1. Introduction
A human microbiome is a group of communities of
symbiotic and pathogenic microorganisms' genomes within certain
body regions. Bacteria, archaea, fungi, algae, small protists,
phages, viruses, and some genetic elements (plasmids) should be
considered a part of it, i.e. all non-human material. The term
‘microbiota’ defines living microorganisms at a certain location.
There are many distinct microbial ecosystems residing outside and
inside the human body. Gastrointestinal microbiota is the most
complex and most populated microbiota containing 100 trillion
microorganisms (1). The Human
Microbiome Project in 2007 revealed new data that was not
accessible by older methods. DNA sequencing methods, including 16S
ribosomal RNA sequencing, metagenomic sequencing, and microbial
metatranscriptomics changed our understanding of human microbial
communities entirely. The dogma of sterile lungs was deconstructed
and the microbiome in the lungs was revealed (2). The maintenance of microbial
homeostasis is recognized as an important health factor and its
susceptibility to environmental factors, like antibiotics, diet,
alcohol, and smoking, is intensively studied (3). We will hereby summarize the current
understanding of the microbiome-environment interactions, and the
involvement of microbiota in the pathogenesis of respiratory
diseases. We will also underscore some important future directions.
The field of human microbiomes and their clinical significance is
developing swiftly. An increasingly growing toolkit to investigate
microbiomes and their relationships with host systems delivers new
data continuously which needs to be reviewed again and again.
Microbial factors play a crucial role in the
development of human airways and lungs. Microorganisms determine
immune tolerance by recruiting immune cells with a regulatory
capacity and directly modulating the structural integrity of the
respiratory tissues and remodeling in the diseased lungs (4,5).
Furthermore, the development of immune tissues, like
mucosa-associated lymphoid tissue in the nose 55 and nasopharynx,
is orchestrated by microbial ecosystems (6). Viruses, bacteria, fungi, and protozoa
co-reside within specific niches created by structural and immune
cells, microbial symbionts, and spatial and biochemical factors,
where microbial cooperation is balanced by host systems. Symbiosis
may manifest in mutualistic, commensal, or antagonistic
relationships.
Already present prenatally respiratory microbiome is
further affected by birthing style, breastfeeding, childhood
antibiotic and antipyretic treatments, lifestyle, and many other
key factors, like living and crowding conditions, presence of
siblings, owning furry pets, etc.
With the age, the upper respiratory tract is
gradually and transiently colonized primarily by micro-aspiration
of typical resident bacterial, viral and fungal assemblages with
their distinct topography. Some direct dispersal via mucosa was
also demonstrated (7). In healthy
subjects, microbial ecosystems limit pathogens preventing their
overgrowth and spread (8).
Microbial ecosystems might be defined by characteristics, such as
healthy, infection-prone, pro-inflammatory, or others. The
knowledge behind these definitions is not yet sufficient.
The upper respiratory tract is the primary source of
the lower tract microbiome, i.e. lower airways and lungs are seeded
via the aspiration (9). The upper
respiratory tract microbiome is replenished from the environmental
microorganisms' populations and oral microflora (10). The microbiome in the lower airways
and lungs consists of transient microorganisms and its composition
is determined by the balance between microbial immigration and
elimination. New-generation sequencing enables detailed
characterization of previously unknown microbiomes, i.e., their
bacterial, viral, and fungal content (11). The size of the respiratory fungal
community, i.e. mycobiome, may comprise several percent of the
total microbiome as it does in the skin and gut (12). A bacterial portion of the
respiratory microbiome is the overwhelmingly dominating (13) and consists of varying proportions
of Firmicutes, Actinobacteria, Bacteroidetes,
Proteobacteria, and Fusobacteria representatives. Virome
represents a relatively small portion of the microbiome and differs
in healthy and inflammatory states. Bacteriophages comprise the
majority of the virome and modulate human respiratory health via
bacterial hosts. Complex inter-microbial and microbial-host
interactions ensure competence and maintenance clues to the immune
and respiratory systems. Accumulating data demonstrate a
possibility to improve that early in life when microbiota signaling
is essential for immune maturation and further respiratory health.
Ways to improve human respiratory microbiota and enhance
respiratory health are among the major interests of scientists and
clinicians worldwide.
Environmental factors and respiratory
microbiomes
Environmental elements conditioning human
microbiota, include air pollution, tobacco smoking, exposure to
secondhand smoke, and others. Smoking modifies human microbiomes
paving the way for diseases, like periodontitis, asthma, chronic
obstructive pulmonary disease (COPD), cancer, etc. Effects produced
by smoking include a direct influx of bacteria from the cigarettes,
impairment of the host's immune responses, and changes in oxidative
and proteolytic balance in the airways and alveoli. Indeed, oxygen
deprivation is an important factor for microaerophilic and
anaerobic bacteria enabling their dominance in the airways of
smokers (14). Moreover, the
smoking-induced effects might be correlated to COPD patients'
microbiota (2). Cigarettes harbor
microorganisms ranging from soil microorganisms and commensals to
potential human pathogens, capable of causing pneumonia,
bacteremia, and other infections (15).
Tobacco smoking is among the major factors
modulating human airway microbiota composition and participating in
disease development. Similarly, air pollution affects microbiomes
via chemical and physical effects and also via the influx of
airborne microorganisms. Particulate matter (PM)-associated
microbiome is dominated by bacteria, belonging to Actinobacteria
and Proteobacteria phyla. PM-bound viruses spike in January and
February (16). The level of
pollution does not correlate with the number of PM-associated
microorganisms, but the ambient temperature does. Seasonal and
indoor/outdoor variations are also described (17). The most prevalent microorganism is
Proteobacteria, followed by Bacteroidetes, Actinobacteria,
Cyanobacteria, and Firmicutes (18). Human pathogens were found in more
than 10% of PM samples. In addition, PM levels might be an
important factor in the spread of respiratory viruses. For
instance, among PM collected in Bergamo, Italy, during the
coronavirus outbreak more than half of the samples carried
SARS-CoV-2(19). Seasonal PM
microbial characteristics were studied by Italian scientists and
winter microbiota was dominated by the spore-forming bacteria,
while summer microbial composition differed and plant-associated
bacteria dominated (20). In
addition, the PM-associated microbiome composition correlates with
the human upper airway microbiome (21). Thus, the ambient air microbiome
serves as a reservoir to replenish the human airway microbiome.
Importantly, direct effects of air pollution on the human airway
microbiome include a decrease in Actinobacteria, which is known to
be associated with a healthy microbiome, and an increase in
Moraxella, which is a known respiratory pathogen (22). However, more studies are needed to
elucidate the exact effects of air pollution on the human
microbiomes of the exposed airways and lungs.
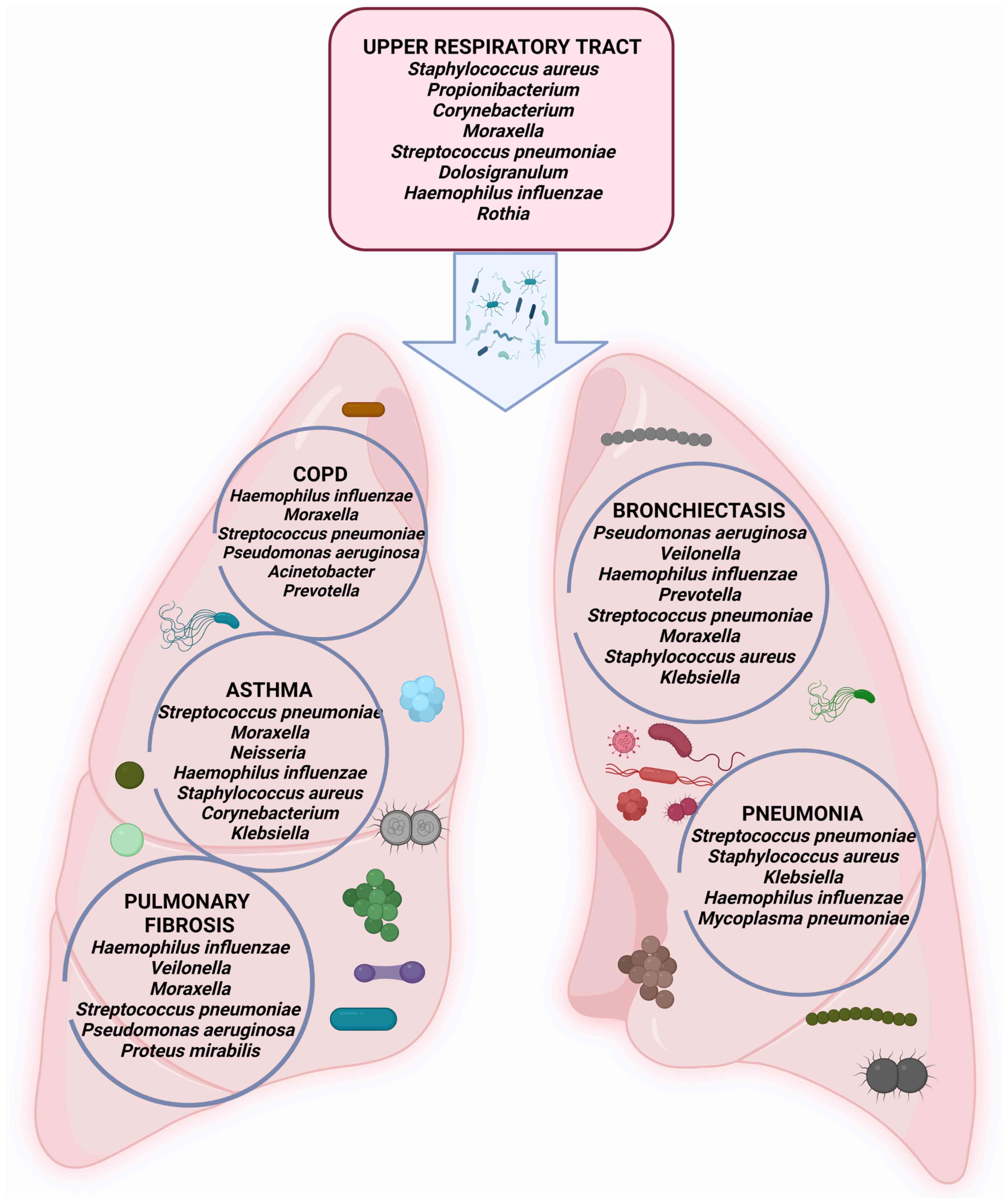
2. Bacteriome part of the respiratory
microbiome
Alterations of lung bacterial communities have been
associated with numerous lung diseases including COPD, bronchial
asthma (BA), bronchiectasis (BE), and others. Bacteria dominate
fungi and viruses with four phyla (Firmicutes, Proteobacteria,
Bacteroidetes, and Actinobacteria) making 97% of all sequences.
Homeostasis of respiratory tract-resident bacterial communities
depends on microbial immigration, mucosal dispersion, and
elimination. Patients with respiratory diseases often have
defective airway clearance, bacterial biofilms formed and resistant
microbial communities persisting through immune clearance and
antibiotics. Major players of the human respiratory bacteriome are
represented in Fig. 1.
Bacteriome and COPD
COPD is an umbrella term for several irreversible
chronic inflammatory diseases affecting airways and parenchyma.
Data show that the airway microbiome is implicated in COPD
manifestation, severity, and long-term prognosis. The
microbiome-based approaches for therapeutic interventions may be
needed.
The abundance and diversity of microbiota differ in
COPD and correlate with the disease severity (23). Moreover, exacerbations, persistent
inflammation, and antibiotic/steroid treatments impact the
composition of lung microbiota further. Multiple studies report
decreased microbial diversity and colonization by Haemophilus
influenzae, beta-lactamase-positive Haemophilus influenza,
Moraxella catarrhalis, and Streptococcus pneumonia in
COPD and Pseudomonas aeruginosa-in severe COPD (24).
Lung bacterial composition is associated with
respiratory function as demonstrated in the BALF study of
never-smokers and smokers with or without COPD. Severely decreased
respiratory function was associated with Veillonella,
Prevotella, and Streptococcus increase. However, such
an association between bacterial content and respiratory function
but not the disease itself supports the idea that lung bacteriome
shifts are part of the pathogenesis of many diseases, not only COPD
(25). In a sputum study
Proteobacteria, H. influenzae, M. catarrhalis
and P. aeruginosa together were named important players for
COPD exacerbations, and cooperation of the resident microorganisms
was demonstrated leading to enrichment for specific taxa (26). In lung explants, many separate,
distinct, and individual microbial communities were mapped
(27). COPD bacteriome varies not
only spatially but also in time. Many studies describe transitory
microbiota changes during exacerbations. For instance, stable COPD
sputum microbiota differs from exacerbated COPD (28). In COPD patients on ventilatory
support and antibiotics, bacterial communities differ significantly
and changes are treatment duration-dependent (29). In sum, some reports support the
existence of a distinct COPD microbiome while others show
overlapping healthy, smokers', and COPD microbiomes. It may be
explained by the heterogeneity of COPD, different study designs,
and small group sizes.
Bacteriome in bronchial asthma
Bronchial asthma is a heterogeneous chronic
inflammatory airway disease characterized by bronchial
hyperactivity and obstruction. It is increasingly accepted that
microbiota plays an important role in disease etiology and
development. Decreased bacterial diversity is detected in BA and
correlates with the disease severity (30). Certain bacteria might be associated
with bronchial hyperactivity and obstruction, i.e.,
Proteobacteria, Firmicutes (Streptococci), and
Gammaproteobacteria (31).
Respiratory commensals Veillonella and Prevotella
were less prevalent. Haemophilus influenzae, Streptococcus
pneumoniae, and Moraxella catarrhalis have been found in
the lower and upper respiratory tract of children during asthma
crises (32).
Although respiratory infections may not be the
crucial triggers in BA, specific bacterial-host interactions may
significantly increase the risk of BA exacerbations (33). Moreover, the differences in nasal
bacteriome may serve as indicators of different BA phenotypes
(34). Furthermore, the risk to
develop BA is microbiome-related according to the pediatric study
(35). Further microbiome studies
of BA patients are needed to open new insights, suggest
microbiome-based biomarkers of the disease, and design better
treatment options.
Bacteriome in bronchiectasis
Bronchiectasis (BE) is a disease of permanent
abnormal bronchial dilation, infection, and inflammation. P.
aeruginosa and H. influenzae are the most common
pathogens in BE (36).
Pseudomonas dominant patients have poor clinical outcomes,
worse lung function, and require recurrent antibiotic treatments
(37). Other important bacteria
are Prevotella spp., Str. pneumoniae, nontuberculous
mycobacteria, Moraxella catarrhalis, S. aureus,
Escherichia, and Klebsiella spp. (38). Culture-independent methods
corroborated the findings of traditional culture-based methods.
Interestingly, the frequency of bacteria varies geographically,
H. influenza and P. aeruginosa are more prevalent in
Europe and Asia, while Mycobacterium avium, M. abscessus,
M. chelonae, and P. aeruginosa are more common in the US
(39,40).
It is known that BE exacerbations occur in less
complex microbial co-occurrence networks, and reduced diversity,
where a higher degree of antagonism exists. Microbial antagonism
deepens during exacerbations and interactions, but not the
abundance of certain microbial groups defines the risk of
exacerbations (41).
However, BE microbiome is little understood and
requires further studies to clarify the development and progression
of the disease.
Bacteriome and pulmonary fibrosis
Pulmonary fibrosis (PF) is a progressive alveolar
fibrosis with inflammatory infiltration. Genetics, autoimmunity,
certain medicines, toxic agents, and ionizing radiation contribute
to PF development. The importance of respiratory microbiome is
among the risk factors for PF. Haemophilus influenzae, Moraxella
catarrhalis, Streptococcus pneumoniae, Haemophilus parainfluenza,
Pseudomonas aeruginosa, and Proteus mirabilis were
detected in PF patients (42).
Microbiome findings are insufficient to explain the pathogenesis of
the disease but might serve as a source of the disease biomarkers.
When compared to other diseases, bacterial abundance in PF patients
was significantly higher than in COPD or healthy controls (43). Exacerbated PF was related to a
four-fold higher bacterial burden, with an increase in
Campylobacter and Stenotrophomonas and a decrease in
Veillonella (44).
Microbiota and fibrosis have a bidirectional
relationship, i.e. fibrosis impairs microbial clearance and blunts
innate immune responses (45),
while bacterial products directly promote fibrosis. For instance,
staphylococci release a peptide corisin and induce apoptosis of
lung epithelial cells. PF is detected in the lungs of
corisin-exposed mice. Moreover, lung corisin levels are
significantly increased in PF patients with acute exacerbation
compared to stable PF (46). Such
dual interrelationships should be considered when designing
treatment strategies. Equally important is to consider microbiome
composition and richness as a reflection of the fibrotic state of
the host lung tissue and a possibility to target the microbiome for
the diagnostics and management of the disease.
Bacteriome and acute respiratory
infections and pneumonia
Upper airways are the first line of defense
constantly exposed to various environmental and host factors which
contribute to, shape, damage, and replenish airway microbiota.
Specific local conditions, like secretions, mucus flow, and air
circulation, are important determinants of bacterial colonization.
Bacteria reside in patch-type populations and are dependent on
migration, dispersal, colonization, extinction, and transition of
the incoming and resident bacteria, e.g. the ability of S.
aureus to invade populations dominated by Str.
pneumoniae is limited, while other species may invade (47). Disease states in the upper airways
correlate with microbiome shifts, especially it's virome part.
However, bacteriome remains an important factor in all infectious
and noninfectious diseases of the upper airways and other
organs.
Pneumonia is an acute respiratory infection of the
alveoli and distal airways and remains a major cause of high
morbidity and mortality worldwide. Various microorganisms can cause
pneumonia, including bacteria, viruses, and fungi, also members of
healthy lung microbiota. Pneumonia manifests with the rapid shift
from a healthy microbiome to dysbiosis where low diversity, high
pathogen burden, and inflammation of host tissues dominate.
Pathogenetic mechanisms behind this shift include environmental
exposure, like tobacco smoke or air pollution, mechanical
ventilation, direct and indirect interactions between
microorganisms, etc. Pneumonia appears as the major complication of
the dysbiosis of the lungs. Culture-independent detection methods
have proved that a healthy lower respiratory tract accommodates
various microbes without induction of any symptoms of
infection.
Nasopharyngeal samples, collected during the
infection episodes, show the presence of Moraxella, Haemophilus
and Streptococcus, Corynebacterium, Dolosigranulum, Staphylococcus,
Acinetobacter, Pseudomonas, and Bifidobacterium
(48). Bacteriome's role in
disease onset, progression, and therapeutic response is undisputed
although the major pathogens are viruses. New studies have shown
the connection between the lung microbiome and the pathogenesis of
pneumonia. Typical pneumonia pathogens include Streptococcus
pneumoniae, Staphylococcus aureus, Klebsiella pneumoniae,
Haemophilus influenzae, also Mycoplasma pneumoniae, Legionella
pneumophilia, and Chlamydophila psittaci. The potential
pathogens often are residents within the microbial ecosystem in the
lower airways. Certain combinations might be associated with more
severe pneumonia or oppositely, disease resistance. For instance,
the Prevotella-rich microbiome supports inflammation and
increases mortality, while Pseudomonas species support
disease-resistant lung microbiome and suppression of pathogens
(49).
The upper airways' microbiome replenishes the
microbiome of the lower airways and has direct implications for
pneumonia. Pneumonia was not only associated with dysbiosis in the
nose but also with bacterial overgrowth of single species and the
absence of distinct anaerobic bacteria. Also, less rich microbiomes
might be associated with the susceptibility to inflammation. It is
becoming increasingly clear that pneumonia is a multifactorial
disease where pathogenic bacteria are only partially responsible,
and the entire human microbiome and host factors are also
implicated.
3. Human respiratory mycobiome
Culture-independent detection methods prove that
human airways and lungs contain fungi as an integral part of their
microbiomes. Mycobiome is a diverse array of fungal species
residing within a specific body space. Inhalation of spores and
complex interaction with the bacterial and host systems are
determining factors for fungal entrance, dispersion, and growth in
the airways and lungs (50). Fungi
contain so-called pathogen-associated molecular patterns, like
glucans, chitin, and mannans, able to trigger immune responses in
the respiratory epithelium (51).
Fungal overgrowth in the human airways has been linked to many
chronic diseases (52). Fungal
communities also have systemic effects executed via biologically
active molecules (53).
Studies of the inter-kingdom relationships between
bacteriomes and mycobiomes show that Aspergillus and
Malassezia might be associated with exacerbations of cystic
fibrosis (CF), while Scedosporium and Pseudomonas-
with the decline of lung function (50). In addition, simultaneous assessment
of mycobiome and bacteriome revealed fungus-to-bacteria diversity
10 times higher in lungs in comparison to the gut, supporting the
notion that lung mycobiome is replenished differently, most likely
via spore inhalation. The complex interaction between members of
different kingdoms is realized via cross-feeding, specialized
metabolites, and other mechanisms.
In CF Aspergillus fumigatus colonization
correlates with lower lung capacity, more frequent
hospitalizations, and more prominent radiological abnormalities
(54). Indeed, fungal
complications in CF patients are mostly caused by filamentous
fungi. Mycobiome is an important etiological component not only in
CF but also in other pulmonary diseases, like COPD. Implications of
the fungi in COPD development were studied in patients from
Singapore, Malaysia, and Scotland (55). The airway mycobiome in stable COPD
was diverse and dependent on geography. Distinct genera, i.e.
Alternaria, Aspergillus, Cladosporium, Cryptococcus,
Mycosphaerella, Penicillium, Trametes, and
Wickerhamomyces, were found in COPD lungs but not in the
healthy lungs. Importantly, no differences between mycobiome
profiles were detected between patients with COPD and patients with
BE and COPD overlap. Clustering analysis revealed that increased
exacerbation rate and higher mortality might be characterized by
microbiome enrichment with Aspergillus, Penicillium, and
Curvularia genera. In these patients systemic specific-IgE
responses to the fungi were detectable. In addition, loss of fungal
diversity was associated with increased two-year mortality in
COPD.
Inter-microbiome relationships define fungal
presence, e.g., human intestinal microbiome data demonstrate that
affecting bacterial communities will significantly impact fungal
species and vice versa (56).
Similar relationships were detected in other microbiomes suggesting
that respiratory microbiomes are not an exception. Disruption of
airway bacterial-fungal balance, characterized by the loss of
commensal bacterial taxa and by the enrichment of pathogenic fungal
taxa, is implicated in COPD, i.e., Prevotella and
Veillonella exhibit inverse relationships with pathogenic
fungal taxa such as Candida palmioleophila and
Aspergillus spp. (57). In
a respiratory tract mycobiome study of HIV patients with and
without COPD, oral washes, sputum, and BALF were analyzed, and 39
fungal species were more abundant in the BALF and 203 species-in
the sputum, proving species-specific distribution. The primary
fungus enriched in the lungs of individuals with HIV and COPD was
Pneumocystis.
The role of the mycobiome in BE was investigated and
Aspergillus, Cryptococcus, Clavispora, Botrytis, and
Alternaria genera were identified (58). In the other study, healthy
individuals had no detectable airway Aspergillus, while high
proportions of BE patients had detectable A. fumigatus
and/or A. terreus. Indeed, A. fumigatus followed by
Aspergillus niger, Aspergillus terreus, and
Aspergillus flavus is the most common in BE (59).
In sum, fungal genera within respiratory microbiomes
are low in diversity, individually shaped, linked to gut mycobiome,
and play a significant role in the decline of lung functions and
disease progression.
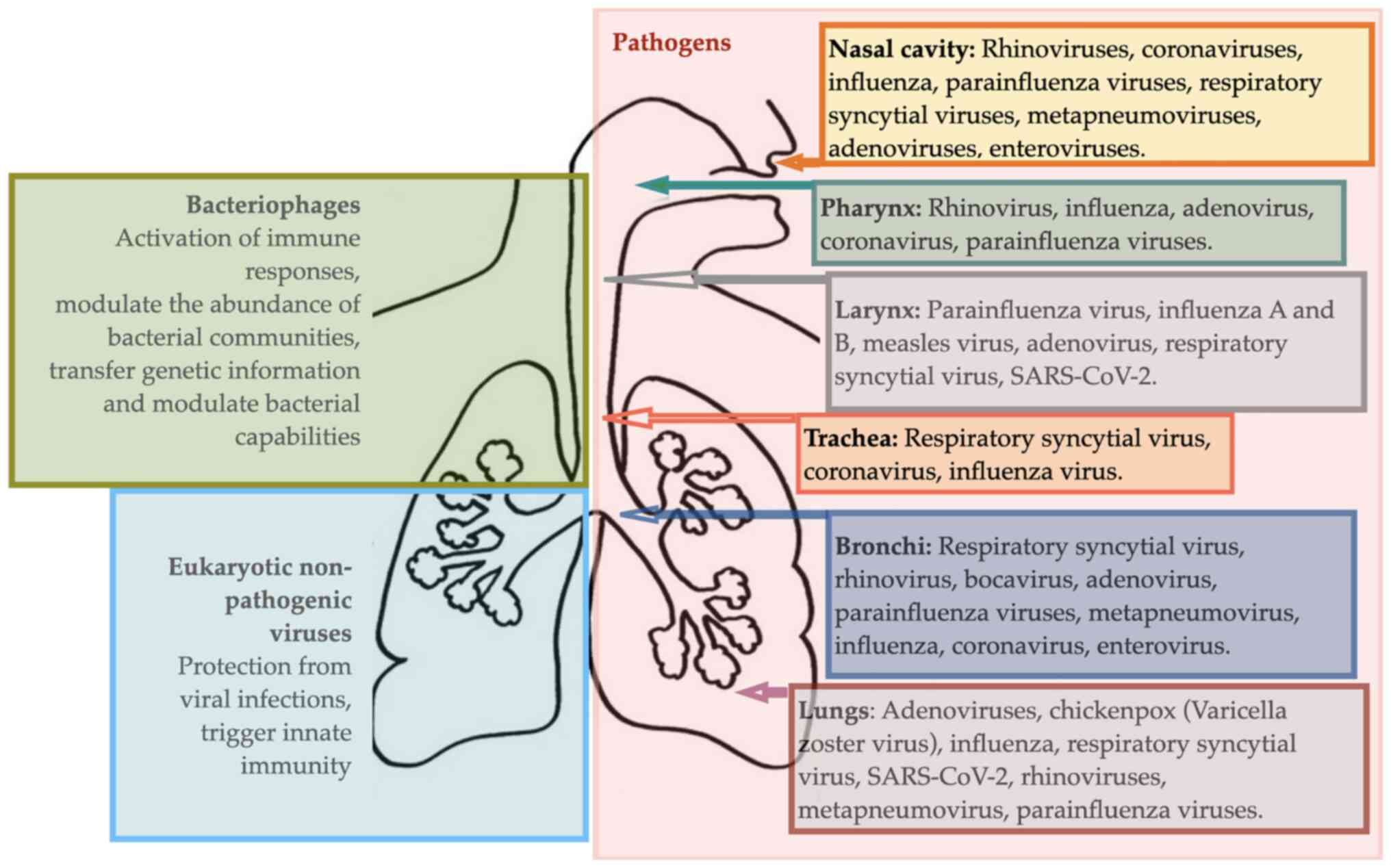
4. Human respiratory virome
The previous view of viruses being obligate
pathogens is changed. The human virome is a part of the microbiome
and includes pathogenic viruses, resident viruses, bacteriophages,
and retroviral elements. Novel detection methods revealed viral
genetic diversity and new viruses present in humans. The prevalence
of respiratory viruses among asymptomatic children is documented,
including rhinoviruses, bocaviruses, and coronaviruses (60). However, the roles of these viruses
in asymptomatic individuals are still unclear. Bacteriophages make
a major part of the virome. They intervene in human health by
regulating the prevalence of bacteria.
Human airways and lungs are the major sources of
viral infection-related mortality worldwide. The recent
coronavirus-caused disease 2019 (COVID-19) outbreak was a unique
pandemic due to the combination of a high reproducibility,
super-spreading, and global immunologically naïve population. It
has led to the highest global number of deaths in the past 20
decades compared to any other pandemic. An overview of respiratory
viral diseases is provided in Fig.
2.
Viral infections of upper airways
High morbidity and mortality associated with viral
infections are partially related to complicated diagnostics since
viral infections often do not produce detectable lesions. Novel
detection techniques are needed. Moreover, some viral infections
can cause a cascade of destructive processes and swiftly disappear,
like influenza. At the host level, viral infections affect the
epithelium, phagocytes, T lymphocytes, and macrophages, support
adherence of bacteria to the epithelium, up-regulate inflammatory
mediators and change the extracellular environment and microbiota.
The impact of viruses on the development of noninfectious, chronic
pulmonary diseases such as BA and COPD is also well-known (61).
Viral infections of the upper respiratory tract are
a group of diseases mainly caused by viruses entering the organism
via inhalation of droplets, later invading the mucosa, and damaging
epithelium in the upper airways.
The common cold is the most common disease with more
than 200 different viruses, differently active during summer and
wintertime, as causative factors. Rhinoviruses are the most common
pathogens. Other pathogens include coronaviruses, influenza,
parainfluenza, respiratory syncytial viruses, and many others
(62). People with weakened immune
systems and respiratory or cardiac diseases are at higher risk of
developing severe viral infections and complications. The role of
microbiota in common cold is dual, i.e., invading viruses may
initiate secondary local bacteria-caused infections, while local
dysbiosis could cause impairment of epithelium and predispose an
individual to the viral infection. Interventions targeting
microbiota are among preventative and treatment strategies for
combating common colds. Exposure to environmental (pollution, cold,
dry air), microbial and other factors, such as medications
(antibiotics and similar), damages airway microbiota and is
associated with more prevalent and more severe common colds. It is
becoming clear that viral infections may be prevented or
ameliorated via supporting resilient local microbiomes (48). Knowledge of microbiome resiliency,
microbial competition, and interactions within the microbiota are
needed to develop probiotic solutions.
Sinusitis is an infectious inflammation within the
sinuses that become inflamed and blocked by mucus. Rhinoviruses,
influenza, and parainfluenza viruses are the most common causes of
sinusitis (63). Microbiota's role
in the onset and development of sinusitis has recently gained
attention. Sinus and nasal microbiota is a source of pathogens but
also serve as a protection against infection. In health, bacteria,
including S. aureus, Str. epidermidis and
Corynebacterium genera, reside in sinuses. Disruptions in
this balance, like an increase in S. aureus
concentration, may perpetuate inflammatory changes within the nasal
mucosa, leading to sinusitis.
Human respiratory microbiome and
Coronavirus-caused Disease 2019
In the course of COVID-19 microbiota contributes
directly. It is known that dysbiosis leads to epithelial cell loss,
an increase in permeability, and inflammation, thus to the
increasing levels of angiotensin-converting enzyme 2 (ACE2), the
target of coronavirus (64).
Moreover, dysbiosis may trigger an increase in circulating
inflammatory mediators (65) and
self-perpetuating pro-inflammatory cytokine production, i.e.
cytokine storm. Reduced microbiome diversity may be regarded as a
predictive biomarker of COVID-19 severity (66). Respiratory microbiota has a
distinct role in COVID-19 course and severity also due to bacterial
co-infections often arising from resident bacterial communities
(67). Study authors have explored
the microbiome of COVID-19 patients and demonstrated gut microbiome
of COVID-19 patients has a significant reduction of bacterial
diversity and a significantly higher relative abundance of
opportunistic pathogens and less beneficial symbionts as compared
to the control group. Several gut commensals with known modulatory
potential, like Faecalibacterium prausnitzii, Eubacterium
rectale, and bifidobacteria, were underrepresented in
COVID-19 patients and remained low up to 30 days after COVID-19
resolution. Additionally, butyrate-producing bacteria such as
Faecalibacterium prausnitzii, Clostridium butyricum,
Clostridium leptum, and Eubacterium were less
abundant. Moreover, depletion of commensals, like Eubacterium
ventriosum, Faecalibacterium prausnitzii, and others,
correlated with COVID-19 severity. The respiratory microbiome of
COVID-19 patients was studied in bronchoalveolar lavage fluid
(BALF) and compared to pneumonia patients and healthy controls.
Both, COVID-19 and community-acquired pneumonia patients had
enrichment of pathogenic and commensal bacteria, indicating a
significant dysbiosis (68). The
post-mortem biopsies exhibited mixed bacterial and fungal
infections complicating COVID-19(69).
Overall, further studies with a bigger sample size
are required to clarify the composition and the role of the
respiratory microbiome in the severity of coronavirus
infections.
Viral infections of the lower
airways
Viral infections of the lower airways include
laryngotracheitis, bronchitis, bronchiolitis, and pneumonia which
are all more common in children. Often infections involve both the
upper and lower respiratory tract. Respiratory infections in the
lower airways and lungs may be caused by more than 200 types of
viruses.
Healthy lower airways are inhabited by specific
microbial ecosystems. They are accessed and investigated using
modern molecular techniques combined with bronchoscopy, biopsies,
post-mortem tissue analysis, and some others, although precise
detection techniques ensuring no compromising, overlapping, or
contamination are still lacking.
Viral lower airway infections manifest with cough
and difficulty breathing. Parainfluenza virus accounts for more
than 75% of these infections (70)
and the cause of the disease is a virus in 90% of all cases
(71). In addition, distinct
dysbiotic signatures are identified, viral infection-prone
microbiomes are described and metatranscriptome data reveals an
association between disease severity and microbiome (72).
Pneumonia is an infectious inflammatory condition
affecting lung parenchyma and impairing its major function, i.e.
gas exchange. The main causative agents of pneumonia vary, i.e. may
include bacteria, fungi, parasites, and viruses. Community-acquired
pneumonia remains a major cause of morbidity and mortality
worldwide. Viral pathogens are increasingly often implicated due to
pneumococcal vaccination programs, sensitive diagnostic tests, and
other factors. Non-influenza viral pathogens include rhinovirus,
metapneumovirus, respiratory syncytial virus, parainfluenza virus,
and adenoviruses.
Chronic non-infectious respiratory
diseases and viruses
In chronic inflammatory respiratory diseases, like
BA, respiratory viruses are among the major pathogenetic factors of
exacerbation and progression. Viral infections were often
under-recognized as causes of exacerbations due to the low
detection rates (73). Applying
molecular detection techniques viruses were detected in nearly 40%
of COPD exacerbations (74) and
nearly 60% of the CF exacerbations (75). The progression of chronic pulmonary
disease and it's exacerbations are increasingly linked to
respiratory viruses nowadays mainly due to modern diagnostic
techniques. Host responses in these diseases are imbalanced and
microbiomes are often shifted. Understanding microbiota and host
interplay in chronic pulmonary diseases stimulate the development
of new therapies for virus-related exacerbations.
5. Concluding remarks
It is still not clear whether the respiratory
disease state might be estimated based on microbiome biomarkers.
However, in some diseases, like bronchiectasis, microbiome analysis
may be used as a diagnostic tool. Translation of human airway
microbiome-associated extensive research data and experience into
the clinical practice and introduction of a diagnostic ‘microbiome
test’ is imminent. We predict a substantial improvement in the
diagnostics and management of certain diseases, like COPD, when
airway and lung microbiome data will be made readily available to
clinicians and patients.
Two directional relationships are observed between
microbial ecosystems and host susceptibility to infectious and
other diseases, i.e. microbiomes may serve as the source of
infection-causing pathogens, and at the same time invading
pathogens modulate the host's microbial communities for long
periods of time.
As discussed above, the environmental insults
predispose not only hosts' tissues but also human microbiota to the
disease development by changing microbial composition and also a
state of the host's immunity, epithelial integrity, and other
factors. We believe that improvements to the human respiratory
microbiome, i.e. replenishing and promoting certain species, are
possible by exposing humans to rich and healthy ambient air
microbiomes (e.g. forest microbiome) and may become a central
therapeutic strategy for some diseases.
Although bacteriome, virome, and mycobiome are
important components of respiratory microbiomes and play role in
the pathogenesis of many diseases, they are differentially
weighted, and certain players, like viruses or filamentous fungi,
may be regarded as major pathogens in certain diseases.
Acknowledgements
Not applicable.
Funding
Funding: This work was supported by a grant (grant no.
#01.2.2-LMT-K-718-03-0079) from the Lithuanian Research
Council.
Availability of data and materials
Not applicable.
Authors' contributions
JR drafted the bacteriome part of the review and
Fig. 1. DB drafted the virome part
of the review and Fig. 2. EB
drafted the mycobiome part of the manuscript. IK drafted the
introductory part of the review. BJ and ED edited and revised the
manuscript. RA was a major contributor in compiling and editing the
entire manuscript and figures. Data authentication is not
applicable. All authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Human Microbiome Project Consortium.
Structure, function and diversity of the healthy human microbiome.
Nature. 486:207–214. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Dy R and Sethi S: The lung microbiome and
exacerbations of COPD. Curr Opin Pulm Med. 22:196–202.
2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Owyang C and Wu GD: The gut microbiome in
health and disease. Gastroenterology. 146:1433–1436. 2014.
|
|
4
|
Zheng J, Wu Q, Zou Y, Wang M, He L and Guo
S: Respiratory microbiota profiles associated with the progression
from airway inflammation to remodeling in mice with OVA-induced
asthma. Front Microbiol. 12(723152)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Littman DR and Pamer EG: Role of the
commensal microbiota in normal and pathogenic host immune
responses. Cell Host Microbe. 10:311–323. 2011.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Fukuyama S, Hiroi T, Yokota Y, Rennert PD,
Yanagita M, Kinoshita N, Terawaki S, Shikina T, Yamamoto M, Kurono
Y and Kiyono H: Initiation of NALT organogenesis is independent of
the IL-7R, LTbetaR, and NIK signaling pathways but requires the Id2
gene and CD3(-)CD4(+)CD45(+) cells. Immunity. 17:31–40.
2002.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Dickson RP, Erb-Downward JR, Freeman CM,
McCloskey L, Falkowski NR, Huffnagle GB and Curtis JL: Bacterial
topography of the healthy human lower respiratory tract. mBio.
8:e02287–16. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Man WH, de Steenhuijsen Piters WA and
Bogaert D: The microbiota of the respiratory tract: Gatekeeper to
respiratory health. Nat Rev Microbiol. 15:259–270. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Gleeson K, Eggli DF and Maxwell SL:
Quantitative aspiration during sleep in normal subjects. Chest.
111:1266–1272. 1997.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Segal LN, Alekseyenko AV, Clemente JC,
Kulkarni R, Wu B, Gao Z, Chen H, Berger KI, Goldring RM, Rom WN, et
al: Enrichment of lung microbiome with supraglottic taxa is
associated with increased pulmonary inflammation. Microbiome.
1(19)2013.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Eidi S, Kamali SA, Hajari Z, Fata A, Farid
Hosseini R, Naseri A and Bakhshaee M: Nasal and indoors fungal
contamination in healthy subjects. Health Scope. 5(e30033)2016.
|
|
12
|
Qin J, Li R, Raes J, Arumugam M, Burgdorf
KS, Manichanh C, Nielsen T, Pons N, Levenez F, Yamada T, et al: A
human gut microbial gene catalogue established by metagenomic
sequencing. Nature. 464:59–65. 2010.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Dai W, Wang H, Zhou Q, Li D, Feng X, Yang
Z, Wang W, Qiu C, Lu Z, Xu X, et al: An integrated respiratory
microbial gene catalogue to better understand the microbial
aetiology of Mycoplasma pneumoniae pneumonia. Gigascience.
8(giz093)2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Mason MR, Preshaw PM, Nagaraja HN, Dabdoub
SM, Rahman A and Kumar PS: The subgingival microbiome of clinically
healthy current and never smokers. ISME J. 9:268–272.
2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sapkota AR, Berger S and Vogel TM: Human
pathogens abundant in the bacterial metagenome of cigarettes.
Environ Health Perspect. 118:351–356. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Qin N, Liang P, Wu C, Wang G, Xu Q, Xiong
X, Wang T, Zolfo M, Segata N, Qin H, et al: Longitudinal survey of
microbiome associated with particulate matter in a megacity. Genome
Biol. 21(55)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Pereira EL, Madacussengua O, Baptista P
and Feliciano M: Assessment of indoor air quality in geriatric
environments of Southwestern Europe. Aerobiologia. 37:139–153.
2021.
|
|
18
|
Dong SR, Han YJ, Wu J, Zeng CL, Zhu KH,
Chen XJ, Liu YM, Zou XQ, Zheng SL, Wen ZH, et al: Distribution of
microbiota in fine particulate matter particles in Guangzhou,
China. Biomed Environ Sci. 33:306–314. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Setti L, Passarini F, De Gennaro G,
Barbieri P, Perrone MG, Borelli M, Palmisani J, Di Gilio A, Torboli
V, Fontana F, et al: SARS-Cov-2RNA found on particulate matter of
Bergamo in Northern Italy: First evidence. Environ Res.
188(109754)2020.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Brodie EL, DeSantis TZ, Parker JP,
Zubietta IX, Piceno YM and Andersen GL: Urban aerosols harbor
diverse and dynamic bacterial populations. Proc Natl Acad Sci USA.
104:299–304. 2007.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Biswas K, Hoggard M, Jain R, Taylor MW and
Douglas RG: The nasal microbiota in health and disease: Variation
within and between subjects. Front Microbiol. 9(134)2015.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mariani J, Favero C, Spinazzè A, Cavallo
DM, Carugno M, Motta V, Bonzini M, Cattaneo A, Pesatori AC and
Bollati V: Short-term particulate matter exposure influences nasal
microbiota in a population of healthy subjects. Environ Res.
162:119–126. 2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Ghebre MA, Pang PH, Diver S, Desai D,
Bafadhel M, Haldar K, Kebadze T, Cohen S, Newbold P, Rapley L, et
al: Biological exacerbation clusters demonstrate asthma and chronic
obstructive pulmonary disease overlap with distinct mediator and
microbiome profiles. J Allergy Clin Immunol. 141:2027–2036.e12.
2018.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Dima E, Kyriakoudi A, Kaponi M,
Vasileiadis I, Stamou P, Koutsoukou A, Koulouris NG and Rovina N:
The lung microbiome dynamics between stability and exacerbation in
chronic obstructive pulmonary disease (COPD): Current perspectives.
Respir Med. 157:1–6. 2019.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Opron K, Begley LA, Erb-Downward JR,
Freeman C, Madapoosi S, Alexis NE, Barjaktarevic I, Graham Barr R,
Bleecker ER, Bowler RP, et al: Lung microbiota associations with
clinical features of COPD in the SPIROMICS cohort. NPJ Biofilms
Microbiomes. 7(14)2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Huang YJ, Sethi S, Murphy T, Nariya S,
Boushey HA and Lynch SV: Airway microbiome dynamics in
exacerbations of chronic obstructive pulmonary disease. J Clin
Microbiol. 52:2813–2823. 2014.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Erb-Downward JR, Thompson DL, Han MK,
Freeman CM, McCloskey L, Schmidt LA, Young VB, Toews GB, Curtis JL,
Sundaram B, et al: Analysis of the lung microbiome in the ‘healthy’
smoker and in COPD. PLoS One. 6(e16384)2011.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Tangedal S, Nielsen R, Aanerud M, Persson
LJ, Wiker HG, Bakke PS, Hiemstra PS and Eagan TM: Sputum microbiota
and inflammation at stable state and during exacerbations in a
cohort of chronic obstructive pulmonary disease (COPD) patients.
PLoS One. 14(e0222449)2019.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Huang WC, Wu MF and Huang CC, Liu SY, Chen
HC, Chen YY, Hsu JY and Huang CC: Dynamics of the lung microbiome
in intensive care patients with chronic obstructive pulmonary
disease and community-acquired pneumonia. Sci Rep.
10(11046)2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Huang YJ, Nariya S, Harris JM, Lynch SV,
Choy DF, Arron JR and Boushey H: The airway microbiome in patients
with severe asthma: Associations with disease features and
severity. J Allergy Clin Immunol. 136:874–884. 2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Hilty M, Burke C, Pedro H, Cardenas P,
Bush A, Bossley C, Davies J, Ervine A, Poulter L, Pachter L, et al:
Disordered microbial communities in asthmatic airways. PLoS One.
5(e8578)2010.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kloepfer KM, Lee WM, Pappas TE, Kang TJ,
Vrtis RF, Evans MD, Gangnon RE, Bochkov YA, Jackson DJ, Lemanske RF
Jr and Gern JE: Detection of pathogenic bacteria during rhinovirus
infection is associated with increased respiratory symptoms and
asthma exacerbations. J Allergy Clin Immunol. 133:1301–1307.e3.
2014.PubMed/NCBI View Article : Google Scholar
|
|
33
|
McCauley KE, Flynn K, Calatroni A, DiMassa
V, LaMere B, Fadrosh DW, Lynch KV, Gill MA, Pongracic JA, Khurana
Hershey GK, et al: Seasonal airway microbiome and transcriptome
interactions promote childhood asthma exacerbations. J Allergy Clin
Immunol. 150:204–213. 2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Perez-Losada M, Authelet KJ, Hoptay CE,
Kwak C, Crandall KA and Freishtat RJ: Pediatric asthma comprises
different phenotypic clusters with unique nasal microbiotas.
Microbiome. 6(179)2018.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Teo SM, Tang HHF, Mok D, Judd LM, Watts
SC, Pham K, Holt BJ, Kusel M, Serralha M, Troy N, et al: Airway
microbiota dynamics uncover a critical window for interplay of
pathogenic bacteria and allergy in childhood respiratory disease.
Cell Host Microbe. 24:341–352.e5. 2018.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Rogers GB, Zain NM, Bruce KD, Burr LD,
Chen AC, Rivett DW, McGuckin MA and Serisier DJ: A novel microbiota
stratification system predicts future exacerbations in
bronchiectasis. Ann Am Thorac Soc. 11:496–503. 2014.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Araújo D, Shteinberg M, Aliberti S,
Goeminne PC, Hill AT, Fardon TC, Obradovic D, Stone G, Trautmann M,
Davis A, et al: The independent contribution of Pseudomonas
aeruginosa infection to long-term clinical outcomes in
bronchiectasis. Eur Respir J. 51(1701953)2018.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Amati F, Simonetta E, Gramegna A, Tarsia
P, Contarini M, Blasi F and Aliberti S: The biology of pulmonary
exacerbations in bronchiectasis. Eur Respir Rev.
28(190055)2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Aksamit TR, O'Donnell AE, Barker A,
Olivier KN, Winthrop KL, Daniels MLA, Johnson M, Eden E, Griffith
D, Knowles M, et al: Adult patients with bronchiectasis: A first
look at the US bronchiectasis research registry. Chest.
151:982–992. 2017.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Guan WJ, Gao YH, Xu G, Lin ZY, Tang Y, Li
HM, Lin ZM, Zheng JP, Chen RC and Zhong NS: Aetiology of
bronchiectasis in Guangzhou, Southern China. Respirology.
20:739–748. 2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Mac Aogain M, Narayana JK, Tiew PY, Ali
NABM, Yong VFL, Jaggi TK, Lim AYH, Keir HR, Dicker AJ, Thng KX, et
al: Integrative microbiomics in bronchiectasis exacerbations. Nat
Med. 27:688–699. 2021.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Richter AG, Stockley RA, Harper L and
Thickett DR: Pulmonary infection in Wegener granulomatosis and
idiopathic pulmonary fibrosis. Thorax. 64:692–697. 2009.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Molyneaux PL, Cox MJ, Willis-Owen SA,
Mallia P, Russell KE, Russell AM, Murphy E, Johnston SL, Schwartz
DA, Wells AU, et al: The role of bacteria in the pathogenesis and
progression of idiopathic pulmonary fibrosis. Am J Respir Crit Care
Med. 190:906–913. 2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Molyneaux PL, Cox MJ, Wells AU, Kim HC, Ji
W, Cookson WO, Moffatt MF, Kim DS and Maher TM: Changes in the
respiratory microbiome during acute exacerbations of idiopathic
pulmonary fibrosis. Respir Res. 18(29)2017.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Warheit-Niemi HI, Edwards SJ, SenGupta S,
Parent CA, Zhou X, O'Dwyer DN and Moore BB: Fibrotic lung disease
inhibits immune responses to staphylococcal pneumonia via impaired
neutrophil and macrophage function. JCI Insight.
7(e152690)2022.PubMed/NCBI View Article : Google Scholar
|
|
46
|
D'Alessandro-Gabazza CN, Kobayashi T,
Yasuma T, Toda M, Kim H, Fujimoto H, Hataji O, Takeshita A,
Nishihama K, Okano T, et al: A Staphylococcus pro-apoptotic peptide
induces acute exacerbation of pulmonary fibrosis. Nat Commun.
11(1539)2020.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Cremers AJ, Zomer AL, Gritzfeld JF,
Ferwerda G, van Hijum SA, Ferreira DM, Shak JR, Klugman KP,
Boekhorst J, Timmerman HM, et al: The adult nasopharyngeal
microbiome as a determinant of pneumococcal acquisition.
Microbiome. 2(44)2014.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Chonmaitree T, Jennings K, Golovko G,
Khanipov K, Pimenova M, Patel JA, McCormick DP, Loeffelholz MJ and
Fofanov Y: Nasopharyngeal microbiota in infants and changes during
viral upper respiratory tract infection and acute otitis media.
PLoS One. 12(e0180630)2017.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Wu BG and Segal LN: The lung microbiome
and its role in Pneumonia. Clin Chest Med. 39:677–689.
2018.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Soret P, Vandenborght LE, Francis F, Coron
N, Enaud R, Avalos M, Schaeverbeke T, Berger P, Fayon M, Thiebaut
R, et al: Respiratory mycobiome and suggestion of inter-Kingdom
network during acute pulmonary exacerbation in cystic fibrosis. Sci
Rep. 10(3589)2020.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Tipton L, Ghedin E and Morris A: The lung
mycobiome in the next-generation sequencing era. Virulence.
8:334–341. 2017.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Weaver D, Gago S, Bromley M and Bowyer P:
The human lung mycobiome in chronic respiratory disease:
Limitations of methods and our current understanding. Curr Fungal
Infect Rep. 13:109–119. 2019.
|
|
53
|
Runge S and Rosshart SP: The mammalian
metaorganism: A holistic view on how microbes of all Kingdoms and
niches shape local and systemic immunity. Front Immunol.
12(702378)2021.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Speirs JJ, van der Ent CK and Beekman JM:
Effects of Aspergillus fumigatus colonization on lung function in
cystic fibrosis. Curr Opin Pulm Med. 18:632–638. 2012.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Tiew PY, Dicker AJ, Keir HR, Poh ME, Pang
SL, Mac Aogáin M, Chua BQY, Tan JL, Xu H, Koh MS, et al: A
high-risk airway mycobiome is associated with frequent exacerbation
and mortality in COPD. Eur Respir J. 57(2002050)2021.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Sovran B, Planchais J, Jegou S, Straube M,
Lamas B, Natividad JM, Agus A, Dupraz L, Glodt J, Da Costa G, et
al: Enterobacteriaceae are essential for the modulation of colitis
severity by fungi. Microbiome. 6(152)2018.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Liu H, Liang Z, Cao N, Tan X, Liu Z, Wang
F, Yang Y, Li C, He Y, Su J, et al: Airway bacterial and fungal
microbiome in chronic obstructive pulmonary disease. bioRxiv. 2020:
2020.10.05.327536.
|
|
58
|
Mac Aogáin M, Chandrasekaran R, Lim AYH,
Low TB, Tan GL, Hassan T, Ong TH, Hui Qi Ng A, Bertrand D, Koh JY,
et al: Immunological corollary of the pulmonary mycobiome in
bronchiectasis: The CAMEB study. Eur Respir J.
52(1800766)2018.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Máiz L, Nieto R, Cantón R, Gómez G, de la
Pedrosa E and Martinez-García MÁ: Fungi in Bronchiectasis: A
concise review. Int J Mol Sci. 19(142)2018.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Camargo CN, Carraro E, Granato CF and
Bellei N: Human rhinovirus infections in symptomatic and
asymptomatic subjects. Braz J Microbiol. 43:1641–1645.
2012.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Biancardi E, Fennell M, Rawlinson W and
Thomas PS: Viruses are frequently present as the infecting agent in
acute exacerbations of chronic obstructive pulmonary disease in
patients presenting to hospital. Intern Med J. 46:1160–1165.
2016.PubMed/NCBI View Article : Google Scholar
|
|
62
|
Harris AM, Hicks LA and Qaseem A: High
Value Care Task Force of the American College of Physicians and for
the Centers for Disease Control and Prevention. Appropriate
antibiotic use for acute respiratory tract infection in adults:
Advice for high-value care from the American college of physicians
and the centers for disease control and prevention. Ann Intern Med.
164:425–434. 2016.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Osur SL: Viral respiratory infections in
association with asthma and sinusitis: A review. Ann Allergy Asthma
Immunol. 89:553–560. 2002.PubMed/NCBI View Article : Google Scholar
|
|
64
|
Burchill E, Lymberopoulos E, Menozzi E,
Budhdeo S, McIlroy JR, Macnaughtan J and Sharma N: The unique
impact of COVID-19 on human Gut microbiome research. Front Med
(Lausanne). 8(652464)2021.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Thevaranjan N, Puchta A, Schulz C, Naidoo
A, Szamosi JC, Verschoor CP, Loukov D, Schenck LP and Jury J:
Age-associated microbial dysbiosis promotes intestinal
permeability, systemic inflammation, and macrophage dysfunction.
Cell Host Microbe. 21:455–466.e4. 2017.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Dhar D and Mohanty A: Gut microbiota and
Covid-19-possible link and implications. Virus Res.
285(198018)2020.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Chhibber-Goel J, Gopinathan S and Sharma
A: Interplay between severities of COVID-19 and the gut microbiome:
Implications of bacterial co-infections? Gut Pathog.
13(14)2021.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Khatiwada S and Subedi A: Lung microbiome
and coronavirus disease 2019 (COVID-19): Possible link and
implications. Hum Microb J. 17(100073)2020.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Fan J, Li X, Gao Y, Zhou J, Wang S, Huang
B, Wu J, Cao Q, Chen Y, Wang Z, et al: The lung tissue microbiota
features of 20 deceased patients with COVID-19. J Infect.
81:e64–e67. 2020.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Johnson DW: Croup. BMJ Clin Evid.
2014(0321)2014.PubMed/NCBI
|
|
71
|
Llor C and Bjerrum L: Antibiotic
prescribing for acute bronchitis. Expert Rev Anti Infect Ther.
14:633–642. 2016.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Fujiogi M, Camargo CA Jr, Bernot JP,
Freishtat RJ, Harmon B, Mansbach JM, Castro-Nallar E, Perez-Losada
M and Hasegawa K: In infants with severe bronchiolitis:
Dual-transcriptomic profiling of nasopharyngeal microbiome and host
response. Pediatr Res. 88:144–146. 2020.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Greenberg SB: Viral respiratory infections
in elderly patients and patients with chronic obstructive pulmonary
disease. Dis Mon. 49:201–209. 2003.PubMed/NCBI View Article : Google Scholar
|
|
74
|
Seemungal T, Harper-Owen R, Bhowmik A,
Moric I, Sanderson G, Message S, Maccallum P, Meade TW, Jeffries
DJ, Johnston SL and Wedzicha JA: Respiratory viruses, symptoms, and
inflammatory markers in acute exacerbations and stable chronic
obstructive pulmonary disease. Am J Respir Crit Care Med.
164:1618–1623. 2001.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Wat D: Impact of respiratory viral
infections on cystic fibrosis. Postgrad Med J. 79:201–203.
2003.PubMed/NCBI View Article : Google Scholar
|