Introduction
Surgical ciliated cyst (SCC), also known as
postoperative maxillary cyst, paranasal cyst, or respiratory
implantation cyst, was first described by Kubo in 1927 in the
Japanese literature (1) as a
maxillary cyst after treatment of chronic maxillary sinusitis. In
the Japanese population, this lesion accounts for up to 20% of
maxillary cysts (2), being the
largest published series of 71 cases of postoperative maxillary
cysts (3). However, to date, few
reports have been published in the English literature on non-Asian
populations (4).
SCC is a benign lesion that is considered a late
complication, as it can develop from a few months to several years
after an initial surgical procedure or trauma involving the
maxillary sinus or midface (4). It
is assumed to arise from unintentional entrapment of the maxillary
sinus mucosa in patients with a history of Caldwell-Luc
antrostomies, orthognathic surgery, and sinus lift procedures, or
in association with midface trauma involving the maxillary sinus
(5).
In the present clinical report, we describe an
interesting case of a patient with a large SCC located in the
maxilla that was found 20 years after a LeFort I osteotomy that had
been performed to correct a class II dentofacial deformity.
Therefore, we extensively discuss the main clinical-radiological,
histological findings and appropriate management of this unusual
pathology among the Spanish population compared to the Asian
literature.
Case report
A healthy 41-year-old woman came to the Department
of Oral and Maxillofacial Surgery, Virgen del Rocio University
Hospital (Seville, Spain) in September 2020 due to swelling in the
maxillary region and intense and progressive pain of two months
evolution. Previously, her dentist had medicated her with
antibiotics and analgesics and performed endodontic treatment on
the upper lateral incisor because of worsening pain, in an attempt
to eliminate any focus of dental inflammation, without clinical
improvement. Her medical history highlighted that, 20 years
earlier, she had undergone orthognathic surgery at our centre to
correct an Angle class II malocclusion and vertical excess by means
of bimaxillary advancement using LeFort I osteotomy and bilateral
ramus sagittal osteotomy with genioplasty.
Physical examination revealed a midfacial deformity
in the premaxilla and nostrils with a slight airflow limitation.
Intraoral view showed an expansion of the vestibular and palatal
cortex in the anterior maxilla. Palpation detected a fluctuating
and painful swelling with an overlying normal mucosa. No discharge
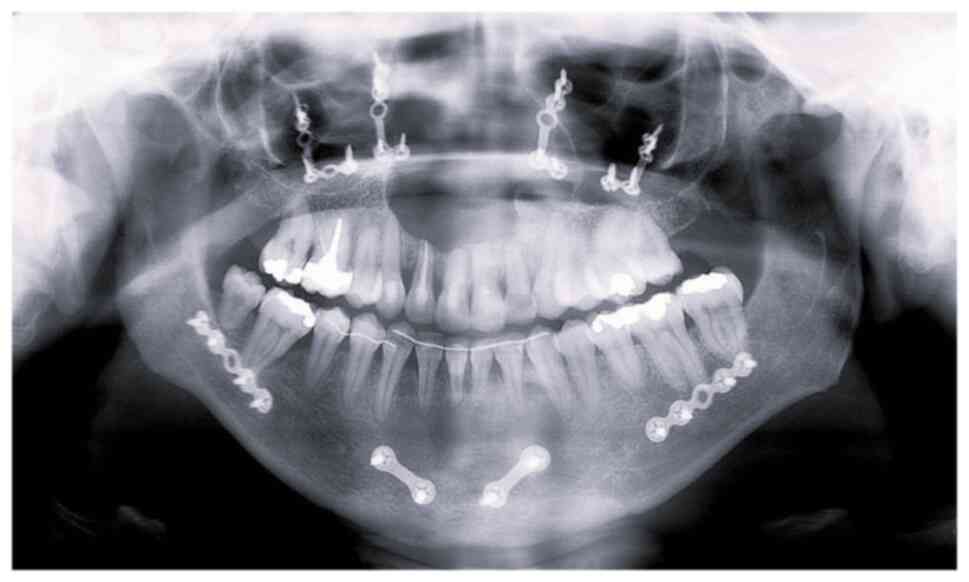
or oronasal fistula was identified. Panoramic radiography revealed
a rounded, well-defined unilocular radiolucent lesion in the
central region of the maxilla, 3.5 cm in size, which did not appear
to be related to neighbouring teeth (Fig. 1). Four L-shaped titanium plates in
the maxilla and four straight ones in the mandible associated with
previous orthognathic surgery, fixed with screws, were observed.
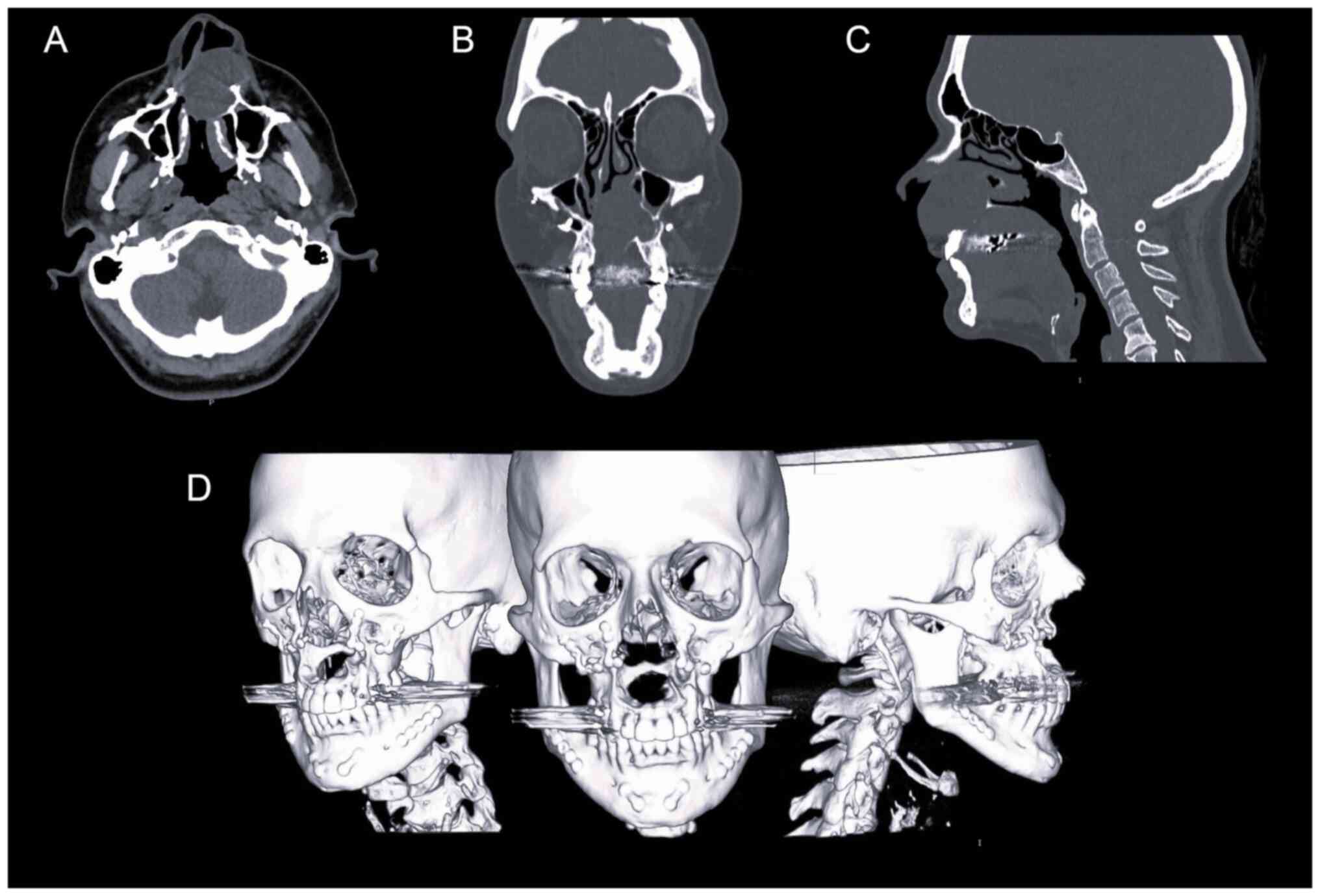
Computed tomography (CT) demonstrated an extensive and well-defined
unilocular cystic lesion, measuring 4.3x3.7x3.7 cm, located in the
centre of the anterior maxillary region, involving the apical
region of the maxillary incisor, and fenestrating the vestibular
and palatal cortical bone, affecting the floor of the pyriform
aperture (Fig. 2). Under local
anaesthesia, a preoperative incisional biopsy was taken, which
confirmed the benign nature of the lesion. The diagnostic
hypothesis was a cystic lesion.
Treatment consisted of cyst enucleation and removal
of the osteosynthesis material intraorally under general
anaesthesia. During surgery, the cystic lesion was found to be
easily enucleable and communicated with the nasal cavity but not
with the maxillary sinus. No dental focus was found in relation to
the lesion. Bone reconstruction was not necessary.
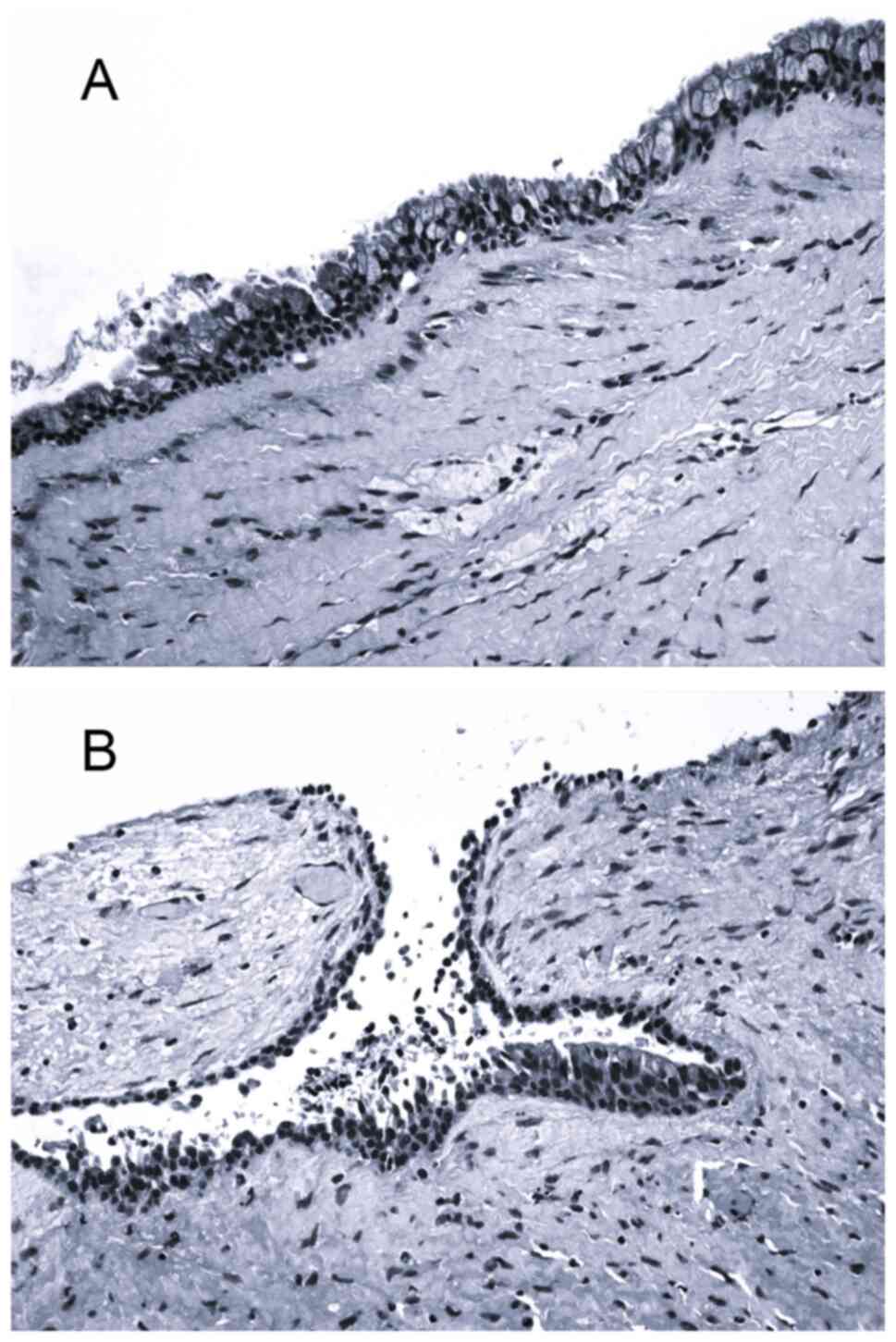
Histopathological examination confirmed the presence of a cystic
lesion with fibrous walls and a pseudostratified ciliated columnar
epithelium lining with mucus-secreting cells, consistent with a
ciliated cyst (Fig. 3). On the
basis of the clinical-radiological and microscopic findings, a
diagnosis of non-odontogenic SCC was made. No postoperative
complications were identified, and the site healed uneventfully.
The patient is doing well after 24 months of follow-up. CT scans
showed progressive regeneration of the bone cavity, with no
evidence of recurrence of the lesion.
Discussion
SCC is a rare pathology that is normally located in
the maxilla and arises as a complication of a previous aggressive
surgical procedure involving the maxillary sinuses and bone. They
have been reported more frequently in the Japanese literature,
probably due to the high prevalence of chronic sinusitis in that
country and the preference for surgical treatment over antibiotics
(4). This variable incidence has
also been attributed to some extent to underdiagnosis or
misdiagnosis of expanding mucoceles, as well as differences in
facial bone structure between ethnic groups. The lack of reports is
possibly related to the late presentation of these types of cysts,
which are usually diagnosed 15-20 years after initial surgery
(range 3-60 years) (6). In this
case, the patient presented with a large maxillary cyst found 20
years after a LeFort I osteotomy. They are detected in the fourth
or fifth decade of life, with a variable gender distribution
(7).
SCC is probably an iatrogenic consequence of
entrapment of the maxillary sinus mucosa during radical surgery. It
is generally lined by a respiratory-type pseudostratified columnar
epithelium compatible with the Schneider membrane, although mixed
patterns with simple columnar, cuboidal, or squamous epithelium
have been described in the literature (8). The appearance of SCC after
orthognathic surgery is an exceptional complication that has rarely
been reported (5,9,10).
During a LeFort I osteotomy, the mucosal cells of the maxillary
sinuses, nasal sinuses, and nasopalatal mucosa can become embedded
between the bony edges of the osteotomies (10). Over time, these trapped cells can
undergo cystic degeneration and, subsequently, expansion caused by
the osmotic difference with locoregional tissue (11). In the mandible, respiratory
epithelium transplantation has been associated with the use of
nasal osteocartilage graft and maxillary bone graft used to
stabilize genioplasty (12,13).
These cysts could also arise from accidental transport of the sinus
mucosa on the saw blade during bimaxillary surgeries (14).
The main clinical signs of SCC are progressive
maxillary swelling, facial deformity, severe pain, and nasal or
oral discharge. The most common location is the lateral and
posterior wall of the maxilla, although they have also been
described in the central region, the infraorbital rim, and the
medial canthal region (4). In this
case, the patient presented all the above clinical signs except the
oronasal fistula, the main reason for consultation being severe and
progressive pain. In its initial stage, it can be completely
asymptomatic and can be discovered on routine x-rays, but as it
expands, it gradually causes pain or infection. Clinically, this
cyst behaves like a solitary, unilateral, but locally aggressive
lesion. As it increases in size, the cyst can displace or perforate
the sinus and nasal walls and invade adjacent tissues.
Radiographically, it is characterized by a
well-defined, expansive, unilocular, or multilocular radiolucent
image close to the sinus and the previous surgical or traumatic
area (6). Even though panoramic
and Waters radiographs are the imaging modalities initially used,
CT is recommended to fully assess the lesion and select the best
treatment (10). Despite the low
number of SCCs reported in the Western literature, this lesion
should be considered in the differential diagnosis of cystic
lesions in patients with a history of risk. The clinical and
radiographic characteristics of these lesions can mimic those of
inflammatory cysts of dental origin. In the present case, these
typical radiographic features were observed. Assuming that their
clinical radiographic features may resemble those of inflammatory
cysts of dental origin, pulp vitality tests may help in the
differential diagnosis, although they are often inconclusive. The
patient had root resorption and her dentist had previously
performed unsuccessful endodontic treatment. It is important to
distinguish knife-shaped root resorption from other aggressive
odontogenic lesions, such as ameloblastoma, which may have a
similar radiographic appearance. The differential diagnosis usually
includes odontogenic or non-odontogenic developmental cysts (e.g.,
residual cyst, odontogenic keratocyst, central giant cell
granuloma), fibro-osseous lesions, traumatic bone cysts, aneurysmal
bone cysts, odontogenic tumours (e.g., ameloblastoma, odontogenic
fibroma), mucoceles, retention cysts, and pseudocysts of the
maxillary sinus (5-10,15).
Early recognition of this pathology and its
consideration in differential diagnosis helps to reduce treatment
delay time and the growth of these lesions. In this case, the
initial biopsy established the suspicion of a benign cystic lesion.
However, the definitive histopathological examination corroborated
the diagnosis of a maxillary cyst lined with pseudostratified
ciliated columnar columnar cells. Regardless of its etiological
cause, definitive treatment of SCC consists of complete enucleation
with primary closure, which is generally curative given its benign
nature. The most commonly used accesses are the direct intraoral
approach and the Caldwell-Luc procedure, although transnasal
endoscopic surgery has also been described (7). Enucleation and curettage alone, open
packing, or even marsupialization have been used (8). However, in the case of large lesions,
bone perforation, or recurrence, a more aggressive approach with
subsequent bone reconstruction may be necessary.
Since these lesions can remain asymptomatic and
appear many years after the initial intervention, long-term
follow-up of patients with a possible history of risky procedures
is recommended. Recurrence rates have not yet been established but
are estimated to be extremely low (7). The prognosis seems to be excellent
after complete enucleation in reported cases (9).
In summary, the growing demand for orthognathic
surgery could increase the number of SCCs related to these
procedures in the medium to long term. Assuming that this
complication is underreported in the literature, the clinician
should be aware to this type of cyst in patients with a history of
maxillary surgery or trauma to establish a differential diagnosis
and ensure appropriate management. Simple surgical gestures, such
as avoiding entrapment of the epithelium between the osteosynthesis
material, suturing the nasal or sinus mucosa if broken, checking
cartilage and bone grafts, and changing the saw blade between
maxillary and mandibular osteotomies, could reduce the appearance
of this pathology. Complete enucleation with primary closure and
subsequent reconstruction when necessary is the most widely used
treatment.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
TCG, RLR and PIC wrote the manuscript. RLR was a
major contributor to the conception and design of the study. TCG,
RLR, MFA, JLGP and PIC confirm the authenticity of all the raw
data. TCG and RLR performed the patient's surgery and acquired the
data. MFA performed the patient's examination. TCG, RLR, MFA, JLGP
and PIC analysed and interpreted the data. TCG, RLR, MFA, JLGP and
PIC critically revised the manuscript for intellectual content. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and the accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kubo I: A buccal cyst occurred after a
radical operation of the maxillary sinus in Japanese. Z F Otol
Tokyo. 3:896–897. 1927.
|
|
2
|
Ragsdale BD, Laurent JL, Janette AJ and
Epker BN: Respiratory implantation cyst of the mandible following
orthognathic surgery. J Oral Maxillofac Pathol. 13:30–34.
2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kaneshiro S, Nakajima T, Yoshikawa Y,
Iwasaki H and Tokiwa N: The postoperative maxillary cyst: Report of
71 cases. J Oral Surg. 39:191–198. 1981.PubMed/NCBI
|
|
4
|
Cano J, Campo J, Alobera MA and Baca R:
Surgical ciliated cyst of the maxilla. Clinical case. Med Oral
Patol Oral Cir Bucal. 14:E361–E364. 2009.PubMed/NCBI
|
|
5
|
Theofilou NE, Lombardi T and Scolozzi P:
Maxillary surgical ciliated cysts following advancement Le Fort I
osteotomy with concomitant autogenous bone grafting: A simple
coincidence or a cause-effect relationship? J Stomatol Oral
Maxillofac Surg. 122:618–624. 2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Golaszewski J, Muñoz R, Barazarte D and
Perez L: Surgical ciliated cyst after maxillary orthognathic
surgery: A literature review and case report. Oral Maxillofac Surg.
23:281–284. 2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Soares JC, Villalba NC, Sanromán JF, Ferro
MF, Fernández PL, Betancourt AL and López AC: Surgical ciliated
cysts in orthognathic surgery. J Craniofac Surg. 32:e2–e5.
2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Amin M, Witherow H, Lee R and Blenkinsopp
P: Surgical ciliated cyst after maxillary orthognathic surgery:
Report of a case. J Oral Maxillofac Surg. 61:138–141.
2003.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Shakib K, McCarthy E, Walker DM and Newman
L: Post operative maxillary cyst: Report of an unusual
presentation. Br J Oral Maxillofac Surg. 47:419–421.
2009.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Lee JH, Huh KH, Yi WJ, Heo MS, Lee SS and
Choi SC: Bilateral postoperative maxillary cysts after orthognathic
surgery: A case report. Imaging Sci Dent. 44:321–324.
2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Leung YY, Wong WY and Cheung LK: Surgical
ciliated cysts may mimic radicular cysts or residual cysts of
maxilla: Report of 3 cases. J Oral Maxillofac Surg. 70:e264–e269.
2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Cai M, Shen G, Lu X and Wang X: Two
mandibular surgical ciliated cysts after le Fort I osteotomy and
genioplasty. Br J Oral Maxillofac Surg. 53:1040–1042.
2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Youn S, Oh HJ, Yoon HJ and Seo BM:
Surgical ciliated cyst of the mandible after orthognathic surgery:
A case report with review of the literature. Maxillofac Plast
Reconstr Surg. 44(26)2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bourgeois SL Jr and Nelson BL: Surgical
ciliated cyst of the mandible secondary to simultaneous Le Fort I
osteotomy and genioplasty: Report of case and review of the
literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
100:36–39. 2005.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Martinelli-Kläy CP, Chatelain S, Salvado F
and Lombardi T: Respiratory epithelium lined cyst of the maxilla:
Differential diagnosis. Case Rep Pathol.
2017(6249649)2017.PubMed/NCBI View Article : Google Scholar
|