Introduction
Type 1 diabetes mellitus (T1DM) is the most common
type of DM in children. The pathogenesis of T1DM has not been
elucidated, but it is considered to be mainly related to the
destruction of pancreatic β cells by autoimmune responses and
oxidative stress caused by genetic and environmental factors
(1,2). The global incidence of T1DM has been
increasing steadily at an average annual rate of 3-4% over the past
30 years, and the role of environmental factors in the occurrence
of T1DM is increasingly being emphasized (1).
Vitamin D is a fat-soluble steroid hormone
derivative. Under normal circumstances, 70-80% of vitamin D in the
body is synthesized from 7-dehydrocholesterol in the human skin
after ultraviolet irradiation and becomes biologically active after
two hydroxylations. Serum 25-(OH)D3 levels are typically
used as an evaluation index of vitamin D levels in vivo.
Vitamin D not only regulates calcium and phosphorus metabolism but
also cell proliferation, differentiation, metabolism and immune
functions (3,4). Vitamin D levels have been reported to
be positively associated with the function of pancreatic β cells
due to their immunoregulatory, anti-inflammatory and anti-oxidative
effects, and vitamin D insufficiency or deficiency has been
associated with the development of T1DM and its complications
(3-5).
In a meta-analysis, among children of different ethnicities and
ages, those with T1DM had a higher incidence of vitamin D
deficiency and lower 25-(OH)D3 levels than healthy
children (6). By contrast, vitamin
D or active vitamin D supplementation has been suggested to be
effective in preventing the incidence of T1DM (7). Therefore, the role of vitamin D in
the onset, prevention and treatment of diabetes in children is
receiving increasing attention.
In the present study, the 25-(OH)D3
levels between children with T1DM and healthy children were
collected and compared, and various factors that may affect
25-(OH)D3 levels were analyzed to provide new ideas and
a basis for the clinical prevention and treatment of T1DM in
children.
Materials and methods
Subjects
The present study was retrospective in nature. Data
were collected from electronic medical records, covering the period
between January 2017 and December 2023. The study was approved by
the Ethics Committee of Shanxi Medical University (Taiyuan, China;
approval no. 2020sll003-3) and the Ethics Committee of Shanxi
Children's Hospital/Shanxi Maternal and Child Health Hospital
(Taiyuan, China; approval no. IRB-WZ-2024-032). The ethics
committees approved the waiver of informed consent due to the
retrospective nature of the study. All research was performed in
accordance with relevant guidelines and regulations.
Inpatients with T1DM from the Department of
Endocrinology, Genetics and Metabolism of Shanxi Children's
Hospital who were treated between January 2017 and December 2023
were included in the T1DM group, and outpatients who underwent
health examinations in the same location in the same period were
included in the control group. The inclusion criteria for control
subjects were: i) No history of diabetes or other metabolic
diseases; ii) no chronic diseases affecting vitamin D metabolism,
including chronic liver disease, chronic kidney disease,
parathyroid disorders, inflammatory bowel disease or malabsorption
syndromes; iii) no long-term use of medications known to affect
vitamin D metabolism, such as glucocorticoids, anticonvulsants or
antiretroviral agents; and iv) no acute illnesses at the time of
inclusion. The inclusion criteria for patients with T1DM were
inpatients who met the diagnostic criteria for T1DM, and who had no
diseases or long-term use of drugs that affect calcium and vitamin
D metabolism. For variables with missing data, a complete-case
analysis was performed, and only patients with full data on all
study variables were included. No imputation was used for missing
data. A total of 86 patients were excluded from the T1DM group due
to incomplete clinical data or the presence of other conditions
affecting vitamin D metabolism. The diagnosis of T1DM was made
according to the 1999 and 2019 World Health Organization diagnostic
criteria for T1DM (8,9). The main data collected from children
with T1DM included sex, age, place of residence, duration of
disease, 25-(OH)D3 level, random blood glucose (RBG)
level, glycated hemoglobin (HbA1C) levels, and the presence of
diabetic ketoacidosis (DKA), diabetic ketosis (DK) and infections.
DKA and DK were diagnosed according to the 2014 guidelines issued
by the International Society for Pediatric and Adolescent Diabetes
(10). Data on sex, age, place of
residence and 25-(OH)D3 levels were collected from
healthy children in the control group.
According to the medical history of the inpatients
with T1DM, children who were hospitalized for the first time and
newly diagnosed were divided into the newly diagnosed group, and
those hospitalized more than once were divided into the established
group. According to the recommendations for the prevention and
treatment of the vitamin D deficiency and rickets released by the
National Rickets Prevention and Treatment Research Collaboration
Group in 2015(11), children were
divided into the following five subgroups based on
25-(OH)D3 levels: Excess (>250 nmol/l), normal (≥50
and ≤250 nmol/l), insufficient (37.5-50 nmol/l), deficiency (≤37.5
nmol/l) and severe deficiency (≤12.5 nmol/l). The patients were
also divided into corresponding subgroups based on age (<5 years
old, 5-10 years old and ≥10 years old), sex (male and female),
place of residence (city and rural), presence of DKA/DK or
infections, and the admission quarter. The differences between or
among the control and T1DM groups or different subgroups for T1DM,
HbA1C, RBG and 25-(OH)D3 levels, and the composition
ratio of children with vitamin D insufficiency plus deficiency
[25-(OH)D3 below the normal level of 50 nmol/l] were
compared, and the factors that may affect the 25-(OH)D3
levels were analyzed.
Statistical analysis
GraphPad Prism 6.0 software (Dotmatics) was used for
the statistical analysis. Measurement data with normal or
approximate normal distribution are expressed as the mean ±
standard deviation. For two-group comparisons, the unpaired t-test
was used when variances were equal, and Welch's corrected t-test
was used when variances were unequal. For multiple-group
comparisons, one-way ANOVA followed by Tukey's test was applied
when variances were equal; otherwise, the Kruskal-Wallis test was
used, followed by Dun's post hoc test for pairwise comparisons.
Skewed data are expressed as the median (interquartile range). The
Mann-Whitney test was used for two-group comparisons, and the
Kruskal-Wallis test was used for multiple-group comparisons,
followed by Dun's post hoc test for pairwise comparisons.
Qualitative data are expressed as n (%), and the differences in
composition ratios were compared using the χ2 test. For
multiple comparisons, P-values were adjusted using Bonferroni's
correction to control for Type I errors. Pearson correlation
analysis was used to analyze the linear correlation between
25-(OH)D3 levels and quantitative variables such as age,
HbA1C and RBG in the T1DM group, and multiple linear regression was
used to screen the variables affecting the 25-(OH)D3
level. To evaluate the association between T1DM status and vitamin
D status, logistic regression analysis was performed. Vitamin D
status was dichotomized as insufficiency/deficiency
[25-(OH)D3 <50 nmol/l] vs. normal (≥50 nmol/l). Both
crude and adjusted odds ratios (ORs) with 95% confidence intervals
(CIs) were calculated. All subgroup analyses were exploratory. No
adjustment for multiple testing was applied, and results should be
interpreted accordingly. P<0.05 was considered to indicate a
statistically significant difference.
Results
General information of the study
subjects
As shown in Table
I, 757 inpatients with T1DM and 136 healthy outpatients were
included in the present study. The age distribution was consistent
between the control group and the newly-diagnosed diabetes subgroup
(P>0.05; data not shown), whereas the age distribution in the
overall T1DM group differed from that in the control group
(P<0.0001). No significant differences were observed in terms of
sex or place of residence between the control and T1DM groups
(P>0.05). Due to the significant age difference, further
analyses were adjusted for age to minimize potential confounding.
Most newly-diagnosed children with T1DM were aged >5 years.
 | Table IGeneral information of children in
the control and T1DM groups. |
Table I
General information of children in
the control and T1DM groups.
| | | Sex | Place of
residence | Age |
|---|
| Groups | n | Male/female, n | P-value | City/rural, n | P-value | Median (IQR),
years | P-value | <5 years, n | 5-10 years, n | ≥10 years, n |
|---|
| Control | 136 | 67/69 | 0.1049a | 73/63 | 0.6629 | 8.0 (5.0-11.0) |
<0.0001a | 25 | 77 | 34 |
| T1DM | 757 | 433/324 | | 425/332 | | 10.0
(7.0-12.0) | | 101 | 241 | 415 |
| Newly
diagnosed | 324 | 157/167 |
<0.0001b | 201/123 | 0.0058 | 8.0 (5.0-11.0) |
<0.0001b | 77 | 126 | 121 |
| Established | 433 | 276/157 | | 224/209 | | 11.0
(8.5-13.0) | | 24 | 115 | 294 |
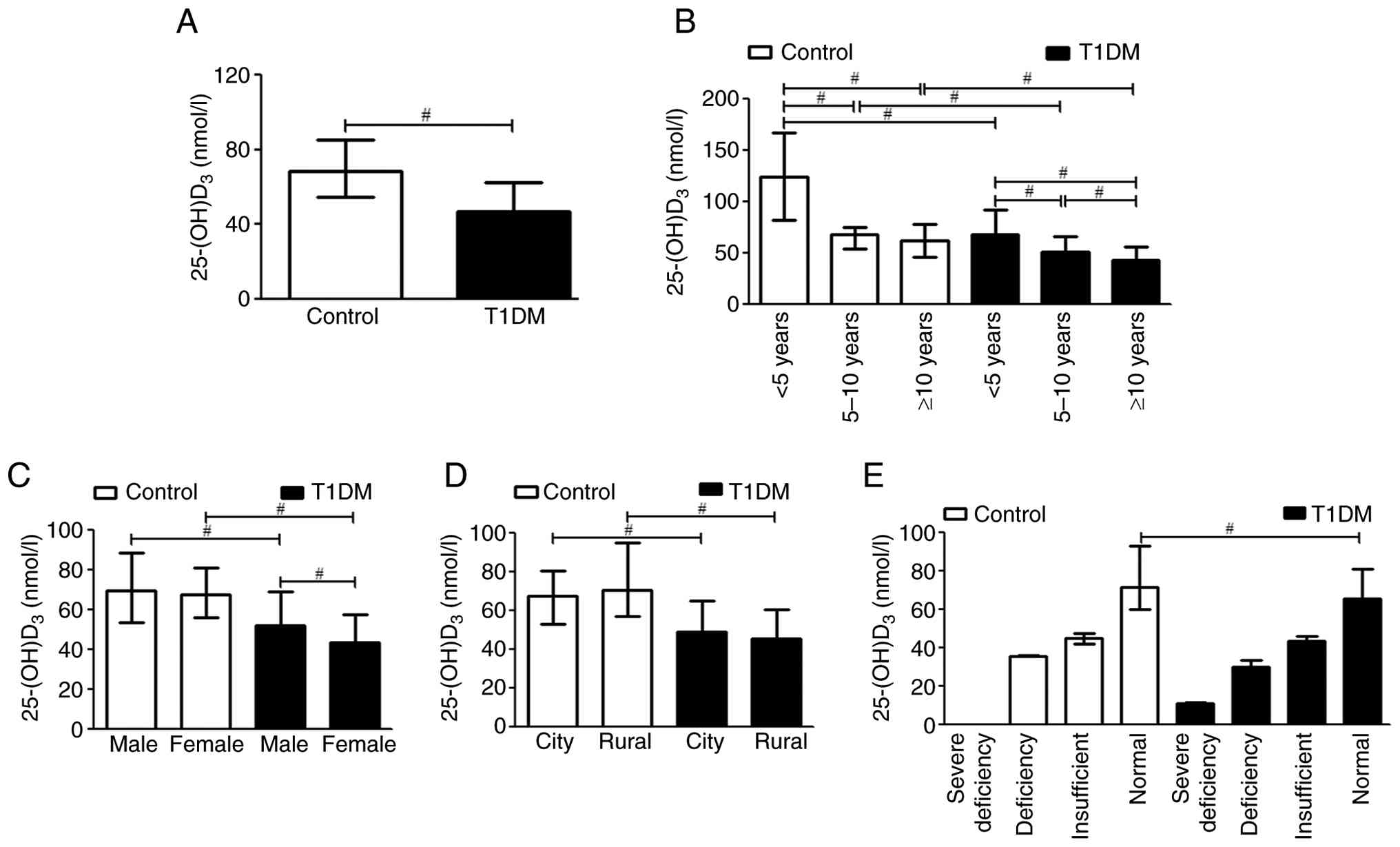
Lower 25-(OH)D3 levels are
present in inpatients with T1DM, especially in those newly
diagnosed or in those cases complicated with DKA/DK or
infection
As shown in Table
II, 54.4% of the inpatients with T1DM had vitamin D
insufficiency or deficiency, compared to only 13.2% in the control
group (χ2 test; P<0.0001), and as shown in Fig. 1A, the 25-(OH)D3 level of
the T1DM group was significantly lower than that of the control
group (Mann-Whitney test, P<0.01). The 25-(OH)D3
level in each age subgroup in the T1DM group was also significantly
lower than that in the same age subgroup in the control group (all
Mann-Whitney test with Bonferroni correction, P<0.01; Table II and Fig. 1B). Notably, the
25-(OH)D3 levels in both T1DM and control groups
decreased with age, and children <5 years had the highest
25-(OH)D3 levels in both groups, whereas the proportion
of patients with <50 nmol/l 25-(OH)D3 was the lowest
in the <5 years subgroup (all Kruskal-Wallis test with
Bonferroni correction, P<0.05; Table II and Fig. 1B). Compared with those of the
control group, the 25(OH)D3 levels of the same sex or
place of residence subgroups in the T1DM group were significantly
lower, while the proportion of patients with <50 nmol/l
25(OH)D3 was significantly higher in the T1DM group than
in the control group (all Mann-Whitney test or χ2 test
with Bonferroni correction, P<0.01; Table II; Fig. 1C and D). No significant differences were
observed in 25(OH)D3 levels and the proportion of
patients with <50 nmol/l 25(OH)D3 between different
sex or place of residence subgroups in the control group, whereas
the 25(OH)D3 level of females was lower and the
proportion of patients with <50 nmol/l 25(OH)D3 was
higher in the T1DM group (all Mann-Whitney test or χ2
test with Bonferroni correction, P<0.01; Table II; Fig. 1C and D). Even in the same subgroups with normal
25-(OH)D3 levels, the 25-(OH)D3 levels in the
children with T1DM were significantly lower than those in the
control group (Mann-Whitney test, P<0.01; Table II; Fig. 1E).
| Table IIBetween-group and within-group
comparisons of the proportion of children with 25-(OH)D3
levels <50 nmol/l. |
Table II
Between-group and within-group
comparisons of the proportion of children with 25-(OH)D3
levels <50 nmol/l.
| Grouping basis
subgroups | Control group, n
(%) | T1DM group, n
(%) | P-value |
|---|
|
25-(OH)D3 levels | | | |
|
Excess | 0 (0.0) | 0 (0.0) | |
|
Normal | 118 (86.8) | 345 (45.6) | |
|
Insufficient | 16 (11.8) | 194 (25.6) | |
|
Deficiency | 2 (1.5) | 216 (28.5) | |
|
Severe
deficiency | 0 (0.0) | 2 (0.3) | |
|
25-(OH)D3 <50 nmol/l | 18 (13.2) | 412 (54.4) |
<0.0001a |
|
Age,
years | | | |
|
<5 | 0 (0.0) | 31 (30.7) | 0.0034a |
|
5-10 | 9 (11.7) | 115 (47.7) |
<0.0001a |
|
≥10 | 9 (26.5) | 266 (64.1) |
<0.0001a |
|
P-value | 0.0103b |
<0.0001b | |
|
Sex | | | |
|
Male | 9 (13.4) | 266 (61.4) |
<0.0001a |
|
Female | 9 (13.0) | 146 (45. 1) |
<0.0001a |
|
P-value | 0.8625b |
<0.0001b | |
|
Residence | | | |
|
City | 11 (15.1) | 217 (51.1) |
<0.0001a |
|
Rural | 7 (11.1) | 195 (58.7) |
<0.0001a |
|
P-value | 0.8065b | 0.0424b | |
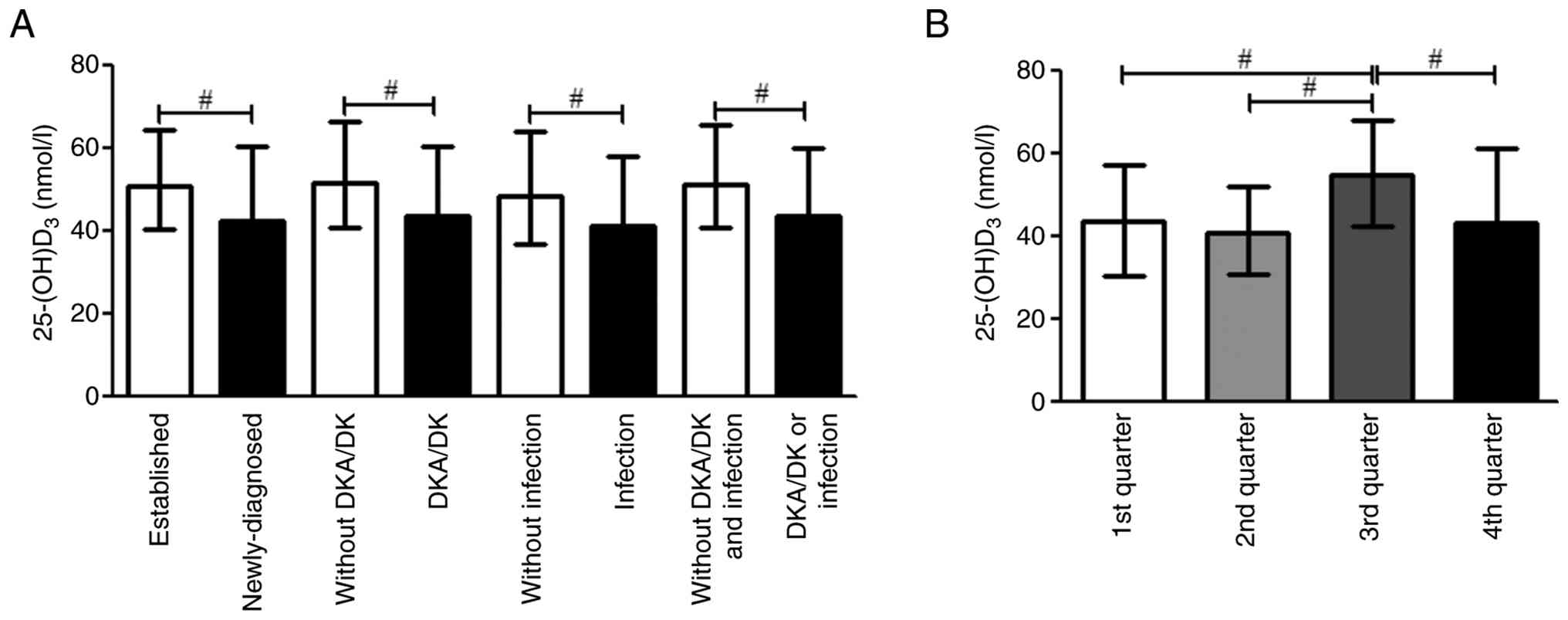
As shown in Table
III and Fig. 2A, in children
with T1DM who were newly diagnosed or in those cases complicated
with DKA/DK or infection, lower 25(OH)D3 levels, and
higher RBG and HbA1c levels were noted, as well as higher
proportions of patients with vitamin D insufficiency or deficiency
(all Mann-Whitney test with Bonferroni correction, P<0.01;
Table III). The proportions of
patients with vitamin D insufficiency or deficiency were 63.0, 62.5
and 65.9% in newly diagnosed children, those cases complicated with
DKA/DK and those with infection, respectively, compared with 48.0%
in established T1DM inpatients, 46.1 in those without DKA/DK and
52.0% in those without infection (all Mann-Whitney test or
χ2 test with Bonferroni correction, P<0.01, Table III). In addition, the
25(OH)D3 level in patients admitted to the hospital in
the third quarter was higher than that in other quarters (Table III and Fig. 2B), meanwhile, RBG, HbA1c and the
proportion of patients with vitamin D insufficiency or deficiency
were lower (all Mann-Whitney test or χ2 test with
Bonferroni correction, P<0.0001; Table III).
| Table IIIComparisons of 25-(OH)D3
and related indices between or among T1DM subgroups. |
Table III
Comparisons of 25-(OH)D3
and related indices between or among T1DM subgroups.
| | | RBG | HbA1c |
25-(OH)D3 |
25-(OH)D3 <50 nmol/l |
|---|
| Subgroups | n | Value, mmol/l | P-value | Value, % | P-value | Value, nmol/l | P-value | n (%) | P-value |
|---|
| Normal range | | <11. 1 | | 4-5.6 | | 50-250 | | | |
| T1DM group | 757 | 14.04
(7.66-22.58) | | 10.70
(8.30-12.95) | | 47.13
(35.72-62.66) | | 412 (54.4) | |
|
Disease | | | | | | | | | |
|
Established | 433 | 11.28
(6.59-18.07) | <0.0001 | 8.70
(7.20-10.50) | <0.0001 | 50.69
(40.43-64.30) | <0.0001 | 208 (48.0) | <0.0001 |
|
Newly-diagnosed | 324 | 19.37
(10.96-26.44) | | 12.60
(11.50-13.90) | | 42.64
(30.91-60.49) | | 204 (63.0) | |
|
DKA/DK | | | | | | | | | |
|
Without | 373 | 9.04
(6.04-13.65) | <0.0001 | 8.40
(7.10-10.20) | <0.0001 | 51.25
(40.78-65.73) | <0.0001 | 172 (46.1) | <0.0001 |
|
With | 384 | 20.22
(12.65-27.19) | | 12.50
(10.95-13.80) | | 43.72 (32.09-60.
16) | | 240 (62.5) | |
|
Infection | | | | | | | | | |
|
Without | 625 | 12.45
(7.01-20.64) | <0.0001 | 10.30
(8.10-12.80) | <0.0001 | 48.39 (36.76-64.
17) | <0.0001 | 325 (52.0) | 0.0048 |
|
With | 132 | 19.83
(13.57-27.09) | | 12.05
(9.85-13.70) | | 41.15
(32.47-58.03) | | 87 (65.9) | |
|
Complication
status | | | | | | | | | |
|
Without
DKA/DK and infection | 346 | 9.00
(6.03-13.38) | <0.0001 | 8.50
(7.10-10.20) | <0.0001 | 51.25
(40.78-65.73) | <0.0001 | 162 (46.8) | 0.0021 |
|
With
DKA/DK or infection | 411 | 19.65
(12.30-26.52) | | 12.40
(10.70-13.75) | | 43.72
(32.09-60.16) | | 250 (60.8) | |
|
Admission
quarter | | | | | | | | | |
|
1st
quarter | 135 | 14.71
(7.89-23.56) | <0.0001 | 10.90
(8.00-13.38) | <0.0001 | 43.67
(30.63-57.21) | <0.0001 | 85 (63.0) | <0.0001 |
|
2nd
quarter | 147 | 15.88
(9.71-25.72) | | 11.30±3.03 | | 40.75
(31.01-52.26) | | 103 (70.1) | |
|
3rd
quarter | 316 | 10.55
(6.36-17.75) | | 9.05
(7.40-11.70) | | 54.93
(42.47-68.25) | | 130 (41.1) | |
|
4th
quarter | 159 | 18.81
(11.04-24.39) | | 12.03±2.42 | | 43.14
(33.09-61.35) | | 94 (59.1) | |
Analysis of factors influencing
25-(OH)D3 levels
As shown in Table
IV, 25-(OH)D3 level was negatively associated with
age, HbA1c and RBG, and positively associated with the duration of
disease. As shown in Table V,
using multiple linear regression analysis to screen the factors
associated with 25-(OH)D3 levels, age, month of
admission, duration of disease, sex, place of residence and
HbA1C level were all significant factors associated with
25-(OH)D3 levels (all P<0.05).
| Table IVPearson's correlation analysis of
25-(OH)D3 levels and quantitative variables in the type
1 diabetes mellitus group. |
Table IV
Pearson's correlation analysis of
25-(OH)D3 levels and quantitative variables in the type
1 diabetes mellitus group.
|
25-(OH)D3 | r | P-value |
|---|
| Age | -0.3589 | <0.0001 |
| HbA1C | -0.2275 | <0.0001 |
| RBG | -0.127 | 0.0021 |
| Disease
duration | 0.1054 | 0.0037 |
| Table VVariable screening of
25-(OH)D3 influencing factors by multiple linear
regression analysis. |
Table V
Variable screening of
25-(OH)D3 influencing factors by multiple linear
regression analysis.
| Parameter | b | P-value |
|---|
| (Intercept) | 78.522 | <0.001 |
| Age | -2.818 | <0.001 |
| Admission
month | -2.622 | <0.001 |
| Disease
duration | 1.13 | 0.002 |
| Sex | 5.565 | 0.002 |
| Place of
residence | 4.399 | 0.016 |
| HbA1C | -0.823 | 0.014 |
Discussion
In the present study, inpatients with T1DM,
especially those who were newly diagnosed or whose cases were
complicated with DKA/DK or infection, admitted in the third quarter
had lower 25-(OH)D3 levels, with a higher proportion of
patients with vitamin D insufficiency or deficiency. Age, month of
admission, duration of disease, sex, place of residence and
HbA1C were the factors significantly associated with
25-(OH)D3 levels.
Vitamin D insufficiency or deficiency in childhood
may be an important risk factor for the onset and progression of
T1DM and development of its complications (2,5,7-9).
The mechanism by which vitamin D affects the development of T1DM
may be as follows: i) Polymorphisms of vitamin D metabolism genes:
Genetic susceptibility to T1DM is affected by different
polymorphisms of genes encoding the vitamin D receptor (VDR),
vitamin D-dependent calcium-binding protein (VDBP) and vitamin D
hydroxylase (10,11). Vitamin D regulates the amount of
VDR and the level of VDBP in pancreatic islet β cells, acting as a
transcription factor to regulate the expression of cell cycle, cell
differentiation, apoptosis- and insulin-related genes, and promotes
insulin synthesis and secretion (11,12).
ii) Immunomodulatory effects: Vitamin D inhibits the expression of
antigen-presenting cell surface costimulatory and MHC II molecules,
inhibits the differentiation, maturation and antigen presentation
ability of dendritic cells, and increases their apoptosis (3,11).
Vitamin D inhibits the proliferation, differentiation and
activation of T lymphocytes and promotes immune tolerance, as well
as inhibiting the secretion of pro-inflammatory cytokines, and
enhancing the production of anti-inflammatory cytokines (3,13).
The vitamin reduces the proliferation of B lymphocytes and the
production of autoantibodies, induces B cell apoptosis, prevents
the overactivation of the immune system and reduces the destruction
of normal islet β cells (3,11,13).
iii) Antioxidant effect: Vitamin D can fight intracellular
oxidative stress by reducing the myeloperoxidase content, protein
carbonyl groups and glycation end products, and by upregulating the
mRNA expression of superoxide dismutase and other anti-oxidative
pathways (14,15). Vitamin D reduces the oxidative
damage of chromosomal telomere sequences and mitochondria in
pancreatic islet β cells, and reduces insulin resistance (11,14,15).
Although a high-quality ongoing prospective cohort
study in Finland (16) showed that
no significant differences were observed in the serum
25(OH)D3 levels between 126 children who progressed to
T1DM and 126 matched controls, and that the occurrence of T1DM was
not associated with vitamin D status, the study had limited samples
with vitamin D deficiency and left possible variables affecting
vitamin D metabolism, such as dietary vitamin D intake, physical
activity, and genetic polymorphisms of VDR and VDBP, unassessed.
The present findings, derived from a larger case-control sample,
contribute additional descriptive data on the association between
T1DM and vitamin D status in a different geographic and clinical
context, but do not resolve the causal question addressed by
prospective designs (16). Serum
25(OH)D3 levels in T1DM children were lower than those
in controls (8,10,17),
even when exposed to abundant sunlight. However, the reported
differences in 25(OH)D3 levels appeared after the
diagnosis of T1DM and the associated complications may affect
vitamin D metabolism. Therefore, changes in vitamin D levels during
the development of T1DM need to be detected and analyzed in more
ongoing prospective case-cohort studies.
Some prospective studies (18,19)
have shown that vitamin D intake or 25(OH)D3 levels
during pregnancy and childhood are not significantly associated
with the development of T1DM, as concluded in a review (1). Some observational studies have found
that timely vitamin D supplementation in early childhood,
especially infancy, reduces the risk of developing T1DM later in
life. The effect of vitamin D on reducing the incidence of T1DM was
dose-dependent, and the incidence of T1DM was the lowest in
participants with a daily intake of vitamin D >2,000 IU
(20,21). Therefore, the efficacy of vitamin D
intake in preventing T1DM remains controversial and requires
additional randomized controlled trials (RCTs) to provide evidence.
However, for children at a high risk of developing T1DM, such as
those with a T1DM family history, islet autoantibodies and
high-risk HLA genotypes, vitamin D insufficiency and deficiency
should be diagnosed and treated promptly in the first few years of
life, given the greater benefits of vitamin D and the fact that
prevention is better than a cure.
Many direct and indirect factors affect vitamin D in
children, such as related gene polymorphisms, exposure time to
sunlight, regular and appropriate vitamin D supplementation, diet,
medications, underlying medical conditions, gestational age and
maternal vitamin D status at birth (22). The present analysis was limited by
the absence of data on several important confounders, including
BMI, dietary vitamin D and calcium intake, daily outdoor activity
time, sun protection habits, history of vitamin D supplementation,
family history of diabetes and birth history (22-24).
Failure to account for these factors means that the observed
association between T1DM and low 25-(OH)D3 levels may be
subject to residual confounding. The present study found that age,
month of admission, sex, place of residence, duration of disease
and HbA1C levels were the significant factors affecting
25-(OH)D3 levels. With increasing age,
25-(OH)D3 levels and the proportion of children with
normal 25-(OH)D3 levels decreased, and
25-(OH)D3 levels were negatively correlated with age.
Although the traditional peak incidence of T1DM is in children aged
10-14 years, recent studies indicate a shift toward younger age at
onset, with the peak now occurring at 4-5.9 years and significant
changes in age distribution observed more recently (12,14,25-27).
The present study also found that the number of children aged 5-10
years was relatively high among newly-diagnosed children with T1DM.
Studies have shown an overall downward trend in the proportion of
children taking outdoor activities and regular/moderate and
irregular/insufficient vitamin D supplementation with increasing
age, which may lead to more severe vitamin D insufficiency and
deficiency and a higher risk of T1DM (23,24,28).
In addition, according to the admission quarter, in the present
study, the 25-(OH)D3 level and the proportion of
children with normal 25-(OH)D3 levels were highest in
the third quarter, which may be related to the greater accumulation
of vitamin D in the summer. Shanxi Province is located at a
latitude between 35 and 40° north, and July and August are the
hottest months of the third quarter, as well as being summer
vacation time. During this period, the sunlight hours are long,
ultraviolet rays are strong, children wear less and have more skin
exposure, and outdoor activities are long, which can greatly
increase the synthesis and storage of vitamin D in the body. In
addition, the present study found that girls had lower
25-(OH)D3 levels, and a lower proportion of girls had
normal 25-(OH)D3 levels, compared with boys, which may
be related to the fact that girls usually spend less time outdoors
(24). Although place of residence
was also a significant factor affecting 25(OH)D3 levels,
no significant differences were observed in 25(OH)D3
levels and the proportion of patients with 25(OH)D3
levels <50 nmol/l between different place of residence subgroups
within the control group. A significant difference was observed
only in the proportion of patients with 25(OH)D3 level
<50 nmol/l between different place of residence subgroups in the
T1DM group, which may require more sample data for analysis.
In addition to the aforementioned factors, T1DM can
affect 25-(OH)D3 levels, which may be related to
oxidative stress caused by blood glucose fluctuations (2). Oxidative stress can lead to decreased
25-hydroxylase levels and 25-(OH)D3 synthesis (11). In addition, some pancreatic islets
can produce vitamin D, which binds to VDR to promote insulin
synthesis and secretion (28,29).
Oxidative stress can also damage the pancreatic islet cells
(2) and reduce vitamin D
production. The present study found that the RBG and HbA1C levels
of newly-diagnosed T1DM children were significantly higher than the
normal ranges and the levels of those children with established
T1DM, whereas the 25-(OH)D3 levels and the proportion of
children with normal 25-(OH)D3 levels were lower.
25-(OH)D3 levels were negatively correlated with RBG and
HbA1C, indicating that lower 25-(OH)D3 levels in
newly-diagnosed children with T1DM may be due to larger blood
glucose fluctuations and more serious oxidative stress damage,
which is consistent with the results of some studies (15,17,30).
In addition, Vitamin D levels are inversely correlated with
oxidative stress in patients with T1DM (31). Therefore, 25-(OH)D3 may
serve as an indirect indicator of oxidative stress in patients with
T1DM.
In addition, DKA may affect vitamin D metabolism,
and low vitamin D levels may contribute to a higher risk of DKA
presentation in patients with T1DM (13,32-34).
DKA can inactivate 1-α-hydroxylase, increase renal excretion of
VDBP and decrease vitamin D levels (32). The present study found that the RBG
and HbA1C levels in children with DKA/DK were significantly higher
than those in children without DKA/DK, and the 25-(OH)D3
levels and the proportion of children with normal
25-(OH)D3 levels were lower, which is also consistent
with the aforementioned study (32). Although, whether the patient case
was complicated with DKA/DK was not a variable affecting
25-(OH)D3 levels in the multiple linear regression
analysis, univariate analysis revealed significantly lower
25-(OH)D3 levels in children with DKA/DK, a clinically
meaningful difference. Thus, clinical attention to vitamin D status
in T1DM children with DKA/DK remains warranted.
Children with vitamin D insufficiency or deficiency
are more susceptible to infections (3,34).
When cases in children are complicated by infection, glycemic
control is affected, and acute complications such as DKA and DK are
more likely to occur, thus affecting 25-(OH)D3 levels.
In the present study, 106 of 132 co-infected children also
experienced complications with DKA/DK. The mean RBG level was as
high as 23.12 mmol/l, while the median 25-(OH)D3 level
was only 39.66 nmol/l, and the proportion of patients with
25-(OH)D3 <50 nmol/l was up to 78/106 (73.6%).
Therefore, prompt vitamin D supplementation in children with T1DM
may reduce the occurrence of infections and the risks of DKA and
DK.
Vitamin D deficiency can affect blood glucose
control and the development of metabolic diseases in patients with
T1DM, while vitamin D or active vitamin D supplementation is
effective in preventing the incident of T1DM and improving the
prognosis, including improving the function of residual pancreatic
β cells and insulin resistance, reducing blood glucose and HbA1c
levels in diabetic patients, and preventing and improving acute and
chronic complications (5,35-39).
Owing to the shorter observation duration in most studies, most
children with diabetes have not yet developed chronic complications
at the time of the study; therefore, relevant studies, long-term
observation and follow-up are lacking (25). However, as a relatively safe,
reliable, effective and inexpensive drug, vitamin D as an
additional therapy may open new perspectives for the control of
T1DM and the improvement of patient health (7,28).
The present study has certain limitations. First,
the main limitation was the lack of dynamic and long-term
monitoring of 25-(OH)D3 levels in the patients. Second,
the retrospective, observational design means that the findings
only support associations, not causality. Reverse causation (i.e.,
disease state affecting vitamin D levels rather than the converse)
and confounding by disease severity, acute metabolic stress (such
as DKA) and hospitalization status are important limitations that
must be considered when interpreting the observed associations
(17,29,30).
Specifically, it is plausible that the metabolic disturbances
associated with T1DM, particularly during acute presentation with
DKA, directly contribute to lower measured 25-(OH)D3
levels, rather than vitamin D deficiency predisposing to T1DM
onset. Third, the control group was not matched to the case group
for age, and significant age differences existed between groups.
Although adjustments were made for age in the logistic regression
models, residual confounding may persist. Additionally, the control
group (n=136) was substantially smaller than the case group
(n=757). Consequently, subgroup comparisons between T1DM subgroups
and their corresponding control subgroups (for example, stratifying
by age or sex) may be too underpowered to detect small-to-moderate
effects. Therefore, findings from underpowered subgroup analyses
should be interpreted cautiously and considered
hypothesis-generating rather than conclusive. Fourth, Due to the
retrospective design, several key covariates, including dietary
vitamin D/calcium intake, daily outdoor activity time, sun
protection habits and history of vitamin D supplementation, were
not routinely documented in the electronic medical records of
Shanxi Children's Hospital (Taiyuan, China). Covariates such as
BMI, family history of diabetes and birth history (for example,
prematurity) should have been recorded in standard clinical
practice; however, due to incomplete documentation, high missing
rates or unstructured text formats, they could not be reliably
extracted for analysis. An additional complexity was that BMI in
children must be interpreted via age- and sex-specific percentiles
or z-scores, requiring precise age, sex, height and weight data
fields that were often incomplete or inconsistently recorded in
this retrospective cohort. While such standardization is feasible
in well-curated prospective datasets, applying it here would risk
imputation errors, misclassification (especially at age extremes
where BMI changes rapidly) and further sample size reduction.
Forcing their inclusion would have led to a substantial reduction
in sample size and introduced selection bias. Notably, any residual
confounding from these unmeasured factors would likely bias the
effect estimate toward the null, as lower vitamin D levels tend to
cluster with unfavorable profiles of these variables (for example,
higher BMI, less outdoor activity and no supplementation), all of
which are independently associated with increased T1DM risk. Thus,
the observed association is likely conservative. Moreover, all
participants were recruited from the same geographic region during
a similar calendar period, and lifestyle factors are relatively
homogeneous across this pediatric population. Consequently,
differential confounding between groups is unlikely. Prospective
studies with standardized covariate collection are required to
counter this limitation.. Fifth, this was a single-center,
hospital-based study in a specific region of Shanxi Province.
Vitamin D status is strongly influenced by geographic, climatic and
local practice factors, which limits the generalizability of the
findings to other populations or outpatient settings. Finally, the
effects of vitamin D supplementation on patients with T1DM were not
investigated.
In conclusion, in the present single-center
retrospective case-control study, children with T1DM had
significantly lower serum 25-(OH)D3 levels and a higher
prevalence of vitamin D insufficiency or deficiency compared with
healthy controls, even after adjusting for age, sex and admission
quarter. These associations were particularly pronounced in
children with newly-diagnosed T1DM, those with DKA/DK and those
with concurrent infections. Age, admission quarter, disease
duration, sex, place of residence and HbA1c levels were
significantly associated with 25-(OH)D3 levels. However, due to the
observational design, the absence of matching for key confounders,
and the lack of data on important covariates such as BMI, dietary
intake and sun exposure, the findings support only associations and
cannot establish causality. The possibility of reverse causation,
whereby T1DM or its acute complications lead to reduced vitamin D
levels, remains a major alternative explanation. Given the various
benefits of vitamin D, the timely diagnosis and treatment of
vitamin D insufficiency and deficiency are necessary, especially in
infants and adolescents at the peak of growth and at high risk of
diabetes. Future high-quality, large-scale prospective
interventional RCTs and well-designed prospective cohort studies
with comprehensive covariate assessment are needed to fully
elucidate the role of vitamin D in T1DM, to clarify the direction
of the association and to guide clinical practice.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
JJW and XJC were responsible for the study
conceptualization and methodology. Collection of clinical data was
performed by JSW and XTF. Data analysis was performed by GQF, JNX
and XYY. JJW and JSW wrote the original manuscript. JJW and XJC
reviewed and edited the manuscript. The study was supervised by JJW
and XJC. All authors have read and approved the final manuscript.
JJW and XJC confirm the authenticity of all the raw data.
Ethical approval and consent to
participate
This study was approved by the Ethics Committee of
Shanxi Medical University (Taiyuan, China; approval no.
2020sll003-3) and the Ethics Committee of Shanxi Children's
Hospital/Shanxi Maternal and Child Health Hospital (Taiyuan, China;
approval no. IRB-WZ-2024-032). The requirement for written informed
patient consent was waived by the Ethics Committee of Shanxi
Medical University, since this study was a retrospective
investigation without any interventions, and no personal
information was involved.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Norris JM, Johnson RK and Stene LC: Type 1
diabetes-early life origins and changing epidemiology. Lancet
Diabetes Endocrinol. 8:226–238. 2020.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Meng X, Gong C, Cao B, Peng X, Wu D, Gu Y,
Wei L, Liang X, Liu M, Li W and Su C: Glucose fluctuations in
association with oxidative stress among children with T1DM:
Comparison of different phases. J Clin Endocrinol Metab.
100:1828–1836. 2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Charoenngam N and Holick MF: Immunologic
effects of vitamin D on human health and disease. Nutrients.
12(2097)2020.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Harinarayan CV: Vitamin D and diabetes
mellitus. Hormones (Athens). 13:163–181. 2014.PubMed/NCBI View Article : Google Scholar
|
|
5
|
He LP, Song YX, Zhu T, Gu W and Liu CW:
Progress in the relationship between Vitamin D deficiency and the
incidence of type 1 diabetes mellitus in children. J Diabetes Res.
2022(5953562)2022.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Shen L, Zhuang QS and Ji HF: Assessment of
vitamin D levels in type 1 and type 2 diabetes patients: Results
from metaanalysis. Mol Nutr Food Res. 60:1059–1067. 2016.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Kawahara T, Okada Y and Tanaka Y: Vitamin
D efficacy in type 1 and type 2 diabetes. J Bone Miner Metab.
42:438–446. 2024.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Liu C, Wang J, Wan Y, Xia X, Pan J, Gu W
and Li M: Serum vitamin D deficiency in children and adolescents is
associated with type 1 diabetes mellitus. Endocr Connect.
7:1275–1279. 2018.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chakhtoura M and Azar ST: The role of
vitamin d deficiency in the incidence, progression, and
complications of type 1 diabetes mellitus. Int J Endocrinol.
2013(148673)2013.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Abd-Allah SH, Pasha HF, Hagrass HA and
Alghobashy AA: Vitamin D status and vitamin D receptor gene
polymorphisms and susceptibility to type 1 diabetes in Egyptian
children. Gene. 536:430–434. 2014.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Jain SK, Parsanathan R, Achari AE,
Kanikarla-Marie P and Bocchini JA Jr: Glutathione Stimulates
Vitamin D Regulatory and Glucose-metabolism genes, lowers oxidative
stress and inflammation, and increases 25-Hydroxy-vitamin D levels
in blood: A novel approach to treat 25-hydroxyvitamin D deficiency.
Antioxid Redox Signal. 29:1792–1807. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Kandemir N, Vuralli D, Ozon A, Gonc N,
Ardicli D, Jalilova L, Gulcek ON and Alikasifoglu A: Epidemiology
of type 1 diabetes mellitus in children and adolescents: A 50-year,
single-center experience. J Diabetes. 16(e13562)2024.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Devidayal Singh MK, Sachdeva N, Singhi S,
Attri SV, Jayashree M and Bhalla AK: Vitamin D levels during and
after resolution of ketoacidosis in children with new onset Type 1
diabetes. Diabet Med. 30:829–834. 2013.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Sracic K, Uli N and Heksch R: Change in
age of diagnosis and demographics of type 1 diabetes mellitus
during the COVID-19 Era. Pediatr Diabetes.
2025(7276579)2025.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Borkar VV, Devidayal Verma S and Bhalla
AK: Low levels of vitamin D in North Indian children with newly
diagnosed type 1 diabetes. Pediatr Diabetes. 11:345–350.
2010.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Mäkinen M, Mykkänen J, Koskinen M, Simell
V, Veijola R, Hyöty H, Ilonen J, Knip M, Simell O and Toppari J:
Serum 25-Hydroxyvitamin D concentrations in children progressing to
autoimmunity and clinical Type 1 diabetes. J Clin Endocrinol Metab.
101:723–729. 2016.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Greer RM, Portelli SL, Hung BS, Cleghorn
GJ, McMahon SK, Batch JA and Conwell LS: Serum vitamin D levels are
lower in Australian children and adolescents with type 1 diabetes
than in children without diabetes. Pediatr Diabetes. 14:31–41.
2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Simpson M, Brady H, Yin X, Seifert J,
Barriga K, Hoffman M, Bugawan T, Barón AE, Sokol RJ, Eisenbarth G,
et al: No association of vitamin D intake or 25-hydroxyvitamin D
levels in childhood with risk of islet autoimmunity and type 1
diabetes: The diabetes autoimmunity study in the Young (DAISY).
Diabetologia. 54:2779–2788. 2011.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Silvis K, Aronsson CA, Liu X, Uusitalo U,
Yang J, Tamura R, Lernmark Å, Rewers M, Hagopian W, She JX, et al:
Maternal dietary supplement use and development of islet
autoimmunity in the offspring: TEDDY study. Pediatr Diabetes.
20:86–92. 2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Zipitis CS and Akobeng AK: Vitamin D
supplementation in early childhood and risk of type 1 diabetes: A
systematic review and meta-analysis. Arch Dis Child. 93:512–517.
2008.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Dong JY, Zhang WG, Chen JJ, Zhang ZL, Han
SF and Qin LQ: Vitamin D intake and risk of type 1 diabetes: A
meta-analysis of observational studies. Nutrients. 5:3551–3562.
2013.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Holick MF: The vitamin D deficiency
pandemic: Approaches for diagnosis, treatment and prevention. Rev
Endocr Metab Disord. 18:153–165. 2017.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Littorin B, Blom P, Schölin A, Arnqvist
HJ, Blohmé G, Bolinder J, Ekbom-Schnell A, Eriksson JW,
Gudbjörnsdottir S, Nyström L, et al: Lower levels of plasma
25-hydroxyvitamin D among young adults at diagnosis of autoimmune
type 1 diabetes compared with control subjects: Results from the
nationwide Diabetes Incidence Study in Sweden (DISS). Diabetologia.
49:2847–2852. 2006.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Xu R-B, Gao D, Wang Z-H, Zou Z-Y, Hu P-J,
Ma J and Song Y: Analysis of the current status of outdoor activity
time of Chinese students in 2016. Chin J Child Health Care.
26:254–257. 2018.
|
|
25
|
Katsarou A, Gudbjörnsdottir S, Rawshani A,
Dabelea D, Bonifacio E, Anderson BJ, Jacobsen LM, Schatz DA and
Lernmark Å: Type 1 diabetes mellitus. Nat Rev Dis Primers.
3(17016)2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Weng J, Zhou Z, Guo L, Zhu D, Ji L, Luo X,
Mu Y and Jia W: T1D China Study Group. Incidence of type 1 diabetes
in China, 2010-13: Population based study. BMJ.
360(j5295)2018.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Patterson CC, Dahlquist GG, Gyürüs E,
Green A and Soltész G: EURODIAB Study Group. Incidence trends for
childhood type 1 diabetes in Europe during 1989-2003 and predicted
new cases 2005-20: A multicentre prospective registration study.
Lancet. 373:2027–2033. 2009.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Park CY, Shin S and Han SN: Multifaceted
roles of Vitamin D for diabetes: From immunomodulatory functions to
metabolic regulations. Nutrients. 16(3185)2024.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Maestro B, Dávila N, Carranza MC and Calle
C: Identification of a Vitamin D response element in the human
insulin receptor gene promoter. J Steroid Biochem Mol Biol.
84:223–230. 2003.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Bouichrat N, Benyakhef S, Assarrar I,
Draoui N, Lazreg Y, Abda N, Rouf S and Latrech H: Vitamin D status
in diabetic Moroccan children and adolescents: A Case-control
study. Rev Diabet Stud. 19:1–7. 2023.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Šebeková K, Stürmer M, Fazeli G, Bahner U,
Stäb F and Heidland A: Is vitamin D deficiency related to
accumulation of advanced glycation end products, markers of
inflammation, and oxidative stress in diabetic subjects? Biomed Res
Int. 2015(958097)2015.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Iqbal A, Hussain A, Iqbal A and Kumar V:
Correlation between Vitamin D deficiency and diabetic ketoacidosis.
Cureus. 11(e4497)2019.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Huynh T, Greer RM, Nyunt O, Bowling F,
Cowley D, Leong GM, Cotterill AM and Harris M: The association
between ketoacidosis and 25(OH)-vitamin D levels at presentation in
children with type 1 diabetes mellitus. Pediatr Diabetes. 10:38–43.
2009.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Petkova GS, Mineva EN and Botsova VT:
Clinical study of Vitamin D levels in Hospitalized children with
acute respiratory infections. Pediatr Rep. 16:1034–1041.
2024.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Grammatiki M, Karras S and Kotsa K: The
role of vitamin D in the pathogenesis and treatment of diabetes
mellitus: A narrative review. Hormones (Athens). 18:37–48.
2019.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Ordooei M, Shojaoddiny-Ardekani A,
Hoseinipoor SH, Miroliai M and Zare-Zardini H: Effect of vitamin D
on HbA1c levels of children and adolescents with diabetes mellitus
type 1. Minerva Pediatr. 69:391–395. 2017.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Al Shaikh A and Al Zahrani AM: Impact of
vitamin D status on cardiometabolic complications among children
and adolescents with type 1 diabetes mellitus. J Clin Res Pediatr
Endocrinol. 8:48–54. 2016.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Savastio S, Cadario F, Genoni G, Bellomo
G, Bagnati M, Secco G, Picchi R, Giglione E and Bona G: Vitamin D
deficiency and glycemic status in children and adolescents with
type 1 diabetes mellitus. PLoS One. 11(e0162554)2016.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Treiber G, Prietl B, Fröhlich-Reiterer E,
Lechner E, Ribitsch A, Fritsch M, Rami-Merhar B,
Steigleder-Schweiger C, Graninger W, Borkenstein M and Pieber TR:
Cholecalciferol supplementation improves suppressive capacity of
regulatory T-cells in young patients with new-onset type 1 diabetes
mellitus-A randomized clinical trial. Clin Immunol. 16:217–224.
2015.PubMed/NCBI View Article : Google Scholar
|