Introduction
Cervical cancer is the fourth most common cancer in
women globally, with ~660,000 new cases and ~350,000 associated
deaths in 2022. Following the lung and liver, bone is the
third-most common site of distant metastasis (1). The incidence of clinical bone
metastasis in cervical cancer is 0.8-23.0% (2). Bone metastasis most frequently occurs
in the axial skeleton, with the lumbar spine being the most common
(36.4%), followed by the thoracic spine and the pelvis, while
metastases to the femur, humerus and fibula are relatively rare
(3). Unlike patients with
early-stage or locally advanced cervical cancer who can be
effectively treated with conventional therapies such as surgery,
chemotherapy or radiotherapy, there is currently no standard
treatment for patients with metastatic cervical cancer due to its
heterogeneous manifestation (2).
For bone metastasis, surgery should be considered. However, since
most patients with bone metastasis die within 1 year, treatment
should not only aim to improve quality of life and relieve pain but
also prolong survival (4).
In recent years, the application of 3D-printed
prostheses in orthopedic oncology has become increasingly
widespread (5,6). These prostheses provide
patient-specific implants that precisely match the morphology of
bone defects, promote osseointegration through porous trabecular
structures and improve surgical accuracy in complex limb-salvage
procedures (6,7). These advantages are particularly
valuable in cases involving extensive bone defect, tumor recurrence
and periprosthetic infection, where conventional implants typically
fail to meet the demands of such complex cases (5,6).
The present study reports a rare case of recurrent
cervical cancer with femoral metastasis complicated by
periprosthetic infection.
Case report
Patient history and preoperative
preparation
A 53-year-old female patient underwent a total
hysterectomy due to cervical cancer 4 years before at an external
hospital. In June 2024, the patient presented to the Department of
Orthopaedics, Yunnan Cancer Hospital, The Third Affiliated Hospital
of Kunming Medical University (Kunming, China) with pain in the
left thigh and limited mobility. A total of 2 years later, tumor
recurrence with metastasis to the left femur led to left hip
arthroplasty The patient was admitted in June 2024, with pain in
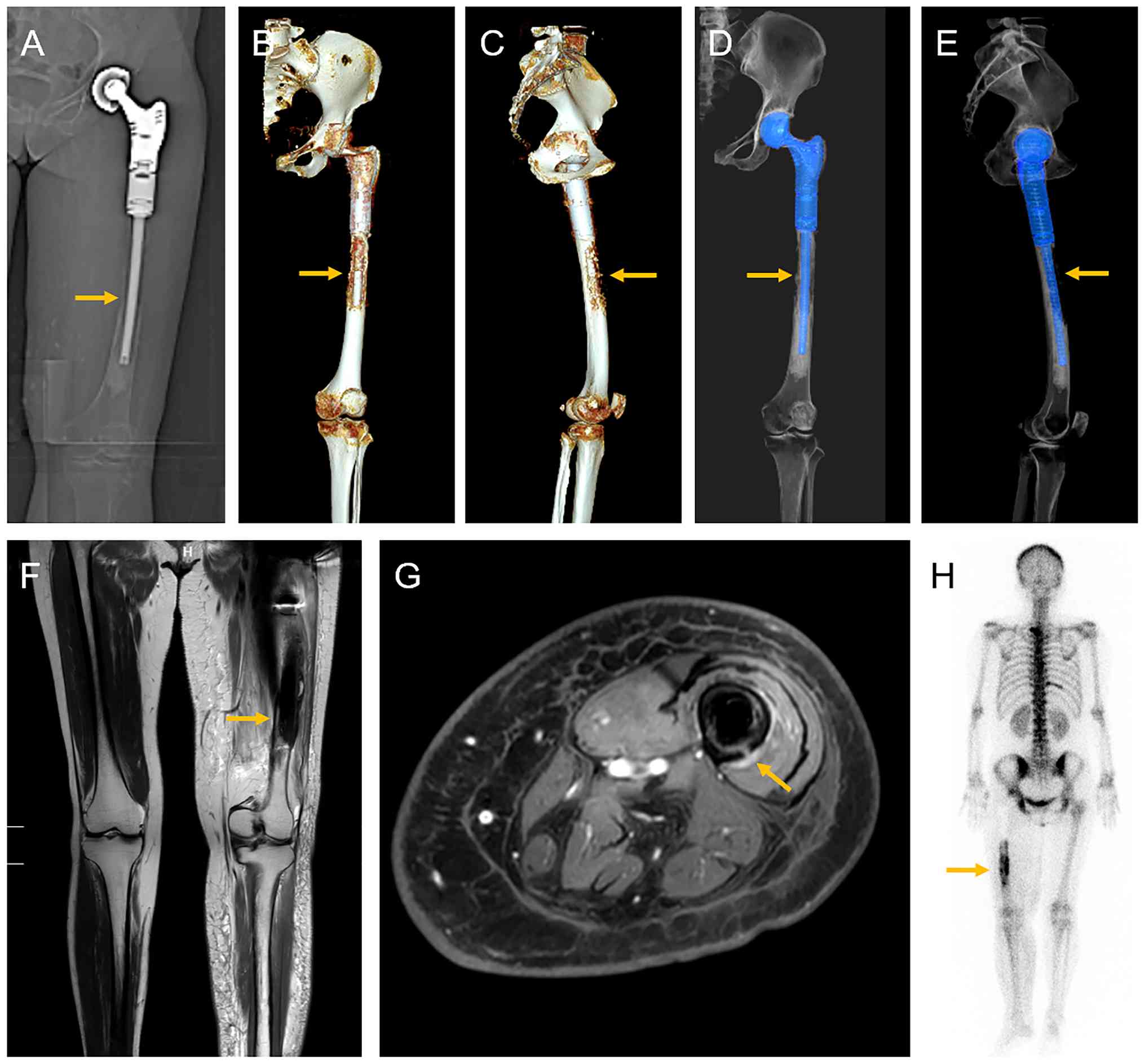
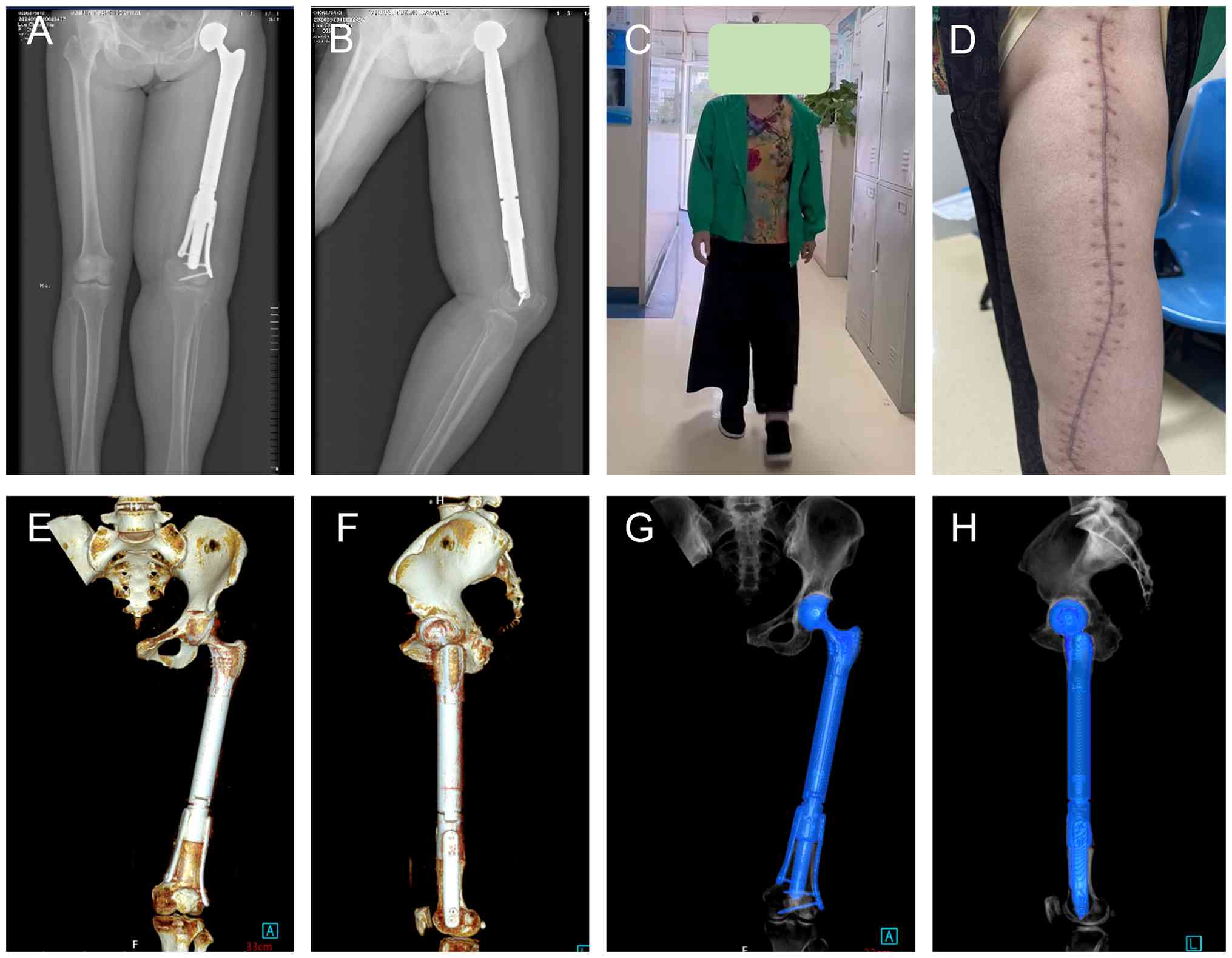
the left thigh and limited mobility. Imaging examination (plain
radiography: 60 kV, 10 mAsec; contrast-enhanced MRI: 3.0 T, Siemens
Magnetom Skyra, slice thickness 4 mm) revealed bone destruction in
the distal left femur, suggesting tumor recurrence, and the
swelling of the left thigh was considered to be due to lymphatic
atresia resulting from postoperative radiotherapy for cervical
cancer (Fig. 1). Whole-body single
photon emission computed tomography bone scans revealed multiple
areas of abnormal increased bone metabolism throughout the skeletal
system, including a solitary lesion in the left femur. Preoperative
serum tumor markers, namely, cancer antigen (CA)72-4 (13.30 U/ml;
normal range, <6.9 U/ml), carcinoembryonic antigen (804.0 ng/ml;
normal range, <5.0 ng/ml for smokers, <2.5 ng/ml for
non-smokers), neuron-specific enolase (22.20 ng/ml; normal range,
<16.3 ng/ml), squamous cell carcinoma antigen (2.20 µg/l; normal
range, <1.5 µg/l), cancer CA-125 (35.3 U/ml; normal range,
<35 U/ml) and CA19-9 (44.9 U/ml; normal range, <37 U/ml),
were elevated. Preoperative hematological examination on the first
day of admission showed: White blood cell count (WBC),
4.89x109/l (normal range, 4.0-10.0x109/l);
C-reactive protein, 5.31 mg/l (normal range, <5.0 mg/l); and
erythrocyte sedimentation rate, 88 mm/h (normal range, 0-20 mm/h
for women). Postoperative body temperature was normal, with no
other sign of preoperative infection. Considering the patient
history of cervical cancer, absence of other recorded tumor-related
medical history and imaging findings demonstrating typical features
of bone destruction, the preliminary diagnosis was metastatic
cervical cancer to the left distal femur.
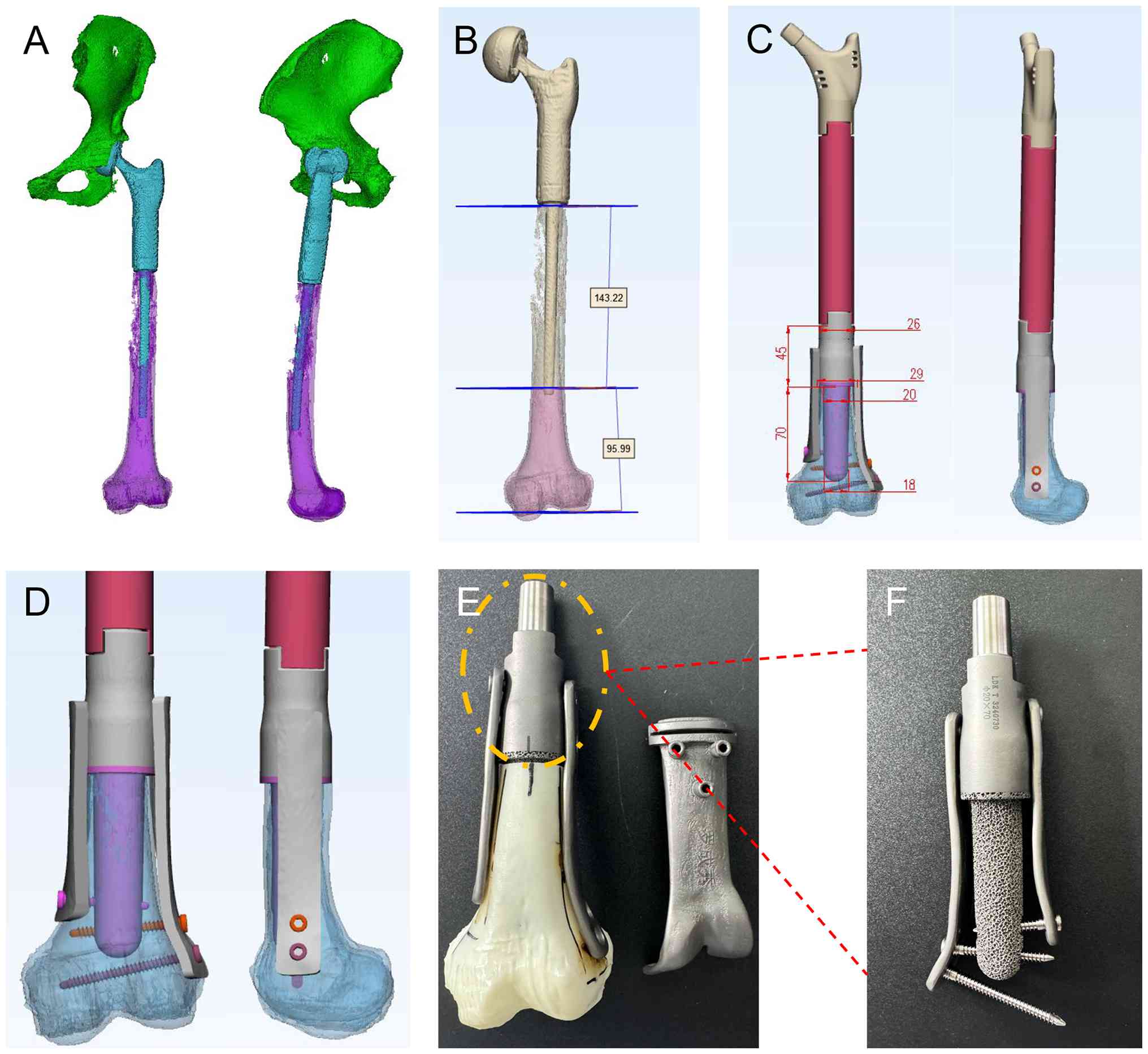
Due to notable bone destruction at the left distal
femur, the surgeon opted for surgical resection of the distal femur
lesion and performed reconstruction using a 3D-printed custom
prosthesis (Fig. 2). Because the
length of the distal medullary canal was short and intramedullary
nail fixation could not provide sufficient stability, additional
plates were applied on both sides of the construct to augment
fixation. The interface between the prosthesis and the distal femur
was composed of trabecular bone structure, which facilitated
osseointegration and effectively decreased the risk of mechanical
complications, such as long-term loosening and fracture. The 3D
printed artificial femur prosthesis was designed and manufactured
by Beijing Lidakang Technology Co., Ltd.
Surgical procedure and postoperative
diagnosis
A 30 cm surgical incision was made along the lateral
left thigh to expose the proximal femoral shaft prosthesis. Fluid
accumulation was observed around the prosthesis, and a sample was
collected for microbiological analysis. The upper femoral segment
wound was protected with sterile gauze, while the lower femoral
segment was exposed. The bone destruction in the middle of the left
femur was notable, accompanied by a soft tissue mass. A femoral
osteotomy was performed 9.6 cm above the lateral femoral condyle of
the distal femur. After complete incision of the scarred hip
capsule, the hip prosthesis and distal femur were removed. When the
hip prosthesis was separated from the distal femur, yellow-white
pus was observed around the prosthesis, and the pus was retained to
detect microorganisms. The tissue around the hip prosthesis and the
middle and upper femur, including scar and necrotic tissue, was
completely removed. The wound was rinsed with iodophor and hydrogen
peroxide five times, and surgical gloves and sheets were replaced.
The 3D-printed distal femoral prosthesis was implanted into the
medullary cavity of the femur retention segment and the upper
segment of the prosthesis was connected to the newly implanted
modular tumor type half-hip prosthesis. The wound was irrigated
twice with iodophor saline and hydrogen peroxide. Following
surgery, the left lower limb was placed in a T-shape shoe to
prevent external rotation and maintained in 30˚ of abduction with
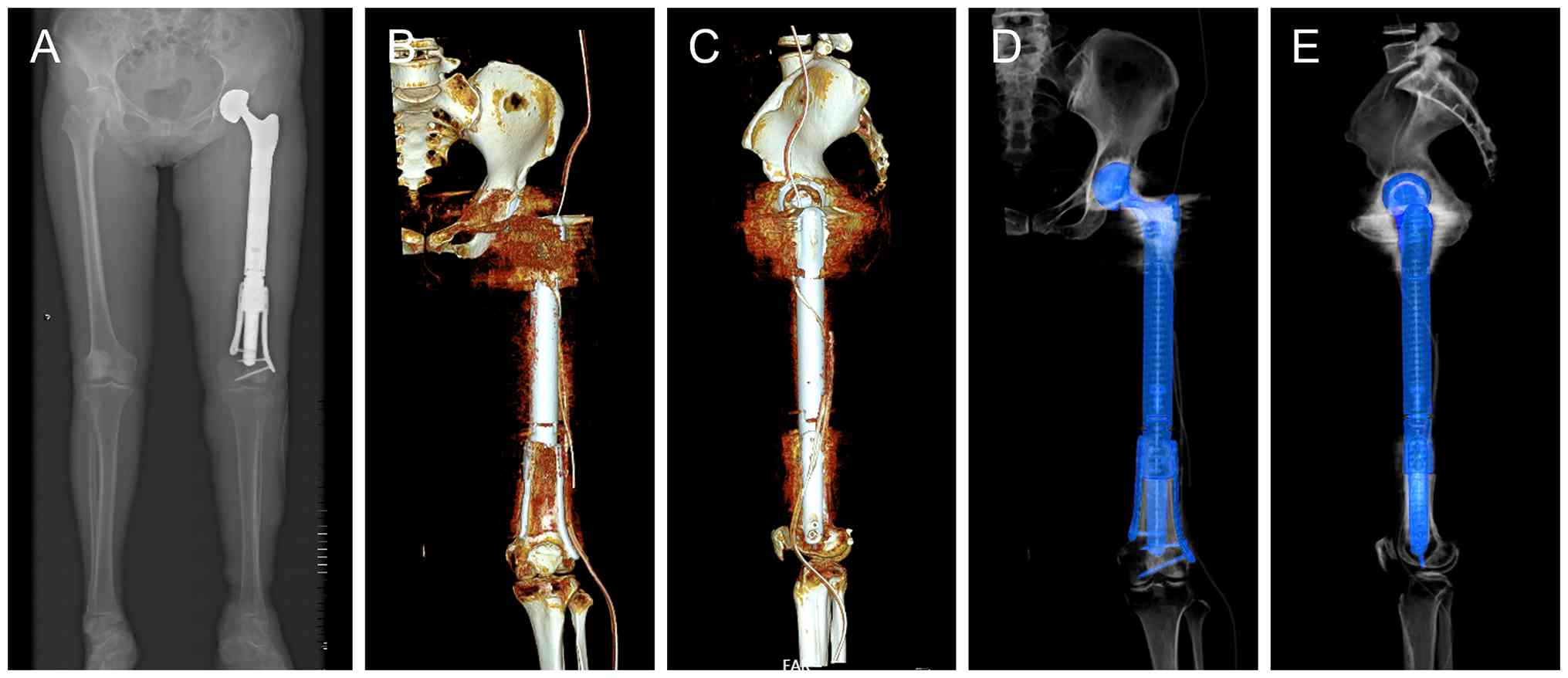
neutral rotation. A total of 3 days after the surgery, the lumbar
spine anteroposterior and lateral X-ray and CT scan showed that 3D
printed artificial femoral prosthesis and modular tumor type
half-hip prosthesis. were in good position and the intervertebral
height was satisfactory (Fig.
3).
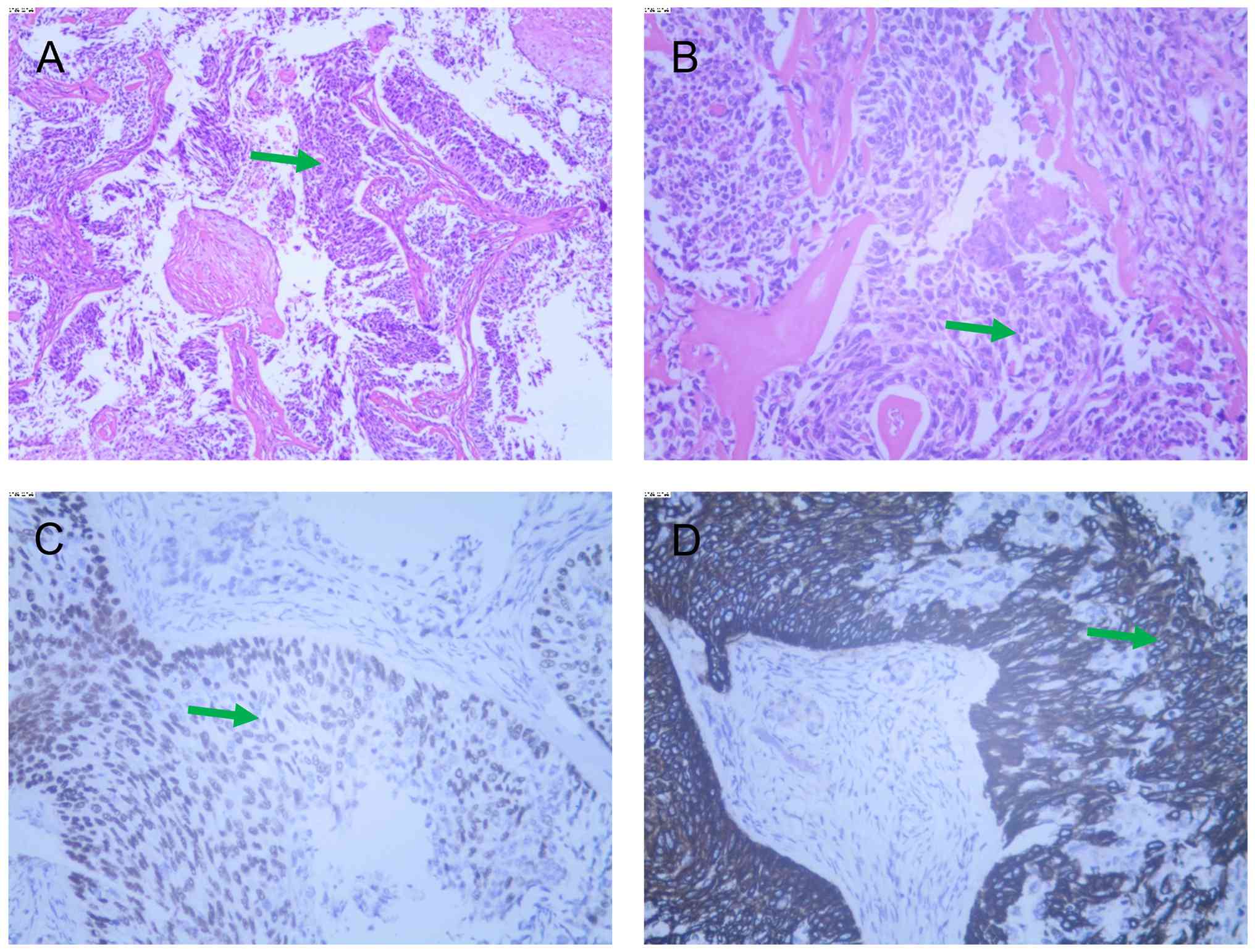
Routine hematoxylin and eosin (HE) staining (10%
neutral buffered formalin, room temperature, 24 h; 4-µm sections;
hematoxylin 5 min, eosin 1 min, at room temperature; light
microscope) was performed on the pathological specimens and
re-evaluation of the immunological marker. Heterotypic cell nest
specimens were found between the fibrous tissue and no clear
malignant tumors were found at the four incisal margins of soft
tissue and the pulp cavity of the broken end. Immunohistochemical
(IHC) staining was performed on formalin-fixed, paraffin-embedded
tissue sections as previously described (8), and the IHC results were as follows:
Pan cytokeratin (CK)(+), vimentin(-), CK7(+), CK20(-),
synaptophysin(-), chromogranin A(-), CD56(-), Ki-67(+, ~60%), tumor
protein p63 (p63)(partially +), p40(partially +), CK5/6(partially
+), CD10(-), high molecular weight CK(partially +), thyroid
transcription factor-1(-), napsin A(-) and thyroglobulin(-)
(Fig. 4). HE staining and
immunohistochemical results supported the diagnosis of metastatic
poorly differentiated carcinoma, with a phenotype indicating
squamous differentiation. Cervical cancer metastasis was first
considered in combination with medical history. Pus was observed
around the prosthesis and the bacterial culture was positive for
Staphylococcus lugdunensis. Combined with pathological and
microbial culture results, the postoperative diagnosis was
recurrence of cervical cancer with metastasis to the left femur
accompanied by periprosthetic infection of the left femoral
prosthesis.
Postoperative treatment and
follow-up
According to the results of microbial culture and
drug sensitivity test (Table I),
intravenous cefazolin sodium (1 g) was administered three times
daily combined with oral rifampicin 300 mg twice daily during the 1
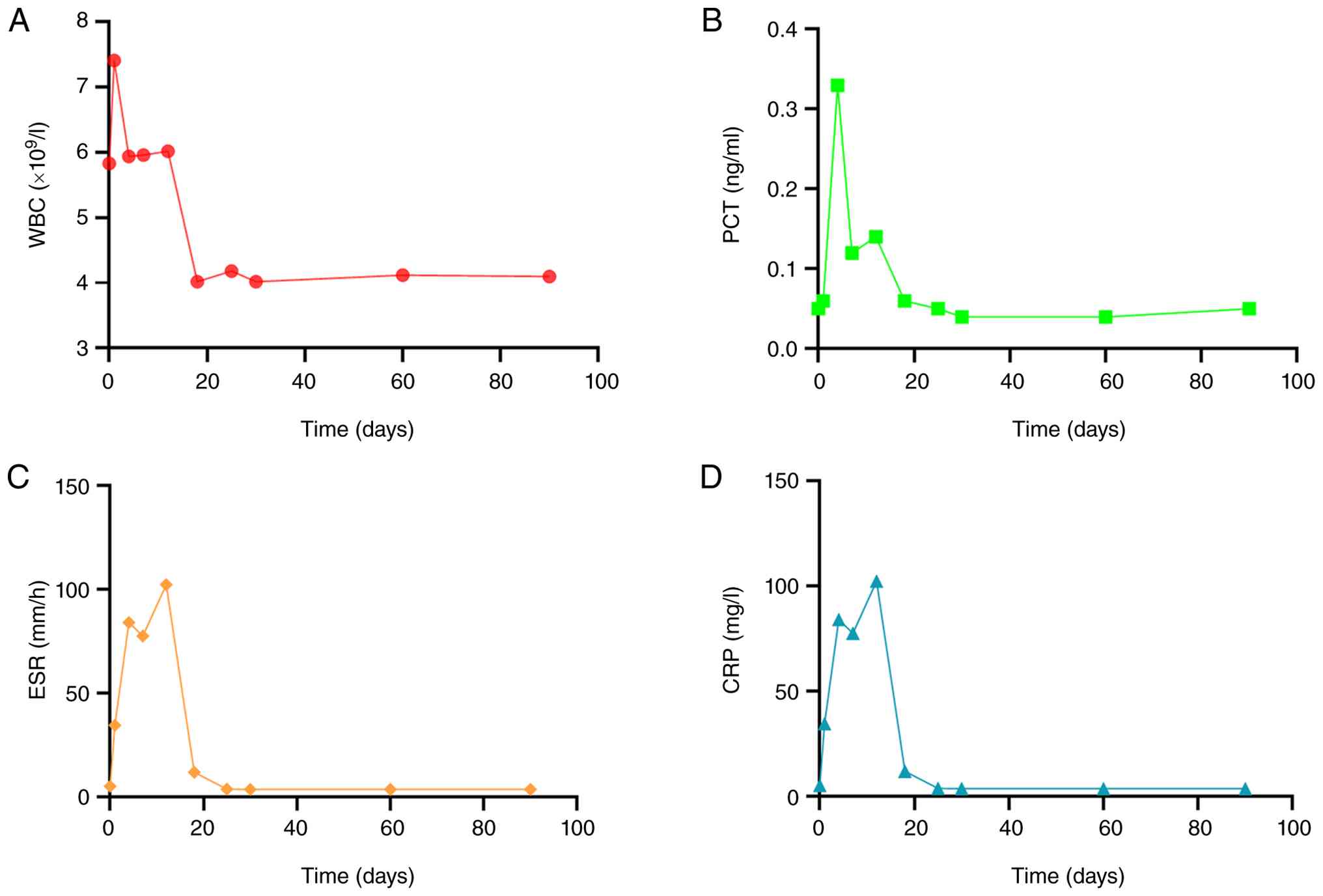
month antibiotic treatment period. Postoperative infection markers
(C-reactive protein, ESR, procalcitonin) were monitored daily;
these markers rose on postoperative days 2-3, followed by a gradual
decline and return to normal by postoperative day 90 (Fig. 5). In addition, the patient body
temperature remained normal following surgery. Bacterial culture
was performed on wound drainage every 2 days and the results were
negative for bacterial growth. The patient underwent outpatient
follow-up visits at 1, 2 and 12 months postoperatively, with no
postoperative complications observed during this period. X-ray and
CT scan at 12 months after surgery demonstrated satisfactory
positioning of the prosthesis without any signs of loosening,
periprosthetic infection and fracture. In addition, no bone
absorption was observed between the distal residual femur and the
prosthesis and new bone growth was evident within the trabecular
structure of the 3D-printed prosthesis. The patient was
asymptomatic at the 12-month follow-up in June 2025, walking
without a crutch and reported a visual analog scale score (9) of 0 for left thigh pain (Fig. 6).
 | Table IAntimicrobial susceptibility. |
Table I
Antimicrobial susceptibility.
| Antibiotic | MIC, mg/l | Interpretation | Reference range,
mg/l |
|---|
| Ciprofloxacin | ≤0.50 | S | 1.00-4.00 |
| Clindamycin | ≤0.25 | S | 0.50-4.00 |
| Erythromycin | ≤0.25 | S | 0.50-8.00 |
| Gentamicin | ≤0.50 | S | 4.00-16.00 |
| Linezolid | 2.00 | S | 4.00-8.00 |
| Levofloxacin | ≤0.12 | S | 1.00-4.00 |
| Moxifloxacin | ≤0.25 | S | 0.50-2.00 |
| Furantoin | ≤16.00 | S | 32.00-128.00 |
| Oxacillin | 0.50 | S | 2.00-4.00 |
| Penicillin | ≥0.50 | R | 0.13-0.25 |
| Rifampicin | ≤0.50 | S | 1.00-4.00 |
| Cotrimoxazole | ≤0.50 | S | 2.00-4.00 |
| Tetracycline | 2.00 | S | 4.00-16.00 |
| Tigacycline | ≤0.12 | S | ≤0.50 |
| Vancomycin | ≤0.50 | S | 4.00-32.00 |
Discussion
Cervical cancer is a notable burden in developing
countries. Bone is the third most common site of distant metastasis
after the lung and liver (3).
Among patients with bone recurrence, 62-93% experience bone-related
symptoms, such as bone pain or neurological deficit (3,10).
Diagnostic imaging techniques such as bone scan, CT, MRI and
18F-fluorodeoxyglucose (18FDG)-positron emission
tomography are widely used for the diagnosis of bone metastasis. In
the present patient, a bone scan performed 2 years after cervical
cancer surgery demonstrated abnormal nuclide concentration in the
left proximal femur, suggesting recurrence of cervical cancer with
bone metastasis. Subsequently, left hip prosthesis replacement was
performed and the postoperative pathology confirmed bone
metastasis. Therefore, scanning served an important role in
detecting bone metastasis. Treatment strategies for patients with
cervical cancer accompanied by bone metastasis are complex and
require consideration of factors such as the primary treatment,
metastasis site, recurrence-free interval, metastasis symptoms and
ECOG performance status (11) when
determining whether to employ surgery, chemotherapy and/or
radiotherapy (12). Patients with
bone metastasis typically have a poor prognosis, with a 5-year
overall survival rate of ~10% after bone recurrence (13).
Tumor-type endoprostheses have facilitated
limb-salvage procedures in primary bone and soft tissue sarcomas
and are increasingly being used in symptomatic metastases of the
long bones (14,15). Although artificial joint
implantation improves patient quality of life, it is often
accompanied by complications, including aseptic failure and
prosthetic joint infection (PJI). The diagnosis and optimal
treatment of PJI remains a challenge. Early postoperative and acute
hematogenous infection are typically easier to identify, but
late-onset chronic infection is difficult to predict. Clinical
signs and symptoms, laboratory tests, radiography and joint
aspiration are insensitive and non-specific (16). In addition, artifacts produced by
the prosthetic devices interfere with tomographic imaging
techniques such as CT and MRI. In the present patient, imaging
studies showed no evidence of periprosthetic infection and the
levels of CRP, procalcitonin and WBC, which are indicators of
infection, were in normal range, although ESR was elevated.
Additionally, patients with malignant tumors or periprosthetic
infection may also have elevated ESR (17). Bone scans suggested recurrence of
periprosthesis bone metastases. Considering the patient history of
cervical cancer bone metastasis, there was concern about the
recurrence of bone metastasis around the femoral prosthesis.
Periprosthetic infection can be easily overlooked, as its clinical
manifestations and imaging features may be obscured by or mimic
tumor recurrence. In the present case, preoperative bone
scintigraphy suggested tumor recurrence but failed to detect
periprosthetic infection, which was only confirmed
intraoperatively. This highlights the limitation of bone scans in
distinguishing infection from tumor-associated inflammation.
18F-FDG PET-CT may offer an enhanced imaging modality for more
accurate characterization of lesions by integrating anatomical and
metabolic imaging (18). As
demonstrated by Mulita et al (19), PET-CT scan detects occult lesions
and improve target delineation in 76.5% of patients. PET-CT
exhibits higher sensitivity in characterizing metabolically active
lesions, which may improve preoperative diagnostic accuracy in
complex cases, guiding surgical planning and potentially avoiding
unexpected intraoperative findings (20). Beyond precise diagnosis, Internet
of Surgical Things (IoST) enables early detection of complications
and improves surgical precision to optimize patient management. As
highlighted by Mulita et al (21), the IoST enhances healthcare through
remote surgery and continuous patient monitoring. In the context of
bone tumor recurrence and infection, perioperative remote
monitoring could enable early detection of recurrent infection or
mechanical complications, while IoST-based systems integrate
preoperative 3D planning with intraoperative navigation, thereby
improving surgical precision. Thus, incorporating IoST technology
into multidisciplinary bone tumor management may facilitate more
responsive healthcare delivery.
3D printing, also known as additive manufacturing,
converts digital models into physical objects through a process
beginning with computer-aided design and converting images into
standard triangular mesh files readable by printers. Since its
emergence in the 1980s, its applications in medicine have expanded
rapidly. An early report described the use of stereolithography to
create cardiac structural models, which were used to optimize
surgical planning (6). In bone
tumors, 3D printing technology enables the fabrication of
customized prostheses that precisely match the morphology of bone
defects, facilitates preoperative simulation to enhance surgical
accuracy and allows design of porous trabecular structures at the
bone-implant interface to promote osseointegration (22). These capabilities are valuable in
complex cases involving large bone defect, tumor recurrence and
periprosthetic infection, where conventional implants typically
fail to meet clinical requirements (23). Lu et al (6) performed segmental resection of
malignant bone tumors in the bone shaft with 3D printed titanium
alloy prosthesis replacement and reported all cases achieved limb
function recovery and prosthesis stability. The present study
reconstructed a large segmental bone defect after tumor resection
using a 3D-printed femoral prosthesis, resulting in a favorable
clinical outcome. The present case reports the concurrent
management of tumor recurrence and periprosthetic infection, which
are challenging complications rarely reported together. The primary
mechanism underlying periprosthetic infection involves pathogenic
bacteria colonizing the surface of joints and forming irreversible
biofilms. The biofilms formed by pathogens around the prosthesis
render conventional antibiotics ineffective (24). Studies have confirmed that only
rifampicin and quinolones effectively eradicate bacteria in
biofilms (25,26). Therefore, rifampicin was
administered to the present patient for 1 month after surgery and
the infection was well controlled without recurrence.
In conclusion, 3D-printed prostheses provide a
promising reconstructive option for large extensive bone defect
following tumor resection. Combined surgical debridement and with
targeted antibiotic therapy may effectively control periprosthetic
infection and enable successful limb salvage.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the National Natural
Science Foundation of China (grant no. 82301534), the Basic
Research Project of Yunnan Province (grant no. 202401CF070010), the
High-Level Talent Introduction Program of Yunnan Provincial Health
Commission (grant no. 2023-KHRCBZ-B17), the First-level Discipline
Team of Kunming Medical University (grant no. 2024XKTDYS05), the
Scientific Research Fund Project of Yunnan Provincial Department of
Education (grant no. 2024J0244) and the Science and Technology Plan
Project of Yunnan Provincial Department of Science and Technology
(grant no. 202501CF070030).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
JL wrote the manuscript. JL and HL revised the
manuscript. YZ, JK, YN and SC performed follow-up. CT collected
associated references. JL and CT performed the analysis and
interpretation of data. YX and HL conceived the study and edited
the manuscript. All authors have read and approved the final
manuscript. JL and YX confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Informed consent was obtained from the patient for
the publication of this case report, including the publication of
all images, clinical data and other data included in the
manuscript.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gioe A, Arciuolo D, Carbone V, Zannoni G,
Gambacorta MA, Maccauro G, Scambia G and Corrado G: Isolated
humeral metastasis in cervical cancer: A case report and review of
the literature. J Cancer Res Ther. 18:273–276. 2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Li H, Wu X and Cheng X: Advances in
diagnosis and treatment of metastatic cervical cancer. J Gynecol
Oncol. 27(e43)2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Thanapprapasr D, Nartthanarung A,
Likittanasombut P, Na Ayudhya NI, Charakorn C, Udomsubpayakul U,
Subhadarbandhu T and Wilailak S: Bone metastasis in cervical cancer
patients over a 10-year period. Int J Gynecol Cancer. 20:373–378.
2010.PubMed/NCBI View Article : Google Scholar
|
|
4
|
van Meir H, Kenter GG, Burggraaf J, Kroep
JR, Welters MJ, Melief CJ, van der Burg SH and van Poelgeest MI:
The need for improvement of the treatment of advanced and
metastatic cervical cancer, the rationale for combined
chemo-immunotherapy. Anticancer Agents Med Chem. 14:190–203.
2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Huang X, Huang D, Lin N, Yan X, Qu H and
Ye Z: 3D-Printed prosthesis with an articular interface for
anatomical acetabular reconstruction After Type I + II (+ III)
Internal Hemipelvectomy: Clinical outcomes and finite element
analysis. J Bone Joint Surg Am. 107:184–195. 2025.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Anagnostopoulos S, Baltayiannis N,
Koletsis NE, Mulita F, Spanou F, Leivaditis V, Katsakiori P,
Tsakaldimis G, Nikolakopoulos K and Mitsos S: 3D printing in
medicine: Bridging imaging, education, and practice. Arch Med Sci
Atheroscler Dis. 10:e172–e188. 2025.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Lu Y, Chen G, Long Z, Li M, Ji C, Wang F,
Li H, Lu J, Wang Z and Li J: Novel 3D-printed prosthetic composite
for reconstruction of massive bone defects in lower extremities
after malignant tumor resection. J Bone Oncol.
16(100220)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Magaki S, Hojat SA, Wei B, So A and Yong
WH: An introduction to the performance of immunohistochemistry.
Methods Mol Biol. 1897:289–298. 2019.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Huskisson EC: Measurement of pain. Lancet.
2:1127–1131. 1974.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Nartthanarung A, Thanapprapasr K,
Udomsubpayakul U and Thanapprapasr D: Age and survival of cervical
cancer patients with bone metastasis. Asian Pac J Cancer Prev.
15:8401–8404. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982.PubMed/NCBI
|
|
12
|
Atjimakul T and Hanprasertpong J: Clinical
outcomes and their prognostic factors among cervical cancer
patients with bone recurrence. Obstet Gynecol Int.
2022(3446293)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kim TH, Kim MH, Kim BJ, Park SI, Ryu SY
and Cho CK: Prognostic importance of the site of recurrence in
patients with metastatic recurrent cervical cancer. Int J Radiat
Oncol Biol Phys. 98:1124–1131. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Smolle MA, Andreou D, Tunn PU and Leithner
A: Advances in tumour endoprostheses: A systematic review. EFORT
Open Rev. 4:445–459. 2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Kendal JK, Hamad CD, Abbott AG, Greig D,
Trikha R, Christ AB, Wessel LE, Puloski SKT, Monument MJ and
Bernthal NM: What are the indications and survivorship of tumor
endoprosthetic reconstructions for patients with extremity
metastatic bone disease? J Surg Oncol. 127:1196–1202.
2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Cobo J and Del Pozo JL: Prosthetic joint
infection: Diagnosis and management. Expert Rev Anti Infect Ther.
9:787–802. 2011.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Brigden ML: Clinical utility of the
erythrocyte sedimentation rate. Am Fam Physician. 60:1443–1450.
1999.PubMed/NCBI
|
|
18
|
Mulita A, Bekou E, Valsamaki P,
Koukourakis IM, Mulita F, Liolis E, Zissimopoulos A, Giatromanolaki
A and Koukourakis MI: 18F-FDG PET-CT-vs. CT-Based radiotherapy
treatment planning for head and neck cancer. Life (Basel).
16(263)2026.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Mulita A, Valsamaki P, Bekou E, Anevlavis
S, Nanos C, Zisimopoulos A, Giatromanolaki A and Koukourakis MI:
Benefits from 18F-FDG PET-CT-based radiotherapy planning in stage
III Non-small-cell lung cancer: A prospective Single-center study.
Cancers (Basel). 17(1969)2025.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Li L, Hu X, Ma J, Yang S, Gong W and Zhang
C: A systematic review of [68Ga]Ga-DOTA-FAPI-04 and [18F]FDG PET/CT
in the diagnostic value of malignant tumor bone metastasis. Front
Oncol. 12(978506)2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mulita F, Verras GI, Anagnostopoulos CN
and Kotis K: A smarter health through the internet of surgical
things. Sensors (Basel). 22(4577)2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Park JW and Kang HG: Application of
3-dimensional printing implants for bone tumors. Clin Exp Pediatr.
65:476–482. 2022.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Liang H, Guo W, Yang Y, Li D, Yang R, Tang
X and Yan T: Efficacy and safety of a 3D-printed arthrodesis
prosthesis for reconstruction after resection of the proximal
humerus: Preliminary outcomes with a minimum 2-year follow-up. BMC
Musculoskelet Disord. 23(635)2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Almasri D and Dahman Y: Prosthetic joint
infections: Biofilm formation, management, and the potential of
mesoporous bioactive glass as a new treatment option.
Pharmaceutics. 15(1401)2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Zimmerli W: Clinical presentation and
treatment of orthopaedic implant-associated infection. J Intern
Med. 276:111–119. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Aboltins C, Daffy J, Choong P and Stanley
P: Current concepts in the management of prosthetic joint
infection. Intern Med J. 44:834–840. 2014.PubMed/NCBI View Article : Google Scholar
|