Introduction
Extramammary Paget disease (EMPD) is a rare
cutaneous adenocarcinoma characterised by predominant
intraepithelial growth of carcinoma cells (1). Primary EMPD originates from skin
appendages, whereas secondary EMPD represents intraepithelial
involvement by an underlying adenocarcinoma, most commonly
originating from the lower gastrointestinal or urinary tract
(1). The most common sites of
primary EMPD include the vulva, perianal region, scrotum, and penis
(1,2). The characteristic histopathological
features of this rare carcinoma include intraepithelial
proliferation of neoplastic cells with abundant amphophilic
cytoplasm, mucin, and vesicular nuclei with prominent nucleoli,
known as Paget cells. These cells appear as solitary cells, solid
nests, or occasionally glandular structures, and may involve hair
follicles and eccrine ducts (1).
The origin of primary EMPD remains controversial, as this
adenocarcinoma is hypothesised to arise from pluripotent
germinative cells within the epidermis or skin adnexa.
Alternatively, Toker cells, mammary gland-related intraepithelial
cells present in the epithelium of the normal external genital
region, have been proposed as a potential cell of origin (3-5).
The hallmark immunohistochemical characteristic of
primary EMPD is positive immunoreactivity for MUC5AC (6-10),
a gastric-type mucin core protein (10,11).
MUC5AC is expressed in normal mucous cells of the surface foveolar
epithelium of the stomach but not in the pyloric and fundic glands
(11,12). MUC5AC expression has been reported
in several types of carcinomas, including gastric, lung, and
pancreatobiliary carcinomas (11).
Its expression has also been described in non-digestive system
carcinomas, such as primary EMPD and endocervical adenocarcinoma
(6-10,13).
However, whether MUC5AC expression correlates with the invasiveness
of EMPD remains controversial. Two studies reported higher MUC5AC
expression in in situ lesions than in invasive lesions
(6,9), whereas another study demonstrated
higher MUC5AC expression in invasive lesions compared with in
situ lesions (7).
Recently, several gastric-type markers have been
utilised in pathological diagnosis through immunohistochemical
analysis and explored for targeted therapeutic applications.
Claudin 18 is a member of the claudin family and a major component
of tight junction complexes (14).
Its expression is restricted to non-neoplastic gastric mucosa and
alveolar epithelial cells (14)
and is frequently observed in gastric carcinoma, oesophageal and
pancreatobiliary tract adenocarcinomas, as well as mucinous
carcinomas of the female genital tract (15-18).
Accordingly, analysis of this tight junction protein may aid in
identifying the primary origin of metastatic carcinoma (17). Moreover, claudin 18 has recently
attracted attention as a promising therapeutic target in claudin
18-expressing malignant tumours (15,16).
Zolbetuximab, a monoclonal antibody targeting claudin 18.2, a
gastric mucosa-specific isoform, has been shown to improve survival
in patients with claudin 18.2-positive advanced gastric cancer
(15). In addition, hepatocyte
nuclear factor 4α (HNF4α) is a nuclear transcription factor
involved in liver and kidney development and intestinal functions;
accordingly, its expression is observed in normal liver, kidney,
stomach, and intestinal tissues (19,20).
Although HNF4α is not a specific gastric-type marker, it has been
shown to induce MUC5AC expression in the normal stomach (21), and most gastric adenocarcinomas
demonstrate positive immunoreactivity for this marker (22). To date, the expression profiles of
claudin 18 and HNF4α in primary EMPD have not been fully
investigated. Therefore, the present study aimed to examine the
expression profiles of MUC5AC, claudin 18, and HNF4α in EMPD, as
well as the differences in MUC5AC expression between in situ
and invasive lesions.
Materials and methods
Patient selection
Consecutive patients with primary EMPD who underwent
surgical resection at Osaka Medical and Pharmaceutical University
Hospital between January 2016 and December 2024 were included.
Patients who underwent biopsy without subsequent surgical resection
were excluded.
This retrospective, single-institution study was
conducted in accordance with the tenets of the Declaration of
Helsinki, and the study protocol was approved by the Institutional
Review Board of Osaka Medical and Pharmaceutical University
Hospital (Approval No.: #2025-030). All data were anonymised.
Informed consent was obtained using the opt-out method because of
the retrospective study design, in which medical records and
archived samples were used and posed no risk to participants. In
addition, the present study did not include minors. Information
regarding the study, including the inclusion criteria and the
opportunity to opt out, was provided on the institutional website
(https://www.ompu.ac.jp/u-deps/path/img/file36.pdf).
Histopathological analysis
Surgically resected specimens were fixed in 10%
neutral buffered formalin, sectioned, and stained with haematoxylin
and eosin. Two researchers (NK and MI) independently evaluated the
histopathological features of the slides. When invasive neoplastic
growth was identified (defined as the growth of carcinoma cells
over the basement membrane of the epidermis or skin appendages into
the dermis), the tumours were classified as invasive EMPD,
regardless of the depth of tumour invasion.
Immunohistochemical analysis
Immunohistochemical analysis was performed using an
automated immunostainer (Discovery Ultra System; Roche
Diagnostics), according to the manufacturer's instructions. The
OptiView DAB Universal Kit (cat. no. 518-111427; Roche Diagnostics)
was used for immunostaining. The primary antibodies used in the
present study were mouse monoclonal antibody against claudin 18
(43-14A; Abcam, Cambridge, UK, diluted 1:8,000), rabbit monoclonal
antibody against HNF4α (C11F12; Cell Signaling Technology, Danvers,
MA, USA, diluted 1:200), and mouse monoclonal antibody against
MUC5AC (45M1; Thermo Fisher Scientific Inc., MA, USA, diluted
1:4,000). Non-neoplastic gastric and colon mucosae and skin tissues
were concurrently stained as the positive and negative controls,
respectively, for these three markers.
Expression of these markers was assessed
semi-quantitatively as follows: 0, <5%; 1, 5-25%; 2, 26-50%; 3,
>50% of positive neoplastic cells, using the same method as in a
previous study (7).
Immunohistochemical expression in in situ and invasive
lesions (when present) was evaluated separately.
Two researchers (NK and MI) independently evaluated
the immunohistochemical findings. In cases of discrepancy, a final
consensus was reached through reassessment using a multi-headed
microscope.
Statistical analysis
Differences between the two groups were analysed
using the Mann-Whitney U test or the Wilcoxon signed-rank
test. Statistical significance was set at P<0.05.
Results
Patient characteristics
This study included 40 patients with EMPD,
comprising nine women (22.5%) and 31 men (77.5%). The median age at
the time of surgery was 74 (range: 45-89) years. Tumour locations
were as follows: scrotum (26 patients), external genitalia (10
patients), penis (2 patients), and anus and vulva (1 patient each).
Lymph node dissection was performed in seven patients. No follow-up
analysis including recurrence was performed in the present
study.
Histopathological characteristics
This cohort included 25 in situ and 15
invasive EMPD cases. In all invasive EMPD cases, in situ
lesions were present overlying and/or surrounding the invasive
components. Typical histopathological features of in situ
and invasive EMPD are shown in Fig.
1A and B. Lymph node
metastasis was identified in two patients with invasive EMPD; among
the seven patients who underwent lymph node dissection, five had
only in situ lesions, and no metastasis was observed in
these cases.
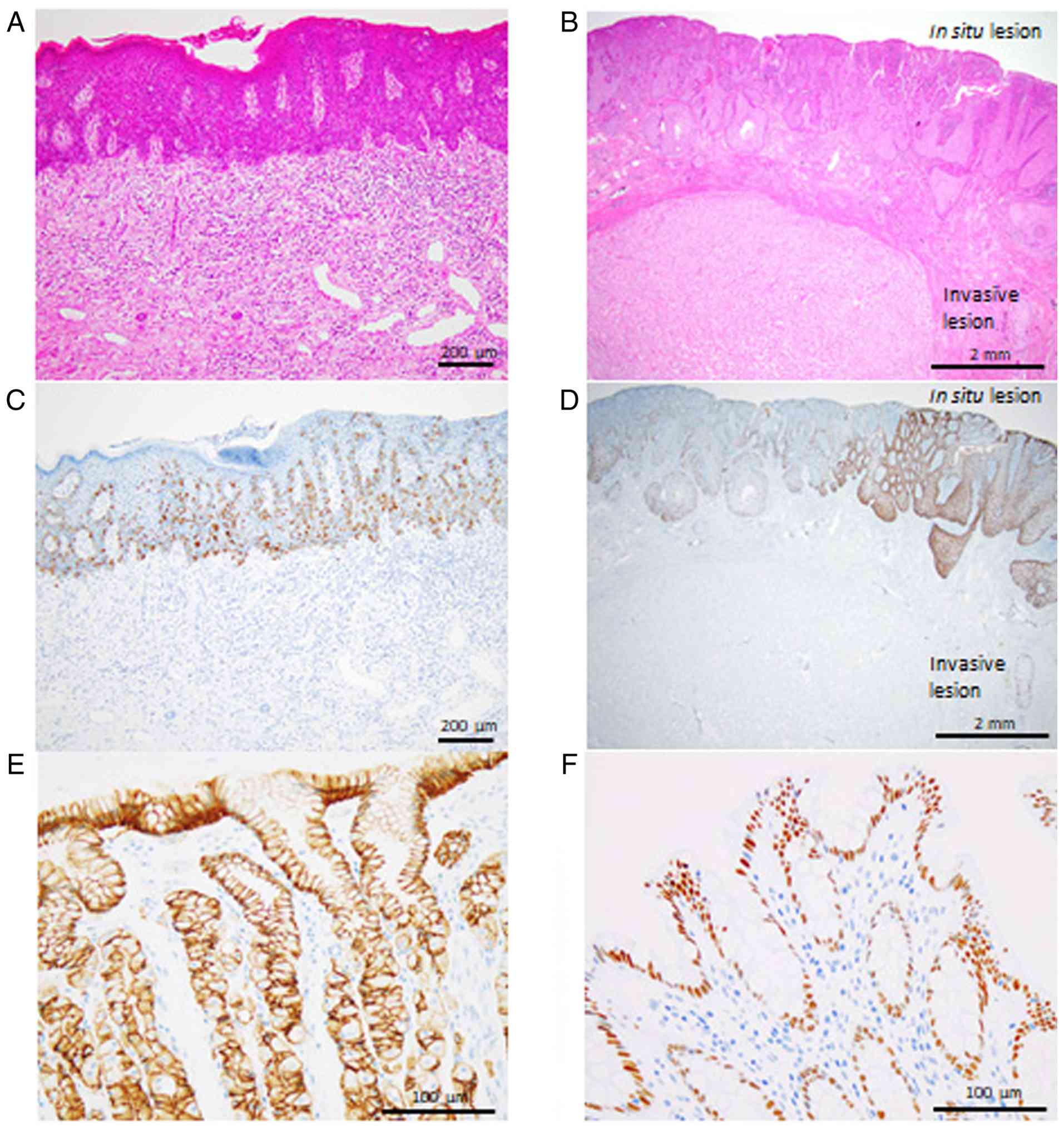 | Figure 1Histopathological and
immunohistochemical features of primary EMPD. (A) Typical
histopathological features of in situ EMPD, showing
intraepidermal proliferation of the neoplastic cells with slightly
eosinophilic cytoplasm, predominantly in a single-cell pattern
(haematoxylin and eosin staining; original magnification, x200).
(B) Typical histopathological features of invasive EMPD.
Intraepidermal proliferation (in situ lesion) and invasive
neoplastic growth into the dermis (invasive lesion) are present
(haematoxylin and eosin staining; original magnification, x20). (C)
Immunohistochemical staining for MUC5AC showing cytoplasmic
positive immunoreactivity in the neoplastic cells of the in
situ lesion (original magnification, x200). (D)
Immunohistochemical staining for MUC5AC showing positive
immunoreactivity in the in situ lesion, but not in the
invasive lesion (original magnification, x20). (E)
Immunohistochemical staining for claudin 18 as a positive control.
Membranous positivity is noted in the non-neoplastic gastric
epithelial cells (original magnification, x400). (F) Immunostaining
for hepatocyte nuclear factor 4α as a positive control. Nuclear
positivity is noted in the non-neoplastic colon epithelial cells
(original magnification, x400). EMPD, extramammary Paget
disease. |
Immunohistochemical
characteristics
Table I summarises
the expression scores of MUC5AC in both in situ and invasive
EMPD. MUC5AC expression was observed in 23 in situ and 15
invasive EMPD cases, whereas no MUC5AC expression was observed in
one in situ case and one invasive case. Representative
immunohistochemical features of in situ and invasive EMPD
are shown in Fig. 1C and D.
 | Table IImmunohistochemical staining results
of patients with primary EMPD. |
Table I
Immunohistochemical staining results
of patients with primary EMPD.
| A, EMPD |
|---|
| | MUC5AC expression
score |
|---|
| Group | 0, n | 1, n | 2, n | 3, n |
|---|
| In situ
EMPD | 1 | 4 | 5 | 15 |
| Invasive EMPD | 1 | 4 | 3 | 7 |
| B, Invasive EMPD |
| In situ
lesions | 1 | 4 | 3 | 7 |
| Invasive
lesions | 11 | 3 | 1 | 0 |
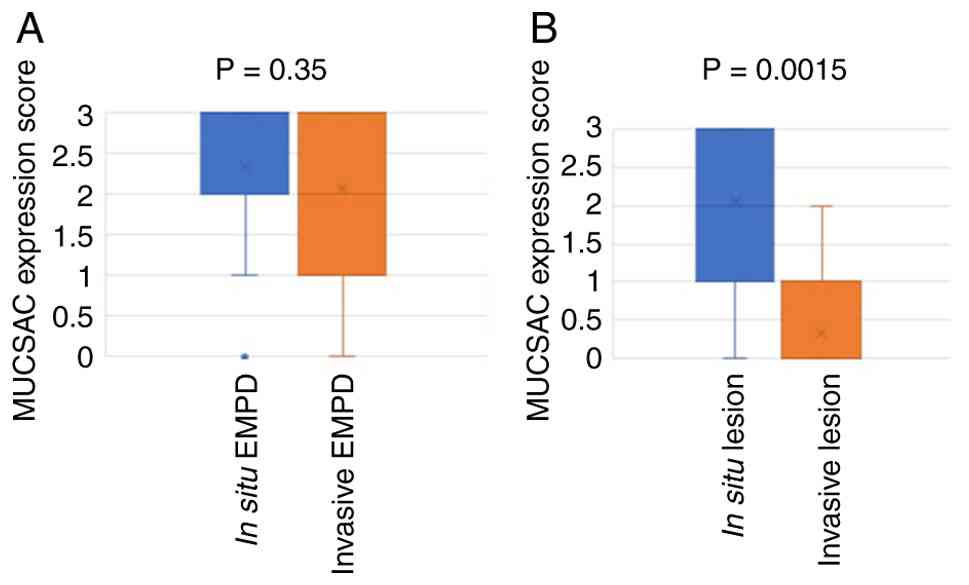
There was no significant difference between the
MUC5AC expression scores of in situ lesions in patients with
in situ-only and invasive EMPD, as the mean expression score
was 2.36 (range, 0-3) in patients with in situ EMPD and 2.07
(range, 0-3) in those with invasive EMPD (P=0.35) (Fig. 2A).
In patients with invasive EMPD, MUC5AC expression
scores in the invasive EMPD lesions were significantly lower than
those in the corresponding in situ lesions, with mean
expression scores of 2.07 (range, 0-3) for in situ lesions
and 0.33 (range, 0-2) for invasive lesions (P=0.0015) (Fig. 2B).
Moreover, MUC5AC expression scores in lymph node
metastasis were 0 in both patients. Neither HNF4α nor claudin 18
expression was observed in any in situ or invasive EMPD
lesions. Notably, claudin 18 and HNF4α positivity were observed in
the non-neoplastic gastric and colon mucosae used as positive
control (Fig. 1E and F).
Discussion
This study clearly demonstrated that MUC5AC
expression scores were significantly lower in invasive lesions than
in the corresponding in situ lesions of invasive EMPD, and
that MUC5AC expression in in situ lesions did not differ
significantly between in situ-only and invasive EMPD.
Moreover, the present study is the first to demonstrate the absence
of immunohistochemical expression of HNF4α and claudin 18 in
primary EMPD.
It is well recognised that MUC5AC expression is
present in primary EMPD, with reported positive expression rates
ranging from 42.1 to 89% (6-10).
The findings of the present study are consistent with previous
reports (6-10),
as 95% (38 of 40) of primary EMPD cases showed positive
immunoreactivity for MUC5AC. In normal gastric mucosa, MUC5AC
expression is induced by HNF4α (21), and most gastric adenocarcinomas
also demonstrate positive immunoreactivity for this transcription
factor (22). Although MUC5AC
expression is observed in normal endocervical glandular cells and
respiratory epithelium (13,23),
HNF4α expression is not detected in these normal epithelial tissues
(24). These findings suggest that
the mechanisms regulating MUC5AC expression may differ among
organs. In the present study, no immunohistochemical expression of
HNF4α was detected in primary EMPD, including both in situ
and invasive tumours. Further studies are required to elucidate the
hitherto unknown molecular mechanisms underlying MUC5AC expression
in patients with primary EMPD.
The expression profiles of MUC5AC in in situ
and invasive lesions of primary EMPD remain controversial. Table II summarises the expression
profiles of MUC5AC in invasive EMPD reported in previous studies,
as well as in the present study (6,7,9).
Three of four studies, including the present one, demonstrated that
MUC5AC expression was significantly lower in invasive lesions than
in situ lesions, although the methods used to evaluate
MUC5AC expression differed among these studies. Specifically, the
cut-off value for positivity was set at 5% of carcinoma cells in
three studies including the present one (6,7),
whereas the tumour was considered to be positive for MUC5AC
expression when more than one MUC5AC-positive cell was present in
one study (9). Moreover,
expression scores were evaluated separately for in situ and
invasive lesions in two studies, including the present study
(9); however, the methods for
evaluating MUC5AC expression scores in invasive EMPD were not fully
described (whether only invasive lesions or both in situ and
invasive lesions were evaluated) in the remaining two studies
(6,7). The present study represents the
second-largest cohort of both total and invasive EMPD cases
(Table II) (6,7,9) and
included a statistical comparison of MUC5AC expression scores
between in situ and invasive lesions. Accordingly, MUC5AC
expression may be decreased in invasive EMPD lesions, although
further analyses in larger cohorts are required to clarify the
expression profiles of MUC5AC in EMPD. In the present cohort, both
lymph node metastases showed loss of MUC5AC expression implying
that metastatic EMPD cells might lack MUC5AC expression; however,
this preliminary observation was seen in only two patients.
Finally, the molecular mechanisms underlying these changes remain
unresolved, and it is still unclear whether these changes are the
cause or the effects of invasion. Therefore, further studies are
required to elucidate the mechanisms responsible for altered MUC5AC
expression in invasive EMPD.
| Table IIExpression profiles of MUC5AC in
invasive EMPD. |
Table II
Expression profiles of MUC5AC in
invasive EMPD.
| | MUC5AC-positive, n
(%) | |
|---|
| First author/s,
year | In situ
EMPD | Invasive EMPD | (Refs.) |
|---|
| Rao et al,
2022 | 64/72 (88.9) | 23/46 (50.0) | (6) |
| Hata et al,
2014 | 12/28 (42.9) | 9/11 (81.8) | (7) |
| Yoshii et
al, 2002 | 23/23 (100.0) | 11/13 (84.6) | (9) |
| Present study | 24/25 (96.0) | 4/15 (26.7) | - |
Claudin 18 is a major component of tight junction
proteins and plays an important role in epithelial barrier function
and cellular polarity (14). Its
expression is restricted to non-neoplastic gastric mucosa and
alveolar epithelial cells of the lung (14). Claudin 18 has two splice variants,
among which claudin 18.2 is a gastric mucosa-specific isoform
(14). Recent advances in
molecular-targeted therapy have demonstrated that zolbetuximab, a
monoclonal antibody against claudin 18.2, significantly improves
survival in patients with claudin 18.2-positive advanced gastric
cancer (15). In addition,
positive immunoreactivity for claudin 18 has been reported in
pancreatobiliary tract adenocarcinomas and mucinous carcinomas of
the female genital tract (15-18),
suggesting that patients with these malignancies may be candidates
for molecular-targeted therapy. However, the present study
demonstrated a lack of claudin 18 expression in all primary EMPD
cases examined. Accordingly, patients with primary EMPD are
unlikely to benefit from anti-claudin 18-targeted therapy.
Moreover, a monoclonal antibody against claudin 18 (clone 43-14A)
was used for immunohistochemical detection in the present study.
This antibody reacts with both claudin 18.1 and 18.2. Although the
specific antibody against claudin 18.2 might have helped retrieve
more information regarding expression of gastric-type marker in
EMPD, we used this claudin 18 antibody clone because it was used
for detecting claudin 18 expression in cancer tissues in a clinical
trial that demonstrated the significant survival benefits of
zolbetuximab in patients with claudin 18-positive gastric cancer
(25) and is used as a companion
diagnostics tool.
The present study had a few limitations. First,
although this is the second-largest cohort of EMPD to be studied so
far, it included a relatively small number of patients with EMPD
(25 in situ and 15 invasive EMPD). As this study was a pilot
study, further study with a larger cohort is required to overcome
statistical bias. Moreover, the relationship between MUC5AC
expression status and survival was not analysed, because this
cohort included only two patients with metastatic EMPD. Second, the
methods used to evaluate MUC5AC expression profiles differed among
studies, as mentioned earlier, resulting in bias. Further analysis
using standardized methods for evaluation of MUC5AC expression in a
larger cohort is required. Third, the present study demonstrated
that MUC5AC expression in EMPD was not correlated with HNF4α
expression. Although different mechanisms of MUC5AC expression may
be present, molecular analysis was not performed in the present
study. Thus, further molecular study is needed to clarify the
mechanism underlying MUC5AC expression in EMPD.
In conclusion, the present study demonstrated that
MUC5AC expression was significantly lower in invasive lesions than
in in situ lesions of invasive EMPD; however, MUC5AC
expression in in situ lesions did not differ significantly
between in situ-only and invasive EMPD. Although HNF4α
induces MUC5AC expression in normal gastric mucosa, HNF4α
expression was not detected in primary EMPD. Therefore, the
molecular mechanisms underlying MUC5AC expression in primary EMPD
warrant further investigation.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
NK and MI conceived and designed the present study.
NK and MI analysed histological and immunohistochemical staining.
NK and MI confirm the authenticity of all the raw data. NK, MI, SO
and YH analysed the data. NK and MI performed the statistical
analyses. NK and MI wrote the manuscript and prepared figures and
tables. All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present retrospective, single-institution study
was conducted in accordance with the tenets of The Declaration of
Helsinki, and the study protocol was approved by the Institutional
Review Board of Osaka Medical and Pharmaceutical University
Hospital (approval no. 2025-030; Takatsuki, Japan). All data were
anonymised. Informed consent was obtained from the patients using
the opt-out methodology because of the retrospective study design,
in which medical records and archived samples were used. The
present study did not include minors.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Prieto VG, Kazakov DV, Konstantinova AM,
McCluggage WG and Michal M: Extramammary Paget disease. In: WHO
classification of tumours, Skin Tumours. 5th edition. IARC, Lyon,
pp313-314, 2025.
|
|
2
|
Ishizuki S and Nakamura Y: Extramammary
Paget's disease: Diagnosis, pathogenesis, and treatment with focus
on recent developments. Curr Oncol. 28:2969–2986. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Shah RR, Shah K, Wilson BN, Tchack M,
Busam KJ, Moy A, Leitao MM, Cordova M, Neumann NM, Smogorzewski J,
et al: Extramammary Paget disease. Part I. Epidemiology,
pathogenesis, clinical features, and diagnosis. J Am Acad Dermatol.
91:409–418. 2024.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Simonds RM, Segal RJ and Sharma A:
Extramammary Paget's disease: A review of the literature. Int J
Dermatol. 58:871–879. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Belousova IE, Kazakov DV, Michal M and
Suster S: Vulvar toker cells: the long-awaited missing link: A
proposal for an origin-based histogenetic classification of
extramammary Paget disease. Am J Dermpathol. 28:84–86.
2006.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Rao Y, Zhu J, Zheng H, Ren Y and Ji T:
Cell origin and genome profile difference of penoscrotum invasive
extramammary Paget disease compared with its in situ counterpart.
Front Oncol. 12(972047)2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Hata H, Abe R, Hoshina D, Saito N, Homma
E, Aoyagi S and Shimizu H: MUC5AC expression correlates with
invasiveness and progression of extramammary Paget's disease. J Eur
Acad Dermatol Venereol. 28:727–732. 2014.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Liegl B, Leibl S, Gogg-Kamerer M, Tessaro
B, Horn LC and Moinfar F: Mammary and extramammary Paget's disease:
An immunohistochemical study of 83 cases. Histopathology.
50:439–447. 2007.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Yoshii N, Kitajima S, Yonezawa S,
Matsukita S, Setoyama M and Kanzaki T: Expression of mucin core
proteins in extramammary Paget's disease. Pathol Int. 52:390–399.
2002.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Kuan SF, Montag AG, Hart J, Krausz T and
Recant W: Differential expression of mucin genes in mammary and
extramammary Paget's disease. Am J Surg Pathol. 25:1469–1477.
2001.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Krishn SR, Ganguly K, Kaur S and Batra SK:
Ramifications of secreted mucin MUC5AC in malignant journey: a
holistic view. Carcinogenesis. 39:633–651. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Johansson MEV, Sjövall H and Hansson GC:
The gastrointestinal mucus system in health and disease. Nat Rev
Gastroenterol Hepatol. 10:352–361. 2013.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Riethdorf L, O'Connell JT, Riethdorf S,
Cviko A and Crum CP: Differential expression of MUC2 and MUC5AC in
benign and malignant glandular lesions of the cervix uteri.
Virchows Arch. 437:365–371. 2000.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Niimi T, Nagashima K, Ward JM, Minoo P,
Zimonjic DB, Popescu NC and Kimura S: Claudin-18, a novel
downstream target gene for the T/EBP/NKX2.1 homeodomain
transcription factor, encodes lung- and stomach-specific isoforms
through alternative splicing. Mol Cell Biol. 21:7380–7390.
2001.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Nakayama I, Qi C, Chen Y, Nakamura Y, Shen
L and Shitara K: Claudin 18.2 as a novel therapeutic target. Nat
Rev Clin Oncol. 21:354–369. 2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Hashimoto T, Iida N, Nakamura Y, Nonomura
N, Morizane C, Iwata H, Okano S, Yamagami W, Yamazaki N, Kadowaki
S, et al: Landscape analysis of CLDN18 expression and isoform
distribution in solid tumors: Insights from MONSTAR-SCREEN-2 study.
Cancer Sci. 116:2218–2231. 2025.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Li WT, Jeng YM and Yang CY: Claudin-18 as
a marker for identifying the stomach and pancreatobiliary tract as
the primary sites of metastatic adenocarcinoma. Am J Surg Pathol.
44:1643–1648. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Kiyokawa T, Hoang L, Pesci A,
Alvarado-Cabrero I, Oliva E, Park KJ, Soslow RA and Stolnicu S:
Claudin-18 as a promising surrogate marker for endocervical
gastric-type carcinoma. Am J Surg Pathol. 46:628–636.
2022.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Sladek FM, Zhong WM, Lai E and Darnell JE
Jr: Liver-enriched transcription factor HNF-4 is a novel member of
the steroid hormone receptor superfamily. Genes Dev. 4:2353–2365.
1990.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Qu N, Luan T, Liu N, Kong C, Xu L, Yu H,
Kang Y and Han Y: Hepatocyte nuclear factor 4 a (HNF4α): A
perspective in cancer. Biomed Pharmacother.
169(115923)2023.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jonckheere N, Vincent A, Franquet-Ansart
H, Witte-Bouma J, Korteland-van Male A, Leteurtre E, Renes IB and
van Seuningen I: GATA-4/-6 and HNF-1/-4 families of transcription
factors control the transcriptional regulation of the murine Muc5ac
mucin during stomach development and in epithelial cancer cells.
Biochim Biophys Acta. 1819:869–876. 2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
van der Post RS, Bult P, Vogelaar IP,
Ligtenberg MJL, Hoogerbrugge N and van Krieken JH: HNF4A
immunohistochemistry facilitates distinction between primary and
metastatic breast and gastric carcinoma. Virchows Arch.
464:673–679. 2014.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Okuda K, Chen G, Subramani DB, Wolf M,
Gilmore RC, Kato T, Radicioni G, Kesimer M, Chua M, Dang H, et al:
Localization of secretory mucins MUC5AC and MUC5B in normal/healthy
human airways. Am J Respir Crit Care Med. 199:715–727.
2019.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tanaka T, Jiang S, Hotta H, Takano K,
Iwanari H, Sumi K, Daigo K, Ohashi R, Sugai M, Ikegame C, et al:
Dysregulated expression of P1 and P2 promoter-driven hepatocyte
nuclear factor-4alpha in the pathogenesis of human cancer. J
Pathol. 208:662–672. 2006.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Shitara K, Lordick F, Bang YJ, Enzinger P,
Ilson D, Shah MA, Van Cutsem E, Xu RH, Aprile G, Xu J, et al:
Zolbetuximab plus mFOLFOX6 in patients with CLDN18.2-positive,
HER2-negative, untreated, locally advanced unresectable or
metastatic gastric or gastro-oesophageal junction adenocarcinoma
(SPOTLIGHT): A multicentre, randomised, double-blind, phase 3
trial. Lancet. 401:1655–1668. 2023.PubMed/NCBI View Article : Google Scholar
|