Introduction
Syphilis is a sexually transmitted infection caused
by the spirochete Treponema pallidum (1,2).
Despite its long history, syphilis continues to pose a notable
public health challenge due to its ability to mimic a wide array of
clinical conditions. Neurosyphilis (NS), a severe complication
resulting from the invasion of Treponema pallidum into the
central nervous system, can occur at any stage of syphilis.
Historically, up to ~30% of untreated patients with syphilis
developed NS; however, with antibiotic treatment, symptomatic NS is
now estimated to occur in 1.5-13% of syphilis cases, and cohort
data indicate that, among individuals with human immunodeficiency
virus (HIV) infection, the incidence of NS is twice that of those
without HIV infection (3,4). Cerebral syphilitic gummata (CSG) are
rare manifestations typically associated with tertiary syphilis
(5). In Cushing's (6) frequently cited case series of 2,203
intracranial tumors published in 1932, only 12 cases (0.5%) were
identified as CSG. In a review of intracranial tumors by Grant
(7) in 1956, which included 2,326
patients, only 5 cases (0.2%) were diagnosed as CSG. Likewise,
Katsura et al (8), in a
review of all neurosurgical cases in Japan prior to 1959,
identified only 12 cases of syphilitic gummas among 3,312 patients,
yielding an incidence of 0.4%. Although large-scale retrospective
studies from recent years are lacking, the limited number of
sporadic case reports published over the past two decades suggests
that CSG has become an even rarer disease entity. The gummata are
granulomatous lesions that may develop in various organs, including
the brain, as a consequence of a chronic inflammatory response to
persistent infection (9). Within
the central nervous system, these lesions can give rise to diverse
neurological symptoms depending on lesion size and location,
including headaches, seizures, focal neurological deficits,
cognitive impairment and behavioral disturbances. Owing to their
rarity and heterogeneous presentation, CSG are frequently
misdiagnosed or mistaken for other conditions, such as neoplasms,
abscesses or other infectious or inflammatory disorders (10). The present study reports a case of
CSG in a 60-year-old male patient who rapidly developed hemiplegia
of the right upper and lower limbs over several days. The present
case underscores the importance of considering NS in patients
presenting with atypical neurological symptoms, particularly those
with risk factors for syphilis infection.
Case report
Patient information
A 60-year-old man with a 6-month history of syphilis
was admitted to to Jiangnan University Medical Center (Wuxi, China)
in December 2023 for progressive right-sided limb weakness and
slurred speech over a 2-week period. On admission, the patient
presented with complete right-sided hemiplegia. The patient's
medical history was unremarkable, with no hypertension, diabetes or
other chronic illnesses, and the patient was not taking any regular
medications and denied any substance abuse. There was no family
history of sexually transmitted infections or related
conditions.
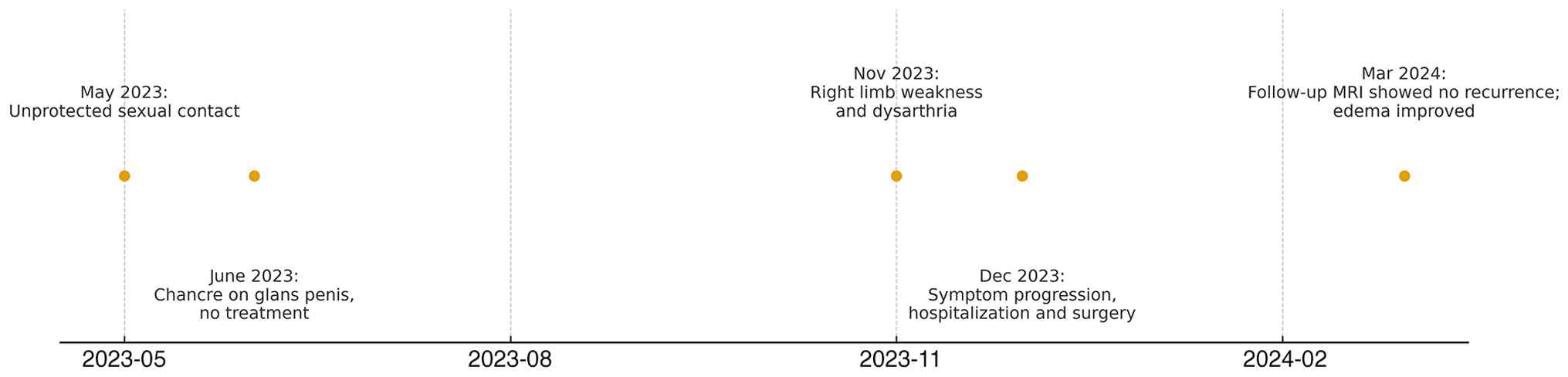
Because the lesion, which was detected during the
present hospitalization on brain magnetic resonance imaging (MRI)
as a left frontal parasagittal mass, exhibited a firm consistency
during surgical resection, appearing grayish, poorly circumscribed
and lacking a clear capsule, which differed from that of typical
neoplastic lesions, a review of the patient's medical history was
conducted after surgery and revealed that the patient had a single
hard chancre, that was 0.5x0.5 cm in size, on the glans penis that
appeared ~20 days after a sexual encounter 6 months prior to
presentation at the hospital; however, the patient did not receive
any treatment at the time. The clinical course is summarized in a
timeline diagram (Fig. 1).
Clinical presentation
During the initial examination, the patient
demonstrated slurred speech with dysarthria. Neurological
assessment revealed right-sided hemiparesis accompanied by mild
hyperreflexia. Cranial nerve function was intact, and the remainder
of the physical examination was unremarkable. The patient exhibited
no signs of meningismus, and the vital signs were stable.
Diagnostic workup
Initial laboratory tests, including complete blood
count, basic metabolic panel and liver function tests, were within
normal limits. Infectious disease screening showed a
signal-to-cutoff ratio value of 26.91 for Treponema pallidum
antibodies; testing for HIV was negative at the time of admission.
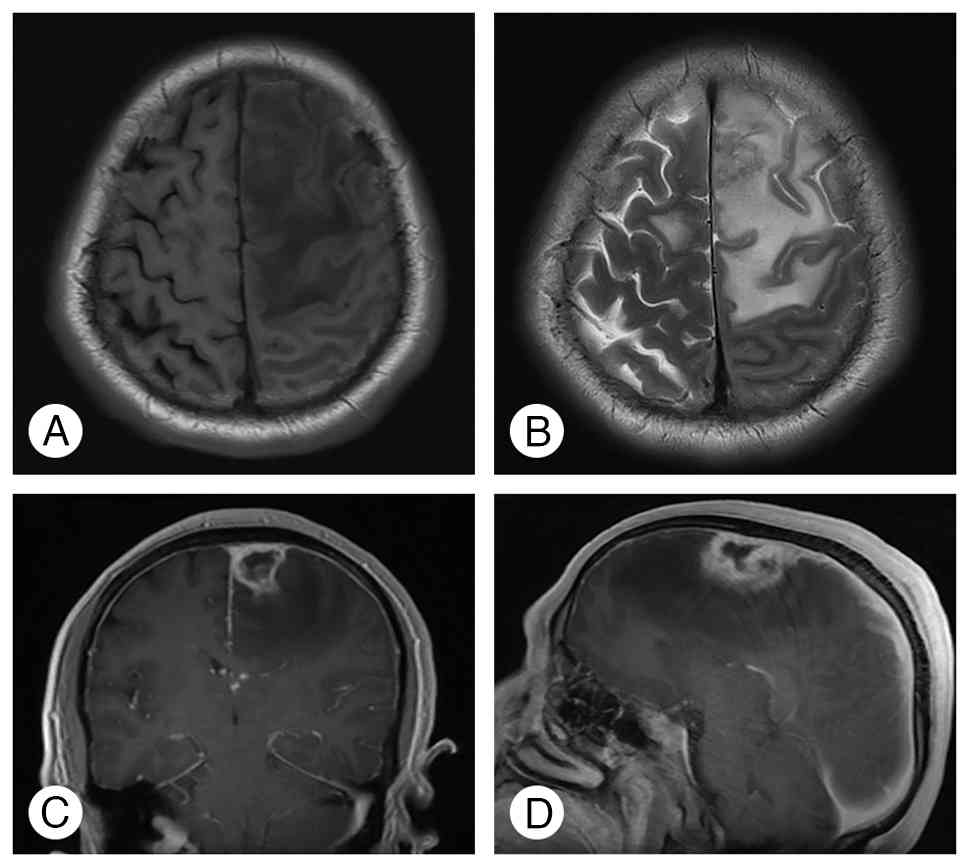
Given the neurological deficits of the patient, brain MRI was
performed, which demonstrated a nodule in the left frontal lobe
with extensive surrounding edema. On contrast-enhanced imaging, the
lesion appeared as an abnormally enhancing mass measuring ~18x21x28
mm, involving the adjacent dura mater and the falx cerebri
(Fig. 2).
Treatment
Based on the clinical symptoms and imaging findings,
a preliminary diagnosis of a left frontal lobe space-occupying
lesion was made, with the consideration of a malignant neoplastic
lesion or metastatic tumor; however, a high-grade glioma could not
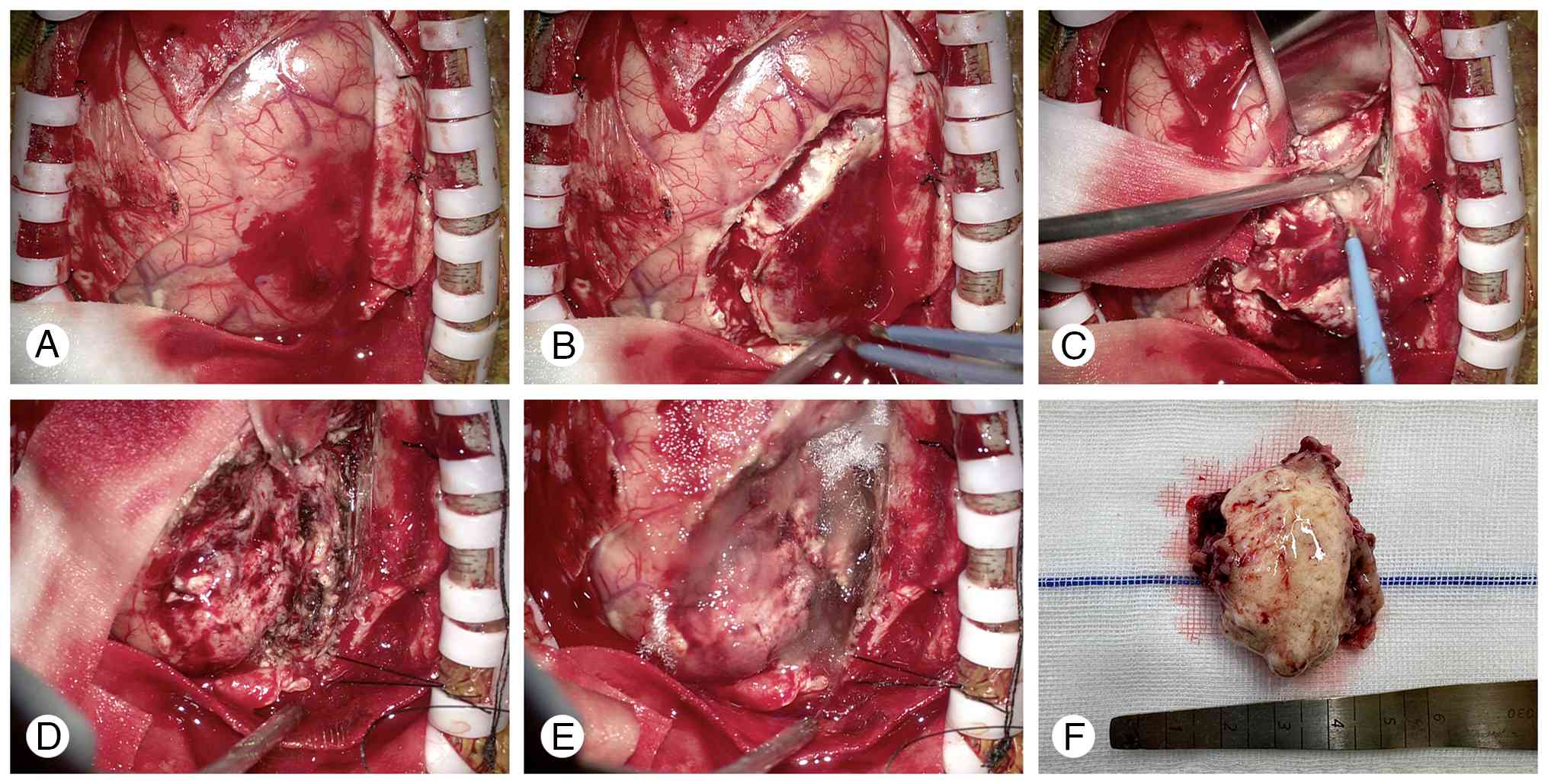
be excluded. Consequently, the patient underwent a craniotomy for
the resection of the intracranial mass. Intraoperatively, a
gray-yellow lesion was observed near the midline of the left
frontal lobe, which was markedly adherent to the meninges and falx
cerebri; the lesion had a firm texture and lacked a distinct
capsule, and swelling of the brain tissue was evident. Under the
microscope, dissection was performed along the surrounding edema
zone of the lesion until a complete resection was achieved. During
the craniotomy, the intracranial pressure was elevated and marked
brain bulging was observed; consequently, the local bone flap was
removed. The bone flap was not replaced at wound closure, resulting
in a left frontal decompressive craniectomy (Fig. 3). During follow-up, cerebral edema
gradually resolved; however, no secondary cranioplasty was
performed because the patient declined cranial reconstruction.
Postoperatively, the patient was treated with routine measures such
as dehydration therapy to reduce intracranial pressure.
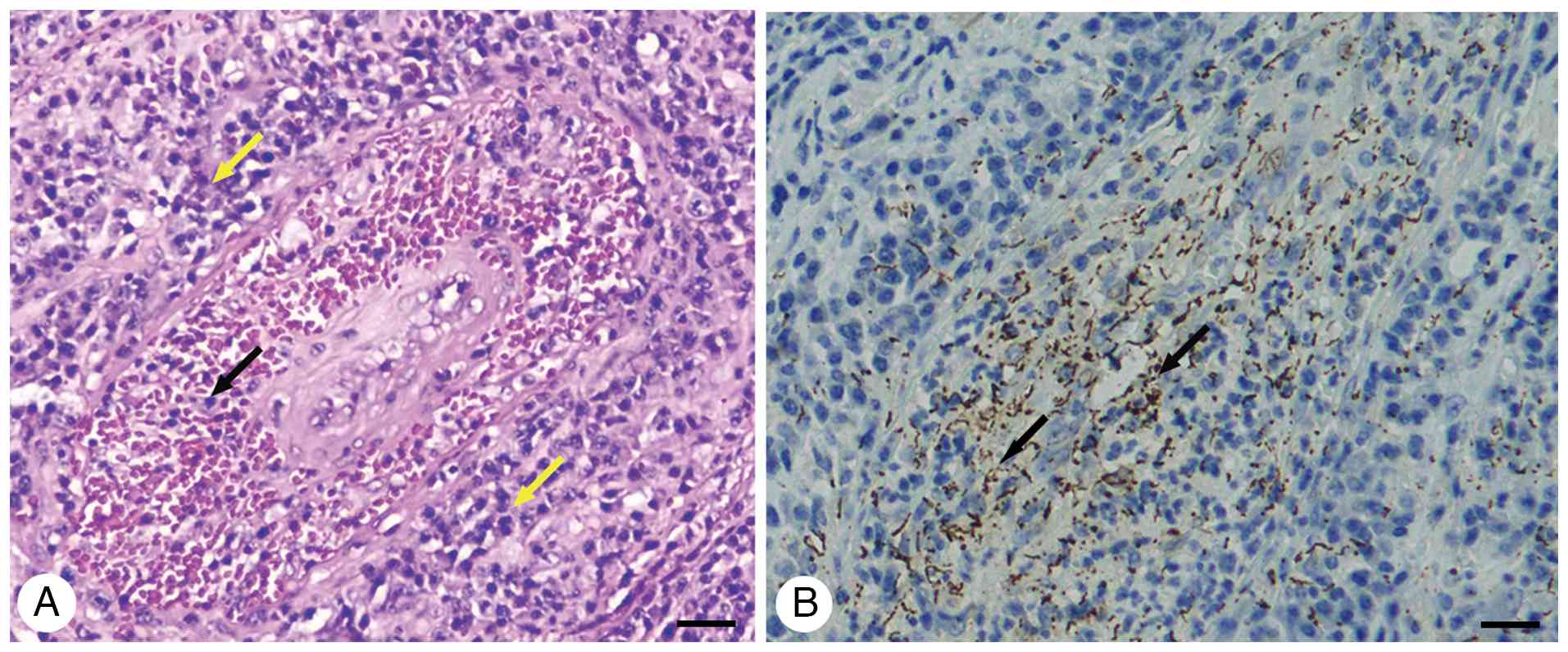
Intraoperatively, it was observed that the lesion
was firmer than commonly encountered neoplastic lesions, and
histopathological analysis confirmed the diagnosis of a gummatous
lesion consistent with tertiary syphilis, showing granulomatous
inflammation with central necrosis, surrounded by lymphocytes,
plasma cells and macrophages. For histopathological examination,
the resected tissue was fixed in 10% neutral buffered formalin at
room temperature for 24 h, embedded in paraffin and sectioned at a
thickness of 4 µm. Sections were stained with H&E using
standard protocols at room temperature, with hematoxylin staining
for 5 min followed by eosin staining for 2 min. Microscopic
evaluation was performed using a light microscope at magnifications
of x100 and x400. No evidence of malignancy or other infectious
agents was found. Extensive plasma cell infiltration was observed
around the small vessels in the brain tissue, leading to the
formation of vasculitis.
For immunohistochemical analysis, the resected
tissue was fixed in 10% neutral buffered formalin at room
temperature for 24 h, paraffin-embedded and sectioned at a
thickness of 4 µm. Sections were deparaffinized in xylene and
rehydrated through a descending ethanol series (100, 95, 85 and
75%), followed by rinsing in PBS (41404ES76; Shanghai Yeasen
Biotechnology Co., Ltd.). Antigen retrieval was performed by
heating the sections in citrate buffer (pH 6.0) at 95-100˚C for 15
min. Endogenous peroxidase activity was quenched by incubation with
3% hydrogen peroxide. The sections were permeabilized with 0.1%
Triton X-100 and blocked with 5% normal goat serum (36119ES10;
Shanghai Yeasen Biotechnology Co., Ltd.) at room temperature for 30
min. Sections were incubated overnight at 4˚C with a commercially
available imported primary antibody against Treponema pallidum
(dilution, 1:200; ZA-0199; Beijing Zhongshan Jinqiao Biotechnology
Co., Ltd.). After washing with PBS (41404ES76; Shanghai Yeasen
Biotechnology Co., Ltd.), an HRP-conjugated goat anti-rabbit
secondary antibody (dilution, 1:500; ab6721; Abcam) was applied at
room temperature for 30 min. Chromogenic detection was performed
using 3,3'-diaminobenzidine. Immunostained sections were examined
and imaged using a light microscope at magnifications of x200 and
x400. Immunohistochemical staining with anti-syphilis spirochetes
antibodies revealed numerous brown spirochetes (Fig. 4A and B).
Routine cerebrospinal fluid (CSF) testing and
biochemical analysis were performed postoperatively. The CSF was
clear in appearance, with a normal cell count and a protein
concentration of 48.2 mg/dl (reference range, 15-45 mg/dl). Serum
and CSF toluidine red unheated serum test (TRUST) and Treponema
pallidum particle agglutination (TP-PA) tests were performed;
the serum TRUST test showed a result of 1:64, whereas the result in
the CSF was negative. The syphilis antibody by TP-PA results for
both serum (18.84) and CSF (23.30) were markedly higher than the
reference range (<1); these results are presented in Table I.
 | Table ISyphilis test results. |
Table I
Syphilis test results.
| Sample | Test | Result | Reference range |
|---|
| Serum | TRUST | 1:64 | Negative |
| Serum | Syphilis Ab by TP-PA,
S/CO | 18.84 | <1 |
| Serum | HIV status | Negative | Negative |
| CSF | TRUST | Negative | Negative |
| CSF | Syphilis Ab by TP-PA,
S/CO | 23.30 | <1 |
| CSF | WBCs
(x106/l) | 5 | 0-8 |
| CSF | Protein, mg/dl | 48.2 | 15-45 |
After a definitive pathological diagnosis, the
patient was started on high-dose intravenous penicillin G (24
million units per day, administered as 6 million units every 6 h)
for 14 days to address the remaining infection in the central
nervous system. Corticosteroid therapy was also initiated to reduce
postoperative cerebral edema and mitigate the risk of the
Jarisch-Herxheimer reaction, a common inflammatory response to the
treatment of syphilis. Dexamethasone was administered at a dose of
10 mg/day intravenously for 3 days, followed by gradual tapering
over the subsequent 5 days.
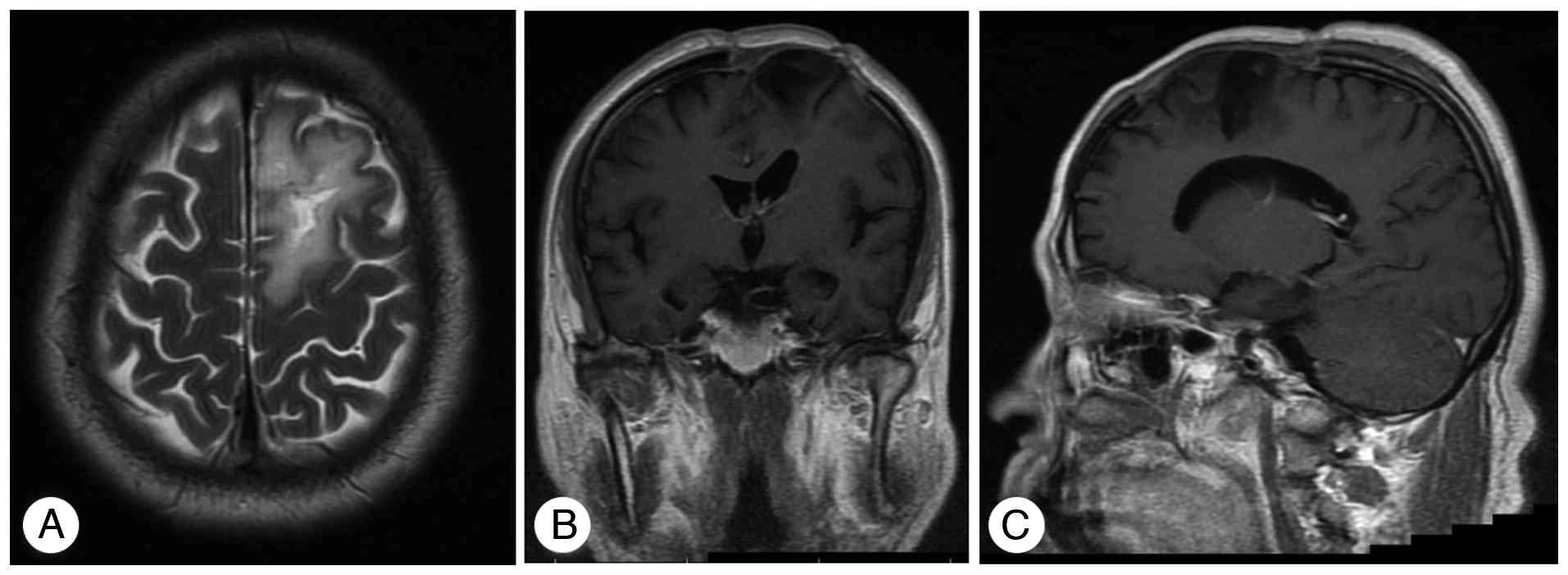
Outcome and follow-up
The patient recovered well from surgery, with
gradual improvement in neurological function. The headaches
resolved and there was marked improvement in speech function and
right-sided hemiparesis. On the seventh postoperative day, the
patient's muscle strength of the right upper and lower limbs
reached grade IV (grade II preoperatively), and speech was clear.
The patient was discharged on oral amoxicillin (500 mg every 8 h)
for an additional 2 weeks. Regular follow-up was arranged with
neurology and infectious disease specialists at 1, 3 and 6 months
after discharge, including neurological examinations, repeat
serological testing for syphilis and follow-up brain MRI to assess
lesion resolution. At the 3-month follow-up, the patient remained
asymptomatic, with no recurrence of neurological symptoms. The
3-month follow-up MRI showed a marked reduction in the size of the
cerebral lesions and surrounding edema, indicating a favorable
prognosis (Fig. 5A-C).
Discussion
NS complications occur in 4-10% of untreated or
inadequately treated patients with syphilis. The neurological
manifestations in advanced NS are diverse (11); early NS often presents without
neurological symptoms and primarily affects the meninges and blood
vessels, whereas late NS can involve the meninges, blood vessels
and brain parenchyma. This progression can lead to conditions such
as meningitis, gummas or cerebral infarctions (12-14).
CSG is a rare clinical manifestation of NS. In a review of 286
reported cases of NS, Drago et al (4) identified only 10 cases of CSG (3.5%).
In a more recent cross-sectional study, the incidence of CSG was
found to be 1.8% among 397 patients with NS (15); however, in both large studies, the
cases of CSG occurred years or even decades after the initial
infection. In the present study, the case is unusual in that the
patient developed a gummatous lesion in the brain within just 6
months of being diagnosed with syphilis, representing an atypical
and rare presentation of this condition in the early stage of the
disease. To the best of our knowledge, this rapid progression is
rarely documented in the literature and it underscores the
variability in the clinical manifestations of syphilis (16,17).
The radiological appearance of syphilitic gummas
frequently mimics other intracranial pathologies. Gliomas,
especially high-grade variants, may present with irregular
enhancement, marked perilesional edema and a mass effect similar to
that observed in gummas. However, gliomas tend to show infiltrative
margins and elevated perfusion metrics, whereas gummas more often
demonstrate well-circumscribed granulomatous enhancement with a
surrounding inflammatory halo.
Reports have suggested that penicillin treatment can
reduce the size of CSG lesions, thereby avoiding the need for
surgery (18,19). However, in the present case, the
condition of the patient deteriorated rapidly, making it
impractical to wait for the time required for penicillin therapy.
Therefore, in the present case, the decision to pursue surgical
intervention was based on the severity of the patient's symptoms
and the need to alleviate the mass effect caused by the gummatous
lesion. Surgical removal of the lesion not only provided
symptomatic relief but also allowed for histopathological
confirmation of the diagnosis, revealing granulomatous inflammation
consistent with syphilitic gummata. Therefore, surgical biopsy
plays a particularly notable role when imaging is inconclusive,
allowing definitive histopathological confirmation and exclusion of
neoplasia. Decompression may also provide symptomatic relief when
rapid deterioration occurs. Nevertheless, once a diagnosis is
established, medical therapy alone is often sufficient and
unnecessary extensive resections should be avoided (20,21).
The present case is noteworthy as it illustrates
that CSG can occur much earlier in the course of syphilis than is
typically expected. It emphasizes the importance of considering NS
and its atypical manifestations, even in patients with a relatively
short history of syphilis. Clinicians should maintain a high degree
of suspicion for NS in patients presenting with new-onset
neurological symptoms, regardless of the duration since syphilis
diagnosis, especially when accompanied by risk factors or
inadequate treatment history.
The occurrence of CSG in early syphilis may reflect
an aggressive host response or a particularly virulent strain of
Treponema pallidum (22).
To the best out our knowledge, the pathophysiology behind the
formation of gummata in such a short time frame is not well
understood. Typically, gummatous lesions result from a chronic
granulomatous inflammatory response to persistent infection. In the
present patient, elevated Treponema pallidum antibody titers
(signal-to-cutoff ratio, 18.84) and cerebrospinal fluid
abnormalities, including increased protein and the positive CSF
TP-PA test, suggested that the immune response in the present
patient might have been unusually robust or dysregulated; this
could be due to genetic predisposition, immune status or other
unknown factors (23). As part of
the present study, a literature review of reported cases of
early-onset syphilitic gummas was conducted, as summarized in
Table II. Among the cases, a
substantial proportion of patients had comorbid conditions
associated with immunosuppression, including diabetes, HIV
infection or concurrent systemic infections, which may have
contributed to the early development of gummatous lesions. Most
lesions involved the frontal or temporal lobes, frequently
presented with focal neurological deficits such as hemiparesis or
speech disturbances, and were generally treated with a combination
of surgical resection and antibiotic therapy. Follow-up data
indicated that most patients achieved favorable neurological
recovery when treated promptly. This detailed overview underscores
the importance of considering underlying immunosuppressive
conditions and lesion location when evaluating early-onset
intracranial syphilitic gummas.
| Table IILiterature review on early-onset
cerebral syphilitic gummata. |
Table II
Literature review on early-onset
cerebral syphilitic gummata.
| First author,
year | Age, years | Sex | Onset time,
months | Lesion location | Past history | Treatment | Outcome | (Refs.) |
|---|
| Sasaki et al,
2019 | 47 | M | 9 | Left frontal and
temporal lobes | Type 2 diabetes | Penicillin G | No neurological
deficits or residual lesions on MRI. | (13) |
| Zhang et al,
2017 | 56 | M | 7 | Left parietal
lobe | - | Operation and
penicillin G | Edema resolved, no
lesion recurrence. | (17) |
| Mu et al,
2024 | 65 | F | 12 | Multiple intracranial
lesions | Liver abscess | Penicillin G | Symptoms resolved,
lesion disappeared | (20) |
| Tsuboi et al,
2016 | 21 | M | 5 | Left frontal
lobe | HIV(+) | Penicillin G | Symptoms improved,
lesion shrunk | (21) |
| Present case | 60 | M | 6 | Left frontal
lobe | - | Operation and
penicillin G | Symptoms improved, no
lesion recurrence | - |
As syphilis rates continue to rise each year, it
becomes increasingly more important to consider CSG, a condition
that is often overlooked and occurs less frequently (24). There is no definitive standard for
diagnosing CSG; although craniocerebral tumors are more common than
syphilis, it is crucial to differentiate patients exhibiting
nervous system symptoms and positive serological test results for
syphilis from those with CSG. Imaging plays a key role in
diagnosing CSG; however, when faced with a rapidly deteriorating
patient, surgical intervention is often the most effective
approach. For patients experiencing severe cerebral edema,
decompressive craniectomy can be a viable option.
In conclusion, the present case highlights an
atypical and rare presentation of CSG occurring just 6 months after
the initial diagnosis of syphilis, challenging the conventional
understanding that such manifestations are predominantly associated
with tertiary syphilis after numerous years of infection.
Clinicians should consider NS in the differential diagnosis of
unexplained neurological symptoms, regardless of the duration of
syphilis, to facilitate a timely and effective intervention.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
YJ, SL and YW analyzed clinical data, obtained
medical images and advised on patient treatment. YZ performed the
pathological diagnosis and contributed to the interpretation of
pathological findings. ZC and BL designed the study and performed
the surgery. ZC and BL confirm the authenticity of all the raw
data. All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
The present case report was prepared in accordance
with the CARE guidelines.
Patient consent for publication
Written informed consent was obtained from the
patient and their family for the publication of the present case
report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ghanem KG, Ram S and Rice PA: The modern
epidemic of syphilis. N Engl J Med. 382:845–854. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Peeling RW, Mabey D, Chen XS and Garcia
PJ: Syphilis. Lancet. 402:336–346. 2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ropper AH: Neurosyphilis. N Engl J Med.
381:1358–1363. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Drago F, Merlo G, Ciccarese G, Agnoletti
AF, Cozzani E, Rebora A and Parodi A: Changes in neurosyphilis
presentation: A survey on 286 patients. J Eur Acad Dermatol
Venereol. 30:1886–1900. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Fargen KM, Alvernia JE, Lin CS and Melgar
M: Cerebral syphilitic gummata: A case presentation and analysis of
156 reported cases. Neurosurgery. 64:568–575, discussioin 575-6.
2009.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cushing H: Further concerning a
parasympathetic center in the interbrain: VII. The effect of
intraventricularly-injected histamine. Proc Natl Acad Sci USA.
18:500–510. 1932.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Grant FC: A study of the results of
surgical treatment in 2,326 consecutive patients with brain tumor.
J Neurosurg. 13:479–488. 1956.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Katsura S, Suzuki J and Wada T: A
statistical study of brain tumors in the neurosurgical clinics in
Japan. J Neurosurg. 16:570–580. 1959.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Barthel L, Hetze S, Teuber-Hanselmann S,
Chapot V and Sure U: Syphilitic gummata in the central nervous
system: A narrative review and case report about a noteworthy
clinical manifestation. Microorganisms. 9(906)2021.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kanayama S, Nagata S, Akiyama Y, Miyazato
Y, Ishikane M, Inoue M, Ohmagari N and Hara T: Cerebral syphilitic
gumma in the modern era: A report of an unusual case and brief
review of recent published reports. Br J Neurosurg. 38:1283–1288.
2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ramrakhiani N, Sukhani PK and Dubey R:
Neurosyphilis-a forgotten disease: Case reports with ten years
follow-up and review of literature. Neurol India. 68:889–893.
2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Baskar D, R Taallapalli AV, Kishore P,
Arshad F, Kulanthaivelu K, Nashi S, Rajendran SP, Kulkarni GB and
Alladi S: A rare case of neurosyphilis presenting as normal
pressure hydrocephalus syndrome. Neurol India. 70:377–379.
2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Sasaki R, Tanaka N, Okazaki T and Yonezawa
T: Multiple cerebral syphilitic gummas mimicking brain tumor in a
non-HIV-infected patient: A case report. J Infect Chemother.
25:208–211. 2019.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Drago F, Ciccarese G and Rebora A:
Treatment of late-stage syphilis. JAMA. 313(969)2015.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Zhang W, Xu D, Qin K, Song C, Miao R, Ma
X, Kou C and Huang Y: Clinical, radiological, and pathological
features of cerebral and spinal syphilitic gumma: A cross-sectional
study. Int J Gen Med. 18:4501–4510. 2025.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Zayet S, Poloni S, Gendrin V, Chanal J,
Dupin N and Klopfenstein T: Early neurosyphilis with serofast
state. Emerg Microbes Infect. 13(2373305)2024.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Zhang L, Zhou Y, Chen J, Yan W, Kong Q,
Chen P and Sang H: A case of a cerebral syphilitic gumma developed
in a few months mimicking a brain tumor in a human immunodeficiency
virus-negative patient. Br J Neurosurg. 31:481–483. 2017.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Forrestel AK, Kovarik CL and Katz KA:
Sexually acquired syphilis: Laboratory diagnosis, management, and
prevention. J Am Acad Dermatol. 82:17–28. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Shen S, Yang R, Wang L, Tang L and Liu B:
Multiple intracranial and spinal cord syphilitic gummas in a human
immunodeficiency virus-negative man with untreated syphilis: A case
report. Medicine (Baltimore). 98(e16887)2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Mu LK, Cheng LF, Ye J, Zhao MY and Wang
JL: Cerebral syphilitic gumma misdiagnosed as brain abscess: A case
report. World J Clin Cases. 12:650–656. 2024.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Tsuboi M, Nishijima T, Teruya K, Kikuchi
Y, Gatanaga H and Oka S: Cerebral syphilitic gumma within 5 months
of syphilis in HIV-infected patient. Emerg Infect Dis.
22:1846–1848. 2016.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Waugh S, Ranasinghe A, Gomez A, Houston S,
Lithgow KV, Eshghi A, Fleetwood J, Conway KME, Reynolds LA and
Cameron CE: Syphilis and the host: Multi-omic analysis of host
cellular responses to treponema pallidum provides novel
insight into syphilis pathogenesis. Front Microbiol.
14(1254342)2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
McVey M, Cameron W and MacPherson P: When
infections collide-gummatous syphilis in an HIV-infected
individual. Int J Infect Dis. (14 Suppl 3):e283–e286.
2010.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Ramchandani MS, Cannon CA and Marra CM:
Syphilis: A modern resurgence. Infect Dis Clin North Am.
37:195–222. 2023.PubMed/NCBI View Article : Google Scholar
|