Introduction
Totally implantable venous access port (TIVAP) is a
closed intravenous infusion device that may be implanted under the
skin and retained in the body for a long duration (1,2). It
mainly comprises an injection seat for puncture and an intravenous
catheter system and may be used for infusion, rehydration,
nutritional support and blood transfusion of various chemotherapy
drugs (3,4). Compared with peripherally placed
central venous catheter (PICC) and central venous catheter, TIVAP
has obvious advantages in terms of safety, infection rate and
patient satisfaction (5,6). It is widely used in clinical
applications, is superior to other long-term central venous
catheters and is the best choice for cancer patients (7-9).
At present, TIVAP is mainly implanted through the subclavian vein,
internal jugular vein and upper arm vein. Compared with the
subclavian vein and internal jugular vein, TIVAP implanted in the
upper arm has the advantages of a higher puncture success rate and
a lower risk of haemopneumothorax (10). Arm ports are more cosmetically
appealing (11) and are more
popular with female patients.
TIVAP in the upper arm is an operation performed by
nurses and completed with the cooperation of doctors, which has
been gradually popularized and applied in patients with malignant
tumours in recent years. Accurate positioning of the catheter tip
is one of the most critical technical steps in central venous
catheter insertion. Traditionally, the reserved length of the
catheter is measured by the surface measurement method and the
length of the catheter is adjusted according to the placement of
the catheter tip under digital subtraction angiography (DSA)
guidance (12). This method
frequently has a large deviation and increases the X-ray exposure
of clinicians and patients.
In recent years, the intracavitary ECG-guided tip
positioning technique has been widely used in PICC tip placement,
and research has confirmed the stability and accuracy of this
technology (13,14). However, only a small number of
studies have reported on the application of intracavitary
ECG-guided tip positioning techniques of TIVAP in the upper arm. In
the present study, an intracavitary ECG positioning technique
guided by a trocar needle was used to insert the tip of the
catheter of the TIVAP in the upper arm of patients with malignant
tumours. It was determined that this technique is a safe and
effective method for catheter tip placement and has high prospects
for clinical application.
Materials and methods
Patients and study design
The present study was a retrospective study
according to the Strengthening the Reporting of Observational
Studies in Epidemiology guidelines (15). This study was approved by the
Ethics Committee of The Affiliated Suzhou Hospital of Nanjing
Medical University (Suzhou, China; no. KL171072). Clinical data
were acquired from medical records (mainly surgical and nursing
records). The inclusion criteria were as follows: i) Cancer
patients who received a TIVAP in the upper arm in our department;
and ii) ECG displaying a sinus rhythm with a normal P wave.
Furthermore, the following exclusion criteria were applied: i)
Patients with severe primary diseases, such as those of the heart,
liver, kidney and haematopoietic systems; ii) previous upper limb
oedemaedema; iii) dysfunction of blood coagulation; and iv)
patients with alcoholism and drug addictions. Finally, a total of
255 adult inpatients who required TIVIP in the upper arm between
March 2017 and July 2020 at the Affiliated Suzhou Hospital of
Nanjing Medical University (Suzhou, China) were included. There
were no significant differences between the two groups in terms of
age, sex, body height, body weight, smoking or venipuncture site
(Table I). In the present
retrospective study, all cancer patients who received a TIVAP in
the upper arm at our department using ECG guidance were compared
with those in whom the traditional surface measurement method was
applied.
 | Table IClinical characteristics of
patients. |
Table I
Clinical characteristics of
patients.
| Item | Overall (n=255) | Surface measurement
group (n=117) | ECG-guided group
(n=138) | P-value |
|---|
| Age, years | 54.91±14.29 | 53.42±13.68 | 56.19±16.44 | NS |
| Males/females | 127/128 | 56/61 | 71/67 | NS |
| Body height, cm | 165.16±15.18 | 164.72±9.68 | 165.54±13.26 | NS |
| Body weight, kg | 60.58±10.43 | 59.77±11.37 | 61.27±9.87 | NS |
| Smoker | 73 | 35 | 38 | NS |
| Venipuncture
site | | | | |
|
Basilic vein
left | 22 | 10 | 12 | NS |
|
Basilic vein
right | 143 | 78 | 65 | NS |
|
Brachial
vein left | 24 | 10 | 14 | NS |
|
Brachial
vein right | 66 | 32 | 34 | NS |
Procedure
All patients were implanted an Infusion Port, Model
5 Fr (B. Braun). The procedure for intracavitary ECG-guided tip
positioning used in the first cohort was as follows (16,17):
A three-electrode ECG monitoring mode was used to connect the ECG
monitor (Philips Medical Systems B.V.) and the ECG monitor was
adjusted to lead II to record the basic ECG on the patient's body
surface. After skin disinfection and local anaesthesia, puncture
was performed through the basilic vein or brachial vein under the
guidance of ultrasound (Volcano). Subsequently, the sheath was
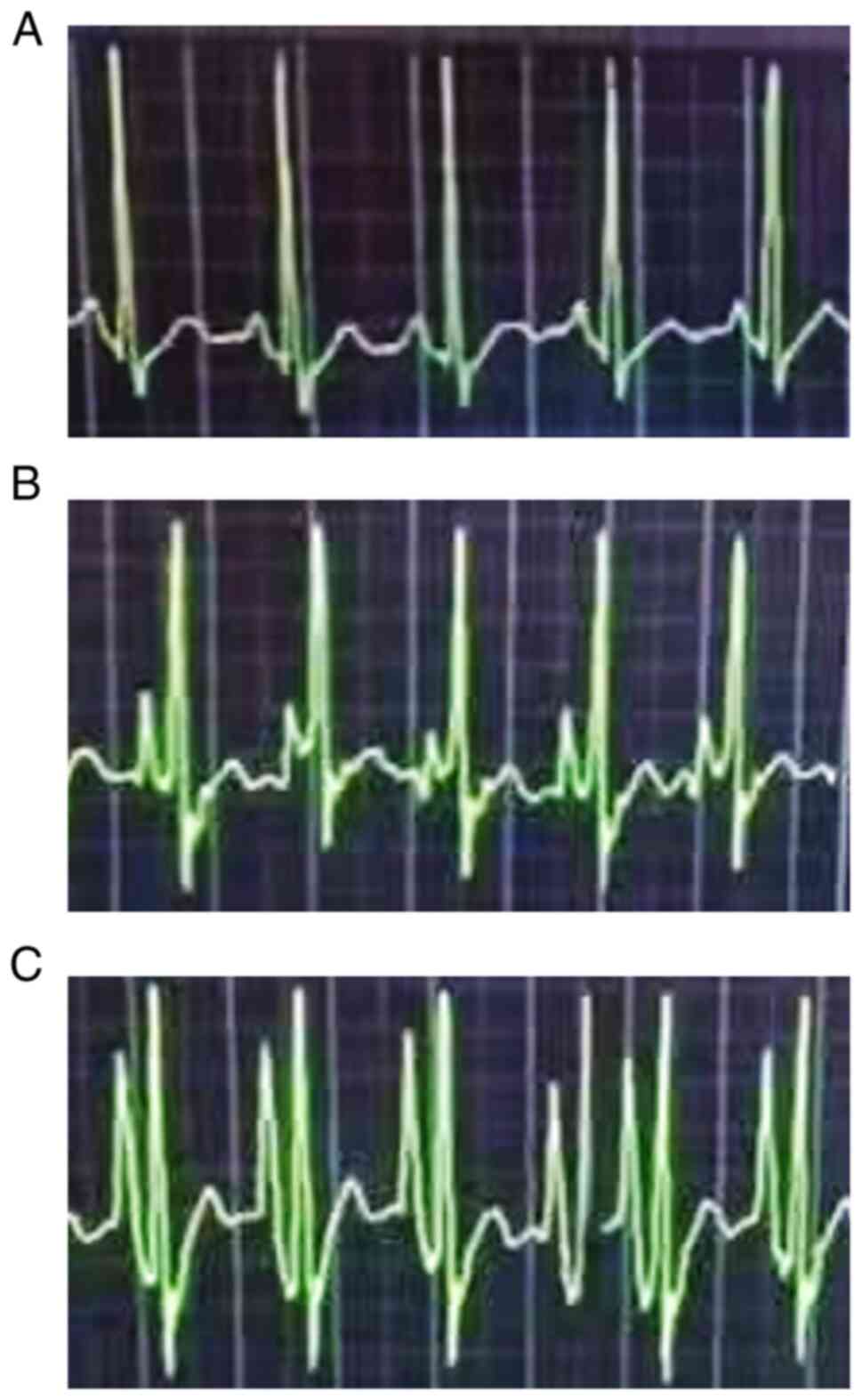
inserted using the Seldinger technique. When the catheter was
inserted 5 cm, the delivery of the catheter was stopped and the
intracavitary ECG connection was made through a trocar needle. With
the catheter tip entering the superior vena cava, the P wave of the
ECG exhibited characteristic changes (Fig. 1). When the P wave fell back after
reaching the peak or a bidirectional P wave appeared, the catheter
was judged to have entered the right atrium (18,19).
At this time, when the catheter was stopped and retreated to
achieve the horizontal position of the highest peak of the positive
P wave (exited for 20 mm), the catheter was fixed and the catheter
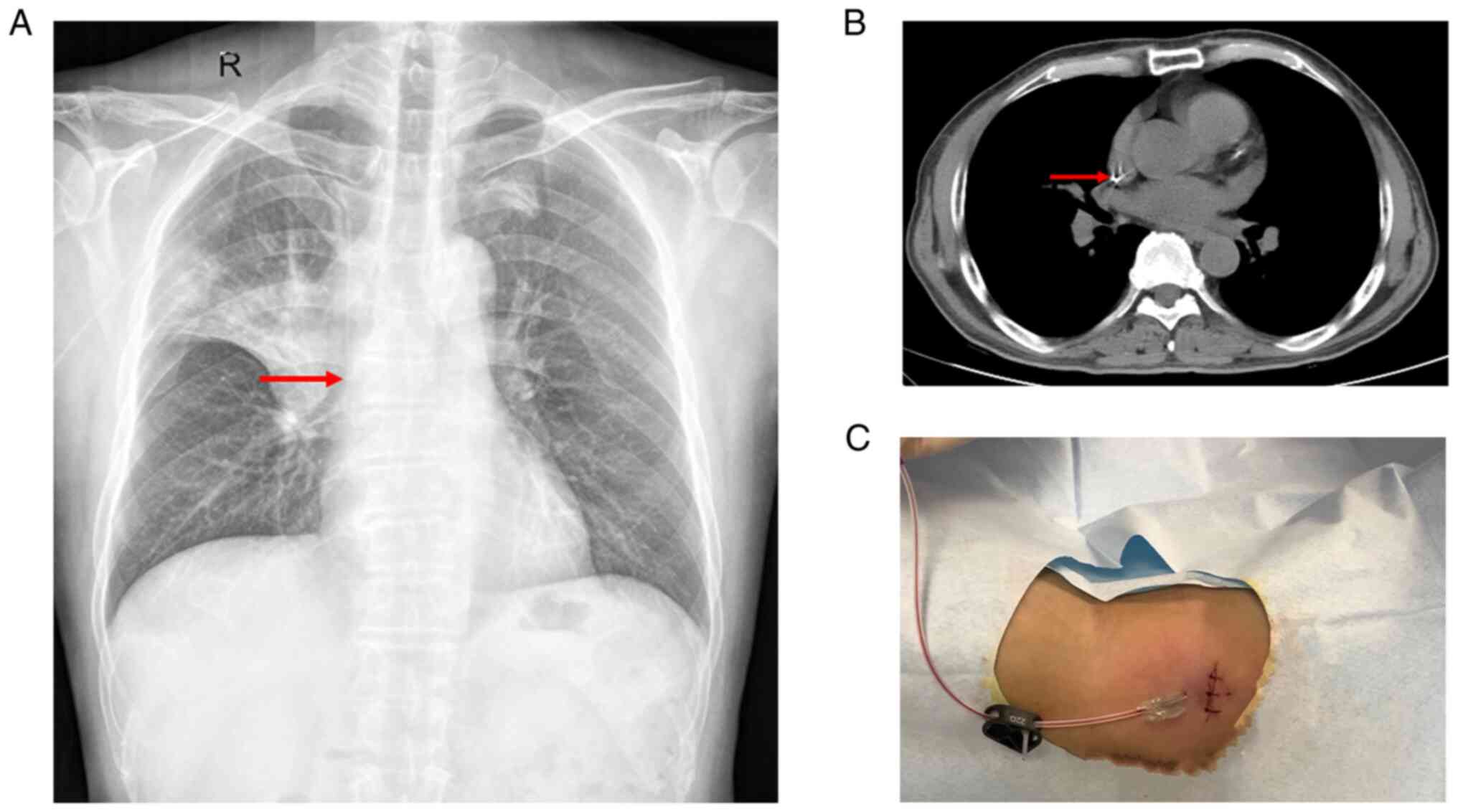
scale was recorded. The catheter position was confirmed by X-ray
(Fig. 2A and B). Finally, a doctor set up a
subcutaneous tunnel under the puncture point, cut the skin ~2 cm
horizontally, made a pouch, connected the catheter with the
injection seat and wrapped it with a sterile dressing after suture
(Fig. 2C).
In the second cohort, the traditional surface
measurement method was used for catheter tip positioning. First,
the distance was measured from the puncture point to the right
sternoclavicular joint and then down to the third rib. The
insertion technique was similar to the above. Subsequently, the
catheter was inserted with the predicted length. The length of the
catheter was adjusted according to the position of the catheter tip
under the visual guidance of DSA (Siemens AG). The next steps were
the same as those for intracavitary ECG-guided tip positioning.
Outcomes
The number of cases in whom the correct position of
the catheter tip and the best position were achieved on first
attempt, as well as the operation time, were compared between the
two groups. When the catheter tip was located in the superior vena
cava (SVC) and caval-atrial junction, it was judged as the correct
position of the catheter tip and the catheter tip located in the
lower third of the SVC was judged as the best position. Early
complications within 14 days after placement, including phlebitis,
venous thrombosis and arrhythmia, were compared between the two
groups.
Statistical analysis
Statistical analysis was performed using the SPSS 20
software package (IBM Corporation). Where appropriate, Student's
t-test and the χ2 test were used to examine the
significance of the results. P<0.05 was considered to indicate a
statistically significant difference.
Results
Success of catheter positioning and
operation time
The correct positioning rate and the rate of
achieving the best position of the catheter tip at the first
attempt were higher in the ECG-guided group than in the traditional
surface measurement method group (Table II). The mean operation time was
significantly shorter in the ECG-guided group than in the surface
measurement group (46.28 vs. 63.26 min; P=0.0226; Table II).
| Table IIComparison of correct placement and
best position of catheter tip and operation time. |
Table II
Comparison of correct placement and
best position of catheter tip and operation time.
| Item | Overall (n=255) | Surface measurement
group (n=117) | ECG-guided group
(n=138) | P-value |
|---|
| Correct placement of
catheter tip | 229 (89.80) | 97 (82.91) | 132 (95.65) | 0.0018 |
| Best position | 205 (80.39) | 80 (68.38) | 125 (90.58) | <0.0001 |
| Operation time,
min | 54.07±9.77 | 63.26±8.76 | 46.28±9.76 | 0.0226 |
Complications
Complications were phlebitis, venous thrombosis and
arrhythmia. The incidence of complications in the ECG-guided group
was 6.52% (9/138), while that in the surface measurement group was
10.26% (12/117) (Table III).
| Table IIIDetails regarding complications. |
Table III
Details regarding complications.
| Complication | Overall (n=255) | Surface measurement
group (n=117) | ECG-guided group
(n=138) | P-value |
|---|
| Phlebitis | 8 (3.14) | 5 (4.27) | 3 (2.17) | NS |
| Thrombosis | 6 (2.35) | 4 (3.42) | 2 (1.45) | NS |
| Arrhythmia | 7 (2.76) | 3 (2.56) | 4 (2.90) | NS |
Discussion
Compared with chest TIVAP, the arm implementation
site provides an improvement in patient satisfaction and
quality-of-life categories during chemotherapy (20). The position of the catheter tip is
important for central venous catheters, particularly for long-term
devices (21,22). Accurate positioning of the catheter
tip is one of the most critical technical steps in central venous
catheter insertion (23). The
traditional measurement method is the most common and convenient
one, while intracavitary ECG-guided tip positioning has high
specificity and sensitivity (24).
Recent research on PICC ports recommended using the intracavitary
ECG technique to locate the catheter tip (25). The principle of intracavitary ECG
localization technology is to guide the patient's intracavitary ECG
using the conductivity of blood, normal saline or a guide wire. In
the present study, the accuracy and the best positioning rate of
the catheter tip were compared between the ECG-guided positioning
technique and the traditional measurement method. The results
suggested that intracavitary ECG guidance is able to improve the
accuracy and the best positioning rate of the catheter tip compared
with the traditional measurement method, which proved that the
intracavitary ECG-guided tip positioning technique is feasible and
effective in placing the upper arm implantable infusion port in
patients with malignant tumours.
Improper catheter placement not only prolongs the
operation time but also increases the radiation exposure of
patients and medical staff by repeated DSA fluoroscopy (26). The present study indicated that the
intracavitary ECG-guided tip positioning technique is able to
improve the accuracy of tip catheter placement and save operation
time, thus reducing exposure to ionizing radiation due to repeated
positioning. Considering the accuracy of intracardiac ECG
localization at the tip of the central venous catheter and the
influence of X-ray irradiation on patients, an increasing number of
researchers suggested that X-ray examination should be cancelled
after intracavitary ECG-guided tip positioning (26,27).
However, this technology requires medical staff to have a high
ability to analyse and interpret ECG. In the clinic, it may be
suggested that surgeons with certain operating experience cancel
the X-ray examinations after the operation.
Compared with the chest wall port, TIVIP in the
upper arm is able to reduce complications such as pneumothorax,
haemothorax and pinch-off syndrome. The latest research indicates
that the PICC port is a safe vascular device and may be an
alternative option to traditional arm ports and chest ports
(25). Compared with the PICC
port, the arm ports may have a slightly higher incidence of
complications. However, the arm ports also have the advantages of
relatively simple operation and less restriction on arm movement.
The only constant issue is that they all require accurate
positioning of the catheter tip. If the central venous catheter is
too shallow, the incidence of phlebitis and venous thrombosis
increases (28). If the catheter
is implanted too deeply, the head end may enter the right atrium,
which may lead to complications such as arrhythmia or myocardial
injury (29). The intracavitary
ECG-guided tip positioning technique has the function of real-time
positioning. The optimal position of the catheter may be found in
time and adjusted during the operation, without repeated adjustment
after the operation, which may reduce the occurrence of
complications (30).
Adjusting the position of the catheter tip causes
friction between the catheter and the blood vessel, which leads to
intimal damage and subsequently to phlebitis and venous thrombosis.
The present study suggested that the intracavitary ECG-guided tip
positioning technique may reduce the occurrence of complications
caused by catheter placement. Further studies and prospective
multicentre clinical trial data should be collected to confirm the
results.
Based on the above results, it may be recommended to
use the intracavitary ECG technique to locate the catheter tip as
an alternative to the traditional surface measurement method. This
is in line with the recommendations of other researchers (25,31).
However, there are certain limitations to this study. First, as
with any retrospective study, there was poor control over the
factors influencing outcomes, covariates and potential confounders.
Furthermore, the present study was a single-centre study. The
sample size of the study was small and larger-sample studies should
be performed to validate the results. In addition, late
complications should be assessed in a multicentre, prospective
study.
In conclusion, the intracavitary ECG-guided tip
positioning technique may accurately locate the tip of the catheter
of the upper arm implantable infusion port and reduce the operation
time, which has great clinical significance. The related operation
steps and procedures provided in the present study have been
implemented in clinical practice and the results are remarkable.
However, the sample size of the present study was small and methods
require to be constantly revised and improved in future clinical
practice.
Acknowledgements
Not applicable.
Funding
Funding: This study was funded by the Nursing Society of Suzhou
(grant no. 2019C06).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JZ was the main leader and director of the project.
JZ and HL were responsible for the conception and design of the
study. LS, HC and HL collected the data, analysed the datasets and
provided academic support. LS and HC analysed and interpreted the
datasets and wrote the manuscript. YY assisted in the experiments
and provided data analysis. HL critically revised the manuscript.
LS and HC confirm the authenticity of all the raw data. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
The Affiliated Suzhou Hospital of Nanjing Medical University
(Suzhou, China). Consent to participate was provided by each of the
patients. All procedures of this study were performed in accordance
with the Declaration of Helsinki.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests regarding this work.
References
|
1
|
Canfora A, Mauriello C, Ferronetti A,
Marte G, Di Maio V, Ciorra G, Esposito MG, Giuliano ME, Fregola G,
Barra L, et al: Efficacy and safety of ultrasound-guided placement
of central venous port systems via the right internal jugular vein
in elderly oncologic patients: Our single-center experience and
protocol. Aging Clin Exp Res. 29 (Suppl 1):S127–S130.
2017.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Bow EJ, Kilpatrick MG and Clinch JJ:
Totally implantable venous access ports systems for patients
receiving chemotherapy for solid tissue malignancies: A randomized
controlled clinical trial examining the safety, efficacy, costs,
and impact on quality of life. J Clin Oncol.
17(1267)1999.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Klaiber U, Probst P, Hackbusch M, Jensen
K, Dörr-Harim C, Hüttner FJ, Hackert T, Diener MK, Büchler MW and
Knebel P: Meta-analysis of primary open versus closed cannulation
strategy for totally implantable venous access port implantation.
Langenbecks Arch Surg. 406:587–596. 2021.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Pinelli F, Cecero E, Degl'Innocenti D,
Selmi V, Giua R, Villa G, Chelazzi C, Romagnoli S and Pittiruti M:
Infection of totally implantable venous access devices: A review of
the literature. J Vasc Access. 19:230–242. 2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Dariushnia SR, Wallace MJ, Siddiqi NH,
Towbin RB, Wojak JC, Kundu S and Cardella JF: Society of
Interventional Radiology Standards of Practice Committee. Quality
improvement guidelines for central venous access. J Vasc Interv
Radiol. 21:976–981. 2010.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Kurul S, Saip P and Aydin T: Totally
implantable venous-access ports: Local problems and extravasation
injury. Lancet Oncol. 3:684–692. 2002.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Minichsdorfer C, Füreder T, Mähr B,
Berghoff AS, Heynar H, Dressler A, Gnant M, Zielinski C and Bartsch
R: A cross-sectional study of patients' satisfaction with totally
implanted access ports. Clin J Oncol Nurs. 20:175–180.
2016.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sun X, Bai X, Shen J, Yu Z, Zhuang Z and
Jin Y: Comparison between ultrasound-guided TIVAD via the right
innominate vein and the right internal jugular vein approach. BMC
Surg. 19(189)2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Tabatabaie O, Kasumova GG, Eskander MF,
Critchlow JF, Tawa NE and Tseng JF: Totally implantable venous
access devices: A review of complications and management
strategies. Am J Clin Oncol. 40:94–105. 2017.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Gonda SJ and Li R: Principles of
subcutaneous port placement. Tech Vasc Interv Radiol. 14:198–203.
2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tippit D, Siegel E, Ochoa D, Pennisi A,
Hill E, Merrill A, Rowe M, Henry-Tillman R, Ananthula A and Makhoul
I: Upper-extremity deep vein thrombosis in patients with breast
cancer with chest versus arm central venous port catheters. Breast
Cancer (Auckl). 12(1178223418771909)2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Zhou C, Lu L, Yang L, Xi W, Ma T, Yang C,
Wu J, Shangguan C, Zhu Z and Zhang J: Modified surface measurement
method to determine catheter tip position of totally implantable
venous access port through right subclavian vein. J Vasc Surg
Venous Lymphat Disord. 9:409–415. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Liu G, Hou W, Zhou C, Yin Y, Lu S, Duan C,
Li M, Toft ES and Zhang H: Meta-analysis of intracavitary
electrocardiogram guidance for peripherally inserted central
catheter placement. J Vasc Access. 20:577–582. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yuan L, Li R, Meng A, Feng Y, Wu X, Yang
Y, Chen P, Qiu Z, Qi J, Chen C, et al: Superior success rate of
intracavitary electrocardiogram guidance for peripherally inserted
central catheter placement in patients with cancer: A randomized
open-label controlled multicenter study. PLoS One.
12(e0171630)2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cuschieri S: The STROBE guidelines. Saudi
J Anaesth. 13 (Suppl 1):S31–S34. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Xu H, Chen R, Jiang C, You S, Zhu Q, Li Y,
Li S, Zha X and Wang J: Implanting totally implantable venous
access ports in the upper arm is feasible and safe for patients
with early breast cancer. J Vasc Access. 21:609–614.
2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Akahane A, Sone M, Ehara S, Kato K, Tanaka
R and Nakasato T: Subclavian vein versus arm vein for totally
implantable central venous port for patients with head and neck
cancer: A retrospective comparative analysis. Cardiovasc Intervent
Radiol. 34:1222–1229. 2011.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Hinck SM: Implementing the infusion
therapy standards of practice. Home Healthc Now.
39(295)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Gorski LA: The 2016 infusion therapy
standards of practice. Home Healthc Now. 35:10–18. 2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Burbridge B and Goyal K: Quality-of-life
assessment: Arm TIVAD versus chest TIVAD. J Vasc Access.
17:527–534. 2016.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jheengut Y and Fan B: Intraoperative
identification of persistent left superior vena cava with
intracavitary electrocardiogram during venous port insertion: A
report of eight cases. J Vasc Access. 22:834–839. 2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Sousa B, Furlanetto J, Hutka M, Gouveia P,
Wuerstlein R, Mariz JM, Pinto D and Cardoso F: ESMO Guidelines
Committee. Central venous access in oncology: ESMO clinical
practice guidelines. Ann Oncol. 26 (Suppl 5):v152–v168.
2015.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Li J, Chen W, Zhao W, Zhang H, Huang Z,
Zhang S and Li Y: Surface measurement, intracardiac
electrocardiogram and tracheal bifurcation techniques for locating
the catheter tips of totally implantable venous access port. Comput
Methods Programs Biomed. 187(105238)2020.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Rosche N and Stehr W: Evaluation of a
magnetic tracking and electrocardiogram-based tip confirmation
system for peripherally inserted central catheters in pediatric
patients. J Infus Nurs. 41:301–308. 2018.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Bertoglio S, Annetta MG, Brescia F, Emoli
A, Fabiani F, Fino M, Merlicco D, Musaro A, Orlandi M, Parisella L,
et al: A multicenter retrospective study on 4480 implanted
PICC-ports: A GAVeCeLT project. J Vasc Access: 11297298211067683,
Jan 17, 2022. (Epub ahead of print).
|
|
26
|
Bloemen A, Daniels AM, Samyn MG, Janssen
RJ and Elshof JW: Electrocardiographic-guided tip positioning
technique for peripherally inserted central catheters in a Dutch
teaching hospital: Feasibility and cost-effectiveness analysis in a
prospective cohort study. J Vasc Access. 19:578–584.
2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Walker G, Chan RJ, Alexandrou E, Webster J
and Rickard C: Effectiveness of electrocardiographic guidance in
CVAD tip placement. Br J Nurs. 24:S4, S6. S8–S12. 2015.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Jonczyk M, Gebauer B, Rotzinger R,
Schnapauff D, Hamm B and Collettini F: Totally implantable central
venous port catheters: Radiation exposure as a function of puncture
site and operator experience. In vivo. 32:179–184. 2018.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Gurkan S, Seber S, Gur O, Yetisyigit T,
Okan Donbaloglu M and Ozkaramanli Gur D: Retrospective evaluation
of totally implantable venous access port devices: Early and late
complications. J BUON. 20:338–345. 2015.PubMed/NCBI
|
|
30
|
Li A, Jiao J, Zhang Y, Tian L, Miao J, Hao
X, Sun Z and Sun Q: A randomized controlled study of bedside
electrocardiograph-guided tip location technique & the
traditional chest radiography tip location technique for
peripherally inserted central venous catheter in cancer patients.
Indian J Med Res. 147:477–483. 2018.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Bertoglio S, Cafiero F, Meszaros P,
Varaldo E, Blondeaux E, Molinelli C and Minuto M: PICC-PORT totally
implantable vascular access device in breast cancer patients
undergoing chemotherapy. J Vasc Access. 21:460–466. 2020.PubMed/NCBI View Article : Google Scholar
|