Introduction
Preeclampsia (PE) is a form of ischemic placental
disease and its physiopathology remains unclear, although recent
advances have been made in increasing its understanding. Despite
being a rare disorder, which affects between 2-10% of pregnant
women, PE is still a significant cause of maternal and perinatal
morbidity and mortality (1).
Galectins are carbohydrate-binding proteins that
control cell growth, proliferation, differentiation, apoptosis,
signal transduction, mRNA splicing, and extracellular matrix
interactions (2). To date,
approximately 20 members of the galectin family have been
identified, and one in particular, protein-galectin-13 or placental
protein-13 (PP-13), has gained recognition as an important factor
in the pathogenesis of preeclampsia (3). It seems that PP-13 is involved in deep
placentation, vascular remodeling and immune tolerance (4). Therefore, the background for its use
in preeclampsia screening with or without intrauterine growth
restriction has been proposed.
In the present systematic review and meta-analysis,
we aimed to assess the predictive performance of PP-13 for
preeclampsia screening in the first trimester of pregnancy.
Research methods
From the onset of each database through March 14,
2021, we conducted a comprehensive manual and electronic search
using the Preferred Reporting Items for Systematic Reviews and
Meta-Analyses guidelines (PRISMA) to discover literature on the
predictive value of PP-13 in preeclampsia (5).
PubMed, Web of Science, Scopus, Embase, BIOSIS, and
Cochrane Library were used (6-11).
‘Preeclampsia’, ‘first trimester’, ‘screening’, ‘placental protein
13’, ‘PP-13’, and ‘galectin-13’ were employed as medical topic
headings (MeSH) or key words, which were combined with Boolean
operators AND and OR. There were no restrictions on the type of
study or the language used. The bibliographies of the selected
publications were rechecked to ensure that all relevant studies
were included. The inclusion criteria (summarized in Table I) were: observational studies, such
as cross-sectional, case-control, or cohort studies that analyzed
the predictive performance of PP-13 in the first trimester of
pregnancy; studies published until March 2021. Studies that did not
fulfill the abovementioned criteria were excluded from our
review.
 | Table IInclusion criteria of the studies. |
Table I
Inclusion criteria of the studies.
| Study design | Observational study
with a well-defined study population |
|---|
| Source | Peer-reviewed
journals |
| Language | Any |
| Disease | Preeclampsia |
| Sample type | Blood, serum, or
plasma |
| Gestational age | First trimester |
| Assay type | Any |
| Onset of
preeclampsia | Any (early or
late) |
| Sample size | ≥50 |
The full-text papers were independently reviewed by
two physician investigators (DN and IAV) to establish their
eligibility for the review. Any differences between the two were
remedied through conversation. A third reviewer (AC) added a
casting vote if a consensus could not be reached.
Two reviewers (DN and IAV) retrieved data from the
eligible studies separately using a standard process. Most of the
published research used various cut-offs to assess the level of
PP-13 at various gestational ages. Data concerning the first
author, publication year, study design, characteristics of the
population examined, number of cases and controls, gestational age
at sampling, cut-offs used, test kits, and the information needed
to create a 2x2 table were obtained.
Two independent reviewers assessed the
methodological quality of the included studies using the QUADAS-2
technique (Quality Assessment of Diagnostic Accuracy Studies-2)
(12,13).
The number of pregnant women with true-positive,
true-negative, false-positive, and false-negative test results were
retrieved from all of the studies. A 2x2 diagnosis table was
created by calculating the accuracy measures, the illness
prevalence, and the sample size stated in the study. Each study's
sensitivity, specificity, positive, and negative probability ratios
were determined using a 95% confidence interval (CI).
For hierarchical modeling, a hierarchical summary
receiver operating characteristic (HSROC) model was utilized to
generate equal summary estimates for sensitivity and specificity,
taking into account variability both between and within studies
(heterogeneity) (random sampling error). The Der Simonian-Laird
approach was used to estimate random effects (14). The Q test was used to assess
statistical heterogeneity among the studies, and the I2
statistic was used to measure the degree of heterogeneity.
The area under the summary receiver operating
characteristic curve (AUC) was determined using the accuracy data
from all the included investigations, which were plotted on a
summary receiver operating characteristic SROC with sensitivity on
the x-axis and specificity on the y-axis. This is the same as the
summary diagnostic odds ratio (OR), which measures the strength of
the link between the test and the disease. The random-effects model
was adopted because of the expected clinical and statistical
heterogeneity among the trials. StataMP 16.0 (StataCorp) was used
to statistically analyze all of the data.
Results
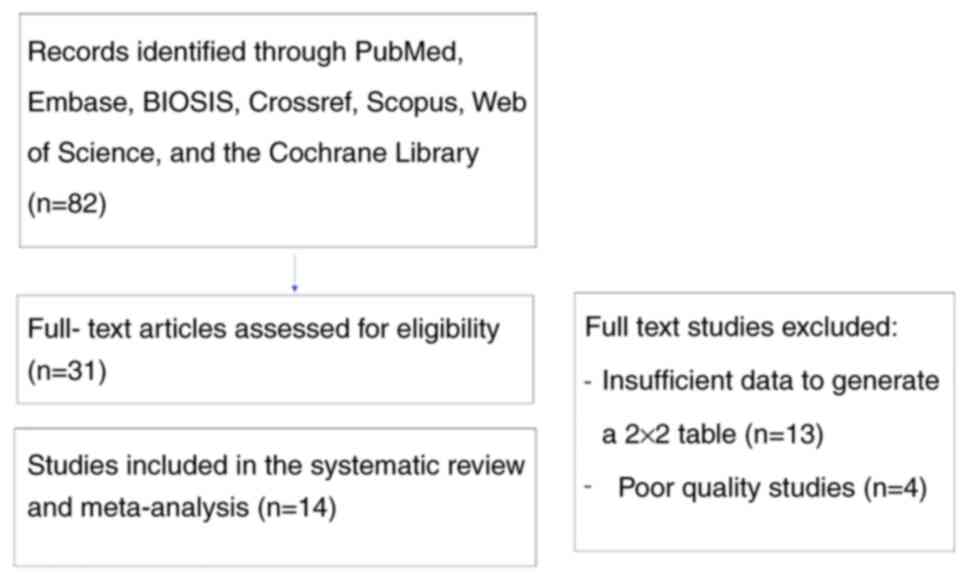
A total of 82 studies were identified. After
screening the titles and abstracts, the systematic review and
meta-analysis comprised 14 studies (15-28)
(Fig. 1).
The quality assessment of these studies is
summarized in Table II. In most of
the studies, there was good reporting with a prospective design,
consecutive recruitment, adequate description of the selection
criteria, patient spectrum, test, and use of appropriate reference
standards.
| Table IIQuality analysis of the included
studies. |
Table II
Quality analysis of the included
studies.
| | Risk of bias | Applicability
concerns |
|---|
| Authors of the study
(Refs.) | Patient
selection | Index test | Reference
standard | Flow and timing | Patient
selection | Index test | Reference
standard |
|---|
| Spencer et al
(15) | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Chafetz et al
(16) | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Gonen et al
(17) | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Khalil et al
(18) | Low risk | High risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Akolekar et
al (19) | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Khalil et al
(20) | Low risk | Unclear risk | Low risk | Low risk | Low risk | Unclear risk | Low risk |
| Wortelboer et
al (21) | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Odibo et al
(22) | Low risk | Unclear risk | Low risk | Low risk | Low risk | Unclear risk | Low risk |
| Schneuer et
al (23) | Low risk | Unclear risk | Low risk | Low risk | Low risk | Low risk | Low risk |
| Deurloo et
al (24) | Low risk | Unclear risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Meiri et al
(25) | Low risk | Unclear risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Luo and Han
(26) | Low risk | Unclear risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Asiltas et
al (27) | Low risk | Unclear risk | Low risk | High risk | Low risk | Low risk | Low risk |
| Soongsatitanon and
Phupong (28) | Low risk | Unclear risk | Low risk | High risk | Low risk | Low risk | Low risk |
Early-(EO-PE) or late-onset (LO-PE) preeclampsia and
preeclampsia associated with small for gestational age fetuses
(PE-SGA) were considered separate study groups and studied
individually. Table III
summarizes the study characteristics.
| Table IIICharacteristics of the included
studies. |
Table III
Characteristics of the included
studies.
| Authors of the
study (Refs.) | Year | Country | Study design | Characteristics of
the population | Disease
endpoint | Sample type | Assay used | age (week) | Gestational Cases
(n) | Controls (n) |
|---|
| Spencer et
al (15) | 2006 | UK | Prospective | Screening in
ANC | All PE, EO-PE | Serum | ELISA | 11-13+6 | All PE (88) EO-PE
(44) | 446 |
| Chafetz et
al (16) | 2007 | USA | Prospective | Screening in
ANC | All PE | Serum | ELISA | 9-12 | 47 | 290 |
| Gonen et al
(17) | 2008 | Israel | Prospective | Screening in
ANC | All PE, EO-PE,
LO-PE | Serum | ELISA | 6-10 | All PE (20) EO-PE
(5) LO-PE (5) | 1,178 |
| Khalil et al
(18) | 2009 | UK | Prospective | Women with high
risk of PE | EO-PE, term and
preterm PE | Serum | ELISA | 11-13+6 | EO-PE (14) Preterm
PE (36) Term PE (6) | 210 |
| Akolekar et
al (19) | 2009 | UK | Prospective | Screening in
ANC | EO-PE | Serum | DELFIA | 11-13+6 | 48 | 416 |
| Khalil et al
(20) | 2010 | UK | Prospective | Women with high
risk of PE | All PE, EO-PE,
PE+SGA | Serum | ELISA | 11-13+6 | All PE (42) EO-PE
(14) PE+SGA (13) | 210 |
| Wortelboer et
al (21) | 2010 | The
Netherlands | Prospective | Screening in
ANC | EO-PE | Serum | DELFIA | 8-13+6 | 45 | 480 |
| Odibo et al
(22) | 2011 | USA | Prospective | Screening in
ANC | All PE, EO-PE | Serum | DELFIA | 11-14 | All PE (42)
EO-PE-12 | 410 |
| Schneuer et
al (23) | 2012 | Australia | Prospective | Screening in
ANC | All PE, EO-PE | Serum | DELFIA | 10-14 | All PE (71) EO-PE
(5) | 2,423 |
| Deurloo et
al (24) | 2013 | Amsterdam | Retrospective | Screeening in
ANC | All PE | Serum | ELISA | 9-13+6 | 17 | 165 |
| Meiri et al
(25) | 2014 | Israel | Prospective | Screening in
ANC | All PE | Serum | ELISA | 8-14 | 63 | 757 |
| Luo and Han
(26) | 2017 | China | Prospective | Screening in
ANC | All PE | Serum | ELISA | 9-13+6 | 33 | 71 |
| Asiltas et
al (27) | 2018 | Turkey | Prospective | Screening in
ANC | All PE | Serum | ELISA | 11-13+6 | 38 | 122 |
| Soongsatitanon and
Phupong (28) | 2020 | Thailand | Prospective | Screening in
ANC | All PE | Serum | ELISA | 11-13+6 | 29 | 324 |
The 14 publications studied were published between
2006 and 2020 and were worldwide, with no preference for one
region. The meta-analysis included a total of 737 cases of
preeclampsia and 7,502 controls.
The mean value of PP-13 expressed in multiples of
median (MoM) and standard deviation was 0.92±0.95 for all
preeclampsia group, 0.62±0.22 for the early-onset preeclampsia
(EO-PE) group, and 0.5±0.19 for the late-onset preeclampsia (LO-PE)
or small for gestational age and preeclampsia group (PE + SGA)
group, respectively. No statistically significant difference was
observed between the groups regarding the cut-off value of PP-13
(P=0.414). The accuracy of the test in the various studies is
tabulated in Table IV.
| Table IVDiagnostic accuracy of PP-13 for the
prediction of PE in the various studies. |
Table IV
Diagnostic accuracy of PP-13 for the
prediction of PE in the various studies.
| Authors of the
study (Refs.) | Year | Type of PE | LR(+) | LR(-) | DOR |
|---|
| Spencer et
al (15) | 2006 | All PE | 2.22 | 0.70 | 3.19 |
| Chafetz et
al (16) | 2007 | All PE | 7.87 | 0.24 | 33.30 |
| Khalil et al
(18) | 2009 | All PE | 6.90 | 0.34 | 20.08 |
| Odibo et al
(22) | 2011 | All PE | 6.35 | 0.73 | 8.74 |
| Odibo et al
(22) | 2011 | All PE | 4.52 | 0.61 | 7.43 |
| Odibo et al
(22) | 2011 | All PE | 2.50 | 0.63 | 4.00 |
| Schneuer et
al (23) | 2012 | All PE | 3.10 | 0.89 | 3.49 |
| Deurloo et
al (24) | 2013 | All PE | 1.18 | 0.96 | 1.23 |
| Meiri et al
(25) | 2014 | All PE | 3.69 | 0.26 | 14.02 |
| Meiri et al
(25) | 2014 | All PE | 5.22 | 0.53 | 9.86 |
| Luo and Han
(26) | 2017 | All PE | 3.07 | 0.49 | 6.26 |
| Asiltas et
al (27) | 2018 | All PE | 9.10 | 0.12 | 77.92 |
| Soongsatitanon and
Phupong (28) | 2020 | All PE | 1.51 | 0.73 | 2.06 |
| Spencer et
al (15) | 2006 | EO-PE | 2.51 | 0.62 | 4.01 |
| Gonen et al
(17) | 2008 | EO-PE | 3.99 | 0.25 | 15.97 |
| Gonen et al
(17) | 2009 | EO-PE | 7.14 | 0.32 | 22.50 |
| Khalil et al
(20) | 2010 | EO-PE | 6.43 | 0.40 | 16.20 |
| Akolekar et
al (19) | 2009 | EO-PE | 4.13 | 0.83 | 4.95 |
| Akolekar et
al (19) | 2009 | EO-PE | 3.71 | 0.70 | 5.34 |
| Wortelboer et
al (21) | 2010 | EO-PE | 4.89 | 0.80 | 6.15 |
| Wortelboer et
al (21) | 2010 | EO-PE | 4.00 | 0.67 | 6.00 |
| Odibo et al
(22) | 2011 | EO-PE | 3.75 | 0.31 | 12.00 |
| Schneuer et
al (23) | 2012 | EO-PE | 4.00 | 0.84 | 4.76 |
| Spencer et
al (15) | 2006 | LO-PE/PE + SGA | 1.94 | 0.77 | 2.53 |
| Gonen et al
(17) | 2008 | LO-PE/PE + SGA | 3.99 | 0.25 | 15.97 |
| Khalil et al
(18) | 2009 | LO-PE/PE + SGA | 5.00 | 0.56 | 9.00 |
| Khalil et al
(18) | 2009 | LO-PE/PE + SGA | 6.11 | 0.43 | 14.14 |
| Khalil et al
(20) | 2010 | LO-PE/PE + SGA | 6.15 | 0.43 | 14.40 |
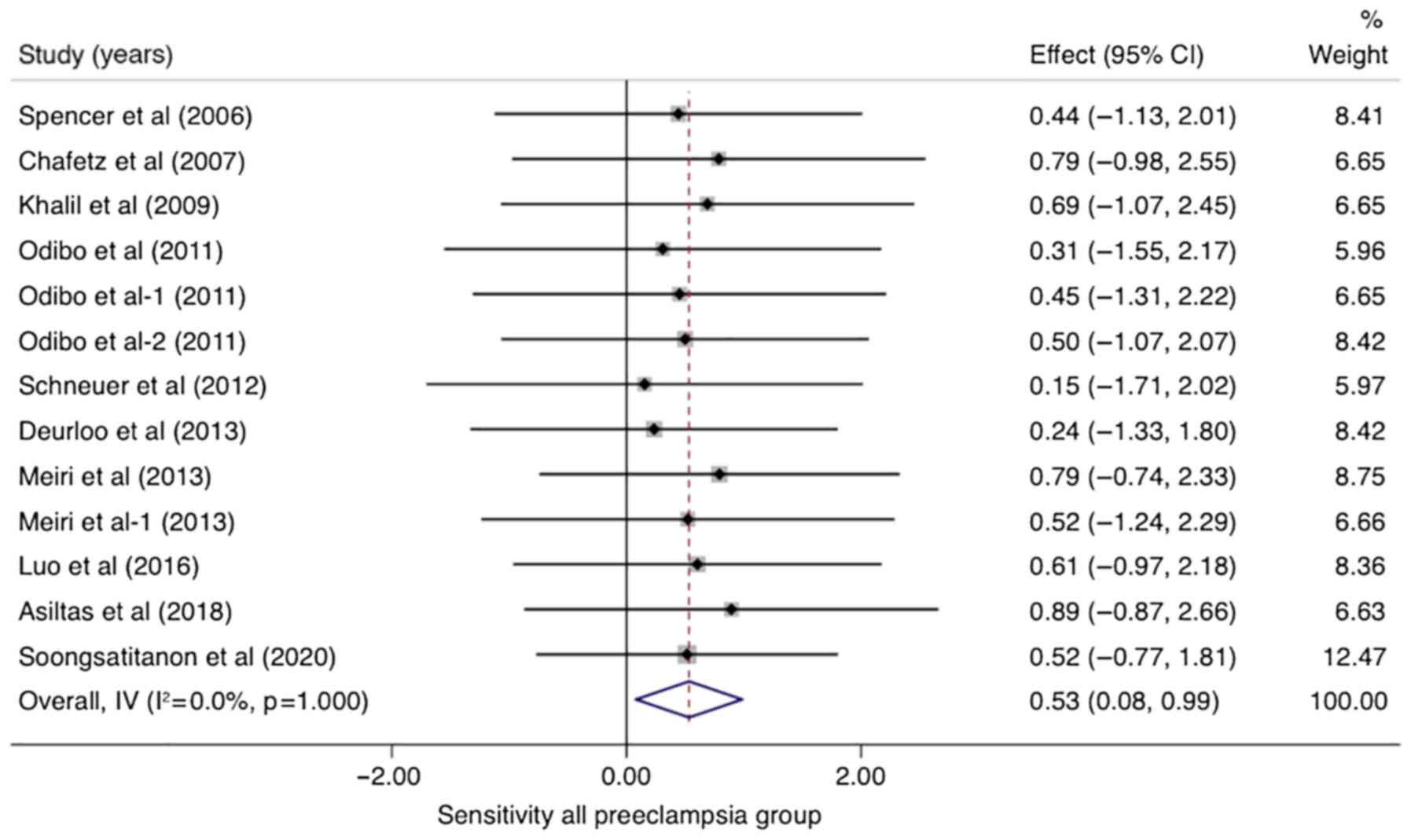
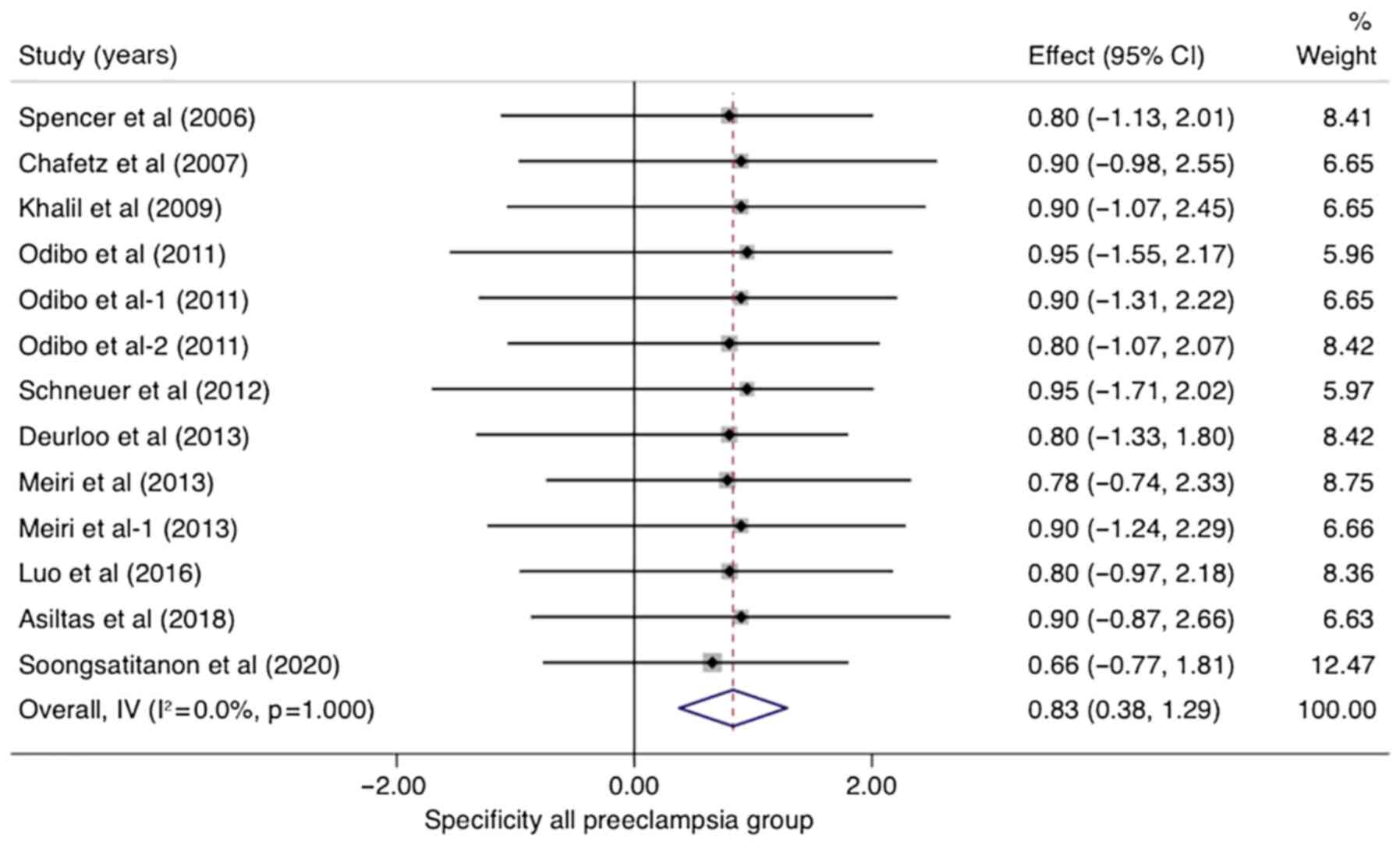
In studies that analyzed women with PE without
sub-classifying the population into EO-PE and LO-PE (n=10), the
pooled sensitivity of PP-13 was 0.53 (95% CI, 0.08-0.99,
I2 0.0%) and the pooled specificity of PP-13 was 0.83
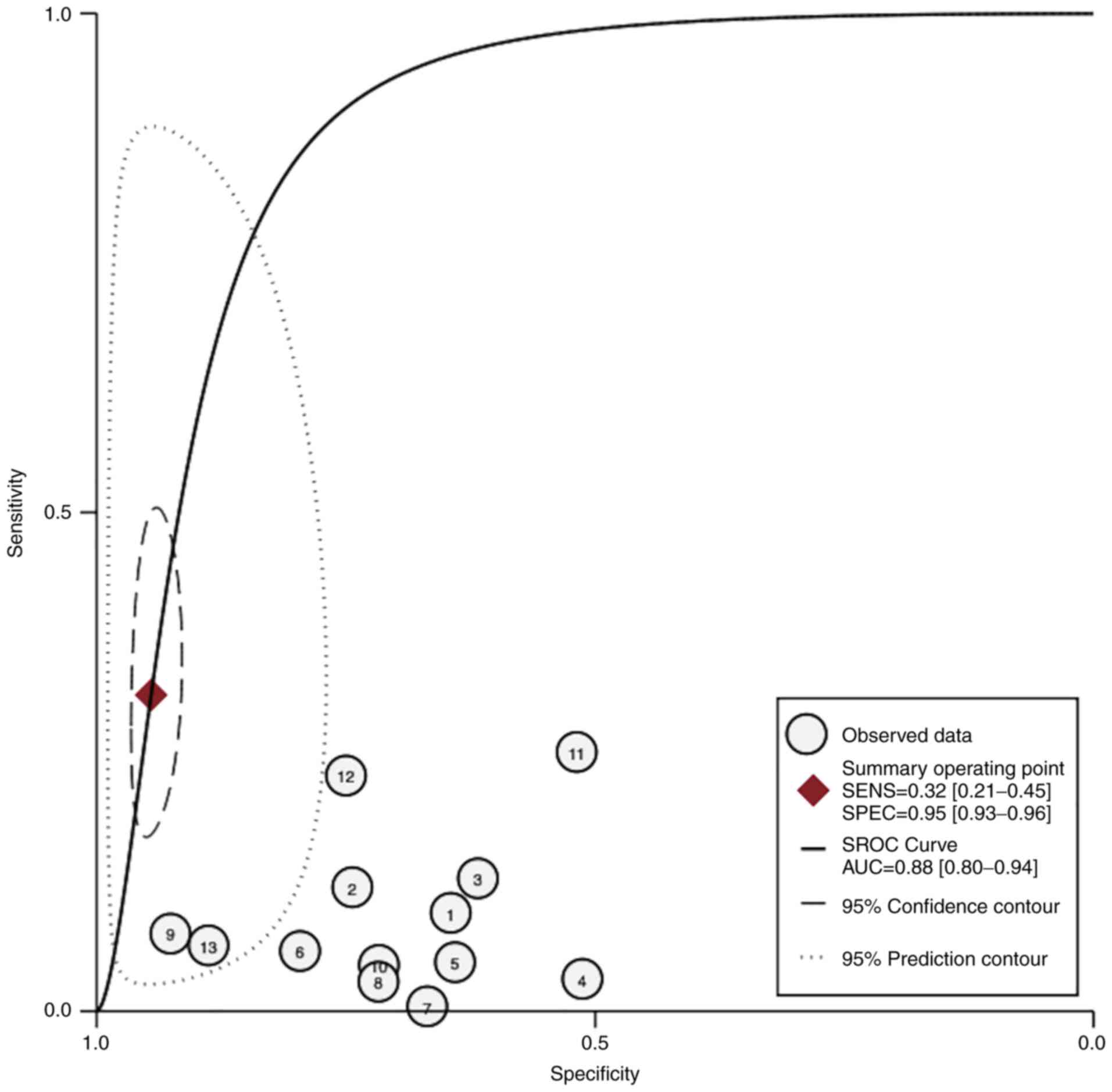
(95% CI, 0.38-1.29, I2 0.0%) (Figs. 2 and 3). The summary receiver operating
characteristic curve (SROC) was 0.88 (95% CI, 0.80-0.94) (Fig. 4).
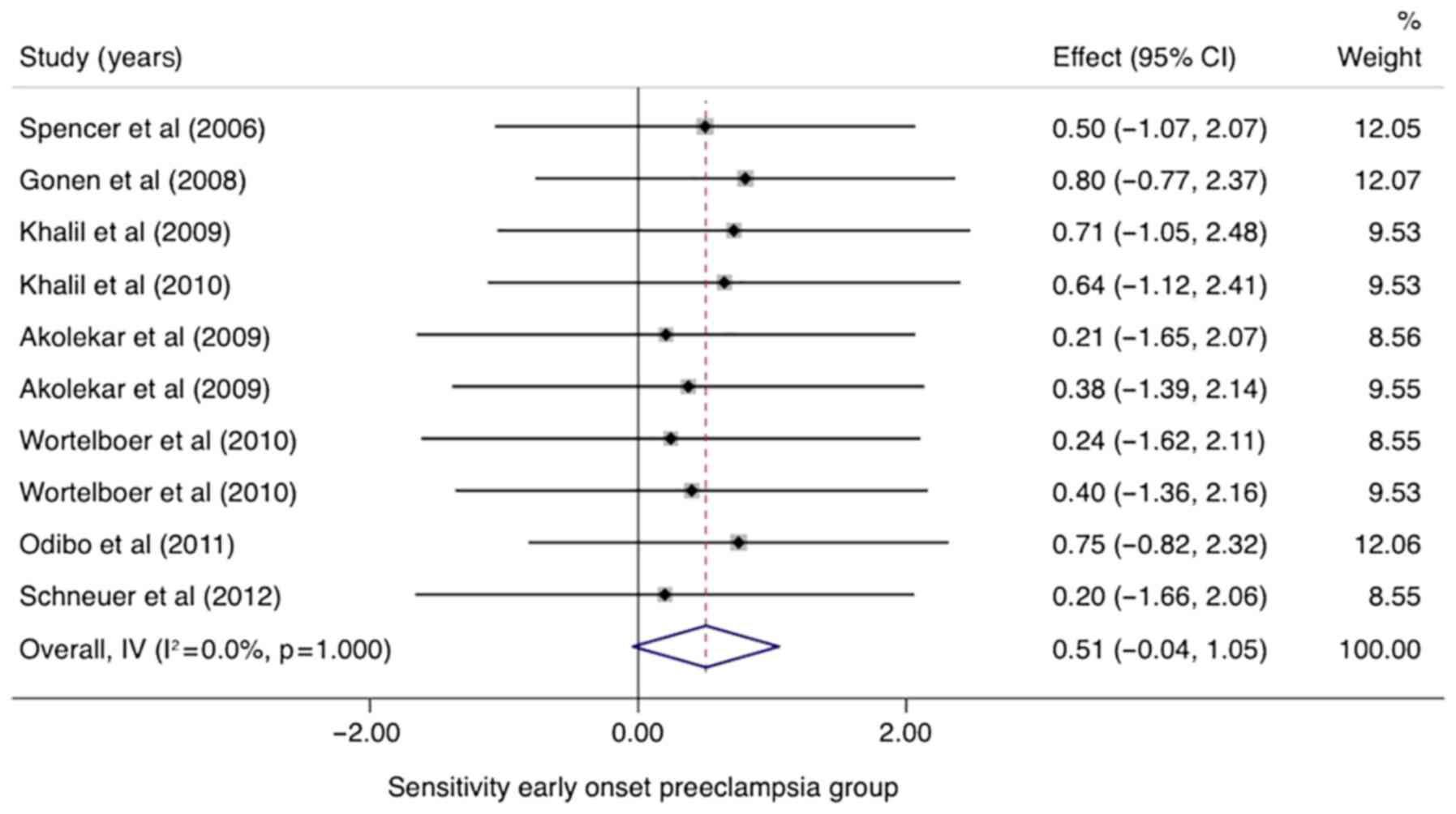
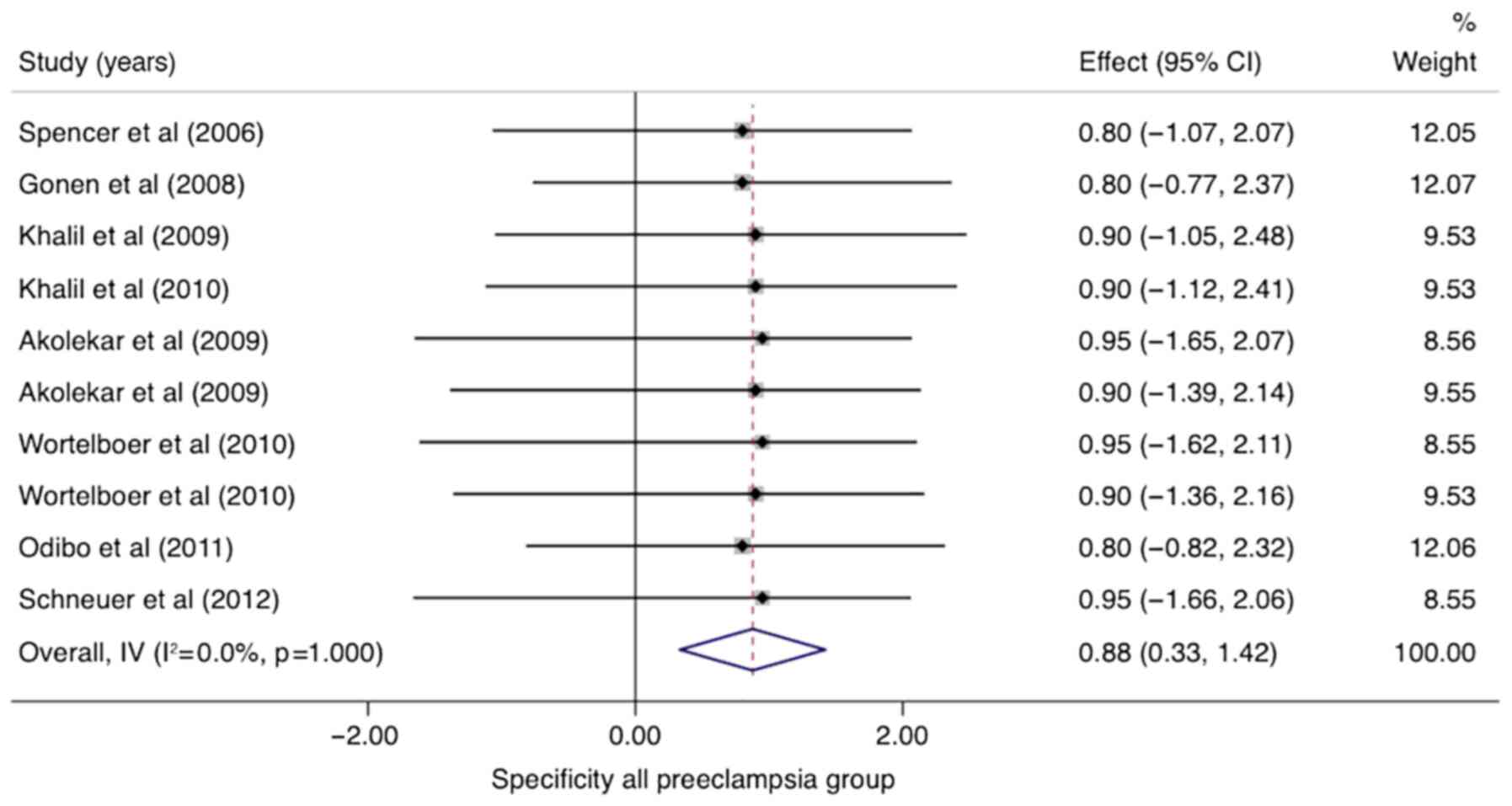
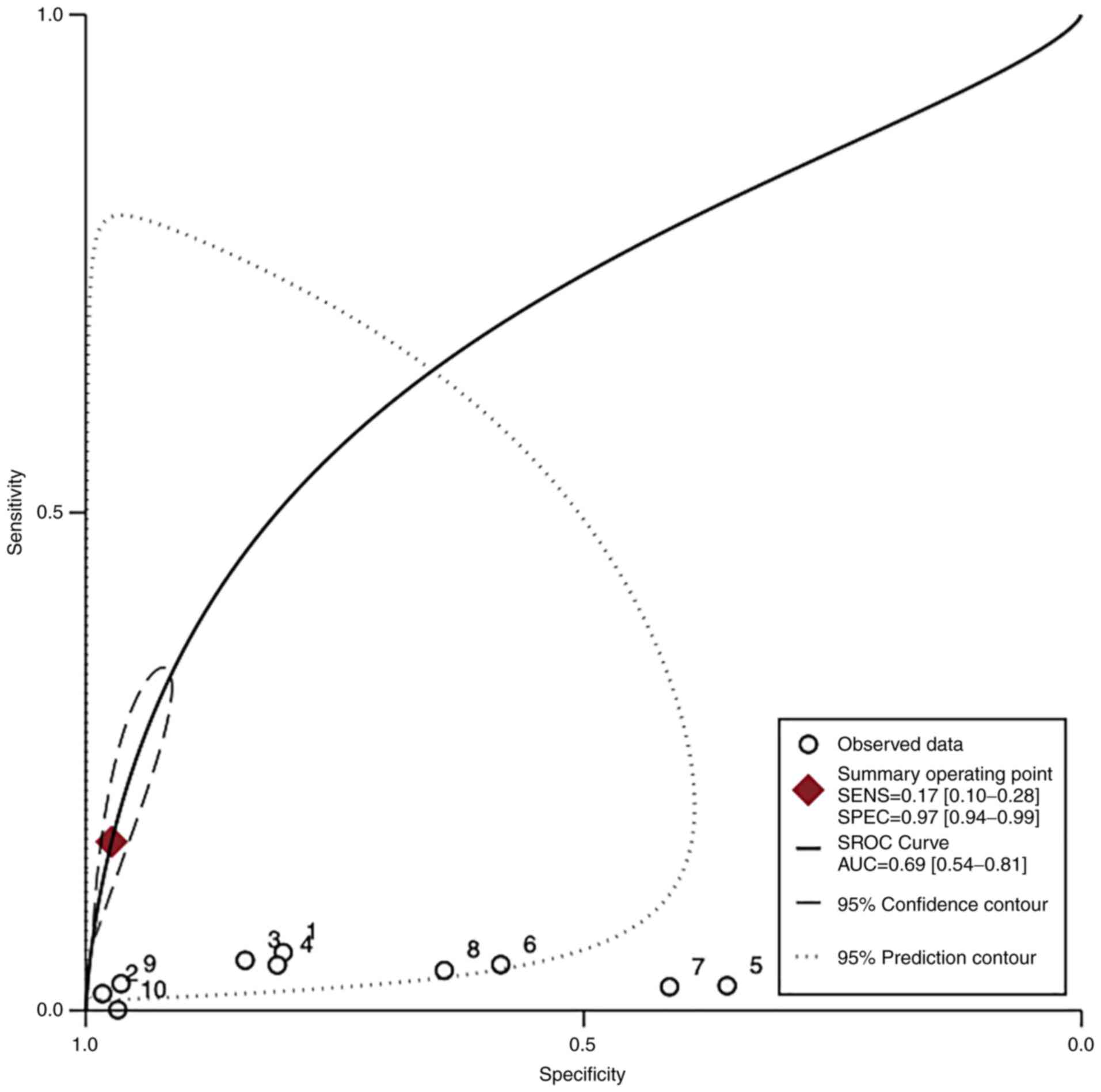
In the group of studies that categorized EO-PE
separately, the pooled sensitivity of PP-13 was 0.51 (95% CI,
-0.04-1.05, I2 0.0%) with a specificity of 0.88 (95% CI,
0.33-1.42, I2 0.0%) (Figs.
5 and 6). The area under the
SROC was 0.69 (95% CI, 0.54-0.81) (Fig.
7).
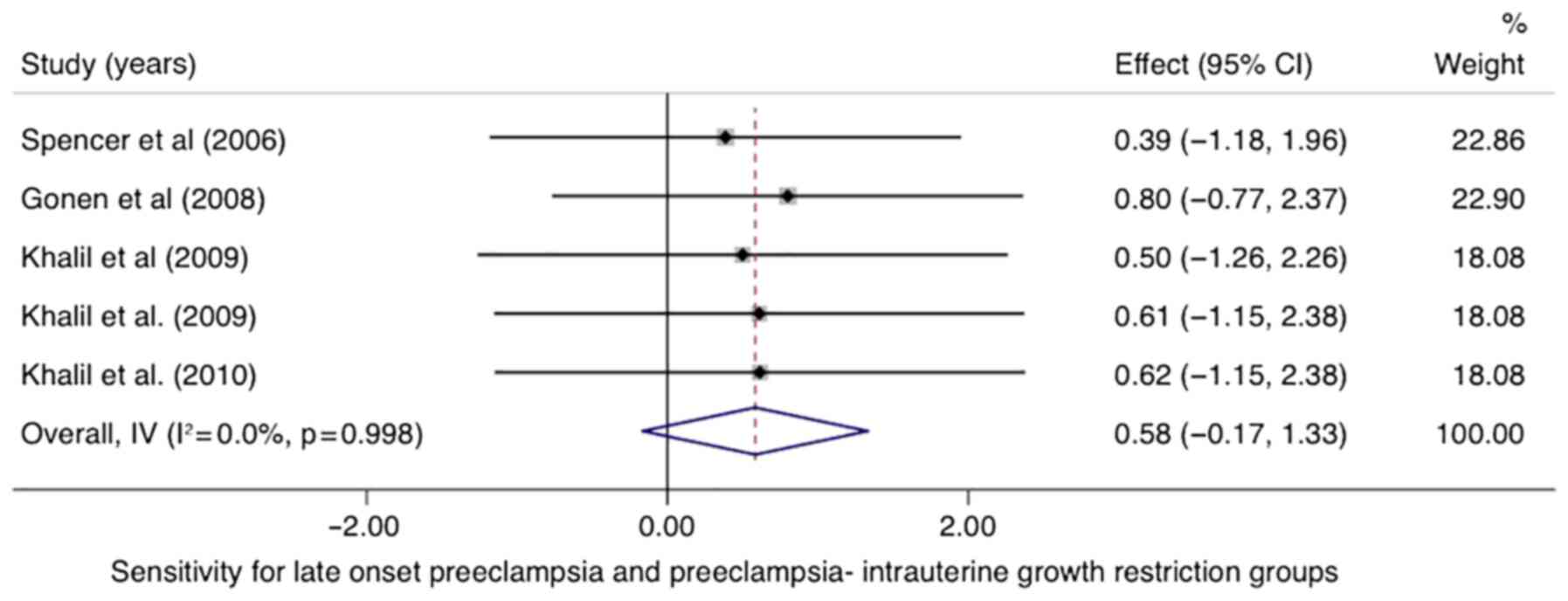
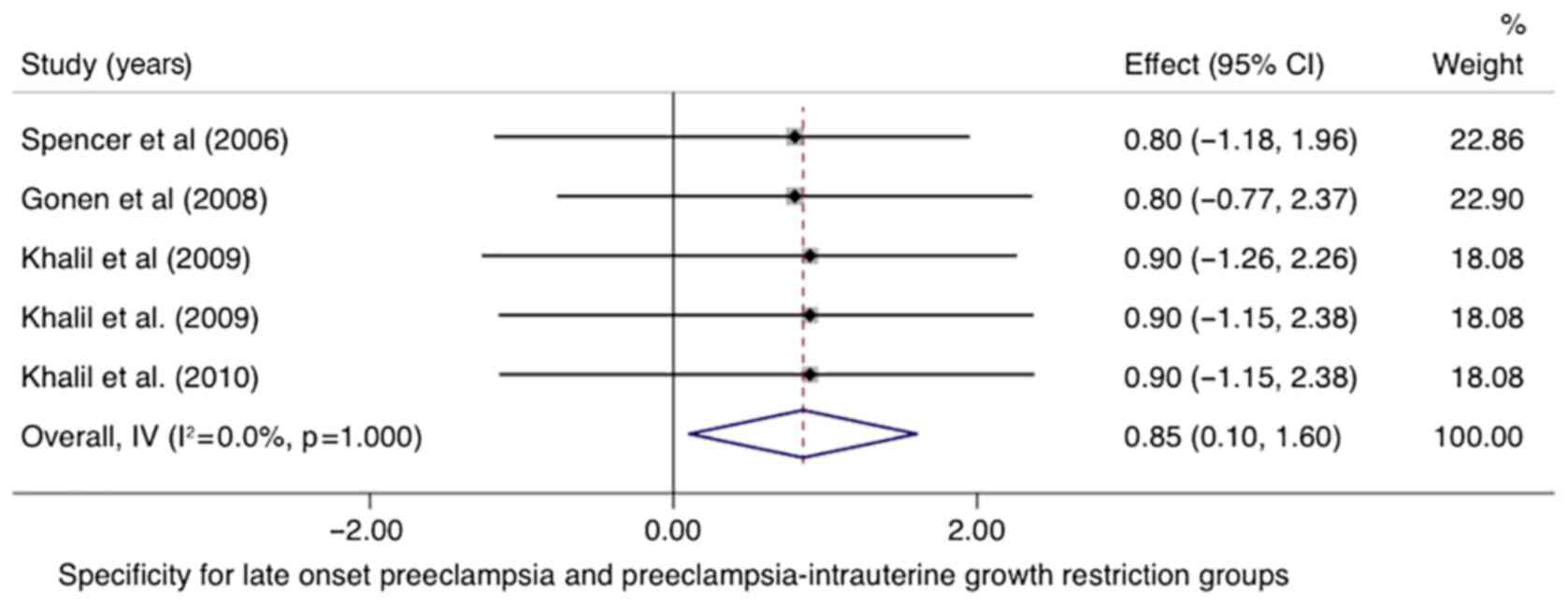
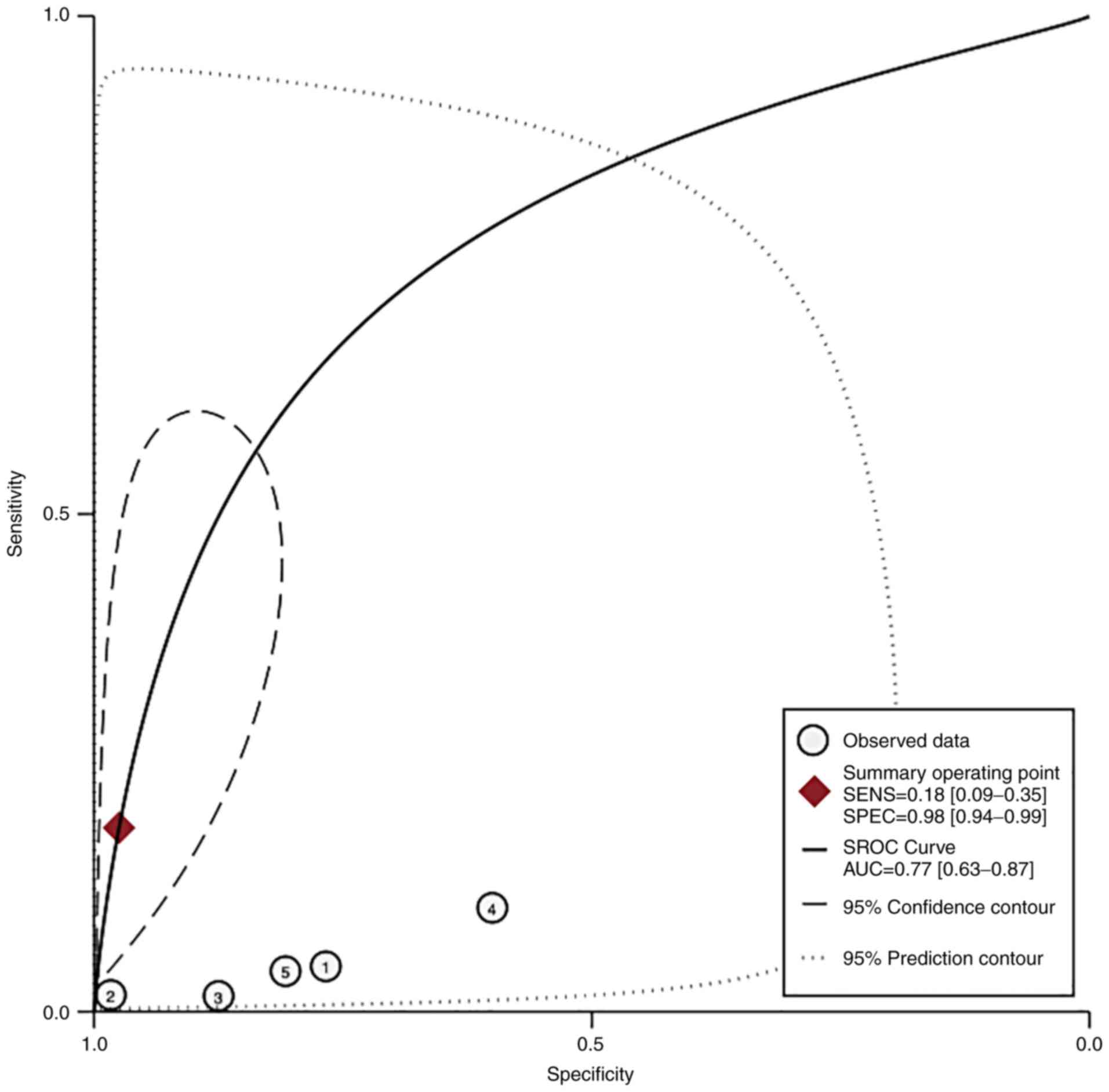
In the LO-PE/PE + SGA groups, the pooled sensitivity
of PP-13 was 0.58 (95% CI, -0.17-1.33, I2 0.0%) with a
specificity of 0.85 (95% CI, 0.10-1.60, I2 0.0%)
(Figs. 8 and 9). The area under the SROC was 0.77 (95%
CI, 0.63-0.87) (Fig. 10).
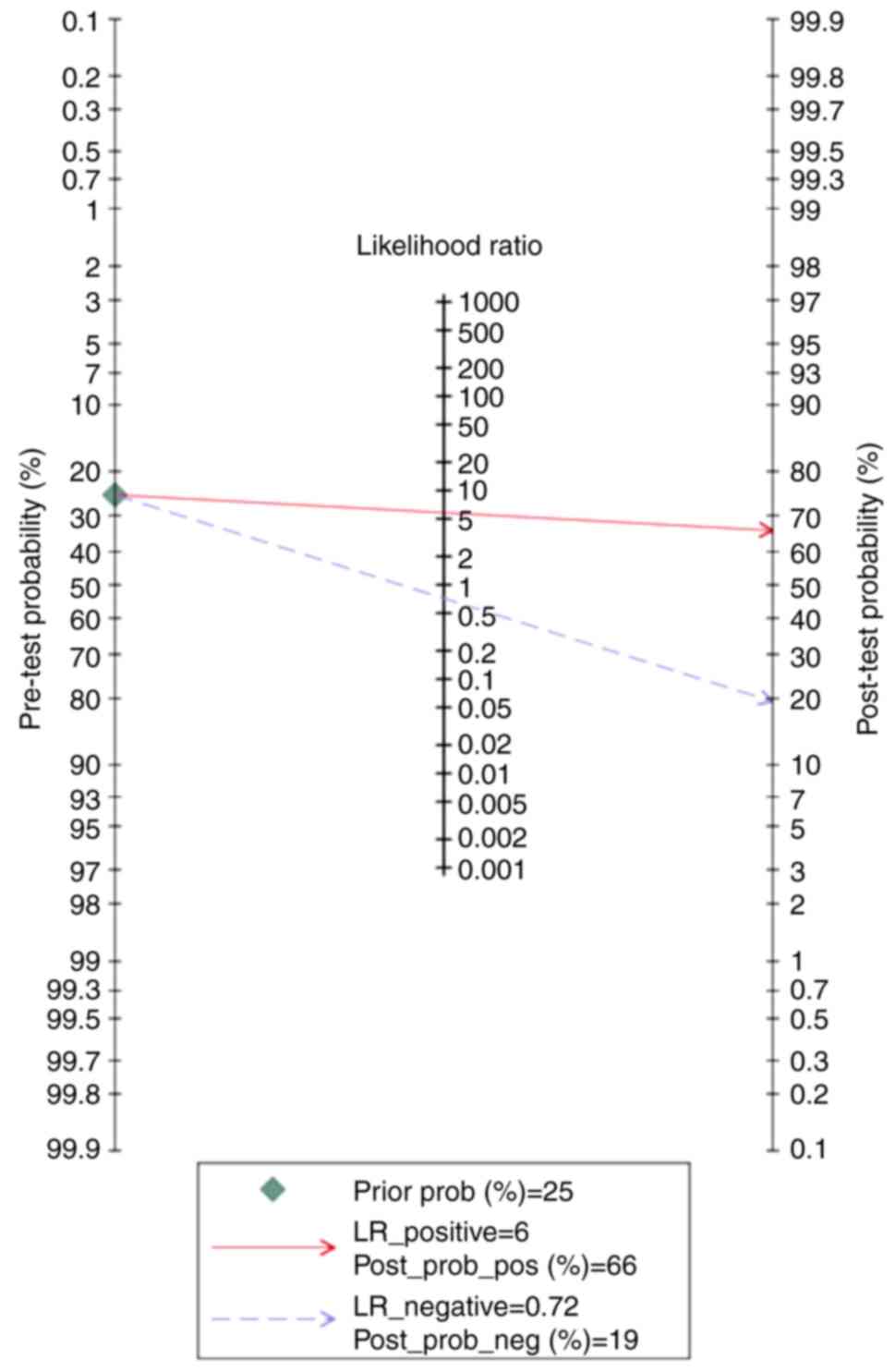
According to the Fagan nomogram, for a given
pre-test probability of 25% for the preeclampsia group, the
post-test probability was 66 and 19% for positive and negative
PP-13 biomarker readings, respectively (Fig. 11).
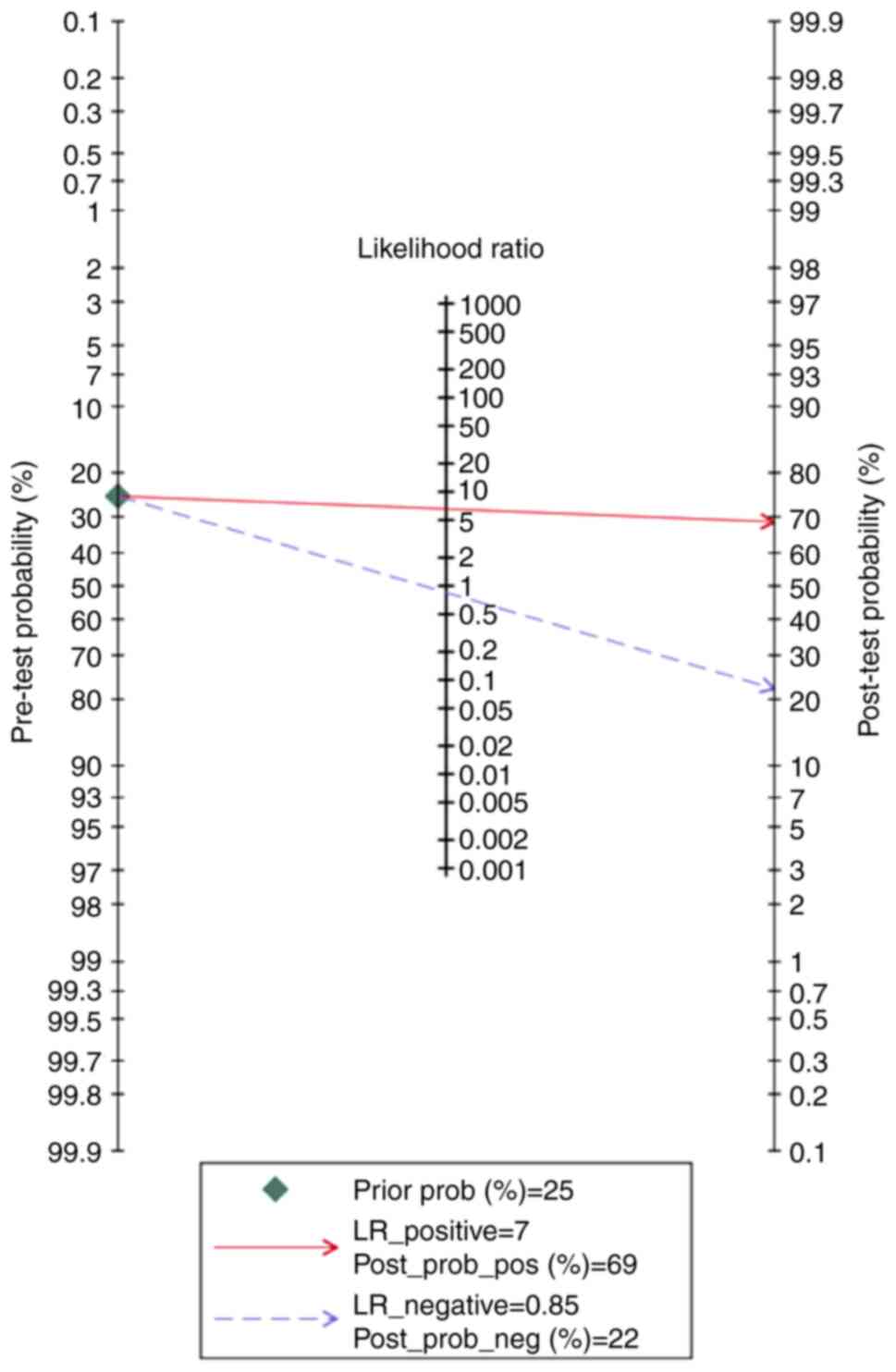
According to the Fagan nomogram, the positive and
negative results of the PP-13 biomarker had a post-test probability
of 69 and 22%, respectively, for the specified pre-test probability
of 25% for the EO-PE group (Fig.
12).
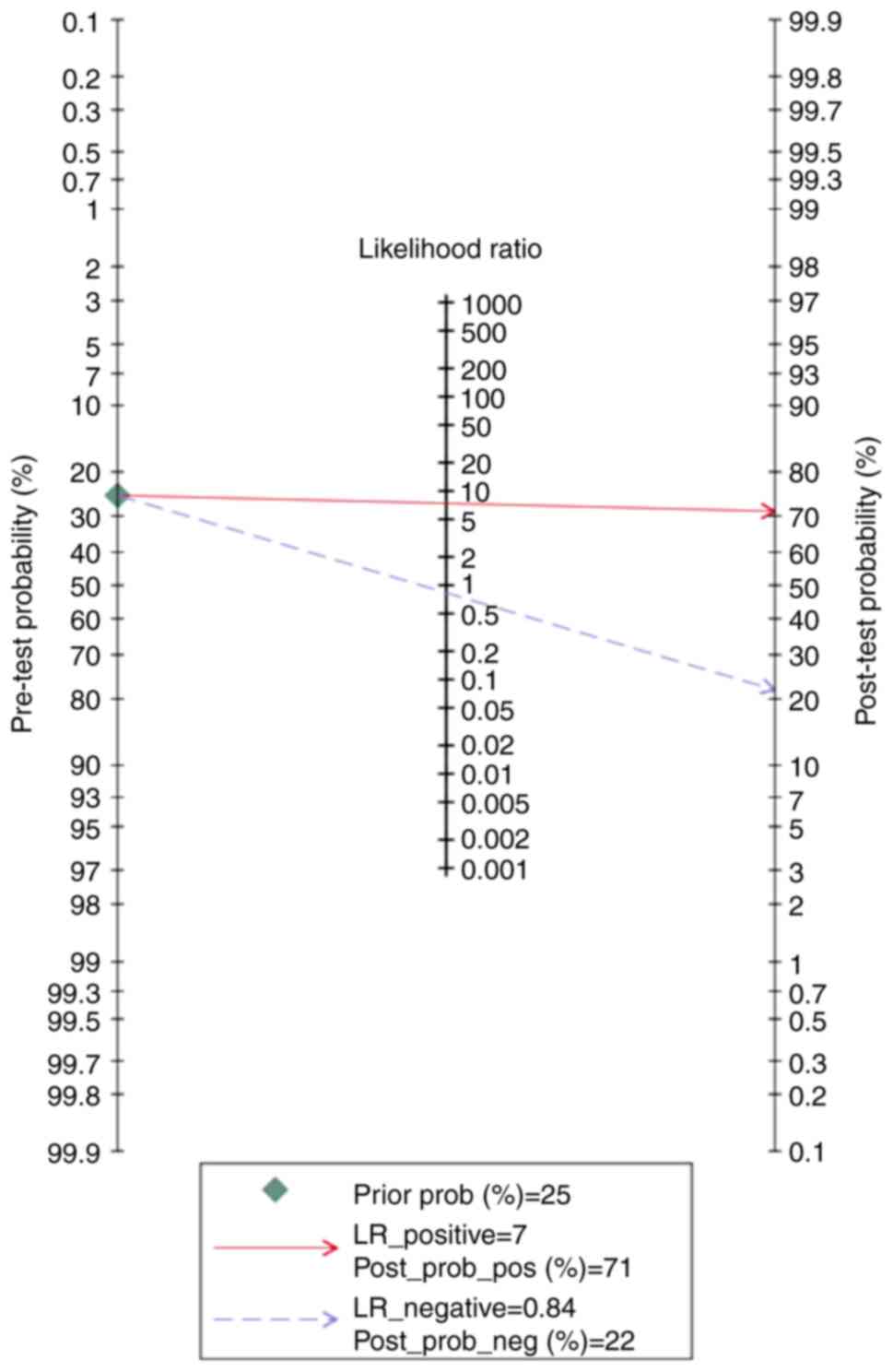
Finally, the Fagan nomogram revealed that, for a
given pre-test probability of 25% for the LO-PE/PE + SGA groups,
the post-test probability for positive and negative PP-13 biomarker
values was 71 and 22%, respectively (Fig. 13).
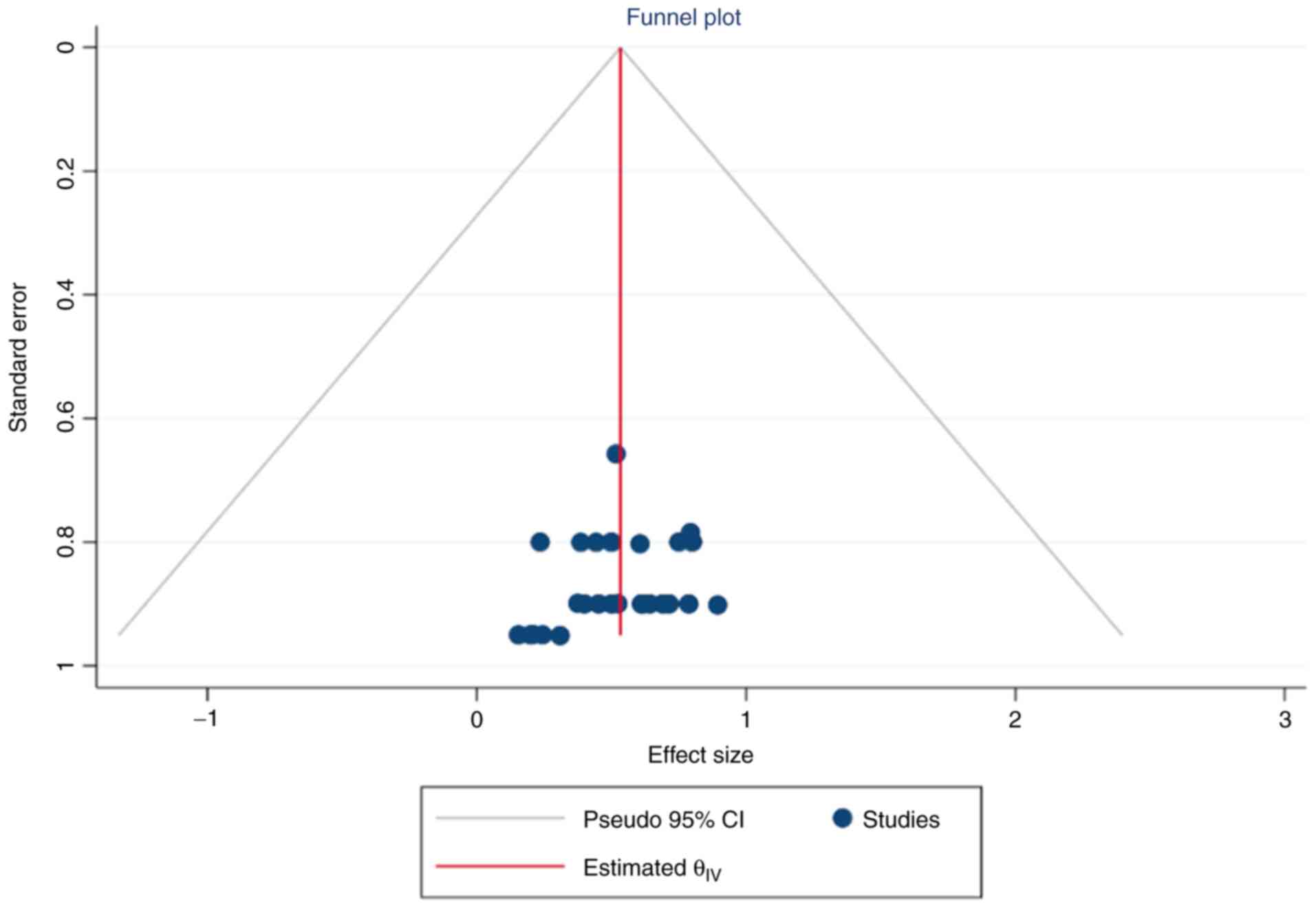
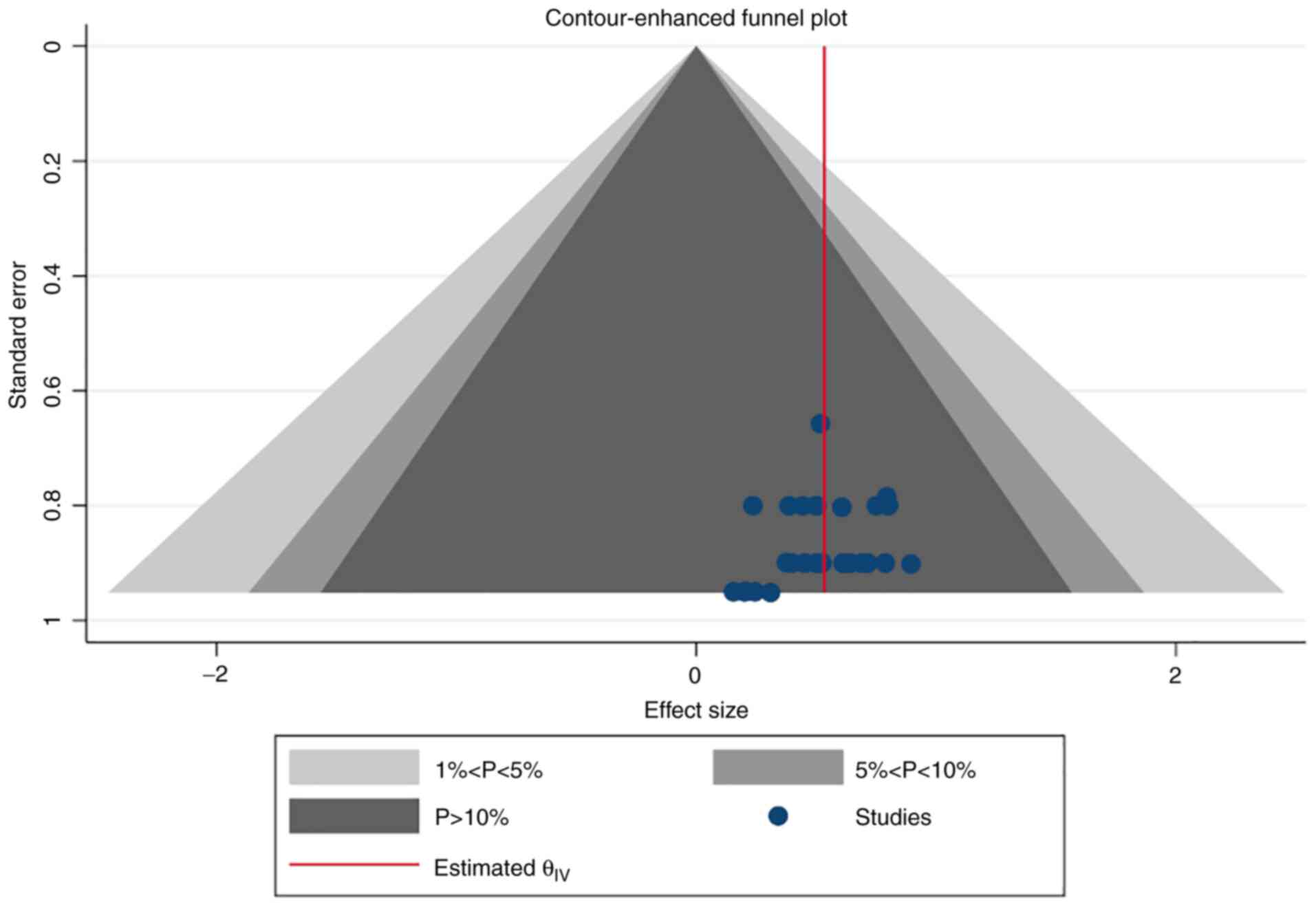
Simple and contour-enhanced funnel plots did not
indicate a risk of publication bias (Figs. 14 and 15).
Discussion
Preeclampsia is a multisystem condition with a
complex etiology. As a consequence, much research has been
conducted to identify the women at risk to improve pregnancy
outcomes. Clinical criteria alone, such as previous medical and
obstetric history, are ineffective in predicting the condition
(29). Therefore, it is important
to develop integrative algorithms to predict preeclampsia. These
include the use of novel biomarkers, sonographic features, and
maternal characteristics to obtain higher detection rates.
Protein-galectin-13 or placental protein-13 (PP-13),
a protein linked to cell differentiation and inflammatory processes
in the placenta, seems to be an effective biomarker for
preeclampsia screening (16,30).
This work is the first meta-analysis that offers an
overview of the discriminatory performance and predictive capacity
of the PP-13 biomarker for first trimester preeclampsia
screening.
A total of 14 studies met the inclusion criteria and
were subjected to quality testing using the QUADAS-2 tool. Our
results demonstrated good overall test accuracy in disease
prediction. Given the sensitivity and specificity of this marker,
the findings of this meta-analysis showed that maternal PP-13
concentration was lower in preeclampsia and could serve as a
valuable diagnostic marker (0.53 and 0.83, respectively).
The diagnostic accuracies in the various subgroups
further highlight the importance of PP-13 in preeclampsia. Studies
have demonstrated that the two forms of preeclampsia, early-onset
preeclampsia (EO-PE) and late-onset preeclampsia (LO-PE), have
different physiopathological backgrounds. EO-PE manifests secondary
to poor placentation, while LO-PE appears to be a placental
malperfusion, caused by limited uterine vascular capacity (31).
It is the EO-PE disease that contributes most to
perinatal morbidity, mortality and long-term maternal
complications, and therefore numerous efforts are put into its
recognition.
Our meta-analysis demonstrated that the predictive
performance of PP-13 in LO-PE was higher, although not
statistically significant, than that of EO-PE, indicating a good
screening performance of this biomarker for both forms of the
disease. Moreover, PP-13 had a good negative post-test probability
for all included groups (preeclampsia group, 19%; EO-PE group, 22%;
LO-PE/PE + SGA group, 22%).
The predictive performance of PP-13 could be
increased when using this biomarker in conjunction with maternal
characteristics and uterine artery Doppler parameters as shown by
previous studies (28,32).
Studies linking PP-13 to fetal growth restriction
(FGR) and oxidative stress indices in preeclamptic women suggest
the importance of PP-13 as a biomarker of poor placentation
throughout the prenatal period. In our meta-analysis, the summary
receiver operating characteristic curve (SROC) for the LO-PE and
the preeclampsia associated with small for gestational age fetuses
(PE-SGA) groups was 0.77.
Our meta-analysis has several limitations. Because
the results of our analysis were based mostly on case-control and
retrospective studies that examined PP-13 serum levels, the
possibility of selection bias must be considered. Furthermore, as
PP-13 serum levels were assessed during the first trimester of
pregnancy, its prognostic usefulness during the second and third
trimesters remains unknown.
The present meta-analysis could serve as a pilot for
future research as it provides substantial evidence that can be
employed in the design of future studies, especially when it comes
to assessing the predictive accuracy of the various cut-offs that
have been offered to date. This way, the possibility of bias will
be reduced, and comparable results will be produced, allowing for
the generalization of findings. PP-13 should be investigated in
multivariate models alongside other emerging biomarkers to develop
algorithms for providing the best predictive efficacy.
PP-13 could be used as a promising biomarker in
preeclampsia screening from the first trimester of pregnancy.
Compared to EO-PE, its predictive performance seems better for
LO-PE, but the difference between the two was not found to be
statistically significant. Because the current data is based on
first-trimester readings, more research is needed to determine its
prognostic accuracy later in pregnancy.
Given this information, more well-designed
prospective studies are needed to shed light on patient phenotypes
that appear to demonstrate the most noticeable differences (those
with severe, early-onset preeclampsia and those who are prone to
developing eclampsia).
The inclusion of PP-13 in predictive models with
existing biomarkers could aid in determining its potential
additional value in predicting disease and the severity of the
associated consequences.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
This meta-analysis was written as part of the
doctoral program for IAV at ‘Grigore T. Popa’ University. DN, AC
and IAV performed the systematic review, analyzed data, and wrote
the manuscript; AC, DN and DS interpreted the data; DN, IAV, RM and
IP developed the study concept and design. DN and DS carried out
the literature search, and were assisted by AC and IAV, who
retrieved the evidence and chose the papers. The data were
extracted by AC, IAV and DS. The final version of the publication
was written by IAV, AC, DN and DS. A final inspection of the
manuscript was entrusted to IAV and DN. All authors read and
approved the final manuscript for publication.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
All authors report no competing interests.
References
|
1
|
Ananth CV, Keyes KM and Wapner RJ:
Pre-eclampsia rates in the United States, 1980-2010:
Age-period-cohort analysis. BMJ. 347(f6564)2013.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Barondes SH, Castronovo V, Cooper DN,
Cummings RD, Drickamer K, Feizi T, Gitt MA, Hirabayashi J, Hughes
C, Kasai K, et al: Galectins: A family of animal
beta-galactoside-binding lectins. Cell. 76:597–598. 1994.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kang HG, Kim DH, Kim SJ, Cho Y, Jung J,
Jang W and Chun KH: Galectin-3 supports stemness in ovarian cancer
stem cells by activation of the Notch1 intracellular domain.
Oncotarget. 7:68229–68241. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Sammar M, Drobnjak T, Mandala M,
Gizurarson S, Huppertz B and Meiri H: Galectin 13 (PP13)
facilitates remodeling and structural stabilization of maternal
vessels during pregnancy. Int J Mol Sci. 20(3192)2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Page MJ, Moher D, Bossuyt PM, Boutron I,
Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: PRISMA 2020 explanation and elaboration: Updated
guidance and exemplars for reporting systematic reviews. BMJ.
372(n160)2021.PubMed/NCBI View
Article : Google Scholar
|
|
6
|
National Center for Biotechnology
Information (NCBI). PubMed database. https://pubmed.ncbi.nlm.nih.gov/. Accessed February
28, 2021.
|
|
7
|
Clarivate. Web of Science database.
https://clarivate.com/webofsciencegroup/solutions/web-of-science/.
Accessed on 28.02.2021.
|
|
8
|
Elsevier. Scopus database. https://www.scopus.com/home.uri. Accessed
February 28, 2021.
|
|
9
|
Elsevier. Embase database. https://www.embase.com/landing?status=grey. Accessed
February 28, 2021.
|
|
10
|
Clarivate. BIOSISCitationIndex. https://clarivate.com/webofsciencegroup/solutions/webodscience-biosis-citation-index/.
Accessed February 28, 2021.
|
|
11
|
Cochrane Library. Cochrane database.
https://www.cochranelibrary.com/.
Accessed February 28, 2021.
|
|
12
|
Whiting P, Rutjes AW, Reitsma JB, Bossuyt
PM and Kleijnen J: The development of QUADAS: A tool for the
quality assessment of studies of diagnostic accuracy included in
systematic reviews. BMC Med Res Methodol. 3(25)2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Whiting PF, Rutjes AW, Westwood ME,
Mallett S, Deeks JJ, Reitsma JB, Leeflang MM, Sterne JA and Bossuyt
PM: QUADAS-2 Group. QUADAS-2: A revised tool for the quality
assessment of diagnostic accuracy studies. Ann Intern Med.
155:529–536. 2011.PubMed/NCBI View Article : Google Scholar
|
|
14
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials revisited. Contemp Clin Trials. 45:139–145.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Spencer K, Cowans NJ, Chefetz I, Tal J and
Meiri H: First-trimester maternal serum PP-13, PAPP-A and
second-trimester uterine artery Doppler pulsatility index as
markers of pre-eclampsia. Ultrasound Obstet Gynecol. 29:128–134.
2007.PubMed/NCBI View
Article : Google Scholar
|
|
16
|
Chafetz I, Kuhnreich I, Sammar M, Tal Y,
Gibor Y, Meiri H, Cuckle H and Wolf M: First-trimester placental
protein 13 screening for preeclampsia and intrauterine growth
restriction. Am J Obstet Gynecol. 197:35.e1–e7. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Gonen R, Shahar R, Grimpel YI, Chefetz I,
Sammar M, Meiri H and Gibor Y: Placental protein 13 as an early
marker for pre-eclampsia: A prospective longitudinal study. BJOG.
115:1465–1472. 2008.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Khalil A, Cowans NJ, Spencer K, Goichman
S, Meiri H and Harrington K: First trimester maternal serum
placental protein 13 for the prediction of pre-eclampsia in women
with a priori high risk. Prenat Diagn. 29:781–789. 2009.PubMed/NCBI View
Article : Google Scholar
|
|
19
|
Akolekar R, Syngelaki A, Beta J,
Kocylowski R and Nicolaides KH: Maternal serum placental protein 13
at 11-13 weeks of gestation in preeclampsia. Prenat Diagn.
29:1103–1108. 2009.PubMed/NCBI View
Article : Google Scholar
|
|
20
|
Khalil A, Cowans NJ, Spencer K, Goichman
S, Meiri H and Harrington K: First-trimester markers for the
prediction of pre-eclampsia in women with a-priori high risk.
Ultrasound Obstet Gynecol. 35:671–679. 2010.PubMed/NCBI View
Article : Google Scholar
|
|
21
|
Wortelboer EJ, Koster MP, Cuckle HS,
Stoutenbeek PH, Schielen PC and Visser GH: First-trimester
placental protein 13 and placental growth factor: Markers for
identification of women destined to develop early-onset
pre-eclampsia. BJOG. 117:1384–1389. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Odibo AO, Zhong Y, Goetzinger KR, Odibo L,
Bick JL, Bower CR and Nelson DM: First-trimester placental protein
13, PAPP-A, uterine artery Doppler and maternal characteristics in
the prediction of pre-eclampsia. Placenta. 32:598–602.
2011.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Schneuer FJ, Nassar N, Khambalia AZ,
Tasevski V, Guilbert C, Ashton AW, Morris JM and Roberts CL: First
trimester screening of maternal placental protein 13 for predicting
preeclampsia and small for gestational age: In-house study and
systematic review. Placenta. 33:735–740. 2012.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Deurloo KL, Linskens IH, Heymans MW,
Heijboer AC, Blankenstein MA and van Vugt JM: ADAM12s and PP13 as
first trimester screening markers for adverse pregnancy outcome.
Clin Chem Lab Med. 51:1279–1284. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Meiri H, Sammar M, Herzog A, Grimpel YI,
Fihaman G, Cohen A, Kivity V, Sharabi-Nov A and Gonnen R:
Prediction of preeclampsia by placental protein 13 and background
risk factors and its prevention by aspirin. J Perinat Med.
42:591–601. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Luo Q and Han X: Second-trimester maternal
serum markers in the prediction of preeclampsia. J Perinat Med.
45:809–816. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Asiltas B, Surmen-Gur E and Uncu G:
Prediction of first-trimester preeclampsia: Relevance of the
oxidative stress marker MDA in a combination model with PP-13,
PAPP-A and beta-HCG. Pathophysiology. 25:131–135. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Soongsatitanon A and Phupong V: Prediction
of preeclampsia using first trimester placental protein 13 and
uterine artery Doppler. J Matern Fetal Neonatal Med: Nov 16, 2020
(Epub ahead of print).
|
|
29
|
North RA, McCowan LM, Dekker GA, Poston L,
Chan EH, Stewart AW, Black MA, Taylor RS, Walker JJ, Baker PN and
Kenny LC: Clinical risk prediction for pre-eclampsia in nulliparous
women: Development of model in international prospective cohort.
BMJ. 342(d1875)2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kliman HJ, Sammar M, Grimpel YI, Lynch SK,
Milano KM, Pick E, Bejar J, Arad A, Lee JJ, Meiri H and Gonen R:
Placental protein 13 and decidual zones of necrosis: An immunologic
diversion that may be linked to preeclampsia. Reprod Sci. 19:16–30.
2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Redman CW, Sargent IL and Staff AC: IFPA
Senior award lecture: Making sense of pre-eclampsia-two placental
causes of preeclampsia? Placenta. 35 (Suppl 1):S20–S25.
2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Monte S: Biochemical markers for
prediction of preclampsia: Review of the literature. J Prenat Med.
5:69–77. 2011.PubMed/NCBI
|