Introduction
Cystic echinococcosis is a zoonotic parasitic
disease caused by Echinococcus granulosus, with humans
serving as incidental hosts (1).
The disease, endemic in specific geographic regions, most notably
the Mediterranean and the Middle East, is a zoonosis caused by
Echinococcus granulosus larvae in areas where there is a
close link between sheep, dogs and humans (2). Echinococcal cysts are most commonly
located in the liver (59-75%); whereas extrahepatic involvement has
been reported less frequently, with the lungs representing the
second most common site (27%). Isolated hydatid cysts in organs
such as the spleen, heart, kidneys, bones, brain, pancreas and
retroperitoneal space are rare (3).
E. granulosus, the causative agent of the
disease, belongs to the Taeniidae family of the Cestoda class
(1). In terms of genetic and
biological characteristics, a total of six different types of E.
granulosis have been identified (sheep, cattle, horse, camel,
pig and deer). Of these, four are pathological for human health:
E. granulosus (disease, cystic echinococcosis), E.
multilocularis (disease, alveolar echinococcosis), E.
vogeli and E. oligarthrus (disease, polycystic
echinococcosis) (4).
Hydatid disease remains a notable public health
issue in endemic regions, in large part due to insufficient
preventive healthcare measures. In addition, extrahepatic hydatid
cysts often do not present with clinical symptoms, and most cases
are asymptomatic (5). At present,
imaging studies serve as the cornerstone of diagnosis, where
radiological findings may range from purely cystic to a more
complex, solid appearance. Characteristic radiologic features
include the ‘floating membrane’ sign, which is due to detachment of
the endocyst from the pericyst, and is often accompanied by
multiple daughter cysts; however, the rarity of extrahepatic
involvement and the absence of typical imaging features can make
diagnosis challenging (6).
The present study aimed to evaluate the diagnosis,
clinical characteristics and treatment of isolated extrahepatic
cysts, hydatid cysts and hepatic cysts occurring in various regions
of the abdominal cavity, and report the cohort results.
Materials and methods
The medical records of patients, who were surgically
treated for intra-abdominal extrahepatic hydatid disease at Erciyes
University School of Medicine Hospital (Kayseri, Turkey) between
January 2010 and April 2020, were retrospectively analysed. The
present study was performed in accordance with the principles of
the World Medical Association Declaration of Helsinki and was
approved by the Local Ethics Committee of Erciyes University
Faculty of Medicine (approval no. 279; date, June 2020). Although
informed consent was not obtained due to the retrospective nature
of the study, pre-operative informed consent was obtained for all
interventional and surgical procedures performed. The study
included patients >18 years of age who were diagnosed with
extrahepatic hydatid cysts in the Department of Surgery, Erciyes
University, and underwent surgical treatment. Patients with
isolated liver cysts only, those lacking imaging or
clinical-demographic data, those without postoperative follow-up
data and those who did not undergo surgical treatment were excluded
from the study. Among the 341 patients who underwent surgery for
intra-abdominal hydatid disease, extrahepatic cysts were identified
in 49 cases. Due to missing data or loss to follow-up, 8 patients
were excluded from the present study, and the remaining 41 patients
were included in the final analysis. Following ethics approval,
patient charts, electronic records, pathology and operative reports
and anaesthesia records were examined. Using this data, the
following specific factors were retrospectively analysed:
Demographic characteristics, cyst localization, serologic test
results, intraoperative findings, surgical procedures, length of
hospital stay, postoperative medical treatment and recurrence
status.
For preoperative diagnostic evaluation, patients
underwent ultrasound (US), computed tomography (CT) and/or magnetic
resonance imaging (MRI), either individually or in combination. The
choice of diagnostic modality was based on the clinician's
experience and the diagnostic performance of the imaging method
(e.g., CT was performed in some patients when US did not provide a
definitive diagnosis). Regarding serological testing, a positive
result was defined as a titre of ≥1/320 in the indirect
haemagglutination assay (IHA). Western blot (WB) test analysis was
performed using parasite-derived tissue protein extracts. Proteins
were extracted using radioimmunoprecipitation assay buffer (50 mM
Tris-HCl, 150 mM NaCl, 1% NP-40, 0.5% sodium deoxycholate and 0.1%
SDS) supplemented with a protease inhibitor cocktail
(MilliporeSigma). Protein concentrations were determined using the
bicinchoninic acid assay. Equal amounts of protein (30 µg per lane)
were separated on 12% SDS-polyacrylamide gels and transferred onto
polyvinylidene difluoride membranes. Membranes were blocked with 5%
non-fat dry milk in Tris-buffered saline containing 0.1% Tween-20
(TBST; MilliporeSigma) for 1 h at room temperature. Membranes were
incubated overnight at 4˚C with patient sera diluted 1:200 as the
primary antibody, followed by incubation with horseradish
peroxidase (HRP)-conjugated anti-human IgG secondary antibody
(1:5,000; MilliporeSigma) for 1 h at room temperature. β-actin was
used as a reference protein. Immunoreactive bands were visualized
using enhanced chemiluminescence substrate (MilliporeSigma), and
the presence of a p7 band was considered a positive result.
Statistical analyses were performed using IBM SPSS
22.0 (IBM Corp.). Normal distribution of data was analyzed using
Kolmogorov-Smirnov and Shapiro-Wilk tests. Continuous variables
were presented as the mean ± standard deviation, whereas nominal
variables were expressed as frequencies (n) and percentages (%) and
were compared using the Fisher's Exact (used to compare groups with
sample sizes <5). P<0.05 was considered to indicate a
statistically significant difference.
Results
Data from 41 patients who met the study inclusion
criteria were analysed, revealing 30 cases of isolated extrahepatic
hydatid disease and 11 cases of extrahepatic hydatid disease with
concurrent hepatic involvement. Of these 41 patients, 14 (34.1%)
were men and 27 (65.9%) were women, with a mean age of 42.9±15.1
years (range, 19-75 years). The most common presenting symptom was
abdominal pain, reported by 22 (53.6%) patients, followed by flank
pain in 9 (21%) patients. Less frequent symptoms included urinary
retention (n=1, 2.4%), vaginal bleeding (n=1, 2.4%), lumbar pain
(n=1, 2.4%) and general malaise (n=1, 2.4%); 6 patients (14.6%)
were asymptomatic, and hydatid cysts were detected incidentally
during imaging studies performed for other reasons in these
patients. None of the patients showed any signs of acute abdominal
pathology and findings from abdominal examinations were normal in
all cases. Demographic and clinical characteristics of the 41
patients included in the present study are summarised in Table I.
 | Table IDemographic data and clinical
characteristics of patients (n=41). |
Table I
Demographic data and clinical
characteristics of patients (n=41).
| Variable | Value |
|---|
| Age, years
(range) | 42.9±15.1
(19-75) |
| Sex, n (%) | |
|
Female | 27 (65.9) |
|
Male | 14 (34.1) |
| Mean ± SD hospital
stay, days | 5.5±2.2 |
| Extrahepatic cyst
rate, n/total n (%) | 41/341 (12.0) |
|
Isolated
extrahepatic cyst | 30 (73.2) |
|
Hepatic +
extrahepatic cyst | 11 (26.8) |
| Radiological
positivity, n/total n (%) | 29/41 (70.7) |
| Average cyst
diameter, mm | 84.1±36.8 |
| IHA titre of positive
patients (n=13) | 640 (320-1,280) |
| WB positivity rate,
n/total n (%) | 18/34 (52.9) |
| Symptom, n (%) | |
|
Abdominal
pain | 22 (53.6) |
|
Flank
pain | 9 (21.0) |
|
Inability to
urinate | 1 (2.4) |
|
Vaginal
bleeding | 1 (2.4) |
|
Lumbar
pain | 1 (2.4) |
|
Malaise | 1 (2.4) |
|
No
complaints | 6 (14.5) |
For diagnostic purposes, 16 patients were evaluated
by CT, 8 by US and 3 by MRI imaging. An additional 7 patients were
evaluated by both US and CT, whereas 4 were evaluated using CT and
MRI, 2 using US and MRI and 1 patient using US, CT and MRI imaging.
Based on these data, the mean cyst diameter was calculated to be
84.12±36.78 mm. Imaging findings were suggestive of hydatid cyst in
29 (70.7%) patients, whereas no radiological indication of hydatid
disease was observed for the remaining 12 (29.3%) patients.
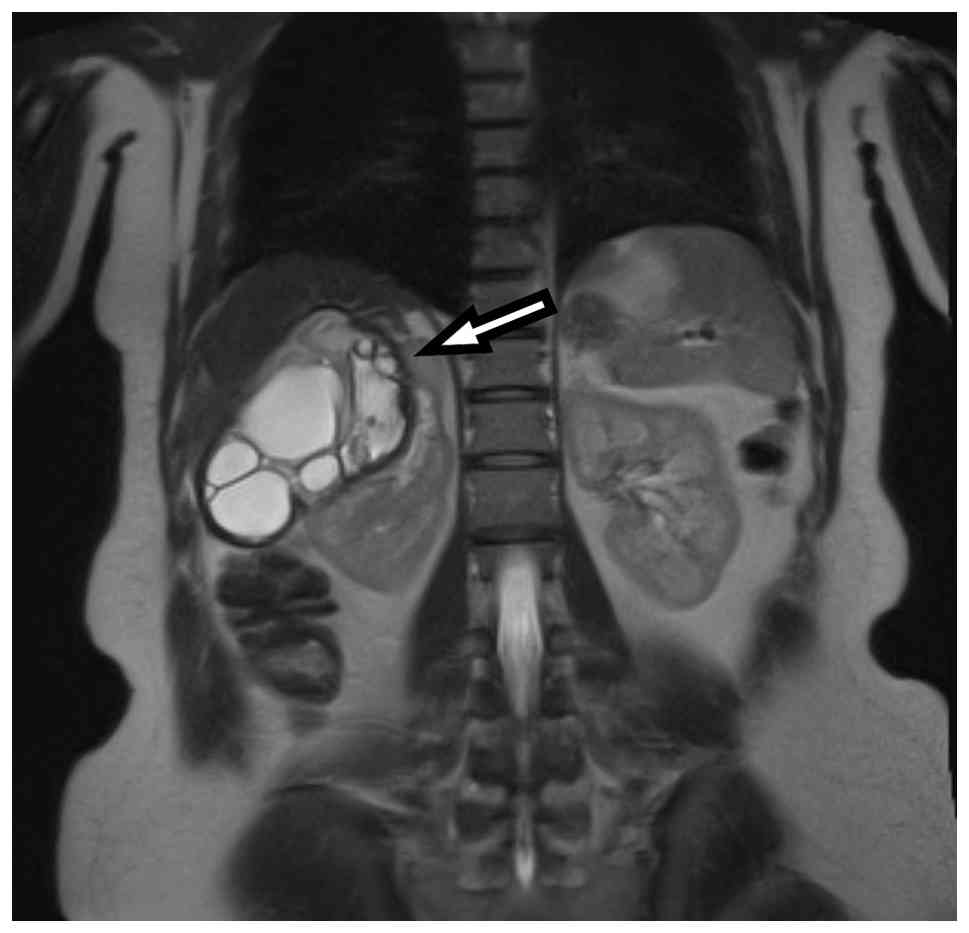
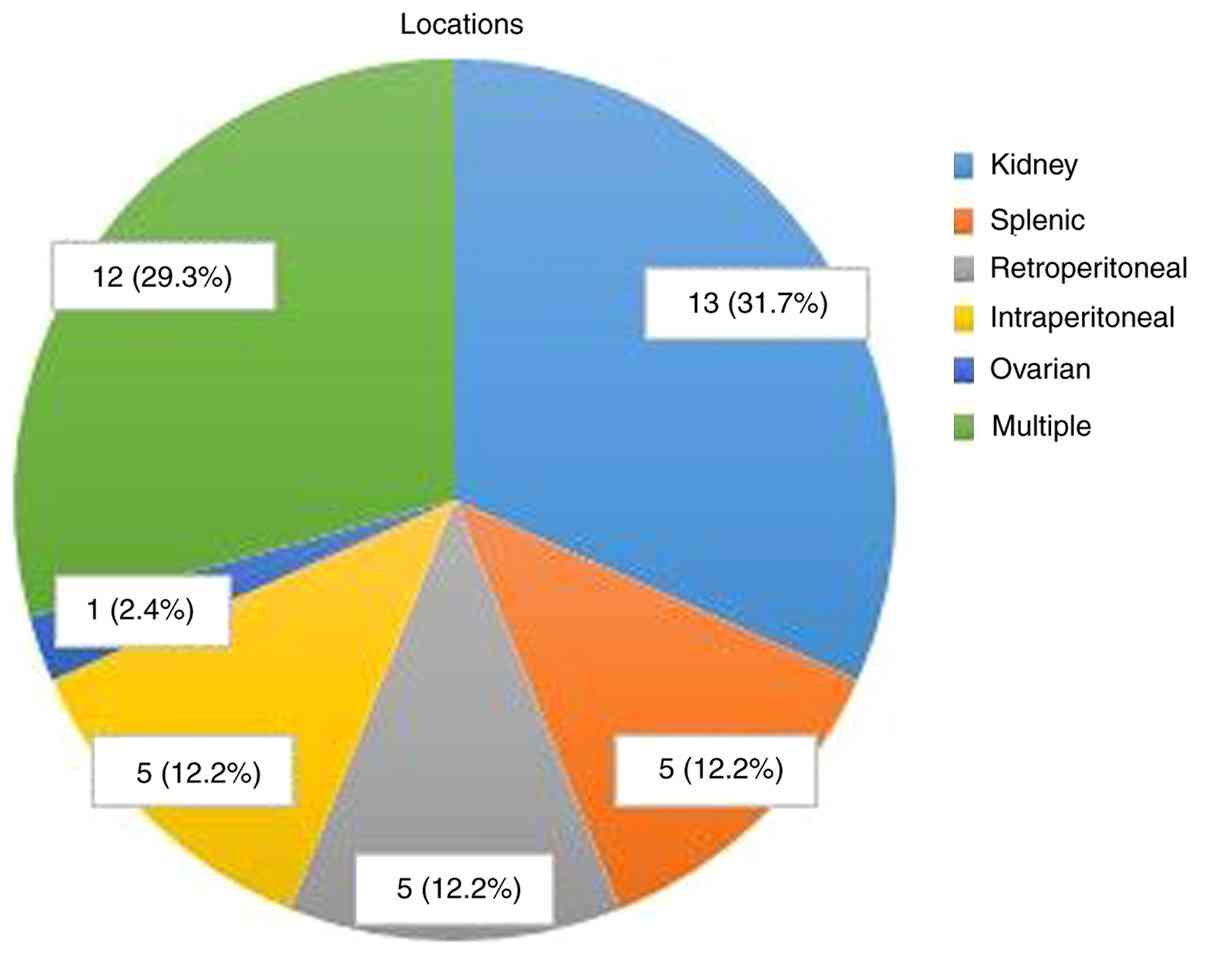
Analysis of cyst locations revealed isolated kidney
involvement in 13 patients (31.7%) (Fig. 1); isolated splenic involvement in 5
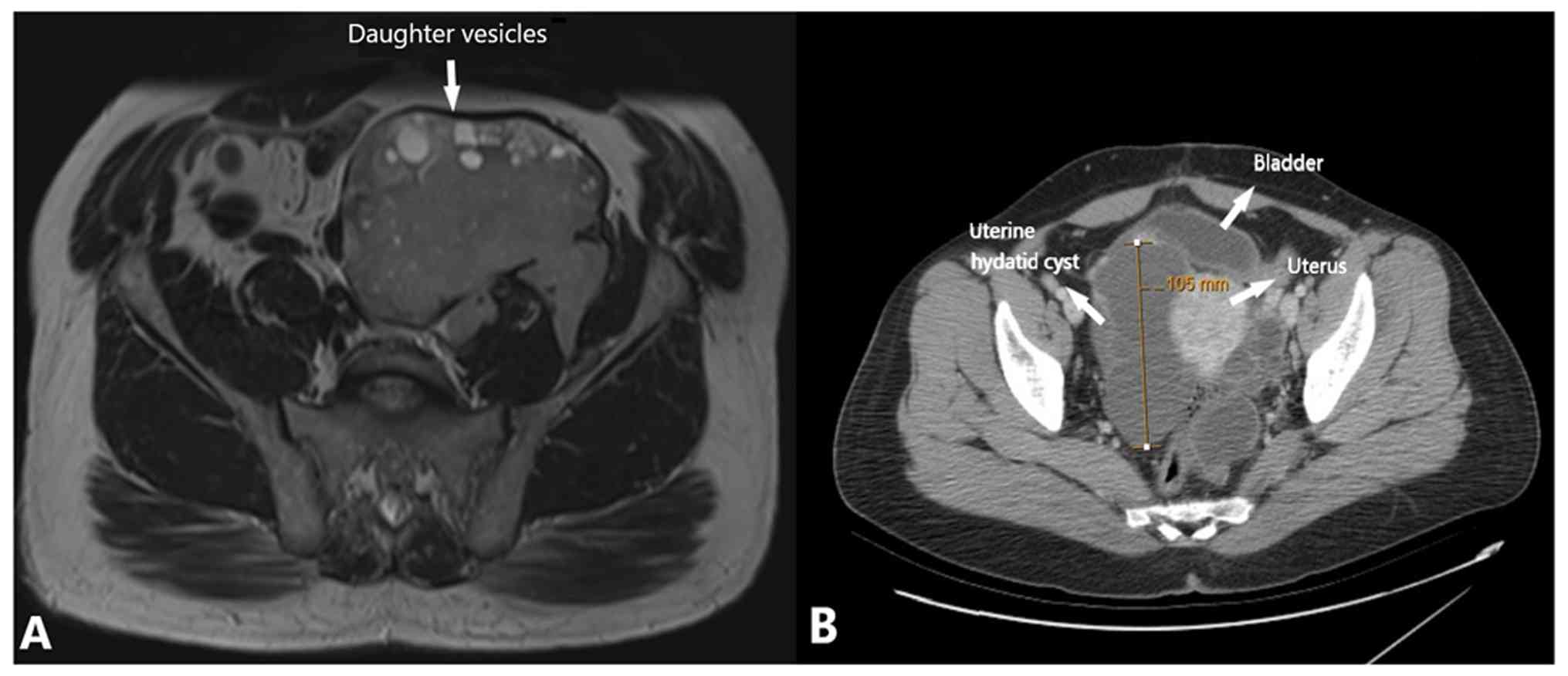
patients (12.1%); isolated retroperitoneal involvement in 5
patients (12.1%) (Fig. 2A);
isolated intraperitoneal involvement in 5 patients (12.1%); and
isolated ovarian involvement in 1 patient (Fig. 2B); cyst localization data are
summarised in Fig. 3. For the
remaining 11 patients, cysts were identified in multiple locations.
Out of the 41 patients included in the present study, 30 (73.2%)
had isolated extrahepatic hydatid cysts, whereas 11 (26.8%) also
had concurrent hepatic involvement.
Serological testing, including an IHA test and WB
analyses, were performed on 34 patients. The IHA test was positive
for 13 patients (38.2%); whereas the WB test was positive for 18
(52.9%) patients. Of the 30 patients diagnosed with isolated
extrahepatic disease, 26 underwent serological testing, with 9
(34.6%) yielding positive results (both IHA and WB). Of the 11
patients with concurrent hepatic hydatid disease, 8 underwent
serological testing and 6 (75%) tested positive for both IHA and
WB. In addition, 7 out of 10 patients with a history of previous
hydatid surgery had positive serological test results.
Out of the 41 patients included in the present
study, 31 (75.6%) had no prior history of surgery for hydatid
disease; whereas 5 patients (12%) had previously undergone surgical
and puncture, aspiration, injection, re-aspiration (PAIR)
treatments for hepatic hydatid cysts in the liver and spleen; 3
patients (7%) had surgery for pulmonary hydatid cysts; and 1
patient (2%) had surgery for both hepatic and pulmonary hydatid
cysts. In addition, 1 patient (2%) received only PAIR treatment for
hepatic hydatid cysts.
Based on analysis of the surgical procedures used
for patient treatments, 7 patients (17%) underwent simultaneous
surgery for hepatic hydatid cysts; whereas 34 patients (83%)
underwent surgery solely for extrahepatic hydatid disease. With
respect to surgical treatment procedures used, partial or total
cyst excision was performed on 28 patients (68%), a splenectomy on
5 patients (12%), a combined splenectomy and cyst excision was
performed on 4 out of these 5 patients (10%), a partial nephrectomy
on 2 patients (5%) and a total abdominal hysterectomy with
bilateral salpingo-oophorectomy was used to treat 2 patients (5%).
The mean hospital stay was 5.5±2.2 days (range, 2-12 days).
Post-operatively, 10 patients received medical therapy (albendazole
treatment was administered for varying durations depending on the
patient's clinical condition); and recurrence was observed in 4
patients (9.7%), all of whom were receiving post-operative medical
treatment. Out of the 4 patients with recurrence, 3 had undergone
concurrent surgery for intra-abdominal and hepatic hydatid
cysts.
Statistical analysis identified the following as
significant risk factors for post-operative recurrence in
extrahepatic cystic echinococcosis: Hepatic involvement (P=0.003),
the presence of cysts at multiple sites (P=0.033), the presence of
multiple cysts (P=0.001), a prior surgical history (P=0.002),
concurrent liver surgery (P=0.019) and positive results from both
serological tests (P=0.030). Factors affecting postoperative
recurrence are detailed in Table
II.
| Table IIRisk factors for recurrence in
operated extrahepatic hydatid cysts. |
Table II
Risk factors for recurrence in
operated extrahepatic hydatid cysts.
| Variable | Recurrence, n | Non-recurrence,
n | P-value |
|---|
| Sex | | | 0.107 |
|
Male | 3 | 11 | |
|
Female | 1 | 26 | |
| Cyst location | | | 0.003 |
|
Isolated
extrahepatic cyst | 0 | 30 | |
|
Hepatic +
extrahepatic cyst | 4 | 7 | |
| Number of
cysts | | | 0.001 |
| One | 0 | 28 | |
| Multiple | 4 | 9 | |
| Number of regions
in which the cyst is found | | | 0.033 |
|
Single | 1 | 29 | |
|
Multiple | 3 | 8 | |
| IHA/WB | | | 0.030 |
|
Negative | 0 | 14 | |
|
Only one
positive | 0 | 5 | |
|
Both
positive | 4 | 25 | |
| Previous cyst
surgery | | | 0.002 |
|
Negative | 0 | 31 | |
|
Positive | 4 | 6 | |
| Concurrent liver
surgery | | | 0.019 |
|
No | 1 | 32 | |
|
Yes | 3 | 5 | |
Discussion
Hydatid disease is common in endemic regions, where
it predominantly affects the liver and lungs; extrahepatic and
extrapulmonary involvement is relatively rare and can present
specific diagnostic challenges. Reported rates of extrahepatic
hydatid disease in general vary between 6.9-20.3% (7-9);
primary extrahepatic involvement without hepatic or pulmonary
disease is rare, with an incidence rate ranging from 2.1 to 11.1%
(7,10,11).
Akcam et al (8) reported an
extrahepatic involvement rate of 20.3% in the authors' cohort and
noted extra-abdominal sites, such as the central nervous system,
bones, thyroid, breasts, muscles and the heart; while the most
common intra-abdominal sites included the peritoneal cavity,
kidneys and spleen. Lianos et al (12) observed pulmonary involvement with
concurrent extrahepatic disease in 7.8% of patients, with
peritoneal and splenic involvement most frequently reported.
Another study reported a 16.3% rate of extrahepatic involvement,
predominantly in the peritoneum and spleen (9). Tsaroucha et al (11) found extrahepatic involvement in
17.8% of patients, including concurrent hepatic involvement in 6.7%
and isolated extrahepatic involvement in 11.1%, with peritoneal and
splenic sites most commonly affected. In the present study, the
rate of extrahepatic intraperitoneal involvement was 14.3%, with
the kidneys and spleen being the most frequently identified sites.
Balik et al (7) reported
that 70.4% of the patients were diagnosed with concurrent hepatic
hydatid disease, while 29.6% were found to have isolated
extrahepatic disease. By contrast, in the present study, concurrent
hepatic involvement was found in 24.3% of the patients, with
isolated extrahepatic disease observed in 75.6%. Nonetheless, while
malignant mechanisms, such as hepatic cancer, have been
well-investigated, the mechanisms governing development of
extrahepatic hydatid cysts remain to be fully clarified (13).
Similar to hepatic hydatid disease, some patients
with extrahepatic involvement also remain asymptomatic, whereas
others develop symptoms related to complications or compression of
adjacent structures by the cystic mass. In the present study, 22
patients (53.6%) presented with abdominal pain and 11 patients
(22%) reported flank pain, whereas 6 patients (12%) were
asymptomatic. In agreement with this, Gündeş et al (14) also reported abdominal and flank
pain as the predominantly reported symptoms in their cohort,
whereas Makni et al (15)
identified abdominal pain as the most common presenting complaint
(80%), while 18% of the patients were asymptomatic.
The diagnosis of hydatid disease primarily relies on
imaging studies, with serological testing used to support
radiological findings. However, diagnoses involving extrahepatic
hydatid cysts are more challenging because of their relatively
lower occurrence rate and lack of typical radiological features. US
is the preferred imaging method for the evaluation and diagnosis of
hepatic hydatid disease. A staging system consisting of five grades
has been established based on the ultrasonographic characteristics
of the cysts and the US findings (6,16).
In addition, it is also useful for diagnosing extrahepatic hydatid
disease in US-accessible regions, enabling visualisation of
daughter cysts and the germinal layer and providing diagnostic
support (6). In the present study,
out of 14 patients evaluated by US, hydatid disease was diagnosed
in 4 cases with splenic involvement and 2 with renal involvement;
however, due to the narrowness of the pelvic area and the bony
structures, US failed to diagnose cysts located in the pelvic
region.
CT can effectively detect calcified cyst walls and
provides valuable information regarding cyst size and its
relationship with adjacent organs (6). In the present study, 31 patients
underwent CT evaluation, which was used to facilitate diagnosis of
cases with intraperitoneal, retroperitoneal and renal involvement.
Inan et al (17) reported
that in addition to conventional MRI imaging, diffusion-weighted
MRI may be helpful for the diagnosis of extrahepatic hydatid cysts.
DWI images provide rapid and effective imaging, particularly in
differentiating between benign and malignant lesions, and between
simple cysts and hydatid cysts. In a 2021 study, Guo et al
(18) found that CT and MRI
demonstrated similar efficacy for the diagnosis of extrahepatic
hydatid cysts. In the present study, conventional MRI images were
evaluated, and, to the best of our knowledge, the number of
patients previously diagnosed by this MRI-based method is limited
(17). Moreover, 4 of the present
patients were evaluated using MRI, which was used to effectively
visualise internal cysts and enabled diagnosis of 2 patients with
splenic and retroperitoneal cysts. Beside this, although a
definitive preoperative radiological diagnosis could not be made in
12 of the patients included in the present study, numerous had
suspected hydatid cysts on imaging (mostly US). However, these
patients were diagnosed by perioperative imaging or
histopathological diagnosis. Furthermore, because the
Interventional Radiology Unit at Erciyes University School of
Medicine Hospital is the leading hydatid cyst diagnosis and
treatment centre in the Middle Anatolian region, US was used for
most of the diagnoses, eliminating the need to use World Health
Organization Informal Working Group on Echinococcosis
classification of cystic echinococcosis (CE), such as CE1, CE3c and
CE4(16). In addition, since the
present study was retrospective, it was not possible to apply all
three imaging methods (US, MRI or CT) to all patients; diagnosis
was made using one or more of the appropriate imaging methods.
Although serological tests using IHA and WB are
commonly used for the diagnosis of hydatid disease; their
diagnostic accuracy is reduced in patients with extrahepatic
involvement vs. those with hepatic disease (19). In the present study, of the 29
patients evaluated by serological testing, 10 patients (34.4%) were
found to be positive by IHA and 15 patients (51.7%) by WB. In the
literature, serological positivity rates range from 50-77%
(8,13,14,20).
Among these tests, WB generally demonstrates a higher positivity
rate than IHA, whereas overall serological positivity is lower in
extrahepatic vs. hepatic hydatid disease (19). Similarly, in the present study,
42.8% of patients with extrahepatic hydatid cysts tested positive
in serological assays, compared with a 75% positivity rate for
those with hepatic involvement.
Albendazole-based therapy has been shown to have
limited efficacy for the treatment of hydatid disease and is
generally only recommended for smaller (<5 cm) asymptomatic
cysts. Percutaneous treatments such as PAIR have been proposed as
first-line therapy for eligible patients with hepatic hydatid
disease (21). However, surgery
remains the preferred approach for more complicated cases, such as
those designated CE4 or CE5, as well as for patients deemed to be
unsuitable for PAIR. Experience with percutaneous treatment of
extrahepatic hydatid cysts is limited, and thus surgery is
considered the primary treatment modality for such cases (22). When pre-operative diagnosis is
uncertain, exploratory surgery may become necessary and can be used
to both eradicate the disease and prevent recurrence, while
minimising morbidity and mortality.
For surgical treatment of hepatic hydatid cysts,
complete cyst resection is associated with a low recurrence rate
and total cyst excision is preferred (1); however, when this is not feasible,
partial excision should still be considered. Organ-preserving
resections are recommended for lesions involving specific organs,
such as the kidneys, spleen or ovaries, although organ removal may
be required in cases of extensive damage. Due to technical
challenges and the high complication risks associated with partial
splenectomy, total splenectomy is recommended for splenic
involvement (23); in the present
cohort, 9 patients underwent splenectomy. For renal hydatid cysts,
kidney-preserving total or partial cyst excision is preferred. Out
of the 11 patients with kidney involvement in the present cohort, 2
patients underwent partial nephrectomy whereas 9 underwent cyst
excision.
Wani et al (24) reported a 0% recurrence rate during
follow-up in their study of 12 patients with extrahepatic
intra-abdominal hydatid cysts, and Gündeş et al (14) observed no recurrence in 22 patients
diagnosed with primary intra-abdominal hydatid cysts. In this
study, the mean follow-up period of the patients was 40 months
(range, 6-68 months). In addition, in a 2025 study involving 31
patients with extrahepatic hydatid cysts, a 0% recurrence rate was
reported after a 36-month follow-up period in patients treated
percutaneously (25). However,
contrary to these results, recurrence rates in other studies have
reached as high as 22% (11,26,27).
In the present study, a recurrence rate of 9.7% was found during
the follow-up period, which is consistent with recurrence rates
reported in the literature.
To the best of our knowledge, in the literature a
limited number of studies have been published that investigated
factors influencing recurrence rates. A study by Gollackner et
al (28) suggested that
radical surgery reduces the risk of recurrence; whereas another
study, published in 2015, identified a laparoscopic approach as the
only factor influencing recurrence and reported a higher recurrence
rate in patients that underwent laparoscopic surgery (29). The present study represents a
detailed investigation on this topic, and identified the following
factors associated with increased risk of recurrence: Hepatic
involvement, cysts located in multiple sites, multiple cysts, a
history of previous surgery, concurrent liver surgery and positive
results by both serologic tests. Due to the limited number of
patients and recurrence cases reported in the literature for
extrahepatic hydatid cysts, factors associated with recurrence may
have not been thoroughly investigated. In the present study,
extensive disease was associated both with recurrence and treatment
challenges, as evidenced by the development of recurrent disease
despite post-operative medical therapy.
Total cyst excision should be performed whenever
possible in cases with intraperitoneal and retroperitoneal lesions;
however, if total excision is not feasible, evacuation of the cyst
contents followed by partial resection should be carried out, with
careful attention to avoid contamination of the surrounding
tissues. Hamamci et al (9)
reported performing a partial cystectomy on 4 patients with
retroperitoneal hydatid cysts; one of these four patients reported
a recurrence in the same area 1 year after surgery. In the present
study, cyst excision was performed on 11 patients with peritoneal
cysts, and of these, 6 patients had retroperitoneal cysts. A total
of 4 out of these 11 patients underwent total cyst excision whereas
2 patients underwent partial cyst excision.
The present study has limitations similar to those
frequently encountered in other studies addressing this topic;
these include retrospective design, a single-centre study and a
small sample size. In addition, due to the retrospective nature of
the present study, the inability to access CT, MRI and US images of
some patients is another limitation. Moreover, diagnosis of
extrahepatic hydatid cysts is complicated by their lack of a
characteristic radiological appearance; therefore, hydatid disease
should be considered in patients presenting with cystic lesions in
atypical locations, particularly in endemic regions. Due to the
limited experience with medical and percutaneous treatments for
these cases, surgery remains the primary and most effective
treatment modality.
In conclusion, the demographic and clinical data
collected from patients included in this study and followed
throughout the study period are consistent with those reported in
the literature. Furthermore, the present results contribute to the
literature, as the present study is one of the rare studies
investigating and analyzing factors influencing recurrence.
Nevertheless, there is a need for larger-scale, multicenter
clinical trials that analyze factors affecting disease
recurrence.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
FD and MA were responsible for the conceptualization
of the present study and TT, UT and GS were responsible for the
study design. DGİ, FD and MA contributed to the analysis using
statistical software. FD, EMS and HYA checked the accuracy of the
data and analyses; FD, SC and MK conducted the formal analysis; FD
and MA were the primary investigators; FD and DGİ provided the
resources; FD and TT wrote the original draft of the manuscript
and; FD, MA and TT reviewed and edited the manuscript; and FD and
UT supervised the study. All authors have read and agreed to the
final version of the manuscript. TT and FD confirm the authenticity
of all the raw data.
Ethics approval and consent to
participate
The present research was conducted ethically
following The Code of Ethics of the World Medical Association
(Declaration of Helsinki). The responsible authorities approved the
study (Local Ethics Committee of Erciyes University Faculty of
Medicine; approval no. 279/June 2020). Although informed consent
could not be obtained from patients for the study due to its
retrospective nature, pre-operative informed consent was obtained
for all interventional and surgical procedures performed.
Patient consent for publication
Not applicable.
Competing interests
The authors declared that they have no competing
interests.
References
|
1
|
Sozuer E, Akyuz M and Akbulut S: Open
surgery for hepatic hydatid disease. Int Surg. 99:764–769.
2014.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ahmad BS, Afzal A, Ashraf P, Abubakar SA
and Munir A: Manifestation of hydatid cyst of liver with
pancreatitis, cholangitis and jaundice: A case report. J Pak Med
Assoc. 68:1097–1099. 2018.PubMed/NCBI
|
|
3
|
Kushwaha JK, Sonkar AA, Verma AK and
Pandey SK: Primary disseminated extrahepatic abdominal hydatid
cyst: A rare disease. Case Rep. 2012(bcr0220125808)2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bhutani N and Kajal P: Hepatic
echinococcosis: A review. Ann Med Surg (Lond). 36:99–105.
2018.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Ahire P, Iyer N and Gada PB: Complication
of hepatic hydatid cyst surgery presenting as obstructive jaundice.
Cureus. 15(e35410)2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Zalaquett E, Menias C, Garrido F, Vargas
M, Olivares JF, Campos D, Pinochet N, Luna A, Dahiya N and Huete Á:
Imaging of hydatid disease with a focus on extrahepatic
involvement. Radiographics. 37:901–923. 2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Balik AA, Celebi F, Başglu M, Oren D,
Yildirgan I and Atamanalp SS: Intra-abdominal extrahepatic
echinococcosis. Surg Today. 31:881–884. 2001.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Akcam AT, Ulku A, Koltas IS, Izol V, Bicer
OS, Kilicbagir E, Sakman G, Poyrzoglu H, Erman T, Aridogan IA, et
al: Clinical characterization of unusual cystic echinococcosis in
southern part of Turkey. Ann Saudi Med. 34:508–516. 2014.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Hamamci EO, Besim H and Korkmaz A: Unusual
locations of hydatid disease and surgical approach. ANZ J Surg.
74:356–360. 2004.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Mandal S and Mandal MD: Human cystic
echinococcosis: Epidemiologic, zoonotic, clinical, diagnostic and
therapeutic aspects. Asian Pac J Trop Med. 5:253–260.
2012.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Tsaroucha AK, Polychronidis AC,
Lyrantzopoulos N, Pitiakoudis MS, J Karayiannakis A, Manolas KJ and
Simopoulos CE: Hydatid disease of the abdomen and other locations.
World J Surg. 29:1161–1165. 2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Lianos GD, Lazaros A, Vlachos K, Georgiou
GK, Harissis HV, Mangano A, Rausei S, Boni L, Frattini F, Biondi A,
et al: Unusual locations of hydatid disease: A 33 year's experience
analysis on 233 patients. Updates Surg. 67:279–282. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Rizzo A and Ricci AD: Challenges and
future trends of hepatocellular carcinoma immunotherapy. Int J Mol
Sci. 23(11363)2022.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Gündeş E, Küçükkartallar T, Çakir M, Aksoy
F, Ali B and Kartal A: Ekstrahepatik yerleşimli primer
intraabdominal hidatik kist olguları. J Clin Exp Invest. 4:175–179.
2013.
|
|
15
|
Makni A, Jouini M, Kacem M and Safta ZB:
Extra-hepatic intra-abdominal hydatid cyst: Which characteristic,
compared to the hepatic location? Updates Surg. 65:25–33.
2013.PubMed/NCBI View Article : Google Scholar
|
|
16
|
WHO Informal Working Group. International
classification of ultrasound images in cystic echinococcosis for
application in clinical and field epidemiological settings. Acta
Trop. 85:253–261. 2003.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Inan N, Akhun N, Akansel G, Arslan A,
Ciftçi E and Demirci A: Conventional and diffusion-weighted MRI of
extrahepatic hydatid cysts. Diagn Interv Radiol. 16:168–174.
2010.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Guo H, Liu W, Wang J and Xing Y:
Extrahepatic alveolar echinococcus on multi-slice computed
tomography and magnetic resonance imaging. Sci Rep.
11(9409)2021.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Biava MF, Dao A and Fortier B: Laboratory
diagnosis of cystic hydatic disease. World J Surg. 25:10–14.
2001.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Aksakal N, Kement M, Okkabaz N, Altuntaş
YE and Öncel M: Unusually located primary hydatid cysts. Ulus
Cerrahi Derg. 32:130–133. 2015.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Brunetti E, Kern P and Vuitton DA: Writing
Panel for the WHO-IWGE. Expert consensus for the diagnosis and
treatment of cystic and alveolar echinococcosis in humans. Acta
Trop. 114:1–16. 2010.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Arslan S, Bakdik S, Oncu F, Tolu I and
Eryilmaz MA: Successful percutaneous treatment of extrahepatic
cystic echinococcosis through PAIR and single puncture catheter
techniques. Jpn J Radiol. 35:296–302. 2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Mejri A, Arfaoui K, Ayadi MF, Aloui B and
Yaakoubi J: Primitive isolated hydatid cyst of the spleen: Total
splenectomy versus spleen saving surgical modalities. BMC Surg.
21(46)2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Wani RA, Malik AA, Chowdri NA, Wani KA and
Naqash SH: Primary extrahepatic abdominal hydatidosis. Int J Surg.
3:125–127. 2005.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Kahriman G, Onem MM and Talih G:
Percutaneous management of extrahepatic cystic echinococcosis:
Long-term outcomes and insights on rare locations. J Vasc Interv
Radiol. 36:1567–1575. 2025.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Chautems R, Buhler L, Gold B, Chilcott M,
Morel P and Mentha G: Long term results after complete or
incomplete surgical resection of liver hydatid disease. Swiss Med
Wkly. 133:258–262. 2003.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Cirenei A and Bertoldi I: Evolution of
surgery for liver hydatidosis from 1950 to today: Analysis of a
personal experience. World J Surg. 25:87–92. 2001.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Gollackner B, Längle F, Auer H, Maier A,
Mittlböck M, Agstner I, Karner J, Langer F, Aspöck H, Loidolt H, et
al: Radical surgical therapy of abdominal cystic hydatid disease:
Factors of recurrence. World J Surg. 24:717–721. 2000.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Jerraya H, Khalfallah M, Osman SB, Nouira
R and Dziri C: Predictive factors of recurrence after surgical
treatment for liver hydatid cyst. Surg Endosc. 29:86–93.
2015.PubMed/NCBI View Article : Google Scholar
|