Introduction
A proximal humerus fracture (PHF) is a type of bone
trauma caused by external forces, such as direct or indirect impact
to the shoulder (1). This kind of
injury leads to a series of symptoms, including persistent pain at
the fracture site, especially when the shoulder is moved or the
injured area is touched, which intensifies the pain Local swelling
may occur due to soft tissue damage, leading to the exudation of
blood and tissue fluid. Additionally, shoulder joint mobility
becomes limited, and patients have difficulty lifting, abducting,
or rotating the arm normally (2,3).
Severe cases may also involve deformities of the shoulder
appearance, such as local protrusion or depression, which are
asymmetrical to the opposite shoulder (4,5).
Proximal humeral fractures account for ~4-5% of all fractures in
the body, 26% of shoulder fractures, and up to one-third of
fractures in older adults (6). Its
incidence rate is second only to that of the hip and distal radial
fractures. It is more common in the elderly population,
particularly in postmenopausal women. The increased incidence of
PHFs is closely related to several factors. For example,
osteoporosis reduces bone strength and toughness of the bones
decrease, and even a slight external force can easily cause
fractures (7,8). In addition, because the risk of
shoulder injury increases among people engaged in high-intensity
physical labor or extreme sports, the incidence rate of proximal
humeral fractures also increases. With the intensification of the
aging global population, its incidence is expected to continue
rising (9,10). In the treatment of PHFs, the
existing options include conservative treatment and surgical
treatment (11,12). Surgical intervention has become the
primary treatment modality for most patients (13,14).
Therefore, selecting an appropriate surgical approach is critical,
as different techniques vary substantially in terms of operative
time, length of hospital stay, and postoperative rehabilitation
(15). Among the available
surgical options, open reduction and internal fixation (ORIF) and
reverse total shoulder arthroplasty (RTSA) are the two most
commonly employed procedures. ORIF involves surgical exposure of
the fracture site, followed by anatomical reduction and
stabilization using internal fixation devices such as plates and
screws. It is generally indicated for relatively simple fractures
with limited displacement and allows the restoration of anatomical
continuity and mechanical stability (16,17).
By contrast, RTSA is typically indicated for complex fracture
patterns, including comminuted fractures, osteoporotic fractures
and humeral head necrosis (18).
By replacing the native joint with a prosthesis, RTSA enables the
restoration of shoulder function. Although RTSA is technically more
demanding and may entail a longer operative time than ORIF, it
provides improved articular surface reconstruction and may
facilitate earlier functional rehabilitation in selected patients
(19). Although both RTSA and ORIF
are commonly used to treat PHFs, current literature presents
inconsistent conclusions regarding their relative effectiveness.
Previous studies have reported inconsistent findings regarding the
comparative efficacy of ORIF and RTSA. Some studies suggested that
ORIF may be associated with a shorter operative time (20), whereas others indicated that RTSA
may provide superior improvements in postoperative forward flexion
and abduction (21). These
discrepancies underscore the need for a comprehensive and
systematic comparison of the two surgical approaches; therefore,
the present meta-analysis was conducted to compare the clinical
outcomes of RTSA and ORIF in the treatment of proximal humeral
fractures. By synthesizing evidence from multiple studies, the aim
of the present study was to provide more robust evidence to inform
surgical decision-making in clinical practice. It was aimed to
provide reliable, evidence-based guidance for surgeons in selecting
the most appropriate surgical plan, ultimately improving treatment
outcomes and patient quality of life.
Materials and methods
Retrieval strategy
Search databases such as PubMed, Embase, CINAHL,
Cochrane Library, CNKI (China National Knowledge Infrastructure)
and Wanfang. Relevant literature was retrieved from all databases.
The search strategy was: (‘RTSA’ OR Reverse Total Shoulder
Arthroplasty) AND (‘ORIF’ OR ‘Open Reduction and Internal
Fixation’) AND (‘Proximal Humeral Fractures’ OR ‘Proximal Humerus
Fracture’).
Inclusion and exclusion criteria
Inclusion criteria were as follows: i) Research
subjects: Patients diagnosed with PHF requiring surgery; ii)
Intervention measures: The experimental group received RTSA, and
the control group received ORIF; iii) Outcome indicators: Six items
including angles of forward flexion, abduction, external rotation,
DASH score, Constant score and operation duration; iv) Study
design: Clinical controlled trials. Exclusion criteria were as
follows: i) Treatment involving shoulder hemiarthroplasty; ii)
Reviews, systematic reviews, case reports, letters, or duplicate
publications; iii) non-case-control studies; iv) Incomplete outcome
data or irrelevant studies.
Data extraction
Two independent researchers extracted data using a
standardized protocol. Any disagreements were resolved through
discussion or reviewed by senior researchers until consensus was
reached. The included studies were assessed using the
Newcastle-Ottawa Scale (NOS). In the outcome assessment, a
follow-up time of ≥1 year and a loss to follow-up rate of ≤15% were
considered acceptable. Study quality was categorized as low (<5
points), moderate (5-7 points), or high (8-9 points).
Statistical methods
All meta-analyses were performed using Review
Manager (RevMan version 5.4; Cochrane Collaboration). Dichotomous
outcomes were expressed as odds ratios (ORs) with 95% confidence
intervals (CIs), whereas continuous outcomes were expressed as mean
differences (MDs) or standardized mean differences (SMDs) with 95%
CIs. Statistical significance was defined as a two-sided P≤0.05.
Heterogeneity among studies was assessed using the I2
statistic. When the heterogeneity was low (I2<50%), a
fixed-effects model was applied; otherwise (I2>50%),
a random-effects model was used. Sensitivity and subgroup analyses
were conducted to explore potential sources of heterogeneity.
Sensitivity analysis was performed by sequentially excluding
individual studies to evaluate the stability of the results.
Publication bias was assessed using funnel plots.
Results
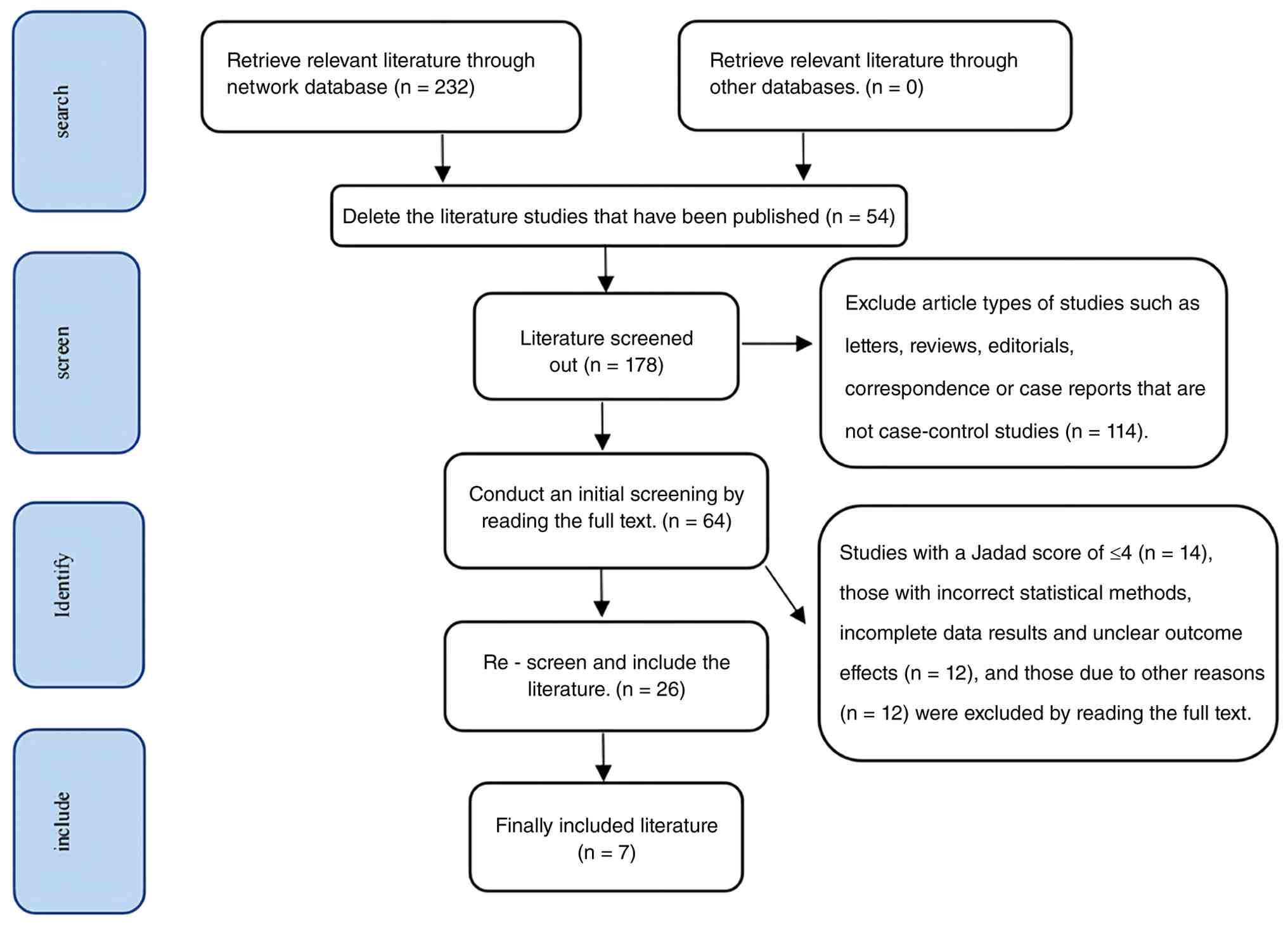
Retrieval results
A total of 232 relevant studies were retrieved from
the databases. After applying the inclusion and exclusion criteria,
7 studies were included in the analysis.
Basic information of the included
literatures
Among the included studies, 5 reported forward
flexion angles, 4 reported abduction angles, 5 reported external
rotation angles, 4 reported DASH scores, 3 reported Constant
scores, and 4 reported operation duration. In total, 514 patients
were included: 257 received the RTSA, and 257 received the ORIF.
The study selection process is shown in Fig. 1, and basic study characteristics
are presented in Table I (22-28).
 | Table IBasic characteristics of the included
studies. |
Table I
Basic characteristics of the included
studies.
| First author/s,
year | Research type | Country | Surgical
approach | Number of cases
(n) | Average age/year | Sex
(male/female) | Outcome | Quality evaluation
(NOS) | (Refs.) |
|---|
| Repetto et al,
2017 | Retrospective cohort
study | Italy | RTSA ORIF | 27 19 | 71..2±7.5
65.3±12.4 | 7/20 6/13 | (1) (2) (3) (4) | 7 | (22) |
| Giardella et
al, 2017 | Retrospective cohort
study | Italy | RTSA ORIF | 21 23 | 63.7±8.4
68.2±7.3 | 8/13 9/14 | (1) (2) (3) (5) | 7 | (23) |
| Tong et al,
2023 | Retrospective cohort
study | Hong Kong | RTSA ORIF | 25 25 | 77.0±7.14
75.2±6.79 | 3/22 3/22 | (1) (2) (3) (4) (5)
(6) | 8 | (24) |
| Lanzetti et
al, 2023 | Retrospective cohort
study | Italy | RTSA ORIF | 72 66 | 73.00±10.00
63.00±14.00 | 18/54 20/46 | (1) (2) (3) (4) (5)
(6) | 8 | (25) |
| Samborski et
al, 2022 | Retrospective cohort
study | USA | RTSA ORIF | 24 23 | 77.30±9.50
67.10±5.50 | 1/23 5/18 | (1) (3) | 6 | (26) |
| Ott et al,
2022 | Retrospective cohort
study | Germany | RTSA ORIF | 71 90 | 82.20±6.10
82.00±6.50 | 18/53 17/73 | (6) | 4 | (27) |
| Jaekel et
al, 2025 | Retrospective
cohort study | Germany | RTSA ORIF | 17 17 | 77.8±5.9
75.3±6.3 | 1/16 3/14 | (4) (6) | 6 | (28) |
Quality evaluation of the included
literatures
A total of seven retrospective cohort studies were
included in this meta-analysis. The NOS was used to assess
methodological quality. Specifically, two studies scored 8 points,
indicating high methodological quality, two scored 7 points, and
another two scored 6 points, resulting in four studies with
moderate methodological quality. One study scored 4 points,
indicating low methodological quality.
Results of meta-analysis. Comparison
of postoperative indicators
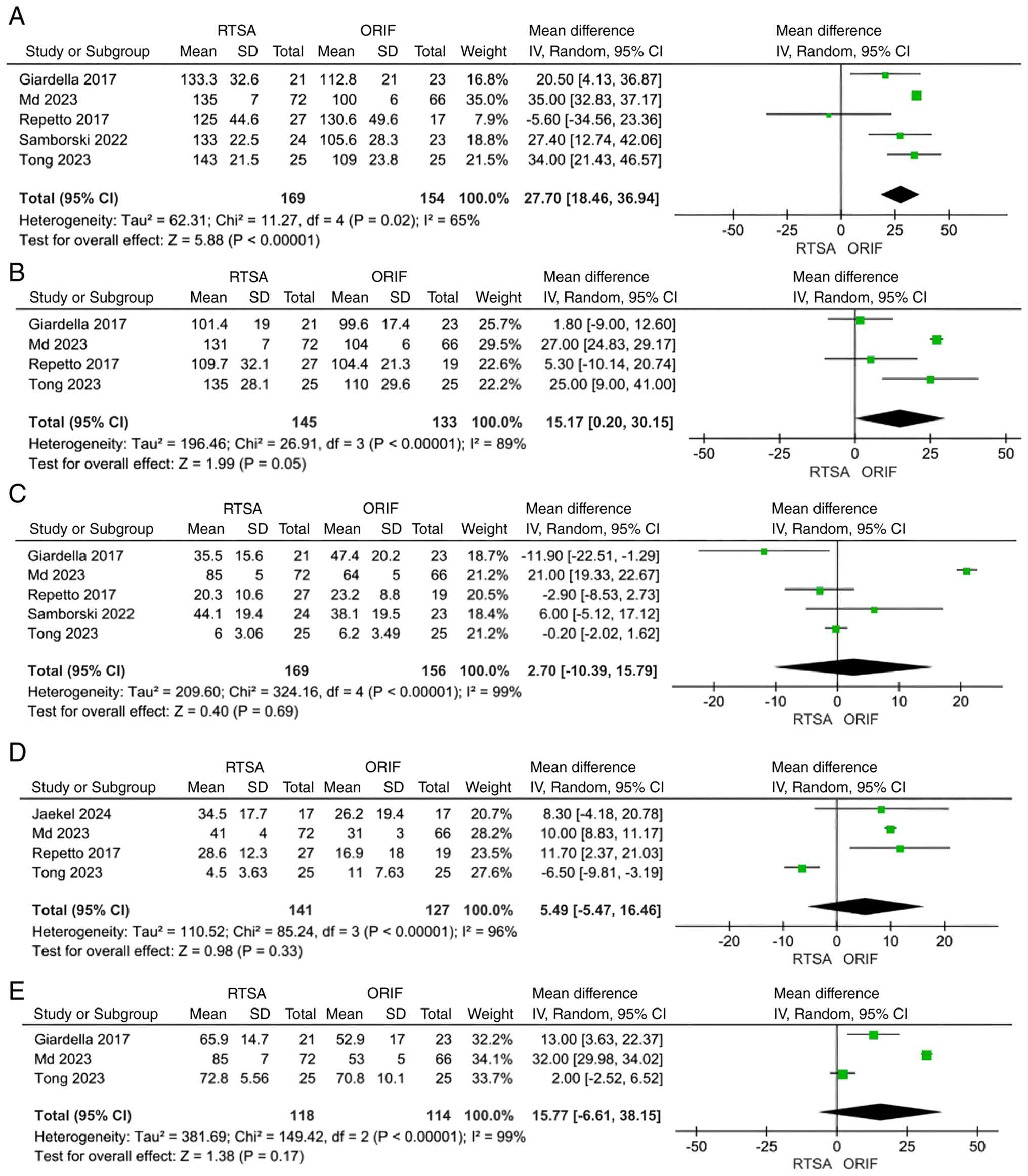
Postoperative outcomes included forward flexion,
abduction and external rotation angles, as well as Disabilities of
the Arm, Shoulder, and Hand (DASH) and Constant scores. Five
studies compared forward flexion between RTSA and ORIF. Moderate
heterogeneity was observed (I²=65%); therefore, a random-effects
model was used. The pooled analysis demonstrated that forward
flexion was significantly greater in the RTSA group than in the
ORIF group (MD=27.70; 95% CI: 18.46 to 36.94; P<0.00001;
Fig. 2A). Four studies reported
abduction. Given the substantial heterogeneity (I²=89%), a
random-effects model was used. The results indicated that abduction
was significantly improved in the RTSA group compared with the ORIF
group (MD=15.18; 95% CI: 0.20 to 30.15; P=0.05; Fig. 2B). No statistically significant
differences were observed between the two groups in external
rotation (MD=2.70; 95% CI: -10.39 to 15.79; P=0.69; Fig. 2C), DASH score (MD=5.50; 95% CI:
-5.47 to 16.46; P=0.33; Fig. 2D),
or Constant score (MD=15.77; 95% CI: -6.61 to 38.15; P=0.17;
Fig. 2E).
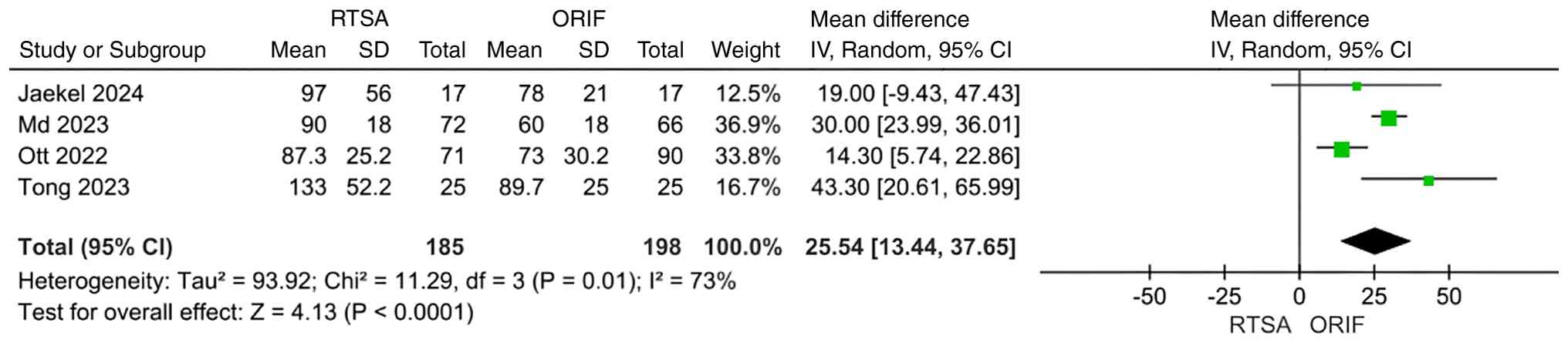
Comparison of intraoperative efficacy
indicators. Operative time was evaluated as an intraoperative
outcome. Four studies compared operative time between RTSA and
ORIF. Substantial heterogeneity was observed (I²=73%); therefore, a
random-effects model was used. The pooled analysis demonstrated
that operative time was significantly longer in the RTSA group than
in the ORIF group (MD=25.55; 95% CI: 13.44 to 37.65; P<0.0001)
(Fig. 3).
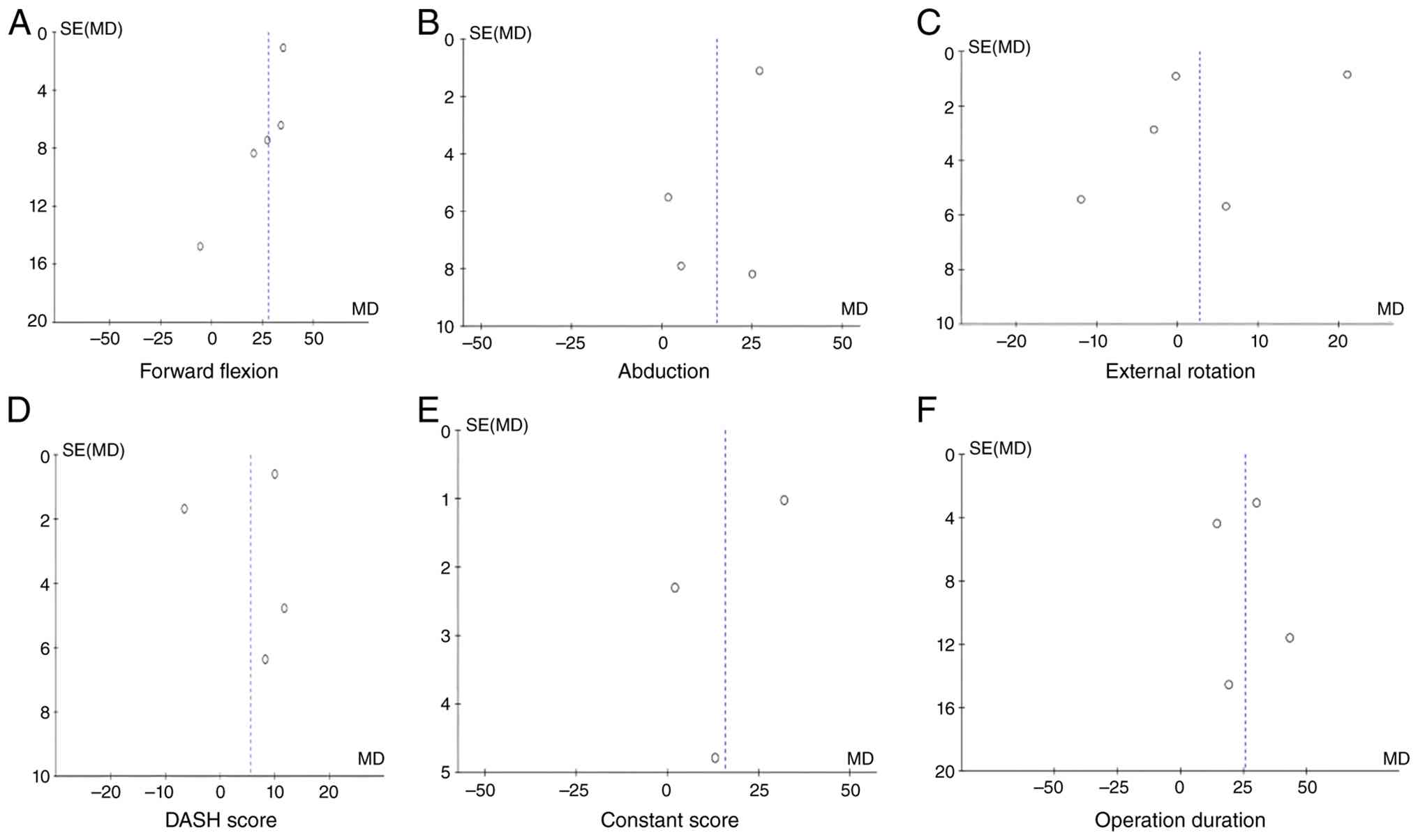
Publication bias and sensitivity analysis.
Review Manager 5.4 statistical software was used to perform
publication bias analysis for six outcome measures in the treatment
of PHF, including forward flexion angle, abduction angle, external
rotation angle, DASH score, Constant score (corrected spelling) and
operative duration. The results demonstrated that each funnel plot
was symmetrical (Fig. 4),
indicating the absence of significant publication bias.
Discussion
The present meta-analysis compared the clinical
efficacy of RTSA with ORIF in the management of PHF. The results
demonstrated significant differences in key outcome measures
between the two surgical approaches, thereby providing valuable
evidence for clinical surgical decision-making.
The findings of the present meta-analysis indicated
that RTSA conferred distinct advantages over ORIF with respect to
postoperative forward flexion and abduction angles, with
statistically significant differences [95% CI (18.46, 36.94),
P<0.00001; and 95% CI (0.20, 30.15), P=0.05; respectively]. This
result is consistent with the outcomes of previously published
relevant studies (21,29), which may be attributed to the
inherent surgical characteristics of RTSA. Clinical practice has
demonstrated that RTSA allows superior articular surface
reconstruction and is well-suited for severe comminuted fractures
or osteoporotic fractures (18),
thereby facilitating improved postoperative shoulder joint range of
motion. In addition, RTSA can effectively compensate for rotator
cuff functional deficits. When the rotator cuff is severely
impaired and unable to function normally, the prosthetic design of
RTSA enables the deltoid muscle to drive shoulder joint movement
directly, thereby promoting recovery of shoulder joint function
(30,31). By contrast, ORIF is associated with
an increased risk of complications, such as nonunion, malunion and
humeral head avascular necrosis, in the management of severe
fractures (16), which may limit
the recovery of shoulder joint mobility and further compromise
postoperative forward flexion and abduction angles. However, the
extent of shoulder joint function improvement achieved with RTSA
may also be influenced by factors such as the surgical technique
and postoperative rehabilitation protocols, which warrant further
validation through additional high-quality studies.
In terms of operative duration, ORIF demonstrated a
significant advantage over RTSA, with a statistically significant
difference [95% CI: 13.44 to 37.65; P<0.00001]. This finding is
primarily attributed to the greater complexity of the RTSA
procedure. Surgeons are required to accurately implant prostheses
(including glenoid and humeral components), precisely prepare the
bony bed to ensure optimal prosthesis position and angulation, and
reconstruct the soft tissue balance and biomechanical structure
surrounding the shoulder joint (32). In addition, the management and
repair of soft tissues, such as the rotator cuff and the deltoid
muscle, are necessary during RTSA to accommodate the new prosthesis
and restore normal shoulder joint motor function (33). In particular, when addressing
narrow and complex anatomical structures, such as the glenoid
cavity, surgical difficulty increases, thereby prolonging the
operative time. By contrast, ORIF primarily involves fixation of
the fracture site using internal fixation materials such as plates
and screws, following fracture reduction, with a relatively
straightforward surgical procedure (16,17),
resulting in a shorter operative duration.
It should be emphasized that the clinical efficacy
of RTSA and ORIF is influenced by multiple factors. For patients
with severe comminuted fractures, osteoporotic fractures, or
concomitant rotator cuff injury, RTSA may represent a more
appropriate therapeutic option as it can effectively address the
challenges of fracture healing and postoperative joint function
recovery. For patients with relatively simple fracture patterns and
no significant displacement, ORIF can meet clinical treatment
requirements, with the distinct advantage of a shorter operative
time, which reduces the risk of intraoperative complications.
Therefore, the selection of a surgical approach should be
determined comprehensively based on individual patient
characteristics, including age, fracture classification,
preoperative shoulder joint function status, and other relevant
clinical factors, to achieve optimal therapeutic outcomes.
The present meta-analysis has certain limitations
that should be acknowledged. A paucity of randomized controlled
trials was identified among the included studies, which resulted in
a relatively low level of evidence. The present meta-analysis was
not pre-registered on PROSPERO or any other public protocol
registration platform, which might have compromised the
transparency of the study design. All included studies were
retrospective cohort studies, with one study achieving a NOS score
of only 4 points, indicating low methodological quality. Although
the sensitivity analysis, excluding this low-quality study,
confirmed the robustness of the primary findings, the retrospective
nature of the included studies may still introduce selection bias
and indication confounding, potentially affecting the reliability
of the results. High heterogeneity was observed across all outcome
measures (forward flexion, I²=65%; abduction, I²=89%; operative
duration, I²=73%), thereby limiting the reliability and
generalizability of the pooled effect estimates. Owing to the lack
of relevant data in the included studies, important clinical
outcomes, such as dislocation, infection, revision surgery and
implant failure, were not analyzed, thereby affecting the
comprehensiveness of the study. Follow-up durations varied across
the included studies, and this variability may introduce bias into
the comparison of functional scores, as longer or shorter follow-up
periods can lead to differential evaluations of functional
recovery. The number of included studies ranged from 3 to 5 for all
outcome measures. The heterogeneity among these studies, coupled
with variations in final follow-up times, may have affected the
results. Additionally, the long-term efficacy remains unclear, and
discrepancies may exist between the findings of this study and
real-world clinical outcomes. Therefore, additional studies with
larger sample sizes are warranted. Future publication of more
high-quality clinical studies focusing on the surgical management
of PHF is anticipated, which will help reduce bias and facilitate
the derivation of more valid and reliable conclusions.
Acknowledgements
Not applicable.
Funding
Funding: This study was supported by the 2023 Research Project
Plan of Changzhi Municipal Health Commission [Changwei Renshi Han
(2023); grant no. 29] (Project title: Screening and Functional
Analysis of Differentially Expressed Metabolites in Plasma of a Rat
Model of Post-Traumatic Osteoarthritis of the Knee after Anterior
Cruciate Ligament Injury).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
PFH, YL and MXN conceived and designed the study.
FZH, XQ and WWW acquired the data. YL, MXN and PFH conducted the
statistical analysis and data interpretation. YL, MXN and FZH
drafted the manuscript. All authors critically revised the
manuscript for important intellectual content, read and approved
the final manuscript, and agree to be accountable for all aspects
of the work. PFH and YL confirm the authenticity of all raw
data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pai S, Kotekar MF, Pawaskar SM and Kumar
MA: Proximal humerus fractures in the elderly. Indian J Orthop.
59:346–357. 2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Younis Z, Hamid MA, Amin J, Khan MM,
Gurukiran G, Sapra R, Singh R, Wani KF and Younus Z: Proximal
humerus fractures: A review of anatomy, classification, management
strategies, and complications. Cureus. 16(e73075)2024.PubMed/NCBI View Article : Google Scholar
|
|
3
|
de Souza Serenza F, Rizzato MMSA, Vieira
F, McQuade KJ and de Oliveira AS: Kinematic analysis of upper limb
fractures: Insights for rehabilitation strategies. Clin Biomech
(Bristol). 122(106432)2025.PubMed/NCBI View Article : Google Scholar
|
|
4
|
De Crescenzo A, Garofalo R, Pederzini LA
and Celli A: Malunion of distal humeral fractures: Current
concepts. J ISAKOS. 9:744–749. 2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Schiffman CJ, Cohn MR, Austin LS and
Namdari S: Reverse shoulder arthroplasty to treat proximal humerus
fracture sequelae: A review. J Am Acad Orthop Surg. 32:681–691.
2024.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Reiad TA, Peveri E, Dinh PV and Owens BD:
Epidemiology of shoulder injuries presenting to US emergency
departments. Orthopedics. 48:e81–e87. 2025.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Malyavko A, Agarwal AR, Mikula JD, Best MJ
and Srikumaran U: Shoulder arthroplasty patients are underscreened
for osteoporosis. J Am Acad Orthop Surg. 33:362–369.
2025.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Ng WX, Acharyya S, Huang S, Kwek EBK and
Tan BY: Deltoid tuberosity index for proximal humerus fracture:
Reliability and a predictor of systemic osteoporosis in an Asian
population. J Shoulder Elbow Surg. 34:e133–e140. 2025.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Fones L, Kachooei AR and Beredjiklian PK:
Trends in orthopaedic surgery on patients 90 years old and older
2014-2023. Arch Bone Jt Surg. 13:157–163. 2025.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Patel AH, Wilder JH, Ofa SA, Lee OC,
Iloanya MC, Savoie FH III and Sherman WF: How age and gender
influence proximal humerus fracture management in patients older
than fifty years. JSES Int. 6:253–258. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Stockwell E, Ahmed A and Mir HR:
Contemporary management of proximal humeral fractures. J Am Acad
Orthop Surg. 33:1082–1091. 2025.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Roivas IA, Leino OK, Lehtimäki KK,
Matilainen M and Ekman E: Proximal humeral fractures in Finland:
Regional differences in incidence and methods of treatment. J
Shoulder Elbow Surg. 34:1081–1087. 2025.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Bezirgan U, Kısmet M, Kıratlıoğlu Y,
Yalçın M and Armangil M: Comparison of locking plate and
conservative treatment in elderly patients with displaced proximal
humerus fractures. Int Orthop. 49:737–745. 2025.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Hernandes Júnior PR, Garcia TA, de
Oliveira Caravellos Glória R, Waldolato G, de Andrade ALL,
Labronici PJ and Belangero WD: Is surgical treatment better than
non-surgical treatment for proximal humeral fracture in elderly
people? A meta-analysis and meta-regression. Eur J Orthop Surg
Traumatol. 35(51)2025.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Thamrongskulsiri N, Prasathaporn N,
Limskul D, Tanpowpong T, Kuptniratsaikul S and Itthipanichpong T:
Lower revision rate of cemented humeral stem reverse total shoulder
arthroplasty compared to cementless humeral stem in proximal
humerus fractures: A systematic review and meta-analysis. Arch
Orthop Trauma Surg. 145(184)2025.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Ye Z, Chen M and Huang Z: Therapeutic
effect of titanium locking plate combined with suture anchor repair
in proximal humeral fractures. Pak J Med Sci. 41:77–82.
2025.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Whiting Z, Haase L, Moon T, Raju A, Wetzel
R, Sontich J, Ochenjele G and Napora J: Comparative outcomes of
operative treatment for two and three-part proximal humerus
fractures with or without ipsilateral shaft fractures and
head-split patterns: Intramedullary nail versus open reduction
internal fixation. Eur J Orthop Surg Traumatol.
35(6)2024.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Barnett JS, Wilson SB, Barry LW, Katayama
ES, Patel AV, Cvetanovich GL, Bishop JY and Rauck RC: Clinical and
functional outcomes of reverse total shoulder arthroplasty for
proximal humerus fracture versus rotator cuff arthropathy: A
retrospective analysis. J Orthop. 68:58–61. 2025.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Goguen J, Forbes J, Jackson GR, Movassaghi
A, Lapica H, Routman H and Sabesan VJ: Optimal timing of reverse
total shoulder arthroplasty for proximal humerus fractures. J
Shoulder Elbow Surg. 34:2537–2542. 2025.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Iking J, Fischhuber K, Katthagen JC,
Oenning S, Raschke MJ, Stolberg-Stolberg J and Köppe J: Reverse
total shoulder arthroplasty versus locked plate fixation for
proximal humeral fractures in the elderly: A systematic review.
PLoS One. 20(e0317005)2025.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Heo SM, Faulkner H, An V, Symes M,
Nandapalan H and Sivakumar B: Outcomes following reverse total
shoulder arthroplasty vs operative fixation for proximal humerus
fractures: A systematic review and meta-analysis. Ann R Coll Surg
Engl. 106:562–568. 2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Repetto I, Alessio-Mazzola M, Cerruti P,
Sanguineti F, Formica M and Felli L: Surgical management of complex
proximal humeral fractures: pinning, locked plate and arthroplasty:
Clinical results and functional outcome on retrospective series of
patients. Musculoskelet Surg. 101:153–158. 2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Giardella A, Ascione F, Mocchi M,
Berlusconi M, Romano AM, Oliva F and Maradei L: Reverse total
shoulder versus angular stable plate treatment for proximal humeral
fractures in over 65 years old patients. Muscles Ligaments Tendons
J. 7:271–278. 2017.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Tong CH and Fang CX: Rehabilitation
progress following reverse total shoulder replacement and internal
fixation for geriatric three and four-part proximal humerus
fractures-a propensity score matched comparison. BMC Musculoskelet
Disord. 24(566)2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Lanzetti RM, Gaj E, Berlinberg EJ, Patel
HH and Spoliti M: Reverse total shoulder arthroplasty demonstrates
better outcomes than angular stable plate in the treatment of
three-part and four-part proximal humerus fractures in patients
older than 70 years. Clin Orthop Relat Res. 481:735–747.
2023.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Samborski SA, Haws BE, Karnyski S, Soles
G, Gorczyca JT, Nicandri G, Voloshin I and Ketz JP: Outcomes for
type C proximal humerus fractures in the adult population:
Comparison of nonoperative treatment, locked plate fixation, and
reverse shoulder arthroplasty. JSES Int. 6:755–762. 2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Ott N, Müller C, Jacobs A, Paul C, Wegmann
K, Müller LP and Kabir K: Outcome of geriatric proximal humeral
fractures: A comparison between reverse shoulder arthroplasty
versus open reduction and internal fixation. OTA Int. 5 (2
Suppl)(e188)2022.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Jaekel C, Oezel L, Leibnitz F, Wilms LM,
Windolf J, Gehrmann SV and Scholz AO: Clinical outcome and quality
of life after modular reverse total shoulder arthroplasty in
comparison with joint-preserving locking plate osteosynthesis in
aged patients: A retrospective comparison study. Orthop Surg.
17:224–232. 2025.PubMed/NCBI View
Article : Google Scholar
|
|
29
|
Colasanti CA, Anil U, Rodriguez K, Levin
JM, Leucht P, Simovitch RW and Zuckerman JD: Optimal combination of
arthroplasty type, fixation method, and postoperative
rehabilitation protocol for complex proximal humerus fractures in
the elderly: A network meta-analysis. J Shoulder Elbow Surg.
33:e559–e574. 2024.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Torchia MT, Austin DC, Cozzolino N,
Jacobowitz L and Bell JE: Acute versus delayed reverse total
shoulder arthroplasty for the treatment of proximal humeral
fractures in the elderly population: A systematic review and
meta-analysis. J Shoulder Elbow Surg. 28:765–773. 2019.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sebastiá-Forcada E, González-Casanueva J,
Miralles-Muñoz FA, Bello Tejeda LL, de la Pinta-Zazo C and
Vizcaya-Moreno MF: Effectiveness over time of the reverse shoulder
prosthesis for acute proximal humeral fracture. J Shoulder Elbow
Surg. 34:847–852. 2025.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Kee HT, Yeak RDK, Ahmad Hanif KA, Seri
Masran SM and Che-Hamzah F: A reshaping recovery: The reverse
shoulder arthroplasty triumphs in salvaging chronic four-part
proximal humerus fractures. Cureus. 15(e50363)2023.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Kramer M, Olach M, Zdravkovic V, Manser M,
Jost B and Spross C: Cemented vs uncemented reverse total shoulder
arthroplasty for the primary treatment of proximal humerus
fractures in the elderly-a retrospective case-control study. BMC
Musculoskelet Disord. 23(1043)2022.PubMed/NCBI View Article : Google Scholar
|