Introduction
Essential hypertension is a highly prevalent chronic
disease with >30% of adults having hypertension in 2010
globally; the disease is associated with cardio- and
cerebrovascular diseases, such as stroke, myocardial infarction and
heart failure (1,2). It has been reported that essential
hypertension is more prevalent in the older (age ≥65 years)
population compared with young adults or middle-aged subjects,
partially due to arterial stiffness, worse renal function and
comorbidities observed in older individuals (3,4).
Considering the aging population and the increase in life
expectancy, essential hypertension in older adults may pose a
critical burden on the public health system in the future (5-7).
Regarding the pharmacological management of essential hypertension
in older patients, numerous factors should be taken into
consideration, including contraindications due to comorbidity,
frailty and ability to follow medical instructions. Therefore, more
alternative routes of pharmacological management are needed for
these patients (3,8,9).
Olmesartan medoxomil-amlodipine besylate (OM-AML)
tablets are a dose-fixed antihypertensive drug, containing an
angiotensin receptor blocker (OM) and a calcium channel blocker
(AML) (10,11). Compared with combined
administration of OM and AML tablets, dose-fixed OM-AML tablets are
more convenient and can promote drug adherence (12). Currently, dose-fixed
antihypertensive drugs are recommended by several guidelines,
including guidelines from the World Health Organization, American
College of Cardiology and American Heart Association, and European
Society Of Hypertension-European Society Of Cardiology (13,14).
According to previous studies, OM-AML tablets exhibit better
efficacy in controlling blood pressure (BP) compared with OM or AML
monotherapy (15-17).
This could be due to the fact that OM-AML tablets not only combine
two effective antihypertensive drugs, but also improve patient
compliance due to convenience (18). However, the majority of studies
evaluating the efficacy and safety of OM-AML tablets have been
performed in Western countries, with Caucasian, Hispanic and Black
individuals being the primary study subjects (15-17).
Since China accounts for a large proportion of hypertensive
individuals globally (7), it is
necessary to evaluate OM-AML tablets in Chinese patients with
essential hypertension.
Therefore, the current prospective, multicenter,
real-world study aimed to evaluate the efficacy and safety of
OM-AML tablets in older (age, ≥65 years) Chinese patients with
essential hypertension.
Materials and methods
Study population
A subgroup analysis of 463 older patients with
essential hypertension from the Sevikar® (SVK) study was
performed. The SVK study was a prospective, single-arm,
multicenter, real-world study aiming to investigate the efficacy
and safety of SVK in patients with essential hypertension in China.
A detailed description of the SVK study design is available in the
Chinese Clinical Trial Registry (chictr.org.cn/; registration no., ChiCTR1900026574). A
total of 463 older patients were screened from the SVK study based
on the following criteria: i) Patients diagnosed with essential
hypertension; ii) aged ≥65 years; iii) treated with SVK as
antihypertensive therapy; iv) with at least one follow-up BP
measurement in addition to baseline measurement and v) signed
informed consent. The present study was approved by the Ethics
Committee of Zhongshan Hospital, Fudan University (approval no.
B2019-174R2; Shanghai, China).
Administration of medication
SVK [Daiichi Sankyo (Shanghai) Holdings Co., Ltd.]
was a compound preparation; each SVK tablet contained 20 mg OM and
5 mg AML. The dose of SVK recommended by the physicians was one
oral tablet once a day.
Measurement
The seated diastolic BP (SeDBP) and seated systolic
BP (SeSBP) of patients were measured at baseline (week 0, W0) and
then at W4±7 days (W4) and W8±7 days (W8) in outpatient clinics.
From the first day of medication, the patients measured their BP
every day (home-measured BP). Furthermore, the daily
medication-taking of patients and adverse events (AEs) were
recorded to determine the medication possession rate (MPR) and
safety profiles. Additionally, both attending physicians and
patients scored satisfaction with the current hypertension
treatment at W0 and W8 using a 10-cm visual analogue scale (VAS)
(19); a higher score indicated
higher satisfaction.
Outcomes and definitions
The outcomes included mean change in SeDBP and SeSBP
from W0 to W8, proportion of patients achieving American Heart
Association (AHA) and China BP targets (20,21),
proportion of patients achieving BP response, changes in
home-measured BP from W0 to W8, change in physician and patient
satisfaction with hypertension treatment (VAS) from W0 to W8, MPR
and onset of AEs. The AHA BP target was defined as SeSBP <130
mmHg and SeDBP <80 mmHg (20).
The China BP target was defined as SeSBP and SeDBP <140 and
<90 mmHg, respectively (21).
The BP response rate was defined as proportion of patients who
achieved SeSBP <140 mmHg (or a decrease of ≥20 mmHg) and SeDBP
of <90 mmHg (or a decrease of ≥10 mmHg). MPR was calculated as
follows: MPR=actual days of medication use/total number of
days.
Statistical analysis
Statistical analysis was performed using R version
4.0.5 (r-project.org) and SPSS version 26.0
(IBM Corp.). Categorical data are expressed as number and
percentage, and were analyzed using χ2 or Fisher's exact
test. Measured data are expressed as the mean ± SD or SEM, or
median and interquartile range. Comparisons of the measured data
were carried out by Mann Whitney U test or Kruskal-Wallis test.
Data on blood pressure are usually presented as the mean ± SD in
the field of hypertension, so this convention has been followed.
Post hoc comparison for multiple groups was conducted by Bonferroni
test. Related factors were screened using a logistic regression
model. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patient characteristics
The mean ± SD age of patients was 70.4±4.1 years. In
addition, a total of 238 (51.4%) female patients (mean age,
70.5±4.2 years) and 225 (48.6%) male patients (mean age, 70.4±4.0
years) were included. The median (IQR) time since hypertension
diagnosis was 13.1 (6.1-21.2) years, while 259 (55.9%) patients had
a family history of hypertension. At baseline, mean ± SD SeSBP and
SeDBP were 142.8±16.7 and 82.1±10.2 mmHg, respectively. A total of
264 (57.0%) and 108 (23.3%) patients had abnormal SeSBP and SeDBP,
respectively (defined as SeSBP ≥140 mmHg and SeDBP ≥90 mmHg,
accordingly). Furthermore, 349 (75.4%) patients received OM-AML
tablets without lipid-modifying agents or other medication (any
medication apart from antihypertensive agents and lipid-modifying
agents), 33 (7.1%) patients were co-treated with OM-AML tablets and
lipid-modifying agents, while 81 (17.5%) patients received OM-AML
tablets and lipid-modifying agents and other drugs. The main
characteristics of patients are listed in Table I.
 | Table IBaseline characteristics (n=463). |
Table I
Baseline characteristics (n=463).
| Characteristic | Value |
|---|
| Mean age,
years | 70.4±4.1 |
| Sex, n (%) | |
|
Female | 238 (51.4) |
|
Male | 225 (48.6) |
| Mean BMI,
kg/m2 | 25.2±3.1 |
| Highest completed
education level, n (%) | |
|
Primary
school or less | 83 (17.9) |
|
High
school | 269 (58.1) |
|
Undergraduate
or above | 111 (24.0) |
| Smoker, n (%) | |
|
No | 339 (73.2) |
|
Yes | 124 (26.8) |
| Alcohol intake, n
(%) | |
|
No | 408 (88.1) |
|
Yes | 55 (11.9) |
| Median (IQR) time
since hypertension diagnosis, years | 13.1
(6.1-21.2) |
| Family history of
hypertension, n (%) | |
|
No | 185 (40.0) |
|
Yes | 259 (55.9) |
|
Unknown | 19 (4.1) |
| History of allergy,
n (%) | |
|
No | 410 (88.6) |
|
Yes | 47 (10.2) |
|
Unknown | 6 (1.3) |
| History of
respiratory disease, n (%) | |
|
No | 416 (89.8) |
|
Yes | 45 (9.7) |
|
Unknown | 2 (0.4) |
| History of kidney
disease, n (%) | |
|
No | 432 (93.3) |
|
Yes | 30 (6.5) |
|
Unknown | 1 (0.2) |
| History of
diabetes, n (%) | |
|
No | 358 (77.3) |
|
Yes | 102 (22.0) |
|
Unknown | 3 (0.6) |
| History of CCVD, n
(%) | |
|
No | 256 (55.3) |
|
Yes | 207 (44.7) |
| History of
dyslipidemia, n (%) | |
|
No | 266 (57.5) |
|
Yes | 188 (40.6) |
|
Unknown | 9 (1.9) |
| Mean baseline
respiratory rate, breaths/min | 17.7±1.9 |
| Mean heart rate,
beats/min | 73.6±9.6 |
| Mean SeSBP,
mmHg | 142.8±16.7 |
| Abnormal SeSBP, n
(%) | 264 (57.0) |
| Mean SeDBP,
mmHg | 82.1±10.2 |
| Abnormal SeDBP, n
(%) | 108 (23.3) |
| Hypertension
severity, n (%) | |
|
No | 188 (40.6) |
|
Mild | 197 (42.5) |
|
Moderate | 67 (14.5) |
|
Severe | 11 (2.4) |
| History of
hypertension treatment, n (%) | |
|
Yes | 446 (96.3) |
|
No | 17 (3.7) |
| History of
antihypertensive drugs, n (%) | |
|
Monotherapy | 237 (51.2) |
|
Double
combination | 164 (35.4) |
|
Triple
combination | 37 (8.0) |
|
Unknown | 25 (5.4) |
| History of
antihypertensive medication, n (%) | |
|
Calcium
channel blocker | 281 (60.7) |
|
Angiotensin
II antagonist | 338 (73.0) |
|
Angiotensin-converting
enzyme inhibitor | 36 (7.8) |
| Combination, n
(%) | |
|
No
combination | 349 (75.4) |
|
Lipid-modifying
agent | 33 (7.1) |
|
Lipid-modifying
agent and othersa | 81 (17.5) |
SeSBP and SeDBP are reduced after
OM-AML treatment
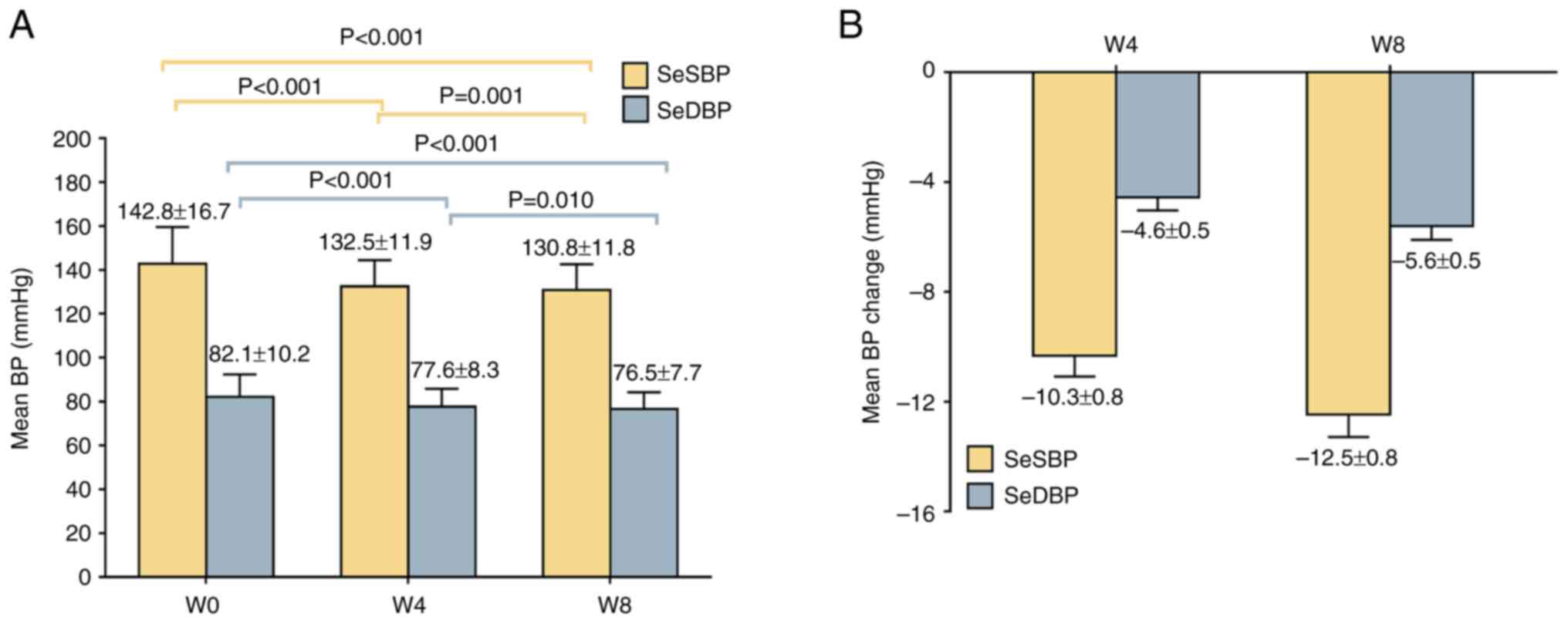
The mean ± SD SeSBP and SeDBP values at W4 were
132.5±11.9 and 77.6±8.3 mmHg, respectively, which were decreased
compared with at W0. At W8, mean ± SD SeSBP and SeDBP values were
130.8±11.8 and 76.5±7.7 mmHg, respectively, which were decreased
compared with those recorded at W4 and W0 (Fig. 1A). In addition, the mean ± SEM
change of SeSBP and SeDBP was -10.3±0.8 and -4.6±0.5 mmHg at W4 and
-12.5±0.8 and -5.6±0.5 mmHg at W8 (Fig. 1B).
Comparison revealed greater changes in SeSBP or
SeDBP in patients with shorter time since diagnosis of
hypertension, patients with a history of allergy and kidney
disease, patients without history of cardiovascular disease or
dyslipidemia, patients with abnormal SeSBP and SeDBP at baseline,
patients with moderate or severe hypertension, or patients without
history of hypertension treatment and patients treated with OM-AML
tablets and lipid-modifying agents (Table SI). Patients who continued their
existing antihypertensive therapy (n=118) showed the most
significant changes in SeSBP and SeDBP compared with patients
without history of antihypertensive drugs (n=17) and those who
discontinued existing antihypertensive therapy (n=328; Table SII).
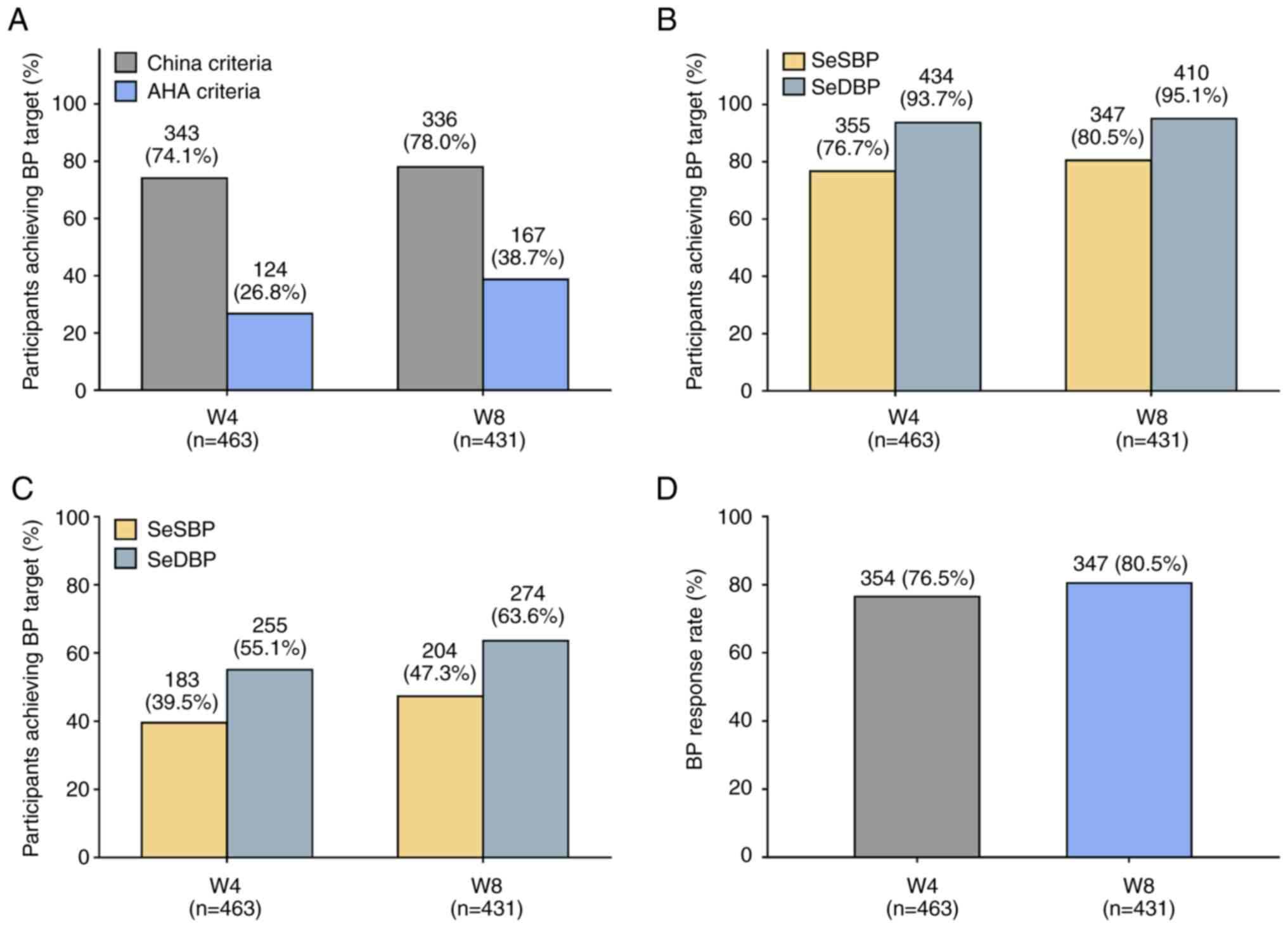
BP target achievement was satisfactory
after OM-AML treatment
At W4, 343 (74.1%) and 124 (26.8%) patients achieved
BP targets according to the China or AHA criteria, respectively.
Additionally, at W8 (n=431 due to lack of assessment data at W8 for
some patients), 336 (78.0%) and 167 (38.7%) patients achieved the
China and AHA criteria of BP target, respectively (Fig. 2A). A total of 355 (76.7%) and 434
(93.7%) patients at W4, and 347 (80.5%) and 410 (95.1%) patients at
W8, met the China criteria of SeSBP and SeDBP target, respectively
(Fig. 2B). A total of 183 (39.5%)
and 255 (55.1%) patients at W4, as well as 204 (47.3%) and 274
(63.6%) patients at W8, achieved SeSBP and SeDBP targets according
to AHA criteria, respectively (Fig.
2C). BP response rates of 76.5 and 80.5% were recorded at W4
and W8, respectively (Fig.
2D).
Subgroup analysis showed that female patients or
patients with shorter time since hypertension diagnosis, normal
SeSBP or SeDBP at baseline, a history of monotherapy of
antihypertensive drugs or those treated with OM-AML tablets alone
more significantly achieved China or AHA BP targets or BP response
rate at W8 (Table II).
Furthermore, male patients (vs. females), time since hypertension
diagnosis of ≥10 were associated with a lower probability of
achieving AHA BP target at W8. Abnormal SeSBP at baseline (vs.
normal) and treatment with OM-AML tablets and lipid-modifying
agents and other drugs (vs. OM-AML tablets without lipid-modifying
agent or other drugs) were also independently associated with lower
probability of achieving AHA BP target at W8 (Table SIII). In addition, abnormal SeSBP
at baseline (vs. normal) and patient treatment with OM-AML tablets
and lipid-modifying agents and other drugs (vs. OM-AML tablets
without lipid-modifying agent or other drugs) were independently
associated with lower probability of achieving China BP target at
W8 (Table SIV). At W8 after the
initiation of OM-AML tablet administration, the history of double
combination of antihypertensive drugs (vs. monotherapy) and
treatment with OM-AML tablets and lipid-modifying agents and other
drugs (vs. OM-AML tablets without lipid-modifying agent or other
drugs) were independently associated with lower BP response rate
(Table SV).
| Table IIAchievement of BP target rate and BP
response rate at week 8 (n=431). |
Table II
Achievement of BP target rate and BP
response rate at week 8 (n=431).
| Characteristic | N | AHA BP target, n
(%) | P-value | China BP target, n
(%) | P-value | BP response, n
(%) | P-value |
|---|
| Sex | | | 0.002 | | 0.096 | | 0.069 |
|
Female | 223 | 102 (45.7) | | 181 (81.2) | | 187 (83.9) | |
|
Male | 208 | 65 (31.3) | | 155 (74.5) | | 160 (76.9) | |
| BMIa, kg/m2 | | | 0.878 | | 0.767 | | 0.371 |
|
<30 | 394 | 152 (38.6) | | 306 (77.7) | | 315 (79.9) | |
|
≥30 | 30 | 12 (40.0) | | 24 (80.0) | | 26 (86.7) | |
| Highest completed
education level | | | 0.306 | | 0.515 | | 0.530 |
|
Primary
school or less | 80 | 37 (46.3) | | 60 (75.0) | | 62 (77.5) | |
|
High
school | 249 | 93 (37.3) | | 199 (79.9) | | 205 (82.3) | |
|
Undergraduate
or above | 102 | 37 (36.3) | | 77 (75.5) | | 80 (78.4) | |
| Smoker | | | 0.067 | | 0.199 | | 0.297 |
|
No | 317 | 131 (41.3) | | 252 (79.5) | | 259 (81.7) | |
|
Yes | 114 | 36 (31.6) | | 84 (73.7) | | 88 (77.2) | |
| Alcohol intake | | | 0.078 | | 0.176 | | 0.126 |
|
No | 380 | 153 (40.3) | | 300 (78.9) | | 310 (81.6) | |
|
Yes | 51 | 14 (27.5) | | 36 (70.6) | | 37 (72.5) | |
| Time since
hypertension diagnosis, years | | | 0.016 | | 0.307 | | 0.668 |
|
<5 | 87 | 45 (51.7) | | 73 (83.9) | | 73 (83.9) | |
|
5-9 | 55 | 22 (40.0) | | 43 (78.2) | | 44 (80.0) | |
|
≥10 | 289 | 100 (34.6) | | 220 (76.1) | | 230 (79.6) | |
| Family history of
hypertension | | | 0.657 | | 0.676 | | 0.803 |
|
No | 178 | 70 (39.3) | | 140 (78.7) | | 144 (80.9) | |
|
Yes | 234 | 87 (37.2) | | 180 (76.9) | | 187 (79.9) | |
| History of
allergy | | | 0.845 | | 0.813 | | 0.840 |
|
No | 382 | 148 (38.7) | | 296 (77.5) | | 306 (80.1) | |
|
Yes | 43 | 16 (37.2) | | 34 (79.1) | | 35 (81.4) | |
| History of
respiratory disease | | | 0.436 | | 0.556 | | 0.565 |
|
No | 386 | 147 (38.1) | | 299 (77.5) | | 309 (80.1) | |
|
Yes | 43 | 19 (44.2) | | 35 (81.4) | | 36 (83.7) | |
| History of kidney
disease | | | 0.210 | | 0.701 | | 0.451 |
|
No | 402 | 153 (38.1) | | 314 (78.1) | | 325 (80.8) | |
|
Yes | 28 | 14 (50.0) | | 21 (75.0) | | 21 (75.0) | |
| History of
diabetes | | | 0.814 | | 0.637 | | 0.735 |
|
No | 332 | 127 (38.3) | | 260 (78.3) | | 268 (80.7) | |
|
Yes | 96 | 38 (39.6) | | 73 (76.0) | | 76 (79.2) | |
| History of
CCVD | | | 0.596 | | 0.713 | | 0.923 |
|
No | 234 | 88 (37.6) | | 184 (78.6) | | 188 (80.3) | |
|
Yes | 197 | 79 (40.1) | | 152 (77.2) | | 159 (80.7) | |
| History of
dyslipidemia | | | 0.743 | | 0.060 | | 0.105 |
|
No | 245 | 98 (40.0) | | 200 (81.6) | | 205 (83.7) | |
|
Yes | 177 | 68 (38.4) | | 131 (74.0) | | 137 (77.4) | |
| Respiratory
rate | | | 1.000 | | 1.000 | | 1.000 |
|
Normal | 356 | 146 (41.0) | | 283 (79.5) | | 294 (82.6) | |
|
Abnormal | 5 | 2 (40.0) | | 4 (80.0) | | 4 (80.0) | |
| Heart rate (%) | | | 0.246 | | 0.193 | | 0.441 |
|
Normal | 397 | 153 (38.5) | | 308 (77.6) | | 319 (80.4) | |
|
Abnormal | 26 | 13 (50.0) | | 23 (88.5) | | 23 (88.5) | |
| SeSBP | | | <0.001 | | <0.001 | | <0.001 |
|
Normal | 180 | 90 (50.0) | | 162 (90.0) | | 168 (93.3) | |
|
Abnormal | 251 | 77 (30.7) | | 174 (69.3) | | 179 (71.3) | |
| SeDBP | | | 0.001 | | 0.034 | | 0.017 |
|
Normal | 330 | 142 (43.0) | | 265 (80.3) | | 274 (83.0) | |
|
Abnormal | 101 | 25 (24.8) | | 71 (70.3) | | 73 (72.3) | |
| Hypertension
severity | | | 0.950 | | 0.097 | | 0.034 |
|
Mild | 189 | 57 (30.2) | | 138 (73.0) | | 143 (75.7) | |
|
Moderate or
severe | 72 | 22 (30.6) | | 45 (62.5) | | 45 (62.5) | |
| History of
hypertension treatment | | | 0.420 | | 0.774 | | 0.754 |
|
Yes | 414 | 162 (39.1) | | 323 (78.0) | | 334 (80.7) | |
|
No | 17 | 5 (29.4) | | 13 (76.5) | | 13 (76.5) | |
| History of
antihypertensive drugs | | | 0.566 | | 0.005 | | 0.070 |
|
Monotherapy | 224 | 92 (41.1) | | 187 (83.5) | | 189 (84.4) | |
|
Double
combination | 146 | 54 (37.0) | | 106 (72.6) | | 109 (74.7) | |
|
Triple
combination | 36 | 12 (33.3) | | 23 (63.9) | | 29 (80.6) | |
| History of calcium
channel blockers | | | 0.192 | | 0.814 | | 0.209 |
|
No | 64 | 30 (46.9) | | 53 (82.8) | | 56 (87.5) | |
|
Yes | 271 | 103 (38.0) | | 221 (81.5) | | 219 (80.8) | |
| History of
angiotensin II antagonists | | | 0.119 | | 1.000 | | 1.000 |
|
No | 7 | 5 (71.4) | | 6 (85.7) | | 6 (85.7) | |
|
Yes | 328 | 128 (39.0) | | 268 (81.7) | | 269 (82.0) | |
| History of
angiotensin-converting enzyme inhibitors | | | 0.736 | | 0.058 | | 0.140 |
|
No | 302 | 119 (39.4) | | 251 (83.1) | | 251 (83.1) | |
|
Yes | 33 | 14 (42.4) | | 23 (69.7) | | 24 (72.7) | |
| Combination | | | 0.009 | | 0.001 | | 0.002 |
|
No
combination | 325 | 139 (42.8) | | 266 (81.8) | | 273 (84.0) | |
|
Lipid-modifying
agent | 32 | 10 (31.3) | | 24 (75.0) | | 25 (78.1) | |
|
Lipid-modifying
agent and other | 74 | 18 (24.3) | | 46 (62.2) | | 49 (66.2) | |
Home-measured BP is reduced after
OM-AML treatment
Home-measured SeSBP and SeDBP were significantly
decreased from W1 to W8 (Fig. 3A).
The mean changes of weekly home-measured SeSBP from W2 to W8 were
-1.9, -2.4, -2.9, -3.8, -4.5, -4.8 and -5.0, respectively.
Additionally, the mean changes of weekly home-measured SeDBP from
W2 to W8 were -0.8, -1.2, -1.5, -1.7, -2.0, -2.3 and -2.1,
respectively (Fig. 3B). The post
hoc comparisons of home-measured BP are shown in Table SVI.
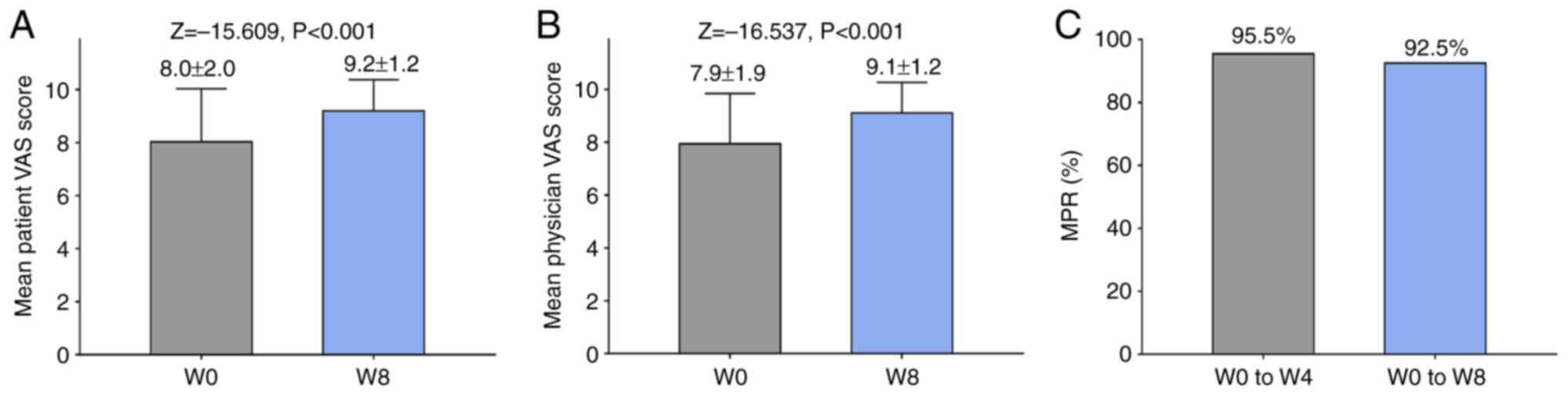
Satisfaction is improved and
medication possession is high after OM-AML treatment
The satisfaction of both patients and physicians was
significantly increased at W8 compared with W0 (Fig. 4A and B). MPR for W0-W4 and W0-W8 was 95.5 and
92.5%, respectively (Fig. 4C).
OM-AML treatment is generally
tolerable
The most common AEs were nervous system disorder
(13.4%), vascular disorder (9.7%), general disorder and
administration site conditions (6.5%) and cardiac disorder (4.5%).
Additionally, severe AEs (grade 3-4 AEs) included vascular disorder
(0.6%), cardiac disorder (0.4%), respiratory, thoracic and
mediastinal disorder (0.2%), general disorders and administration
site conditions (0.2%), and reproductive system and breast
disorders (0.2%). Furthermore, the most common drug-associated AEs
(AEs that were associated with the drug use, as evaluated by the
investigators) were nervous system disorder (4.5%), vascular
disorder (2.8%), and general disorder and administration site
conditions (2.6%; Table
III).
| Table IIIAEs by system organ class. |
Table III
AEs by system organ class.
| System organ
class | Any AE, n (%) | Severe AE, n
(%) | Drug-associated AE,
n (%) |
|---|
| Nervous system
disorder | 62 (13.4) | 0 (0.0) | 21 (4.5) |
| Vascular
disorder | 45 (9.7) | 3 (0.6) | 13 (2.8) |
| General disorder
and administration site conditions | 30 (6.5) | 1 (0.2) | 12 (2.6) |
| Cardiac
disorder | 21 (4.5) | 2 (0.4) | 9 (1.9) |
| Gastrointestinal
disorder | 18 (3.9) | 0 (0.0) | 6 (1.3) |
| Respiratory,
thoracic and mediastinal disorder | 15 (3.2) | 2 (0.4) | 1 (0.2) |
| Metabolism and
nutrition disorder | 12 (2.6) | 0 (0.0) | 0 (0.0) |
| Psychiatric
disorder | 8 (1.7) | 0 (0.0) | 6 (1.3) |
| Skin and
subcutaneous tissue disorder | 7 (1.5) | 0 (0.0) | 2 (0.4) |
| Musculoskeletal and
connective tissue disorder | 7 (1.5) | 0 (0.0) | 0 (0.0) |
| Investigations | 4 (0.9) | 0 (0.0) | 0 (0.0) |
| Eye disorder | 3 (0.6) | 0 (0.0) | 1 (0.2) |
| Reproductive system
and breast disorder | 3 (0.6) | 1 (0.2) | 0 (0.0) |
| Renal and urinary
disorder | 3 (0.6) | 0 (0.0) | 0 (0.0) |
| Endocrine
disorder | 2 (0.4) | 0 (0.0) | 0 (0.0) |
| Immune system
disorder | 1 (0.2) | 0 (0.0) | 1 (0.2) |
| Hepatobiliary
disorder | 1 (0.2) | 0 (0.0) | 0 (0.0) |
Discussion
OM-AML tablets are an effective antihypertensive
agent not only for the general population, but also for older
patients, and patients with diabetes mellitus or obesity (22,23).
Regarding the effect of OM-AML tablets on older patients with
essential hypertension, a previous study demonstrated that the mean
change of SeSBP/SeDBP was -14.5/-7.8 mmHg in older patients with
uncontrolled hypertension who had previously received monotherapy
followed by administration of OM-AML tablets for 20 weeks (24). Another study showed that after
treatment with OM-AML tablets for 36 months, SeSBP/SeDBP decreased
from 157.2/84.6 to 132.6/72.6 mmHg in older patients with
hypertension (25), resulting in a
mean change of -24.6/-12.0 mmHg for SeSBP/SeDBP. To the best of our
knowledge, however, no similar studies have been performed in
China. Due to differences in ethnicity, as well as lifestyle
factors of Chinese patients, including high sodium and low
potassium intake, low levels of physical exercise and high levels
of alcohol abuse, evaluating the efficacy of OM-AML tablets in
older patients with essential hypertension in China is of marked
importance. The present study revealed that the mean change of
SeSBP/SeDBP in older patients with essential hypertension was
-12.5/-5.6 mmHg. The change of SeSBP/SeDBP was lower compared with
that reported in previous studies (20 weeks and 36 months,
respectively) (24,25). This may be due to the different
duration of treatment, which was 8 weeks in the present study.
However, OM-AML tablets could effectively lower BP in older
patients with essential hypertension.
Decreasing BP to a particular threshold is the main
objective of antihypertensive treatment. A previous study showed
that 62.5% of older patients with resistant hypertension achieved
the goal of SeSBP/SeDBP <140/90 mmHg following treatment with
OM-AML tablets for 8 weeks (26)
Additionally, a BP threshold of <140/90 mmHg was achieved by
86.8% of older patients with essential hypertension receiving
OM-AML tablets for 20 weeks (24).
Furthermore, another study reported that 51.4% of older patients
with essential hypertension achieved a BP goal of <140/90 mmHg
after treatment with OM-AML tablets for 10 weeks (27). In the present study, 78.0 and 38.7%
of older patients achieved a BP target of <140/90 and <130/80
mmHg, based on the China and AHA criteria, respectively. The
aforementioned results were consistent with those reported in
previous studies, which used a BP goal of <140/90 mmHg (24,26,27).
Additionally, compared with previous studies on older patients with
hypertension treated with OM or AML monotherapy (22,28),
the present study revealed that a higher proportion of patients
achieved a BP target of <140/90 mmHg. This could be due to the
fact that OM-AML tablets combine two antihypertensive drugs with
high efficacy, thus displaying superior treatment efficacy.
During the treatment of essential hypertension, both
patient and physician satisfaction should be considered.
Satisfaction is commonly associated with treatment efficacy,
convenience of treatment and cost (8,9,18).
Consistent with a previous study (29), satisfaction of both patients and
physicians in the present study was increased at W8 compared with
at W0. This may be because OM-AML tablets were effective in
controlling BP, thus enhancing both patient and physician
satisfaction and OM-AML tablets were convenient to take due to
their single-pill, dose-fixed design, reducing the probability of
missing doses, thus also increasing the satisfaction of both
patients and physicians. Additionally, the present study reported a
MPR of 92.5% at W8, which was similar to that reported in Korean
patients with essential hypertension treated with a dose-fixed
OM/AML/hydrochlorothiazide regimen (29).
Due to comorbidities and frailty, the safety of
antihypertensive drugs is a key issue during the treatment of older
patients with essential hypertension (3,5). The
present study revealed that the incidence of OM-AML-associated AEs
in older patients with essential hypertension was similar to that
reported in previous studies (24-27).
In addition, the incidence of severe AEs was relatively low,
indicating that OM-AML tablets could be considered a safe
antihypertensive drug.
The present study had some limitations. Firstly, the
present study was a prospective, observational, single-cohort study
that evaluated the efficacy and safety of OM-AML tablets in older
patients with essential hypertension. However, further randomized,
controlled trials should be performed to provide more evidence for
the administration of OM-AML tablets in these patients. Secondly, a
10-cm VAS scale was used to assess the satisfaction of both
patients and physicians. This scale is characterized by ease of
assessment; however, this leads to an increased risk of bias.
Thirdly, the long-term efficacy and safety of OM-AML tablets in
older patients with essential hypertension should be further
explored in the future.
In conclusion, the present study indicated that
OM-AML tablets were an effective and safe antihypertensive drug,
facilitating the achievement of BP targets in older patients with
essential hypertension.
Supplementary Material
Change in BP from W0 to W8.
BP in patients with existing
antihypertensive medication.
Factors affecting probability of
achieving AHA BP target rate at week 8 by logistic regression model
analysis.
Factors affecting probability of
achieving China BP target rate at week 8 by logistic regression
model analysis.
Factors affecting probability of
achieving BP response rate at week 8 by logistic regression model
analysis.
Post hoc comparisons of home-measured
BP after treatment.
Investigators and group in the SVK
Study.
Acknowledgements
The authors thank all the investigating groups of
the SVK study, as listed in Table
SVII, for their contributions.
Funding
Funding: The present study was supported by Daiichi Sankyo
(China) Holdings Co., Ltd, Shanghai, China.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JG, ZC and JD contributed to conception and design
of study. ZC, ZQ, WH, GM, YL, RW, LC, LF, MH, YH, MW, JX, YX, ZW,
XJ, JH, DF, LT, WC, XCa, YJ, YZ, LH, PB, XCh, PD, XH, MLL, XW, KH,
YLL, YWL, DL, JuW, JiW, GF, LW and MQL were responsible for
acquisition of data. JG, ZC, ZQ, WC, WH, GM, JD, LW and ML
performed data analysis and interpreted data. JG and ZC confirm the
authenticity of all the raw data. JG, ZC, JD, LW and ML drafted the
manuscript and all other authors provided critical revision. All
authors read and approved the final version of manuscript.
Ethics approval and consent to
participate
A detailed description of the SVK study design is
available in Chinese Clinical Trial Registry (chictr.org.cn/; registration no. ChiCTR1900026574).
The present study was approved by the Ethics Committee of Zhongshan
Hospital, Fudan University (approval no. B2019-174R2; Shanghai,
China). All patients provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
JD, LW and MLi are employees of Daiichi Sankyo
(China) Holdings Co., Ltd., the company that makes SVK. The other
authors declare that they have no competing interests.
References
|
1
|
Zhou B, Perel P, Mensah GA and Ezzati M:
Global epidemiology, health burden and effective interventions for
elevated blood pressure and hypertension. Nat Rev Cardiol.
18:785–802. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Boutouyrie P, Chowienczyk P, Humphrey JD
and Mitchell GF: Arterial stiffness and cardiovascular risk in
hypertension. Circ Res. 128:864–886. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Oliveros E, Patel H, Kyung S, Fugar S,
Goldberg A, Madan N and Williams KA: Hypertension in older adults:
Assessment, management, and challenges. Clin Cardiol. 43:99–107.
2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Benetos A, Petrovic M and Strandberg T:
Hypertension management in older and frail older patients. Circ
Res. 124:1045–1060. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Yasuda S, Miyamoto Y and Ogawa H: Current
status of cardiovascular medicine in the aging society of Japan.
Circulation. 138:965–967. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Mohsen Ibrahim M: Hypertension in
developing countries: A major challenge for the future. Curr
Hypertens Rep. 20(38)2018.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Mills KT, Stefanescu A and He J: The
global epidemiology of hypertension. Nat Rev Nephrol. 16:223–237.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Thomas NF and Dunn KS: Self-transcendence
and medication adherence in older adults with hypertension. J
Holist Nurs. 32:316–326. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Lo SH, Chau JP, Woo J, Thompson DR and
Choi KC: Adherence to antihypertensive medication in older adults
with hypertension. J Cardiovasc Nurs. 31:296–303. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Erdine S: Olmesartan/amlodipine: Blood
pressure lowering and beyond in special populations. Ther Adv
Cardiovasc Dis. 6:31–44. 2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Zhang X, Zhang H, Ma Y, Che W and Hamblin
MR: Management of hypertension using olmesartan alone or in
combination. Cardiol Ther. 6:13–32. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Parati G, Kjeldsen S, Coca A, Cushman WC
and Wang J: Adherence to Single-Pill versus free-equivalent
combination therapy in hypertension: A systematic review and
meta-analysis. Hypertension. 77:692–705. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Al-Makki A, DiPette D, Whelton PK, Murad
MH, Mustafa RA, Acharya S, Beheiry HM, Champagne B, Connell K,
Cooney MT, et al: Hypertension pharmacological treatment in adults:
A World Health organization guideline executive summary.
Hypertension. 79:293–301. 2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Bakris G, Ali W and Parati G: ACC/AHA
Versus ESC/ESH on hypertension guidelines: JACC guideline
comparison. J Am Coll Cardiol. 73:3018–3026. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Derosa G, Mugellini A, Pesce RM, D'Angelo
A and Maffioli P: Olmesartan combined with amlodipine on oxidative
stress parameters in type 2 diabetics, compared with single
therapies: A randomized, controlled, clinical trial. Medicine
(Baltimore). 95(e3084)2016.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Chrysant SG, Melino M, Karki S, Lee J and
Heyrman R: The combination of olmesartan medoxomil and amlodipine
besylate in controlling high blood pressure: COACH, a randomized,
double-blind, placebo-controlled, 8-week factorial efficacy and
safety study. Clin Ther. 30:587–604. 2008.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Volpe M, Brommer P, Haag U and Miele C:
Efficacy and tolerability of olmesartan medoxomil combined with
amlodipine in patients with moderate to severe hypertension after
amlodipine monotherapy: A randomized, double-blind, parallel-group,
multicentre study. Clin Drug Investig. 29:11–25. 2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Levi M, Pasqua A, Cricelli I, Cricelli C,
Piccinni C, Parretti D and Lapi F: Patient adherence to
olmesartan/amlodipine combinations: Fixed versus extemporaneous
combinations. J Manag Care Spec Pharm. 22:255–262. 2016.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Lucas C, Romatet S, Mekiès C, Allaf B and
Lantéri-Minet M: Stability, responsiveness, and reproducibility of
a visual analog scale for treatment satisfaction in migraine.
Headache. 52:1005–1018. 2012.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Whelton PK, Carey RM, Aronow WS, Casey DE
Jr, Collins KJ, Dennison Himmelfarb C, DePalma SM, Gidding S,
Jamerson KA, Jones DW, et al: 2017 ACC/AHA/AA
PA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the
prevention, detection, evaluation, and management of high blood
pressure in adults: A report of the american college of
Cardiology/American heart association task force on clinical
practice guidelines. Hypertension. 71:e13–e115. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Wu S, Xu Y, Zheng R, Lu J, Li M, Chen L,
Huo Y, Xu M, Wang T, Zhao Z, et al: Hypertension Defined by 2017
ACC/AHA guideline, ideal cardiovascular health metrics, and risk of
cardiovascular disease: A nationwide prospective cohort study.
Lancet Reg Health West Pac. 20(100350)2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Chrysant SG, Lee J, Melino M, Karki S and
Heyrman R: Efficacy and tolerability of amlodipine plus olmesartan
medoxomil in patients with difficult-to-treat hypertension. J Hum
Hypertens. 24:730–738. 2010.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Oparil S, Lee J, Karki S and Melino M:
Subgroup analyses of an efficacy and safety study of concomitant
administration of amlodipine besylate and olmesartan medoxomil:
Evaluation by baseline hypertension stage and prior
antihypertensive medication use. J Cardiovasc Pharmacol.
54:427–436. 2009.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Weir MR, Shojaee A and Maa JF: Efficacy of
amlodipine/olmesartan medoxomil +/- hydrochlorothiazide in patients
aged >/=65 or <65 years with uncontrolled hypertension on
prior monotherapy. Postgrad Med. 125:124–134. 2013.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Ogawa H, Kim-Mitsuyama S, Matsui K,
Jinnouchi T, Jinnouchi H and Arakawa K: OlmeSartan and Calcium
Antagonists Randomized (OSCAR) Study Group. Angiotensin II receptor
blocker-based therapy in Japanese elderly, high-risk, hypertensive
patients. Am J Med. 125:981–990. 2012.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Ding S, Liu J, Fu Q and Zheng Y: Clinical
effects of combined olmesartan medoxomil and amlodipine on clinic
and ambulatory blood pressure in elderly patients with resistant
hypertension. Arch Gerontol Geriatr. 57:423–427. 2013.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Kreutz R, Ammentorp B, Laeis P and de la
Sierra A: Efficacy and tolerability of triple-combination therapy
with olmesartan, amlodipine, and hydrochlorothiazide: A subgroup
analysis of patients stratified by hypertension severity, age, sex,
and obesity. J Clin Hypertens (Greenwich). 16:729–740.
2014.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Zhu JR, Zhang SY and Gao PJ: Efficacy and
safety of olmesartan medoxomil/amlodipine fixed-dose combination
for hypertensive patients uncontrolled with monotherapy. Arch Pharm
Res. 37:1588–1598. 2014.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sohn IS, Ihm SH, Kim GH, Park SM, Hong BK,
Lee CH, Lee SH, Chang DI, Joo SP, Lee SC, et al: Real-world
evidence on the strategy of olmesartan-based triple single-pill
combination in Korean hypertensive patients: A prospective,
multicenter, observational study (RESOLVE-PRO). Clin Hypertens.
27(21)2021.PubMed/NCBI View Article : Google Scholar
|