Introduction
Lung cancer ranks among the most common malignancies
worldwide in terms of both incidence and mortality, with non-small
cell lung cancer (NSCLC) accounting for the majority of cases. In
recent years, immune checkpoint inhibitors (ICIs), particularly
monoclonal antibodies targeting programmed cell death protein 1
(PD-1) and its ligand (PD-L1), have revolutionized the treatment
landscape for advanced NSCLC. By blocking the PD-1/PD-L1 signaling
pathway, these agents release inhibitory effects on T cells and
enhance antitumor immune responses, leading to significant and
durable survival benefits for patients (1). Tislelizumab is a humanized IgG4
anti-PD-1 monoclonal antibody. Its Fc segment has been engineered
to minimize binding to FcγR on macrophages, thereby reducing
antibody-dependent cellular phagocytosis and potentially mitigating
effector T-cell exhaustion, which may enhance antitumor activity
(2,3). It has demonstrated promising efficacy
and a manageable safety profile across various malignancies,
including advanced squamous and non-squamous NSCLC. However, like
other ICIs, tislelizumab can also induce a spectrum of
immune-related adverse events (irAEs) (4). Although management guidelines for
irAEs are continually being refined, clinical practice still faces
substantial challenges (5). This
article reports the case of a 70-year-old female with advanced lung
squamous cell carcinoma who developed severe dual irAEs involving
the liver and skin following treatment with nab-paclitaxel,
carboplatin and tislelizumab. The case aims to provide an in-depth
analysis of the clinical features, potential mechanisms and
management strategies of this rare dual grade 4 toxicity, hoping to
alert and inform clinicians in the recognition and management of
similar complex cases.
Case presentation
A 70-year-old non-smoking female patient was
diagnosed at Liaohua Hospital (Liaoyang, China) with
non-keratinizing squamous cell carcinoma of the right upper lobe
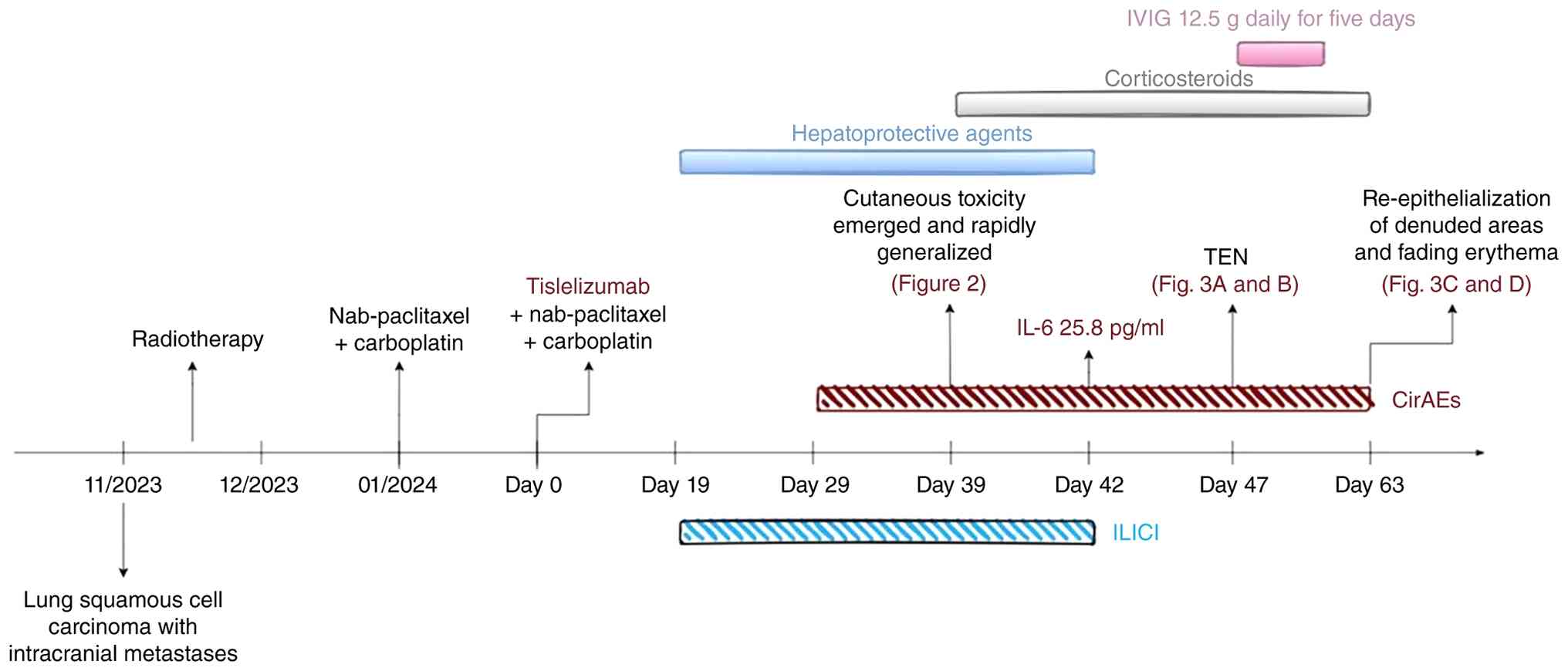
with multiple intracranial metastases in November 2023. After
completing radiotherapy in December 2023, first-line chemotherapy
was initiated in January 2024: Nab-paclitaxel (100 mg on day 1, 200
mg on day 8) plus carboplatin (450 mg on day 1), every 3 weeks. The
first cycle was well tolerated with no adverse events. At 21 days
after the first-line chemotherapy, the patient started the second
cycle of the same regimen with the addition of intravenous
tislelizumab 200 mg (Fig. 1); this
day was designated as day 0. Baseline laboratory tests before
treatment showed normal liver function (Table I) and no skin rash. On day 19, the
patient developed a sharp elevation in liver enzymes: Alanine
transaminase (ALT), 1,741.6 U/l (normal range: 7-40 U/l); aspartate
transaminase (AST), 1,310 U/l (normal range: 13-35 U/l). Despite
the initiation of hepatoprotective agents-bicyclol (50 mg three
times daily), polyenylphosphatidylcholine (300 mg three times
daily), and ursodeoxycholic acid (250 mg three times daily)-the
biochemical abnormalities persisted, accompanied by elevated total
bile acids, indicating mixed hepatocellular and cholestatic liver
injury. On day 29, the patient experienced unexplained low-grade
fever (37.8˚C); IL-6 was normal (normal range: <5.9 pg/ml by
chemiluminescence method). After spontaneous defervescence,
scattered purpuric macules and papules with pruritus appeared on
the occipital region, face and abdomen. Oral cetirizine was
ineffective and the rash gradually spread to the trunk, limbs, neck
and scalp, with worsening pruritus. On day 39, yellowish vesicles
developed, which ruptured upon scratching (Fig. 2). Intravenous methylprednisolone
(120 mg; 2 mg/kg/day) was given for 3 days, without improvement. On
day 42, the patient was transferred to the dermatology department,
where the Severity-of-Illness Score for Toxic Epidermal Necrolysis
(SCORTEN) score was determined to be 4 (age ≥40 years, malignancy,
heart rate ≥120 bpm, involved body surface area ≥10% on day 1),
indicating a high risk of death from toxic epidermal necrolysis
(TEN). At that time, liver function had returned to near normal
(ALT, 53 U/l; AST, 81 U/l), but IL-6 was markedly elevated to 25.8
pg/ml. Comprehensive treatment was initiated: Methylprednisolone
was adjusted to 60 mg (1 mg/kg)/day, combined with antihistamines,
gastric mucosal protectants, topical emollients and antiseptic
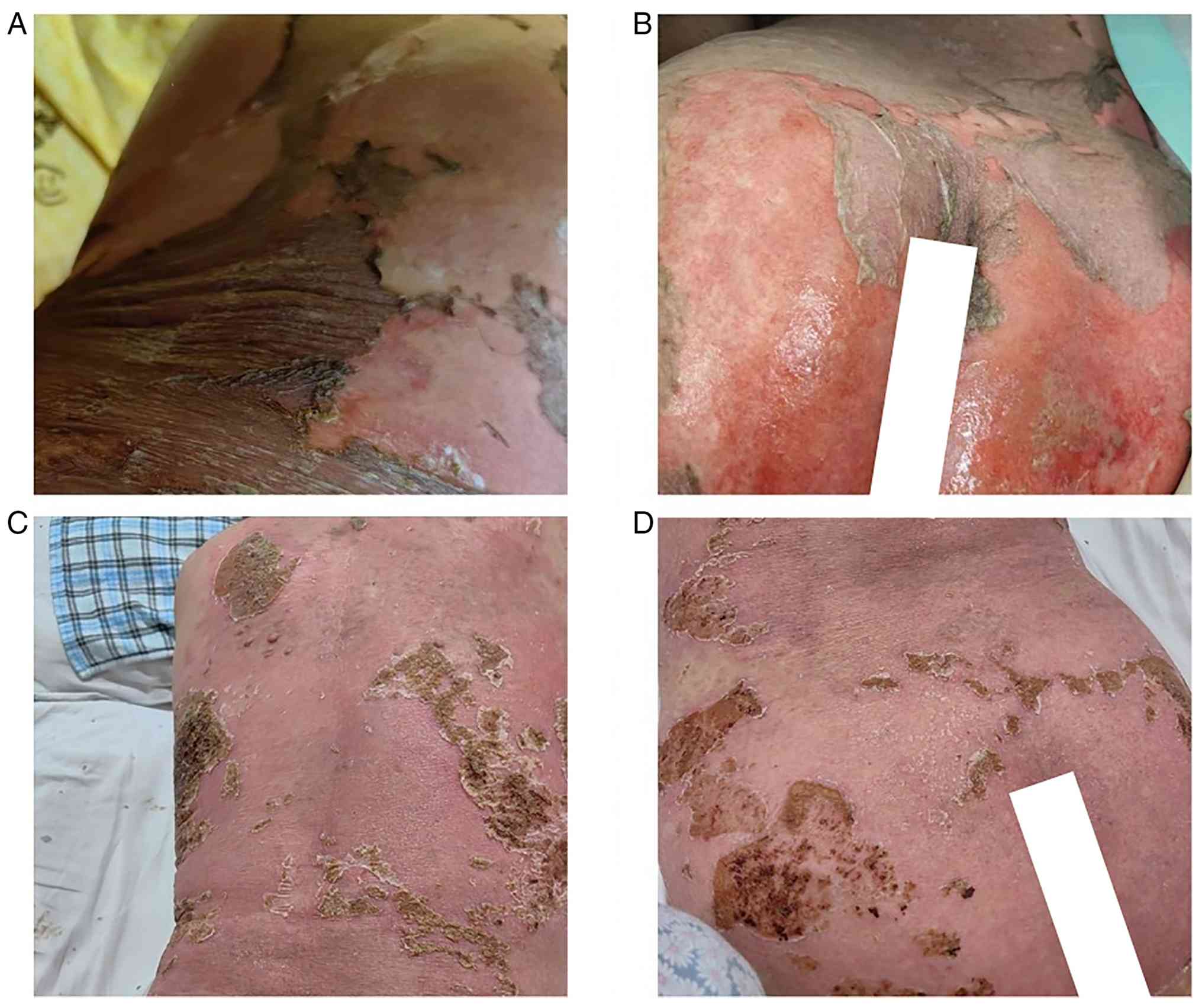
mouthwash. Because the TEN-like skin lesions continued to progress
(widespread epidermal detachment involving ~50% of body surface
area, positive Nikolsky sign) (Fig.
3A and B), intravenous
immunoglobulin (IVIG) was added on day 47 at a dose of 12.5 g/day
(0.25 g/kg/day) for 5 days. After treatment, IL-6 gradually
decreased, reaching 5.2 pg/ml on day 57, and liver function
remained normal. The glucocorticoid was tapered to 40 mg/day
orally. On day 63, the skin lesions had markedly improved, with
complete re-epithelialization of the eroded areas and resolution of
erythema (Fig. 3C and D). The patient was discharged in a stable
condition. After discharge, the patient was followed up monthly. No
further laboratory or imaging examinations were performed. The
patient received no additional anti-tumor therapy and was managed
with palliative symptomatic care only. The patient died in July
2024. No autopsy was performed.
 | Table ILaboratory values of the patient over
the clinical course. |
Table I
Laboratory values of the patient over
the clinical course.
| Laboratory value | Normal range | Day 0 | Day 19 | Day 24 | Day 29 | Day 32 | Day 39 | Day 42 | Day 50 | Day 57 |
|---|
| TBiL, µmol/l | 0-21 | 5.7 | 27.8 | 73.4 | 70.1 | 61.8 | 83 | 30.4 | 28.7 | 24.8 |
| DBiL, µmol/l | 0-6.84 | 1.5 | 15.8 | 48.5 | 47.5 | 42.5 | 54.9 | 21.9 | 18.8 | 15.2 |
| TBA, µmol/l | 0-12 | 3.3 | 9.8 | 30.9 | 77.6 | 122 | 8.2 | 6 | 5 | 9 |
| ALT, U/l | 7-40 | 26.9 | 1741.6 | 641.1 | 204.5 | 122.9 | 66.4 | 53 | 46 | 57 |
| AST, U/l | 13-35 | 18 | 1310 | 1303 | 752 | 337 | 108 | 81 | 38 | 34 |
| ALP, U/l | 50-135 | 67 | 133 | 144 | 151 | 130 | 159 | 77 | 68 | 83 |
| GGT, U/l | 7-45 | 22.5 | 211.3 | 316 | 425.1 | 365.1 | 343.5 | 250 | 124 | 97 |
| IL-6, pg/ml | <5.9 | - | - | - | 4.04 | - | - | 25.8 | - | 5.2 |
| CRP, mg/l | 0-6 | - | - | - | 9.89 | - | 56.2 | 19.29 | 18.8 | 3.7 |
Discussion
Immunotherapy has revolutionized the cancer
treatment landscape over the past few decades. With the
increasingly widespread application of ICIs in oncology, there has
been a corresponding significant rise in reports of irAEs (5). Most irAEs occur in barrier organs,
including the skin, gastrointestinal tract, liver and lungs
(6). Unlike adverse reactions
induced by chemotherapy or targeted therapy, irAEs are challenging
to predict in terms of both severity and timing. These toxicities
may lead to treatment delays or discontinuation and can even be
life-threatening (7). Notably, the
occurrence of irAEs is closely associated with the efficacy of
ICIs. Certain studies suggest that patients who develop irAEs are
more likely to mount a potent antitumor response. For instance, a
retrospective study of cancer patients treated with ICIs indicated
that the development of cutaneous irAEs (cirAEs) served as a
significant protective factor for treatment response and overall
survival (8). Similar findings
have been observed in multisystem irAEs. An analysis of patients
with NSCLC treated with ICIs targeting both PD-1 and programmed
death-ligand 1 (PD-L1) suggested that multisystem irAEs were
associated with improved survival following immunotherapy (9). Another retrospective study in
patients with stage IV SCLC receiving PD-(L)1 inhibitors
demonstrated that those who developed multisystem irAEs had longer
survival compared to those with single-system irAEs or no irAEs-an
association that persisted even after the administration of
systemic corticosteroids for irAE management (10). Therefore, early recognition, timely
intervention and multidisciplinary collaboration are crucial in the
management of irAEs to improve patient outcomes.
Immune-mediated liver injury caused by ICIs (ILICI)
is one of the commonly reported irAEs (11-13).
The mechanisms driving ILICI are not yet fully elucidated. The
liver possesses a unique immune profile, typically maintained in a
state of immune tolerance (14-17),
achieved through anti-inflammatory responses by both
non-parenchymal and parenchymal cells under homeostatic conditions,
along with checkpoint molecule expression across various cell
subsets. After ICI blockade, this hepatic immune tolerance may be
compromised, rendering the organ more susceptible to tissue
inflammation. Data indicate that immune-related acute hepatitis
occurs in ~18% of patients receiving combined anti-PD-1 and
anti-cytotoxic T-lymphocyte-associated protein 4 monoclonal
antibodies, whereas the incidence drops to 1-4% with PD-1
inhibitors alone; severe fatal hepatotoxicity is relatively rare in
clinical practice (17,18). Liver injury induced by
anti-PD-1/PD-L1 monoclonal antibodies primarily manifests as
lobular hepatitis, characterized by inflammatory cell infiltration
within the lobules. The most common clinical presentations are
elevated ALT and AST levels, occasionally accompanied by abnormal
bilirubin (19). Management of
PD-1/PD-L1 inhibitor-induced liver injury primarily follows
guidelines from authoritative oncology and hepatology societies
(20-23).
For grade 1-2 liver injury, the emphasis is on identifying and
excluding other potential causative factors, closely monitoring
liver function and temporarily withholding ICIs. For grade 3-4
hepatotoxicity, ICIs should be discontinued immediately,
hospitalization considered and corticosteroid therapy initiated. In
the present case, the patient developed sharply elevated ALT and
AST along with significantly increased total bile acids after the
second cycle of combined PD-1 inhibitor therapy, suggesting mixed
liver injury. Despite prompt administration of multiple
hepatoprotective agents (such as bicyclol, polyene
phosphatidylcholine and ursodeoxycholic acid), liver enzymes
continued to fluctuate until corticosteroids were introduced,
leading to gradual recovery. This course underscores the potential
severity of immune-mediated hepatotoxicity and its poor
responsiveness to conventional liver-protective therapies. It is
noteworthy that hepatotoxicity is closely associated with T-cell
overactivation and cytokine release, making early recognition and
steroid intervention critical for controlling disease
progression.
CirAEs are among the earliest and most frequently
observed irAEs (6). Mild to
moderate skin irAEs most commonly include pruritus, nonspecific
maculopapular rash, lichenoid/lichen planus-like eruptions,
psoriasiform dermatitis and eczematous rash, followed by vitiligo
and alopecia. Severe cutaneous irAEs encompass bullous pemphigoid,
Stevens-Johnson syndrome and TEN (24). Notably, significant associations
exist between specific cirAE morphological features and types of
irAEs (25); for instance,
mucositis has been linked with overall irAE risk, gastrointestinal
irAEs and gastroenteritis, while psoriasis is associated with
endocrine irAEs. TEN is a rare yet life-threatening T-cell-mediated
severe cutaneous adverse reaction with substantial mortality
(26). TEN induced by PD-1
inhibitors exhibits sustained immune hyperactivation distinct from
conventional drug-induced TEN, rendering monotherapy with
glucocorticoids often inadequate to halt progression (27). For severe cases, IVIG combined with
adjunctive immunosuppressants such as infliximab or cyclosporine
should be considered (28). In the
present case, the patient presented with generalized purpuric
macules, ecchymoses and blisters that progressed to extensive
epidermal detachment, consistent with TEN-like manifestations.
Markedly elevated IL-6 levels suggested involvement of a cytokine
storm in the pathogenesis. Treatment with methylprednisolone
combined with IVIG played a key role in gradually controlling the
condition and promoting re-epithelialization. This case illustrates
that multimodal treatment strategies, including immunosuppression
and supportive care, are indispensable for managing severe
cutaneous irAEs.
Unfortunately, liver and skin biopsies were not
performed due to the patient's financial constraints.
Histopathological examination would have provided definitive
evidence of immune-mediated injury: In the liver, interface
hepatitis with lymphocytic infiltration, lobular necroinflammation
and exclusion of other etiologies (e.g., biliary obstruction or
viral inclusions) (11); in the
skin, full-thickness epidermal necrosis, sparse lymphocytic
infiltrate (typical of TEN) and distinction from other severe
cutaneous reactions such as acute generalized exanthematous
pustulosis or linear IgA disease (26). The absence of tissue confirmation
modestly reduces diagnostic certainty for both hepatotoxicity
(grade 4) and TEN, as rare confounding pathologies [e.g.,
drug-induced autoimmune-like hepatitis (29) or paraneoplastic pemphigus (30)] cannot be formally ruled out.
Nevertheless, the triad of a robust temporal association with
tislelizumab, systematic exclusion of common alternative etiologies
(viral, autoimmune, chemotherapy-alone, drug reaction with
eosinophilia and systemic symptoms) (31), and a marked clinical response to
corticosteroids combined with IVIG supports the clinical diagnoses
with a high degree of confidence. Non-invasive alternatives, while
not equivalent to histology, include serial serum biomarkers
(elevated IL-6 and CRP) and the SCORTEN score (32) (score 4 in this case), which
collectively strengthen the clinical reasoning. Future studies
should validate non-invasive panels as surrogates for biopsy in
similar resource-limited settings. Although older patients are
traditionally considered less tolerant to chemotherapy, the
mechanism of action of ICIs differs fundamentally from that of
chemotherapeutic agents, relying on T-cell-mediated antitumor
immune activation (33). Multiple
studies have shown that age itself does not significantly influence
the incidence of irAEs or overall survival (24-37);
however, combination with chemotherapy may substantially increase
the severity and diversity of irAEs (38). Therefore, when using combined
immunotherapy in elderly populations, heightened vigilance for
multisystem toxicity and individualized risk management are
essential.
In conclusion, this case appears to be the first to
document the sequential development of grade 4 drug-induced liver
injury and TEN induced by tislelizumab. The patient was
successfully managed with glucocorticoids combined with IVIG.
Further prospective studies are warranted to optimize immunotherapy
strategies and improve the management of irAEs.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
ZW was involved in conceptualization, data curation,
writing-original draft and writing-review & editing. CL
performed data curation and investigation. LY contributed to
conceptualization and writing-review & editing. ZW and CL
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012.PubMed/NCBI View
Article : Google Scholar
|
|
2
|
Lee A and Keam SJ: Tislelizumab: First
approval. Drugs. 80:617–624. 2020.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Zhang L, Geng Z, Hao B and Geng Q:
Tislelizumab: A modified anti-tumor programmed death receptor 1
antibody. Cancer Control. 29(10732748221111296)2022.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Li C, Ding Y, Cai S, Liu BC and Wang X:
Post-marketing safety concerns with Tislelizumab: A
disproportionality analysis of the FDA adverse event reporting
system. Front Immunol. 16(1596842)2025.PubMed/NCBI View Article : Google Scholar
|
|
5
|
No authors listed. Immune-related adverse
events of checkpoint inhibitors. Nat Rev Dis Primers.
6(39)2020.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Wang SJ, Dougan SK and Dougan M: Immune
mechanisms of toxicity from checkpoint inhibitors. Trends Cancer.
9:543–553. 2023.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Martins F, Sofiya L, Sykiotis GP, Lamine
F, Maillard M, Fraga M, Shabafrouz K, Ribi C, Cairoli A,
Guex-Crosier Y, et al: Adverse effects of immune-checkpoint
inhibitors: Epidemiology, management and surveillance. Nat Rev Clin
Oncol. 16:563–580. 2019.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Tang K, Seo J, Tiu BC, Le TK, Pahalyants
V, Raval NS, Ugwu-Dike PO, Zubiri L, Naranbhai V, Carrington M, et
al: Association of cutaneous immune-related adverse events with
increased survival in patients treated with anti-programmed cell
death 1 and anti-programmed cell death ligand 1 therapy. JAMA
Dermatol. 158:189–193. 2022.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Shankar B, Zhang J, Naqash AR, Forde PM,
Feliciano JL, Marrone KA, Ettinger DS, Hann CL, Brahmer JR,
Ricciuti B, et al: Multisystem immune-related adverse events
associated with immune checkpoint inhibitors for treatment of
non-small cell lung cancer. JAMA Oncol. 6:1952–1956.
2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zhang J, Gao A, Wang S and Sun Y, Wu J,
Wang D, Ge Y, Li J, Sun H, Cheng Q and Sun Y: Correlation between
immune-related adverse events and efficacy of PD-(L)1 inhibitors in
small cell lung cancer: A multi-center retrospective study. Respir
Res. 25(256)2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Gudd CLC, Sheth R, Thursz MR,
Triantafyllou E and Possamai LA: Immune checkpoint
inhibitor-induced liver injury. Semin Liver Dis. 43:402–417.
2023.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Larkin J, Hodi FS and Wolchok JD: Combined
nivolumab and ipilimumab or monotherapy in untreated melanoma. N
Engl J Med. 373:1270–1271. 2015.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Robert C, Schachter J, Long GV, Arance A,
Grob JJ, Mortier L, Daud A, Carlino MS, McNeil C, Lotem M, et al:
Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med.
372:2521–2532. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Shojaie L, Bogdanov JM, Alavifard H,
Mohamed MG, Baktash A, Ali M, Mahov S, Murray S, Kanel GC, Liu ZX,
et al: Innate and adaptive immune cell interaction drives
inflammasome activation and hepatocyte apoptosis in murine liver
injury from immune checkpoint inhibitors. Cell Death Dis.
15(140)2024.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Gudd CLC and Possamai LA: The role of
myeloid cells in hepatotoxicity related to cancer immunotherapy.
Cancers (Basel). 14(1913)2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Triantafyllou E, Woollard KJ, McPhail MJW,
Antoniades CG and Possamai LA: The role of monocytes and
macrophages in acute and acute-on-chronic liver failure. Front
Immunol. 9(2948)2018.PubMed/NCBI View Article : Google Scholar
|
|
17
|
De Martin E, Michot JM, Papouin B,
Champiat S, Mateus C, Lambotte O, Roche B, Antonini TM, Coilly A,
Laghouati S, et al: Characterization of liver injury induced by
cancer immunotherapy using immune checkpoint inhibitors. J Hepatol.
68:1181–1190. 2018.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Wang DY, Salem JE, Cohen JV, Chandra S,
Menzer C, Ye F, Zhao S, Das S, Beckermann KE, Ha L, et al: Fatal
toxic effects associated with immune checkpoint inhibitors: A
systematic review and meta-analysis. JAMA Oncol. 4:1721–1728.
2018.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Yue M, Li C and Li G: New advances in the
study of PD-1/PD-L1 inhibitors-induced liver injury. Int
Immunopharmacol. 131(111799)2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Haanen J, Obeid M, Spain L, Carbonnel F,
Wang Y, Robert C, Lyon AR, Wick W, Kostine M, Peters S, et al:
Management of toxicities from immunotherapy: ESMO clinical practice
guideline for diagnosis, treatment and follow-up. Ann Oncol.
33:1217–1238. 2022.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Thompson JA, Schneider BJ, Brahmer J, Zaid
MA, Achufusi A, Armand P, Berkenstock MK, Bermas B, Braaten T,
Budde LE, et al: NCCN guidelines® insights: Management
of immunotherapy-related toxicities, version 2.2024. J Natl Compr
Canc Netw. 22:582–592. 2024.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Schneider BJ, Naidoo J, Santomasso BD,
Lacchetti C, Adkins S, Anadkat M, Atkins MB, Brassil KJ, Caterino
JM, Chau I, et al: Management of immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: ASCO
guideline update. J Clin Oncol. 39:4073–4126. 2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Dougan M, Wang Y, Rubio-Tapia A and Lim
JK: AGA clinical practice update on diagnosis and management of
immune checkpoint inhibitor colitis and hepatitis: Expert review.
Gastroenterology. 160:1384–1393. 2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kaunitz GJ, Loss M, Rizvi H, Ravi S, Cuda
JD, Bleich KB, Esandrio J, Sander I, Le DT, Diaz LA Jr, et al:
Cutaneous eruptions in patients receiving immune checkpoint
blockade: Clinicopathologic analysis of the nonlichenoid histologic
pattern. Am J Surg Pathol. 41:1381–1389. 2017.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Thompson LL, Krasnow NA, Chang MS, Yoon J,
Li EB, Polyakov NJ, Molina GE, Said JT, Huang K, Kuchroo JR, et al:
Patterns of cutaneous and noncutaneous immune-related adverse
events among patients with advanced cancer. JAMA Dermatol.
157:577–582. 2021.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Harr T and French LE: Toxic epidermal
necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis.
5(39)2010.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Molina GE, Yu Z, Foreman RK, Reynolds KL
and Chen ST: Generalized bullous mucocutaneous eruption mimicking
Stevens-Johnson syndrome in the setting of immune checkpoint
inhibition: A multicenter case series. J Am Acad Dermatol.
83:1475–1477. 2020.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Storgard R and Markova A: Cutaneous
hypersensitivity reactions to immune checkpoint inhibitors. J
Allergy Clin Immunol Pract. 12:1132–1136. 2024.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Andrade RJ, Aithal GP, de Boer YS, Liberal
R, Gerbes A, Regev A, Terziroli Beretta-Piccoli B, Schramm C,
Kleiner DE, De Martin E, et al: Nomenclature, diagnosis and
management of drug-induced autoimmune-like hepatitis (DI-ALH): An
expert opinion meeting report. J Hepatol. 79:853–866.
2023.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Huang S, Anderson HJ and Lee JB:
Paraneoplastic pemphigus/paraneoplastic autoimmune multiorgan
syndrome: Part II. Diagnosis and management. J Am Acad Dermatol.
91:13–22. 2024.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Sullivan RJ and Weber JS: Immune-related
toxicities of checkpoint inhibitors: Mechanisms and mitigation
strategies. Nat Rev Drug Discov. 21:495–508. 2022.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Bastuji-Garin S, Fouchard N, Bertocchi M,
Roujeau JC, Revuz J and Wolkenstein P: SCORTEN: A
severity-of-illness score for toxic epidermal necrolysis. J Invest
Dermatol. 115:149–153. 2000.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Okiyama N and Tanaka R: Immune-related
adverse events in various organs caused by immune checkpoint
inhibitors. Allergol Int. 71:169–178. 2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Wong SK, Nebhan CA and Johnson DB: Impact
of patient age on clinical efficacy and toxicity of checkpoint
inhibitor therapy. Front Immunol. 12(786046)2021.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Ferrara R, Mezquita L, Auclin E, Chaput N
and Besse B: Immunosenescence and immunecheckpoint inhibitors in
non-small cell lung cancer patients: Does age really matter? Cancer
Treat Rev. 60:60–68. 2017.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Hayashi-Tanner Y, Polewski PJ, Gaddam M,
Fisher NR, Kovacs AJ and Marinier DE: Immune checkpoint inhibitor
toxicity and associated outcomes in older patients with cancer. J
Geriatr Oncol. 13:1011–1016. 2022.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Yang F, Markovic SN, Molina JR,
Halfdanarson TR, Pagliaro LC, Chintakuntlawar AV, Li R, Wei J, Wang
L, Liu B, et al: Association of sex, age, and eastern cooperative
oncology group performance status with survival benefit of cancer
immunotherapy in randomized clinical trials: A systematic review
and meta-analysis. JAMA Netw Open. 3(e2012534)2020.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Zhou X, Yao Z, Bai H, Duan J, Wang Z, Wang
X, Zhang X, Xu J, Fei K, Zhang Z, et al: Treatment-related adverse
events of PD-1 and PD-L1 inhibitor-based combination therapies in
clinical trials: A systematic review and meta-analysis. Lancet
Oncol. 22:1265–1274. 2021.PubMed/NCBI View Article : Google Scholar
|