Introduction
The mediastinum has a narrow gap. Anatomically, it
is divided into the superior and inferior mediastinum based on the
sternal angle and the lower margin of the fourth thoracic vertebra;
the inferior mediastinum is divided into the anterior, middle and
posterior parts based on the anterior and posterior walls of the
pericardium. Mediastinal cysts are rare benign mediastinal lesions
that account for ~25% of mediastinal masses (1). They are generally asymptomatic and
are frequently discovered during health check-ups. However, they
may be complicated by infection, enlargement, spontaneous rupture
or malignant transformation (2).
When cysts become larger or malignant, oppression or invasion of
adjacent anatomical structures may cause various types of
discomfort, such as chest tightness, chest pain, cough, shortness
of breath, hoarseness, hiccups, palpitation and dyspnoea (3). The tissue origin of cysts frequently
depends on the close relationship between their location and
mediastinal anatomy, such as thymic, bronchogenic, pericardial,
esophageal and neurogenic cysts. Clinically, the diagnosis and
treatment of mediastinal cysts is primarily surgical resection.
Endoscopic ultrasound (EUS) is a well-established
imaging modality that helps to determine the nature, layer of
origin and extent of lesions, and is mostly used to diagnose and
treat of gastrointestinal and biliary pancreatic diseases (4). In mediastinal lesions, it is mainly
used for the evaluation and biopsy of mediastinal masses and lymph
nodes (5), as it may distinguish
complex structures in the mediastinum, such as blood vessels, lymph
nodes and soft tissues, and display the relative position of blood
vessels, organs and masses, helping clinicians to avoid damage to
blood vessels or tissues during puncture. In recent years, the
development of EUS has opened up a new field of vision for precise,
minimally invasive diagnosis and treatment of diseases, and its
application and scope are becoming increasingly extensive. However,
EUS-guided fine-needle aspiration (EUS-FNA) of mediastinal cysts
remains controversial due to the risk of complications. The present
study reported a case of posterior mediastinal cyst treated with
EUS-FNA combined with an intracapsular injection of antibiotics and
ethanol, which provides a new method for diagnosing and treating
mediastinal cysts.
Case report
A 53-year-old male was admitted to the cardiology
department of Mianyang Central Hospital (Mianyang, China) in
February 2022 as a referral from the emergency department for
persistent chest pain for 20 days. It was the first time the
patient had this complaint. The patient did not have any other
symptoms/complaints such as fever, cough, chest tightness, fatigue,
palpitation, dyspnea or abdominal pain, and he denied any weight
loss with a BMI of ~24.2. On physical examination, there were no
obvious positive signs, except bradycardia, with a heart rate of 55
bpm. Laboratory workup revealed that only serum tumor marker CA199
(381.83 U/ml; reference range, <37 U/ml) level was significantly
increased. Other indicators, including blood routine, myocardial
markers, liver function, blood lipids, renal function,
electrolytes, coagulation function, thyroid function, glycosylated
hemoglobin, myocardial markers and pro-B-type natriuretic peptide,
were all normal.
Since the patient had chest pain, the cardiologist
ordered color doppler echocardiography, coronary computed
tomography (CT) and enhanced chest CT to determine the cause. Color
echocardiography indicated a posterior left atrial cystic
hypoechoic mass and coronary CT displayed a cystic mass in the
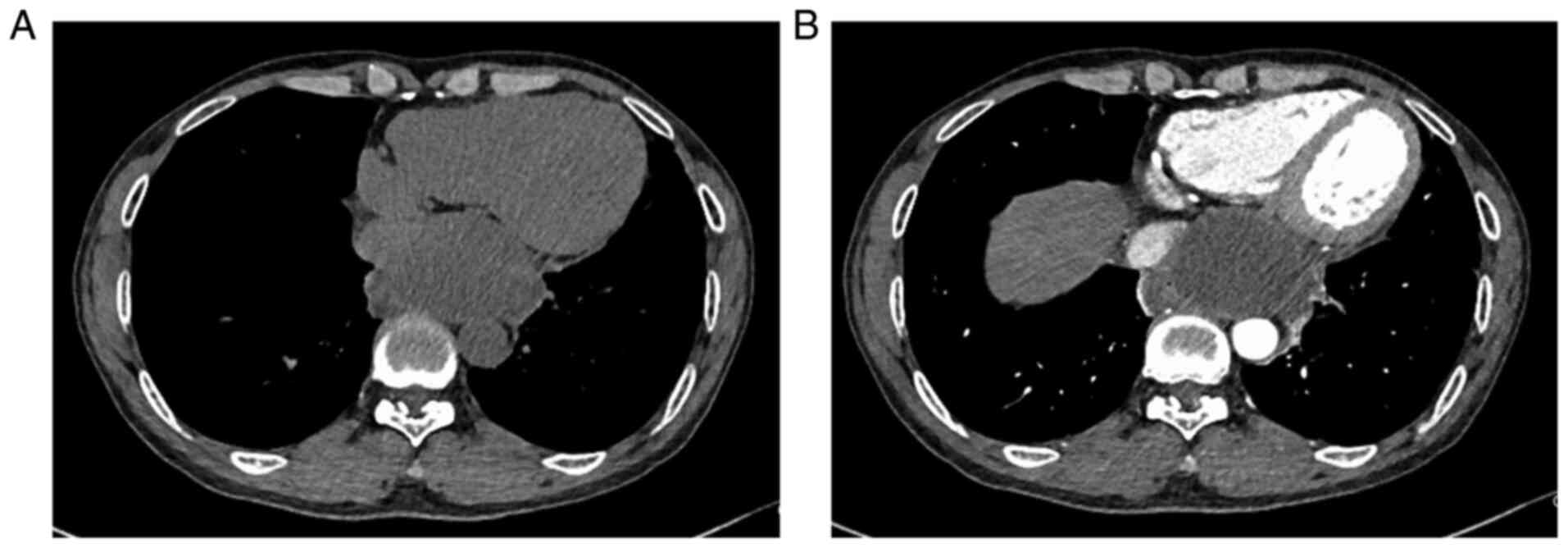
posterior mediastinum. Plain and enhanced thoracic CT indicated a
cystic hypodense mass of ~7.7x4.7 cm above the esophageal hiatus in
the posterior mediastinum, with a thick wall, mild enhancement,
partly clear boundary, arc-shaped indentation adjacent to the
heart, esophagus and inferior vena cava, and the boundary between
the inner margin and esophagus was unclear, which revealed a
possible mediastinal cyst (Fig.
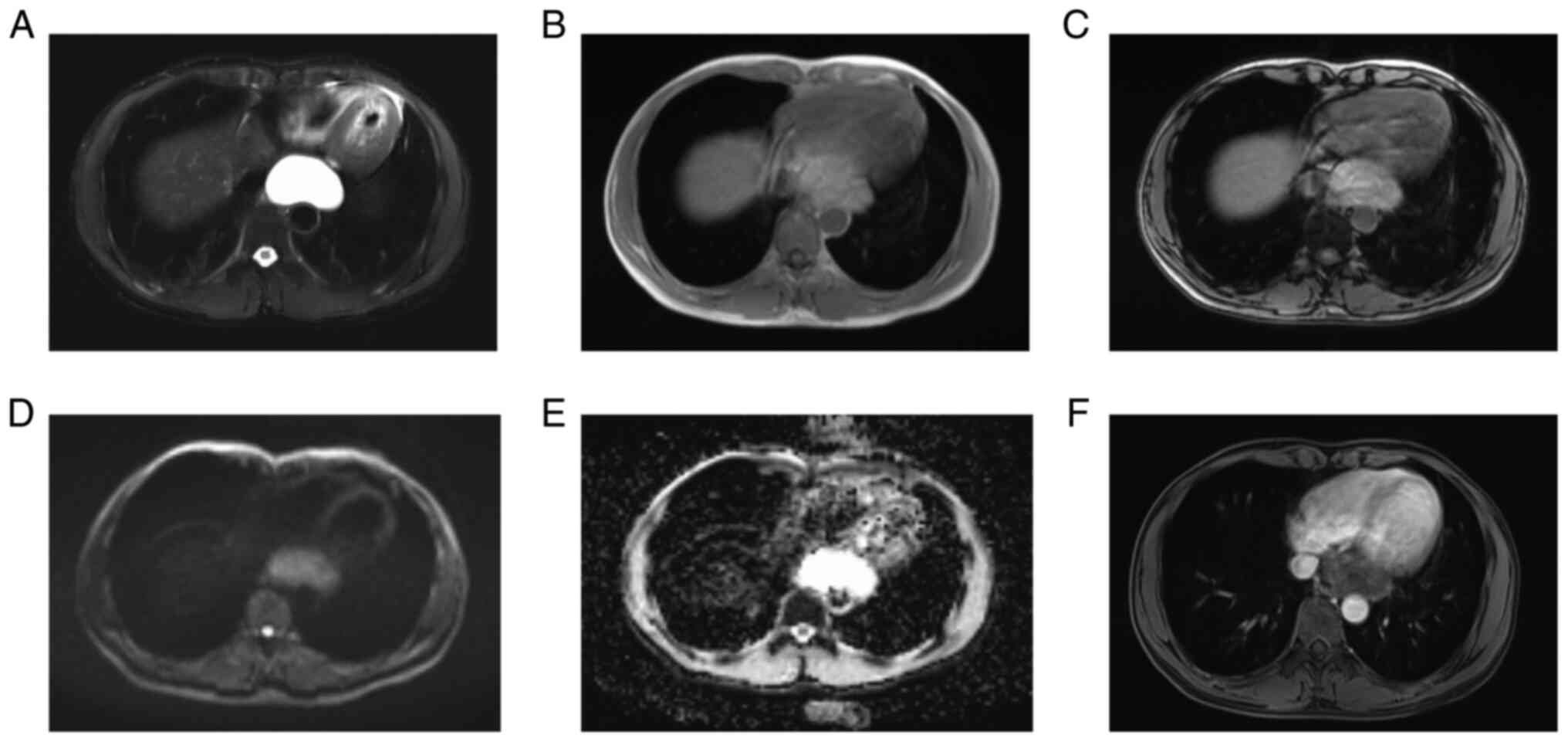
1). Plain and enhanced mediastinal magnetic resonance imaging
(MRI) revealed a lumpy abnormal signal shadow in the posterior
mediastinum, with a clear boundary of ~6.0x4.0x5.2 cm,
hyperintensity on T2-weighted imaging, iso-slight hyperintensity on
T1-weighted imaging, a slightly increased signal on reverse phase,
a slightly higher signal on diffusion-weighted imaging, obvious
hyperintensity on apparent diffusion coefficients mapping, no
obvious enhancement overall and suspicious slight enhancement on
the edge, which further supported that the cystic mass was a benign
lesion, most likely a cyst (Fig.
2). The upper gastrointestinal barium contrast indicated that
the mass compressed the lower part of the esophagus to form an
arc-shaped indentation. Endoscopy was performed to clarify further
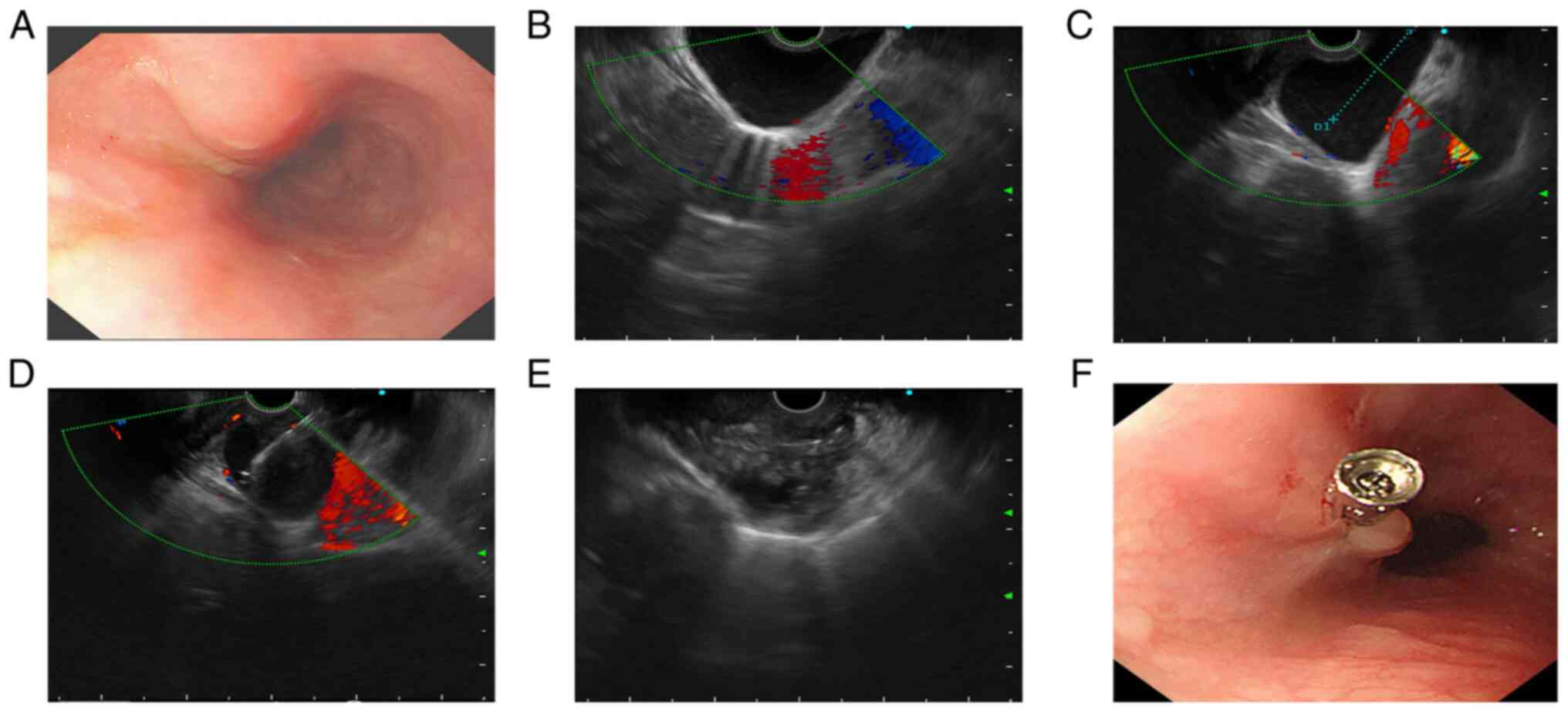
the relationship between the cyst and the esophagus. Gastroscopy
indicated a strip of submucosal eminence at a distance of 24-40 cm
from the incisors with a smooth mucosal surface (Fig. 3A). EUS (Olympus Ltd) further
revealed a cystic mass of ~6x4.5 cm outside the esophageal wall and
no blood flow signal under color doppler imaging (Fig. 3B).
Based on these findings, cardiothoracic surgeons and
gastroenterologists at our hospital were consulted regarding the
diagnosis and treatment, and the patient was referred to our
department for further treatment after careful consideration. Under
EUS guidance, a 19-gauge needle (Cook Medical, Inc.) was used to
puncture the cyst through the lower part of the esophagus while
avoiding the blood flow signal. Turbid cystic fluid (~40 ml) was
extracted and the capsular wall was lavaged repeatedly with
metronidazole (Sichuan Kelun Pharmaceutical Co., Ltd.) and
anhydrous alcohol, leaving 3 ml of anhydrous alcohol in the cyst. A
small amount of oozing blood was found at the puncture point in the
lower part of the esophagus and a titanium clip was used to clamp
the puncture point (Fig. 3C-F).
Finally, the patient received prophylactic treatment to prevent
infection [0.75 g cefuroxime (Guangzhou Baiyunshan Tianxin
Pharmaceutical Co., Ltd.); single dose intravenous drip; once in
total]. A fluid-based smear of the puncture fluid of the posterior
mediastinal cyst revealed a small number of neutrophils and
lymphocytes. After 3 days of observation, the patient's chest pain
was relieved and there were no symptoms such as fever, cough,
expectoration, hematemesis or black stool. The patient's condition
improved and he was discharged from the hospital. At a follow-up
visit 3 months later, the patient had no further symptoms and chest
CT indicated no recurrence of the cyst.
Discussion
The mediastinum harbors the living organs, including
the heart and the great blood vessels, esophagus, trachea, thymus,
nerves and lymphoid tissues. Chest CT and MRI are the preferred
diagnostic methods for mediastinal cysts. Mediastinal cysts of
various etiologies share common imaging findings and their shape is
generally round and oval with a soft texture when less hindered by
surrounding structures. Even when occurring in the organ space,
their shape also has certain compliance with adjacent structures
and exhibits a corresponding irregular shape. Most cysts have
smooth outlines, clear borders and no enhancement. Certain cysts
display with regular soft-tissue density walls with a thickness of
2-3 mm, which are usually enhanced on enhanced scans. The cyst has
a uniform watery density; CT indicates the characteristic liquid CT
value and the MRI shows low signals on T1-weighed and T2-weighted
images. For certain proteinaceous, hemorrhagic or infected cysts,
CT manifestations and MRI images are atypical, which may indicate
soft tissue density CT values and higher T1-weighed signal images
(6,7). In the present case, the radiological
appearance of the cystic mass was consistent with that described
above, suggesting that it was likely to be a benign cyst.
It is well known that histopathology is the gold
standard for the diagnosis of masses. Most experts recommend
surgical treatment of mediastinal cysts, including thoracotomy,
mediastinoscopy and thoracoscopy, which may clarify its pathologic
diagnosis, remove the lesion, alleviate the patient's discomfort
and prevent possible complications (2,8,9).
However, for the present case, chest CT indicated a cystic mass
adjacent to the heart, esophagus and inferior vena cava, and
surgery had the disadvantages of high risk, postoperative trauma,
high cost and slow recovery. Furthermore, certain patients cannot
be definitely diagnosed due to advanced age, underlying diseases
such as cardiopulmonary insufficiency, other surgical
contraindications, intolerance or lack of surgical opportunities.
Therefore, it is important and necessary to use a minimally
invasive diagnosis and treatment for mediastinal cysts.
Mediastinal cysts appear as well-circumscribed, oval
or round, liquid dark areas on intraluminal ultrasonography. EUS is
able to delineate the originating layer of the cyst in the
esophageal wall and the relationship between the cyst and the
esophagus (10). In the patient of
the present study, barium in the upper gastrointestinal tract
indicated that the esophagus was compressed by the mass, which was
further identified by EUS as a cyst outside the esophageal wall.
Furthermore, all examination results inferred that the cyst may be
benign and located in the posterior mediastinum, which is least
likely to contain a malignant mass in the three mediastinal
cavities (11). All of these
observations indicated that EUS-FNA could be performed. Using
EUS-FNA for cyst fluid, a qualitative diagnosis of mediastinal
cysts may be made, while avoiding missed diagnosis of malignant
diseases and significantly alleviating patients' discomfort
symptoms. Compared to surgery, it has the advantages of lower risk,
higher safety, wider indications, fewer complications, lower cost,
less trauma and faster recovery. Furthermore, even if the puncture
fluid confirms malignancy, it is not too late to perform additional
surgery after EUS-FNA. In the present case, the results indicated
no malignant cells in the puncture fluid, which proved that the
cystic mass in this patient was indeed a benign cyst, and surgery
was avoided.
However, EUS-FNA of mediastinal cysts remains
controversial due to the risk of complications. One potential
complication is infection. Certain studies suggest caution in
aspirating for suspected mediastinal cysts due to mediastinum
(12). Annema et al
(13) reported a case of bronchial
cyst EUS-FNA without antibiotics causing mediastinitis. Valli et
al (14) reported that
patients in a case series developed severe FNA-induced cyst
infection without antibiotics, leading to mediastinitis requiring
surgical debridement. Another previous study indicated that EUS-FNA
was effective in preventing mediastinitis with a small 22G needle,
an intravenous dose of ciprofloxacin (400 mg) before puncture and
an oral dose of ciprofloxacin (500 mg 12-hourly for 5 days) after
puncture (15). The American
Society for Gastrointestinal Endoscopy guidelines also recommended
prophylactic antibiotics (mainly intravenous and oral) for EUS-FNA
in mediastinal cystic lesions (16). However, Diehl et al
(17) noted that 3 patients with
mediastinal cysts developed infections after EUS-FNA despite
receiving accepted techniques, including prophylactic antibiotics;
therefore, intravenous antibiotics may not completely prevent
mediastinal infection complications. In addition, there is a
paucity of studies on intracapsular antibiotic injection.
Considering the large cyst in the patient of the present study, to
shorten the suction time, a 19G needle and intracapsular injection
of metronidazole were used to prevent anaerobic infection, which
proved to be successful, and the patient had no infection after
EUS-FNA. At 3 days after puncture, the patient was discharged,
which not only relieved the symptoms of chest pain but also
shortened the hospital stay and saved the hospitalization cost.
Another possible risk is a cyst recurrence, thought
to be caused by failure to clear the lining of the cyst wall
completely. Ethanol sclerotherapy is an effective treatment for
numerous types of benign cyst, such as liver, kidney and
bronchogenic cysts. Ethanol can not only dehydrate epithelial cells
of the cyst wall, coagulate and denature proteins, and destroy
cells to impair their secretory function, but also induces aseptic
inflammation and sealing of the cyst cavity, so as to prevent cyst
recurrence (18,19). Lee et al (20) reported that EUS-guided
ethanol-sparing therapy for treating a large symptomatic liver cyst
did not result in cyst recurrence at a median follow-up of 66
months, revealing that ethanol may prevent cyst recurrence.
Lakadamyali et al (21)
reported good results with CT-guided aspiration and ethanol
sclerotherapy for bronchogenic cysts, with no recurrence observed
on follow-up MRI after 1 year. In the present case, the cyst wall
was repeatedly lavaged with ethanol and a portion of the ethanol
was retained within the cyst. There was no recurrence of the cyst
during the 3-month follow-up chest CT. Of course, this also
requires a longer follow-up and a larger sample size. If cyst
recurrence is unfortunately found during longer follow-up, EUS-FNA
treatment may be repeated, but even then, the benefit to the
patient is greater than that of surgery.
In conclusion, EUS-FNA combined with intracapsular
injection of antibiotics and ethanol is safe and feasible for
treating mediastinal cysts, without complications of mediastinal
infection and cyst recurrence. It may relieve the discomfort
symptoms of patients, avoid surgery, shorten the length of hospital
stay and reduce hospitalization costs, so that patients get the
maximum benefit. It is a new diagnosis and treatment method worth
attempting and recommending for benign posterior mediastinal cysts
indicated by multiple imaging examinations.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
LW and MF were responsible for the clinical
management of the patient. LW reviewed the literature and
contributed to data collection, analysis, interpretation and
manuscript drafting. XZ contributed to data collection, analysis
and interpretation. MF contributed to the literature search, data
collection, analysis and manuscript revision. XL contributed to the
design of the study, analysis and interpretation of data, and
reviewed and edited the manuscript. XZ, MF and XL confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent for the publication of the
case data/information and images was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Davis RD Jr, Oldham HN Jr and Sabiston DC
Jr: Primary cysts and neoplasms of the mediastinum: Recent changes
in clinical presentation, methods of diagnosis, management, and
results. Ann Thorac Surg. 44:229–237. 1987.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ponn RB: Simple mediastinal cysts: Resect
them all? Chest. 124:4–6. 2003.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Aroor AR, Prakasha SR, Seshadri S, S T and
Raghuraj U: A study of clinical characteristics of mediastinal
mass. J Clin Diagn Res. 8:77–80. 2014.PubMed/NCBI View Article : Google Scholar
|
|
4
|
DiMagno EP, Buxton JL, Regan PT, Hattery
RR, Wilson DA, Suarez JR and Green PS: Ultrasonic endoscope.
Lancet. 1:629–631. 1980.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Wang Z and Jiang C: Endoscopic ultrasound
in the diagnosis of mediastinal diseases. Open Med (Wars).
10:560–565. 2015.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hwang EJ, Paek M, Yoon SH, Kim J, Lee HY,
Goo JM, Kim H, Kim H and Ackman JB: Quantitative thoracic magnetic
resonance criteria for the differentiation of cysts from solid
masses in the anterior mediastinum. Korean J Radiol. 20:854–856.
2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Liu W, Wang Y, Zhang W, Wu H and Liu Z:
Pneumonia, pleurisy, mediastinitis, and mediastinal cyst infection
secondary to endobronchial ultrasound-guided transbronchial needle
aspiration: A case report. Medicine (Baltimore).
100(e25973)2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Burjonrappa SC, Taddeucci R and Arcidi J:
Mediastinoscopy in the treatment of mediastinal cysts. JSLS.
9:142–148. 2005.PubMed/NCBI
|
|
9
|
Brzeziński D, Łochowski MP and Kozak J:
Videothoracoscopy in the treatment of mediastinal cysts. Wideochir
Inne Tech Maloinwazyjne. 9:393–397. 2014.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Cioffi U and de Simone M: Should
video-assisted surgery be the first line approach for bronchogenic
cysts? Asian Cardiovasc Thorac Ann. 19(289)2011.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Chao C, Vanguri V and Uy K: Robot-Assisted
thoracoscopic resection of a posterior mediastinal mullerian cyst.
Case Rep Pulmonol: Feb 4, 2018 (Epub ahead of print).
|
|
12
|
Wildi SM, Hoda RS, Fickling W, Schmulewitz
N, Varadarajulu S, Roberts SS, Ferguson B, Hoffman BJ, Hawes RH and
Wallace MB: Diagnosis of benign cysts of the mediastinum: The role
and risks of EUS and FNA. Gastrointest Endosc. 58:362–368.
2003.PubMed/NCBI
|
|
13
|
Annema JT, Veselic M, Versteegh MI and
Rabe KF: Mediastinitis caused by EUS-FNA of a bronchogenic cyst.
Endoscopy. 35:791–793. 2003.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Valli PV, Gubler C and Bauerfeind P:
Severe infectious complications after endoscopic ultrasound-guided
fine needle aspiration of suspected mediastinal duplication cysts:
A case series. Inflamm Intest Dis. 1:165–171. 2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Fazel A, Moezardalan K, Varadarajulu S,
Draganov P and Eloubeidi MA: The utility and the safety of
EUS-guided FNA in the evaluation of duplication cysts. Gastrointest
Endosc. 62:575–580. 2005.PubMed/NCBI View Article : Google Scholar
|
|
16
|
ASGE Standards of Practice Committee.
Khashab MA, Chithadi KV, Acosta RD, Bruining DH, Chandrasekhara V,
Eloubeidi MA, Fanelli RD, Faulx AL, Fonkalsrud L, et al: Antibiotic
prophylaxis for GI endoscopy. Gastrointest Endosc. 81:81–89.
2015.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Diehl DL, Cheruvattath R, Facktor MA and
Go BD: Infection after endoscopic ultrasound-guided aspiration of
mediastinal cysts. Interact Cardiovasc Thorac Surg. 10:338–340.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Larssen TB, Viste A, Horn A, Haldorsen IS
and Espeland A: Single-session alcohol sclerotherapy of symptomatic
liver cysts using 10-20 min of ethanol exposure: No recurrence at
2-16 years of follow-up. Abdom Radiol (NY). 41:1776–1781.
2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Livraghi T, Paracchi A, Ferrari C,
Bergonzi M, Garavaglia G, Raineri P and Vettori C: Treatment of
autonomous thyroid nodules with percutaneous ethanol injection:
Preliminary results. Work in progress. Radiology. 175:827–829.
1990.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Lee DS, Lee SK and Seo DW: Long-term
safety and efficacy of ethanol retention therapy via percutaneous
approach and/or EUS guidance for symptomatic large hepatic cysts
(with video). Endosc Ultrasound. 9:31–36. 2020.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lakadamyali H, Ergun T, Lakadamyali H and
Oguzkurt L: Alcohol ablation therapy of an atypically located
symptomatic bronchogenic cyst: A case report. Cardiovasc Intervent
Radiol. 30:1274–1276. 2007.PubMed/NCBI View Article : Google Scholar
|