Introduction
As a result of iodization programs implemented
throughout the world to address iodine deficiency disorders, giant
goiter is rare today (1). The
incidence of endemic goiter has decreased to 1% worldwide thanks to
those iodization programs (2). The
presence of giant goiter is among the causes of difficult airway
management. Advanced airway procedures may be necessary in cases
requiring intubation. The published literature mainly covers airway
management during thyroid surgery in patients with goiter, but
reports of giant goiter cases requiring emergency intubation at the
intensive care unit (ICU) are scarce. The present study aimed to
share our experience with a type of case that is rarely seen and
may lead to mortal complications if not well managed. The present
report describes a patient with giant retrosternal goiter
presenting with respiratory arrest who underwent emergency
tracheostomy after multiple attempts at orotracheal intubation and
then thyroidectomy during the ICU stay due to the development of
tracheomalacia.
Case report
A 63-year-old male patient was admitted to Ankara
City Hospital (Ankara, Turkey) in November 2021 with respiratory
arrest. The patient with known hypertension had anterior neck
swelling for 5 years and hoarseness symptoms that developed in the
last months. During resuscitation, orotracheal intubation was not
successful despite multiple attempts, including video laryngoscopy
and fiberoptic intubation. According to the difficult airway
management algorithms (3), an
emergency tracheostomy was performed. The emergency percutaneous
tracheostomy was performed with the Griggs method by ear nose
throat surgeons and an intensivist. Tracheostomy was performed by
creating an opening between the 2nd-3rd tracheal rings, above the
thyroid isthmus. An 8-mm tracheostomy cannula was inserted. After
the patient responded to cardiopulmonary resuscitation and his
vital signs became stable, computed tomography (CT) imaging of the
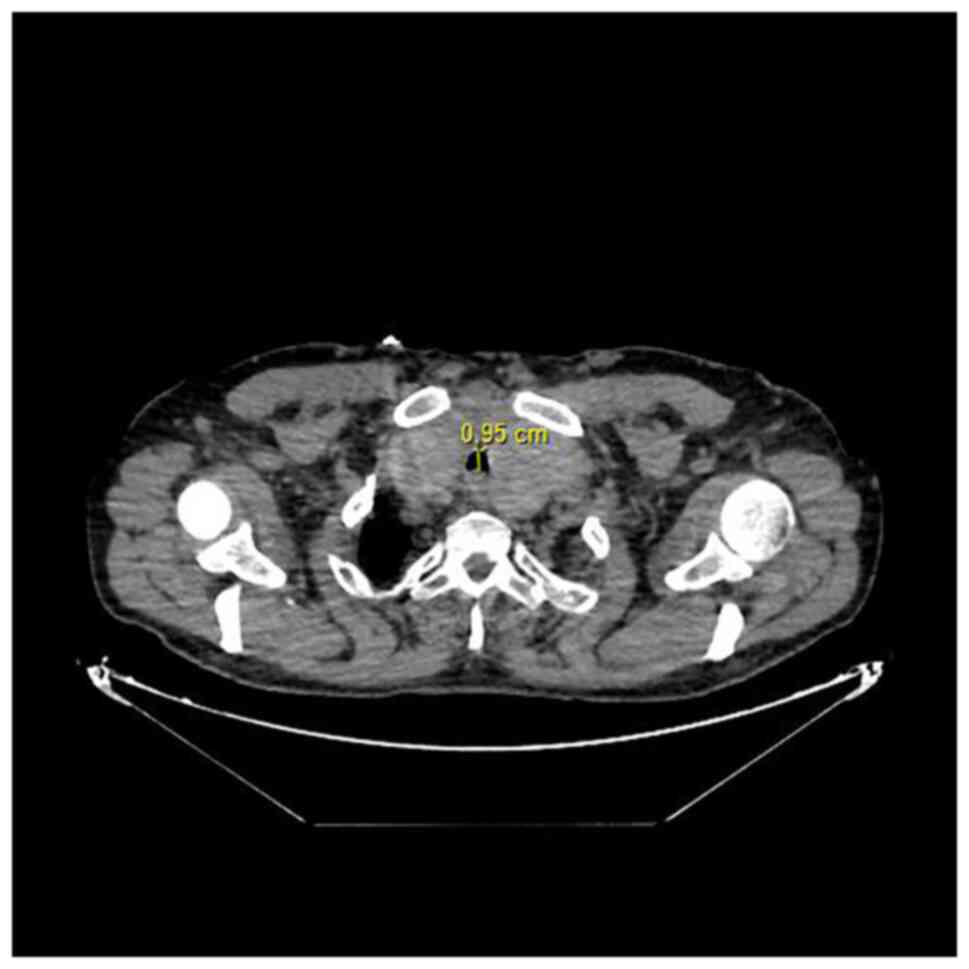
neck was performed. Oropharyngeal, hypopharyngeal and laryngeal
stenoses were evident. At the supraglottic level, the laryngeal air
column was completely obliterated. The tracheal lumen caliber was
markedly narrow along the tracheostomy cannula and the tracheal
stenosis extended up to the supracarinal level (Fig. 1). An extension of the enlarged
thyroid gland into the mediastinal intrathoracic area was
observed.
Monitoring of the patient indicated low tidal
volumes and respiratory distress, necessitating an emergency
bronchoscopy. It was observed that the inserted size 8 mm
tracheostomy cannula was insufficient to access the trachea due to
thyroid enlargement. The cannula was replaced with a size 8 mm
spiral-embedded endotracheal tube. On the first day of ICU
follow-up, no additional conditions were detected and the patient
was conscious and cooperative. Thyroid function tests indicated the
following: Thyroid-stimulating hormone, 0.50 mU/l (normal range,
0.55-4.78 mU/l); free triiodothyronine (T3), 2.34 ng/l (normal
range, 2.3-4.2 ng/l); and free thyroxin (T4), 1.13 ng/dl (normal
range, 0.89-1.76 ng/dl). However, the goiter caused compression;
thus, the patient was evaluated for surgery and a total
thyroidectomy was planned. Because of the urgency of the process,
it was not possible to explore the mobility of the vocal cords
prior to thyroidectomy. Due to the retrosternal extension of the
enlarged thyroid tissue, both general surgery and thoracic surgery
teams were present during the operation including total
thyroidectomy via sternotomy. Bilateral recurrent laryngeal nerves
were carefully identified during thyroidectomy and intraoperative
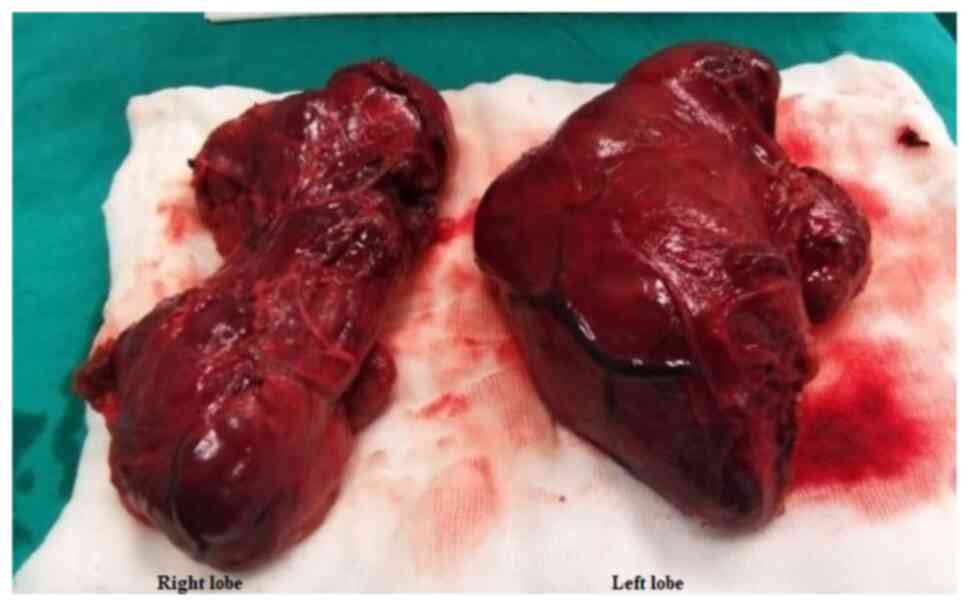
nerve monitoring was performed. The removed right lobe of the
thyroid gland was 19x13x9 cm in size and weighed 295 g and the left
lobe was 23x14x8.5 cm and weighed 465 g (Fig. 2). The surgical specimens sent for
pathology examination were reported as compatible with the
diagnosis of multinodular goiter.
The patient remained stable during the
post-operative follow-up at the ICU and the spiral-embedded
endotracheal tube in the tracheostomy was replaced with a size 8 mm
tracheostomy cannula without any complications. The patient was
then placed on a mechanical ventilator in spontaneous mode.
Post-operative fibreoptic laryngoscopy was performed to examine
vocal cord movements and bilateral vocal cord motions were normal.
On the postoperative first day he was conscious and cooperative and
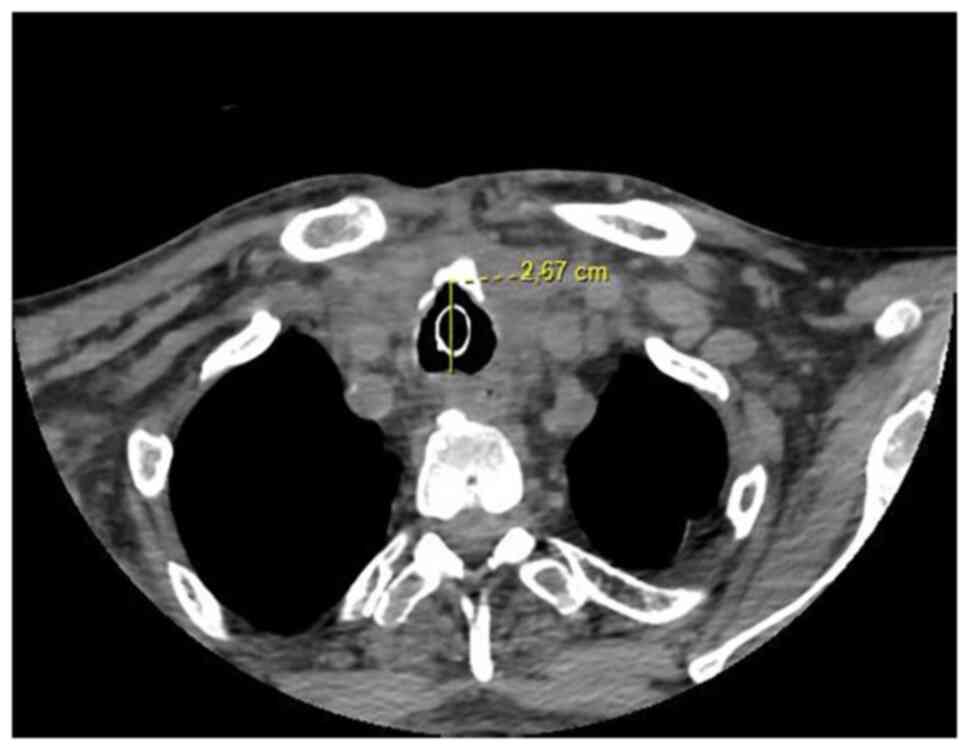
oral intake was normal. Post-operative control CT and bronchoscopy
were evaluated together with the thoracic surgery clinicians
(Fig. 3). Due to tracheomalacia,
it was decided to discharge the patient with the tracheostomy. The
patient was discharged with a home mechanical ventilator, and
rehospitalized one month later for follow-up controls and weaning
trial. The CT of the neck and bronchoscopy control indicated no
abnormality. After successful weaning trials, the tracheostomy tube
was decannulated on the post-operative 45th day. No complications
or oxygen demand occurred after the weaning and the patient was
discharged with full recovery.
Discussion
Retrosternal goiter is common among females and in
the fifth decade of life. The condition is asymptomatic in 15-50%
of patients (4). Giant goiter
frequently causes dyspnea, hoarseness and dysphagia, but may also
lead to life-threatening complications (5).
A difficult airway is a clinical situation
encountered at the ICU due to various reasons and may result in
mortality if not managed well (6).
Video laryngoscopy, fiberoptic intubation or emergency tracheostomy
may be applied in patients with upper airway obstruction (UAO) as
per the algorithms of difficult airway management (3). The preferred method may vary
depending on the size of the thyroid gland, and the level and
location of tracheal obstruction. Emergency tracheostomy stands out
as a life-saving maneuver in UAO but may also be risky in cases
where enlarged thyroid tissue prevents access to the trachea
(7). Selecting the most
appropriate method in line with the algorithms is crucial for
patient safety.
In a study on retrosternal goiter, White et
al (8) reported tracheomalacia
in 50% of their cases, one-third of which underwent tracheostomy.
In patients with giant goiter, it is crucial to plan surgical
intervention at an early phase once airway patency is achieved.
Emergency thyroidectomy is recommended in the literature for
goiters with severe compression (9). It has been reported that acute airway
obstruction is observed in patients with giant goiter due to
intrathyroid hemorrhage, tracheal compression or tumor invasion of
the lumen in thyroid malignancies, and <1% of these patients
require emergency thyroidectomy (10). During the post-operative period,
patients should be carefully evaluated for extubation.
Tracheomalacia and tracheal collapse may develop due to softening
of the tracheal tissue and loss of tone, particularly after
prolonged tracheal compression. If tracheomalacia is present, early
extubation after thyroidectomy may result in severe respiratory
distress (8). However, the
published literature provides no standard recommendations for
weaning from ventilation in patients with tracheomalacia. The
physician should keep in mind that tracheomalacia may have
developed and therefore, gradual and controlled weaning should be
provided in these patients.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HCD conceptualized the study. HCD analyzed patient
data and provided critical revisions. HCD obtained the medical
images and made substantial contributions to data interpretation.
HCD confirmed the authenticity of all the raw data and read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent
regarding treatment interventions, and the collection and
publication of images and other clinical data.
Competing interests
The author declares that she has no competing
interests.
References
|
1
|
Zimmermann MB and Boelaert K: Iodine
deficiency and thyroid disorders. Lancet Diabetes Endocrinol.
3:286–295. 2015.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Vanderpump MP: The epidemiology of thyroid
disease. Br Med Bull. 99:39–51. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Higgs A, McGrath BA, Goddard C, Rangasami
J, Suntharalingam G, Gale R and Cook TM: Difficult Airway Society;
Intensive Care Society; Faculty of Intensive Care Medicine; Royal
College of Anaesthetists. Guidelines for the management of tracheal
intubation in critically ill adults. Br J Anaesth. 120:323–352.
2018.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Doulaptsi M, Karatzanis A, Prokopakis E,
Velegrakis S, Loutsidi A, Trachalaki A and Velegrakis G: Substernal
goiter: Treatment and challenges. Twenty-two years of experience in
diagnosis and management of substernal goiters. Auris Nasus Larynx.
46:246–251. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Wong WK, Shetty S, Morton RP, McIvor NP
and Zheng T: Management of retrosternal goiter: Retrospective study
of 72 patients at two secondary care centers. Auris Nasus Larynx.
46:129–134. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Duwat A, Turbelin A, Petiot S, Hubert V,
Deransy V, Mahjoub Y and Dupont H: French national survey on
difficult intubation in intensive care units. Ann Fr Anesth Reanim.
33:297–303. 2014.PubMed/NCBI View Article : Google Scholar : (In French).
|
|
7
|
Bontempo LJ and Manning SL: Tracheostomy
emergencies. Emerg Med Clin North Am. 37:109–119. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
White ML, Doherty GM and Gauger PG:
Evidence-based surgical management of substernal goiter. World J
Surg. 32:1285–1300. 2008.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Wong P, Chieh Liew GH and Kothandan H:
Anaesthesia for goitre surgery: A review. Procee Singapore
Healthcare. 24:165–170. 2015.
|
|
10
|
Testini M, Logoluso F, Lissidini G,
Gurrado A, Campobasso G, Cortese R, De Luca GM, Franco IF, De Luca
A and Piccinni G: Emergency total thyroidectomy due to non
traumatic disease. Experience of a surgical unit and literature
review. World J Emerg Surg. 7(9)2012.PubMed/NCBI View Article : Google Scholar
|