Introduction
The pandemic caused by severe acute respiratory
syndrome coronavirus 2 (SARS-CoV-2) has spread worldwide since
December 2019; overall, >280 million cases have been reported
globally and the number of deaths exceeds 5 million (1).
Neurological manifestations of SARS-CoV-2 infection
are common, varying from mild cases (including dysgeusia, anorexia,
olfactory dysfunction and nausea) to more debilitant symptoms,
including fatigue, headache and dizziness. Severe diseases such as
encephalitis and meningitis have also been reported as
complications of novel coronavirus disease 2019 (COVID-19)
(1). A series of studies (2-7)
have also shown a possible association between Guillain-Barré
syndrome (GBS), the most common cause of acute flaccid paralysis in
all ages (8), and SARS-CoV-2
infection.
The incidence of GBS increases with age, peaking at
70-80 years old (4-5 cases/100,000 individuals). By contrast, it is
a rare pathology at pediatric age, with an incidence of 0.62
cases/100,000 children aged 0-9 years, and 0.75/100,000 children
aged 10-19(9). GBS is usually
triggered by common infections such as minor respiratory illnesses,
gastrointestinal illnesses and immunizations. The pathogenesis of
SARS-CoV-2-associated GBS remains under debate; several reports
suggested a para-infectious etiology, while others suggest a
classical immune-mediated post-infectious mechanism.
GBS may present in a number of clinical variants,
ranging from the acute demyelinating inflammatory polyneuropathy
(AIDP) to the acute motor axonal neuropathy (AMAN). Both are
characterised by rapidly-progressing, ascending symmetrical
weakness, with attenuation or loss of muscle proprioceptive
reflexes.
Campylobacter plays a significant role among the
infectious triggers, in particular for Miller Fisher Syndrome
(MFS), the localized form of GBS characterized by ophthalmoplegia,
ataxia, and areflexia. In the differential diagnosis of GBS,
Borreliosis, Citomegalovirus infection and rare cases of
paraneoplastic isolated myelopathy must be excluded (10).
Among pediatric patients, 75% can no longer walk
unaided in the acute phase, 30% are tetraparetic, 35-50% show
cranial nerve involvement, and 15-20% have respiratory failure
and/or autonomic dysfunction (9).
Localised forms of GBS such as MFS and Chronic inflammatory
demyelinating polyneuropathy (CIDP) are extremely rare in childhood
(11).
Case reports of COVID-19-associated GBS mainly
include adult patients, while only a few pediatric cases have been
reported (12-25).
Here we describe the case of a GBS in an Italian
9-year-old girl with previous SARS-CoV-2 infection as a possible
trigger and we conduct a literature review on pediatric
COVID-19-associated GBS cases.
Materials and methods
Infectious and immunological research
kits
We used the following kits for the infectious and
immunological tests carried out in our patient: PCR analysis on
cerebrospinal fluid (CSF): BioFire®
FilmArray® meningitis/encephalitis (ME) panel (BioFire
Diagnostics, LLC); CMV PCR search on CSF: CMV ELITe MGB®
Kit(ELITe InGenius® ELITechGroup); Campylobacter search
on stools: culture on Biomerieux plates and identification with
VITEK MS Maldi-Toff Biomerieux; Autoantibodies search on CSF:
GanglioCombiTM ELISA (Buhlmann Laboratories AG);
Paraneoplastic antibodies search on CSF: EUROLINE paraneoplastic
neurological syndromes 12 Ag (igG) (EUROIMMUN Medizinische
Labordiagnostija AG); Viral serologies (SARS-CoV-2, CMV and EBV) on
plasma: LIAISON SARS-CoV-2 S1/S2 IgG; CMV IgG and IgM; EBV IgG and
IgM; DiaSorin
Magnetic resonance imaging (MRI)
parameters
Philips Ingenia 1,5T; Spin-echo, Turbo Spin-Echo,
Inversion Recovery, Gradient Echo, Echo Planar with T1, T2, DP
weighted sequences, pre and post-contrast.
Literature review criteria
We systematically reviewed literature available on
PubMed until November 2021 in order to find all pediatric cases of
GBS associated with SARS-CoV-2 infection (3-17 years) reported as
case report, meta-analysis, randomized controlled trial, review and
systematic review. We only considered papers written in
English.
The PubMed search string was: (‘Coronavirus’ OR
‘Coronavirus disease’ OR ‘novel coronavirus’ OR ‘Severe acute
respiratory syndrome coronavirus 2’ OR ‘COVID-19’ OR ‘nCoV 2019’ OR
‘SARS-CoV-2’) AND (‘Guillain-Barré syndrome’ OR ‘GBS’ OR ‘Miller
Fisher syndrome’ OR ‘MFS’ OR ‘Miller Fisher-GBS overlap syndrome’
OR ‘MFS-GBS overlap syndrome’ OR ‘acute inflammatory demyelinating
polyneuropathy’ OR ‘AIDP’ OR ‘acute motor axonal neuropathy’ OR
‘AMAN’ OR ‘acute motor sensory axonal neuropathy’ OR ‘AMSAN’) AND
[‘Child’(Mesh) OR pediatric* OR children].
Reference lists of all articles were manually
searched for cross-references and additional cases were identified
from the references of the case reports.
We reviewed 41 articles, 14 of which were included.
We have included only articles that reported original case reports
involving pediatric subjects with a form of GBS associated with
SARS-CoV-2 infection.
We excluded articles that repeated cases already
included in our reviewed, those involving subjects aged >18,
infections other than SARS-CoV-2, those written before 2020 and
those not in English.
We obtained the full text of each case we included.
Each article was selected and analysed for inclusion by two authors
in parallel.
For each case, the following data were extracted by
the two authors: Publication data: title and authors of the
article, name and year of the journal; patient information: age,
gender, underlying clinical condition, medical history and
SARS-CoV-2 exposure, signs and symptoms of GBS; and diagnostic
tests for SARS-CoV-2 infection and for GBS, treatment type and
duration, outcome.
Case description
At the end of June 2021, a 9-year-old girl presented
to the pediatric emergency department of the Chivasso Civic
Hospital for progressive weakness and gait instability over the
last month. She claimed no infectious or febrile episodes in the
last months, no COVID-19-contacts. Her family history was negative
for autoimmune or neurological disease.
General examination showed good general condition, T
36.5˚C, bilateral inferior limb weakness with gait instability,
altered sensitivity and complete absence of the patellar reflexes.
Cranial nerves examination was normal, and she showed no
difficulties in breathing and swallowing.
Lumbar puncture showed increased protein level with
normal cell count (CSF appearance: clear; pressure: normal,
glucose: 52 mg/dl; proteins 1.884 g/l, WBC: 2/mm3). CSF
isoelectric focusing was negative for intrathecal oligoclonal
immunoglobulin G synthesis (Table
I).
 | Table ICerebrospinal fluid analysis. |
Table I
Cerebrospinal fluid analysis.
| Parameter | Value |
|---|
| Chemical-physical
analysis | |
|
Appearance | Clear |
|
Pressure | Normal |
|
Glucose | 52 mg/dl (S-glucose
92 mg/dl) |
|
Total
proteins | 1.884 g/l (S-total
proteins, 7.4 g/dl; S-albumine, 4.7 g/dl) |
|
White blood
cell | 2/mm3 |
|
Isoelectric
focusing | Negative for
intrathecal oligoclonal immunoglobulin G synthesis |
| Viral and microbial
PCR searches Film array | |
|
Escherichia
coli K1 | Negative |
|
Haemophilus
influenzae | Negative |
|
Listeria
monocytogenes | Negative |
|
Neisseria
meningitidis | Negative |
|
Streptococcus
agalactiae | Negative |
|
Streptococcus
pneumoniae | Negative |
|
CMV | Negative |
|
Human
Herpesvirus 6 | Negative |
|
Human
Parechovirus | Negative |
|
Varicella
zoster virus | Negative |
|
Enterovirus | Negative |
|
Herpes
simplex virus 1 | Negative |
|
Herpes
simplex virus 2 | Negative |
|
Cryptococcus
neoformans/gattii | Negative |
| Single PCR | |
|
CMV | Negative |
|
SARS-CoV-2 | Negative |
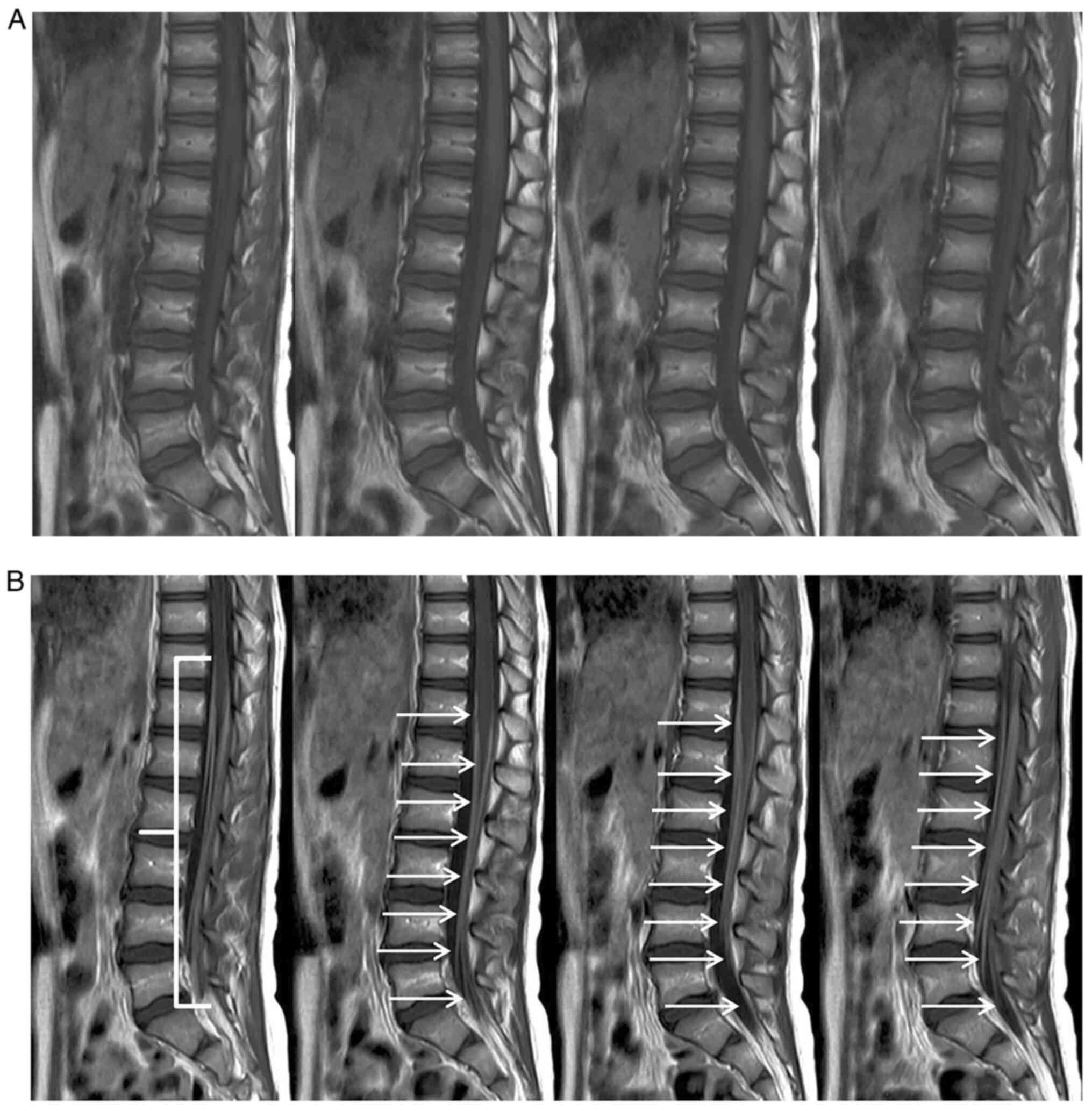
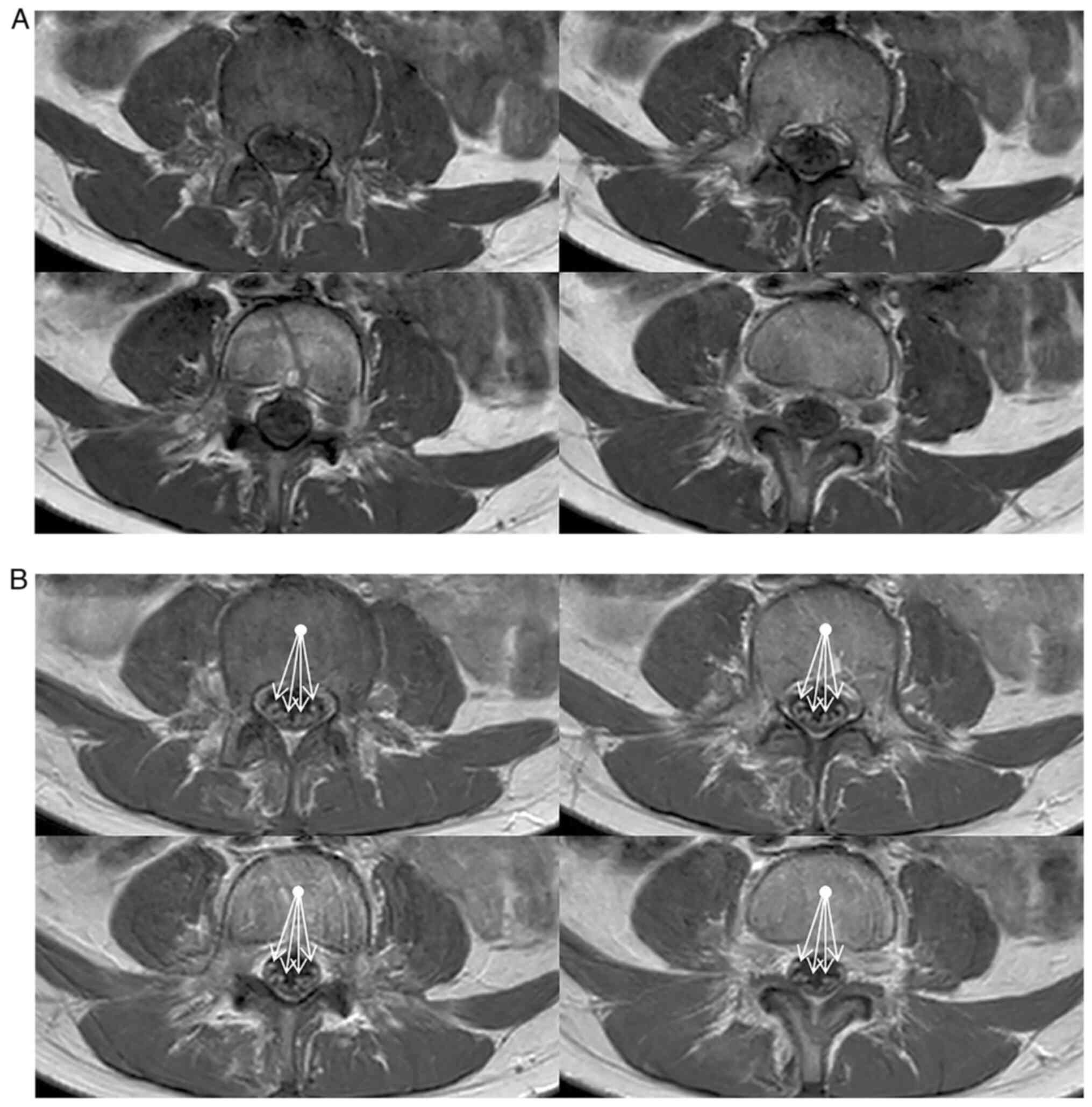
Cranial and spinal MRI (Philips Ingenia 1,5T;
Spin-echo, Turbo Spin-Echo, Inversion Recovery, Gradient Echo, Echo
Planar with T1, T2, DP weighted sequences, pre and post-contrast)
showed marked enhancement of cauda equina roots after contrast
injection, both in the sagittal (Fig.
1) and axial (Fig. 2) views,
according to the clinical hypothesis of Guillain-Barré
polyradiculonevritis.
Nerve conduction study (NCS) pattern was consistent
with acute inflammatory demyelinating polyradiculoneuropathy of
moderate/marked degree in the lower limbs and of a more modest
degree in the upper limbs.
A panel for CSF paraneoplastic and autoimmune
antibodies was negative, in particular we excluded the presence of
IgG anti-GM1 and anti-GQ1b antibodies, respectively frequently
described in AMAN and MFS.
Molecular rhino-pharyngeal swab for SARS-CoV-2 was
negative. Extensive virological and microbiological PCR searches on
CSF, including SARS-CoV-2, and Campylobacter search on stools were
negative. Epstein Barr Virus, Citomegalovirus and Borrelia serology
were negative, while COVID-19 serology was positive (45.2 AU/ml,
nv<12.0) (Table II). We did
not perform specific test for Influenza virus for the absence of
suggestive symptoms (no fever, headache, dizziness, malaise,
rhinitis nor cough) and epidemiological data to support this
suspect (https://www.epicentro.iss.it/influenza/flunews).
| Table IICSF and serum autoantibodies screening
and serologies for infectious diseases. |
Table II
CSF and serum autoantibodies screening
and serologies for infectious diseases.
| Parameter | Value |
|---|
| CSF paraneoplastic
auto-antibodies | |
|
Ab
anti-YO | Negative |
|
Ab
anti-Hu | Negative |
|
Ab
anti-GAD65 | Negative |
|
Ab
anti-CV2 | Negative |
|
Ab
anti-Ri | Negative |
|
Ab
anti-MA2 | Negative |
|
Ab
anti-recoverin | Negative |
|
Ab
anti-anfifisin | Negative |
|
Ab
anti-Tr | Negative |
|
Ab
anti-Sox1 | Negative |
|
Ab
anti-Zic4 | Negative |
|
Ab
anti-titin | Negative |
| Serum
auto-antibodies | |
|
s-Ab
anti-GD1a ganglioside (IgG and IgM) | Negative |
|
s-Ab
anti-GD1b ganglioside (IgG and IgM) | Negative |
|
s-Ab
anti-GQ1b ganglioside (IgG and IgM) | Negative |
|
s-Ab
anti-GM1 ganglioside (IgG and IgM) | Negative |
|
s-Ab
anti-GM2 ganglioside (IgG and IgM) | Negative |
|
s-Ab
anti-MAG IgG | Negative |
| Serologies for
infectious diseases | |
|
s-anti-SARS-CoV2 | |
|
Sample
1 | Positive |
|
Sample
2 | Positive |
|
Hepatitis B
Virus | Negative |
|
Hepatitis C
Virus | Negative |
|
Human
Immunodeficiency Viruses | Negative |
|
Borrelia | Negative |
|
Epstein Barr
Virus | Negative |
|
Cytomegalovirus | Negative |
The girl was initially treated with two courses of
intravenous immunoglobulins (IVIG, 2 g/kg per time, repeated after
7 days) with mild improvement of the clinical picture. She was
discharged after 15 days of hospitalization.
Two months later, shortly after summer holidays, she
experienced a mild recrudescence of gait instability and ataxia
with NCS worsening, and a third course of IVIG was
administered.
The girl is now on strict neurological follow up and
undergoes regular physiotherapy. She underwent the last
neuropsychiatric evaluation in February 2022. Motor and sensory
deficits (hypotonia and hyporeflexia) persisted mainly in the lower
limbs, despite the slight improvement. There was no evidence of
deficits in the cranial nerves. Given the slow clinical
improvement, an additional course of IV immunoglobulin will be
given over the next few weeks.
Discussion
Clinical description of the 19 pediatric cases is
detailed in Table III. Our case
is reported as the 20th.
| Table IIIPatient information, SARS-CoV-2
exposure, signs and symptoms of GBS, diagnostic tests for
SARS-CoV-2 infection and for GBS, treatment type and duration,
clinical outcome of 21 paediatric patients with GBS-associated with
SARS-CoV-2 infection. |
Table III
Patient information, SARS-CoV-2
exposure, signs and symptoms of GBS, diagnostic tests for
SARS-CoV-2 infection and for GBS, treatment type and duration,
clinical outcome of 21 paediatric patients with GBS-associated with
SARS-CoV-2 infection.
| Author and
Country | Case | Sex | Age years | Medical
history | Past SARS-CoV-2
symptoms | Presenting symptoms
and neurological onset | Sars-coV2 airways
test/serology/PCR analysis on CSF | CSF analysis | MRI | Nerve conduction
study | Specific therapy
for GBS | Outcome | Final
diagnosis | (Refs.) |
|---|
| Manji HK,
Tanzania | 1 | M | 12 | PH | Low grade fever and
cough a week earlier | - 5 days of lower
back pain, followed by acute progressive symmetric ascending
quadriparesis with bilateral facial paresis Progression to altered
level of consciousness (GCS 6/15), oxygen saturation of 88% -
Decreased strength and muscle tone: MRC score: LE 1/5, UE 2/5 -
Deep tendon reflexes absent in all four limbs | Positive/NR/NR | NR | NR | NR | 400 mg/kg of IVIG
for 5 days | - PICU admission
and mechanical ventilation - Neurological improvement after IVIG -
Death from respiratory conditions | GBS with acute
respiratory distress in a child with COVID-19 infection | (12) |
| Curtis M, USA | 1 | M | 8 | PH | None | 7 days of lower
back pain, followed by bilateral lower extremity weakness,
progression to paralysis and dyspnea (oxygen saturation of 88%) -
Upper extremity weakness - Possible left sixth nerve palsy - Muscle
strength: MRC score: UE 3/5, LE 2/5 - Deep tendon reflexes absent
in all four limbs and abnormal proprioception of the distal LE |
Positive/positive/negative |
Albumino-cytological dissociation | Abnormal
enhancement of the posterior nerve roots from the T11 level through
the cauda equina | Consistent with
AIDP | 2 g/kg of IVIG over
48 h | - PICU admission, 5
days of mechanical ventilation - Improvement after IVIG - After 6
weeks, regained bilateral dorsiflexion and plantarflexion, the
ability to sit independently, and was working on ambulating | GBS, AIDP form, in
a child with COVID-19 infection child with COVID-19 infection | (13) |
| Khalifa M, Saudi
Arabia | 1 | M | 11 | PH | Low grade fever 20
days earlier and persistent mild dry cough | - Acute onset of
unsteady gait, followed by inability to walk - Symmetrical weakness
of LE, MRC score 3/5, hypotonia No involvement of the UE - Lost
ankle and knee reflexes - Impaired proprioception of both feet up
to the mid-legs | Positive/NR/NR |
Albumino-cytological dissociation | Abnormal
enhancement of the cauda equina nerve roots | Consistent with
AIDP | 1 g/kg/day of IVIG
for 2 days | Gradual improvement
of lower limb power, balanced gait, decreased numbness and normal
proprioception after 14 days of admission | GBS, AIDP form, in
a child with COVID-19 infection | (14) |
| Mehra B, India | 1 | F | 13 | PH | Fever one month
earlier | High-grade fever,
cough, vomits, progressive body rash, evolution to shock: diagnosis
of MIS-C - After 7 days: no motor response to painful stimuli, no
spontaneous eye-opening, quadriparetic with facial weakness, poor
diaphragm excursion, seizure: diagnosis of ADEM, and GBS |
Negative/positive/NR | Not performed | Consistent with
ADEM | Consistent with
AIDP | 1 g/kg IVIG
repeated after 7 days + 5 cycles of plasmapheresis 7 days + 5
cycles of plasmapheresis | - PICU admission
and 2 weeks of ventilation - Complete neurological recovery and
discharged home after 6 weeks of hospitalization | MIS-C complicated
with ADEM and GBS, AIDP form, in post Covid-19 infection | (15) |
| Khera D, India | 1 | F | 11 | PH | History of fever
without any other viral prodrome | - Acute onset of
severe flaccid paralysis with respiratory failure on day 3, bowel
and bladder incontinence - Hypotonia in all four limbs, bilateral
MRC score: UE 4/5, LE 0/5 - No bowel and bladder sensation -
Reflexes absent in ankle, knee and other superficial reflexes |
Negative/positive/NR |
Albumino-cytological dissociation | Acute lesion in
brain along with cauda equina nerve roots enhancement, consistent
with GBS + LETM | AMAN | IVIG (dosage not
available) + 5 cycles of plasmapheresis | - PICU admission
and mechanical ventilation - After 6 weeks she walks independently
with good bowel and bladder control and no neurological
deficit | LETM and GBS, AMAN
form, in post Covid-19 infection | (16) |
| El mezzeoui S,
Morocco | 1 | F | 3 | PH | Mild respiratory
symptoms 2 weeks earlier | - Progressive
symmetric and ascending quadriparesis - MRC score: UE4/5, LE 2/5 -
Deep tendon reflexes absents - Decrease in sensitivity, swallowing
inability | NR/positive/NR |
Albumino-cytological dissociation | Negative | NR | 0.5 g/kg/day IVIG
for 5 days | Clinical
improvement, discharged after one month | GBS in post
Covid-19 infection | (17) |
| Araújo NM,
Brasil | 1 | F | 17 | PH | Fever, abdominal
pain, nausea and severe diarrhea 8 days earlier | - 2 days of severe
low back followed by symmetrical flaccid tetraparesis, worse in the
LE - Mild distal hypoparesthesia in the LE - Areflexia of patellar
and Achilles tendons and hyporeflexia in the UE |
Positive/NR/Positive |
Albumino-cytological dissociation | Abnormal
enhancement of cervical and cauda equina nerve roots | Consistent with
AIDP | 2 g/kg IVIG | Clinical
improvement | SARS-CoV-2
detection in cerebrospinal fluid in a child with GBS, AIDP
form | (18) |
| Das KY, India | 1 | M | 7 | PH | None | 8 days of
bilateral, symmetrical LE weakness and paresthesia - Areflexia,
poor gag reflex, low respiratory rate requiring mechanical
ventilation |
Negative/positive/NR |
Albumino-cytological dissociation | NR | Suggestive of the
inexcitable variant of GBS (AMAN) | IVIG, doses not
reported | - PICU admission,
mechanical ventilation - Extubated after 3 days - Clinical
improvement | GBS (inexcitable
variant, AMAN) in post Covid-19 infection | (19) |
| Frank CHM,
Brazil | 1 | M | 15 | PH | Frontal headaches,
fever and sweating 2 weeks earlier | Emetic episodes,
weakness and pain in the LE, progression to the UE - Progressive
symmetrical limb weakness (MRC score: UE 3/5, LE 2/5) - Absent deep
tendon reflexes |
Positive/positive/negative | Negative | Negative | Compatible with the
AMAN variant of GBS. | 400 mg/kg/day of
IVIG for 5 days | - Clinical
improvement, persistent weakness in the upper and LE. | GBS, AMAN form, in
a child with COVID-19 infection | (20) |
| Paybast S,
Iran | 1 | F | 14 | PH | Upper respiratory
tract infection 3 weeks earlier | 2 days of
progressive ascending quadripareshtesia with LE weakness, headaches
and dizziness - MRC score: LE 4/5, affecting both the distal and
proximal muscles - Deep tendon reflexes hypoactive in UE and absent
in LE - Decreased light touch, position, and vibration sensation in
all distal limbs up to ankle and elbow joints. Ataxic with closed
eyes - Father with the same symptoms | Positive/NR/NR |
Albumino-cytological dissociation | NR | Not performed | 20 g/die IVIG for 5
days | - Complete recovery
of the symptoms except for generalized hyporeflexia and decreased
light touch sensation in distal limbs | Familial occurrence
of Guillain-Barré syndrome in a child with COVID-19 infection | (21) |
| Al Haboob AA, Saudi
Arabia | 1 | M | 11 | PH | 3 weeks of
vomiting, abdominal pain, mild diarrhea and mild headache | - Lethargic,
tachypnic, fatigued, drowny, no fever, bilateral sixth nerve palsy
and double vision on his lateral gaze: Miller-fisher variant of GBS
Treated with IVIG; on 2nd day PRES. | Positive/NR/NR |
Albumino-cytological dissociation | Consistent with
PRES | Abnormal | 0.4 g/kg/day IVIG
for 5 days | PICU admission and
intubation. Discharged to go home with normal level of
consciousness, cranial nerve palsy, normal muscle tone, grade 4
motor power, normal gag and cough reflexes | GBS, Miller Fischer
variant, with PRES in association with COVID-19 infection | (22) |
| Akçay N,
Turkey | 1 | M | 6 | PH | 2 days of
fever | - Symmetric
ascending paralysis progressed over a 4 day course - Bilateral LE
and UE flaccid weakness of 1/5 with absent deep tendon reflexes -
Severe respiratory muscle weakness requiring invasive mechanical
ventilation | Positive/NR/NR |
Albumino-cytological dissociation | Contrast
enhancement of cauda equina and nerve roots | Suggestive of
AMAN | 10 cycles of
plasma-pheresis, followed by methyl-prednisolone (30 mg/kg/day for
5 days) and IVIG (2 g/kg/day, repeated after 14 days) | - PICU admission
and intubation - On Day 60, discharged from the hospital with
weakness (MRC score 2/5) in UE and LE -Discharged with home
ventilation - His reflexes remained absent. | Axonal GBS (AMAN
form) associated with SARS-CoV-2 infection | (23) |
| LaRovere KL,
USA | 1 | NR | 6-12 | PH | Within 1 month
following SARS-CoV-2 exposure | - Classic
neurological signs and symptoms of GBS |
Negative/Positive/NR | NR | NR | Classic
electro-physiologic features of GBS, AIDP form; one with AMAN
form | NR | New deficits,
required outpatient physical therapy | Guillain-Barré
syndrome, 3 AIDP and 1 AMAN form | (24) |
| | 2 | NR | 6-12 | PH | | |
Positive/Positive/NR | NR | NR | | NR | required outpatient
physical therapy. | New deficits, | |
| | 3 | NR | 13-17 | PH | | |
Negative/Positive/NR | NR | NR | | NR | New deficits,
required outpatient physical therapy | | |
| | 4 | NR | 13-17 | Underlying
neuro-logical disorder | | |
Positive/Positive/NR | NR | NR | | NR | Discharged
home | | |
| Sánchez-Morales AE,
Mexico | 1 | M | 9 | GBS at age of
6 | NR | - Pain in LE,
ascendant weakness, hypotonia, diminished tendon reflexes |
Negative/positive/NR |
Albumino-cytological dissociation | NR | AIDP | NR | The patients
recovered the ability to walk and run independently | Recurrent case of
GBS, AIDP form, probable relationship with SARS-Cov2 | (25) |
| | 2 | M | 14 | | Fever,
rhinorrhea | - Paresthesia in
feet, ascendant weakness, hypotonia, diminished tendon reflexes in
LE | NR/positive/NR |
Albumino-cytological dissociation | NR | AIDP | NR | The patients
recovered the ability to walk and run independently | GBS, AIDP form,
possible relationship with SARS-Cov2 | |
| | 3 | F | 12 | GBS 4 months
earlier | NR | - Dysphonia,
hypotonia, ascendant weakness, diminished tendon reflexes in UE,
absent in LE | NR/positive/NR |
Albumino-cytological dissociation | NR | AIDP | NR | The patients
recovered the ability to walk and run independently | Recurrent case of
GBS, AIDP form, possible relationship with SARS-Cov2 | |
| Mussinatto I,
Italy | 1 | F | 9 | | None | - 3 weeks of
progressive ascending weakness with gait instability - Deep tendon
reflexes absent in LE |
Negative/Positive/Negative |
Albumino-cytological dissociation | Abnormal
enhancement of the cauda equina nerve roots | Consistent with
AIDP | 1 g/kg IVIG over 24
h, repeated after 7 days and after 2 months | Clinical
improvement | GBS, AIDP, in post
Covid-19 infection | Current study |
The GBS reported cases (12-25)
come from Africa (Morocco, Tanzania), Asia (Saudi Arabia, India,
Iran), South America (Brasil), North America (USA). The case we
describe is the first from Europe.
Past history showed a recent (1 week to 1 month
before the onset of neurological symptoms) infection suggestive for
COVID-19, or a proven exposure to SARS-CoV-2, in 16/20 children. 17
children were tested for SARS-CoV-2 (antigenic or molecular swab)
on admission, 9/17 were positive. Serology for SARS-CoV-2 was
performed in 14/20 children, resulting positive in all cases. CSF
PCR for SARS-CoV-2 was performed only in 4 cases, resulting
positive in one child.
In our case, we found no history of respiratory or
intestinal symptoms in the previous months. Other two children out
of the reported cases were completely asymptomatic for COVID-19,
had a negative SARS-CoV-2 swab on admission but were proven to have
met the virus by serology (at that time, no vaccine against
COVID-19 had been approved for pediatric age).
This finding is in line with COVID-19 presentation
at pediatric age, often with an asymptomatic course (4).
Our patient did not receive recent vaccinations; she
showed negativity of the common infectious researches on CSF and
serum. In particular, Epstein Barr Virus, Citomegalovirus and
Borrelia serology were negative, as well as Campylobacter search on
stools.
We did not perform specific test for Influenza
virus, because the girl had no suggestive symptoms (no fever,
headache, dizziness, malaise, rhinitis nor cough) in the previous
months. Moreover, during winter 2020-2021, virtually no cases of
Influenza were reported in our region, perhaps thanks to the
prevention measures taken during the COVID pandemic (https://www.epicentro.iss.it/influenza/flunews).
In our girl, the only positive infective result was
the presence of SARS-CoV-2 antibodies in serum.
At the time of her hospital admission, in Italy,
400,000-700,000 total children aged 0-12 years have experienced
COVID-19 since the beginning of the current pandemic, and no
COVID-19 vaccine had been licensed for pediatric age. The
positivity of our patient's SARS-Cov2 serology test in such
epidemiological frame prompts us to consider an asymptomatic
COVID-19 infection as a possible trigger of GBS.
Regarding the diagnostic challenge, GBS remains a
clinical diagnosis that can be sustained by laboratory and
instrumental tests.
CSF analysis was reported in 14/20 children of the
reported series, showing the classical pattern of albumin-cytologic
dissociation in 13/14. CSF was normal in one case.
In our case, the CSF examination showed the typical
increase of total proteins without cellular reaction. We excluded,
by the GanglioCombiTM ELISA kit, the presence of anti-ganglioside
antibodies, frequently described in AMAN (IgG anti-GM1 antibodies)
and MFS (anti-GQ1b antibodies) (26). The panel for CSF paraneoplastic
syndromes (EUROLINE paraneoplastic neurological syndromes 12 Ag)
was negative too.
Central nervous system MRI was reported in 10/20
children, with different results: abnormal enhancement of the cauda
equina nerve roots was the most common finding (6/10), 2/10 were
negative, one case was compatible with acute disseminated
encephalomyelitis (ADEM), one case with posterior reversible
encephalopathy syndrome (PRES) and one with longitudinally
extensive transverse myelitis associated.
Spinal MRI of our girl showed marked enhancement of
cauda equina roots (Figs. 1 and
2).
NCS was performed in 17/20 children, showing
alterations consistent with demyelinating polyneuropathy in all
cases. In 6 of these children, the NCS pattern was compatible with
the acute motor axonal form of GBS (AMAN). One case presented the
rare Miller Fisher variant of GBS. In our case, NCS pattern was
consistent with AIDP.
From 2020, several reports (2-6)
have described the possible causal association between SARS-CoV-2
infection and GBS. A recent systematic review has reported 99 cases
of GBS with confirmed COVID-19 infection, with an average age of
56.07 years (7).
A study in Northern Italy has suggested an increased
incidence of GBS during the pandemic period (from
0.077/100,000/month to 0.202/100,000/month) (27). In contrast, other studies have
reported a reduction in GBS incidence during the pandemic period,
probably due to the influence of lockdown measures on conventional
GBS-inducing pathogens (28).
A clear relationship between specific autoantibodies
and the occurrence of GBS in patients with SARS-CoV-2 infection,
such as that observed in GBS associated with Campylobacter
jejuni, has not yet been shown (28).
The common absence of SARS-CoV-2 in cerebrospinal
fluid reinforces the hypothesis of a post-infectious
immune-mediated mechanism, rather than a para-infectious etiology
(3). However, in one of the cases
reviewed here, SARS-CoV-2 PCR was positive on CSF, indicating a
possible direct action of the virus in the SNC system.
GBS associated with SARS-CoV-2 infections have shown
a distribution of clinical variants and electrophysiological
subtypes resembling those of classic GBS, with a higher prevalence
of the classic sensorimotor form and the acute inflammatory
demyelinating polyneuropathy, although rare variants such as Miller
Fisher syndrome have also been reported (4).
Progressive symmetrical muscle weakness starting
from lower limbs and marked reduction of deep tendon reflexes
remain the hallmark of this syndrome, as reported in the totality
of cases. In 3 cases, lower back pain preceded the onset of muscle
weakness by a few days.
Altered sensitivity was expressly reported in 9/20
cases, described as altered proprioception, decreased perception of
light touch, position, and vibration, paresthesia or bowel and
bladder dysfunction.
A more severe course requiring mechanical
ventilation was reported in 7 children. Involvement of the cranial
nerves was described in 4 cases, all of which required mechanical
ventilation.
The therapy of GBS is focused on supportive
treatment. Treatment with IVIG is recommended in children and
adolescents with severe GBS (9)
and should preferably begin as soon as possible after diagnosis,
within 4 weeks of the onset of symptoms, since early treatment
positively affects prognosis (29).
Among the 19 pediatric cases described in Table III, the therapeutic management
required pediatric intensive care unit admission for 7 children in
the first phase of the disease.
All cases in which treatment was detailed (13/20)
were treated with IVIG with different schedules (mainly 400 mg/kg
for 5 days or 1 g/kg for 2 days). Three children required some
sessions of plasma-exchange therapy.
The overall long-term prognosis for children with
GBS is more favorable than that in adults, whereby the majority of
children largely regain motor function. The AMAN variant has a more
acute and severe course than AIDP, with a higher rate of ventilated
patients and delayed recovery. Nonetheless, it has been repeatedly
shown that the long-term prognosis for both variants is equally
favorable in children (9). The
SARS-CoV-2 associated form had a good prognosis in more than 70% of
patients, especially after treatment with intravenous
immunoglobulins (4): 19/20
children of the reported series were dismissed from the hospital
with varying degrees of motor improvement. One child died from
respiratory complications. In one case, a familial recurrence of
GBS (father of the young girl) was reported.
In conclusion, the SARS-CoV-2 infection is proving
capable of extremely varied clinical pictures at pediatric age,
especially concerning neurological complications. Interestingly, a
substantial similarity has been observed in clinical and laboratory
presentation of COVID-19-associated GBS compared to the clinical
pictures described before the characterization of this novel
virus.
In the absence of universally accepted diagnostic
criteria, the cases we reviewed and the one described above were
attributed to COVID-19 because of the finding of a positive swab
test on admission or a positive serology and the exclusion of other
possible diagnoses, such as infections, autoimmune diseases (in
particular with the exclusion of anti-ganglioside antibodies,
frequently described in AMAN and MFS) and malignancies
(paraneoplastic syndromes).
We suggest our findings need further research for
confirmation, and the clinical suspicion of a possible association
with SARS-CoV-2 infection must remain high to allow a greater
understanding of the disease, its prevention and therapy at
pediatric age.
Acknowledgements
We thank the following individuals for their help in
the diagnostic research: Dr Andrea Piceghello (Laboratory of
Microbiology and Virology, Amedeo di Savoia Hospital, ASL Città di
Torino, Turin, Italy); Dr Francesca Rumbolo (Clinical Biochemistry
Laboratory, Department of Laboratory Medicine, Città della Salute e
della Scienza Hospital, Turin, Italy); and Dr Nicolò Li Vigni
(Laboratory of Microbiology and Virology, Ivrea Hospital, ASL To 4,
Ivrea, Italy).
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
All authors substantially contributed to the present
work, both in the clinical setting and in the elaboration of the
present article. MI, MB, EG and FT were involved in the diagnosis
of the patient through the acquisition, analysis and interpretation
of data. IM, CB, MMC, AC, MI, MB and FT were involved in diagnosis
and clinical management of the patient. IM and CB acquired,
analyzed and interpreted the literature data. IM, CB and FST wrote
and edited the manuscript. FT supervised the study. FT and IM
confirm the authenticity of all data. All authors have read and
approved the final manuscript, and agree to be accountable for all
aspects of the work.
Ethics approval and consent to
participate
The publication of the case report has been approved
by the local ethics committee AOU San Luigi Gonzaga AA SS LL
TO3-TO4-TO5 (approval no. 722; 17/01/2022).
Patient consent for publication
Written informed consent to publication has been
obtained from the parents on behalf of the patient.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
Dr Fabio Timeus, ORCID 0000-0003-0095-283X.
References
|
1
|
World Health Organization (WHO): WHO
COVID-19 Dashboard. WHO, Geneva, 2020. https://covid19.who.int/. Accessed January 5,
2022.
|
|
2
|
Vakili K, Fathi M, Hajiesmaeili M, Salari
M, Saluja D, Tafakhori A, Sayehmiri F and Rezaei-Tavirani M:
Neurological symptoms, comorbidities, and complications of
COVID-19: A literature review and meta-analysis of observational
studies. Eur Neurol. 84:307–324. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Hasan I, Saif-Ur-Rahman KM, Hayat S, Papri
N, Jahan I, Azam R, Ara G and Islam Z: Guillain-Barré syndrome
associated with SARS-CoV-2 infection: A systematic review and
individual participant data meta-analysis. J Peripher Nerv Syst.
25:335–343. 2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Abu-Rumeileh S, Abdelhak A, Foschi M,
Tumani H and Otto M: Guillain-Barré syndrome spectrum associated
with COVID-19: An up-to-date systematic review of 73 cases. J
Neurol. 268:1133–1170. 2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Uncini A, Vallat JM and Jacobs BC:
Guillain-Barré syndrome in SARS-CoV-2 infection: An instant
systematic review of the first six months of pandemic. J Neurol
Neurosurg Psychiatry. 91:1105–1110. 2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Toscano G, Palmerini F, Ravaglia S, Ruiz
L, Invernizzi P, Cuzzoni G, Franciotta D, Baldanti F, Daturi R,
Postorino P, et al: Guillain-Barré syndrome associated with
SARS-CoV-2. N Engl J Med. 382:2574–2576. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Aladawi M, Elfil M, Abu-Esheh B, Abu Jazar
D, Armouti A, Bayoumi A and Piccione E: Guillain barre syndrome as
a complication of COVID-19: A systematic review. Can J Neurol Sci.
49:38–48. 2022.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Leonhard SE, Mandarakas MR, Gondim FAAA,
Bateman K, Ferreira MLB, Cornblath DR, Van Doorn PA, Dourado ME,
Hughes RAC, Islam B, et al: Diagnosis and management of
Guillain-Barré syndrome in ten steps. Nat Rev Neurol. 15:671–683.
2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Korinthenberg R, Trollmann R,
Felderhoff-Müser U, Bernert G, Hackenberg A, Hufnagel M, Pohl M,
Hahn G, Mentzel HJ, Sommer C, et al: Diagnosis and treatment of
Guillain-Barré syndrome in childhood and adolescence: An evidence-
and consensus-based guideline. Eur J Paediatr Neurol. 25:5–16.
2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Flanagan EP, McKeon A, Lennon VA, Kearns
J, Weinshenker BG, Krecke KN, Matiello M, Keegan BM, Mokri B,
Aksamit AJ and Pittock SJ: Paraneoplastic isolated myelopathy:
Clinical course and neuroimaging clues. Neurology. 76:2089–2095.
2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
McMillan HJ, Kang PB, Jones HR and Darras
BT: Childhood chronic inflammatory demyelinating
polyradiculoneuropathy: Combined analysis of a large cohort and
eleven published series. Neuromuscul Disord. 23:103–111.
2013.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Manji HK, George U, Mkopi NP and Manji KP:
Guillain-Barré syndrome associated with COVID-19 infection. Pan Afr
Med J. 35 (Suppl 2)(S118)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Curtis M, Bhumbra S, Felker MV, Jordan BL,
Kim J, Weber M and Friedman ML: Guillain-Barré syndrome in a child
with COVID-19 infection. Pediatrics.
147(e2020015115)2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Khalifa M, Zakaria F, Ragab Y, Saad A,
Bamaga A, Emad Y and Rasker JJ: Guillain-Barré syndrome associated
with severe acute respiratory syndrome coronavirus 2 detection and
coronavirus disease 2019 in a child. J Pediatric Infect Dis Soc.
9:510–513. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Mehra B, Aggarwal V, Kumar P, Kundal M,
Gupta D, Kumar A and Dugaya SK: COVID-19-associated severe
multisystem inflammatory syndrome in children with encephalopathy
and neuropathy in an adolescent girl with the successful outcome:
An unusual presentation. Indian J Crit Care Med. 24:1276–1278.
2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Khera D, Didel S, Panda S, Tiwari S and
Singh K: Concurrent longitudinally extensive transverse myelitis
and Guillain-Barré syndrome in a child secondary to COVID-19
infection: A severe neuroimmunologic complication of COVID-19.
Pediatr Infect Dis J. 40:e236–e239. 2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
El Mezzeoui S, Aftiss FZ, Aabdi M, Bkiyar
H and Housni B: Guillan barre syndrome in post Covid-19 infection
in children. Ann Med Surg (Lond). 67(102524)2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Araújo NM, Ferreira LC, Dantas DP, Silva
DS, Dos Santos CA, Cipolotti R and Martins-Filho PR: First report
of SARS-CoV-2 detection in cerebrospinal fluid in a child with
Guillain-Barré syndrome. Pediatr Infect Dis J. 40:e274–e276.
2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Das KY, Midhun Raj KT, Samprathi M,
Sridhar M, Adiga R and Vemgal P: Guillain-Barré syndrome associated
with SARS-CoV-2 infection. Indian J Pediatr. 88(479)2021.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Frank CHM, Almeida TVR, Marques EA, de
Sousa Monteiro Q, Silveira Feitoza PVS, Borba MGS, Vasconcelos HL,
de Souza Bastos M and Lacerda MVG: Guillain-Barré syndrome
associated with SARS-CoV-2 infection in a pediatric patient. J Trop
Pediatr. 67(fmaa044)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Paybast S, Gorji R and Mavandadi S:
Guillain-Barré syndrome as a neurological complication of novel
COVID-19 infection: A case report and review of the literature.
Neurologist. 25:101–103. 2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Al Haboob AA: Miller Fischer and posterior
reversible encephalopathy syndromes post COVID-19 infection.
Neurosciences (Riyadh). 26:295–299. 2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Akçay N, Menentoğlu ME, Bektaş G and
Şevketoğlu E: Axonal Guillain-Barre syndrome associated with
SARS-CoV-2 infection in a child. J Med Virol. 93:5599–5602.
2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
LaRovere KL, Riggs BJ, Poussaint TY, Young
CC, Newhams MM, Maamari M, Walker TC, Singh AR, Dapul H, Hobbs CV,
et al: Neurologic involvement in children and adolescents
hospitalized in the United States for COVID-19 or multisystem
inflammatory syndrome. JAMA Neurol. 78:536–547. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Sánchez-Morales AE, Urrutia-Osorio M,
Camacho-Mendoza E, Rosales-Pedraza G, Dávila-Maldonado L,
González-Duarte A, Herrera-Mora P and Ruiz-García M: Neurological
manifestations temporally associated with SARS-CoV-2 infection in
pediatric patients in Mexico. Childs Nerv Syst. 37:2305–2312.
2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Willison HJ: The immunobiology of
Guillain-Barré syndromes. J Peripher Nerv Syst. 10:94–112.
2005.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Filosto M, Cotti Piccinelli S, Gazzina S,
Foresti C, Frigeni B, Servalli MC, Sessa M, Cosentino M, Marchioni
G, Ravaglia E, et al: Guillain-Barré syndrome and COVID-19: An
observational multicentre study from two Italian hotspot regions. J
Neurol Neurosurg Psychiatry. 92:751–756. 2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Koike H and Katsuno M: Emerging infectious
diseases, vaccines and Guillain-Barré syndrome. Clin Exp
Neuroimmunol: May 17, 2021 (Epub ahead of print).
|
|
29
|
Hughes RA, Swan AV and van Doorn PA:
Intravenous immunoglobulin for Guillain-Barré syndrome. Cochrane
Database Syst Rev. 9(CD0020639)2014.PubMed/NCBI View Article : Google Scholar
|