Introduction
Esophageal varices are a common and life-threatening
complication of portal hypertension in patients with liver
cirrhosis (1). Endovascular
embolization, often in combination with transjugular intrahepatic
portosystemic shunt (TIPS), is a standard therapeutic approach to
reduce variceal bleeding (2,3).
Although generally effective, complications such as ectopic
embolism may occur, occasionally resulting in catastrophic outcomes
including cerebral, renal or mesenteric infarction (4,5); the
underlying anatomical basis for such events has not been fully
elucidated. In patients with cirrhosis, treatment for ectopic
embolism caused by esophageal varices is relatively rare. Within
the literature, to the best of our knowledge, there is only 1 case
of cerebral embolism (6) and 3
cases of spinal cord embolism (7-9),
but the specific cause of embolism is unclear.
To the best of our knowledge, the present case is
the first reported case of angiographically confirmed direct
venous-to-arterial communication causing ectopic embolism.
Traditionally, right-to-left shunting mechanisms-such as pulmonary
arteriovenous malformations or intracardiac defects-have been
implicated (7,10); however, in several cases, including
the present case, such mechanisms are absent (11-14).
Case report
Case presentation
A 57-year-old man with a long-standing history of
hepatitis B virus-related cirrhosis (Child-Pugh class B; model for
end-stage liver disease score 15) (15) was admitted to The Second Affiliated
Hospital of The Third Military Medical University (Chongqing,
China) in June 2023, for recurrent upper gastrointestinal bleeding
and progressive ascites, which was unresponsive to diuretics.
Previous endoscopic therapy with ligation had been performed twice
over the past year, with partial but temporary hemostasis.
On admission, the patient was hemodynamically
stable. Laboratory investigations revealed anemia (hemoglobin, 82
g/l; reference range, 110-160 g/l), thrombocytopenia (platelets,
55x109/l; reference range, 125-350x109/l),
hypoalbuminemia (albumin, 28 g/l; reference range, 35-50 g/l) and
elevated total bilirubin (34 µmol/l; reference range, 3-22 µmol/l).
Imaging using contrast-enhanced abdominal CT showed marked
splenomegaly, large esophageal varices and ascites. After
multidisciplinary discussion, the patient underwent elective TIPS
combined with embolization of esophageal varices.
Imaging and interventions
The TIPS procedure was performed in June 2023, under
local anesthesia via a right internal jugular approach. Puncture of
the left portal vein branch was achieved via the middle hepatic
vein. Splenic venography revealed large, tortuous esophageal
varices. After balloon dilatation of the puncture channel (Cook 7x8
mm), an 8x80 mm GORE VIATORR stent graft was placed.
Embolization of the varices was performed through a
4F Cobra catheter by slow injection of a 1:1 mixture of 2 ml tissue
adhesive (GLUBRAN2) and 2 ml iodized oil under fluoroscopic
control. Pre- and post-TIPS portal pressure gradients were 32 and
17 mmHg, respectively, indicating successful decompression. At ~24
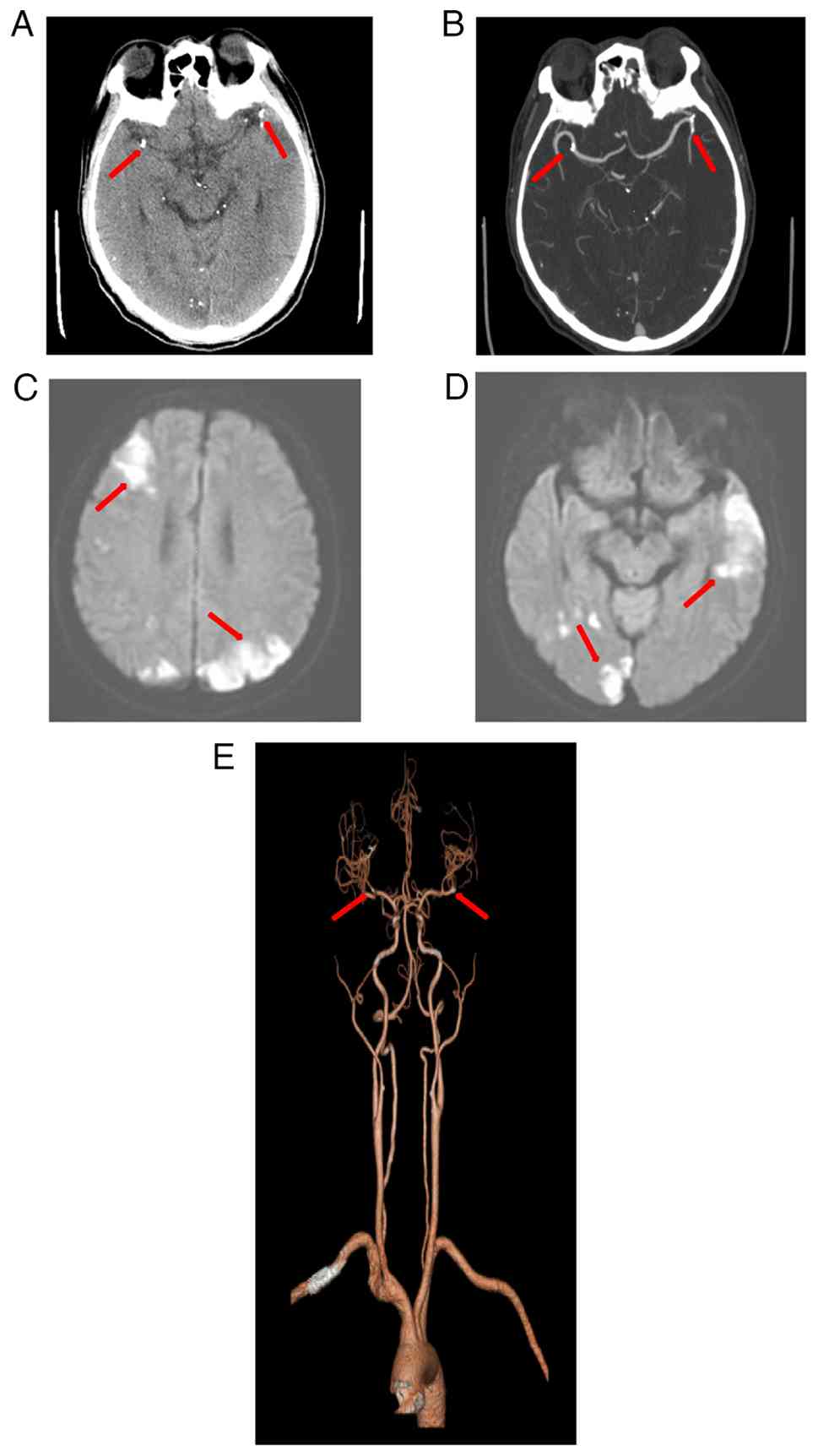
h post-surgery, the patient developed sudden bilateral vision loss
and lower limb weakness (grade III muscle strength bilaterally).
Magnetic resonance angiography showed embolic occlusion of branches
of the middle cerebral artery. Emergent neuroimaging including
non-contrast CT and diffusion-weighted MRI revealed multiple acute
infarctions in the bilateral frontal lobe, parietal lobe, occipital
lobe, temporal lobe, left thalamus and cerebellar hemisphere
(Fig. 1A-E).
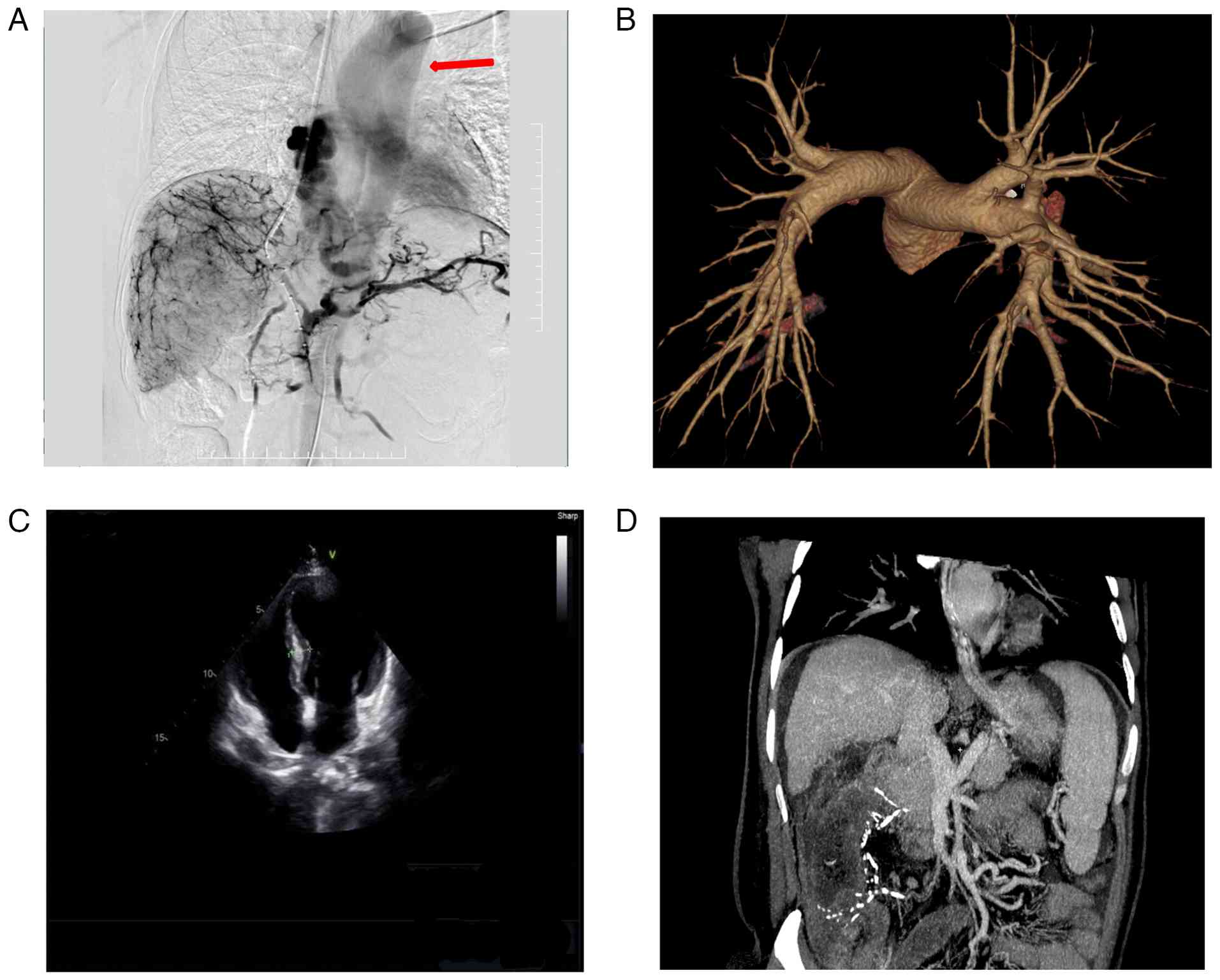
To identify the embolic source, further evaluation
was conducted. Echocardiography excluded patent foramen ovale or
intracardiac thrombus (Fig. 2C).
Additionally, no arteriovenous malformations or pulmonary embolism
was found on pulmonary CT angiography (Fig. 2B).
Notably, retrospective analysis of fluoroscopic
angiography demonstrated direct drainage from the esophageal
variceal plexus to the left atrium and ascending aorta, bypassing
the pulmonary circulation (Fig. 2A
and D and Video S1). This anatomical variant likely
accounted for the cerebral embolism.
Due to the recent hemorrhagic history,
anticoagulation was withheld, and the patient was managed
supportively with neuroprotective agents (0.25 g citicoline once
daily for 5 days). Over 2 weeks, bilateral visual acuity markedly
improved, and motor function partially recovered. At the most
recent follow-up, the patient remained clinically stable with
normal mental status and appetite. He reported no recurrence of
gastrointestinal bleeding (hematemesis or melena), nausea,
vomiting, abdominal pain or ascites.
Discussion
The present case represents a novel mechanism of
ectopic embolism in the setting of esophageal variceal
embolization. To the best of our knowledge, the present case is the
first reported case of angiographically confirmed direct
venous-to-arterial communication causing ectopic embolism.
Traditionally, right-to-left shunting via patent foramen ovale or
pulmonary arteriovenous fistulas has been considered necessary for
systemic embolization following venous embolization procedures
(16-18).
However, in the present case, such conventional shunts were
definitively ruled out.
Instead, angiography revealed a rare and direct
venous drainage route from the esophageal variceal plexus to the
systemic circulation via the left heart, presumably through
pathological dilation of small bronchial or mediastinal collaterals
(19,20). To the best of our knowledge, this
anatomic variant has not been previously described in the
literature, in the context of post-embolization cerebral infarction
(16).
A similar case of spinal cord infarction after
sclerotherapy was reported by Seidman et al (7) in 1984, but no vascular mechanism was
identified. Other studies postulated that the patent foramen ovale
may allow embolic material into the cerebral circulation during
TIPS, but in the absence of identifiable shunts, the mechanism
remained speculative (21-25).
The present case confirms the hypothesis of an alternative, direct
venous-to-arterial conduit.
Due to the difficulty of detecting this vascular
pathway with preoperative routine vascular CT, it is recommended to
extend the display time and fully understand its flow direction in
gastric coronary angiography during TIPS surgery, especially paying
attention to whether the heart and aortic circulatory system are
visible. From the perspective of surgical safety, if direct
esophageal venous to the systemic arterial communication is found
during surgery, it is recommended to avoid using liquid embolic
agents due to their inherent migration risk (26,27).
Solid embolic agents such as coils or embolization are unlikely to
penetrate small caliber blood vessels and may be a safer option,
particularly when imaging suspicion or abnormal communication is
observed prior to embolization (28,29).
In conclusion, the present case highlights a
previously unreported cause of systemic embolization following
esophageal variceal embolization; direct venous communication
between the esophageal variceal plexus and the left heart/ascending
aorta. If the cardiac and aortic circulatory systems are found to
be visualized during gastric coronary angiography during TIPS
surgery, it is recommended to use large-diameter or solid embolic
materials such as coils, which may prevent potentially
life-threatening ectopic embolic events.
Supplementary Material
Dynamic angiography of the present
case. This video demonstrates the direct vascular communication
between the esophageal variceal plexus and the left heart/ascending
aorta during the transjugular intrahepatic portosystemic shunt
procedure, which corresponds to the sequential images shown in
Fig. 2A.
Supplementary data.
Acknowledgements
Not applicable.
Funding
Funding: The authors declare that financial support was received
for the research, authorship and publication of this article. This
study was funded by the General Project of Chongqing Science and
Health Joint Medical Research Project (grant no. 2024MSXM081), the
Science and Technology Research Project of Chongqing Education
Commission (grant no. KJQN202302828), the 2023 Chongqing Nan'an
District Science and Health Union Public Medical Research Project
(grant no. 2023-05), the Open Research Project of the Chongqing Key
Laboratory for Occupational Disease Prevention and Poisoning
Treatment in 2021 (grant no. 2021ZYBKF07), the Chongqing
Pharmaceutical Vocational Education Group General Project (grant
no. CQZJ202352), the General Project of the Incubation Fund within
The First Affiliated Hospital of Chongqing Medical and
pharmaceutical College (grant no. 2022-2023MS02) and the 2023
Chongqing Nan'an District Public Health Key Specialty (Disease
Prevention and Control) Construction Project.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YL and ZX contributed to designing the study and
performed the surgery. YK obtained the medical images. TY advised
on patient treatment and analyzed patient data. ZX and YK confirm
the authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The Ethics Committee of the Second Affiliated
Hospital of the Third Military Medical University (Chongqing,
China) exempted the present study from ethical approval. The
participant provided written informed consent to participate in
this study.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of clinical details and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Zhang CM and Wang X: Suspected
cerebrovascular air embolism during endoscopic esophageal varices
ligation under sedation with fatal outcome: A case report. World J
Clin Cases. 10:371–380. 2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Abuelazm MT, Cheema HA, Jafar U, Awad AK,
Atef M, Abdalshafy H, Alashwah M, Shahid A, Awan RU, Afifi AM, et
al: Transjugular intrahepatic portosystemic shunt with or without
variceal embolization to prevent variceal rebleeding: An updated
meta-analysis. Expert Rev Gastroenterol Hepatol. 17:741–751.
2023.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Betancourt-Torres M, Perez-Torres A,
Figueroa-Diaz L and Labat Alvarez EJ: Iatrogenic cerebral air
embolism during esophago-gastroduodenoscopy. Am J Case Rep.
21(e925046)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Chevallier O, Comby PO, Guillen K,
Pellegrinelli J, Mouillot T, Falvo N, Bardou M, Midulla M,
Aho-Glélé S and Loffroy R: Efficacy, safety and outcomes of
transcatheter arterial embolization with N-butyl cyanoacrylate glue
for non-variceal gastrointestinal bleeding: A systematic review and
meta-analysis. Diagn Interv Imaging. 102:479–487. 2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Davis JPE, Lim JK, Francis FF and Ahn J:
AGA clinical practice update on management of portal vein
thrombosis in patients with cirrhosis: Expert review.
Gastroenterology. 168:396–404.e1. 2025.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wang G, Zhang C and Shi Y: Cerebral
embolism due to portopulmonary venous anastomosis during endoscopic
therapy for gastric varices. Am J Gastroenterol.
114(1833)2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Seidman E, Weber AM, Morin CL, Ethier R,
Lamarche JB, Guerguérian AJ, Geoffroy G and Roy CC: Spinal cord
paralysis following sclerotherapy for esophageal varices.
Hepatology. 4:950–954. 1984.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Mueller D and Gilden DH: Brown-Sequard
syndrome after esophageal sclerotherapy and crack cocaine abuse.
Neurology. 58:1129–1130. 2002.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Heller SL, Meyer JR and Russell EJ: Spinal
cord venous infarction following endoscopic sclerotherapy for
esophageal varices. Neurology. 47:1081–1085. 1996.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Xu SH, Wu F, Guo LH, Zhang WB and Xu HX:
Liver fibrosis index-based nomograms for identifying esophageal
varices in patients with chronic hepatitis B related cirrhosis.
World J Gastroenterol. 26:7204–7221. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
de Sousa CP, Carvalho C, Sousa C and
Amaral R: Treatment of gastric varices with cyanoacrylate
complicated by systemic embolization. Treatment of gastric varices
with cyanoacrylate complicated by systemic embolization. Rev
Gastroenterol Peru. 44:67–70. 2024.PubMed/NCBI
|
|
12
|
Gong T, Tsauo J, Ding M, Jin L, Duan F, Yu
Y and Li X: Transcatheter arterial embolization for cancer-related
non-variceal upper gastrointestinal bleeding: A multicenter
retrospective study of 107 patients. Diagn Interv Imaging.
104:60–66. 2023.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Lee EW, Eghtesad B, Garcia-Tsao G, Haskal
ZJ, Hernandez-Gea V, Jalaeian H, Kalva SP, Mohanty A, Thabut D and
Abraldes JG: AASLD practice guidance on the use of TIPS, variceal
embolization, and retrograde transvenous obliteration in the
management of variceal hemorrhage. Hepatology. 79:224–250.
2024.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Jiang N, Wang WS, Zhu XL and Shen J: Liver
failure after percutaneous transhepatic variceal embolization: A
case report. Asian J Surg. 46:2857–2858. 2023.PubMed/NCBI View Article : Google Scholar
|
|
15
|
D'Amico G, Garcia-Tsao G and Pagliaro L:
Natural history and prognostic indicators of survival in cirrhosis:
A systematic review of 118 studies. J Hepatol. 44:217–231.
2006.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kim JS, Kim BW, Kim DH, Park CH, Lee H,
Joo MK, Jung DH, Chung JW, Choi HS, Baik GH, et al: Guidelines for
non-variceal upper gastrointestinal bleeding. Korean J
Gastroenterol. 75:322–332. 2020.PubMed/NCBI View Article : Google Scholar : (In Korean).
|
|
17
|
Kolb JM and Samarasena JB: EUS-guided
splenic artery embolization for variceal hemorrhage: Balancing
creativity and innovation in Endo-hepatology with caution.
Gastrointest Endosc. 95:184–186. 2022.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Lai HY, Wu KT, Liu Y, Zeng ZF and Zhang B:
Angiography and transcatheter arterial embolization for
non-variceal gastrointestinal bleeding. Scand J Gastroenterol.
55:931–940. 2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Liu B and Li G: Progress in endoscopic and
interventional treatment of esophagogastric variceal bleeding. Dis
Markers. 2022(2940578)2022.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Ohs Z, Jones M, Sharma N and Loveridge K:
Percutaneous transhepatic embolization of ectopic varices in a
patient with portal hypertension presenting with hemorrhagic shock.
Cureus. 13(e18209)2021.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Onishi Y, Shimizu H, Tsunoda S, Obama K
and Nakamoto Y: Direct percutaneous access to a mesenteric vein for
antegrade embolization of esophageal varices: A case report. Radiol
Case Rep. 16:2491–2495. 2021.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Pal A, Blanzy J, Gómez KJR, Preul MC and
Vernon BL: Liquid embolic agents for endovascular embolization: A
review. Gels. 9(378)2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Patidar Y, Chatterjee N, Mukund A and
Sarin SK: Evaluation of clinical outcome and predictors of
mortality in patients undergoing antegrade transvenous variceal
embolization in adjunct to salvage transjugular intrahepatic
portosystemic shunt for active uncontrolled gastric variceal
bleeding. Br J Radiol. 97:1791–1798. 2024.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Sioutas GS, Vivanco-Suarez J, Shekhtman O,
Matache IM, Salem MM, Burkhardt JK, Srinivasan VM and Jankowitz BT:
Liquid embolic agents for middle meningeal artery embolization in
chronic subdural hematoma: Institutional experience with systematic
review and meta-analysis. Interv Neuroradiol.
15(15910199231183132)2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Swaminathan N and Chaudhary S: Oesophageal
variceal-pulmonary venous fistula A rare cause of a right-to-left
shunt. Eur J Case Rep Intern Med. 7(001482)2020.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Vollherbst DF, Chapot R, Bendszus M and
Möhlenbruch MA: Glue, onyx, squid or PHIL? Liquid embolic agents
for the embolization of cerebral arteriovenous malformations and
dural arteriovenous fistulas. Clin Neuroradiol. 32:25–38.
2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Wang DX, Wu XJ, Yu JZ, Zhan JY, Xing FF,
Liu W, Chen JM, Liu P, Liu CH and Mu YP: Visualizing global
progress and challenges in esophagogastric variceal bleeding. World
J Gastrointest Surg. 17(102020)2025.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Wang Z, Zeng Z, Chen L, Shi C, Jin J,
Zhang F, Zhang Q, Mei X and Kong D: Endoscopic
ultrasonography-guided injection of cyanoacrylate in the treatment
of gastroesophageal varices type 1: A single-center randomized
study. Surg Endosc. 37:8277–8284. 2023.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Wong F: Management of refractory ascites.
Clin Mol Hepatol. 29:16–32. 2023.PubMed/NCBI View Article : Google Scholar
|