Introduction
Over the last decade, immune checkpoint inhibitors
(ICIs) have shown considerable potential due to reports of their
impressive efficacy in the field of oncotherapy (1), which has resulted in the development
of radical novel strategies for treating various malignancies
(2). Instead of killing tumour
cells by direct exposure, ICIs function by regulating the behaviour
of immune cells, such as T-cells (3). Unlike conventional chemotherapeutics,
ICIs are generally well tolerated by patients and give rise to a
specific but distinct profile of toxicity, namely immune-related
adverse events (irAEs) (4).
However, despite the promising outcomes of immunotherapy based on
ICIs for the majority of solid tumours, irAEs occur in ~70% of
patients, which is not negligible and must be addressed (5). Although a wide array of organs and
body tissues have been reported to be involved, the skin,
gastrointestinal tract, endocrine glands, lung, liver and joints
are generally the most frequently affected (6). Whilst the majority of irAEs develop
during ongoing therapy (7), irAEs
occurring >90 days after the final administration of ICIs,
defined as delayed immune-related events (8), are becoming increasingly common.
These types of delayed immune-related events include
adrenocorticotropic hormone deficiency (9), hypophysitis (10), type 1 diabetes (11,12),
hepatitis (13) and
thrombocytopenia (14).
Immune checkpoint inhibitor-related pneumonitis
(CIP) has not been frequently observed in previous clinical trials
testing ICIs (15), despite it
being one of the leading causes of ICI-related mortality (16). CIP appears to occur later than
other types of irAEs, with a median time to onset of 2.8 months
since the initiation of treatment (range, between 9 days to 19.2
months) (17,18). Specific cases of late-onset CIP
>90 days following the cessation of ICI treatment are rare
according to the literature, with only seven reported to date
(15,19-22).
Therefore, it remains to be an under-reported adverse event
associated with cancer immunotherapy.
The present report documents a case of a male
patient with late-onset CIP occurring 6 months after the
discontinuation of sintilimab therapy for lung adenocarcinoma.
Other previous reports of late-onset CIP were also reviewed to
facilitate late-onset CIP characterisation and raise awareness of
this condition.
Case report
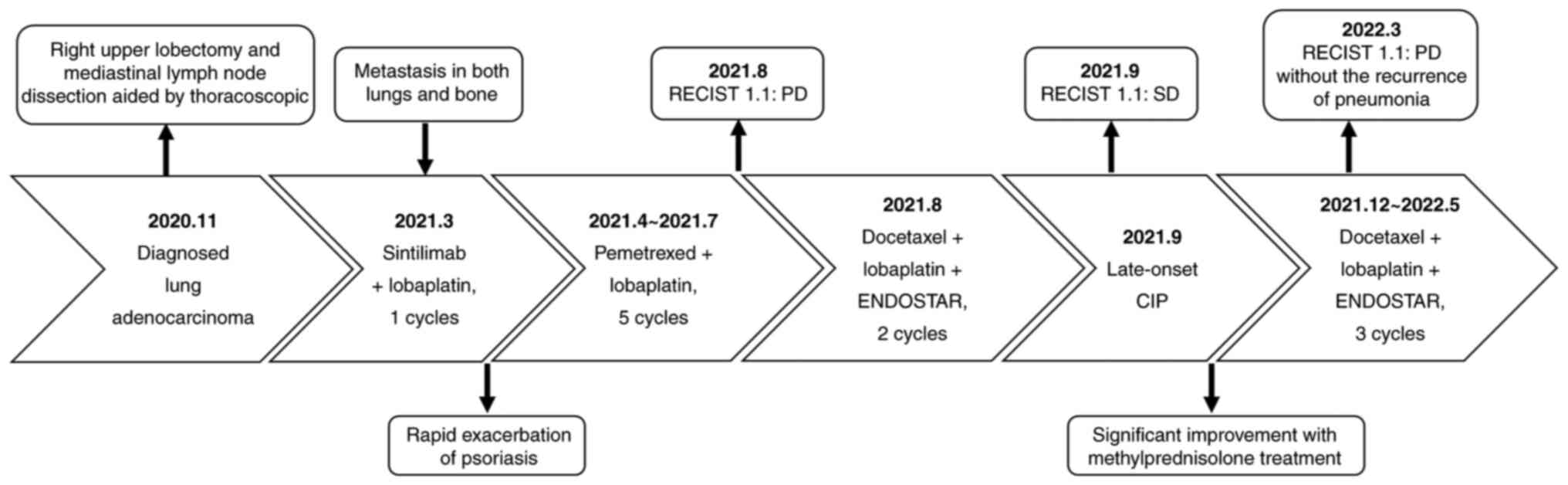
A 69-year-old male, with a 40-year history of
psoriasis for which he was being treated with acitretin, presented
with a cough and expectoration, accompanied by bloody sputum for
>1 month. He was diagnosed with adenocarcinoma of the lung at a
local hospital (Ningjin County Hospital, Xingtai, China; Fig. 1). To get better medical care, he
underwent a positron emission tomography (PET)/CT scan at Hebei
General Hospital (Shijiazhuang, China; performed in November 2020).
They revealed high uptake by the upper lobe of the right lung,
consistent with lung cancer. In addition, high uptake by metabolic
lymph nodes in the right hilum and right mediastinum was observed,
indicating metastasis. The patient subsequently underwent right
upper lobectomy and mediastinal lymph node dissection, aided by
thoracoscopy, followed by the diagnosis of stage pT2bN2M0 IIIa
infiltrating adenocarcinoma. Postoperative recovery was favourable
and no antitumor adjuvant therapy was performed.
In March 2021, a PET/CT (Discovery Elite; GE
Healthcare) scan indicated metastasis in both lungs and bone.
Next-generation sequencing was therefore performed to detect the
statuses of oncogenes, namely EGFR, anaplastic lymphoma kinase,
BRAF V600E, c-ros proto-oncogene 1, neurotrophic tyrosine receptor
kinase, human epidermal growth factor receptor 2 and
tyrosine-protein kinase Met, which revealed no driver mutations.
Detection of the tumour mutational burden and programmed
death-ligand 1 (PD-L1) expression were not conducted due to
financial reasons. Antinuclear antibodies were negative.
Administration of sintilimab [200 mg; intravenous drip (IVD)]
combined with lobaplatin (50 mg; IVD) and pemetrexed (800 mg; IVD)
was recommended as the first-line chemotherapy every 3 weeks for six
cycles. However, the patient strongly refused pemetrexed infusion
in the first cycle due to severe nausea and vomiting within 5 days
after lobaplatin infusion. In the second cycle, sintilimab was
subsequently discontinued due to the rapid exacerbation of
psoriasis after the first infusion. Psoriasis gradually improved
with methylprednisolone treatment (20 mg per day; IVD; 3 days) and
remained stable. Pemetrexed was then reintroduced into the
chemotherapy regimen from the second cycle as the patient's
physical condition improved. A treatment regimen consisting of
pemetrexed (800 mg; IVD, every 3 weeks) and lobaplatin (50 mg; IVD,
every 3 weeks) was subsequently administered over five cycles from
April 2021 to July 2021, before the patient was admitted to Hebei
General Hospital (Shijiazhuang, China) for further tests in August
(Fig. 1). Unfortunately, results
from the CT scan indicated disease progression according to solid
tumor response evaluation criteria version 1.1 (RECIST1.1)
(23). After first-line therapy,
the patient still had a good performance status and was eligible
for further platinum combination chemotherapy (24). To minimise adverse effects, the
dosage of lobaplatin was lowered. Accordingly, the patient was
treated using an individualised scheme of chemotherapy (docetaxel,
100 mg, day 1, IVD; lobaplatin, 40 mg, day 1, IVD) combined with
targeted therapy (recombinant human endostatin, 30 mg, day 1-7,
IVD) (Fig. 1). The final treatment
was scheduled on 28 August 2021, which was well tolerated.
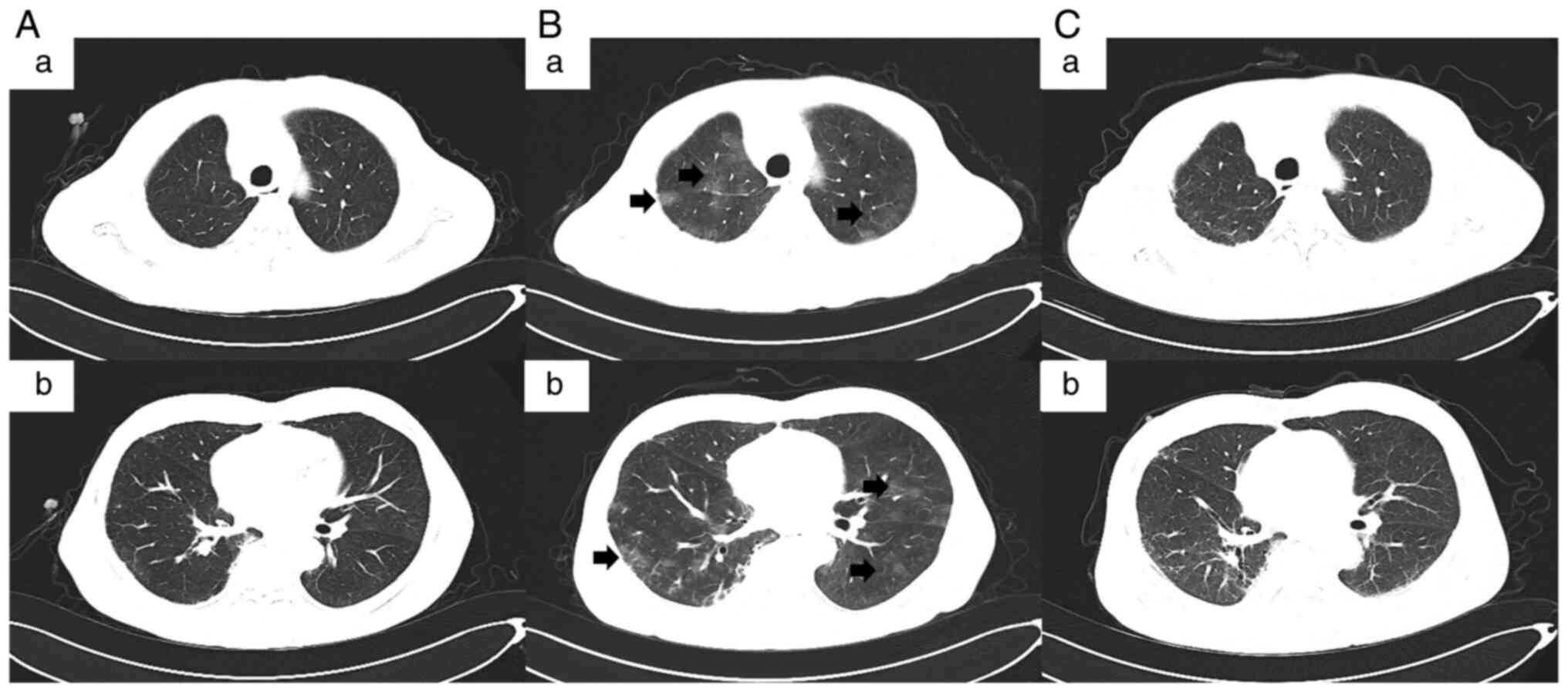
In September 2021, the patient was readmitted to the
hospital after complaining of intermittent cough, yellow phlegm and
fever. A CT scan (Fig. 2A-a and
A-b) showed interstitial changes
in both lungs. The tumor condition was assessed as stable disease
(RECIST1.1). Routine blood examinations (Sysmex XN-3000 Automated
Hematology Analyzer; Sysmex Corporation) revealed white blood cell
(WBC) counts to be 10.62x109/l (normal value,
3.5-9.5x109/l) and neutrophil numbers (NEUT#) of
8.72x109/l (normal value, 1.8-6.3x109/l).
Considering the presence of pulmonary infection, the patient was
administrated with ceftriaxone (2 g, once a day) for 4 days before
being subsequently switched to piperacillin-tazobactam (4.5 g,
every 8 h) for 6 days when pseudomonas aeruginosa was
detected in the sputum samples. Meanwhile, the patient was treated
with inhaled budesonide suspension and acetylcysteine solution
aerosol to relieve the symptoms.
After 10 days, routine blood re-examination revealed
the following: i) WBC was 4.42x109/l (normal value,
3.5-9.5x109/l); ii) NEUT# was 3.04x109/l
(normal value, 1.8-6.3x109/l); iii) C-reactive protein
was 58.69 mg/l (normal value, 0-6 mg/l); and iv) normal levels of
procalcitonin. Cultures of the patient's blood and sputum were both
negative for bacteria. However, the patient remained to be
afflicted with an intermittent fever (≤38˚C), cough with shortness
of breath and occasionally yellow phlegm. Considering the history
of ICI treatment, the development of CIP was not excluded.
Therefore, methylprednisolone sodium succinate (80 mg per day) was
injected before chest CT was performed on that day.
CT scans (Fig. 2B-a
and B-b) revealed interstitial
changes in both lungs in addition to multiple ground-glass
opacities, mainly involving the periphery of both lungs. However,
they did not support bacterial infection, and tumour progression
could also be ruled out. Further analysis of the bronchoalveolar
lavage fluid (BALF) revealed lymphocytosis in 30% of lymphocytes,
with no evidence of infection according to the microbiological
culture and PCR testing. Infectious pneumonia induced by
tuberculosis bacteria, fungi and viruses were therefore eliminated.
In addition, 3 days of methylprednisolone treatment resulted in a
rapid improvement of clinical symptoms without fever or shortness
of breath whilst reducing the frequency of coughing. The
combination of clinical manifestations, CT imaging and
microbiological assays strongly indicated that the patient's
medical condition was consistent with sintilimab-induced CIP,
defined as grade two according to American Society of Clinical
Oncology Clinical Practice Guideline for management of irAEs in
patients treated with ICIs (25).
Antibiotics were discontinued and the patient was treated
continuously with methylprednisolone (40 mg per day) for a further
3 days, resulting in significant improvement on CT scans. Before
discharge, the patient was switched to oral prednisolone (30 mg per
day), which was gradually lowered to 2.5 mg per day over 6 weeks
without the recurrence of CIP. After the remission of pneumonia,
the patient had also been treated with piperacillin sodium and
tazobactam sodium for addressing urinary tract infections at
Ningjin County Hospital (Xingtai, China) in November 2021, which
did not exacerbate the interstitial changes in the lungs. In
December 2021, the patient was readmitted to Hebei General Hospital
(Shijiazhuang, China). CT scans (Fig.
2C-a and C-b) showed
progressive improvement of CIP after corticosteroid administration
without recurrence. In the follow-up treatment (between December
2021 and May 2022), the patient continued to receive docetaxel and
lobaplatin combined with recombinant human endostatin without the
recurrence of pneumonia. The tumor condition was assessed as
progressive disease (RECIST1.1) in March 2022. The Naranjo's
Probability Scale for Adverse Drug Reactions was used to evaluate
the patient's condition (Table I)
(26). A score of seven was
obtained, classifying sintilimab as the probable cause of the
patient's late-onset CIP.
 | Table INaranjo score of the probability that
the late-onset immune checkpoint inhibitor-related pneumonitis was
the result of the cessation of treatment with sintilimab. |
Table I
Naranjo score of the probability that
the late-onset immune checkpoint inhibitor-related pneumonitis was
the result of the cessation of treatment with sintilimab.
| Naranjo scoring
system for adverse reaction |
|---|
| Question | Answer
(points) |
|---|
| 1. Are there
previous conclusive reports on this reaction? | Yes (1) |
| 2. Did the adverse
events appear after the suspected drug was given? | Yes (2) |
| 3. Did the adverse
reaction improve when the drug was discontinued or a specific
antagonist was given? | Yes (1) |
| 4. Did the adverse
reaction appear when the drug was readministered? | Not performed
(0) |
| 5. Are there
alternative causes that could have caused the reaction? | No (2) |
| 6. Did the reaction
reappear when a placebo was given? | Not performed
(0) |
| 7. Was the drug
detected in any body fluid in toxic concentrations? | Not performed
(0) |
| 8. Was the reaction
more severe when the dose was increased or less severe when the
dose was decreased? | Not performed
(0) |
| 9. Did the patient
have a similar reaction to the same or similar drugs in a previous
exposure? | Not performed
(0) |
| 10. Was the adverse
event confirmed by any objective evidence? | Yes (1) |
| | Score=7
(Probable) |
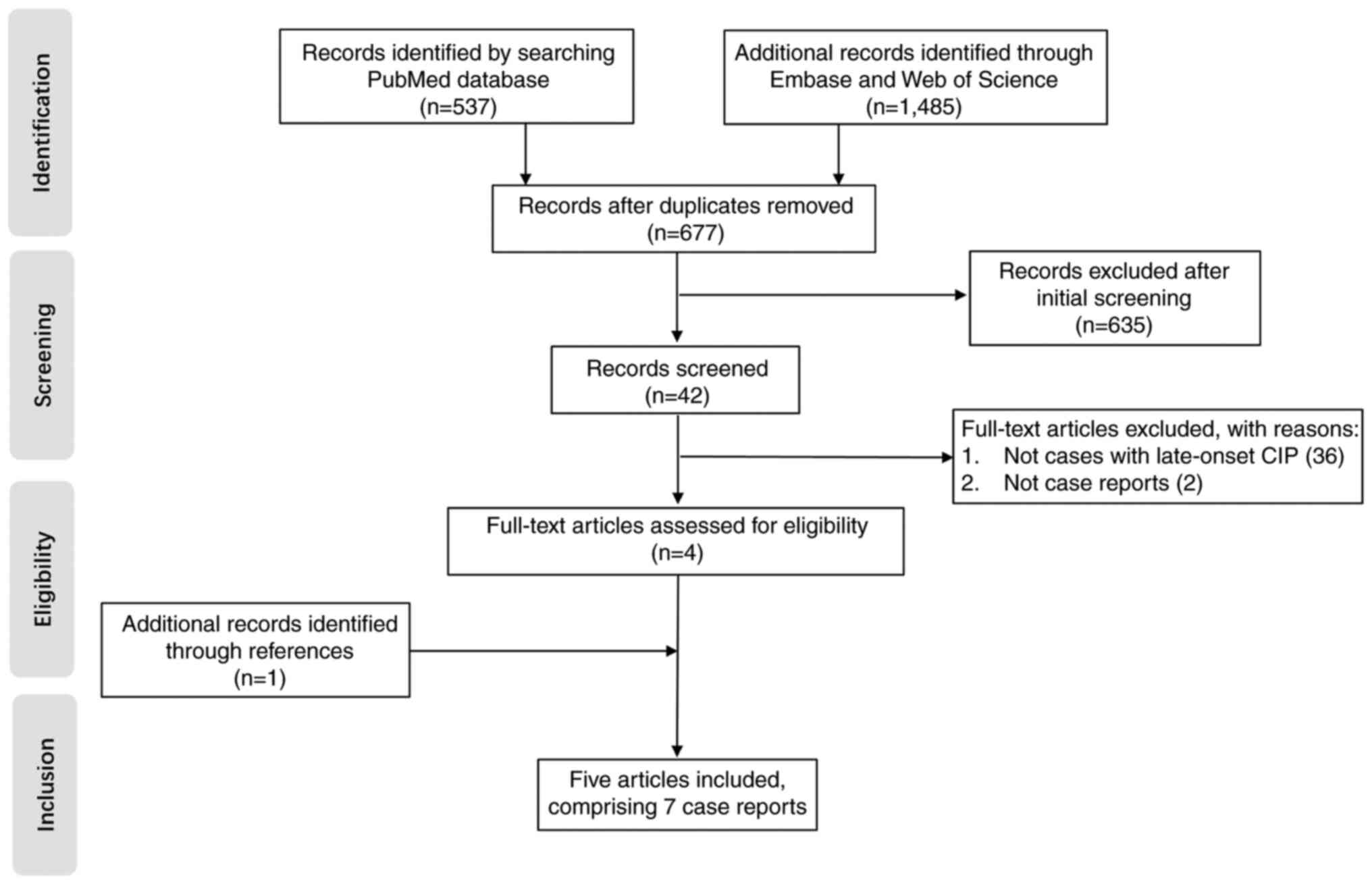
Literature review
Published studies were identified by searching
PubMed (https://pubmed.ncbi.nlm.nih.gov), Embase (https://www.embase.com) and Web of Science (https://www.webofscience.com) until September 2022 for
the following combination of terms: (‘immunotherapy’ OR ‘checkpoint
inhibitors’ OR ‘checkpoint blockade’ OR ‘anti-CTLA 4’ OR
‘anti-PD-1’ OR ‘anti-PD-L1’ OR ‘ipilimumab’ OR ‘nivolumab’ OR
‘pembrolizumab’ OR ‘sintilimab’ OR ‘camrelizumab’ OR ‘toripalimab’
OR ‘atezolizumab’ OR ‘durvalumab’ OR ‘avelumab’ OR ‘cemiplimab’)
AND ‘after’ AND (‘cessation’ OR ‘discontinuation’) AND
(‘immune-related adverse event’ OR ‘immune checkpoint
inhibitor-related pneumonitis’ OR ‘pneumonitis’). In addition, the
reference lists of the retrieved articles were also searched. All
studies identified by this procedure were reviewed independently by
two reviewers (YPW and YSY) and any disagreements were resolved
through discussion. Case reports and case series published in
journals or those presented at conferences were included. Included
studies reported patients who developed CIP, which manifested ≥90
days after the discontinuation of immunotherapy.
Pharmacokinetic/pharmacodynamic studies and randomized controlled
trials were excluded due to lacking detailed data of each patient.
Furthermore, case series that lacked detailed patient data (≥3
terms of patient's disease, age, sex, type and cycles of ICIs,
off-treatment interval treatment, intervention and outcome were
missing) were also excluded. A total of five studies (15,19-22)
were identified in the review. A total of 3 cases were described in
one study (20), bringing the
total number of case reports of late-onset CIP to 7. Fig. 3 shows a flow diagram of the
screening and selection process.
The major clinical features of reported in the seven
cases of late-onset CIP that qualified from the present screening
process are summarized in Table
II (15,19-22).
The median patient age (three females and five males) was 63 years
(range, 25-69 years). Immunotherapy included nivolumab (n=4)
(19-21),
pembrolizumab (n=1) (20),
atezolizumab (n=1) (15),
sintilimab (n=1) and not specified (n=1) (22). The types of cancer treated were
stage IV adenocarcinoma of the lung (n=3) (20), stage III melanoma (n=2) (19,22),
stage IV squamous cell carcinoma of the lung (n=1) (20), metastatic renal cell carcinoma
(n=1) (21) and metastatic
para-osteal osteosarcoma (n=1) (15). In particular, the majority of the
cases of late-onset CIP occurred during the recurrent or metastatic
stages. Notably, the median off-treatment interval for late-onset
CIP was 6.5 months (range, 4-28 months) whereas the median
cumulative immunotherapy exposure was four doses (range, 1-35
doses). Prior on-treatment irAEs (5/8), including abnormal liver
function (n=1), pneumonitis (n=2), colitis (n=1) and exacerbation
of psoriasis (n=1), was the most common cause of immunotherapy
discontinuation. Clinicians should be mindful of recurrent CIP,
since two patients experienced an intermittent recurrence of CIP
over a timescale of months or even years following ICI cessation
(15,20). In addition, one patient with
late-onset CIP concurrently suffered from delayed hepatitis and
renal dysfunction (21). CIP (3-4
grade) was present in only two cases (20,22)
whereas grades 1 and 2 were observed in the other six. Among the
eight patients with late-onset CIP, seven were managed with
corticosteroids with the addition of mycophenolate mofetil for one
patient. A clear improvement was observed in seven of the eight
enrolled patients, but one patient succumbed to CIP despite the
administration of high doses of methylprednisolone (20).
| Table IIClinical data of patients presenting
with late-onset CIP following treatment cessation. |
Table II
Clinical data of patients presenting
with late-onset CIP following treatment cessation.
| First authors,
year | Patient's
disease | Age, years | Sex | Type of ICIs | Combinati on
medication | Cycles of ICIs | Off-treatment
interval | Reasons for
discontinuation | CIP grade | Treatments | Outcome | (Refs.) |
|---|
| Diamantopoulos
et al, 2017 | Melanoma | 62 | F | Nivolumab | Monotherapy | 5 | 6 months | Abnormal liver
function | 2 | Moxifloxacin and
prednisone | Improved | (19) |
| Kimura et
al, 2021 | Adenocarcinoma | 62 | M | Nivolumab | Monotherapy | 4 | 7 months | Financial
reasons | 2 | Prednisolone | Improved | (20) |
| Kimura et
al, 2021 | Squamous cell
carcinoma | 68 | M | Nivolumab | Monotherapy | 2 | 8 months | Pneumonitis | 1 | No treatment | Improved | (20) |
| Kimura et
al, 2021 | Adenocarcinoma | 69 | M | Pembrolizumab | Monotherapy | 4 | 4 months | Progression of
brain metastases | 4 |
Methylprednisolone | Succumbed to
pneumonitis | (20) |
| Nakai et al,
2021 | Renal cell
carcinoma | 50 | M | Nivolumab | Monotherapy | Not specified | 142 days | Multiple metastases
of tumour | 2 | Methylprednisolone
and mycophenolate mofetil | Improved | (21) |
| Kucukarda et
al, 2022 | Osteosarcoma | 25 | F | Atezolizumab | Monotherapy | 35 | 24 months | Pneumonitis | 2 |
Methylprednisolone | Improved | (15) |
| Mandala et
al, 2018 | Melanoma | 64 | F | Not specified | Monotherapy | Not specified | 8 months | Colitis | 3 | Wide-spectrum
antibiotics and methylprednisolone | Improved | (22) |
| Present study | Adenocarcinoma | 69 | M | Sintilimab | Lobaplatin | 1 | 6 months | Exacerbation of
psoriasis | 2 |
Methylprednisolone | Improved | (-) |
Discussion
CIP is one of the major causes of ICI-associated
mortality (16). Symptoms of CIP
include dry cough, shortness of breath with exertion, reduced
oxygen saturation and bilateral ground-glass opacities or patchy
nodular infiltrations in the lung on CT imaging (27,28).
The incidence of pneumonia secondary to ICIs is <5%, with fatal
CIP being reported in 0.2-0.5% patients (16,29).
Although relatively infrequent in occurrence, CIP is complex and
unpredictable in terms of both clinical and radiological
manifestations, which may overlap with those of COVID-19 or other
viral infections (30). This
therefore provide a challenge for oncologists during the early
diagnosis of lung diseases (30).
Diagnosis of CIP is considered to be a ‘process of elimination’ in
the majority of cases (31).
Radiation-induced pneumonitis, all types of infectious pulmonary
inflammation and lung cancer progression, should all be considered
and excluded (2). If making a
differential diagnosis is difficult, CIP can be confirmed by
bronchoscopy or lung biopsy (32).
Lymphocytosis in BALF samples without evidence of infectious
aetiologies can facilitate the confirmation of this diagnosis
(32). However, late-onset CIP
after ICI cessation is easily misdiagnosed due to the brief patient
exposure to ICI and long ICI-free interval, interventions
overlapping with the toxicity patterns, reduced medical vigilance
after discontinuing treatment and the lengthy process of
diagnosis-by-elimination (8).
In the present case report, the patient was admitted
due to fever and coughing with sputum, which persisted after
anti-infection treatment. However, the patient showed neither signs
of tumour progression nor infections by tuberculosis bacteria,
fungi or viruses. The patient had no previous history of autoimmune
diseases other than psoriasis, whereas antinuclear antibodies
tested negative before sintilimab initiation. Psoriasis remained
stable when the patient developed pneumonia. To the best of our
knowledge, there were no previous reports in the literature
associating psoriasis with interstitial pneumonia. It would have
been interesting to explore drug-induced interstitial lung disease
(DIILD). To date, >400 drugs have been reported to cause DIILD,
with anti-cancer drugs, rheumatology drugs, amiodarone and
antibiotics being the most common causes (33,34).
On referring to the patient's treatment and medication history,
docetaxel, recombinant human endostatin, piperacillin sodium and
tazobactam sodium have been reported to cause pneumonia or
interstitial pneumonia in the medicine specifications or literature
(35,36). In fact, after remission for
pneumonia, the patient had also been treated with β-lactam drugs
for infections of the urinary tract at a local hospital and
continued to receive three courses of docetaxel and recombinant
human endostatin in follow-up treatment, without the recurrence of
pneumonia. Therefore, pneumonia induced by chemotherapy, targeted
therapy or antibiotics could be excluded. The patient received one
dose of the sintilimab immunotherapeutic 6 months previously (March
2021). Methylprednisolone treatment resulted in a significant
improvement of pneumonia in both clinical and radiological
manifestations. Therefore, all evidence pointed to late-onset CIP
caused by the administration of sintilimab.
Sintilimab, co-developed by Innovent Biologics and
Eli Lilly, is a fully humanized IgG4 anti-programmed cell death
protein 1 (PD-1) monoclonal antibody (37). Sintilimab binds to PD-1 and
restores endogenous antitumour T-cell responses by blocking the
interaction of PD-1with its ligands PD-L1 and PD-L2(37). The primary adverse events
associated with sintilimab treatment reported in clinical trials
are similar to those following nivolumab and pembrolizumab
treatment, which include pyrexia, hypothyroidism, hepatitis and CIP
(38). The occurrence of irAEs in
general may be attributed to the increased activity of immune cells
that target antigens common to both tumours and normal tissues
(39), which might also serve a
role in the development of CIP. Enrichment of CD8+ T or
CD4+ T-lymphocytes, along with high expression levels of
PD-1, have been detected in the lung or bronchoalveolar lavage
samples of patients with CIP in several previous studies (40,41).
When the immune homeostasis of the lung is altered, typically
characterised by lymphocyte infiltration, an autoimmune reaction
may be triggered, with the first key reaction occurring when the
lymphocytes are being assembled (42). However, the complexity of the
subject is underlined by the fact that radiotherapy, pulmonary
infection, cryoablation of lung metastasis or chemotherapy can all
alter immune homeostasis and cause hyperactivation of the immune
system, leading to CIP (42).
Individuals with pre-existing autoimmune diseases
may harbour a genetic susceptibility, leading to a significantly
increased risk of irAEs (43,44).
Psoriasis is a common immune-mediated skin condition (45). In a retrospective cohort study,
Halle et al (46) noted
that 57% patients with pre-existing psoriasis experienced flare-ups
after receiving ICIs, including cutaneous flare, exacerbation of
arthritis and exacerbation of iritis, whereas 59% experienced other
irAEs. The patient in the present case report had a 40-year history
of psoriasis, which was aggravated by sintilimab immunotherapy. It
is considered that pre-existing autoimmune diseases, previous
exposure to cytotoxic drugs and pulmonary damage from cancer and
inflammation are major risk concerns for the patient in contracting
CIP.
Late-onset CIP remains an under-recognized and
complex diagnostic challenge. The lasting effects of immunotherapy,
even after ICI withdrawal, have been verified by several studies
(47-50)
and may be associated with the underlying mechanism of
immunological ‘memory’ (48). If a
long-term immunological ‘memory’ with a positive outcome does
exist, it may also have implications for late-occurring T
cell-mediated toxicities (22,27).
Brahmer et al (51)
previously reported a serum half-life of 12-20 days for nivolumab
after a single dose treatment, with a mean PD-1 receptor occupancy
on T-cell plateaus of 72% for ≤57 days. This suggests that the
long-lasting pharmacodynamic effects of ICIs generally outlasts
their pharmacokinetic half-life (27,51).
Furthermore, the receptor occupancy remained at 40% for >8
months after three doses (51).
This finding may explain the median off-treatment interval to
late-onset CIP of 6.5 months following the cessation of
immunotherapy in the present study. Compared with nivolumab,
sintilimab has a higher binding affinity with PD-1 molecules
(52,53). Wang et al (53) reported a PD-1 receptor occupancy by
sintilimab of >95% in patients 4 weeks after a single
intravenous infusion. This high binding affinity and sustained
receptor occupancy may contribute to persistent T-cell activation
following the cessation of therapy even when serum levels of this
drug become undetectable.
The present case report specifically highlights the
finding that CIP can manifest in a period following the cessation
of immunotherapy, even following patient exposure to only one dose.
The median off-treatment interval to late-onset CIP was 6.5 months
(range, 4-28 months), which is consistent with the finding made by
Couey et al (8). Careful
monitoring, timely diagnosis and administration of corticosteroids
are essential for controlling the condition. Clinical practice
guidelines for the management of toxicities from immunotherapy
allude to monitoring for delayed immune-related events ≥12 months
following the discontinuation of ICI-based treatment (54,55).
However, to the best of our knowledge, studies on delayed
immune-related events after discontinuation of immunotherapy are
scarce due to limited follow-up periods (8). It would have been interesting to
explore stringent evidence-based surveillance protocols.
Individualized surveillance strategies based on a patient's risk
profile for irAEs after treatment cessation are recommended,
particularly for those patients with pre-existing autoimmune
diseases.
It should be noted that a platinum-based dual-drug
regimen, is generally started at 4-6 weeks after surgery and no
later than 3 months. Unfortunately, the present patient was not
admitted on time due to disruption caused by the COVID-19 pandemic,
personal and objective factors. It is considered that the delay is
one of the major reasons for the recurrence and metastasis of the
tumour only 4 months after surgery. Further accumulation of case
data is required to both enhance confidence in diagnostic
predictors and to improve the clinical outcomes of late-onset CIP
following ICI cessation.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analysed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
YW and YY analysed and interpreted the data,
performed the literature review, and were major contributors in
drafting the manuscript. XY and LF collected the clinical data and
performed the literature research. JS participated in the data
acquisition and interpretation, was involved in drafting the
manuscript and critically revised the manuscript. YW and YY confirm
the authenticity of all the raw data. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Hebei General Hospital (Shijiazhuang, China) and
informed consent was obtained from the patient.
Patient consent for publication
The patient provided written informed consent
regarding the publication of the case details and any associated
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bai J, Li D, Yang P, Xu K, Wang Y, Li Q,
Liu J, Du W, Zhang F and Feng R: Camrelizumab-Related myocarditis
and myositis with myasthenia gravis: A case report and literature
review. Front Oncol. 11(778185)2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Yin B, Xiao J, Li J, Liu X and Wang J:
Immune-related organizing pneumonitis in non-small cell lung cancer
receiving PD-1 inhibitor treatment: A case report and literature
review. J Cancer Res Ther. 16:1555–1559. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Weinmann SC and Pisetsky DS: Mechanisms of
immune-related adverse events during the treatment of cancer with
immune checkpoint inhibitors. Rheumatology (Oxford). 58 (Suppl
7):vii59–vii67. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Huang Y, Liang D, Liu J, Zeng J and Zeng
Y: The breakthroughs in cancer immune checkpoint based therapy: A
review of development in immune checkpoint study and its
application. Comb Chem High Throughput Screen. 20:430–439.
2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yang H, Zhou C, Yuan F, Guo L, Yang L, Shi
Y and Zhang J: Case report: Severe immune-related cholestatic
hepatitis and subsequent pneumonia after pembrolizumab therapy in a
geriatic patient with metastic gastric cancer. Front Med
(Lausanne). 8(719236)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Naidoo J, Page DB, Li BT, Connell LC,
Schindler K, Lacouture ME, Postow MA and Wolchok JD: Toxicities of
the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann
Oncol. 26:2375–2391. 2015.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Safa H, Bhosale P, Weissferdt A and Oliva
ICG: Difficulties in differentiating between checkpoint inhibitor
pneumonitis and lung metastasis in a patient with melanoma.
Immunotherapy. 12:293–298. 2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Couey MA, Bell RB, Patel AA, Romba MC,
Crittenden MR, Curti BD, Urba WJ and Leidner RS: Delayed
immune-related events (DIRE) after discontinuation of
immunotherapy: Diagnostic hazard of autoimmunity at a distance. J
Immunother Cancer. 7(165)2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Takeno A, Yamamoto M, Morita M, Tanaka S,
Kanazawa I, Yamauchi M, Kaneko S and Sugimoto T: Late-onset
isolated adrenocorticotropic hormone deficiency caused by
nivolumab: A case report. BMC Endocr Disord. 19(25)2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Antoniou S, Bazazo G, Rockl L, Papadakis M
and Berg C: Late-onset hypophysitis after discontinuation of
nivolumab treatment for advanced skin melanoma: A case report. BMC
Endocr Disord. 21(191)2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Mae S, Kuriyama A and Tachibana H:
Diabetic ketoacidosis as a delayed immune-related event after
discontinuation of nivolumab. J Emerg Med. 60:342–344.
2021.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Yaura K, Sakurai K, Niitsuma S, Sato R,
Takahashi K and Arihara Z: Fulminant type 1 diabetes mellitus
developed about half a year after discontinuation of immune
checkpoint inhibitor combination therapy with nivolumab and
ipilimumab: A case report. Tohoku J Exp Med. 254:253–256.
2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kanaoka K, Moriizumi K, Okada H, Iwahashi
K, Tsuji H, Yasuoka H and Minami S: Pembrolizumab-Induced
delayed-onset hepatitis. Case Rep Gastroenterol. 14:586–592.
2020.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Fu S, Wang T and Xu F: Delayed immune
thrombocytopenia after discontinuation of nivolumab therapy: A case
report and literature review. J Oncol Pharm Pract. 27:1548–1552.
2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kucukarda A, Gokmen I, Ozcan E, Peker P,
Akgul F and Cicin I: Recurrent delayed immune-related pneumonitis
after immune-checkpoint inhibitor therapy for advanced
osteosarcoma. Immunotherapy. 14:395–399. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Wang DY, Salem JE, Cohen JV, Chandra S,
Menzer C, Ye F, Zhao S, Das S, Beckermann KE, Ha L, et al: Fatal
toxic effects associated with immune checkpoint inhibitors: A
systematic review and meta-analysis. JAMA Oncol. 4:1721–1728.
2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Friedman CF, Proverbs-Singh TA and Postow
MA: Treatment of the immune-related adverse effects of immune
checkpoint inhibitors: A review. JAMA Oncol. 2:1346–1353.
2016.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Naidoo J, Wang X, Woo KM, Iyriboz T,
Halpenny D, Cunningham J, Chaft JE, Segal NH, Callahan MK, Lesokhin
AM, et al: Pneumonitis in patients treated with anti-programmed
death-1/programmed death ligand 1 therapy. J Clin Oncol.
35:709–717. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Diamantopoulos PT, Gaggadi M, Kassi E,
Benopoulou O, Anastasopoulou A and Gogas H: Late-onset
nivolumab-mediated pneumonitis in a patient with melanoma and
multiple immune-related adverse events. Melanoma Res. 27:391–395.
2017.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kimura H, Sone T, Araya T, Murata A,
Yamamura K, Ohkura N, Hara J, Abo M and Kasahara K: Late-onset
programmed cell death protein-1 inhibitor-induced pneumonitis after
cessation of nivolumab or pembrolizumab in patients with advanced
non-small cell lung cancer: A case series. Transl Lung Cancer Res.
10:1576–1581. 2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Nakai Y, Otsuka T, Inoue T, Nawa T, Hatano
K, Yamamoto Y, Nagahara A, Nakayama M, Kakimoto KI and Nishimura K:
Two cases of delayed onset of immune-related adverse events after
discontinuation of nivolumab in patients with metastatic renal cell
cancer. IJU Case Rep. 4:326–329. 2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Mandala M, Merelli B, Indriolo A and
Tondini C: Late-occurring toxicity induced by an immune checkpoint
blockade in adjuvant treatment of a stage III melanoma patient. Eur
J Cancer. 95:130–132. 2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Yi Y, Liu Z, Fang L, Li J, Liu W, Wang F,
Fu P, Xie C, Liu J and Song B: Comparison between single-agent and
combination chemotherapy as second-line treatment for advanced
non-small cell lung cancer: A multi-institutional retrospective
analysis. Cancer Chemother Pharmacol. 86:65–74. 2020.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Brahmer JR, Lacchetti C, Schneider BJ,
Atkins MB, Brassil KJ, Caterino JM, Chau I, Ernstoff MS, Gardner
JM, Ginex P, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: American
Society of clinical oncology clinical practice guideline. J Clin
Oncol. 36:1714–1768. 2018.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Naranjo CA, Busto U, Sellers EM, Sandor P,
Ruiz I, Roberts EA, Janecek E, Domecq C and Greenblatt DJ: A method
for estimating the probability of adverse drug reactions. Clin
Pharmacol Ther. 30:239–245. 1981.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Johnson DB, Nebhan CA, Moslehi JJ and
Balko JM: Immune-checkpoint inhibitors: Long-term implications of
toxicity. Nat Rev Clin Oncol. 19:254–267. 2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Qu Y, Wang Z, Feng J, Wang L, Liu H, Liu
D, Zhao Y, Yu R, Li W, Sun D and Yu H: Pneumonitis, appendicitis,
and biliary obstruction during toripalimab treatment in a patient
with extensive-stage small-cell lung cancer: A case report. Ann
Palliat Med. 10:9267–9275. 2021.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Khunger M, Rakshit S, Pasupuleti V,
Hernandez AV, Mazzone P, Stevenson J, Pennell NA and Velcheti V:
Incidence of pneumonitis with use of programmed death 1 and
programmed death-ligand 1 inhibitors in non-small cell lung cancer:
A systematic review and meta-analysis of trials. Chest.
152:271–281. 2017.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Sullivan RJ, Johnson DB, Rini BI, Neilan
TG, Lovly CM, Moslehi JJ and Reynolds KL: COVID-19 and immune
checkpoint inhibitors: Initial considerations. J Immunother Cancer.
8(e000933)2020.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Li L, Lou A and Yu J: Immune checkpoint
inhibitor-related pneumonitis induced by camrelizumab: A case
report and review of literature. Ann Palliat Med. 10:8460–8466.
2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Wang H, Guo X, Zhou J, Li Y, Duan L, Si X
and Zhang L, Liu X, Wang M, Shi J and Zhang L: Clinical diagnosis
and treatment of immune checkpoint inhibitor-associated
pneumonitis. Thorac Cancer. 11:191–197. 2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Skeoch S, Weatherley N, Swift AJ, Oldroyd
A, Johns C, Hayton C, Giollo A, Wild JM, Waterton JC, Buch M, et
al: Drug-Induced interstitial lung disease: A systematic review. J
Clin Med. 7(356)2018.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Spagnolo P, Bonniaud P, Rossi G,
Sverzellati N and Cottin V: Drug-induced interstitial lung disease.
Eur Respir J. 60(2102776)2022.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Min BD, Kang HW, Kim WT, Kim YJ, Yun SJ,
Lee SC and Kim WJ: Docetaxel-induced fatal interstitial pneumonitis
in a patient with castration-resistant prostate cancer. Korean J
Urol. 53:371–374. 2012.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Wang CJ, Chang HT and Chang CY:
Docetaxel-related interstitial pneumonitis. Ther Clin Risk Manag.
11:1813–1816. 2015.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Hoy SM: Sintilimab: First global approval.
Drugs. 79:341–346. 2019.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Shi Y, Su H, Song Y, Jiang W, Sun X, Qian
W, Zhang W, Gao Y, Jin Z, Zhou J, et al: Safety and activity of
sintilimab in patients with relapsed or refractory classical
Hodgkin lymphoma (ORIENT-1): A multicentre, single-arm, phase 2
trial. Lancet Haematol. 6:e12–e19. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Shibata Y, Murakami S and Kato T: Overview
of checkpoint inhibitor pneumonitis: Incidence and associated risk
factors. Expert Opin Drug Saf. 20:537–547. 2021.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Leroy V, Templier C, Faivre JB,
Scherpereel A, Fournier C, Mortier L and Wemeau-Stervinou L:
Pembrolizumab-induced pneumonitis. ERJ Open Res. 3:00081–2016.
2017.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Delaunay M, Cadranel J, Lusque A, Meyer N,
Gounant V, Moro-Sibilot D, Michot JM, Raimbourg J, Girard N,
Guisier F, et al: Immune-checkpoint inhibitors associated with
interstitial lung disease in cancer patients. Eur Respir J.
50(1700050)2017.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Pozzessere C, Bouchaab H, Jumeau R,
Letovanec I, Daccord C, Bourhis J, Prior JO, Peters S, Lazor R and
Beigelman-Aubry C: Relationship between pneumonitis induced by
immune checkpoint inhibitors and the underlying parenchymal status:
A retrospective study. ERJ Open Res. 6:00165–2019. 2020.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Danlos FX, Voisin AL, Dyevre V, Michot JM,
Routier E, Taillade L, Champiat S, Aspeslagh S, Haroche J, Albiges
L, et al: Safety and efficacy of anti-programmed death 1 antibodies
in patients with cancer and pre-existing autoimmune or inflammatory
disease. Eur J Cancer. 91:21–29. 2018.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Cortellini A, Buti S, Santini D, Perrone
F, Giusti R, Tiseo M, Bersanelli M, Michiara M, Grassadonia A,
Brocco D, et al: Clinical outcomes of patients with advanced cancer
and pre-existing autoimmune diseases treated with anti-programmed
death-1 immunotherapy: A real-world transverse study. Oncologist.
24:e327–e337. 2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Griffiths CE and Barker JN: Pathogenesis
and clinical features of psoriasis. Lancet. 370:263–271.
2007.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Halle BR, Betof Warner A, Zaman FY, Haydon
A, Bhave P, Dewan AK, Ye F, Irlmeier R, Mehta P, Kurtansky NR, et
al: Immune checkpoint inhibitors in patients with pre-existing
psoriasis: Safety and efficacy. J Immunother Cancer.
9(e003066)2021.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Kimura H, Sone T, Murata A, Koba H, Tambo
Y, Hara J, Abo M and Kasahara K: Long-lasting shrinkage in tumour
mass after discontinuation of nivolumab treatment. Lung Cancer.
108:7–8. 2017.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Pesola G, Murianni V, Rebuzzi SE, Banna
GL, Cerbone L, Catalano F, Borea R, Gandini A, Cremante M, Puglisi
S, et al: Durable response after immunotherapy discontinuation for
delayed and severe immune-related adverse events: A case report.
Immunotherapy. 13:1379–1386. 2021.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Umihira S, Koyanagi T, Tamura K, Takahashi
Y, Yoshiba T, Takahashi S, Taneichi A, Saga Y, Takei Y and Fujiwara
H: Durable response after the discontinuation of pembrolizumab
treatment due to an adverse event in a patient with advanced
endometrial cancer: A case report. Exp Ther Med.
23(409)2022.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Eguchi S, Shinkawa H, Sato Y, Nakai K,
Takemura S, Tanaka S, Amano R, Kimura K, Ohira G, Nishio K, et al:
Durable response after discontinuation of pembrolizumab therapy for
intrahepatic cholangiocarcinoma: A case report. Clin J
Gastroenterol. 14:858–865. 2021.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Brahmer JR, Drake CG, Wollner I, Powderly
JD, Picus J, Sharfman WH, Stankevich E, Pons A, Salay TM, McMiller
TL, et al: Phase I study of single-agent anti-programmed death-1
(MDX-1106) in refractory solid tumours: Safety, clinical activity,
pharmacodynamics, and immunologic correlates. J Clin Oncol.
28:3167–3175. 2010.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Zhang L, Lin W, Tan F, Li N, Xue Q, Gao S,
Gao Y and He J: Sintilimab for the treatment of non-small cell lung
cancer. Biomark Res. 10(23)2022.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Wang J, Fei K, Jing H, Wu Z, Wu W, Zhou S,
Ni H, Chen B, Xiong Y, Liu Y, et al: Durable blockade of PD-1
signaling links preclinical efficacy of sintilimab to its clinical
benefit. MAbs. 11:1443–1451. 2019.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Haanen JBAG, Carbonnel F, Robert C, Kerr
KM, Peters S, Larkin J and Jordan K: ESMO Guidelines Committee.
Management of toxicities from immunotherapy: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 28
(suppl_4):iv119–iv142. 2017.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Phan T, Patwala K, Lipton L, Knight V, Aga
A and Pianko S: Very delayed acute hepatitis after pembrolizumab
therapy for advanced malignancy: How long should we watch? Curr
Oncol. 28:898–902. 2021.PubMed/NCBI View Article : Google Scholar
|