optical
signals, the near lumen side usually has high-reflection signals
and the far cavity side usually has low-reflection signals Finally,
the third category is characterized by heterogeneity, with low
reflection and an uneven signal, with local solid signal
attenuation.
With the advancement of technology, OCT study
hasdetermined that the second-generation everolimus-eluting stent
(EES) achieves significantly faster intimal repair compared with
the first-generation sirolimus-eluting stent (SES) and the surface
endothelialization is relatively complete (52). This discovery has prompted several
scholars to consider that the existing dual-antiplatelet therapy
strategy may be changed. It is recommended that the current
dual-antiplatelet therapy is shortened to 9 months and certain
scholars even proposed to shorten it to 6 months (53). It was also reported that, in
patients with EES implantation, the 6-month dual-antibody treatment
is not inferior to the 12-month treatment plan (54). The application of OCT to evaluate
direct intimal coverage appears to be highly promising for guiding
the clinical standards for dual-antibody treatment after stenting.
To date, certain scholars have proposed using OCT to guide
individualized dual-antibody therapy and examined whether it is
possible to use OCT to evaluate the trabecular coverage of the
stent to adopt an individualized antiplatelet therapy plan, and
whether the characteristics of intimal tissue observed on OCT may
be used in individualized dual anti-platelet therapy and basic
anti-atherosclerosis treatment programs (51). However, due to the lack of a
specific evaluation model and a unified evaluation plan, these are
issues worthy of further consideration. Since the incidence of
in-stent thrombosis is inherently low, a large sample size is
required by further clinical studies to confirm the advantages of
OCT in guiding antiplatelet therapy, which is associated with major
practical difficulties. However, with the increase in follow-up
data of OCT stents, real-world registration studies may help solve
this problem and even change the existing guidelines on the
recommended duration of dual-antibody application after
stenting.
In terms of identifying the potential clinical risks
and intervention factors of the neointima, OCT is a powerful tool
that has achieved significant research results. Kubo et al
(55) reported that intimal stent
coverage was significantly delayed in patients with UAP. Kochman
et al (56) used OCT to
follow up the DESs and bare metal stents (BMSs) of diabetic
patients for 2 years and observed that the intima remained
uncovered 2 years after the DES was implanted. Furthermore, the
intimal coverage of the stent is unrelated to whether the patient
has diabetes. A Japanese clinical study on OCT indicated that
atorvastatin treatment may affect the migration of endothelial
progenitor cells (EPCs), thereby accelerating the repair and
endothelialization of the endothelium after SES implantation. In
addition, different statin drugs may affect EPC migration (57). There are apparent differences in
the promotion effect of membrane repair. These studies have
provided research directions and intervention targets for promoting
stent intimal healing and reducing long-term stent-related clinical
problems from the perspective of OCT.
OCT assessment of
neoatherosclerosis
It was initially suggested that, at 6-12 months
after BMS implantation, neointimal hyperplasia caused lumen
stenosis. As the tissue matures, the lumen area tends to stabilize
or even improve (58). However, an
increasing number of studies have confirmed that the stable
fibrotic endometrial tissue in these stents may gradually develop
into unstable atheromatous plaque tissues, leading to late stent
failure (58-60).
Complex atherosclerosis that occurs in the neointimal tissue after
stent implantation is defined as neoatherosclerosis (Fig. 3F). Regarding the phenomenon of
neoatherosclerosis plaques in stents, the underlying mechanisms and
clinical intervention methods remain to be explored, which is an
important direction for future basic and clinical research.
OCT may serve an important role in the mechanism and
intervention of neoatherosclerosis. The neoatherosclerosis in DES
is likely associated with severe local inflammation in the early
stage after stent implantation. Furthermore, neoatherosclerosis is
mainly distributed around the trabeculae. The occurrence of plaque
in a bare stent is gradually formed after the stent intima
proliferates to a certain thickness. The new plaque is at a certain
distance from the trabecula of the stent, which is similar to the
occurrence of coronary plaque in situ. An OCT study
demonstrated that the progression of neointimal atherosclerosis
after stent implantation is associated with the progression of an
in situ plaque in the autologous coronary artery (60). This result is expected, as the new
plaque has the same risk as the in situ plaque. In addition,
similar to in situ plaques, new blood vessels have an
essential role in the occurrence and development of new plaques in
stents, particularly in diabetic patients (61,62).
An OCT study determined through multiple regression analysis that
low-density lipoprotein-cholesterol levels >70 mg/dl, smoking
and chronic kidney disease are risk factors that promote the
occurrence of new plaques. By contrast, angiotensin-converting
enzyme inhibitors are effective defense pathways that prevent the
occurrence of new plaques (63).
Therefore, this type of drug may inhibit the formation of
neoatherosclerosis plaques to a certain extent. Traditional
cardiovascular risk factors, such as sex, hypertension, diabetes
and hyperlipidemia, cannot predict the occurrence of
neoatherosclerosis plaques following stent implantation (64); this demonstrates that, although the
histological and imaging characteristics of neoatherosclerotic
plaques and primary atherosclerosis are similar, there may be
marked differences in the underlying mechanisms. With the
advancement of evaluation methods, early screening of
neoatherosclerosis plaques and active control of related risk
factors may help improve the long-term prognosis after PCI.
OCT determines the cause of stent
failure
The main reasons for stent failure are in-stent
restenosis (ISR), intra-stent thrombosis, SM and stent fracture
(SF). However, it is challenging to discover the pathological
mechanisms leading to the failure of stent implantation by
angiography alone. The use of OCT to follow up patients with late
stent implantation failure may help elucidate their types and
underlying mechanisms, which is conducive to the improvement of
stent design and the optimization of surgical procedures, thereby
preventing stent failure caused by various mechanisms.
ISR
ISR may be divided into imaging and clinical
restenosis. Following stent implantation, the former refers to the
CAG performed to confirm that the stent implantation segment loses
≥50% of the lumen. On OCT images, ISR means that the area in the
neointima of the stent exceeds 50% of the area of the stent. OCT
may quantitatively measure ISR at the lesion level, mainly by
measuring the thickness of the neointima, the area of the
neointima, the calculated volume of the neointima and the volume of
neointimal hyperplasia obstruction rate (the ratio of the average
neointimal volume to the average stent volume) to assess the degree
of ISR.
Previous studyreported that coronary artery balloon
dilatation, paclitaxel drug-coated balloon or DES implantation may
be performed for ISR (65). During
a follow-up over ~200 days, the histological characteristics of the
stent intima detected by OCT were indicated to be associated with
the reappearance of ISR and the prognosis of restenosis with
different tissue characteristics was significantly different with
different treatment methods. It is suggested that the causes of
restenosis of clinical stents are different (intimal hyperplasia,
atherosclerosis and stent thrombosis) and the treatment methods for
restenosis should also be different. Therefore, OCT examination may
help analyze the causes of ISR and the degree of stenosis and help
guide treatment planning.
Stent thrombosis
The detection sensitivity of OCT for stent
thrombosis is higher compared with that of CAG and IVUS. OCT may
identify thrombi and distinguish between red and white thrombi by
the thrombus components, which is of significant reference value
for assessing the composition of acute stent thrombosis. OCT may
detect small thrombi attached between the stent wires that have not
adhered to the wall and provide accurate measurement of the size
and length of the stent and the luminal area of the blood vessel.
In addition, OCT has a specific guiding effect on the dosage and
course of clinical antithrombotic drugs (66).
Guagliumi et al (67) studied 18 patients with advanced
stent thrombosis in DES. All patients underwent thrombus aspiration
prior to OCT and IVUS examinations. It was determined that the
non-filament coverage rate in the stent thrombosisgroup was 12.27%,
which was significantly higher compared with the 4.14% in the
control group. The results of lVUS demonstrated that the stent
expansion degree of the two groups was similar but the positive
vascular remodeling was more significant in the advanced stent
thrombosis group. Multivariate analysis suggested that the
uncovered segment length of the stent wire determined by OCT and
the IVUS remodeling index were independent predictors of advanced
stent thrombosis (67).
Late SM (LSM)
SM refers to the apparent separation of the stent
trabeculae from the vessel wall and may be divided into early and
late SM. A previous study demonstrated that LSM may cause stent
thrombosis. Compared with the control group, the incidence of SM in
patients with very advanced thrombosis (77 vs. 12%, respectively;
P<0.001) and the area of SM (77 vs. 12%, respectively;
P<0.001) were significantly increased (68). A total of 20 cases of late and very
late stent thrombosis were examined through OCT, indicating that 11
cases (55%) had SM, of which 5 cases had LSM caused by abnormal
positive remodeling of the vessel wall (68). However, the incidence of LSM is
notably higher than the incidence of late stent thrombosis,
indicating that, although LSM may not be the sole cause of stent
thrombosis, it may be one of the critical factors contributing to
the formation of stent thrombosis.
OCT carries unique advantages in assessing
postoperative SM. The high resolution of OCT may detect SM not
detected by IVUS. As IVUS cannot detect this type of SM, there is
no corresponding balloon expansion. However, the ratio of SM
detected by OCT is relatively high (69). When compared with IVUS, is it
unclear whether the higher number of SMs detected by OCT require
balloon expansion, whether these SMs may self-repair and what is
their prognosis. These questions must be addressed through further
clinical research.
SF
The incidence of SF is low. However, with the
increase in the number of stent implantations, an increasing number
of SF cases are being reported, particularly in cases of DES
implantation (70). In the past,
OCT machines lacked 3D imaging tools and OCT cross-sectional images
were not associated with obvious advantages in SF. The emergence of
OCT 3D real-time reconstruction systems enables the use of OCT to
study the occurrence of SF and its clinical significance (30,71).
3D OCT may help diagnose SF and determine the effect of SF on local
endometrial repair and local external stent plaque. Through OCT, it
is also possible to identify the factors that are likely to cause
SF.
While, SF may cause local mechanical vascular
irritation, leading to inflammation and neointimal hyperplasia, the
fracture destroys the local stent structure, causing thrombosis and
blood flow blockage and affecting the blood supply to the heart.
Stent trabecular fracture may also represent a potential mechanism
underlying ISR and stent thrombosis. The incidence of SF in EES has
been reported to be 1.7%. The 9-month follow-up indicated that SF
was associated with revascularization of the target lesion caused
by the event (18.7 vs. 2.3%) (72). The incidence of fracture after
implantation of the noboribiolimus-eluting stent reached 4.1%,
which is also associated with the revascularization of the target
lesion induced by ischemic events (73).
6. Factors and common problems affecting OCT
imaging results
OCT imaging results rely on standards
and correct operational techniques
In order to optimize the quality of OCT images, the
operator requires certain techniques to guide catheter operations.
Several factors affect the results of OCT imaging, including
excessive branch blood vessels, excessive lumen width, excessive
vascular bending, severe stenosis of the lumen, the effect of
cardiac cycle motion on the image and factors related to
intraoperative procedures. During the operation, attention should
be paid to the coaxiality of the guide tube and the target vessel,
the use of a contrast agent bolus, the synchronization of image
acquisition and the avoidance of red blood cells or air bubbles in
the imaging catheter or in the bolus contrast agent.
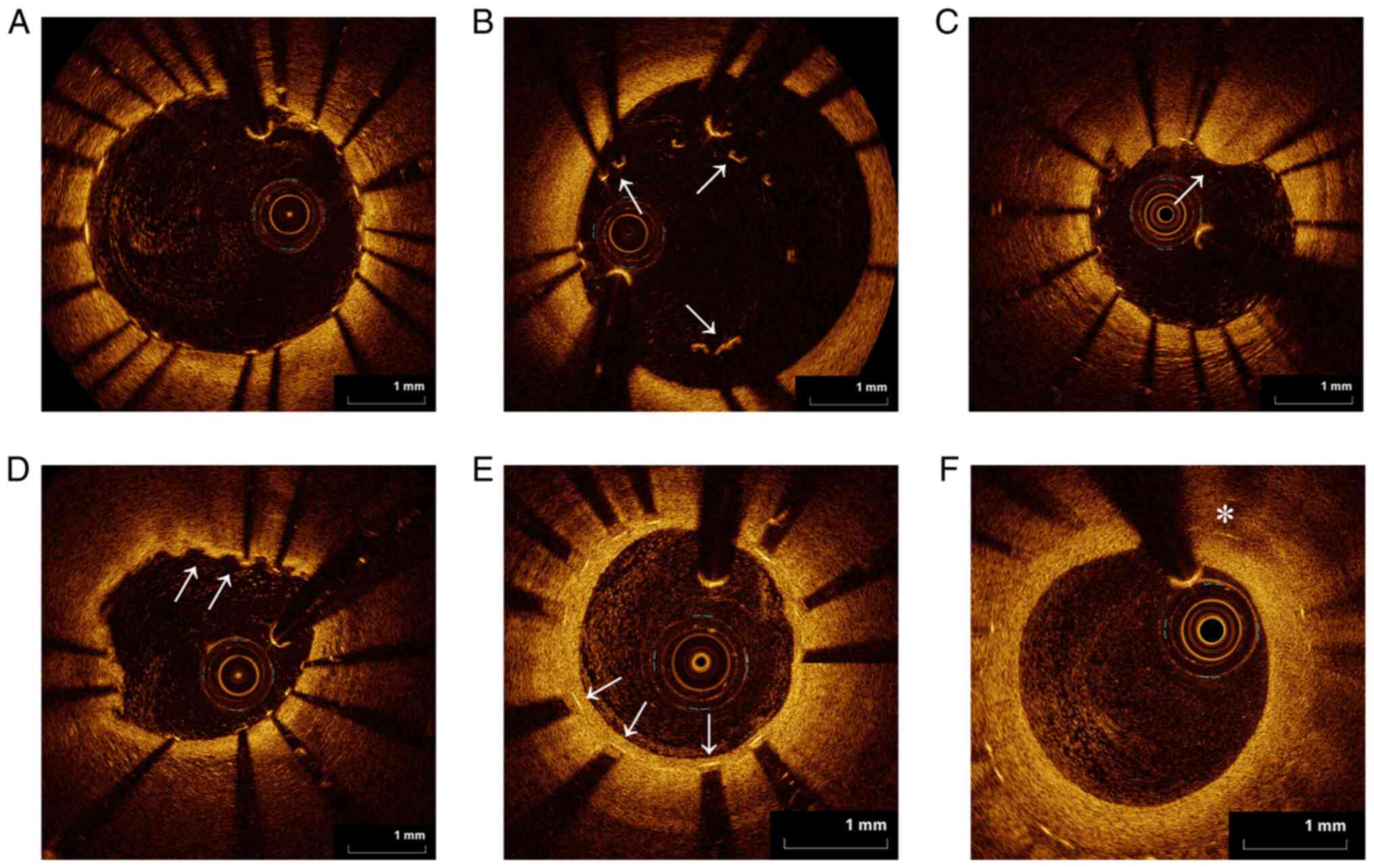
Branch vessel
When encountering a relatively large branch vessel,
it may affect the measurement accuracy and image recognition. At
this time, it is necessary to omit the branch vessel segment and
select a normal lumen to start a new measurement (Fig. 4A).
Bubble artifacts
The formation of small bubbles in the silicone
lubricant between the sheath and the optical fiber may attenuate
the blood vessel wall signal in the corresponding area. This type
of image is not suitable for the analysis of tissue characteristics
(Fig. 4B).
Saturation artifacts
The high specular reflection of the beam (usually
the stent trabeculae) produces an amplified signal, which appears
as axial linear stripes on the image (Fig. 4C).
Incomplete image
If the image area is <3/4 of the normal area, it
is difficult to ensure the accuracy of the measurement data. In
such cases, this frame or segment of the image may be omitted from
the analysis (Fig. 4D).
Unwashed blood
When the blood in the lumen is not washed out during
imaging, the red blood cells defocus the light beam and weaken the
brightness of the vessel wall, creating an artifact. Furthermore,
residual blood must be distinguished from a thrombus (Fig. 4E).
Guidewire damage
When the guidewire is damaged, abnormal images may
be obtained. Fig. 4F presents
images occurring when the two guidewires are damaged.
Splitting artifacts
In one frame of imaging, the artery or the guidewire
is quicker than the other, causing the signal points of the lumen
boundary to be out of sync, resulting in layering artifacts. This
must be distinguished from intimal tears (Fig. 4G and H).
7. Application prospects of OCT in the field
of cardiovascular interventional diagnosis and treatment
With the continuous improvement of OCT, it is
expected to have an important role in the examination of coronary
intravascular lesions, the optimization of PCI strategies and the
development of novel stents. The expected future development
directions and advantages of OCT are listed below (29,74-78).
i) The currently used frequency domain-OCT
retracement speed is up to 40 mm/sec, 158 frames of images/sec, and
the A-line frequency is 81 kHz. This causes 2-3 heartbeats to be
affected every 50 mm of retracement, resulting in blurred 3D
imaging edges. If the withdrawal speed was to be accelerated to
>100 mm/sec, >3,000 frames of images/sec and A-line frequency
>1.5 MHz, and combined with catheter positioning and tracking
technology, the 3D imaging would be clearer and more accurate, and
the clinical guidance value would be significantly improved. The
bolus of the contrast agent should also be markedly reduced.
ii) Micro-resolution OCT (micro-OCT) has a
resolution of up to 1 µm, which may analyze the microstructure of
the atherosclerotic plaque, plaque rupture, thrombus, neointima and
other tissues, at the cellular or subcellular level. The cellular
components of the plaque may provide a novel imaging method. Once
micro-OCT is used in human research, it may dynamically observe
certain cellular components and the stability and correlation of
atherosclerotic plaques or determine which cellular components
(such as endothelial cells, macrophages and smooth muscle cells)
are able to affect the intima of the stent. These future
applications of OCT may lead to breakthroughs in the current
understanding of the development of atherosclerosis and stent
intimal coverage, and may change existing views and provide novel
therapeutic intervention targets.
iii) Combining two or more imaging technologies may
be used to make up for the deficiencies of a single imaging method.
OCT-IVUS: Integrating OCT and IVUS on one imaging catheter not only
takes advantage of the high resolution of OCT, but also penetrates
through the IVUS catheter, and the depth is markedly increased.
OCT-NIRS: NIRS may perform an accurate and real-time in vivo
assessment of lipid core plaques. Combining NIRS technology with
OCT and applying them to intracoronary imaging may not only uncover
the morphological characteristics of the plaques but may also
identify the chemical composition of the plaque.
iv) Real-time integration of structural and
functional imaging information, such as OCT-FFR institutional
functional testing technology, may provide more accurate assessment
and guidance of treatment strategies for critical lesions, while
improving the current status of excessive implantation of stents in
the clinical setting.
v) Combining OCT and fluorescent molecular labeling
technology may provide information on inflammation and endothelial
function in the plaque, which is conducive to the in-depth study of
the pathophysiological processes of the atherosclerotic plaque and
the processes involved in stent repair.
vi) More large-sample OCT prospective clinical
studies are required to change or improve existing interventional
treatment strategies in certain controversial areas. Accumulating
the clinical data of OCT in determining the characteristics of
lesions and guiding precision interventional treatment may promote
the priority recommendation level of OCT in guidelines for the
diagnosis and treatment or revascularization in coronary heart
disease.
8. Summary
OCT is a high-resolution intravascular imaging
method for evaluating the composition of the coronary arterial wall
and the stability of the atherosclerotic plaque, optimizing the
efficacy of stent implantation, and evaluating the long-term
effectiveness and safety of the stent. Currently, the
interventional diagnosis and treatment of coronary heart disease
require better interventional results for patients, as well as
individualized and customized optimal strategies. With the
innovation and progress of OCT technology, clinical research
evidence is markedly more sufficient and interventional physicians
have mastered the OCT operating system. It is thought that the
application of this modality in clinical and basic research of
coronary artery atherosclerosis, the selection of treatment
strategies for acute coronary syndromes, the optimization of
interventional treatment effects, the evaluation of the effect of
novel stents, the stent intima coverage and the selection of double
antibodies, have become increasingly extensive. Furthermore, to a
certain extent, OCT may change or affect the currently applied
coronary interventional treatment strategies (4,5,79).
Acknowledgements
Not applicable.
Funding
Funding: This paper was supported by the Korea Food Research
Institute funded project (grant no. 2017029 to QZ) and the National
Natural Science Foundation of China (grant no. 61671098 to QZ).
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
JW and SY wrote and revised the manuscript. JQ
edited the manuscript. QZ performed the literature review. ZJ
designed and conceived the the study. All authors have read and
approved the final manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ramasamy A, Chen Y, Zanchin T, Jones DA,
Rathod K, Jin C, Onuma Y, Zhang YJ, Amersey R, Westwood M, et al:
Optical coherence tomography enables more accurate detection of
functionally significant intermediate non-left main coronary artery
stenoses than intravascular ultrasound: A meta-analysis of 6919
patients and 7537 lesions. Int J Cardiol. 301:226–234.
2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bouma BE, Villiger M, Otsuka K and Oh WY:
Intravascular optical coherence tomography [Invited]. Biomed Opt
Express. 8:2660–2686. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
van der Sijde JN, Karanasos A, van
Ditzhuijzen NS, Okamura T, van Geuns RJ, Valgimigli M, Ligthart JM,
Witberg KT, Wemelsfelder S, Fam JM, et al: Safety of optical
coherence tomography in daily practice: A comparison with
intravascular ultrasound. Eur Heart J Cardiovasc Imaging.
18:467–474. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tearney GJ, Regar E, Akasaka T,
Adriaenssens T, Barlis P, Bezerra HG, Bouma B, Bruining N, Cho JM,
Chowdhary S, et al: Consensus standards for acquisition,
measurement, and reporting of intravascular optical coherence
tomography studies: A report from the international working group
for intravascular optical coherence tomography standardization and
validation. J Am Coll Cardiol. 59:1058–1072. 2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Prati F, Regar E, Mintz GS, Arbustini E,
Di Mario C, Jang IK, Akasaka T, Costa M, Guagliumi G, Grube E, et
al: Expert review document on methodology, terminology, and
clinical applications of optical coherence tomography: Physical
principles, methodology of image acquisition, and clinical
application for assessment of coronary arteries and
atherosclerosis. Eur Heart J. 31:401–415. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Prati F, Guagliumi G, Mintz GS, Costa M,
Regar E, Akasaka T, Barlis P, Tearney GJ, Jang IK, Arbustini E, et
al: Expert review document part 2: Methodology, terminology and
clinical applications of optical coherence tomography for the
assessment of interventional procedures. Eur Heart J. 33:2513–2520.
2012.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Jang IK, Tearney GJ, MacNeill B, Takano M,
Moselewski F, Iftima N, Shishkov M, Houser S, Aretz HT, Halpern EF
and Bouma BE: In vivo characterization of coronary atherosclerotic
plaque by use of optical coherence tomography. Circulation.
111:1551–1555. 2005.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Muller JE, Tofler GH and Stone PH:
Circadian variation and triggers of onset of acute cardiovascular
disease. Circulation. 79:733–743. 1989.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Kolodgie FD, Burke AP, Farb A, Gold HK,
Yuan J, Narula J, Finn AV and Virmani R: The thin-cap
fibroatheroma: A type of vulnerable plaque: The major precursor
lesion to acute coronary syndromes. Curr Opin Cardiol. 16:285–292.
2001.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Naghavi M, Libby P, Falk E, Casscells SW,
Litovsky S, Rumberger J, Badimon JJ, Stefanadis C, Moreno P,
Pasterkamp G, et al: From vulnerable plaque to vulnerable patient:
A call for new definitions and risk assessment strategies: Part II.
Circulation. 108:1772–1778. 2003.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lin P, Ji HH, Li YJ and Guo SD: Macrophage
plasticity and atherosclerosis therapy. Front Mol Biosci.
8(679797)2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Nagasawa A, Otake H, Kawamori H, Toba T,
Sugizaki Y, Takeshige R, Nakano S, Tanimura K, Takahashi Y,
Fukuyama Y, et al: Relationship among clinical characteristics,
morphological culprit plaque features, and long-term prognosis in
patients with acute coronary syndrome. Int J Cardiovasc Imaging.
37:2827–2837. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kanaya T, Noguchi T, Otsuka F, Asaumi Y,
Kataoka Y, Morita Y, Miura H, Nakao K, Fujino M, Kawasaki T, et al:
Optical coherence tomography-verified morphological correlates of
high-intensity coronary plaques on non-contrast T1-weighted
magnetic resonance imaging in patients with stable coronary artery
disease. Eur Heart J Cardiovasc Imaging. 20:75–83. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Ali ZA, Karimi Galougahi K, Mintz GS,
Maehara A, Shlofmitz RA and Mattesini A: Intracoronary optical
coherence tomography: State of the art and future directions.
EuroIntervention. 17:e105–e123. 2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Chang K, Ahn Y, Lim S, Yang JH, Lee KY,
Choo EH, Kim HK, Nam CW, Kim W, Hwang JY, et al: 2021 Korean
society of myocardial infarction expert consensus document on
revascularization for acute myocardial infarction. Korean Circ J.
51:289–307. 2021.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Sun R, Qiao Y, Yan G, Wang D, Zuo W, Ji Z,
Zhang X, Yao Y, Ma G and Tang C: Association between serum adipsin
and plaque vulnerability determined by optical coherence tomography
in patients with coronary artery disease. J Thorac Dis.
13:2414–2425. 2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Milzi A, Lemma ED, Dettori R, Burgmaier K,
Marx N, Reith S and Burgmaier M: Coronary plaque composition
influences biomechanical stress and predicts plaque rupture in a
morpho-mechanic OCT analysis. Elife. 10(e64020)2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Shi X, Gao J, Lv Q, Cai H, Wang F, Ye R
and Liu X: Calcification in atherosclerotic plaque vulnerability:
Friend or foe? Front Physiol. 11(56)2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Joo SP, Lee SW, Cho YH, Kim YS, Seo BR,
Kim HS and Kim TS: Vasa vasorum densities in human carotid
atherosclerosis is associated with plaque development and
vulnerability. J Korean Neurosurg Soc. 63:178–187. 2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Nishida T, Hiro T, Takayama T, Sudo M,
Haruta H, Fukamachi D, Hirayama A and Okumura Y: Clinical
significance of microvessels detected by in vivo optical coherence
tomography within human atherosclerotic coronary arterial intima: A
study with multimodality intravascular imagings. Heart Vessels.
36:756–765. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Leistner DM, Kränkel N, Meteva D,
Abdelwahed YS, Seppelt C, Stähli BE, Rai H, Skurk C, Lauten A,
Mochmann HC, et al: Differential immunological signature at the
culprit site distinguishes acute coronary syndrome with intact from
acute coronary syndrome with ruptured fibrous cap: Results from the
prospective translational OPTICO-ACS study. Eur Heart J.
41:3549–3560. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Crea F and Libby P: Acute coronary
syndromes: The way forward from mechanisms to precision treatment.
Circulation. 136:1155–1166. 2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wang J, Fang C, Zhang S, Li L, Lu J, Wang
Y, Wang Y, Yu H, Wei G, Yin Y, et al: Systemic and local factors
associated with reduced thrombolysis in myocardial infarction flow
in ST-segment elevation myocardial infarction patients with plaque
erosion detected by intravascular optical coherence tomography. Int
J Cardiovasc Imaging. 37:399–409. 2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kataoka Y, Puri R, Hammadah M, Duggal B,
Uno K, Kapadia SR, Tuzcu EM, Nissen SE and Nicholls SJ: Spotty
calcification and plaque vulnerability in vivo: Frequency-domain
optical coherence tomography analysis. Cardiovasc Diagn Ther.
4:460–469. 2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Vink A, Schoneveld AH, Richard W, de
Kleijn DP, Falk E, Borst C and Pasterkamp G: Plaque burden,
arterial remodeling and plaque vulnerability: Determined by
systemic factors? J Am Coll Cardiol. 38:718–723. 2001.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Usui E, Yonetsu T, Kanaji Y, Hoshino M,
Yamaguchi M, Hada M, Hamaya R, Kanno Y, Murai T, Lee T and Kakuta
T: Efficacy of optical coherence tomography-derived morphometric
assessment in predicting the physiological significance of coronary
stenosis: Head-to-head comparison with intravascular ultrasound.
EuroIntervention. 13:e2210–e2218. 2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
de la Torre Hernandez JM, Baz Alonso JA,
Gómez Hospital JA, Alfonso Manterola F, Garcia Camarero T, Gimeno
de Carlos F, Roura Ferrer G, Recalde AS, Martínez-Luengas IL, Gomez
Lara J, et al: Clinical impact of intravascular ultrasound guidance
in drug-eluting stent implantation for unprotected left main
coronary disease: Pooled analysis at the patient-level of 4
registries. JACC Cardiovasc Interv. 7:244–254. 2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Wijns W, Shite J, Jones MR, Lee SW, Price
MJ, Fabbiocchi F, Barbato E, Akasaka T, Bezerra H and Holmes D:
Optical coherence tomography imaging during percutaneous coronary
intervention impacts physician decision-making: ILUMIEN I study.
Eur Heart J. 36:3346–3355. 2015.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Kedhi E, Berta B, Roleder T, Hermanides
RS, Fabris E, IJsselmuiden AJJ, Kauer F, Alfonso F, von Birgelen C,
Escaned J, et al: Thin-cap fibroatheroma predicts clinical events
in diabetic patients with normal fractional flow reserve: The
COMBINE OCT-FFR trial. Eur Heart J. 42:4671–4679. 2021.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Lee CH and Hur SH: Optimization of
percutaneous coronary intervention using optical coherence
tomography. Korean Circ J. 49:771–793. 2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Maehara A, Ben-Yehuda O, Ali Z, Wijns W,
Bezerra HG, Shite J, Généreux P, Nichols M, Jenkins P,
Witzenbichler B, et al: Comparison of stent expansion guided by
optical coherence tomography versus intravascular ultrasound: The
ILUMIEN II study [observational study of optical coherence
tomography (OCT) in patients undergoing fractional flow reserve
(FFR) and percutaneous coronary intervention]. JACC Cardiovasc
Interv. 8:1704–1714. 2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Imola F, Mallus MT, Ramazzotti V, Manzoli
A, Pappalardo A, Di Giorgio A, Albertucci M and Prati F: Safety and
feasibility of frequency domain optical coherence tomography to
guide decision making in percutaneous coronary intervention.
EuroIntervention. 6:575–581. 2010.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Bangalore S, Barsness GW, Dangas GD, Kern
MJ, Rao SV, Shore-Lesserson L and Tamis-Holland JE: Evidence-based
practices in the cardiac catheterization laboratory: A scientific
statement from the american heart association. Circulation.
144:e107–e119. 2021.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Viceconte N, Chan PH, Barrero EA,
Ghilencea L, Lindsay A, Foin N and Di Mario C: Frequency domain
optical coherence tomography for guidance of coronary stenting. Int
J Cardiol. 166:722–728. 2013.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Räber L, Mintz GS, Koskinas KC, Johnson
TW, Holm NR, Onuma Y, Radu MD, Joner M, Yu B, Jia H, et al:
Clinical use of intracoronary imaging. Part 1: Guidance and
optimization of coronary interventions. An expert consensus
document of the European association of percutaneous cardiovascular
interventions. Eur Heart J. 39:3281–3300. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Im E, Hong SJ, Ahn CM, Kim JS, Kim BK, Ko
YG, Choi D, Jang Y and Hong MK: Long-term clinical outcomes of late
stent malapposition detected by optical coherence tomography after
drug-eluting stent implantation. J Am Heart Assoc.
8(e011817)2019.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Kume T and Uemura S: Current clinical
applications of coronary optical coherence tomography. Cardiovasc
Interv Ther. 33:1–10. 2018.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Onuma Y, Katagiri Y, Burzotta F, Holm NR,
Amabile N, Okamura T, Mintz GS, Darremont O, Lassen JF, Lefèvre T,
et al: Joint consensus on the use of OCT in coronary bifurcation
lesions by the European and Japanese bifurcation clubs.
EuroIntervention. 14:e1568–e1577. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Wang Y, Mintz GS, Gu Z, Qi Y, Wang Y, Liu
M and Wu X: Meta-analysis and systematic review of intravascular
ultrasound versus angiography-guided drug eluting stent
implantation in left main coronary disease in 4592 patients. BMC
Cardiovasc Disord. 18(115)2018.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Gori T, Polimeni A, Indolfi C, Räber L,
Adriaenssens T and Münzel T: Predictors of stent thrombosis and
their implications for clinical practice. Nat Rev Cardiol.
16:243–256. 2019.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Stone GW, Sabik JF, Serruys PW, Simonton
CA, Généreux P, Puskas J, Kandzari DE, Morice MC, Lembo N, Brown WM
III, et al: Everolimus-eluting stents or bypass surgery for left
main coronary artery disease. N Engl J Med. 375:2223–2235.
2016.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Hildick-Smith D, de Belder AJ, Cooter N,
Curzen NP, Clayton TC, Oldroyd KG, Bennett L, Holmberg S, Cotton
JM, Glennon PE, et al: Randomized trial of simple versus complex
drug-eluting stenting for bifurcation lesions: The British
bifurcation coronary study: Old, new, and evolving strategies.
Circulation. 121:1235–1243. 2010.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Ferenc M, Gick M, Comberg T, Rothe J,
Valina C, Toma A, Löffelhardt N, Hochholzer W, Riede F, Kienzle RP,
et al: Culotte stenting vs TAP stenting for treatment of de-novo
coronary bifurcation lesions with the need for side-branch
stenting: The bifurcations bad krozingen (BBK) II angiographic
trial. Eur Heart J. 37:3399–3405. 2016.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Prati F, Jenkins MW, Di Giorgio A and
Rollins AM: Intracoronary optical coherence tomography, basic
theory and image acquisition techniques. Int J Cardiovasc Imaging.
27:251–258. 2011.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Okamura T, Yamada J, Nao T, Suetomi T,
Maeda T, Shiraishi K, Miura T and Matsuzaki M: Three-dimensional
optical coherence tomography assessment of coronary wire
re-crossing position during bifurcation stenting. EuroIntervention.
7:886–887. 2011.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Galassi AR, Sianos G, Werner GS, Escaned
J, Tomasello SD, Boukhris M, Castaing M, Büttner JH, Bufe A,
Kalnins A, et al: Retrograde recanalization of chronic total
occlusions in Europe: Procedural, in-hospital, and long-term
outcomes from the multicenter ERCTO registry. J Am Coll Cardiol.
65:2388–2400. 2015.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Munce NR, Yang VX, Standish BA, Qiang B,
Butany J, Courtney BK, Graham JJ, Dick AJ, Strauss BH, Wright GA
and Vitkin IA: Ex vivo imaging of chronic total occlusions using
forward-looking optical coherence tomography. Lasers Surg Med.
39:28–35. 2007.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Tyczynski P, Ferrante G, Kukreja N,
Moreno-Ambroj C, Barlis P, Ramasami N, De Silva R, Beatt K and Di
Mario C: Optical coherence tomography assessment of a new dedicated
bifurcation stent. EuroIntervention. 5:544–551. 2009.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Tanigawa J, Barlis P and Di Mario C:
Heavily calcified coronary lesions preclude strut apposition
despite high pressure balloon dilatation and rotational
atherectomy: In-vivo demonstration with optical coherence
tomography. Circ J. 72:157–160. 2008.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Cockburn J, Hildick-Smith D, Cotton J,
Doshi S, Hanratty C, Ludman P, Robinson D, Redwood S, de Belder M
and de Belder A: Contemporary clinical outcomes of patients treated
with or without rotational coronary atherectomy-an analysis of the
UK central cardiac audit database. Int J Cardiol. 170:381–387.
2014.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Jaguszewski M, Aloysius R, Wang W, Bezerra
HG, Hill J, De Winter RJ, Karjalainen PP, Verheye S, Wijns W,
Lüscher TF, et al: The REMEDEE-OCT study: An evaluation of the
bioengineered COMBO dual-therapy CD34 antibody-covered
sirolimus-eluting coronary stent compared with a cobalt-chromium
everolimus-eluting stent in patients with acute coronary syndromes:
Insights from optical coherence tomography imaging analysis. JACC
Cardiovasc Interv. 10:489–499. 2017.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Barlis P, Regar E, Serruys PW, Dimopoulos
K, van der Giessen WJ, van Geuns RJ, Ferrante G, Wandel S,
Windecker S, van Es GA, et al: An optical coherence tomography
study of a biodegradable vs. durable polymer-coated limus-eluting
stent: A LEADERS trial sub-study. Eur Heart J. 31:165–176.
2010.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Hamilos MI, Ostojic M, Beleslin B, Sagic
D, Mangovski L, Stojkovic S, Nedeljkovic M, Orlic D, Milosavljevic
B, Topic D, et al: Differential effects of drug-eluting stents on
local endothelium-dependent coronary vasomotion. J Am Coll Cardiol.
51:2123–2129. 2008.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Brugaletta S, Heo JH, Garcia-Garcia HM,
Farooq V, van Geuns RJ, de Bruyne B, Dudek D, Smits PC, Koolen J,
McClean D, et al: Endothelial-dependent vasomotion in a coronary
segment treated by ABSORB everolimus-eluting bioresorbable vascular
scaffold system is related to plaque composition at the time of
bioresorption of the polymer: Indirect finding of vascular
reparative therapy? Eur Heart J. 33:1325–1333. 2012.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Kubo T, Imanishi T, Kitabata H, Kuroi A,
Ueno S, Yamano T, Tanimoto T, Matsuo Y, Masho T, Takarada S, et al:
Comparison of vascular response after sirolimus-eluting stent
implantation between patients with unstable and stable angina
pectoris: A serial optical coherence tomography study. JACC
Cardiovasc Imaging. 1:475–484. 2008.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Kochman J, Pietrasik A, Rdzanek A, Ścibisz
A, Pawlak M, Filipiak KJ and Opolski G: Tissue coverage of
paclitaxel and sirolimus eluting stents in long term follow-up:
Optical coherence tomography study. Cardiol J. 20:247–253.
2013.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Landmesser U, Engberding N, Bahlmann FH,
Schaefer A, Wiencke A, Heineke A, Spiekermann S, Hilfiker-Kleiner
D, Templin C, Kotlarz D, et al: Statin-induced improvement of
endothelial progenitor cell mobilization, myocardial
neovascularization, left ventricular function, and survival after
experimental myocardial infarction requires endothelial nitric
oxide synthase. Circulation. 110:1933–1939. 2004.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Kimura T, Abe K, Shizuta S, Odashiro K,
Yoshida Y, Sakai K, Kaitani K, Inoue K, Nakagawa Y, Yokoi H, et al:
Long-term clinical and angiographic follow-up after coronary stent
placement in native coronary arteries. Circulation. 105:2986–2991.
2002.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Stone GW, Moses JW, Ellis SG, Schofer J,
Dawkins KD, Morice MC, Colombo A, Schampaert E, Grube E, Kirtane
AJ, et al: Safety and efficacy of sirolimus- and paclitaxel-eluting
coronary stents. N Engl J Med. 356:998–1008. 2007.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Jung HW, Lim C, Bae HJ, Lee JH, Lee YJ,
Kim JS, Lee SJ, Hong SJ, Ahn CM, Kim BK, et al: Association between
in-stent neointimal characteristics and native coronary artery
disease progression. PLoS One. 16(e0247359)2021.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Borovac JA, D'Amario D, Vergallo R, Porto
I, Bisignani A, Galli M, Annibali G, Montone RA, Leone AM, Niccoli
G and Crea F: Neoatherosclerosis after drug-eluting stent
implantation: A novel clinical and therapeutic challenge. Eur Heart
J Cardiovasc Pharmacother. 5:105–116. 2019.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Oka N, Kadohira T, Fujii K, Kitahara H,
Fujimoto Y and Kobayashi Y: Microbubble contrast enhancement of
neointima after drug-eluting stent implantation: An optical
coherence tomography study. Heart Vessels. 34:393–400.
2019.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Li S, Luo C and Chen H: Risk factors of
in-stent restenosis in patients with diabetes mellitus after
percutaneous coronary intervention: A protocol for systematic
review and meta-analysis. Medicine (Baltimore).
100(e25484)2021.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Kang SJ, Song HG, Ahn JM, Kim WJ, Lee JY,
Park DW, Lee SW, Kim YH, Lee CW, Park SW and Park SJ: OCT-verified
neoatherosclerosis in BMS restenosis at 10 years. JACC Cardiovasc
Imaging. 5:1267–1268. 2012.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Toutouzas K, Chatzizisis YS, Riga M,
Giannopoulos A, Antoniadis AP, Tu S, Fujino Y, Mitsouras D,
Doulaverakis C, Tsampoulatidis I, et al: Accurate and reproducible
reconstruction of coronary arteries and endothelial shear stress
calculation using 3D OCT: Comparative study to 3D IVUS and 3D QCA.
Atherosclerosis. 240:510–519. 2015.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Kaivosoja TP, Liu S, Dijkstra J, Huhtala
H, Sheth T and Kajander OA: Comparison of visual assessment and
computer image analysis of intracoronary thrombus type by optical
coherence tomography. PLoS One. 13(e0209110)2018.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Guagliumi G, Sirbu V, Musumeci G, Gerber
R, Biondi-Zoccai G, Ikejima H, Ladich E, Lortkipanidze N,
Matiashvili A, Valsecchi O, et al: Examination of the in vivo
mechanisms of late drug-eluting stent thrombosis: findings from
optical coherence tomography and intravascular ultrasound imaging.
JACC Cardiovasc Interv. 5:12–20. 2012.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Gori T: Vascular wall reactions to
coronary stents-clinical implications for stent failure. Life
(Basel). 11(63)2021.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Garcia-Guimaraes M, Antuña P, De la Cuerda
F, Maruri-Sanchez R, Cuesta J, Bastante T, Rivero F and Alfonso F:
High-definition IVUS versus OCT to assess coronary artery disease
and results of stent implantation. JACC Cardiovasc Imaging.
13:519–521. 2020.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Park KW, Park JJ, Chae IH, Seo JB, Yang
HM, Lee HY, Kang HJ, Cho YS, Yeon TJ, Chung WY, et al: Clinical
characteristics of coronary drug-eluting stent fracture: Insights
from a two-center des registry. J Korean Med Sci. 26:53–58.
2011.PubMed/NCBI View Article : Google Scholar
|
|
71
|
Aung SSM, Latt H, Kyaw K and Roongsritong
C: An interesting case and literature review of a coronary stent
fracture in a current generation platinum chromium
everolimus-eluting stent. Case Rep Cardiol.
2018(4579184)2018.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Kan J, Ge Z, Zhang JJ, Liu ZZ, Tian NL, Ye
F, Li SJ, Qian XS, Yang S, Chen MX, et al: Incidence and clinical
outcomes of stent fractures on the basis of 6,555 patients and
16,482 drug-eluting stents from 4 centers. JACC Cardiovasc Interv.
9:1115–1123. 2016.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Kuramitsu S, Iwabuchi M, Yokoi H, Domei T,
Sonoda S, Hiromasa T, Morinaga T, Kobayashi Y, Ohe K, Goya K, et
al: Incidence and clinical impact of stent fracture after the
Nobori biolimus-eluting stent implantation. J Am Heart Assoc.
3(e000703)2014.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Shaw LJ, Berman DS, Maron DJ, Mancini GB,
Hayes SW, Hartigan PM, Weintraub WS, O'Rourke RA, Dada M, Spertus
JA, et al: Optimal medical therapy with or without percutaneous
coronary intervention to reduce ischemic burden: Results from the
clinical outcomes utilizing revascularization and aggressive drug
evaluation (COURAGE) trial nuclear substudy. Circulation.
117:1283–1291. 2018.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Yin J, Li X, Jing J, Li J, Mukai D, Mahon
S, Edris A, Hoang K, Shung KK, Brenner M, et al: Novel combined
miniature optical coherence tomography ultrasound probe for in vivo
intravascular imaging. J Biomed Opt. 16(060505)2011.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Li BH, Leung AS, Soong A, Munding CE, Lee
H, Thind AS, Munce NR, Wright GA, Rowsell CH, Yang VX, et al:
Hybrid intravascular ultrasound and optical coherence tomography
catheter for imaging of coronary atherosclerosis. Catheter
Cardiovasc Interv. 81:494–507. 2013.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Li X, Li J, Jing J, Ma T, Liang S, Zhang
J, Mohar D, Raney A, Mahon S, Brenner M, et al: Integrated IVUS-OCT
imaging for atherosclerotic plaque characterization. IEEE J Sel Top
Quantum Electron. 20(7100108)2014.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Yoo H, Kim JW, Shishkov M, Namati E, Morse
T, Shubochkin R, McCarthy JR, Ntziachristos V, Bouma BE, Jaffer FA
and Tearney GJ: Intra-arterial catheter for simultaneous
microstructural and molecular imaging in vivo. Nat Med.
17:1680–1684. 2011.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Ligthart JM, Diletti R, Witberg K and
Schultz C: Three-dimensional optical coherence tomography for
guidance of complex percutaneous coronary interventions. JACC
Cardiovasc Interv. 7:102–103. 2014.PubMed/NCBI View Article : Google Scholar
|