Introduction
The most common critical incidents in pediatric
anesthesia are perioperative respiratory adverse events (PRAEs) and
account for a third of anaesthesia-associated cardiac arrests
(1). The incidence of PRAEs is 15%
in a general paediatric population, however, the rate of PRAEs is
doubled in infants (aged ≤1 year) (2). Although pediatric anesthesia is
improving, PRAEs remain the most common cause of severe
perioperative morbidity and mortality (3). During general anesthesia in children,
PRAEs are most likely to occur during recovery from anesthesia
(4). Children have high oxygen
demands and low oxygen reserves, making them more susceptible to
PRAEs. Avoiding PRAEs during tracheal tube or laryngeal mask
removal in pediatric anesthesia is a challenging task (1,5).
Dexmedetomidine is a highly selective α2-adrenoceptor
agonist that is increasingly used due to its sedative, analgesic
and anti-sympathetic effects (6,7).
Dexmedetomidine has been reported to decrease airway and
circulatory responses during extubation in children (8). To the best of our knowledge, however,
there are insufficient data to demonstrate that dexmedetomidine can
reduce the incidence of PRAEs in children undergoing anesthesia.
Therefore, the present meta-analysis of randomized controlled
trials was conducted to systematically review the preventive
effects on the occurrence of PRAEs in pediatric anesthesia.
Materials and methods
Protocol registration
The present study was conducted according to the
Preferred Reporting Items for Systematic Review and Meta-Analyses
guidelines (9)and registered in
the PROSPERO database (crd.york.ac.uk/prospero/; ID no. CRD42021268935).
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: i) Prospective
randomized controlled trials comparing dexmedetomidine with placebo
or other drugs and published in English; ii) participants included
in studies were children aged 0-18 years receiving general
anesthesia; iii) primary outcome measures were the incidence of
PRAEs, including breath holding or apnea, laryngospasm,
bronchospasm, arterial oxygen desaturation, cough, fever and
pulmonary rales and secondary outcome measures were the incidence
of emergence agitation (EA), recovery time, post-anesthesia care
unit (PACU) stay duration and heart rate. Exclusion criteria were
as follows: i) Studies on animals; ii) non-randomized clinical
trials; iii) participants with other serious respiratory conditions
that may influence the prognosis and incidence of PRAEs and iv)
studies with insufficient data for analysis.
Search strategy
The databases, including Cochrane Library(cochranelibrary.com/), PubMed (https://pubmed.ncbi.nlm.nih.gov/) and
EMBASE(https://www.embase.com/), were searched
for studies up to May 2, 2022. The multi-search strategy was
employed as follows: i) dexmedetomidine; ii) infants or toddlers or
child or pediatric or pediatric or childhood; iii) ‘respiratory
complications’ or ‘adverse respiratory events’ or ‘perioperative
respiratory adverse events’ or ‘airway complications’ or
‘respiratory depression’; iv) random or trial or placebo or
‘randomized controlled trial’ and v) i, ii, iii and iv. Relevant
references were searched online and included or excluded according
to the aforementioned criteria. The titles and abstracts of the
studies were evaluated independently by two assessors (YL and JY).
For trials that met the inclusion criteria, data extraction from
the full text was performed. Full search strategy for all databases
are shown in Tables SI and
SII and Fig. S1.
Quality assessment and data
extraction
A total of two reviewers extracted the data from the
relevant studies independently. YL and JY assessed and scored the
validity. This was checked by a third researcher (YZ) using the
Jadad scoring system (Table SIII)
(10) which primarily considers
randomization (2 points), double blinding (2 points) and
description of drop-outs (1 point). The following information was
extracted: First author, published year, intervention, age, sample
size, type of procedure and results.
Statistical analysis
Review Manager software 5.4 (Cochrane) was used to
perform data analysis. For dichotomous data, number of participants
experiencing the events in each group was recorded. Continuous data
are reported as the mean ± SD. Incidence of PRAEs was assessed with
the odds ratio (OR) and its 95% CI. The heterogeneity between
studies was evaluated by I2 statistic (ranging from 0 to
100%) and χ2 test. I2>50% was considered
to have significant heterogeneity. A random effect model was used
when I2>50% and subgroup analysis was performed to
determine the possible sources of heterogeneity. A fixed effects
model (the Mantel-Haenszel method) was used when I2≤50%.
Publication bias was evaluated according to Egger's test using
Stata 13.1 software (Stata). P<0.05 was considered to indicate a
statistically significant difference.
Results
Included trials and
characteristics
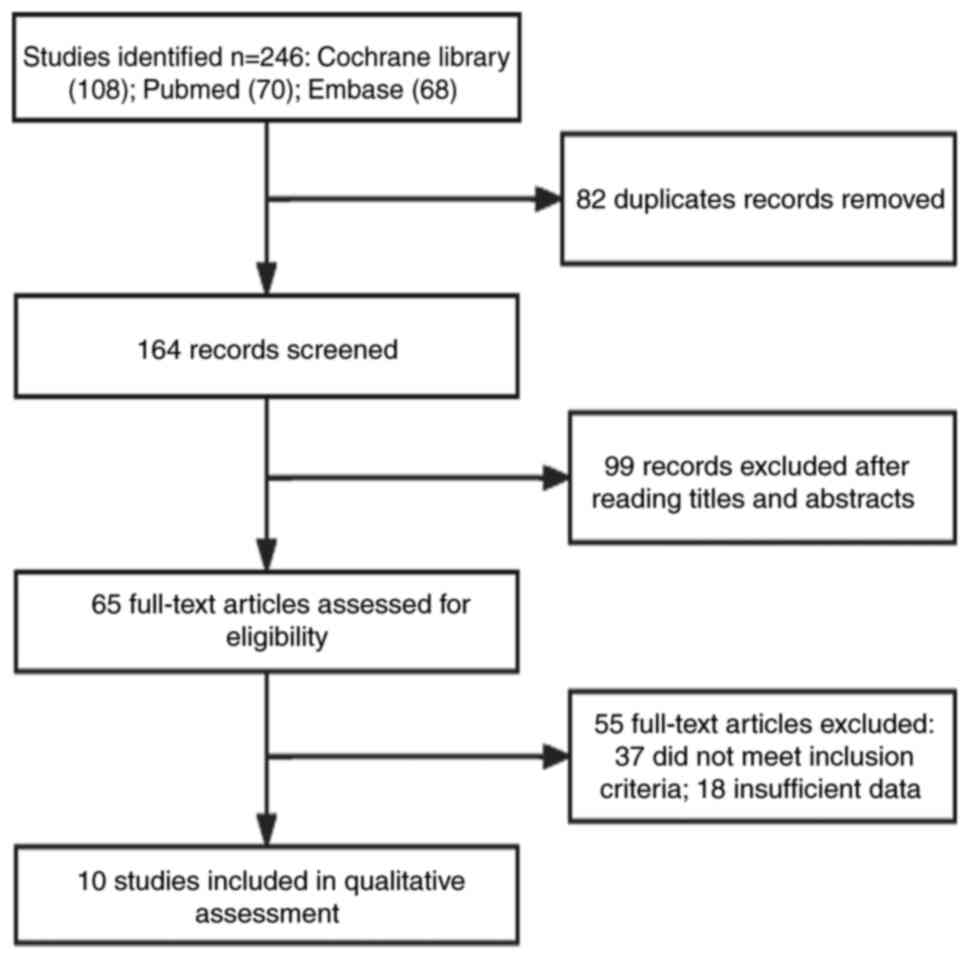
Fig. 1 shows study
screening and selection strategy. Briefly, comprehensive search of
Cochrane Library, EMBASE and PubMed was performed. This produced
246 records of which 82 duplicated records were removed manually.
By screening the title, abstract and full-text of the remaining 164
citations, 99 records and 55 records were excluded based on the
title/abstract and full text, respectively. Finally, 10 eligible
studies with 1,056 patients were included in meta-analysis
(11-20)
and relevant data were extracted.
Table I summarizes
the characteristics of the included studies. A total of 21
participants in three trials dropped out. Participants in three
trials (11-13)
were children aged 0-5 years-old, while patients in the other seven
trials (14-20)
were 2-13 years-old. Participants in three trials underwent foreign
body removal and four trials performed tonsillectomy. A total of
three studies involved minor surface, eye or vitreoretinal surgery.
In 10 trials, sevoflurane with or without propofol was used for
induction and maintenance of anesthesia. In five trials, intubation
was performed and in four trials, laryngeal mask airway (LMA) was
used. Patients in one trial had airways managed using face mask
ventilation without airway instrumentation. Propofol (3 mg/kg),
fentanyl (2 µg/kg) and cisatracurium (0.2 mg/kg) were intravenously
injected after 3 min preoxygenation with a mask (100% oxygen; 6
l/min) before suitable LMA or endotracheal tube (ETT) was placed.
In two trials (8,15), dexmedetomidine were administered
intranasally 40-60 min before induction of anesthesia. In eight
trials, a loading dose of dexmedetomidine was given and
continuously pumped until the end of surgery.
 | Table ICharacteristics of included
studies. |
Table I
Characteristics of included
studies.
| First author,
year | n | Patient age
(years) | Procedure | Anesthesia
method | Intervention and
groups | Jadad score | (Refs.) |
|---|
| Bi et al
2019 | 40 | 0-4 | FB removal | Sevoflurane,
LMA | DEX (n=20): DEX, 1
µg/kg intranasal; P (n=20): Normal saline 25 min before anesthesia
induction. | 5 | (11) |
| Cai et al
2013 | 80 | 0-4 | FB removal | Spontaneous
ventilation | SV (n=40): DEX (4
µg/kg) i.v. and topical lidocaine (3-5 mg/kg); MJV (n=40): Fentanyl
(2 µg/kg) i.v., propofol (3-5 mg/kg) i.v., succinylcholine (1
mg/kg) i.v. | 3 | (12) |
| Chen et al
2014 | 77 | 0-5 | FB removal | Sevoflurane,
LMA | DEX (n=39): DEX4
µg/kg i.v. then 1-2 µg/kg/h; R (n=38): R 0.05 µg/kg/min i.v.
pumping | 4 | (13) |
| Di et al
2017 | 75 | 3-7 | Tonsillectomy | Sevoflurane,
intubation | DEX1 (n=25): DEX 1
µg/kg i.v.; DEX2 (n=25): DEX 2 µg/kg i.v.; P (n=25): Saline i.v.
over 10 min before anesthesia induction. | 4 | (14) |
| Hauber et al
2015 | 393 | 4-10 | Tonsillectomy | Propofol,
intubation | DEX (n=195): DEX
0.5 µg/ml i.v.; P (n=198): Equivalent volume saline i.v. 5 min
before the completion of surgery | 4 | (15) |
| He et al
2013 | 87 | 3-7 | Minor surface
surgery | Sevoflurane,
LMA | DEX1 (n=29): DEX
0.5 µg/kg i.v.; DEX2 (n=32): DEX 1 µg/kg i.v.; P (n=26): Saline
infusion for 10 min | 4 | (16) |
| Koceroglu et
al 2019 | 60 | 2-9 | Tonsillectomy | Sevoflurane,
intubation | DEX (n=30): DEX 1
µg/kg i.v.; T (n=30): T 1.5 mg/kg i.v. for 10 min prior to the end
of surgery | 3 | (17) |
| Qiao et al
2017 | 124 | 2-5 | Eye surgery | Propofol, LMA | DEX (n=42): DEX 2.5
µg/kg intranasal; DK (n=41): Intranasal DEX 2 µg/kg and oral
ketamine 3 mg/kg; K (n=41): Oral ketamine 6 mg/kg | 5 | (18) |
| Xu et al
2012 | 60 | 3-7 | Vitreoretinal
surgery | Sevoflurane,
intubation | DEX (n=30): DEX 0.5
µg/kg i.v.; P (n=30): Normal saline i.v. over 10 min | 4 | (19) |
| Zhuang et al
2011 | 60 | 2-13 | Tonsillectomy | Sevoflurane,
intubation | DEX (n=30): DEX 1.0
µg/kg i.v.; M (n=30): M 100 µg/kg i.v. | 4 | (20) |
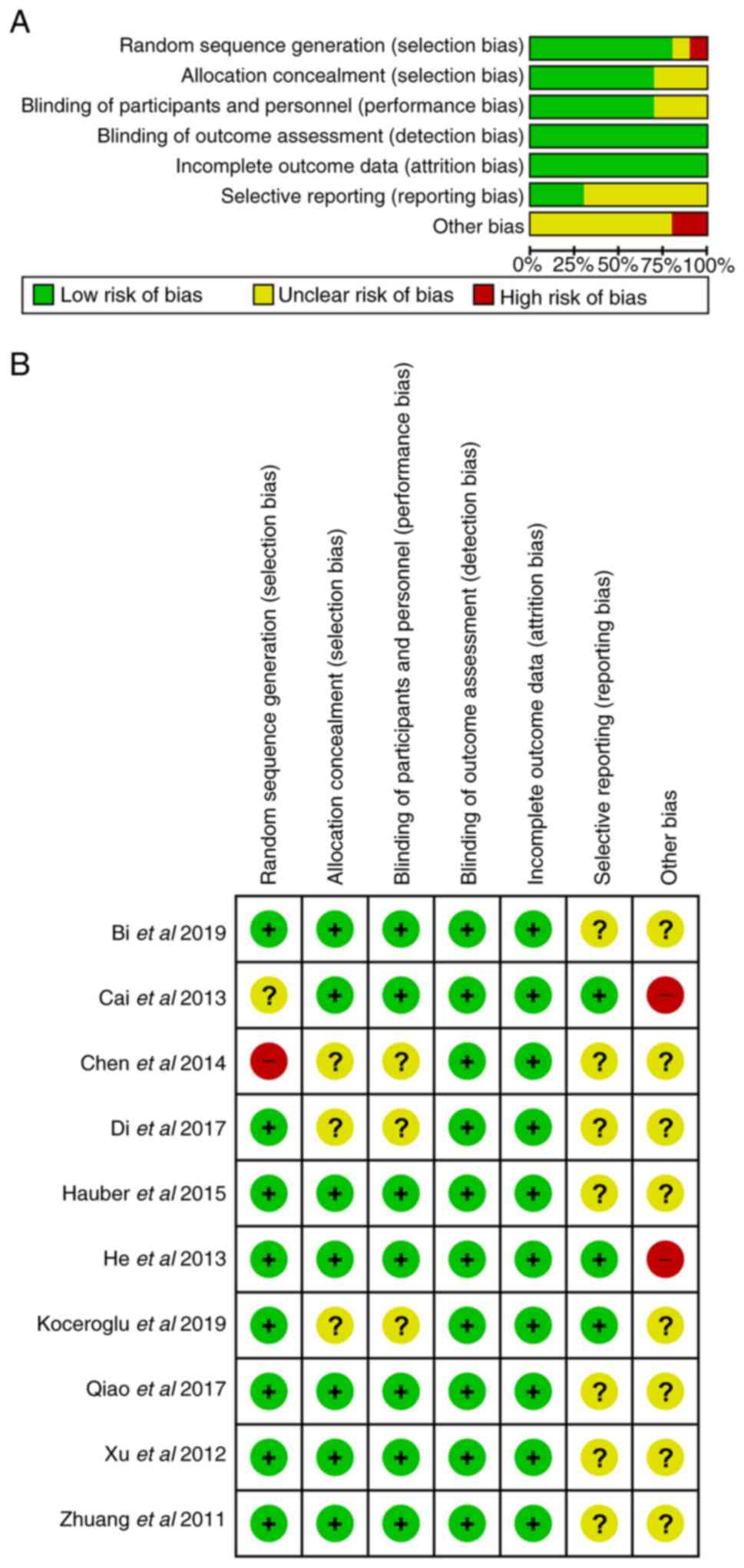
Risk of bias assessment
The risk of bias graph indicated good methodology
(Fig. 2A) as most included studies
had a low risk of bias. Only two studies were rated as high risk of
bias as they did not state the method of sample size determination
(Fig. 2B).
Pooled results of the included
studies
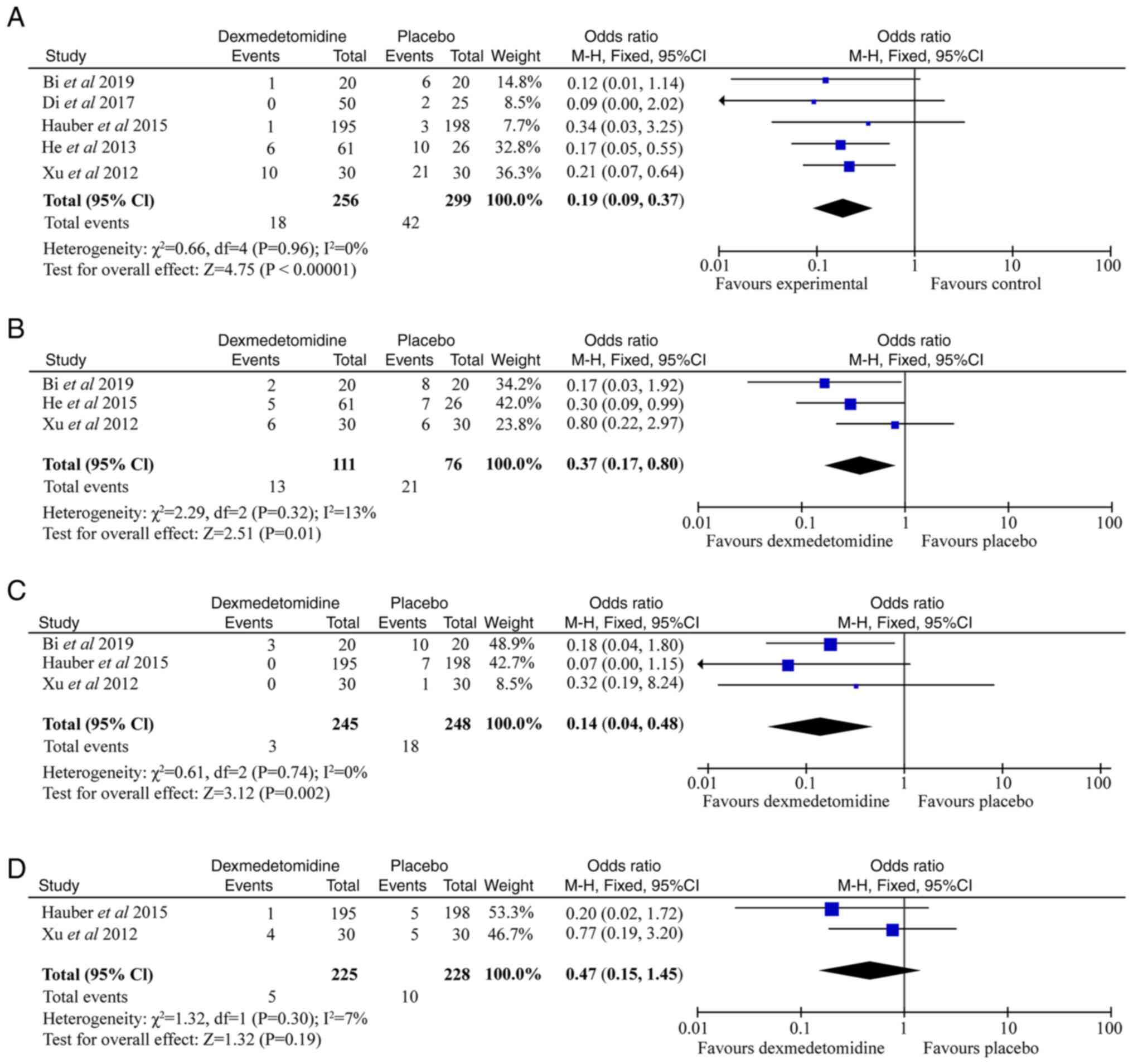
Firstly, the impact of dexmedetomidine on PRAEs was
analyzed. A total of five trials (655 patients) was included for
analysis of the impact of dexmedetomidine on coughing. Incidence of
coughing was significantly decreased in the dexmedetomidine
compared with the placebo group and heterogeneity was not observed
(OR 0.19; 95% CI 0.09-0.37; I2 =0%; P<0.05; Fig. 3A). A total of three trials (187
patients) was included for analysis of the impact of
dexmedetomidine on breath holding (Fig. 3B). The risk of breath holding was
significantly decreased in the dexmedetomidine group when compared
with placebo group and heterogeneity was not observed (OR 0.37; 95%
CI 0.17-0.8; I2=13%; P<0.05). A total of three trials
(493 patients) was included for analysis of the impact of
dexmedetomidine on laryngospasm. Risk of laryngospasm was
significantly reduced in the dexmedetomidine compared with the
placebo group and heterogeneity was not observed (OR 0.14; 95% CI
0.04-0.48; I2=0%; P<0.05; Fig. 3C). A total of two trials (453
patients) was included for analysis of the impact of
dexmedetomidine on desaturation (Fig.
3D). Compared with placebo group, no significant change in
incidence of desaturation was observed after treatment with
dexmedetomidine (OR 0.47; 95% CI 0.15-1.45; I2=7%;
P>0.05).
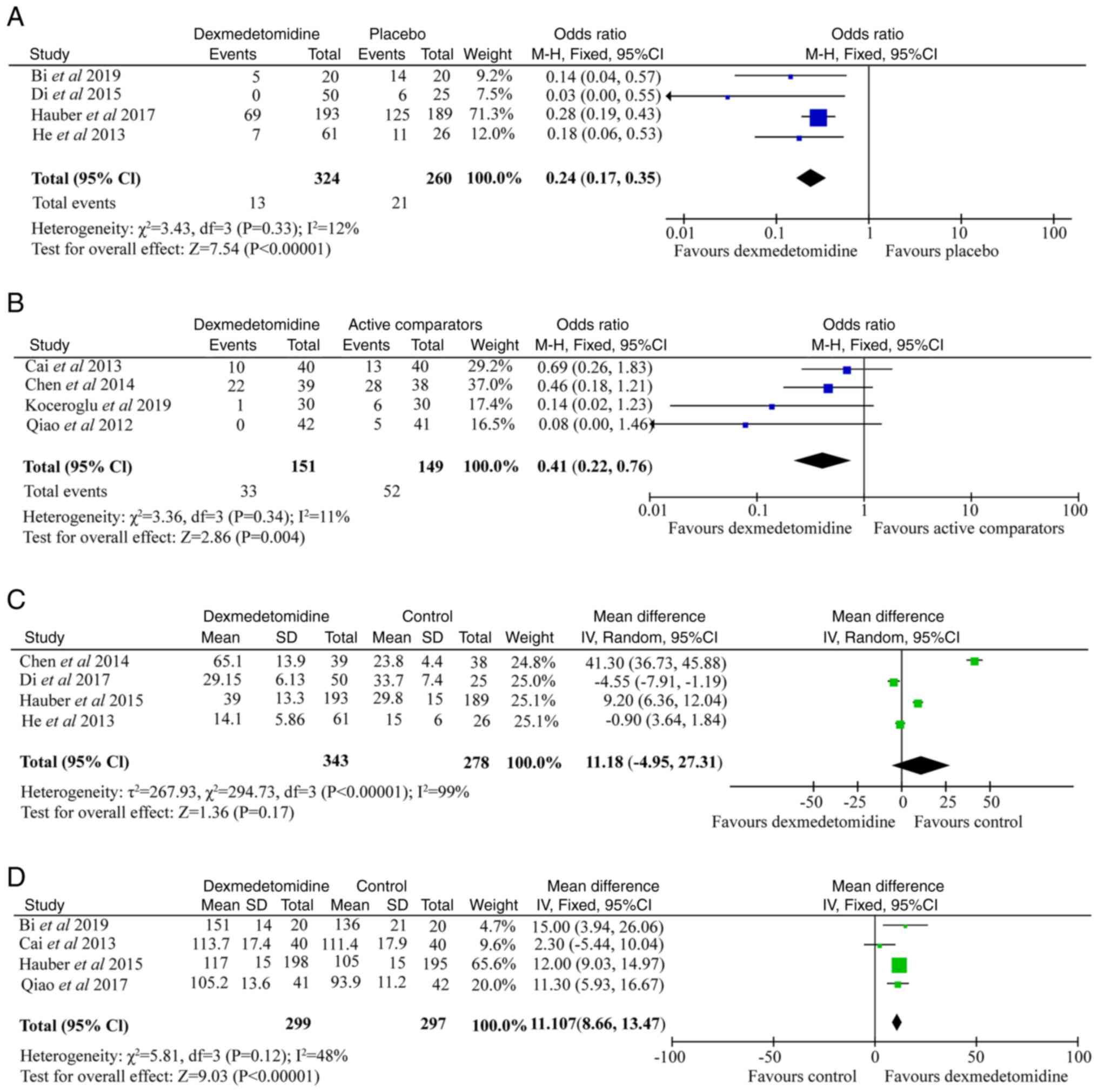
The effect of dexmedetomidine on EA was analyzed. A
total of four trials (584 patients) was included for analysis of
the impact of dexmedetomidine on EA (Fig. 4A). Compared with saline, children
in the dexmedetomidine group experienced a significant decrease of
EA (OR 0.24; 95% CI 0.17-0.35; I2=12%; P<0.05).
Dexmedetomidine vs. active
comparators
There were four studies that used an active
comparator as the control group, including fentanyl, ketamine,
remifentanil and tramadol. These trials (300 patients) were
included for analyzing of the impact of dexmedetomidine on PRAEs
(Fig. 4B). The incidence of PRAEs
was significantly reduced in the dexmedetomidine group compared
with the active comparators group, however, no significant
heterogeneity was observed (OR 0.41; 95% CI 0.22-0.76;
I2=11%; P<0.05).
Dexmedetomidine vs. morphine
Only one study (60 patients) compared the effects of
dexmedetomidine and morphine on PRAEs (17). The study recorded end-tidal carbon
dioxide, Children's Hospital of Eastern Ontario Pain Scale score
and supplementary morphine administration. The results showed that
respiratory depression of dexmedetomidine was less than that of
morphine, but the analgesic effect was poor.
Safety outcomes
PACU stay duration in four trials (621 patients) was
evaluated. Compared with control group, dexmedetomidine increased
PACU stay duration by 11.18 min (OR 6.56; 95% CI 4.97-8.16;
I2=99%; P<0.05; Fig.
4C). A total of four trials (596 patients) was included for
analyzing the impact of dexmedetomidine on heart rate (Fig. 4D). The heart rate of the
dexmedetomidine group was lower than that in the control group (OR
11.07; 95% CI 8.66-13.47; I2=48%; P<0.05). However,
none of the patients required treatment for bradycardia.
Testing for publication bias
Funnel plots of the outcome of coughing, breath
holding, laryngospasm, desaturation and heart rate treatment with
dexmedetomidine and placebo in the included studies demonstrated
symmetry, indicating there was no serious publication bias
(Fig. S2A-D, H). Three funnel
plots of the outcome of EA, the overall PRAEs and PACU stay
duration treatment with dexmedetomidine and placebo or active
comparators in the included studies demonstrated there was
significant publication bias (Fig.
S2E, F, G). However, the number of trials included was <10,
thus this conclusion may not be entirely accurate.
Discussion
The present meta-analysis demonstrated the
protective effect of dexmedetomidine on PRAEs. Treatment with
dexmedetomidine decreased the incidence of PRAEs, including
coughing, breath holding and laryngospasm. Dexmedetomidine most
potently decreased the incidence of EA and exhibited a significant
effect on heart rate and PACU stay duration.
PRAEs remain a major risk in pediatric anesthesia
(4). There was a broad range of
PRAE rates in the included trials, this may be because young age is
associated with higher risk PRAEs (2). The rate of PRAEs is also associated
with the type of surgery (21).
For example, the incidence of PRAEs is higher in foreign body
removal compared with other types of surgery, such as tonsillectomy
(22). The definition of PRAEs,
such as, breath holding or apnea, laryngospasm, bronchospasm,
arterial oxygen desaturation, cough, fever and pulmonary rales, was
chosen based on preliminary assessment of the published literature
(2). Coughing may be a precursor
of laryngeal spasm (12). Studies
have shown that anesthesia for patients with a respiratory
infection increases the risk of complications, including laryngeal
spasm, bronchospasm, atelectasis and arterial oxygen desaturation
(21,23). These changes are typically
transient and well-tolerated by most adult patients, but may be
deleterious in children (2).
It is widely accepted that decreased PRAEs are
associated with airway management or anesthesia (2,24).
Numerous studies have shown that the use of LMAs has a lower
incidence of PRAEs compared with ETT in children (2,25).
However, a few studies (4,26) report the association between
dexmedetomidine and airways. Dexmedetomidine possesses sedative,
analgesic and anxiolytic effects without causing respiratory
depression (6). These properties
render dexmedetomidine a potential useful drug for airway
protection (27). The present data
demonstrated that dexmedetomidine significantly attenuated the
incidence of PRAEs and improved the airway function. Compared with
the active comparators group, dexmedetomidine significantly
decreased the incidence of PRAEs and there was no respiratory
depression in children.
However, compared with opioids, dexmedetomidine has
a weak analgesic effect (28).
Dexmedetomidine cannot replace the analgesic effect of opioids in
general anesthesia and can only be used as an auxiliary drug for
general anesthesia (29).
EA is a common complication after inhaled anesthesia
in children (30). Although EA is
typically self-limited, it can lead to patient injury and increase
hospital length of stay and utilization of PACU resources (27). Many anesthetics and anesthesia
adjuncts (dexmedetomidine, opioids, midazolam, propofol and
clonidine) attenuate the incidence of EA (10). Consistent with a previous study
(31), the present meta-analysis
supported the use of dexmedetomidine as an effective drug to
prevent EA.
Hypotension and bradycardia are the most common
hemodynamic adverse effects because of the direct effect of
dexmedetomidine on the α2 adrenoceptor (8). Koceroglu et al (17) found that bradycardia may be more
common with the use of dexmedetomidine. The heart rate effects of
dexmedetomidine are associated with rate of infusion and dose
(29). The heart rate-lowering
effect of dexmedetomidine is dose-dependent: The higher the dose of
dexmedetomidine, the lower the heart rate (32). At the same time, high dose of
dexmedetomidine may prolong the postoperative recovery time
(5). Consistently, the present
analysis showed that dexmedetomidine decreased heart rate and
increased PACU stay duration by 11.18 min. However, none of the
patients required treatment for bradycardia.
There are limitations in the present meta-analysis.
First, the small sample size limited the presented study. Second,
routes of administration and dose of dexmedetomidine may be biased
by small study effect. Finally, airway management was not analyzed
in subgroups. As a result, more well-designed high-quality studies
are required to draw definitive conclusions.
In conclusion, comprehensive literature search found
a few reports of PRAEs in children and the present data
demonstrated that dexmedetomidine reduced the incidence of PRAEs
and improved airways. More importantly, dexmedetomidine has fewer
side effects compared with opioid analgesics. These results may
affect the choice of anesthetic in children. The present analysis
demonstrated dexmedetomidine had a beneficial effect on children
receiving general anesthesia in regard to preventing PRAEs. Further
studies should identify the effect of age, type of surgery and
patient characteristics on PRAE occurrence.
Supplementary Material
Embase search strategy.
Dexmedetomidine and (infants or toddlers or child or pediatric or
childhood) and (‘respiratory complications’ or ‘adverse respiratory
events’ or ‘perioperative respiratory adverse events’ or ‘airway
complications’ or ‘respiratory depression’) and (random or trial or
‘randomized controlled trial’) and in humans.
Funnel chart for each forest map.
Funnel plot of (A) coughing, (B) breath holding, (C) laryngospasm,
(D) desaturation, (E) emergence agitation, (F) overall
perioperative respiratory adverse events, (G) post-anesthesia care
unit stay duration and (H) heart rate.
Comprehensive search of Cochrane
Library
Comprehensive search of PubMed.
Jadad scoring system for validity
assessment.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JZ and HY confirm the authenticity of all the raw
data. HY made substantial contributions to conception and design.
JY, YL and YZ designed the meta-analysis. JZ and YB analyzed data.
JZ wrote the manuscript. All authors have read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Li L, Zhang Z, Yao Z, Wang HJ, Wang HB, An
H and Yao J: The impact of laryngeal mask versus other airways on
perioperative respiratory adverse events in children: A systematic
review and meta-analysis of randomized controlled trials. Int J
Surg. 64:40–48. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Drake-Brockman TFE, Ramgolam A, Zhang G,
Hall GL and von Ungern-Sternberg BS: The effect of endotracheal
tubes versus laryngeal mask airways on perioperative respiratory
adverse events in infants: A randomised controlled trial. Lancet.
389:701–708. 2017.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Gupta N, Rath GP, Prabhakar H and Dash HH:
Effect of intraoperative dexmedetomidine on postoperative recovery
profile of children undergoing surgery for spinal dysraphism. J
Neurosurg Anesthesioly. 25:271–278. 2013.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bong CL, Tan J, Lim S, Low Y, Sim SW,
Rajadurai VS, Khoo PC, Allen J, Meaney M and Koh WP: Randomised
controlled trial of dexmedetomidine sedation vs general anaesthesia
for inguinal hernia surgery on perioperative outcomes in infants.
Br J Anaesth. 122:662–670. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bhat R, Mudukanagoudar M, Shetty S and
Kamath S: Study of dose related effects of dexmedetomidine on
laryngeal mask airway removal in children-A double blind randomized
study. Anaesthesia Pain Intensive Care. 22:368–373. 2018.
|
|
6
|
Chrysostomou C and Schmitt CG:
Dexmedetomidine: Sedation, analgesia and beyond. Expert Opin Drug
Metab Toxicol. 4:619–627. 2008.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Shi M, Miao S, Gu T, Wang D, Zhang H and
Liu J: Dexmedetomidine for the prevention of emergence delirium and
postoperative behavioral changes in pediatric patients with
sevoflurane anesthesia: A double-blind, randomized trial. Drug Des
Devel Ther. 13:897–905. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Grant MJ, Schneider JB, Asaro LA, Dodson
BL, Hall BA, Simone SL, Cowl AS, Munkwitz MM, Wypij D and Curley
MA: Dexmedetomidine use in critically Ill children with acute
respiratory failure. Pediatr Crit Care Med. 17:1131–1141.
2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Moher D, Shamseer L, Clarke M, Ghersi D,
Liberati A, Petticrew M, Shekelle P and Stewart LA: PRISMA-P Group.
Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Syst Rev. 4(1)2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Peng K, Wu SR, Ji FH and Li J:
Premedication with dexmedetomidine in pediatric patients: A
systematic review and meta-analysis. Clinics (Sao Paulo).
69:777–786. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Bi Y, Ma Y, Ni J and Wu L: Efficacy of
premedication with intranasal dexmedetomidine for removal of
inhaled foreign bodies in children by flexible fiberoptic
bronchoscopy: A randomized, double-blind, placebo-controlled
clinical trial. BMC Anesthesiol. 19(219)2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Cai Y, Li W and Chen K: Efficacy and
safety of spontaneous ventilation technique using dexmedetomidine
for rigid bronchoscopic airway foreign body removal in children.
Paediatr Anaesth. 23:1048–1053. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Chen KZ, Ye M, Hu CB and Shen X:
Dexmedetomidine vs remifentanil intravenous anaesthesia and
spontaneous ventilation for airway foreign body removal in
children. Br J Anaesth. 112:892–897. 2014.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Di M, Han Y, Yang Z, Liu H, Ye X, Lai H,
Li J, ShangGuan W and Lian Q: Tracheal extubation in deeply
anesthetized pediatric patients after tonsillectomy: A comparison
of high-concentration sevoflurane alone and low-concentration
sevoflurane in combination with dexmedetomidine pre-medication. BMC
Anesthesiol. 17(28)2017.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Hauber JA, Davis PJ, Bendel LP, Martyn SV,
McCarthy D, Ecans MC, Cladis FP, Cunningham S, Lang RS, Campbell
NF, et al: Dexmedetomidine as a rapid bolus for treatment and
prophylactic prevention of emergence agitation in anesthetized
Children. Anesth Analg. 121:1308–1315. 2015.PubMed/NCBI View Article : Google Scholar
|
|
16
|
He L, Wang X, Zheng S and Shi Y: Effects
of dexmedetomidine infusion on laryngeal mask airway removal and
postoperative recovery in children anaesthetised with sevoflurane.
Anaesth Intensive Care. 41:328–333. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Koceroglu I, Devrim S, Bingol Tanriverdi T
and Gura Celik M: The effects of dexmedetomidine and tramadol on
post-operative pain and agitation, and extubation quality in
paediatric patients undergoing adenotonsillectomy surgery: A
randomized trial. J Clin Pharm Ther. 45:340–346. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Qiao H, Xie Z and Jia J: Pediatric
premedication: A double-blind randomized trial of dexmedetomidine
or ketamine alone versus a combination of dexmedetomidine and
ketamine. BMC Anesthesiol. 17(158)2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Lili X, Jianjun S and Haiyan Z: The
application of dexmedetomidine in children undergoing vitreoretinal
surgery. J Anest. 26:556–561. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zhuang PJ, Wang X, Zhang XF, Zhou ZJ and
Wang Q: Postoperative respiratory and analgesic effects of
dexmedetomidine or morphine for adenotonsillectomy in children with
obstructive sleep apnoea. Anaesthesia. 66:989–993. 2011.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mamie C, Habre W, Delhumeau C, Argiroffo
CB and Morabia A: Incidence and risk factors of perioperative
respiratory adverse events in children undergoing elective surgery.
Paediatr Anaesth. 14:218–224. 2004.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Wang L, Wei L and Deng X: Other factors
affect the occurrence of perioperative respiratory adverse events.
Anesthesiology. 130:507–508. 2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Steward DJ: Assessment of pediatric
patients for general anesthesia: The child with an upper
respiratory infection and the ex-premature infant. Semin Pediatr
Surg. 8:13–17. 1999.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Al-Mazrou KA, Abdullah KM, ElGammal MS,
Ansari RA, Turkistani A and Abdelmeguid ME: Laryngeal mask airway
vs. uncuffed endotracheal tube for nasal and paranasal sinus
surgery: paediatric airway protection. Eur J Anaesthesiol.
27:16–19. 2010.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kaplan A, Crosby GJ and Bhattacharyya N:
Airway protection and the laryngeal mask airway in sinus and nasal
surgery. Laryngoscope. 114:652–655. 2004.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Mason KP and Lerman J: Review article:
Dexmedetomidine in children: Current knowledge and future
applications. Anesth Analg. 113:1129–1142. 2011.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Shukry M, Clyde MC, Kalarickal PL and
Ramadhyani U: Does dexmedetomidine prevent emergence delirium in
children after sevoflurane-based general anesthesia? Paediatr
Anaesth. 15:1098–1104. 2005.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Sheta SA, Al-Sarheed MA and Abdelhalim AA:
Intranasal dexmedetomidine vs midazolam for premedication in
children undergoing complete dental rehabilitation: A
double-blinded randomized controlled trial. Paediatr Anaesth.
24:181–189. 2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Pestieau SR, Quezado ZMN, Johnson YJ,
Anderson JL, Cheng YI, McCarter RJ, Choi S and Finkel J: High-dose
Dexmedetomidine increases the opioid-free interval and decreases
opioid requirement after tonsillectomy in children. Can J Anaesth.
58:540–550. 2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Ni J, Wei J, Yao Y, Jiang X, Luo L and Luo
D: Effect of dexmedetomidine on preventing postoperative agitation
in children: A meta-analysis. PLoS One. 10(e0128450)2015.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Guler G, Akin A, Tosun Z, Ors S, Esmaoglu
A and Boyaci A: Single-dose dexmedetomidine reduces agitation and
provides smooth extubation after pediatric adenotonsillectomy.
Paediatr Anaesth. 15:762–766. 2005.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Mostafa MF, Abdel Aal FA, Ali IH, Ibrahim
AK and Herdan R: Dexmedetomidine during suprazygomatic maxillary
nerve block for pediatric cleft palate repair, randomized
double-blind controlled study. Korean J Pain. 33:81–89.
2020.PubMed/NCBI View Article : Google Scholar
|