Introduction
Colorectal cancer is the third most common cancer globally, having affected >1.9 million individuals in 2020 alone, and is the second most common cause of cancer-related deaths, having claimed 930,000 lives within the same year (1). For colon cancer, oncological segmental colectomy with high vascular ligation is the conventional operation, whereas rectal cancers require more technically demanding procedures such as low anterior resection or ultra-low anterior resection (ULAR). Surgery for rectal cancer is considered more complex than surgery for colon cancer due to the challenging anatomy and the close proximity of key structures such as nerves, blood vessels, pelvic organs and core musculoskeletal boundaries. Total mesorectal excision (TME) has markedly improved outcomes for patients with rectal cancer by ensuring the precise removal of cancerous tissue along with surrounding mesorectal fat, which is key for reducing local recurrence and improving overall survival (OS) (2). Additionally, advancements in procedures such as ULAR have made sphincter-preserving surgery possible for a number of patients (3), allowing for the maintenance of anal sphincter function and an improved quality of life post-surgery. Traditionally, ULAR has been performed through laparotomy, but laparoscopic ULAR has become the preferred method (4), along with the increasing use of robotic surgery (5) in colorectal cancer treatment.
However, low rectal cancer surgery remains a challenging procedure, particularly in patients who are overweight and have a narrow pelvis (6). Transanal TME (TaTME) was introduced, studied and popularized by Sylla et al (7) in 2010 as a new technique that enhanced visualization of the mesorectal plane, leading to higher R0 resection rates, lower rates of positive circumferential resection margins (CRM) and a notable reduction in the risk of anastomotic leakage. A previous meta-analysis summarized TaTME as an effective technique for low rectal cancers, yielding improved surgical margins, higher-quality specimens, improved anastomotic integrity and a lower probability of conversion to laparotomy (8).
Despite positive outcomes demonstrated in the above studies (7,8), the oncological efficacy of TaTME remains controversial. In 2018, the Norwegian Health Authority placed a moratorium on TaTME after national registry data revealed a high local recurrence rate of 9.5% (9). Similarly, a proctorship program in smaller health centres in the Netherlands reported recurrence rates of ~10% (10). The International TaTME Registryreported that 38% of patients who underwent TaTME had tumours located 10-13 cm above the anal verge, with only a 5-cm distal resection margin (11). This may reflect imprecise intraoperative tumour localisation, and it also suggests that dissection extended unnecessarily deep into the pelvis, thereby increasing the risk of nerve injury and functional complications without oncological justification. While these findings highlight the importance of careful patient selection and rigorous surgeon training, TaTME continues to show promise as an effective approach for complex low rectal cancers. Further research and refined protocols may help optimize its oncological safety and expand its applicability in challenging cases.
Given the controversial data, the present study aimed to analyse the oncological and surgical outcomes of patients with low rectal cancer who underwent TaTME with ULAR, compared with those who underwent abdominal ULAR alone, to assess the potential benefits of TaTME. The present study included patient cohorts with a high mean BMI, who are considered more difficult to operate on, to investigate the effectiveness of TaTME in complex cases.
Materials and methods
Study design and setting
A single-centre cohort study at Monash Health Dandenong Hospital (Melbourne, Australia) was conducted evaluating the introduction of TaTME. The TaTME cohort was assembled prospectively, while the comparator cohort comprised patients who underwent ULAR, identified retrospectively from the institutional database. All surgeries were performed by a single team of colorectal surgeons well-experienced in TaTME and ULAR, with assistance by surgeons in training.
Patient selection and eligibility criteria
Eligibility criteria for TaTME with ULAR (TaTME cohort) included patients aged >18 years who had undergone surgery for rectal adenocarcinoma with a tumour stage of ≤III, without evidence of invasion into adjacent organs or structures and located <10 cm from the anal verge. Tumour location was meticulously confirmed using colonoscopy, flexible sigmoidoscopy, rigid sigmoidoscopy and MRI, ensuring precise eligibility for the present study. Patients with rectal neoplastic lesions that were not adenocarcinoma were excluded. Patients in the ULAR cohort (ULAR alone) were selected retrospectively from the Monash Health Dandenong Hospital database. The TaTME cohort included patients treated between July 2018 and December 2021, whereas the ULAR cohort included patients with surgeries performed between January 2011 and June 2018. The study cohort comprised 78 patients, with a mean age of 59 years. The ULAR group (n=59) had a mean age of 60 years and included 52 males and 7 females, while the TaTME group (n=19) had a mean age of 57 years, with 17 males and 2 females. After data collection, patients in the TaTME and ULAR groups were matched using propensity score matching (PSM) to minimize selection bias.
All patients underwent regular postoperative follow-ups according to national guidelines (12). The primary oncological outcomes were progression-free survival (PFS) for the overall cohort, which included patients with stage IV disease according to the American Joint Committee on Cancer staging system (13), and disease-free survival (DFS) for the subgroup analysis, excluding patients with stage IV disease. Secondary outcomes included intraoperative and postoperative complications, and OS.
Ethics approval and consent to participate
In accordance with the Declaration of Helsinki, the present study was approved by the Monash Health Technology/Clinical Practice Oversight Committee (TCOC; approval no. N_18_07; approved July 2018). The approval comprehensively covered both the introduction of the TaTME procedure and the use of patient data for research and publication. Written informed consent for participation and publication was obtained from all prospectively enrolled patients undergoing TaTME. For retrospectively analysed patients who underwent ULAR, the requirement for individual consent was waived under the same TCOC approval.
Neoadjuvant therapy
A total of 46 patients received long-course chemoradiotherapy (CRT) consisting of 50.4 Gy in 28 fractions (1.8 Gy per fraction) with concurrent capecitabine (825 mg/m2 twice daily on radiotherapy days) or continuous-infusion 5-fluorouracil (225 mg/m2/day). Short-course radiotherapy was received by 3 patients and was delivered as 25 Gy in 5 fractions (5 Gy per fraction) without concurrent chemotherapy. For the 1 patient that received total neoadjuvant therapy, a consolidation capecitabine and oxaliplatin regimen (1,000 mg/m2 capecitabine twice daily on days 1-14 plus 130 mg/m2 oxaliplatin on day 1, every 3 weeks for 3-4 cycles) was administered in conjunction with long-course CRT (50.4 Gy in 28 fractions). Surgery was typically performed 6-8 weeks after completion of radiotherapy (minimum interval of ≥4 weeks), in accordance with institutional practice and national rectal cancer guidelines (12).
Surgical technique for TaTME
All patients underwent bowel preparation before surgery and received rectal washout during the procedure. A purse-string suture was placed to ensure a clean distal rectal resection margin. Transanal dissection was initiated superficial to the folded mucosa of the purse-string suture and continued in a standardized manner in the dorsal TME plane. An AirSeal® system (CONMED Corporation) and a GelPOINT Path Transanal Access Platform (Applied Medical Resources Corporation) were utilized. A posterior approach facilitated mobilization of the distal third of the rectum, following a U-shaped plane to prevent specimen coning. Following specimen removal, a colorectal end-to-end anastomosis was performed using a Procedure for Prolapse and Haemorrhoids stapling unit with an outer diameter of 31 or 33 mm and a closed staple height of 4.8 mm. All staple lines were inspected, and images were captured for database documentation.
Diverting ileostomy creation
A diverting loop ileostomy was routinely considered in patients who underwent ultra-low anastomosis (<5 cm from the anal verge), after neoadjuvant chemoradiotherapy or in those with high-risk features such as intraoperative tension at the anastomosis. The stoma was created in the right lower quadrant through a separate trephine incision, matured in accordance with the standard Brooke technique (14) and reversed after 6-12 weeks following confirmation of anastomotic integrity by contrast-enhanced CT with rectal Gastrografin enema.
Statistical analysis. Statistical methods
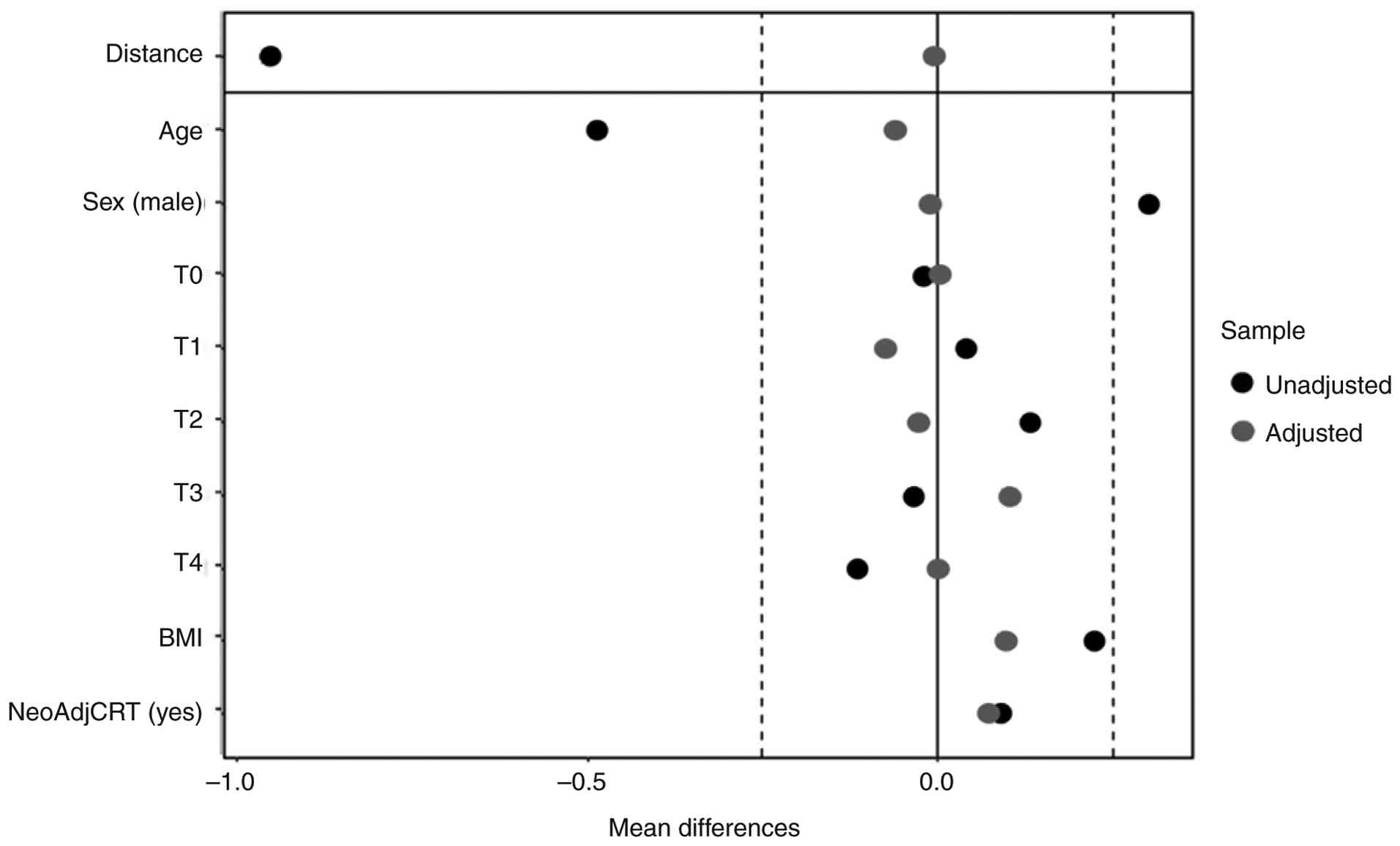
PSM (15) was performed to reduce selection bias and create a balanced comparison between the TaTME and ULAR groups. Propensity scores were calculated using a logistic regression model adjusted for the following covariates: i) Age; ii) sex; iii) pre-treatment tumour stage; iv) BMI; and v) neoadjuvant chemoradiotherapy. Nearest-neighbour matching with a 4:1 ratio (without replacement) was utilized, with a calliper width of 0.2 SD of the log-odds of the propensity score. Balance between groups was assessed using standardized mean differences, variance ratios and empirical cumulative distribution function diagnostics. Graphical representations, including empirical quantile-quantile plots and standardized mean difference plots, were used to confirm balance.
Categorical variables were compared using Fisher's exact test (two-tailed), as a number of variables did not satisfy the expected-count assumptions required for the χ2 test. For categorical variables with multiple categories and small sample sizes, data were dichotomised into clinically meaningful two-group comparisons (including tumour stage I-II vs. III-IV; nodal involvement stage 0 vs. I-II; American Society of Anaesthesiologists physical classification system I-II vs. III-IV; procedure open/hybrid vs. laparoscopic) (13,16) to improve interpretability and avoid unstable multi-cell analyses. Continuous variables were analysed using the Wilcoxon rank-sum test due to non-normal data distributions. P<0.05 was considered to indicate a statistically significant difference. All analyses were conducted using R Studio (version 2023.06.0; Build 421; Posit Software, PBC)
Survival analysis. Cox proportional hazard models were used to compare DFS and OS between the TaTME and ULAR cohorts. The same covariates used in the PSM model were included in the Cox models. These models were evaluated for proportionality assumptions, goodness of fit using the concordance index, and statistical significance using Wald and likelihood ratio tests. Model outputs, including hazard ratios, confidence intervals, P-values, and AIC values, were reported directly in the Results section rather than as separate figures.
Descriptive and subgroup analyses. Descriptive statistics were used to compare patient characteristics, postoperative outcomes, histopathology results, adjuvant therapy and mid-term outcomes. Continuous variables are reported as mean (SD), while categorical variables are reported as frequency (proportion). Kaplan-Meier survival analysis was conducted for PFS, DFS and OS, providing a visual representation of survival probabilities. Subgroup analyses were also conducted for distant metastases and local recurrence.
Results
A total of 178 patients were initially included in the present study (TaTME, n=21; ULAR, n=157) (Table SI). Following PSM, the sample size was reduced to 78 matched patients (TaTME, n=19; ULAR, n=59). Balance diagnostics indicated notable improvements in covariate balance post-matching (Fig. 1) and the propensity-matched cohorts were well balanced, with no significant differences in matched baseline characteristics (Table I). Although the variable ‘Procedure (Open/Hybrid vs. Laparoscopic)’ showed a significant difference between groups (P=0.008), this was expected because the surgical approach was not used as a matching variable in the propensity score model. The BMI used in the analysis was re-measured after hospitalization and was therefore relatively high, with a mean of 29.7 (SD=10.0) in the TaTME group and 27.5 (SD=5.6) in the matched ULAR group.
 |
Table I
Subject characteristics in both ULAR (n=59) and TaTME (n=19) groups.
|
Table I
Subject characteristics in both ULAR (n=59) and TaTME (n=19) groups.
| Characteristic |
ULAR |
TaTME |
P-value |
| Mean age (SD), years |
60(11) |
57(12) |
0.999 |
| Sex (male/female), n |
52/7 |
17/2 |
>0.999 |
| Mean BMI (SD) |
27.8 (4.3) |
29.3 (10.4) |
0.558 |
| NeoAdjCRT (yes/no), n |
37/22 |
14/5 |
0.422 |
| NeoTYPE (long course CRT/short course RT/TNT/other), n |
33/3/0/1 |
13/0/1/0 |
- |
| T stage (I/II/III), n |
6/19/34 |
1/6/12 |
- |
| T stage (I or II/III), n |
25/34 |
7/12 |
0.791 |
| N stage (0/I/II), n |
25/20/14 |
7/8/4 |
- |
| N stage (0/I or II), n |
25/34 |
7/12 |
0.791 |
| M stage (0/I), n |
51/8 |
19/0 |
0.188 |
| ASA score (1/2/3/4), n |
4/30/24/1 |
2/6/11/0 |
- |
| ASA score (1 or 2/3 and 4), n |
34/25 |
8/11 |
0.294 |
| Procedure (open/hybrid/laparoscopic), n |
12/5/42 |
0/0/19 |
- |
| Procedure (open or hybrid/laparoscopic), n |
17/42 |
0/19 |
0.008 |
Operative and postoperative outcomes between the two groups are shown in Table II. Operative time was significantly longer in the TaTME group (ULAR: 322 min, SD=123; TaTME: 554 min, SD=274; P=0.002). However, no patients in the TaTME group required conversion to open surgery, whereas 4 patients in the ULAR group did (P=0.571). Although not statistically significant, no patients in the TaTME group had a positive CRM, anastomotic leakage or required reoperation. The decision to create a diverting ileostomy was made at the surgeon's discretion and the difference in its use between the two groups was not statistically significant (P=0.766. While the rate of postoperative sexual dysfunction appeared higher in the TaTME group (3/16 vs. 1/58; P=0.043), the absolute number of cases was very small and this finding should be interpreted with caution. No other postoperative complications, including anastomotic leak, sepsis or ileus, differed significantly between groups. Histopathological analysis showed minimal differences between the two groups, with no significant differences (Table SII). More patients in the ULAR group completed adjuvant therapy compared with those in the TaTME group, although this difference was not significant (ULAR, n=18; TaTME, n=2; P=0.249).
|
Table II
Operative and postoperative outcomes for both ULAR (n=59) and TaTME (n=19) groups.
|
Table II
Operative and postoperative outcomes for both ULAR (n=59) and TaTME (n=19) groups.
| Characteristic |
ULAR |
TaTME |
P-value |
| Mean operative time (SD), min |
322(123) |
554(274) |
0.002a |
| Conversion to open (yes/no)b, n |
4/55 |
0/19 |
0.567 |
| Circumferential resection margin (positive/negative), n |
1/58 |
0/19 |
>0.999 |
| Anastomotic leak (yes/no), n |
1/58 |
0/19 |
>0.999 |
| Surgical site infection (yes/no), n |
3/56 |
1/18 |
>0.999 |
| Sepsis without surgical site infection (yes/no), n |
1/58 |
0/19 |
>0.999 |
| Ileus (yes/no), n |
10/49 |
2/17 |
0.720 |
| Urinary retention (yes/no), n |
2/57 |
1/18 |
>0.999 |
| Bleeding from surgical site (yes/no), n |
1/58 |
1/18 |
0.430 |
| Return to the theatre (yes/no), n |
3/56 |
0/19 |
>0.999 |
| Mean length of stay in hospital (SD), days |
11(6) |
11(11) |
0.765 |
| Sexual dysfunction (yes/no), n |
1/58 |
3/16 |
0.043 |
| Ileostomy (yes/no), n |
43/16 |
15/4 |
0.766 |
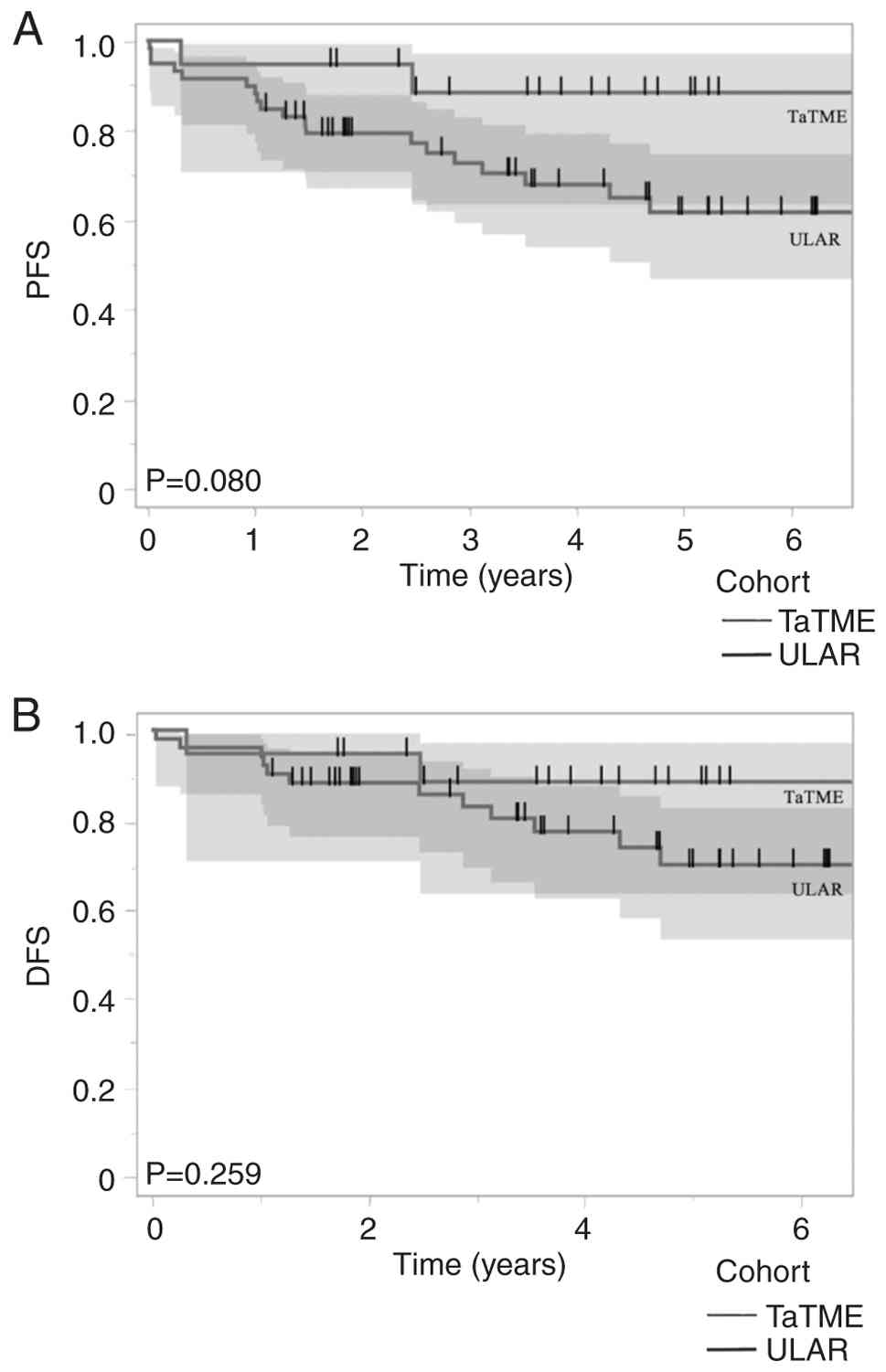
Median follow-up time to assess PFS, DFS and OS was slightly higher at 3.86 years in the TaTME group when compared with 3.84 years in the ULAR group. Kaplan-Meier survival analysis (Fig. 2A) demonstrated no statistically significant difference in the 3-year PFS probability between the TaTME (88%) and ULAR (73%) groups (P=0.080), although the point estimate was numerically higher in the TaTME group. While numerical trends favouring TaTME were observed in both PFS and OS, these differences did not reach statistical significance and should therefore be interpreted with caution. To address potential confounding, a subgroup analysis excluding stage IV disease was performed (Fig. 2B), which also showed no significant difference in 3-year DFS rates (TaTME: 88%; ULAR: 83%; P=0.259).
The Cox proportional hazards model for PFS yielded a hazard ratio of 0.29 for TaTME vs. ULAR (95% CI, 0.07-1.26; P=0.10), indicating a possible but not statistically confirmed reduction in recurrence rates. When restricted to non-metastatic patients, the hazard ratio was 0.43 (P=0.27). The corrected Akaike Information Criterion (AIC) for the PFS model was 168.5, indicating moderate model fit.
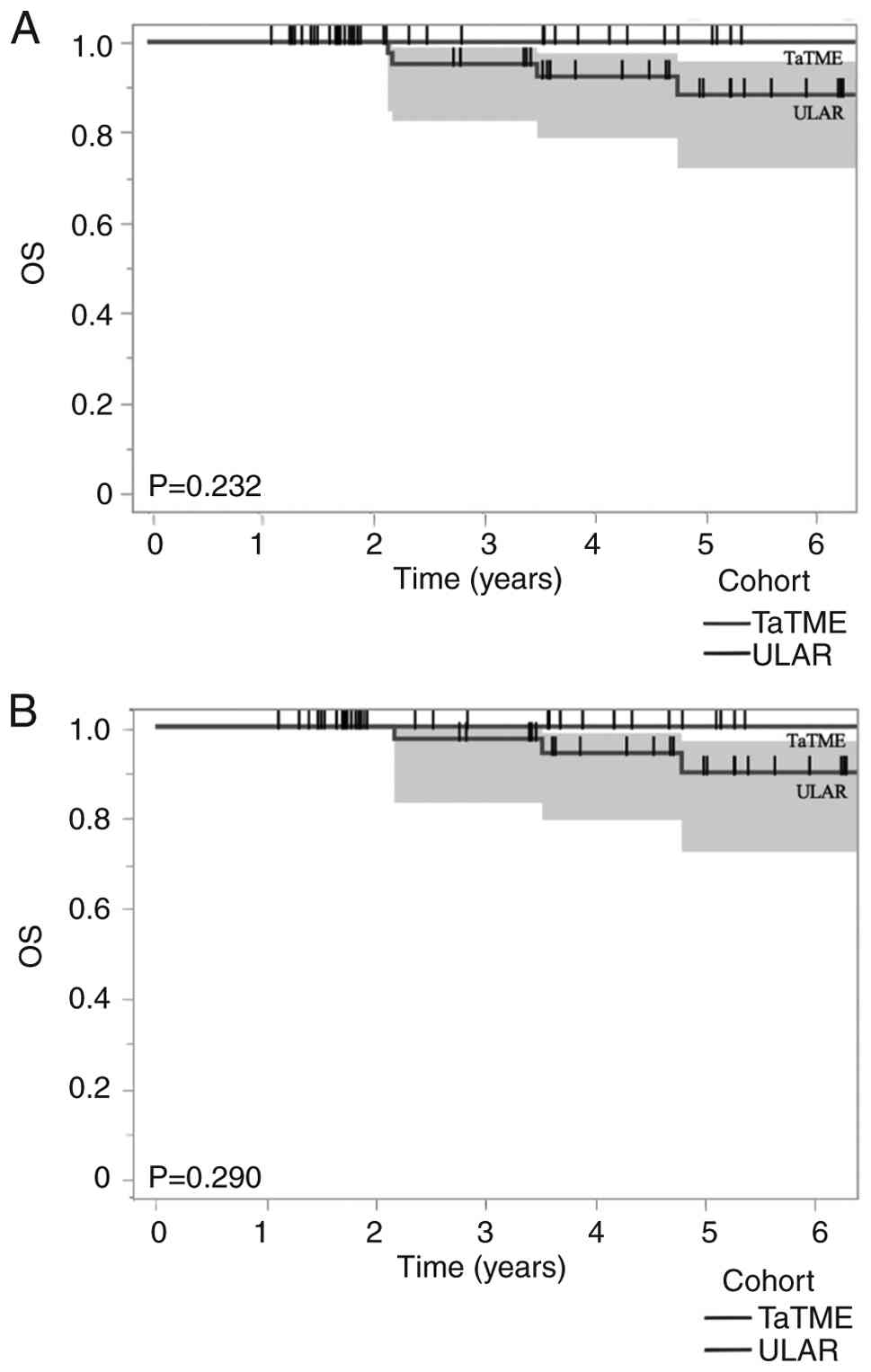
Kaplan-Meier survival analysis (Fig. 3A) revealed no statistically significant difference in 3-year OS between the TaTME and ULAR groups when patients with stage IV disease were included (TaTME: 100%; ULAR: 95%; P=0.232). Following the exclusion of patients with metastatic disease (Fig. 3B), the difference in 3-year OS remained small and statistically non-significant (TaTME: 100%; ULAR: 97%; P=0.290).
Discussion
Surgical and mid-term outcomes of TaTME, a relatively new but technically demanding approach for low rectal cancer were evaluated in the present study within a single-centre setting. TaTME was primarily adopted to overcome the technical limitations of conventional laparoscopic ULAR, particularly in patients with a narrow pelvis or high BMI. Results demonstrated that TaTME achieved negative resection margins and avoided open conversion despite higher anatomical difficulty, supporting its technical feasibility and potential benefits in complex cases.
The present results showed that the TaTME group had no conversions to open surgery, despite the majority of patients having a BMI >30, including two patients with a BMI >50 (1 man and 1 woman), indicating a higher level of surgical difficulty. The absence of open conversion in the TaTME group, despite higher BMI and challenging pelvic anatomy, corroborates the technical advantages of the surgical approach compared with ULAR alone. By contrast, the ULAR group experienced conversions during laparoscopic surgery primarily due to limited visualisation and difficulty in distal rectal mobilisation in patients with a narrow pelvic morphology. Additionally, all resection margins in the TaTME group were negative, suggesting that this approach effectively achieves clear surgical margins, a key factor in reducing recurrence risk for rectal cancer. In terms of safety, TaTME showed no cases of anastomotic leakage, which is particularly relevant for obese male patients who are at higher risk for this complication.
To minimize selection bias, the present study employed PSM, ensuring a balanced comparison between the TaTME and ULAR groups. While a trend toward improved PFS was observed in the overall TaTME group, it is important to note that no stage IV cases were included in this cohort, limiting direct comparison. Subgroup analysis of non-stage IV patients revealed similar outcomes between groups. The Cox model demonstrated moderate predictive capability with an AIC of 168.5.
While the present results are encouraging, they must be interpreted cautiously considering international experience. Reports from Norway and the Netherlands raised notable concerns regarding unusually high local recurrence rates after TaTME, prompting a temporary moratorium by the Norwegian Health Authority and critical reassessment in the Dutch TaTME registry (9,10). By contrast, a number of high-volume centres have demonstrated acceptable oncological safety and improved specimen quality when the procedure is performed by trained, proctored teams (17,18). The absence of local recurrence and clear CRM in the present study suggest that meticulous technique and institutional experience may mitigate these previously reported risks.
Furthermore, ~70% of the present study population were male, a factor known to increase technical difficulty due to the narrower, deeper male pelvis. This anatomical constraint is associated with higher conversion and local recurrence rates in laparoscopic TME. Previous comparative studies indicate that in male patients, laparoscopic TME carries up to twice the risk of local recurrence compared with robotic TME (19), whereas outcomes appear equivalent in females (20,21). TaTME, offering direct visualisation of the distal mesorectum, may provide similar advantages to robotic surgery in these anatomically challenging scenarios, supporting its role as a feasible alternative where robotic systems are unavailable or cost prohibitive.
The present mid-term data revealed no significant differences in DFS or OS between TaTME and ULAR cohorts, consistent with findings from previous meta-analyses (8,22). Notably, no cases of anastomotic leakage or permanent stoma were observed in the TaTME group. A statistically significant difference in postoperative sexual dysfunction was observed (P=0.043); however, this result is likely attributable to the small sample size and limited number of events rather than a true difference in functional outcomes. Prior studies (17-22) have not demonstrated consistent differences in sexual function between TaTME and conventional ULAR, and larger cohorts are needed to clarify this outcome. Longer follow-up is, however, necessary to determine whether these early benefits translate into sustained oncological safety.
The principal limitations of the present study include the small sample size of the TaTME cohort (n=19), the absence of stage IV patients and its single-institution design, all of which limit statistical power and generalisability. The absence of stage IV disease in the TaTME cohort restricts direct prognostic comparisons between groups. Nevertheless, as stage IV status does not affect short-term surgical outcomes, these cases were retained in the overall analysis.
The present findings should therefore be viewed as exploratory and hypothesis-generating. Future research should involve multicentre collaborations or randomised controlled trials to validate these results and delineate the learning curve and training requirements. A structured training and standardisation framework, including proctoring, peer review and simulation, may reduce variability and enhance oncological safety as TaTME adoption expands (23). In conclusion, TaTME demonstrated comparable oncological outcomes to ULAR, with encouraging results in challenging cases, including patients with a high BMI and without requiring conversion to open surgery. While earlier negative data may have been influenced by the steep learning curve, TaTME shows potential as a viable alternative for patients facing technical challenges with traditional laparoscopic surgery. Further multicentre or randomized trials are needed to validate these findings and assess long-term oncological and functional outcomes.
Supplementary Material
Subject characteristics before matching.
Histopathology and adjuvant therapy.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
PPK performed data analysis, interpreted the study findings and drafted the original manuscript. SF conceived and designed the study, curated and verified the data, performed data analysis, coordinated the project and critically revised the manuscript. SC contributed to study design, data analysis, interpretation of results and methodological development. EA curated and managed the study database, contributed to statistical analysis and methodology, developed analytical software tools and critically revised the manuscript. KN contributed to data collection, methodological development, interpretation of findings and manuscript preparation. AA, VN, TSS, YKT, JL, CS, TCN, HC and WT performed the surgical procedures included in the study, contributed to patient identification and recruitment, assisted with clinical data acquisition and interpretation, critically reviewed the manuscript for important intellectual content and approved the final version for publication. HC was also involved in project supervision and overall study oversight. All authors read and approved the final version of the manuscript. PPK and SF confirm the authenticity of all the raw data.
Ethics approval and consent to participate
The present study was conducted in accordance with the Declaration of Helsinki and was approved by the Monash Health Technology/Clinical Practice Committee (approval no. N_18_07). Written informed consent for participation was obtained from all prospectively enrolled patients undergoing TaTME. For retrospectively analysed patients who underwent ULAR, the requirement for individual consent was waived.
Patient consent for publication
Written informed patient consent was obtained for publication of data as part of the present study.
Competing interests
The authors declare that they have no competing interests.
References
|
1
|
World Health Organization (WHO): Colorectal cancer. WHO, Geneva, 2023. https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer.
|
|
2
|
Hasegawa H, Okabayashi K, Tsuruta M, Ishida T, Asahara F and Coleman MG: Evolution of surgery for rectal cancer: Transanal total mesorectal excision~new standard or fad?~. J Anus Rectum Colon. 2:115–121. 2018.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Kim NK, Lim DJ, Yun SH, Sohn SK and Min JS: Ultralow anterior resection and coloanal anastomosis for distal rectal cancer: Functional and oncological results. Int J Colorectal Dis. 16:234–237. 2001.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Park JS, Choi GS, Jun SH, Hasegawa S and Sakai Y: Laparoscopic versus open intersphincteric resection and coloanal anastomosis for low rectal cancer: Intermediate-term oncologic outcomes. Ann Surg. 254:941–946. 2011.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Wu H, Guo R and Li H: Short-term and long-term efficacy in robot-assisted treatment for mid and low rectal cancer: A systematic review and meta-analysis. Int J Colorectal Dis. 39(7)2023.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hasegawa H, Matsuda T, Yamashita K, Sawada R, Harada H, Urakawa N, Goto H, Kanaji S, Oshikiri T and Kakeji Y: Obesity and narrow pelvis prolong the operative time in conventional laparoscopic rectal cancer surgery, but not in a two-team transanal total mesorectal excision approach. Asian J Endosc Surg. 16:189–196. 2023.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Sylla P, Rattner DW, Delgado S and Lacy AM: NOTES transanal rectal cancer resection using transanal endoscopic microsurgery and laparoscopic assistance. Surg Endosc. 24:1205–1210. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Hajibandeh S, Hajibandeh S, Eltair M, George AT, Thumbe V, Torrance AW, Budhoo M, Joy H and Peravali R: Meta-analysis of transanal total mesorectal excision versus laparoscopic total mesorectal excision in management of rectal cancer. Int J Colorectal Dis. 35:575–593. 2020.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Larsen SG, Pfeffer F and Kørner H: Norwegian Colorectal Cancer Group. Norwegian moratorium on transanal total mesorectal excision. Br J Surg. 106:1120–1121. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
van Oostendorp SE, Belgers HJ, Bootsma BT, Hol JC, Belt EJTH, Bleeker W, Den Boer FC, Demirkiran A, Dunker MS, Fabry HFJ, et al: Locoregional recurrences after transanal total mesorectal excision of rectal cancer during implementation. Br J Surg. 107:1211–1220. 2020.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gachabayov M and Bergamaschi R: Is taTME delivering? Updates Surg. 71:13–15. 2019.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Cancer Council Australia Colorectal Cancer Guidelines Working Party: Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Cancer Council Australia, Sydney, 2017. https://www.cancer.org.au/clinical-guidelines/bowel-cancer/colorectal-cancer.
|
|
13
|
American Joint Committee On Cancer (AJCC): AJCC cancer staging handbook: From the AJCC cancer staging manual. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL and Trotti A (eds): Springer, New York, 2010.
|
|
14
|
Brooke BN: The management of an ileostomy, including its complications. Lancet. 2:102–104. 1952.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Austin PC: An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 46:399–424. 2011.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Doyle DJ and Garmon EH: American Society of Anesthesiologists Classification (ASA Class). Nih.gov. StatPearls Publishing, 2019. https://www.ncbi.nlm.nih.gov/books/NBK441940/.
|
|
17
|
Lacy AM, Tasende MM, Delgado S, Fernandez-Hevia M, Jimenez M, De Lacy B, Castells A, Bravo R, Wexner SD and Heald RJ: Transanal total mesorectal excision for rectal cancer: Outcomes after 140 patients. J Am Coll Surg. 221:415–423. 2015.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Penna M, Hompes R, Arnold S, Wynn G, Austin R, Warusavitarne J, Moran B, Hanna GB, Mortensen NJ and Tekkis PP: TaTME Registry Collaborative. Transanal total mesorectal excision: International registry results of the first 720 cases. Ann Surg. 266:111–117. 2017.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Kim MJ, Hur H, Baek JH, et al: Comparative oncological outcomes of robotic versus laparoscopic total mesorectal excision for mid-to-low rectal cancer in male patients. Br J Surg. 108:429–437. 2021.
|
|
20
|
Park EJ, Kim CW, Cho MS, et al: Gender-based outcomes following laparoscopic and robotic surgery for rectal cancer: A propensity-matched analysis. Surg Endosc. 37:2781–2791. 2023.
|
|
21
|
Lee L, de Angelis N, Brunetti F, et al: Robotic versus laparoscopic rectal cancer surgery in female patients: a multicentre analysis. Colorectal Dis. 25:2367–2375. 2023.
|
|
22
|
Arezzo A, Passera R, Salvai A, et al: Long-term oncologic outcomes of transanal total mesorectal excision versus laparoscopic TME: updated meta-analysis. Dis Colon Rectum. 65:301–315. 2022.
|
|
23
|
Adamina M, Spinelli A, Ashrafian H, et al: Educational strategies for safe implementation of TaTME: Consensus from the European TaTME training initiative. Colorectal Dis. 23:2020–2029. 2021.
|