Introduction
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are severe, life-threatening cutaneous adverse reactions, characterized by widespread mucocutaneous necrosis and epidermal detachment. In the most severe cases, these conditions can have mortality rates approaching 50%, which necessitates rapid diagnosis and timely intervention to improve clinical outcomes. Although sulfonamides and β-lactam antibiotics remain the most frequently implicated agents in antibiotic-induced SJS/TEN, emerging evidence indicates that fluoroquinolones account for ~4% of cases, emphasizing the need for clinical vigilance (1-3).
The pathophysiological mechanisms of fluoroquinolone-induced SJS/TEN involve intricate T cell-mediated immune responses (4,5). Clinical manifestations typically evolve from an initial erythematous rash to extensive blistering and epidermal detachment, usually accompanied by severe mucosal involvement. Previous reports have documented six cases of fluoroquinolone-induced SJS/TEN, including four cases using ocular formulations and two using oral formulations. From these, five patients successfully recovered following the administration of supportive care, while the treatment and outcome of one patient were not mentioned. However, the clinical course and outcomes in oncological patients, particularly those with abdominal malignancies, remain inadequately characterized (Table I) (6-11).
 |
Table I
Case reports of fluoroquinolone-induced SJS/TEN.
|
Table I
Case reports of fluoroquinolone-induced SJS/TEN.
| Present situation |
Dosage of fluoroquinolones |
Clinical manifestations |
ADR type |
Treatments |
Prognosis |
(Refs.) |
| Ocular inflammation |
Ciprofloxacin p.o/moxifloxacin gtto. |
Fever, erythematous rashes over face and upper limbs, dyspnea |
SJS |
Corticosteroids, antibiotics |
Recovered after 10 days |
(6) |
| Vasectomy |
Ciprofloxacin p.o. 500 mg qd |
Pruritic, blistering rash |
SJS |
- |
- |
(7) |
| Ocular inflammation |
Moxifloxacin gtto. |
Rashes over trunk |
SJS |
Supportive care |
Recovered within 8 days |
(8) |
| Bacterial conjunctivitis |
Moxifloxacin gtto. bid |
Fever, rashes over entire body |
SJS/TEN |
Supportive care |
Recovered |
(9) |
| Urinary tract infection |
Ciprofloxacin p.o. 500 mg qd |
Pain, epidermal detachment and oral mucosal ulcerations |
SJS/TEN |
Supportive care, corticosteroids, antibiotics |
Recovery over 4 weeks |
(10) |
| Allergic diseases |
Ofloxacin gtto. |
Fever, rashes over the palms, oral mucositis |
SJS |
Supportive care, corticosteroids, antibiotics |
Recovery in 30 days |
(11) |
Recent advances in diagnostic technologies have substantially improved the capability to detect SJS/TEN in the early stages. Granulysin, a cytotoxic protein that is markedly elevated in blister fluid and serum during the acute phase, has been a promising biomarker for an early diagnosis (12). While the SCORTEN scoring system remains the most widely adopted tool for mortality risk stratification (13), its predictive accuracy in the context of increasingly comprehensive intensive care and biological therapies requires further evaluation (14). The SCORTEN system incorporates seven independent clinical variables, including age ≥40 years, presence of cancer, >10% epidermal detachment, heart rate ≥120 bpm, blood urea nitrogen >10 mmol/l, serum glucose >14 mmol/l and serum bicarbonate <20 mmol/l. Each criterion scores one point, with the total score ranging from 0 to 7(13).
The present study reports a rare case of levofloxacin-induced SJS/TEN in a patient with colon cancer. This study aims to clarify the importance of an early diagnosis for SJS/TEN and identify the factors influencing prognosis, which may help inform therapeutic strategies in similar cases.
Case report
A 55-year-old male patient was admitted to Hubei Cancer Hospital (Wuhan, China) in June 2024, presenting with a 1-month history of abdominal distension. Colonoscopy revealed a neoplasm occupying three-quarters of the lumen in the ascending colon near the hepatic flexure, covered with feces and opaque liquid. Biopsy confirmed adenocarcinoma. Subsequent positron emission tomography-computed tomography examination demonstrated a malignant tumor of the ascending colon, with retroperitoneal and mesenteric lymph node metastases, as well as the presence of ascites (data not shown). During the initial hospitalization for the management of intestinal obstruction, the patient underwent an urgent double-lumen ileostomy. Considering the patient's documented hypersensitivity to cefmetazole, antimicrobial therapy was initiated with intravenous levofloxacin at a dose of 0.5 g once daily. Postoperatively, the patient experienced intermittent febrile episodes, with peak temperatures reaching 38.5˚C. Lysine aspirin (1.8 g once daily for 3 days) was administered as an antipyretic.
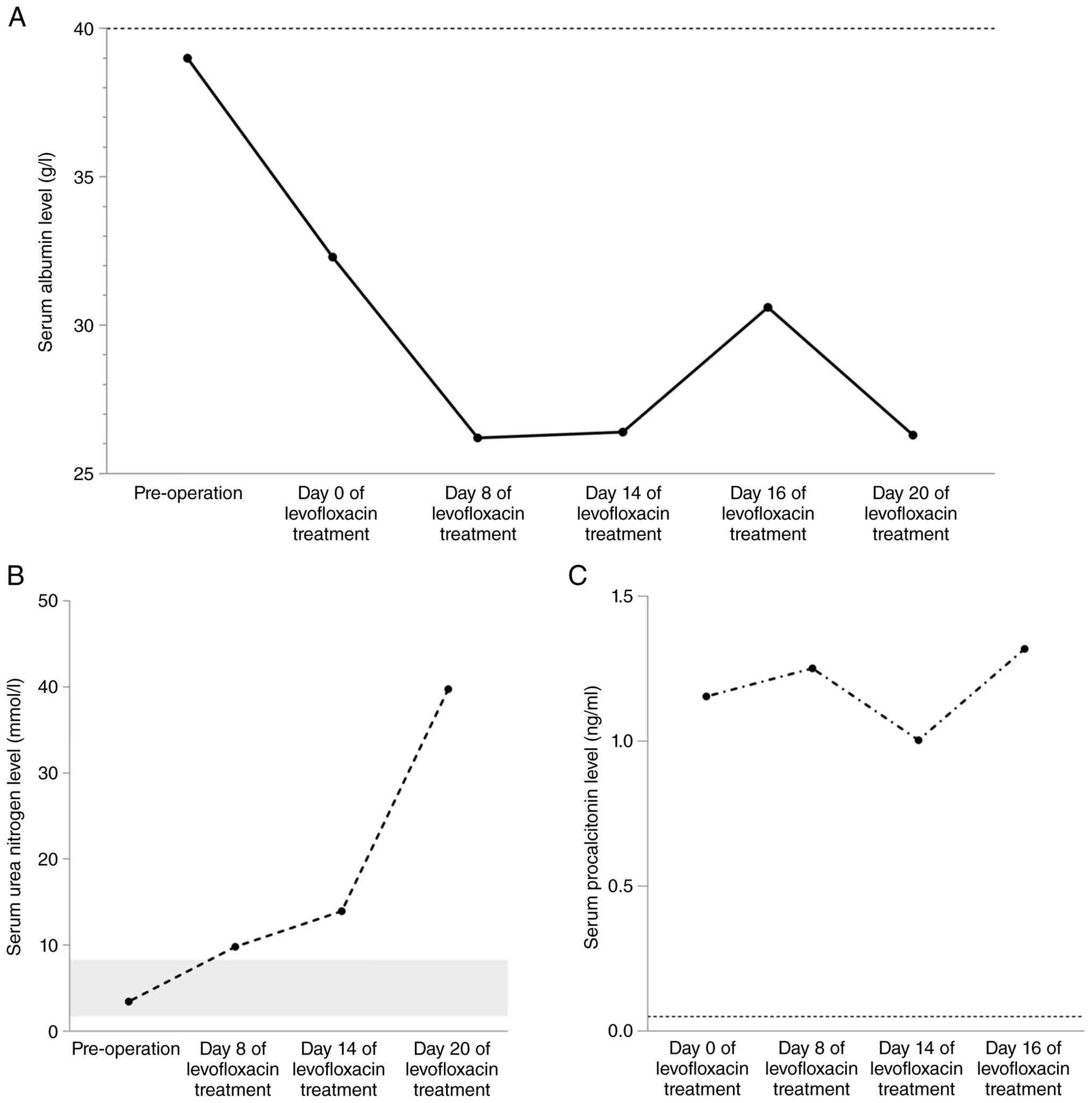
On the third postoperative day, both abdominal drainage fluid and sputum samples were collected and subjected to microbiological examination. At 5 days after submission, the microbiological analysis revealed a negative result for the sputum culture, whereas Enterococcus faecalis was identified in the drainage fluid, exhibiting resistance to levofloxacin. At the same time, the patient developed a widespread erythematous rash affecting the face, neck and upper trunk, along with generalized weakness, oral mucosal ulceration and mild conjunctival hemorrhage. Laboratory findings at this time included marked hypoalbuminemia (serum albumin, 26.2 g/l; reference range, 40-55 g/l), elevated blood urea nitrogen (9.8 mmol/l; reference range, 1.7-8.3 mmol/l) and increased procalcitonin levels (1.252 ng/ml; reference range, <0.05 ng/ml) (Fig. 1). The patient declined a skin biopsy. Considering drug allergic reactions and findings from microbiological testing, the clinical team promptly discontinued levofloxacin and initiated a treatment of dexamethasone (10 mg once daily for 6 days) and promethazine (25 mg once daily for 6 days) to manage the hypersensitivity reaction. At this stage, the SCORTEN score was 2, determined according to the patient's age (>40 years) and the presence of cancer (Table II).
|
Table II
SCORTEN score and ABCD-10 score of the present case.
|
Table II
SCORTEN score and ABCD-10 score of the present case.
| |
8 Days after levofloxacin |
14 Days after levofloxacin |
| Criterion |
SCORTEN score |
ABCD-10 score |
SCORTEN score |
ABCD-10 score |
| Age, years |
|
|
|
|
| ≥40 |
1 |
- |
1 |
- |
| ≥50 |
- |
1 |
- |
1 |
| Presence of cancer |
1 |
2 |
1 |
2 |
| >10% TBSA involved |
0 |
0 |
1 |
1 |
| Tachycardia ≥120 bmp |
0 |
- |
0 |
- |
| Urea nitrogen >10 mmol/l |
0 |
- |
1 |
- |
| Glycemia >14 mmol/l |
0 |
- |
0 |
- |
| Serum bicarbonate <20 mmol/l |
0 |
0 |
0 |
0 |
| Dialysis before presentation |
- |
0 |
- |
0 |
| Total score |
2 |
3 |
4 |
4 |
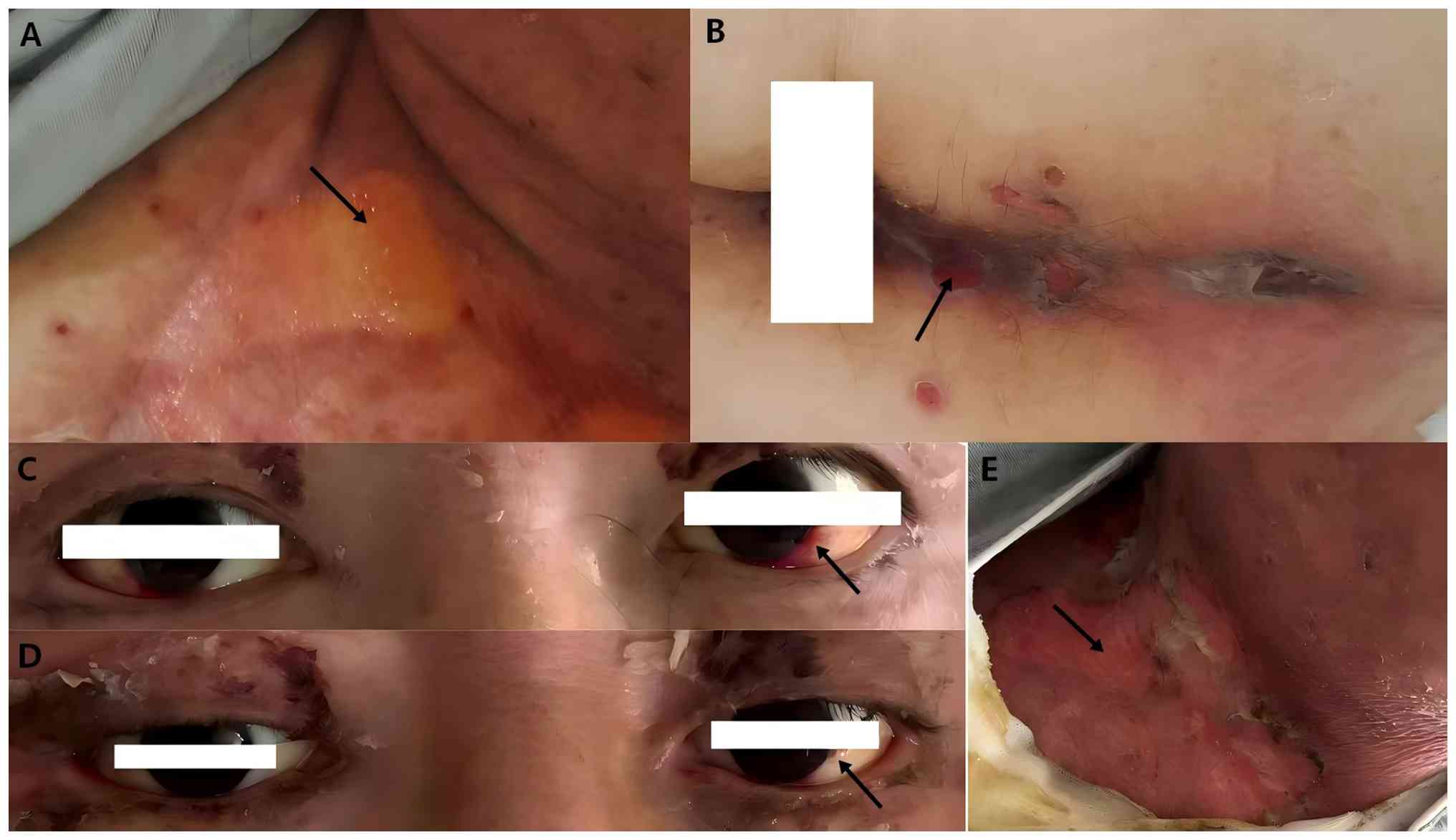
Following an additional 6-day period, the patient's skin condition not only failed to improve but also deteriorated notably, as evidenced by the development of central blisters within erythematous rashes and the presence of Nikolsky's sign (Fig. 2A). As the clinical course progressed, and possibly due to insufficient early corticosteroid therapy before the diagnosis of Stevens-Johnson syndrome (SJS), new erosive lesions appeared around the perianal and scrotal regions (Fig. 2B), while conjunctival hyperemia progressively worsened (Fig. 2C). Serial laboratory testing revealed persistent hypoalbuminemia (26.4 g/l), worsening azotemia (urea nitrogen, 13.94 mmol/l) and a sustained elevation of procalcitonin (1.004 ng/ml) (Fig. 1). Due to the increased blood urea nitrogen and the expansion of the total body surface area, the SCORTEN score increased to 4 (Table II). Based on ALDEN scoring (15) (levofloxacin: 6, ‘very likely’; lysine aspirin: 0, ‘unlikely’), a dermatological consultation confirmed that levofloxacin was the culprit drug for the diagnosis of SJS.
In view of the progressive deterioration of skin symptoms and the presence of purulent secretions, along with the prior antibiotic test results, the patient was administered methylprednisolone (1.5 mg/kg/day), vancomycin (0.5 g every 12 h) and intravenous immunoglobulin (5 g/day). This treatment regimen resulted in a slight improvement in the conjunctival hyperemia (Fig. 2D). However, 4 days later, the syndrome recurred, accompanied by progressive worsening of the epidermal detachment (Fig. 2E). Follow-up laboratory tests showed a substantial increase in serum urea nitrogen levels to 39.77 mmol/l (reference range, 1.7-8.3 mmol/l) (Fig. 1), which is a critical prognostic factor associated with disease severity and clinical outcomes.
The patient's clinical course was complicated by the onset of melena, prompting an urgent transfer from the specialized cancer hospital to Hubei General Hospital (Wuhan, China) for multidisciplinary management. Despite aggressive intensive care and interventions, the patient developed septic shock and subsequently progressed to multiple organ dysfunction syndrome, resulting in death within 1 week.
Discussion
SJS/TEN frequently presents with non-specific symptoms, including fever, ocular irritation, flu-like symptoms and cutaneous discomfort (16). Acute episodes of SJS/TEN are characterized by irregularly shaped, painful erythematous lesions with central blisters, indistinct borders and rapid coalescence. This progression typically results in extensive epidermal detachment and a positive Nikolsky sign (17,18). Mucosal involvement is a defining feature, commonly affecting the eyes, oral cavity, nasal passages and genital regions. Gastrointestinal mucosal injury, including ulceration, erosion and congestion, may also occur, occasionally presenting as symptoms such as hematochezia or diarrhea (19).
SJS/TEN is classified as type IVc hypersensitivity. Histologically, it is distinguished by keratinocyte apoptosis or necrosis (20). This reaction occurs when T cell receptors recognize drug antigens or metabolites presented via human leukocyte antigen (HLA). Type IVc hypersensitivity mainly induces target cell death by cytotoxic T cells (CTL), releasing cytokines such as granulysin, granzyme B and perforin, or through direct interaction of Fas/FasL. This cascade induces keratinocyte apoptosis and varying degrees of epidermal necrosis, which are hallmarks of SJS/TEN (5,20,21).
The progression of symptoms in the present patient, characterized by initial non-specific manifestations that gradually evolved into extensive epidermal detachment (affecting 16% of the total body surface area), highlights the diagnostic challenges associated with SJS/TEN. According to the ALDEN scoring system (15), the optimal interval between initial drug exposure and the onset of reaction ranges from 5 to 28 days. In the present case, the patient developed skin eruptions on the eighth day after starting levofloxacin, which falls with this high-risk timeframe. Moreover, granulysin has been recognized as a critical mediator of keratinocyte apoptosis in SJS/TEN, with serum levels reportedly rising 2 to 4 days prior to the appearance of clinical symptoms (22). The early detection of serum granulysin, particularly at the onset of non-specific fever or flu-like prodromal symptoms, may facilitate a timely diagnosis and intervention. The development of rapid immunochromatographic assays for granulysin represents an important advancement, offering the potential for preventive measures before extensive epidermal detachment occurs (23). Nevertheless, routine clinical application of granulysin detection in CTL-induced severe disorders has yet to gain widespread adoption (24). In the present case, granulysin was not measured, mainly since the patient displayed rapid clinical progression; by the time SJS/TEN was diagnosed, the disease had already advanced, limiting the diagnostic value of granulysin testing at that stage.
The primary treatment for SJS/TEN centers on comprehensive supportive care, which includes wound management, nutritional support, and systemic therapies such as high-dose corticosteroids, intravenous immunoglobulins, cyclosporine and TNF-α inhibitors (20). However, managing SJS/TEN in patients with cancer presents unique challenges, particularly concerning the use of high-dose corticosteroids. Although these agents remain a cornerstone of treatment, their immunosuppressive effects must be carefully balanced against the risk of secondary infections in immunocompromised patients. A prospective study involving 64 patients with SJS/TEN demonstrated that serum granulysin levels increase during the early and acute phases of skin toxicity and decrease during recovery (12). This suggests that granulysin can serve as an ideal biomarker for guiding the tapering or discontinuation of immunosuppressive therapy, potentially reducing complications such as infections and disseminated intravascular coagulation.
While the SCORTEN score is still widely used as a prognostic tool for SJS/TEN, its predictive accuracy may be compromised by advancements in supportive care. The recently proposed ABCD-10 score (25), which incorporates renal dysfunction parameters, was developed to enhance prognostic accuracy in SJS/TEN. Nevertheless, its superiority over the established SCORTEN system remains controversial (26). According to previous studies, the SCORTEN system has demonstrated better performance than the ABCD-10 system in predicting mortality among patients with epidermal necrolysis, although there is evidence of time-associated deterioration in the calibration, leading to an overestimation of mortality risk (26,27). Specifically, in the present study, the SCORTEN score was calculated at the onset of skin lesions (score=2) and after disease progression (score=4). The corresponding predicted mortality risks were 12.1 and 58.3%, respectively, according to the original SCORTEN publication (13). In this case, given that renal dialysis was not performed, the primary distinction between the SCORTEN and ABCD-10 scoring systems was the allocation of points for malignancy: SCORTEN assigns 1 point for the presence of cancer, whereas ABCD-10 assigns 2 points (Table II). Some studies suggest that malignant tumors and certain autoimmune skin diseases may contribute to the development of secondary capillary leak syndrome (28-30). In patients with SJS/TEN, the skin and mucosal surfaces act as open wounds, leading to substantial fluid loss, protein depletion and edema (31). Consequently, malignant ascites and hypoalbuminemia may serve as potential prognostic indicators, underscoring the critical need for malignancy-specific risk stratification tools.
The present study has several limitations that warrant careful consideration. Firstly, the single-case design restricts the generalizability of the findings, although the detailed documentation of clinical progression provides valuable insights. Secondly, the level of granulysin was not measured in this case, and further exploration of its potential role in guiding treatment decisions is warranted. Lastly, the complicated relationship between malignancy-associated immune dysregulation and adverse drug reactions necessitates more comprehensive research.
In addition to antibiotics, antiepileptics, allopurinol and antiviral agents have also been associated with severe cutaneous adverse reactions (SCARs). Accumulating evidence suggests that these adverse reactions are closely linked to pharmacogenomics (32). For example, Chung et al (33) first reported in 2004 that HLA-B*15:02 may serve as a genetic marker for carbamazepine-induced SJS/TEN. Building on this finding, it was further identified that HLA-B*58:01 is associated with allopurinol-induced SCARs in various Asian populations (5,34). Lonjou et al (35) demonstrated that HLA-B*38 is linked to sulfamethoxazole-induced SJS/TEN in European individuals, while HLA-B*35:05 and HLA-Cw*04:01 were found to be associated with nevirapine-induced SJS/TEN in Thai and African individuals, respectively (36,37).
Therefore, future research should focus on developing malignancy-specific risk prediction models that incorporate biomarkers such as granulysin. Additionally, integrating pharmacogenomic testing into routine clinical practice may enhance the ability to prevent severe cutaneous adverse reactions in susceptible individuals.
In conclusion, early and accurate diagnosis is essential for optimizing therapeutic outcomes in SJS/TEN. The results indicate that malignant ascites and hypoalbuminemia may serve as prognostic indicators in patients with SJS/TEN and abdominal malignancies. These findings warrant validation in future large-scale, multicenter studies.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
YZ conceived the study, collected, analyzed and interpreted the data, and drafted the manuscript. GH analyzed the data, produced the graphs and revised the manuscript. HL designed and supervised the study and reviewed the manuscript. YZ and HL confirm the authenticity of all the raw data. All authors have read and approved the final version of the manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the patient before death for the publication of the study and any potentially identifiable images or data, specifically including images showing the face.
Competing interests
The authors declare that they have no competing interests.
References
|
1
|
Lee EY, Knox C and Phillips EJ: Worldwide prevalence of antibiotic-associated Stevens-Johnson syndrome and toxic epidermal necrolysis: A systematic review and meta-analysis. JAMA Dermatol. 159:384–392. 2023.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Martinez Villarreal JD, Cardenas-de la Garza JA, Ionescu MA, Tatu AL, Busila C, Mokni M, Medina LMS, Jasso SMD, Poletti ED and Tomecki KJ: Stevens-Johnson syndrome and toxic epidermal necrolysis: A review of current management and innovative therapies. Int J Dermatol. 64:1164–1172. 2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Martinez JD, Cardenas JA, Soria M, Saenz LM, Estrada K, Delgado SM, Ionescu MA, Busila C and Tatu AL: Role of silver nitrate spray for skin wound care in patients with toxic epidermal necrolysis: our experience in 4 patients. Life (Basel). 13(2341)2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Bellón T: Mechanisms of severe cutaneous adverse reactions: Recent advances. Drug Safety. 42:973–992. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Chu MT, Chang WC, Pao SC and Hung SI: Delayed Drug hypersensitivity reactions: Molecular recognition, genetic susceptibility, and immune mediators. Biomedicines. 11(177)2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Arora R, Pande RK, Panwar S and Gupta V: Drug-related Stevens-Johnson syndrome and toxic epidermal necrolysis: A review. Indian J Crit Care Med. 25:575–579. 2021.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Cravens MG, Sherman N and Sawaya J: Ciprofloxacin-induced Stevens-Johnson syndrome with grapefruit juice consumption: A case report. Cureus. 11(e3827)2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Das A, Banerjee A and Tripathy K: Topical moxifloxacin-induced Stevens-Johnson syndrome. J Cataract Refract Surg. 43:860–861. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dhavaleshwar A, Nayak V, Hande M and Pai R: Topical moxifloxacin-induced toxic epidermal necrolysis and Stevens-Johnson syndrome. J Postgrad Med. 65:125–126. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Memon S, Ahmed N, Nasir Memon M, Zahoor F and Afzal G: Linezolid and ciprofloxacin-induced SJS/TEN (Stevens-Johnson syndrome/toxic epidermolysis necrosis) overlap in a patient with borderline personality disorder during a single hospital stay: A difficult case to manage. Cureus. 15(e39242)2023.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Shaw B, Madden M, Crespo A, Madruga M and Carlan SJ: A rare case of severe Stevens-Johnson syndrome secondary by topical ofloxacin. Am J Case Rep. 24(e941992)2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Chung WH, Hung SI, Yang JY, Su SC, Huang SP, Wei CY, Chin SW, Chiou CC, Chu SC, Ho HC, et al: Granulysin is a key mediator for disseminated keratinocyte death in Stevens-Johnson syndrome and toxic epidermal necrolysis. Nat Med. 14:1343–1350. 2008.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Bastuji-Garin S, Fouchard N, Bertocchi M, Roujeau JC, Revuz J and Wolkenstein P: SCORTEN: A severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol. 115:149–153. 2000.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Torres-Navarro I, Briz-Redón Á and Botella-Estrada R: Accuracy of SCORTEN to predict the prognosis of Stevens-Johnson syndrome/toxic epidermal necrolysis: A systematic review and meta-analysis. J Eur Acad Dermatol Venereol. 34:2066–2077. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Sassolas B, Haddad C, Mockenhaupt M, Dunant A, Liss Y, Bork K, Haustein UF, Vieluf D, Roujeau JC and Le Louet H: ALDEN, an algorithm for assessment of drug causality in Stevens-Johnson Syndrome and toxic epidermal necrolysis: Comparison with case-control analysis. Clin Pharmacol Ther. 88:60–68. 2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Duong TA, Valeyrie-Allanore L, Wolkenstein P and Chosidow O: Severe cutaneous adverse reactions to drugs. Lancet. 390:1996–2011. 2017.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Mockenhaupt M: Severe drug-induced skin reactions: Clinical pattern, diagnostics and therapy. J Dtsch Dermatol Ges. 7:142–162. 2009.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Roujeau JC, Allanore L, Liss Y and Mockenhaupt M: Severe cutaneous adverse reactions to drugs (SCAR): Definitions, diagnostic criteria, genetic predisposition. Dermatol Sinica. 27:203–209. 2009.
|
|
19
|
Harr T and French LE: Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis. 5(39)2010.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Hung SI, Mockenhaupt M, Blumenthal KG, Abe R, Ueta M, Ingen-Housz-Oro S, Phillips EJ and Chung WH: Severe cutaneous adverse reactions. Nat Rev Dis Primers. 10(30)2024.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Mockenhaupt M: The current understanding of Stevens-Johnson syndrome and toxic epidermal necrolysis. Expert Rev Clin Immunol. 7:803–815. 2011.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Abe R, Yoshioka N, Murata J, Fujita Y and Shimizu H: Granulysin as a marker for early diagnosis of the Stevens-Johnson syndrome. Ann Intern Med. 151:514–515. 2009.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Fujita Y, Yoshioka N, Abe R, Murata J, Hoshina D, Mae H and Shimizu H: Rapid immunochromatographic test for serum granulysin is useful for the prediction of Stevens-Johnson syndrome and toxic epidermal necrolysis. J Am Acad Dermatol. 65:65–68. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Chen CB, Kuo KL, Wang CW, Lu CW, Chung-Yee Hui R, Lu KL, Chang WC, Chen WT, Yun F, Teng YC, et al: Detecting lesional granulysin levels for rapid diagnosis of cytotoxic T lymphocyte-mediated bullous skin disorders. J Allergy Clin Immunol Pract. 9:1327–1337.e3. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Noe MH, Rosenbach M, Hubbard RA, Mostaghimi A, Cardones AR, Chen JK, Cotliar J, Davis MDP, Dominguez A, Fox LP, et al: Development and validation of a risk prediction model for in-hospital mortality among patients with Stevens-Johnson syndrome/toxic epidermal necrolysis-ABCD-10. JAMA Dermatol. 155:448–454. 2019.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Koh HK, Fook-Chong S and Lee HY: Assessment and comparison of performance of ABCD-10 and SCORTEN in prognostication of epidermal necrolysis. JAMA Dermatol. 156:1294–1299. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Duplisea MJ, Roberson ML, Chrisco L, Strassle PD, Williams FN and Ziemer CM: Performance of ABCD-10 and SCORTEN mortality prediction models in a cohort of patients with Stevens-Johnson syndrome/toxic epidermal necrolysis. J Am Acad Dermatol. 85:873–877. 2021.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Druey KM, Arnaud L and Parikh SM: Systemic capillary leak syndrome. Nat Rev Dis Primers. 10(86)2024.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Tomai RA, Oancea A, Tomuleasa C and Dima D: Capillary leak syndrome associated with anaplastic T cell lymphoma and transcutaneous exudation: An unusual presentation. Diagnostics (Basel). 14(1924)2024.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Wen J, Xu J, Ji J, Zhang W, Zheng Q, Liu T, Zheng Y and Ma H: Intravascular large B-cell lymphoma as a covert trigger for hemophagocytic lymphohistiocytosis complicated with capillary leak syndrome: A case report and literature review. Front Immunol. 15(1403376)2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Bunker CB and Chapman AB: SCORTEN in SJS/TEN: Hypoalbuminaemia and oedema. J Eur Acad Dermatol Venereol. 35(e369)2021.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Mokbel K, Weedon M and Jackson L: Pharmacogenomic determinants of adverse drug effects: A systematic review and meta-analysis. In Vivo. 38:2098–2106. 2024.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Chung WH, Hung SI, Hong HS, Hsih MS, Yang LC, Ho HC, Wu JY and Chen YT: Medical genetics: A marker for Stevens-Johnson syndrome. Nature. 428(486)2004.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Hung SI, Chung WH, Liou LB, Chu CC, Lin M, Huang HP, Lin YL, Lan JL, Yang LC, Hong HS, et al: HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci USA. 102:4134–4139. 2005.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Lonjou C, Borot N, Sekula P, Ledger N, Thomas L, Halevy S, Naldi L, Bouwes-Bavinck JN, Sidoroff A and de Toma C: A European study of HLA-B in Stevens-Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs. Pharmacogenet Genomics. 18:99–107. 2008.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Chantarangsu S, Mushiroda T, Mahasirimongkol S, Kiertiburanakul S, Sungkanuparph S, Manosuthi W, Tantisiriwat W, Charoenyingwattana A, Sura T, Chantratita W and Nakamura Y: HLA-B*3505 allele is a strong predictor for nevirapine-induced skin adverse drug reactions in HIV-infected Thai patients. Pharmacogenet Genomics. 19:139–146. 2009.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Carr DF, Bourgeois S, Chaponda M, Takeshita LY, Morris AP, Castro EMC, Alfirevic A, Jones AR, Rigden DJ, Haldenby S, et al: Genome-wide association study of nevirapine hypersensitivity in a sub-Saharan African HIV-infected population. J Antimicrob Chemother. 72:1152–1162. 2017.PubMed/NCBI View Article : Google Scholar
|