Introduction
Although villous adenomas (VAs) are an uncommon
subtype of colonic adenomas, they are clinically important due to
their tendency to grow large, produce copious mucus, and induce
fluid and electrolyte disturbances (1,2).
This mucinous and electrolyte-rich secretory activity is thought to
be driven by elevated levels of prostaglandins, especially
prostaglandin E2 (PGE2), which can stimulate intracellular cAMP and
promote fluid secretion (3,4).
Despite this established mechanism, direct comparative analyses of
PGE2 and its related enzymatic pathways between VAs and other
adenoma subtypes remain limited.
VAs account for approximately 5 to 15% of all
colonic adenomas and are predominantly located in the rectosigmoid
colon (1,2). The reported incidence of coexistent
carcinoma in VAs is high. When these tumors reach a substantial
size, they may produce excessive mucin, leading to electrolyte
disturbances, renal dysfunction, and, in some cases,
neuropsychiatric symptoms (2,5). In
certain cases, VAs can secrete large amounts of mucus, resulting in
dehydration and severe electrolyte imbalance, a condition referred
to as Electrolyte Depletion Syndrome (EDS). Originally documented
by McKittrick and Wheelock in 1954(6), this condition, commonly referred to
as McKittrick-Wheelock Syndrome, is typified by potassium-rich,
tumor-derived mucus. The pathogenesis is believed to involve
upregulated PGE2 production with consequent increases in
intracellular cAMP, both contributing to the exaggerated secretory
response (3,4). Reports of symptomatic improvement
with indomethacin, a PGE2 synthesis inhibitor, suggest its
potential usefulness as a temporary bridging therapy prior to
definitive resection (4,7). Moreover, clinical case reports have
described the characteristic features of McKittrick-Wheelock
Syndrome associated with VAs, emphasizing the importance of early
recognition and appropriate management (8).
This study aims to characterize the differential
expression of PGE2, COX-1, and COX-2 in villous vs. tubular
adenomas (TAs), with the goal of elucidating their roles in mucin
hypersecretion and identifying potential therapeutic
implications.
Patients and methods
Patients and tissue samples
VA cases were first identified by reviewing all
patients who underwent endoscopic or surgical resection at Minoh
City Hospital (Minoh, Japan) between January 2011 and September
2021. During this period, twenty consecutive VA cases met the
inclusion criteria and had adequately preserved formalin-fixed,
paraffin-embedded (FFPE) tissue suitable for immunohistochemical
analysis. To allow for a balanced comparison, an equal number of TA
cases were then selected consecutively from the same database,
matched to the availability of high-quality FFPE tissue.
Clinicopathological data, including patient age, sex, tumor
location, and tumor size (maximum diameter measured endoscopically
or pathologically), were collected and compared between groups.
Patients with conditions that could potentially influence
prostaglandin metabolism or mucosal inflammatory status were
excluded. Specifically, exclusion criteria consisted of: i)
Long-term regular use of nonsteroidal anti-inflammatory drugs
(including low-dose aspirin or COX-2 inhibitors); ii) systemic
immunosuppressive therapy such as chronic corticosteroids,
calcineurin inhibitors, or anti-TNF agents; iii) a history of
inflammatory bowel disease (ulcerative colitis or Crohn's disease);
iv) hereditary colorectal cancer syndromes including familial
adenomatous polyposis or Lynch syndrome; and v) inadequate or
poorly fixed tissue unsuitable for immunohistochemical evaluation.
No patients in this cohort met any of these exclusion criteria,
allowing all eligible consecutive cases to be included in the final
analysis. This study was conducted in accordance with The
Declaration of Helsinki and was approved by the Ethics Committee of
Minoh City Hospital (approval no. R0311B64). As a retrospective
study, written informed consent was waived, and an opt-out approach
was implemented by publicly disclosing study information on the
hospital website to provide patients with the opportunity to
decline participation.
Immunohistochemistry
Immunohistochemical staining was performed using
3-µm FFPE sections. Antigen retrieval was carried out by heating
the sections in citrate buffer (pH 6.0) in a pressure cooker for 15
min. The primary antibodies used were anti-PGE2 (ab2318, Abcam,
Cambridge, UK; dilution 1:100), anti-COX-1 (ab109025, Abcam,
Cambridge, UK; dilution 1:150), and anti-COX-2 (ab15191, Abcam,
Cambridge, UK; dilution 1:100). Sections were incubated with
primary antibodies overnight at 4˚C, followed by incubation with
appropriate secondary antibodies (Vector Laboratories, Burlingame,
CA, USA) and visualization using the ImmPACT DAB substrate kit
(SK-4105, Vector Laboratories, Burlingame, CA, USA).
Counterstaining was performed with hematoxylin. Negative controls
were prepared by omitting the primary antibody. As no standardized
or universally accepted cutoff for COX-1, COX-2, or PGE2
immunohistochemical positivity has been established in colorectal
neoplasia, a threshold was determined a priori based on both
morphological clarity and interobserver reproducibility.
Immunostaining was evaluated manually, without the use of
image-analysis software, by three independent investigators. The
percentage positivity was estimated on an area basis by visually
assessing the proportion of the glandular area exhibiting
cytoplasmic or membranous staining within the entire adenomatous
component. Glands were classified as positive when ≥10% of the
glandular area exhibited cytoplasmic or membranous staining.
Staining below this level was consistently interpreted as minimal
and lacked biological significance. This threshold was supported by
the high concordance of independent assessments performed by three
investigators. For each case, at least 50 glands were evaluated to
determine the percentage of positive glands.
Statistical analysis
Comparisons of clinicopathological factors and
immunohistochemical expression between the VA and TA groups were
performed using the Wilcoxon rank-sum test or Fisher's exact test,
as appropriate. Associations between PGE2 and COX-1/COX-2
expression were assessed using simple linear regression to
illustrate the direction and magnitude of the association. All
statistical tests were two-tailed, and P<0.05 was considered to
indicate a statistically significant difference. Statistical
analyses were conducted using JMP Student Edition 18.2.2 (SAS
Institute).
Results
Clinicopathological features
The clinicopathological characteristics of the 40
colorectal adenoma cases, comprising 20 TA and 20 VA, are
summarized in Table I. Patients
with VA tended to be older (mean age 72.5±9.6 years) than those
with TA (68.8±9.9 years), although this difference did not reach
statistical significance (P=0.203). A significant sex difference
was observed between the groups: the TA group had a predominance of
male patients (16 males, 4 females), whereas the VA group showed a
female predominance (8 males, 12 females), a difference that was
statistically significant (P=0.022). The anatomical distribution
also differed slightly. VAs were more frequently located in the
distal colon, especially in the rectum and sigmoid colon, although
the statistical power for segment-based comparison was limited due
to small subgroup sizes. Notably, VAs were significantly larger
than TAs, with mean lesion diameters of 21.3±22.5 mm vs. 9.6±7.8
mm, respectively (P=0.018).
 | Table IClinicopathological characteristics of
patients with tubular and villous adenomas. |
Table I
Clinicopathological characteristics of
patients with tubular and villous adenomas.
| Characteristic | Tubular adenoma
(n=20) | Villous adenoma
(n=20) | P-value |
|---|
| Age, years | 68.8±9.9 | 72.5±9.6 | 0.203 |
| Sex, Male/Female | 16/4 | 8/12 | 0.022 |
| Location,
A/T/D/S/R | 2/3/5/6/4 | 1/2/3/6/8 | -0.729 |
| Size, mm | 9.6±7.8 | 21.3±22.5 | 0.018 |
Immunohistochemical findings
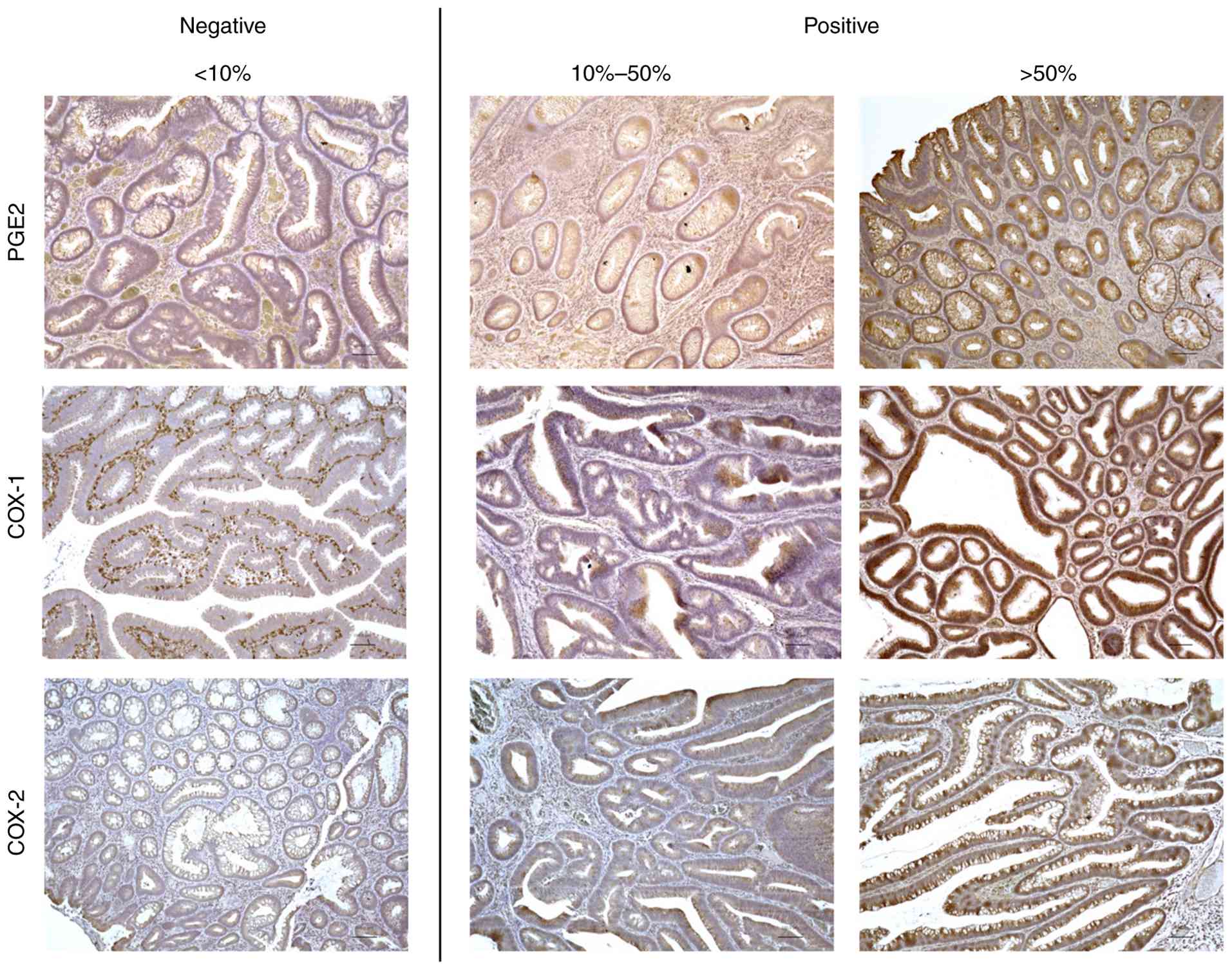
Fig. 1 presents
representative immunohistochemical staining for PGE2, COX-1 and
COX-2. Each gland was assessed based on the proportion of the
stained area. Glands in which the stained area comprised less than
10% were considered negative, whereas those in which the stained
area exceeded 10% were considered positive. The proportion of
positive glands was calculated as follows: (number of positive
glands/total number of glands) x100. The proportion of positive
glands was significantly higher in VAs compared to TAs for PGE2
(83±4.1% vs. 24±4.8%, P<0.001) and COX-2 (59±6.2% vs. 41±6.3%,
P=0.022), while COX-1 expression did not differ between the two
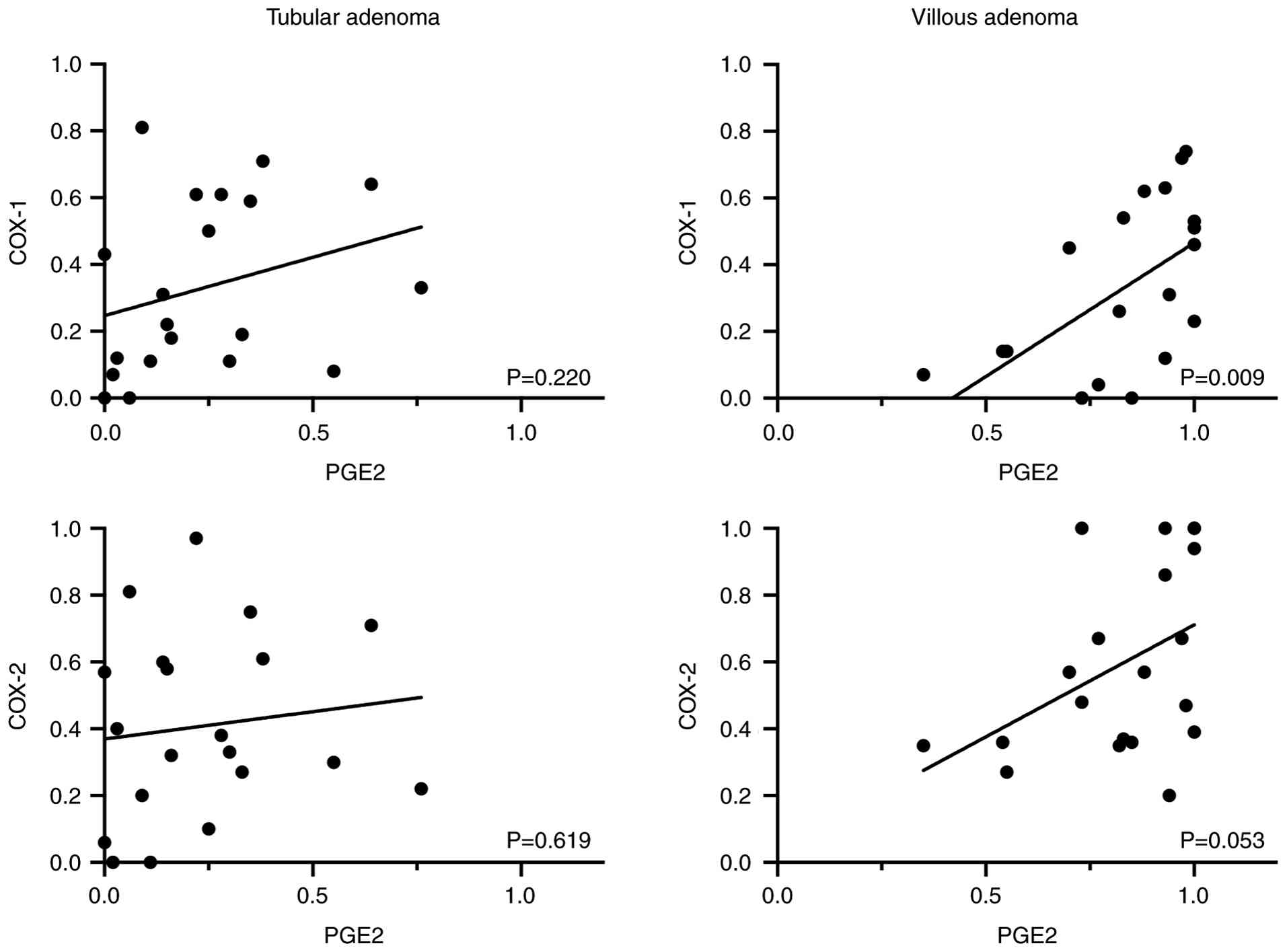
groups (33±5.7% vs. 33±5.8%, P=0.48) (Table II). Association analyses were
performed to assess the relationships between PGE2 expression and
COX-1/COX-2 in tubular and VAs (Fig.
2). In VAs, PGE2 expression demonstrated a weak-to-moderate
association with COX-1, which was statistically significant
(R²=0.325, P=0.009), and a weak association with COX-2, with only a
trend toward significance (R²=0.193, P=0.053). In TAs, no
meaningful associations were observed (R²=0.082, P=0.220 for COX-1;
R²=0.014, P=0.619 for COX-2). These findings indicate that PGE2-COX
associations are more pronounced in VAs than in TAs.
| Table IIProportion of positive glands in
tubular and villous adenoma. |
Table II
Proportion of positive glands in
tubular and villous adenoma.
| Protein | Tubular adenoma
(n=20) | Villous adenoma
(n=20) | P-value |
|---|
| PGE2 | 24±4.8 | 83±4.1 | <0.001 |
| COX1 | 33±5.8 | 33±5.7 | 0.480 |
| COX2 | 41±6.3 | 59±6.2 | 0.022 |
Discussion
In this study, we observed that VAs exhibited
substantially higher expression of PGE2 and COX-2 compared to TAs,
while COX-1 expression showed no notable differences. Association
analyses further revealed that in VAs, PGE2 expression showed a
weak-to-moderate association with COX-1 and a weak association with
COX-2, whereas such associations were not observed in TAs. These
findings suggest a distinct upregulation of the PGE2 signaling
pathway in VAs, potentially contributing to their unique biological
and clinical characteristics (9,10).
Previous reviews have reported that VAs tend to occur more
frequently in the distal colon, which is consistent with our
findings (2). Case-based
literature often describes VAs as large lesions associated with
marked clinical manifestations, such as electrolyte disturbances
seen in McKittrick-Wheelock syndrome (2). In contrast, many VAs in our cohort
were incidentally detected and did not present with overt symptoms,
which likely explains their comparatively smaller size despite
still being significantly larger than TAs. In our institutional
experience, larger VAs showed a tendency to develop electrolyte
derangements (data not shown), supporting the notion that lesion
size may contribute to the likelihood of clinically significant
secretory activity.
The pivotal role of the PGE2 signaling axis in
colorectal tumorigenesis and progression has been well documented
(9,10). PGE2, primarily produced via
COX-2-mediated catalysis, promotes colorectal carcinogenesis by
enhancing cell proliferation, angiogenesis, and immune evasion
(9-11).
Our findings of elevated PGE2 and COX-2 expression in VAs align
with this understanding, suggesting that VAs may represent lesions
with a more aggressive molecular phenotype compared to TAs. In
contrast, the absence of significant associations in TAs indicates
that PGE2 signaling is less active in these lesions, consistent
with their generally lower malignant potential (1).
Previous studies have also indicated that COX-1 may
participate in PGE2 biosynthesis and colorectal neoplasia,
particularly in the early stages of adenoma development (12). This is further supported by
evidence showing that combined COX-1 and COX-2 activity is elevated
in non-neoplastic colonic mucosa from patients with colorectal
neoplasia (13). These data
suggest that COX-1, traditionally considered a constitutive enzyme,
may play a complementary role alongside COX-2 in the biology of
VAs. Although COX-1 is classically regarded as a constitutive
isoform, emerging evidence suggests that its functional
contribution may be selectively amplified in pre-neoplastic and
neoplastic contexts without a corresponding increase in protein
abundance. In intestinal tumorigenesis models, COX-1-derived PGE2
production has been shown to drive the early phase of polyp
initiation before COX-2 induction (14). In our study, COX-1 expression
levels were comparable between TAs and VAs; however, a significant
association with PGE2 was observed only in VAs. This may reflect
the villous architecture, characterized by a large surface area,
high secretory activity, and rapid epithelial turnover,
facilitating more efficient coupling between constitutively
expressed COX-1 and downstream prostanoid synthesis.
Clinically, our findings underscore the importance
of early colonoscopic evaluation and timely intervention in
patients with suspected EDS. VAs are well recognized as the
principal cause of EDS due to their copious secretion of potassium-
and chloride-rich mucus, driven in part by PGE2-mediated mechanisms
(3,4,8). The
markedly elevated PGE2 and COX-2 expression observed in our VA
cohort reinforces the mechanistic link between PGE2 overproduction
and the secretory diarrhea and electrolyte imbalance characteristic
of EDS (4,8). Although VAs are typically managed
with endoscopic or surgical resection (1,7), our
findings highlight the need for prompt recognition and early
treatment in patients presenting with secretory diarrhea,
dehydration, or electrolyte disturbances suggestive of EDS.
Short-term COX inhibition has been reported to ameliorate
PGE2-driven secretory symptoms and may serve as a bridging measure
before definitive resection.
The use of COX-2 selective inhibitors or NSAIDs
could also be considered as temporary supportive therapy to
mitigate secretory symptoms by suppressing PGE2 synthesis (15), although this must be balanced
against the known gastrointestinal and cardiovascular risks
associated with long-term COX-2 inhibition (16,17).
Beyond these immediate implications, understanding
the distinct PGE2 signaling patterns in VAs may provide insights
into early tumorigenic processes, as VAs represent an intermediate
stage between benign adenomas and malignant transformation
(9,10). Advances in digital pathology
(18) and molecular profiling,
including liquid biopsy (19), may
further enhance the precision of VA characterization in future
studies.
This study has several limitations. First, the
retrospective single-center design and small sample size limit the
generalizability of our findings. The number of evaluable VAs was
constrained by the availability of well-preserved archival tissue,
reducing statistical power, particularly for subgroup and
association analyses, and likely contributing to some
nonsignificant results. Second, the 10% positivity cutoff for
immunohistochemistry is not universally standardized and remains an
empirical threshold, although interobserver agreement was high.
Third, we evaluated only PGE2, COX-1, and COX-2 expression and did
not assess downstream pathways or additional regulatory molecules,
limiting mechanistic interpretation. Finally, the lack of
multicenter validation and functional assays underscores the need
for further studies to confirm and expand upon these findings.
In conclusion, this study demonstrates that VAs
exhibit marked activation of the PGE2 signaling pathway, driven by
increased COX-2 expression and strengthened functional coupling
with COX-1. This coordinated upregulation provides a mechanistic
explanation for both the secretory phenotype and the development of
EDS in affected patients. These findings underscore the importance
of early recognition and timely intervention for suspected EDS and
suggest that short-term modulation of PGE2 synthesis may serve as a
potential perioperative strategy to alleviate severe secretory
symptoms prior to definitive resection.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SF conceived and designed the study, performed data
analysis and drafted the manuscript. HF contributed to data
acquisition, assisted in writing and participated in patient
management. KD, TT, MH, KN and TH were responsible for reviewing
the patients' postoperative clinical course, acquisition of data
and data verification. AI and NM conducted immunohistochemistry and
performed laboratory analyses. YO made a substantial contribution
to the conception of the study, provided overall supervision and
critically revised the manuscript. SF and HF confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
This study was conducted in accordance with The
Declaration of Helsinki and was approved by the Ethics Committee of
Minoh City Hospital (approval no. R0311B64). The requirement for
written informed consent for the use of residual specimens was
waived due to the retrospective design, and study information was
disclosed on the hospital website to provide patients the
opportunity to decline participation (opt-out procedure).
Patient consent for publication
The requirement for individual patient consent for
publication was waived, as this study was conducted under an
institutional opt-out policy.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, an AI tool was
used to improve the readability and language of the manuscript, and
subsequently, the authors revised and edited the content produced
by the AI tool, taking full responsibility for the ultimate content
of the present manuscript.
References
|
1
|
Myers DJ and Arora K: Villous Adenoma. In:
Disclosure: Komal Arora declares no relevant financial
relationships with ineligible companies. StatPearls Publishing,
Treasure Island, FL, 2025.
|
|
2
|
Orchard MR, Hooper J, Wright JA and
McCarthy K: A systematic review of McKittrick-Wheelock syndrome.
Ann R Coll Surg Engl. 100:1–7. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Steven K, Lange P, Bukhave K and
Rask-Madsen J: Prostaglandin E2-mediated secretory diarrhea in
villous adenoma of rectum: effect of treatment with indomethacin.
Gastroenterology. 80:1562–1566. 1981.PubMed/NCBI
|
|
4
|
Smelt AH, Meinders AE, Hoekman K, Noort WA
and Keirse MJ: Secretory diarrhea in villous adenoma of rectum:
Effect of treatment with somatostatin and indomethacin.
Prostaglandins. 43:567–572. 1992.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Choi WH, Ryuk J, Kim HJ, Park SY, Park JS,
Kim JG and Choi GS: A case of giant rectal villous tumor with
severe fluid-electrolyte imbalance treated by laparoscopic low
anterior resection. J Korean Surg Soc. 82:325–329. 2012.PubMed/NCBI View Article : Google Scholar
|
|
6
|
McKittrick LS and Wheelock FC: Carcinoma
of the colon 1954. Dis Colon Rectum. 40:1494–1496. 1997.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Chaudhry H, Iqbal H, Gill A and Prajapati
D: McKittrick-Wheelock syndrome: A rare cause of chronic diarrhea
treated with endoscopic polypectomy. SAGE Open Med Case Rep.
11(2050313X231177762)2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Matsuura N, Kawano A, Tai H and Imamura T:
McKittrick-wheelock syndrome (Electrolyte Depletion Syndrome).
Intern Med. 56:1113–1114. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Wang D and Dubois RN: The role of COX-2 in
intestinal inflammation and colorectal cancer. Oncogene.
29:781–788. 2010.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Greenhough A, Smartt HJ, Moore AE, Roberts
HR, Williams AC, Paraskeva C and Kaidi A: The COX-2/PGE2 pathway:
Key roles in the hallmarks of cancer and adaptation to the tumour
microenvironment. Carcinogenesis. 30:377–386. 2009.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Buchanan FG, Wang D, Bargiacchi F and
DuBois RN: Prostaglandin E2 regulates cell migration via the
intracellular activation of the epidermal growth factor receptor. J
Biol Chem. 278:35451–35457. 2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Williams CS, Mann M and DuBois RN: The
role of cyclooxygenases in inflammation, cancer, and development.
Oncogene. 18:7908–7916. 1999.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Jensen TSR, Mahmood B, Damm MB, Backe MB,
Dahllöf MS, Poulsen SS, Hansen MB and Bindslev N: Combined activity
of COX-1 and COX-2 is increased in non-neoplastic colonic mucosa
from colorectal neoplasia patients. BMC Gastroenterol.
18(31)2018.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Pannunzio A and Coluccia M:
Cyclooxygenase-1 (COX-1) and COX-1 inhibitors in cancer: A review
of oncology and medicinal chemistry literature. Pharmaceuticals
(Basel). 11(101)2018.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Bertagnolli MM, Eagle CJ, Zauber AG,
Redston M, Solomon SD, Kim K, Tang J, Rosenstein RB, Wittes J,
Corle D, et al: Celecoxib for the prevention of sporadic colorectal
adenomas. N Engl J Med. 355:873–884. 2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Limburg PJ and Cerhan JR: Aspirin
chemoprevention for colorectal cancer: Helpful, harmful, or still
too soon to tell? Gastroenterology. 133:717–718. 2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Solomon SD, McMurray JJ, Pfeffer MA,
Wittes J, Fowler R, Finn P, Anderson WF, Zauber A, Hawk E and
Bertagnolli M: Adenoma Prevention with Celecoxib (APC) Study
Investigators. Cardiovascular risk associated with celecoxib in a
clinical trial for colorectal adenoma prevention. N Engl J Med.
352:1071–1080. 2005.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Bokhorst JM, Nagtegaal ID, Fraggetta F,
Vatrano S, Mesker W, Vieth M, van der Laak J and Ciompi F: Deep
learning for multi-class semantic segmentation enables colorectal
cancer detection and classification in digital pathology images.
Sci Rep. 13(8398)2023.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Parikh AR, Leshchiner I, Elagina L, Goyal
L, Levovitz C, Siravegna G, Livitz D, Rhrissorrakrai K, Martin EE,
Van Seventer EE, et al: Liquid versus tissue biopsy for detecting
acquired resistance and tumor heterogeneity in gastrointestinal
cancers. Nat Med. 25:1415–1421. 2019.PubMed/NCBI View Article : Google Scholar
|