Introduction
Immune checkpoint inhibitors (ICIs) exert their
antitumor effects through the blockade of inhibitory immune
checkpoints, thereby reactivating T-cell-mediated immune responses
against malignant cells (1). Their
increasing clinical application has markedly improved survival
outcomes in patients with advanced colorectal cancer, with a median
progression-free survival time of 39.3 months for monotherapy
(2). However, this therapeutic
progress is accompanied by the growing recognition of
immune-related adverse events (irAEs) as notable clinical
complications (3). irAEs can
affect almost any organ system, with dermatologic, gastrointestinal
and hepatic toxicities being among the most common manifestations
(4). By contrast, urinary tract
irAEs are relatively rare, with immune-related acute kidney injury
occurring in ~2.2-5.0% of patients. Furthermore, immune-mediated
ureteritis and cystitis are also uncommon and have only been
reported in isolated case reports (5-7).
Currently, the prescribing information for cadonilimab and
adebrelimab does not list ureteritis or cystitis as recognized
adverse effects, increasing the likelihood of clinical
under-recognition and delayed intervention (8). In addition, existing guidelines from
the National Comprehensive Cancer Network (NCCN) and the European
Society for Medical Oncology (ESMO) do not offer specific
recommendations for the diagnosis or management of immune-related
ureteritis or cystitis (9,10), creating a key gap in guidance for
clinicians. The present case report outlines a rare case of
pan-urinary tract irAEs manifesting as concurrent nephritis,
ureteritis and cystitis in a patient with advanced colorectal
cancer following sequential ICI therapy. The present comprehensive
report aims to provide a reference for clinical treatment and
management of these unusual irAEs.
Case report
In 2015, the present patient, a 62-year-old male,
was initially diagnosed with colon cancer and underwent a left
hemicolectomy at the Department of General Surgery, Shanghai East
Hospital (Shanghai, China), followed by 6 cycles of adjuvant
chemotherapy (regimen unspecified). Post-treatment surveillance
indicated stable disease.
In January 2020, a PET/CT scan revealed metastatic
lesions in the liver, leading to a right hepatectomy, lysis of
intestinal adhesions and cholecystectomy at the Department of
Hepatobiliary Surgey, Shanghai East Hospital (Shanghai, China).
Histopathological examination demonstrated moderately
differentiated adenocarcinoma consistent with metastatic colorectal
cancer. Immunohistochemical profiling of the liver metastasis
showed cytokeratin 20+, Ki-67 (20%+),
HER2-, MutL homolog 1+, MutS homolog
(MSH)-2-, MSH6-, PMS1 homolog 2-,
CDX2+ and carcinoembryonic antigen (CEA)+,
demonstrating mismatch repair deficiency. From May 2020, the
patient completed 6 cycles of adjuvant XELOX chemotherapy
(oxaliplatin + capecitabine) in the Department of Oncology,
Changzhou Tumor Hospital (Changzhou, China) with subsequent
follow-ups exhibiting continued disease stability. However, in
April 2022, an abdominal CT scan revealed radiographic evidence of
disease progression. The patient then received 6 cycles of
bevacizumab in combination with XELOX, followed by maintenance
therapy with bevacizumab and capecitabine. The medical history of
the patient included chronic hepatitis B infection, essential
hypertension and a history of smoking. The patient exhibited no
other marked chronic comorbidities. Baseline laboratory assessments
exhibited a urine white blood cell (WBC) count of 0.9/µl (reference
range: 0-25/µl) and red blood cell (RBC) count of 7.3/µl (reference
range: 0-23/µl). The serum creatinine level was 69.8 µmol/l
(reference range: 57-111 µmol/l) and creatinine clearance was
calculated at 127.8 ml/min. Baseline imaging of the urinary system
revealed no abnormalities in the kidneys, ureters or bladder.
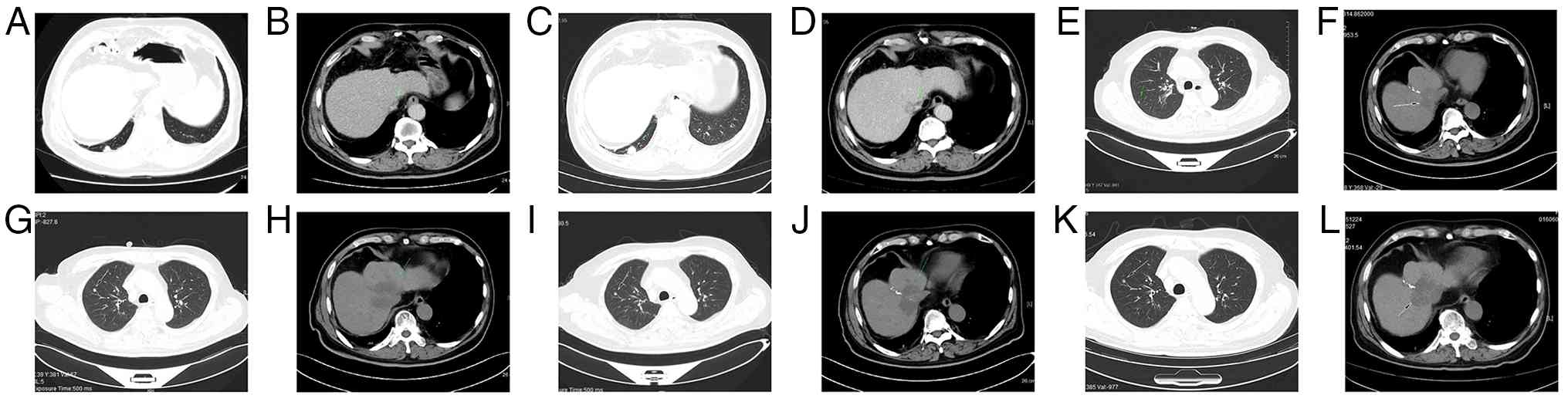
In January 2024, a routine surveillance chest and
abdominal CT scan revealed progression of bilateral pulmonary
metastases (Fig. 1A and B). As a result, the patient commenced
immunotherapy with tislelizumab (200 mg on day 1) in combination
with regorafenib (160 mg orally, once daily from days 1-21). The
regimen was well-tolerated, with no marked treatment-related
adverse effects reported. In April 2024, a CT scan showed stable
disease in the patient (Fig. 1C
and D). A further 13 days after
receiving the 14th cycle of tislelizumab (in November 2024), the
patient developed mild lower urinary tract symptoms, including
urinary frequency, urgency and dysuria. These symptoms were
initially attributed to benign prostatic hyperplasia and showed
partial improvement following treatment with tamsulosin and
Traditional Chinese Medicine (Relinqing granules). However, after
the 15th cycle of tislelizumab, urinalysis revealed markedly
elevated WBC (1,515.3/µl) and RBC (237.6/µl) counts. Despite
empirical treatment with levofloxacin, no clinical improvement was
observed and no further targeted interventions were initiated at
that point. In January 2025, due to CT finding indications of
disease progression relative to previous imaging (Fig. 1E and F), the treatment regimen was escalated to
chemo-immunotherapy consisting of cadonilimab (500 mg on day 1),
irinotecan (400 mg on day 2) and capecitabine (1,500 mg twice daily
from days 1-14). A further 9 days after the first administration of
cadonilimab, the patient experienced worsening of lower urinary
tract symptoms, accompanied by gross hematuria. Urine examination
revealed marked pyuria (WBC count: 21,397.4/µl) and hematuria (WBC
count: 1,455.3/µl), accompanied by acute kidney injury (serum
creatinine: 299.0 µmol/l). Despite these findings, complete blood
counts and inflammatory markers including WBC count, C-reactive
protein and procalcitonin remained within the normal limits.
Repeated urine cultures consistently returned negative results
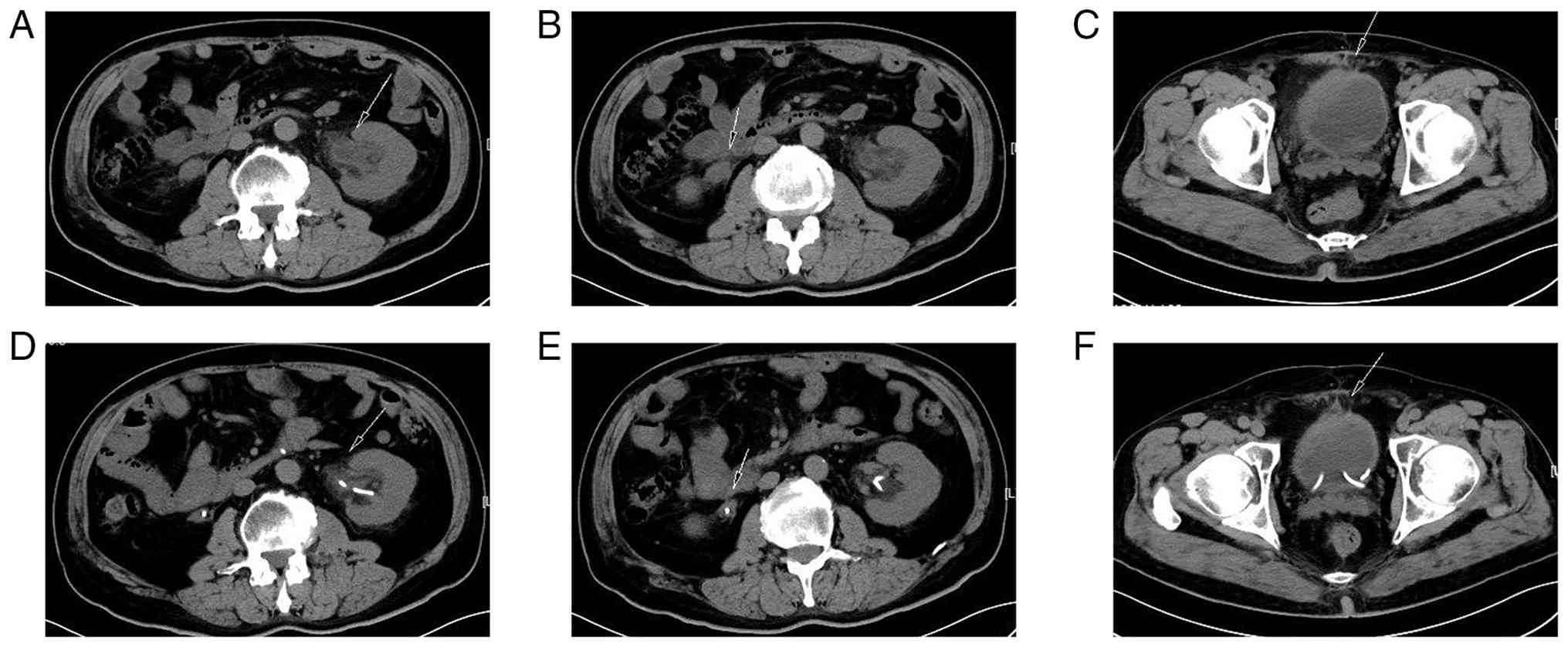
throughout the observation period. Abdominal CT imaging revealed
bilateral hydroureteronephrosis and diffuse thickening of both
ureteral and bladder walls (Fig.
2A-C). Due to marked thrombocytopenia, invasive diagnostic
procedures such as cystoscopy and renal biopsy were too high-risk
owing to an elevated chance of bleeding. Despite immunotherapy
being temporarily withheld and the patient being treated
empirically with piperacillin-tazobactam, there was no marked
clinical improvement in genitourinary symptoms. Notably, follow-up
urinalyses demonstrated a gradual decline in WBC and RBC counts,
accompanied by normalization of serum creatinine, indicating renal
function recovery. In February 2025, systemic chemotherapy was
discontinued and the patient was transitioned to monotherapy with
carbognilumab. Shortly thereafter, the patient developed recurrent
lower urinary tract symptoms accompanied by a decline in renal
function, with serum creatinine rising to 218.4 µmol/l. Urine
culture determined the presence of Escherichia coli and
although targeted antibiotic therapy was initiated, the symptoms
remained unresponsive. As a result, immunotherapy was temporarily
halted, leading to a gradual improvement in clinical symptoms. In
March 2025, the patient received a dose of adebrelimab (1,200 mg on
day 1). This was followed by a recurrence of lower urinary tract
symptoms and the development of bilateral hydronephrosis. Bilateral
ureteral stent placement was performed, which led to improved renal
function. In April 2025, CT scan showed tumor progression but no
further anti-tumor treatment was administered due to irAEs
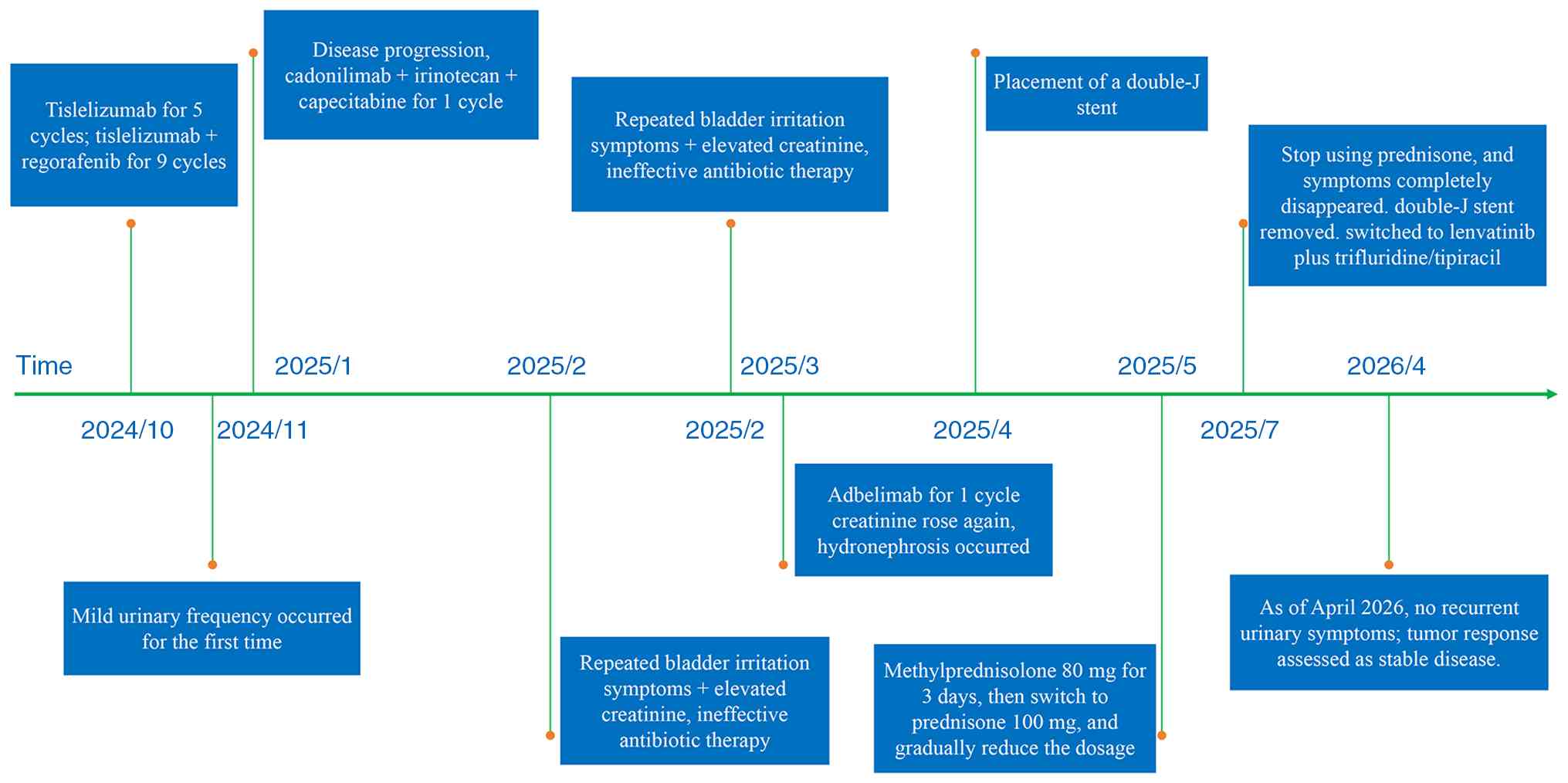
(Fig. 1G and H). The antineoplastic treatment course of
the patient and the occurrence of urinary irAEs is summarized in
Fig. 3. Following a
multi-disciplinary treatment (MDT) meeting, a provisional diagnosis
of ICIs-related urinary irAEs was established. According to the
Common Terminology Criteria for Adverse Events, the patient was
classified as immune-related nephritis (grade 3) and immune-related
ureteritis/cystitis (grade 3) (11).
In May 2025, methylprednisolone treatment was
initiated at 80 mg/day (equivalent to prednisone 1.18 mg/kg/day)
for 3 days, followed by sequential administration of oral
prednisone at 100 mg/day for 2 days. This regimen led to the marked
alleviation of symptoms, with marked improvements in urinary
frequency, urgency, dysuria and gross hematuria, as well as a
return to baseline levels in repeat renal function tests. The
prednisone dosage was subsequently tapered by 20 mg every 3 days
and complete resolution of the bladder irritation symptoms observed
1 week later. In late May, the patient's treatment was changed to
oral prednisone at 30 mg/day, followed by weekly reductions of 5 mg
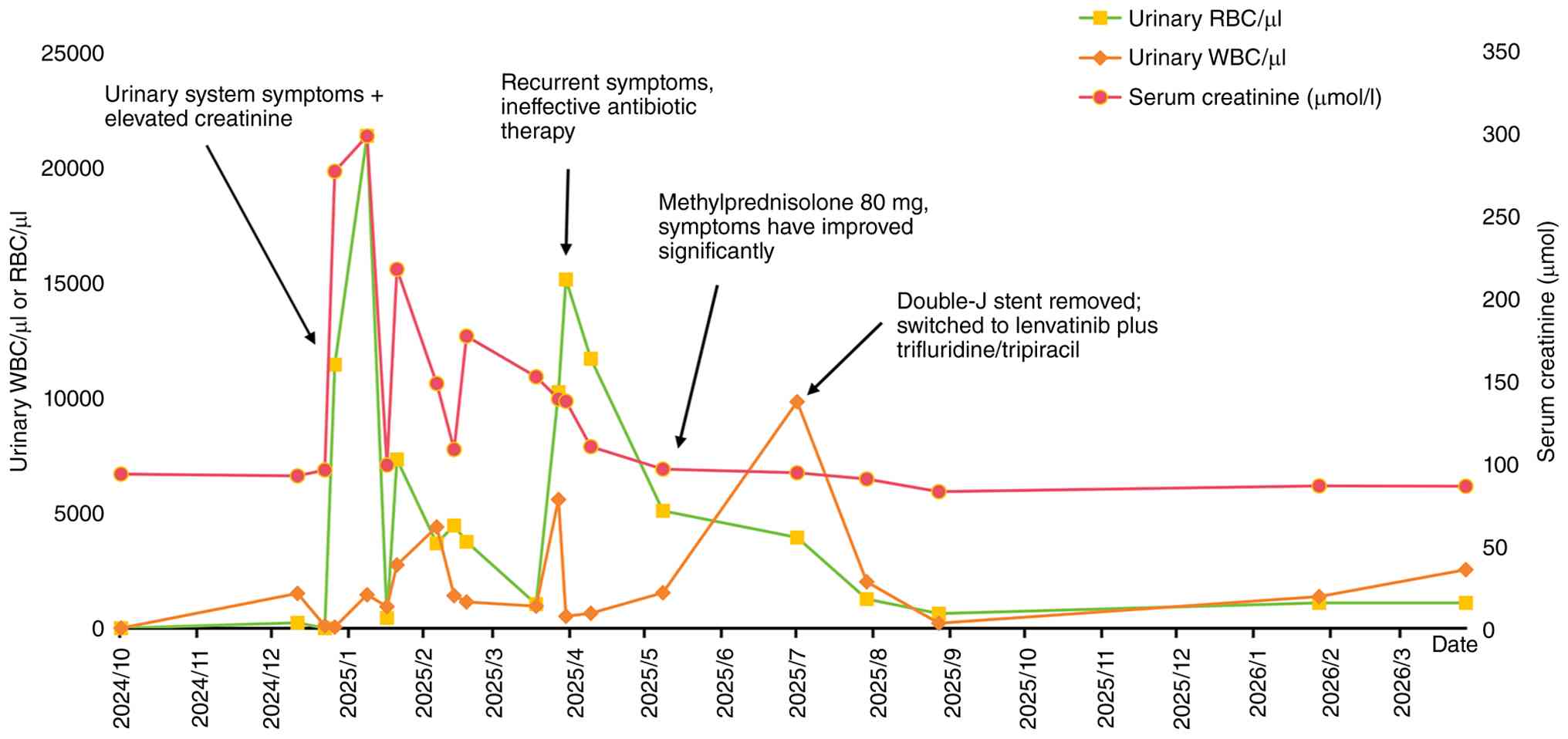
until a maintenance dose of 10 mg/day was reached. The temporal
trends of urinary WBC/RBC counts and serum creatinine throughout
the course of immunotherapy are illustrated in Fig. 4. After 6 weeks of corticosteroid
therapy, follow-up CT imaging of the urinary system exhibited
notable resolution of hydronephrosis and proximal/mid-ureteral
dilation, as well as improvement in bladder wall thickening
(Fig. 2D-F). The stent was removed
on in July 2025, due to potential complications (bladder irritation
and low back pain). After halting immunotherapy, the patient
received lenvatinib + trifluridine/tipiracil. Through comprehensive
evaluation using the Naranjo assessment scale and MDT discussion,
the patient was definitively diagnosed with ICI-related
nephritis/ureteritis/cystitis (12). After recovery from irAEs, the
patient underwent regular follow-up for 1 year. The last laboratory
assessments during follow-up showed a urine white blood cell count
of 1102.6/µl (reference range, 0-25/µl) and a red blood cell count
of 2545.8/µl (reference range, 0-23/µl), and the serum creatinine
level was 71.9 µmol/l (reference range, 57-111 µmol/l) (Fig. 2), with no recurrence of urinary
symptoms such as frequency, urgency or dysuria. Concurrently, as of
December 2025, repeat tumor evaluations showed stable disease
(Fig. 1I-L). From 2026 onward,
although the patient refused routine CT scans due to personal
financial reasons, the CEA levels remained generally stable,
suggesting that tumor control remained favorable.
Discussion
Within the present report, a case of recurrent
immune-related nephritis, ureteritis and cystitis is reported in a
patient with advanced colorectal cancer who received sequential
treatment with three ICIs (tislelizumab, cadonilimab and
adebrelimab). During the initial combination therapy with
tislelizumab and regorafenib, the patient developed symptoms of
mild lower urinary tract irritation. These symptoms progressed
markedly, along with rising serum creatinine levels after
transitioning to cadonilimab monotherapy, demonstrating a clear
temporal association between drug administration and symptom onset.
Temporary suspension of immunotherapy without corticosteroid
intervention resulted in gradual resolution of urinary symptoms and
normalization of creatinine levels, suggesting that irAEs affecting
the urinary system may demonstrate self-limiting characteristics
(13). However, urinary tract
irritation symptoms re-emerged following subsequent administration
of adebrelimab.
Throughout the 6-month treatment period, serial
urine cultures remained persistently negative, with the exception
of a single episode of Escherichia coli isolation. Notably,
the patient exhibited minimal clinical improvement despite a number
of adjustments in antibiotic therapy. Imaging studies including
abdominal ultrasonography and urinary cytology ruled out
malignancy, urolithiasis and benign prostatic hyperplasia. CT
imaging of the urinary tract revealed bilateral hydronephrosis,
proximal and mid-ureteral dilation, circumferential ureteral wall
thickening and irregularity, as well as diffuse bladder wall
thickening with all findings consistent with extensive urinary
tract inflammation. Symptom resolution following corticosteroid
administration, in conjunction with clinical, laboratory and
radiographic evidence, determined the diagnosis of immune-related
ureteritis and cystitis. In addition, the patient experienced an
almost 3-fold increase in serum creatinine from baseline at the
onset of urinary symptoms, followed by the development of bilateral
hydronephrosis, suggestive of acute kidney injury. Based on the
absence of a history of dehydration, hemorrhage or cardiac
dysfunction, prerenal causes of acute kidney injury were initially
excluded. Although a renal biopsy could not be performed due to
thrombocytopenia, intrarenal etiologies (renal causes) could not be
definitively ruled out. Imaging evidence of ureteral wall
thickening and dilation suggested functional obstruction, pointing
to a postrenal component of acute kidney injury. However, a
multifactorial mechanism involving both intrinsic renal injury and
postrenal obstruction remains a likely explanation. Notably, the
symptoms and renal function of the patient improved markedly
following glucocorticoid therapy. In the absence of
histopathological evidence, this rapid response may represent
evidence to support immune-mediated kidney injury.
At present, the lack of validated biomarkers or
standardized diagnostic criteria for urinary irAEs necessitates a
diagnosis of exclusion in clinical settings. In this case, the
favorable response of the patient to glucocorticoid therapy
supported the diagnosis of ICI-related nephritis, ureteritis and
cystitis. To assess the causal association between immunotherapy
and the observed urinary irAEs, the Naranjo Adverse Drug Reaction
Probability Scale was applied, evaluating all 10 items according to
established guidelines (Table I).
The patient received a total score of 7, indicating a probable
association between the ICIs and the urinary irAEs. Notably,
ureteritis and cystitis represent atypical manifestations of irAEs
that are not currently listed in the prescribing information for
either cadonilimab or adebrelimab. Given the sequential exposure to
three different ICIs, it is not possible to definitively attribute
the urinary irAEs to a single agent. Instead, it remains plausible
that all three ICIs may have contributed to the development of this
rare complication.
 | Table INaranjo assessment scale of
ICI-related nephritis, ureteritis and cystitis. |
Table I
Naranjo assessment scale of
ICI-related nephritis, ureteritis and cystitis.
| | Standard for
evaluation | |
|---|
| Related issue | Yes | No | Unknown | Score | Justification for
score |
|---|
| Are there previous
conclusive reports on this reaction? | +1 | 0 | 0 | +1 | Mentioned in the
literature |
| Did the adverse event
occur after administration of the suspected drug? | +2 | -1 | 0 | +2 | irAEs developed
following ICI therapy |
| Did the reaction
improve upon discontinuation of the drug or administration of a
specific antagonist? | +1 | 0 | 0 | +1 | Improved after drug
discontinuation |
| Did the adverse
reaction reappear when the drug was readministered? | +2 | -1 | 0 | +2 | Recurred after
switching ICIs |
| Are there other
plausible explanations (unrelated to the drug) that could
independently account for the reaction? | -1 | +2 | 0 | -1 | Urinary tract
infection or tumor |
| Did the reaction
reappear when a placebo was given? | -1 | +1 | 0 | 0 | Placebo not
administered |
| Was the drug present
in the blood or other bodily fluids at concentrations known to be
toxic? | +1 | 0 | 0 | 0 | Not tested |
| Did the severity of
the reaction increase with a higher dose or decrease with a lower
dose? | +1 | 0 | 0 | 0 | No dose adjustment
was made |
| Has the patient
experienced a similar reaction to the same or a related drug in the
past? | +1 | 0 | 0 | +1 | Recurrent episodes
after switching to different ICIs |
| Was the adverse event
determined by any objective evidence? | +1 | 0 | 0 | +1 | Laboratory and
imaging findings |
| Total score | 7 | |
Epidemiological data indicate that irAEs involving
the urinary tract, while rare, are recognized complications of ICI
therapy (14). Among these, renal
irAEs are the most common, with acute interstitial nephritis being
the predominant histopathological finding. Less frequently,
glomerulonephritis and acute tubular necrosis have also been
reported (15). By contrast, irAEs
affecting the ureter and bladder are markedly rare, with existing
evidence limited to isolated case reports. The present case is a
rare instance of simultaneous irAEs involving numerous segments of
the urinary tract including the kidneys, ureters and bladder, an
occurrence that has been scarcely documented in the literature. To
assess the prevalence of such cases, a systematic search of PubMed
(https://pubmed.ncbi.nlm.nih.gov), Web of
Science (https://www.webofscience.com) and the
China National Knowledge Infrastructure (https://www.cnki.net) from inception to March 31,
2025, was conducted, using the following keywords: ‘Immune
checkpoint inhibitors’, ‘immune-related adverse events’,
‘ureteritis’, and ‘cystitis’. The systematic literature review
identified only 5 cases of concurrent acute kidney injury, with
detailed findings summarized in Table
II (13,16-18).
Patients were all male, with ages ranging from 49-72 years, with
males representing 100.0% (6/6) of the cohort. The onset of urinary
irAEs occurred between 2-16 treatment cycles following ICI
initiation, with the majority (5 cases, 83.3%) manifesting within
2-6 cycles. Primary tumors included lung cancer (n=2), gastric
cancer (n=2), esophageal carcinoma (n=1) and colon cancer (n=1).
Among the 6 cases, cystitis was reported in all, ureteritis in 5
cases and nephritis in only 1 case. This uneven distribution likely
reflects both the under-recognition of concurrent nephritis in
patients presenting with ureteritis or cystitis and the absence of
standardized diagnostic criteria for urinary tract irAEs, which may
contribute to inconsistent identification and reporting.
| Table IIClinical profiles of patients with
immune-related nephritis, ureteritis and cystitis reported in the
literature. |
Table II
Clinical profiles of patients with
immune-related nephritis, ureteritis and cystitis reported in the
literature.
| First author,
year | Age/sex | Carcinoma | ICI (no. cycles) | Symptoms | Scr, µmol/l | Urinalysis | Urine culture | Cystoscopy | Imaging
examination | Treatment | Re-challenge | (Refs.) |
|---|
| Ji et al,
2024 | 55/male | Gastric cancer | Sintilimab
(3) | Renal colic
hematuria hydronephrosis | 126.0 | Elevated
WBC/RBC | Negative | Swollen and
ulcerative bladder mucosa | Hydronephrosis,
dilation renal pelvis, thickened ureter wall and bladder wall | Bilateral ureteral
stenting | No | (13) |
| Tu et al,
2021 | 53/male | Lung cancer | Sintilimab
(3) | Haematuria
pollakiuria painful micturition pain | 299.0 | Elevated
WBC/RBC | Negative | Diffused redness of
bladder mucosa | Thickened bladder,
hydronephrosis lower back and dilated ureter | MP, 1
mg/kg/day | No | (16) |
| Li et al,
2023 | 49/male | Esophageal
carcinoma | Tislelizumab
(6) | Gross hematuria
pollakiuria painful micturition lower back pain | 211.0 | Elevated WBC/RBC
and proteinuria 3+ | Negative | Diffused redness of
the bladder mucosa | Mild
hydronephrosis, dilated ureter and thickened bladder wall | MP, 60 mg; symptom
recurrence after rapid dose reduction | No | (17) |
| | 49/male | Gastric cancer | Nivolumab (2) | Hematuria
pollakiuria painful micturition fever | 190.0 | Elevated WBC/RBC
and proteinuria 3+ | Negative | None | Mild
hydronephrosis, dilated ureters and thickened bladder wall | MP, 60 mg; symptom
recurrence after rapid dose reduction | No | |
| Zhang et al,
2024 | 72/male | Lung cancer | Pembroli zumab
(6) | Urinary frequency
nocturia gross hematuria bilateral flank pain | 169.7 | Elevated
WBC/RBC | Negative | Diffuse erythema,
marked local edema and follicular hyperplasia, with floating mucosa
in the bladder | Mild bilateral
hydroureterosis | MP, 40 mg; symptom
recurrence after rapid dose reduction | Yes, failed | (18) |
| Present study | 62/male | Colon cancer | Tislelizumab,
cadonilimab and adebelimab (16) | Pollakiuria urinary
urgency dysuria hematuria | 299.5 | Elevated WBC/RBC
and proteinuria 3+ | Positive | None | Hydronephrosis,
dilated ureter and thickened bladder wall | MP, 100 mg | Yes, failed | - |
A synthesis of previously reported cases, along with
the clinical course of the current patient, highlighted a set of
consistent features: Pollakiuria, urinary urgency, dysuria, gross
hematuria, hydronephrosis, lumbago and elevated serum creatinine
levels. In all documented cases, urine cultures remained sterile
despite marked pyuria and hematuria on urinalysis, suggesting a
non-infectious inflammatory process rather than a conventional
urinary tract infection. It may therefore be proposed that in
patients undergoing ICI therapy, the presence of urinary tract
symptoms with elevated serum creatinine, negative microbiological
testing and poor response to antibiotics should prompt immediate
consideration of immune-related nephritis, ureteritis or cystitis.
The patient exhibited persistent irAEs involving the urinary tract.
All serial urine cultures were found to be sterile, apart from one
Escherichia coli-positive specimen and there was no clinical
improvement following antibiotic therapy, precluding a definitive
differentiation between sterile pyuria and occult infection. When
clinically feasible, it is recommended that metagenomic
next-generation sequencing of the urine be performed in such
patients to further screen for rare pathogens that are undetectable
by conventional culture, thereby reducing the risk of misdiagnosis
and inappropriate glucocorticoid use (19). Cystoscopy in a number of reported
cases revealed diffuse bladder mucosal congestion, while
histopathological findings were characterized by predominant
lymphocytic and neutrophilic infiltration. However, these findings
closely resemble those of conventional cystitis, limiting the
diagnostic specificity of histopathology in distinguishing irAEs
from other inflammatory conditions (16,17).
Cystoscopy or biopsy is not recommended for routine
diagnostic assessment of patients with suspected immune-mediated
cystitis, given the difficulties in distinguishing its inflammatory
features from those of conventional cystitis, as well as the
invasive nature and inherent diagnostic uncertainty of the
procedure (20). The underlying
pathogenesis of irAEs is hypothesized to stem from dysregulated
immune activation, wherein aberrant immune responses mistakenly
target normal tissues, leading to a cascade of inflammatory events.
Although the precise mechanisms of ICI-associated nephro-urinary
toxicity remain unclear, proposed contributing factors include
impaired immune tolerance, abnormal activation of tissue-resident T
cells and autoantibody production, potentially acting
synergistically (21). The present
case is particularly notable for the rare simultaneous involvement
of the kidney, ureter and bladder, as these organs are typically
affected independently by irAEs (22). The concurrent manifestation
suggests the possibility of shared immunological pathways across
urinary tract tissues, though further research is needed to
elucidate the exact mechanistic connections.
Current NCCN and ESMO guidelines do not provide
standardized treatment protocols specifically for immune-related
ureteritis and cystitis. However, both sets of guidelines emphasize
that early initiation of corticosteroid therapy remains an
established method of management for the majority of irAEs. The
clinical guidelines for nephrotoxicity advise permanent
discontinuation of ICIs in cases of grade 3 nephrotoxicity. The
recommended initial corticosteroid regimen should consist of
prednisone or methylprednisolone at 1-2 mg/kg/day or
methylprednisolone pulse therapy at 250-500 mg/day for 3 days. In
addition, urinary protein and serum creatinine levels should be
monitored every 3-7 days. Once the toxicity resolves to grade 1,
corticosteroid administration may be gradually tapered over 4-6
weeks. At present, the key therapeutic goals in managing urinary
irAEs are to preserve renal function and relieve urinary symptoms.
However, the recommended initial dosing and tapering strategies for
immune-mediated ureteritis/cystitis are derived primarily from
individual case studies. In all 6 cases reported, patients
experienced marked improvement in urinary symptoms following
corticosteroid therapy and discontinuation of immunotherapy. This
clinical response was supported by normalization of serum
creatinine and gradual resolution of pyuria and hematuria,
reinforcing the effectiveness of corticosteroids in treating
urinary tract irAEs. In steroid-refractory cases, second-line
immunosuppressive agents such as infliximab (an anti-TNFα
monoclonal antibody) may be considered (23). The majority of cases employed an
initial corticosteroid dose of methylprednisolone at 1-2 mg/kg/day,
which proved effective in controlling symptoms. However, 3 patients
experienced a recurrence of symptoms following rapid corticosteroid
tapering, highlighting the importance of a gradual dose reduction
to prevent recurrence of irAEs (17,18).
Therefore, the present report recommends maintaining corticosteroid
therapy until urinary irAEs resolve to grade 1 severity, followed
by a gradual taper over a minimum of 4-6 weeks to minimize relapse
risk. For grade 3 renal irAEs, NCCN guidelines advise conducting a
careful risk-benefit assessment before considering reinitiation of
ICIs. If renal function normalizes and symptoms improve to grade
≤1, ICIs may be cautiously resumed either without corticosteroids
or with maintenance low-dose prednisone (10 mg/day), preferably
using an alternative ICI class to reduce the risk of recurrence.
Among the cases reviewed, only 1 patient underwent ICI rechallenge,
but re-treatment was unsuccessful, underscoring the marked risk of
therapeutic failure following urinary tract irAEs. Given that the
rechallenge failure rate for grade ≥3 whole-urinary-tract irAEs
appears to be higher compared with that for irAEs affecting other
organs, permanent discontinuation is recommended in accordance with
current guidelines. In the present case, the patient initially
tolerated monotherapy with the programmed cell death protein 1
(PD-1) inhibitor tislelizumab without complications. However,
progression to combination therapy with the PD-1/cytotoxic
T-lymphocyte-associated protein 4 (CTLA-4) bispecific antibody
cadonilimab triggered severe urinary irAEs. Notably, these symptoms
recurred even after switching to a PD-L1 inhibitor (adebrelimab).
The persistence of urinary irAEs despite sequential treatment with
ICIs targeting distinct immune checkpoints suggests that dual
checkpoint blockade may induce a durable or irreversible state of
T-cell hyperactivation. As a result, even subsequent monotherapy
with PD-1 or programmed death-ligand 1 (PD-L1) inhibitors may be
sufficient to provoke marked urinary tract inflammation (24). Previous epidemiological data have
exhibited a notably higher incidence of irAEs with combination
therapy involving PD-1/PD-L1 inhibitors and CTLA-4 inhibitors
compared with PD-1/PD-L1 inhibitors alone (25). The mechanistic basis for this
difference may be because CTLA-4-mediated negative regulation of
the immune response occurs at an early stage of immune activation;
consequently, immune-related toxicities resulting from CTLA-4
inhibition tend to be more severe. This may explain why the present
patient experienced a dramatic escalation of urinary irAEs after
the switch from tislelizumab to cadonilimab. Furthermore, both PD-1
and CTLA-4 are key negative checkpoint regulators of T-cell
activation and their simultaneous blockade may lead to synergistic
activation of the immune response, thereby notably lowering the
threshold for T-cell activation and amplifying the intensity of the
immune response (26). Therefore,
the risk of urinary irAEs cannot be completely excluded in patients
receiving bispecific antibody therapy, even in those who have
previously tolerated anti-PD-1 monotherapy and enhanced monitoring
during treatment is warranted.
To the best of our knowledge, at present, there are
no validated biomarkers to predict the risk or enable early
detection of urinary tract irAEs. Based on the present case
findings and a comprehensive review of the literature, it may bed
concluded that the diagnosis of immune-related nephritis,
ureteritis and cystitis primarily relies on the exclusion of
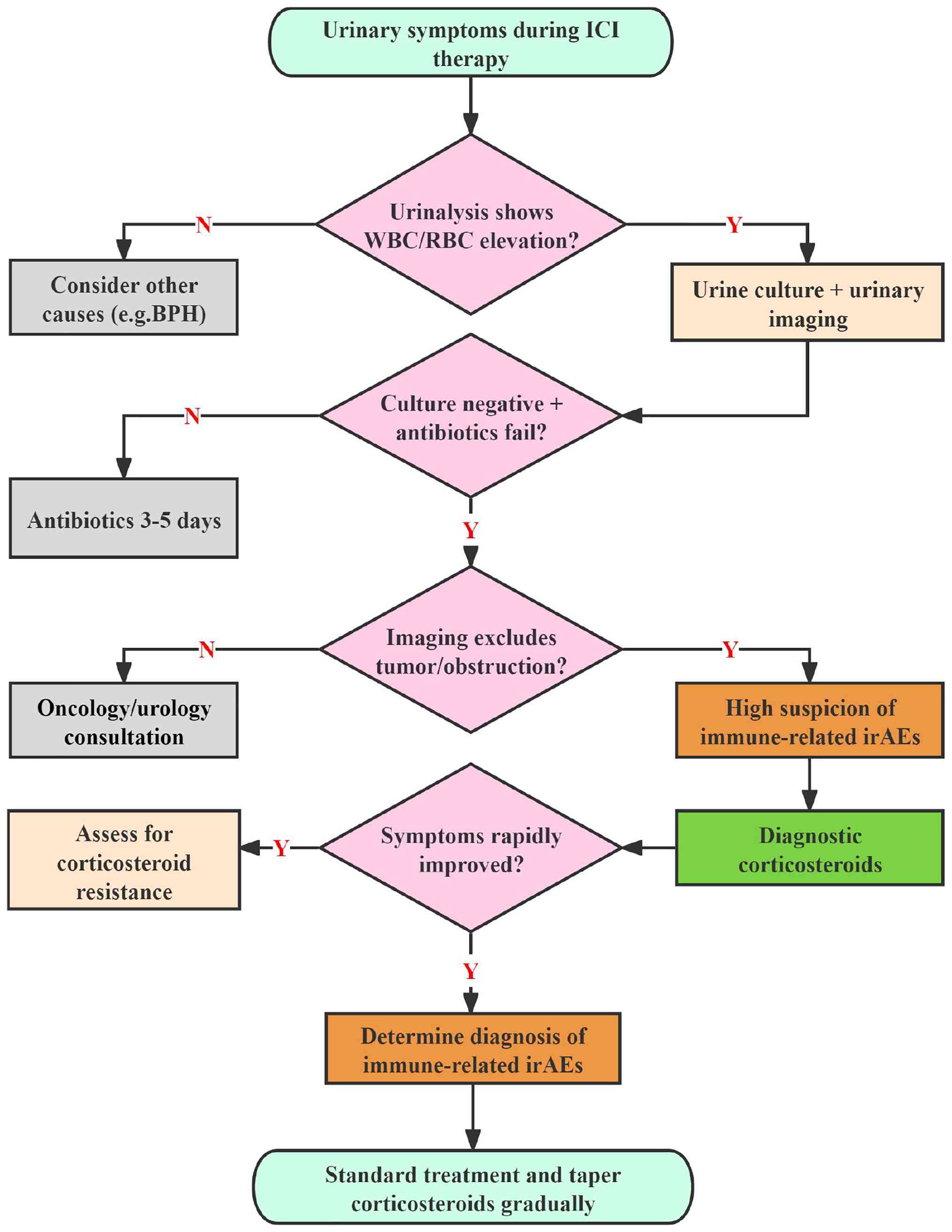
alternative causes. The present evidence-based diagnostic and
therapeutic protocol consists of the following elements: i)
Baseline evaluation: Prior to initiating ICI therapy, patients
should undergo thorough baseline assessments, including urinalysis,
serum creatinine measurement and imaging of the urinary tract; ii)
clinical suspicion: Urinary irAEs should be considered in patients
on ICIs who present with urinary tract irritation symptoms and
renal dysfunction, especially when urine cultures are sterile and
symptoms do not improve with empirical antibiotic treatment; iii)
exclusion of other causes: Diagnostic imaging and cystoscopy are
key in excluding mechanical obstruction, malignancy,
nephrolithiasis or infectious etiologies; iv) timely intervention:
Early recognition and prompt initiation of treatment can reduce the
duration of corticosteroid therapy and help avoid unnecessary use
of antibiotics and analgesics; and v) rechallenge considerations:
Due to the high failure rate of ICI rechallenge, permanent
discontinuation is recommended in cases with grade 3
whole-urinary-tract irAEs. Based on the aforementioned clinical
experience and literature evidence, the present report developed a
diagnostic algorithm for suspected urinary irAEs presented in
Fig. 5.
The present study exhibits a number of important
limitations. First, cadonilimab and adebrelimab were employed as
later-line treatments outside of standard guideline
recommendations, primarily due to limitations in drug
accessibility. Second, thrombocytopenia prevented the timely use of
cystoscopy and renal biopsy in the present patient, resulting in a
lack of histopathological determination for the suspected
immune-related nephro-urinary toxicity.
Overall, although rarely life-threatening,
immune-related nephritis, ureteritis and cystitis often result in
severe urinary symptoms that notably diminish patient quality of
life. At present, there are no standardized guidelines for the
diagnosis and management of immune-related ureteritis and cystitis,
contributing to frequent under-recognition during ICI therapy and
delayed treatment, which may lead to worse clinical outcomes. The
present report outlines a rare case of pan-urinary tract irAEs
following sequential exposure to three different classes of ICIs
and includes a systematic review of similar cases reported in the
literature. In patients receiving ICI therapy who develop urinary
symptoms alongside elevated serum creatinine, a prompt and thorough
diagnostic workup is key. This should include urinalysis, renal
function testing, imaging of the urinary tract, and diagnostic
cystoscopy. After excluding urinary tract infections and
malignancy, the possibility of urinary tract irAEs should be
considered and corticosteroid therapy should be initiated without
delay. The present report outlines the diagnostic rationale and
therapeutic approach for immune-related nephritis, ureteritis and
cystitis, with the aim of facilitating earlier recognition and
appropriate management of these uncommon but impactful
complications.
Acknowledgements
Not applicable.
Funding
Funding: The present study was supported by the Jiangsu
Provincial Health Commission Medical Science Research Project
(grant no. Z2024064) and the Changzhou Science and Technology
Bureau Research Fund (grant no. CJ20229035).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
GZ and SX contributed to the drafting of the
manuscript and the design of the present study. JW and QG performed
a critical literature review and contributed to the acquisition,
analysis and interpretation of data. GZ and MX contributed to the
follow-up and data analysis. YB and MX contributed to the
interpretation of data. YB and MX confirm the authenticity of all
the raw data. All authors read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
The present study was conducted according to the
guidelines of the Declaration of Helsinki and approved by the
Ethics Committee of Changzhou Cancer Hospital (Changzhou, China;
approval no. 2025-SR-NO.022).
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ishida Y, Agata Y, Shibahara K and Honjo
T: Induced expression of PD-1, a novel member of the immunoglobulin
gene superfamily, upon programmed cell death. EMBO J. 11:3887–3895.
1992.PubMed/NCBI View Article : Google Scholar
|
|
2
|
André T, Elez E, Lenz HJ, Jensen LH,
Touchefeu Y, Van Cutsem E, Garcia-Carbonero R, Tougeron D, Mendez
GA, Schenker M, et al: Nivolumab plus ipilimumab versus nivolumab
in microsatellite instability-high metastatic colorectal cancer
(CheckMate 8HW): A randomised, open-label, phase 3 trial. Lancet.
405:383–395. 2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Nasca V, Barretta F, Corti F, Lonardi S,
Niger M, Elez ME, Fakih M, Jayachandran P, Shah AT, Salati M, et
al: Association of immune-related adverse events with the outcomes
of immune checkpoint inhibitors in patients with dMMR/MSI-H
metastatic colorectal cancer. J Immunother Cancer.
11(e005493)2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tang SQ, Tang LL, Mao YP, Li WF, Chen L,
Zhang Y, Guo Y, Liu Q, Sun Y, Xu C and Ma J: The pattern of time to
onset and resolution of immune-related adverse events caused by
immune checkpoint inhibitors in cancer: A pooled analysis of 23
clinical trials and 8,436 patients. Cancer Res Treat. 53:339–354.
2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Seethapathy H, Zhao S, Chute DF, Zubiri L,
Oppong Y, Strohbehn I, Cortazar FB, Leaf DE, Mooradian MJ, Villani
AC, et al: The incidence, causes, and risk factors of acute kidney
injury in patients receiving immune checkpoint inhibitors. Clin J
Am Soc Nephrol. 14:1692–1700. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Cortazar FB, Kibbelaar ZA, Glezerman IG,
Abudayyeh A, Mamlouk O, Motwani SS, Murakami N, Herrmann SM,
Manohar S, Shirali AC, et al: Clinical features and outcomes of
immune checkpoint inhibitor-associated AKI: A multicenter study. J
Am Soc Nephrol. 31:435–446. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ozaki K, Takahashi H, Murakami Y, Kiyoku H
and Kanayama H: A case of cystitis after administration of
nivolumab. Int Cancer Conf J. 6:164–166. 2017.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Gao X, Xu N, Li Z, Shen L, Ji K, Zheng Z,
Liu D, Lou H, Bai L, Liu T, et al: Safety and antitumour activity
of cadonilimab, an anti-PD-1/CTLA-4 bispecific antibody, for
patients with advanced solid tumours (COMPASSION-03): A
multicentre, open-label, phase1b/2 trial. Lancet Oncol.
24:1134–1146. 2023.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Thompson JA, Schneider BJ, Brahmer J, Zaid
MA, Achufusi A, Armand P, Berkenstock MK, Bermas B, Braaten T,
Budde LE, et al: NCCN guidelines® insights: Management
of immunotherapy-related toxicities, version 2.2024. J Natl Compr
Canc Netw. 22:582–592. 2024.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Haanen J, Obeid M, Spain L, Carbonnel F,
Wang Y, Robert C, Lyon AR, Wick W, Kostine M, Peters S, et al:
Management of toxicities from immunotherapy: ESMO clinical practice
guideline for diagnosis, treatment and follow-up. Ann Oncol.
33:1217–1238. 2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Freites-Martinez A, Santana N,
Arias-Santiago S and Viera A: Using the common terminology criteria
for adverse events (CTCAE-version 5.0) to evaluate the severity of
adverse events of anticancer therapies. Actas Dermosifiliogr (Engl
Ed). 112:90–92. 2021.PubMed/NCBI View Article : Google Scholar : (In English,
Spanish).
|
|
12
|
Huang LC, Huang LY, Tseng SY, Hou YM and
Hsiao CC: Amisulpride and symptomatic bradycardia: A case report.
Gen Hosp Psychiatry. 37:497.e1–e2. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ji J, Lai CH, Zhang X and Hu H:
Immune-related adverse events with renal colic as the main
manifestation: A case report of sintilimab-induced
ureteritis/cystitis treated by ureteral stent and review of the
literature. Front Immunol. 15(1501415)2024.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kanz BA, Pollack MH, Johnpulle R, Puzanov
I, Horn L, Morgans A, Sosman JA, Rapisuwon S, Conry RM, Eroglu Z
and Johnson DB: Safety and efficacy of anti-PD-1 in patients with
baseline cardiac, renal, or hepatic dysfunction. J Immunother
Cancer. 4(60)2016.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Meraz-Muñoz A, Amir E, Ng P, Avila-Casado
C, Ragobar C, Chan C, Kim J, Wald R and Kitchlu A: Acute kidney
injury associated with immune checkpoint inhibitor therapy:
Incidence, risk factors and outcomes. J Immunother Cancer.
8(e000467)2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Tu L, Ye Y, Tang X, Liang Z, You Q, Zhou J
and Pan Z: Case report: A case of sintilimab-induced
cystitis/ureteritis and review of sintilimab-related adverse
events. Front Oncol. 11(757069)2021.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Li J, Yu YF, Qi XW, Du Y and Li CQ:
Immune-related ureteritis and cystitis induced by immune checkpoint
inhibitors: Case report and literature review. Front Immunol.
13(1051577)2023.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Zhang P, Yin C and Yang M: Case reports of
immune-related cystitis and the antibody combination hypothesis.
Immunotherapy. 16:1039–1047. 2024.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Jia K, Huang S, Shen C, Li H, Zhang Z,
Wang L, Zhao G, Wu Z, Lin Y, Xia H, et al: Enhancing urinary tract
infection diagnosis for negative culture patients with metagenomic
next-generation sequencing (mNGS). Front Cell Infect Microbiol.
13(1119020)2023.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wang C, Nie M, Liu Y, Qiu W, Zhang Z, Zhou
N, Wang X, Zhao L, Ying H and Bai C: Single-center experience with
immune checkpoint inhibitor-related ureteritis and cystitis. Front
Immunol. 16(1727822)2026.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Kennedy LB and Salama AKS: A review of
cancer immunotherapy toxicity. CA Cancer J Clin. 70:86–104.
2020.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Xiao J, Tang S, Xia Z, Zhou Y and Fang M:
Clinical presentation of PD-1/PD-L1 immune checkpoint inhibitors
induced cystitis. Invest New Drugs. 43:770–779. 2025.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Fukunaga H, Sumii K, Kawamura S, Okuno M,
Taguchi I and Kawabata G: A case of steroid-resistant cystitis as
an immune-related adverse event during treatment with nivolumab for
lung cancer, which was successfully treated with infliximab. IJU
Case Rep. 5:521–523. 2022.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Fan Y, Zhao J, Mi Y and Zhang Z, Geng Y,
Zhou L, Shen L and Zhang Z: Recurrent cystitis associated with 2
programmed death 1 inhibitors: A rare case report and literature
review. J Immunother. 46:341–345. 2023.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Mi Z, Zhang Y, Feng Z, Liu J, Wu J, Tan H,
Ma X, Liu Z and Rong P: Treatment-related adverse events of
PD-1/PD-L1 inhibitors combined with CTLA-4 inhibitors in clinical
trials: A meta-analysis. Artif Cells Nanomed Biotechnol.
50:301–309. 2022.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Larkin J, Chiarion-Sileni V, Gonzalez R,
Grob JJ, Cowey CL, Lao CD, Schadendorf D, Dummer R, Smylie M,
Rutkowski P, et al: Combined nivolumab and ipilimumab or
monotherapy in untreated melanoma. N Engl J Med. 373:23–34.
2015.PubMed/NCBI View Article : Google Scholar
|