Introduction
Ureteropelvic junction obstruction (UPJO) is a
common congenital malformation of the urinary system, which is
mostly unilateral, and laparoscopic pyeloplasty is the optimal
minimally invasive surgical procedure. However, UPJO is frequently
combined with hydronephrosis and kidney stones. The incidence of
kidney stones is ~20%, which markedly increases the difficulty and
risk of surgery (1). In the
present case report, a challenging case is discussed. The patient
underwent laparoscopy and ureteroscopy one-stage surgery for the
treatment of bilateral UPJO with renal stones and the surgery
outcome was ideal.
Case report
The 20-year-old male patient was admitted to the
Affiliated Hospital of Hebei University of Engineering (Handan,
China) due to intermittent right waist and abdomen distension for 2
days in June 2020. The patient had right waist and abdomen soreness
with no obvious cause since 2 days previously, without any symptoms
of urinary frequency, urinary urgency and gross hematuria. Physical
examination revealed mild percussion pain in both renal regions and
no tenderness pain in the bilateral ureteral travel area.
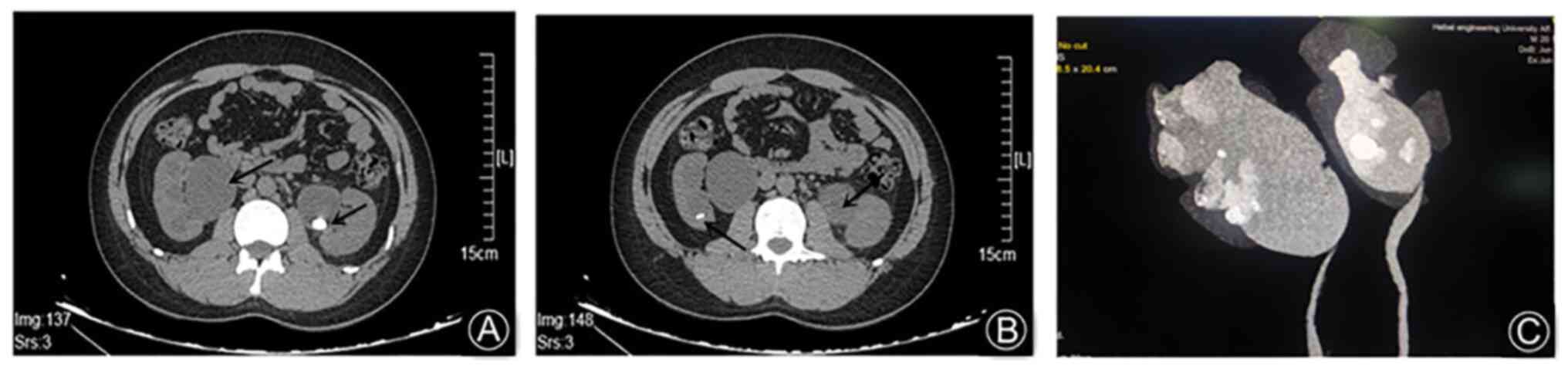
Creatinine was 83 µmol/l. Ultrasound examination revealed bilateral
kidney stones in the renal pelvis and calyces, with dilation of the
renal pelvis and calyces, and the bilateral ureteropelvic junction
was thickened (Fig. 1). Thus,
bilateral UPJO with bilateral renal stones was considered. The
preoperative diagnosis was bilateral UPJO with bilateral kidney
stones. Laparoscopy and ureteroscopy bilateral pyeloplasty and
bilateral kidney stones Holmium laser lithotripsy was performed
under general anesthesia. The right side was elevated at 45˚ and
the pneumoperitoneum was established by entering the Veress needle
at the right margin of the umbilicus. The pressure was set at 15
mmHg. After the pneumoperitoneum reached the set pressure, 10, 5
and 10 mm trocars were placed at the umbilicus, McBurney's point
and 3 cm below the 12th rib of the midclavicular line,
respectively. The right colon and abdominal wall adhesions were
obvious and the ultrasonic knife was used to fully expose the right
renal pelvis and the upper end of the right ureter, and part (~3
mm) of the ureteropelvic junction was cut off and a ureteroscope
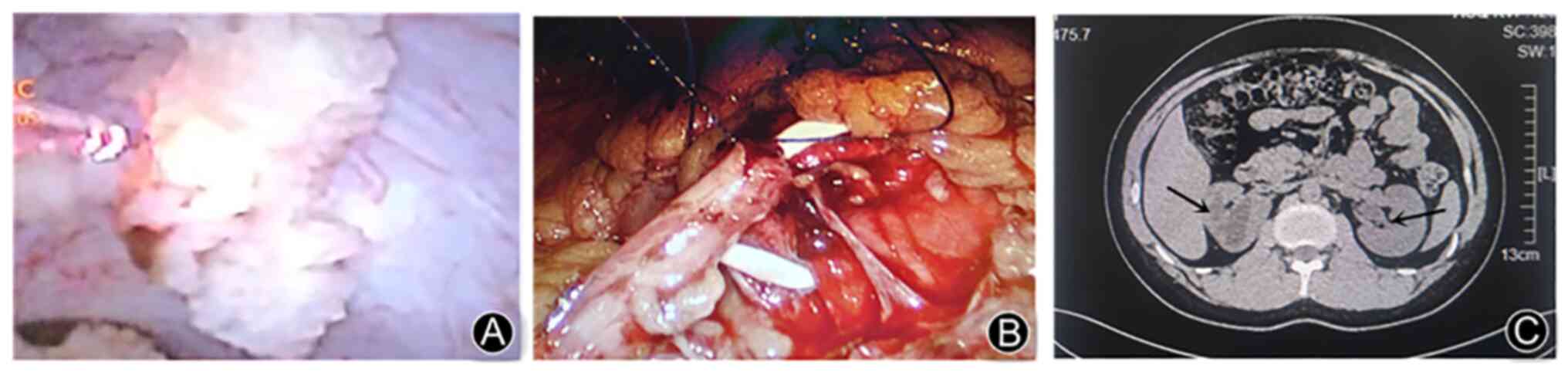
was placed to explore each renal calyx. After finding the stone,
the Holmium laser was used to turn the stone into powder (Fig. 2A). Furthermore, after lithotripsy
was completed, the obstruction was removed and the right
pyeloplasty was continued with laparoscopy (Fig. 2B). A 6F double J stent was placed
in the ureter and a rubber drain was placed and fixed at the pelvic
and ureteral anastomosis. The vital signs of the patient were
stable after operation of the right side. Similarly, trocars were
placed at the left anti-McBurney's point and 3 cm below the 12th
rib of the midclavicular line, and the intestine was pushed into
the right abdomen to expose the left kidney and obtain a field of
view. Part of the left obstruction was cut open and a ureteroscope
was placed for exploration. Holmium laser lithotripsy and
laparoscopic left pyeloplasty were performed. The double J stent
was placed, the absence of active bleeding was confirmed and a
rubber drain was placed at the left anastomosis. The procedure went
smoothly without any complications, such as macrovascular or
adjacent organ damage. The operation time was 264 min and the
exhaust time was 28 h after surgery. Review of diagnostic radiology
of the urinary system 3 days after the surgery revealed that the
double J stents were well placed and no stone residue was observed.
The postoperative body temperature was stable and the patient had
no fever. The drainage was markedly reduced 5 days after the
surgery, the abdominal drainage tube was removed, the urinary
catheter was removed and the patient was discharged 10 days after
the surgery. The double J stents were removed after 2 months.
Review of the CT after 3 months revealed that the hydronephrosis
was markedly reduced and the ureteropelvic junction was patent
without any residual stone (Fig.
2C).
Discussion
UPJO is a common disease of the urinary system and
the pathogenic feature is that normal helical muscle tissue of the
ureter is replaced by abnormal vertical bunch or fibrous tissue,
which leads to the loss of normal peristaltic rushes in the ureter
and the blocking of urine transmission from the renal pelvis to the
ureter (2). Although most patients
have congenital malformations, the majority exhibit clinical
symptoms long after birth; severe obstructions may lead to
inadequate drainage of the upper urinary tract, which leads to a
vicious circle of hydronephrosis, kidney stones and urinary tract
infections (3). Therefore, the
renal function of patients is seriously affected.
The traditional ‘gold standard’ of clinical
treatment is dismembered Anderson-Hynes pyeloplasty (4); however, this has certain
shortcomings, such as large trauma, intense pain and long recovery
time. Laparoscopic pyeloplasty was first proposed by Schuessler in
1993 and has become one of the conventional treatments for UPJO
after >20 years of development (5). The efficacy is comparable to that of
open surgery and an effective rate of 90-95% has been reported in
the literature (6). In recent
years, with the continuous development of medical care,
laparoscopic pyeloplasty has become more common in the treatment of
UPJO and has gradually become the new ‘gold standard’ of UPJO
treatment (7). The primary
advantages include reduced trauma, fewer complications, faster
recovery, a significant therapeutic effect, safety and reliability.
Laparoscopic pyeloplasty has two main surgical approaches:
Transabdominal and retroperitoneal (8). Retroperitoneoscopic pyeloplasty is
widely accepted by Chinese surgeons, as it has a relatively closed
gap with only small interference with the intestine, although the
operational room is tight. UPJO is frequently accompanied by kidney
stones, which makes the operation more difficult, and the operation
requires fenestration with the endoscope through the renal pelvis
during the laparoscopy and ureteroscopy surgery. The
extraperitoneal approach is more difficult due to the large angle
of the endoscope. The abdominal approach has obvious advantages
when investigating the collecting system, as the endoscope placed
through the trocar is facing the renal pelvis (9).
In the present case, laparoscopy and ureteroscopy
one-stage surgery were used to treat UPJO combined with bilateral
kidney stones and the surgical outcomes were ideal; to the best of
our knowledge, the present study was the first to report this type
of procedure. One-stage surgery for bilateral pyeloplasty has been
indicated to be both safe and effective (10), but there are no other relevant
reports for cases accompanied by kidney stones at present.
According to clinical guidelines and clinical practice, if the
patient has bilateral hydronephrosis, the side with severe
hydronephrosis, obvious renal injury or severe symptoms is usually
treated first. Although bilateral staged surgery is safer, patients
are required to undergo two operations. Considering that the
patient was a young male in otherwise good health and with
relatively normal renal function, and the patient and his family
had a strong desire for one-stage treatment, it was explained to
the patient's family that if bilateral pyeloplasty and lithotripsy
could not be completed at the same time, the left side with mild
hydronephrosis would need to be treated in stages, and the family
understood and agreed to the treatment. In order to reduce the
patient's psychological burden, reduce the trauma and avoid the
long operational time caused by changing the position during the
operation, the transabdominal laparoscopy and ureteroscopy
one-stage surgery was performed after comprehensive consideration.
The postoperative review revealed that there was no stone residue,
the temperature was stable and there was no urine extravasation
from the anastomosis. The following observations were made during
the treatment: i) As the transabdominal endoscope placed through
the trocar was facing the renal pelvis, the collecting system was
able to be fully exposed, which markedly improved the stone removal
rate (11); ii) the water pressure
during lithotripsy cannot be too high and a large amount of
high-pressure flushing may easily lead to the spread of infection
and cannot ensure the removal of stones; iii) after freeing the
ureteropelvic junction, the fenestration cannot be too large, so
that the endoscope may pass smoothly, which may effectively prevent
the stone entering into the abdominal cavity with the flushing
fluid; iv) a small amount of residual stone may be removed by a
stone basket; v) since the position of the pelvic fenestration does
not coincide with that of the transurethral procedure, the operator
may miss the stone with regular endoscope exploration habits and
steps, so C-arm fluoroscopy during the operation is recommended to
assist in positioning and observing whether the stone is completely
removed; vi) the drainage tube should be placed at the lowest point
in the abdominal cavity for full drainage; and vii) in the present
study, the combination of laparoscopic pyeloplasty and ureteroscopy
was an ideal treatment for UPJO combined with kidney stones, as it
has the unique advantages of the two minimally invasive treatments,
compensates for the shortcomings of each and allows for the
completion of both ‘forming’ and ‘lithotomy’ in one surgery without
increasing the risk.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Hebei Province
Natural Science Foundation of China (grant no. H2021402018).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
WF and CR collected data, performed data analysis
and drafted the manuscript. JZ and HC designed the operation
procedures and revised the manuscript. JZ contributed to the
minimally invasive surgery. WF and HC provided assistance in the
operation. WF, JZ and HC confirm the authenticity of all the raw
data. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
All clinical application protocols for the
techniques performed were approved by the Ethics Committee of the
Affiliated Hospital of Hebei University of Engineering (Handan,
China). The subject signed an informed consent form and had
complete clinical data.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data and accompanying
figures.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hüttenbrink C, Kelm P, Klein T, Distler F,
Pandey A and Pahernik S: Combination of robotic pyeloplasty and
percutaneous renal surgery for simultaneous treatment of
ureteropelvic junction obstruction and calyx stones. Urol Int.
105:637–641. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Rutchik SD and Resnick MI: Ureteropelvic
junction obstruction and renal calculi. Pathophysiology and
implications for management. Urol Clin North Am. 25:317–321.
1998.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Stasinou T, Bourdoumis A and Masood J:
Forming a stone in pelviureteric junction obstruction: Cause or
effect? Int Braz J Urol. 43:13–19. 2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Paik ML, Wainstein MA, Spirnak JP, Hampel
N and Resnick MI: Current indications for open stone surgery in the
treatment of renal and ureteral calculi. J Urol. 159:374–378.
1998.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Schuessler WW, Grune MT, Tecuanhuey LV and
Preminger GM: Laparoscopic dismembered pyeloplasty. J Urol.
150:1795–1799. 1993.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Szavay P: Laparoscopic pyeloplasty for
ureteropelvic junction obstruction. J Laparoendosc Adv Surg Tech A.
31:1214–1218. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Jia J, Meng Q, Zhang M, Qi J and Wang D: A
comparative study on the efficacy of retroperitoneoscopic
pyeloplasty and open surgery for ureteropelvic junction obstruction
in children. Pak J Med Sci. 37:1768–1774. 2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ji F, Chen L, Wu C, Li J, Hang Y and Yan
B: Meta-analysis of the efficacy of laparoscopic pyeloplasty for
ureteropelvic junction obstruction via retroperitoneal and
transperitoneal approaches. Front Pediatr. 9(707266)2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Song P, Shu M, Peng Z, Yang L, Zhou M,
Wang Z, Lu N, Pei C and Dong Q: Transperitoneal versus
retroperitoneal approaches of pyeloplasty in management of
ureteropelvic junction obstruction: A meta-analysis. Asian J Surg.
45:1–7. 2022.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Juntao X, Wenzong G, Zuoqing L, Li Z and
Zhe X: Robotic-assisted bilateral simultaneous dismembered
pyeloplasties in children. J Clin Ped Sur. 20:257–262. 2021.
|
|
11
|
Ball AJ, Leveillee RJ, Patel VR and Wong
C: Laparoscopic pyeloplasty and flexible nephroscopy: Simultaneous
treatment of ureteropelvic junction obstruction and
nephrolithiasis. JSLS. 8:223–228. 2004.PubMed/NCBI
|