Introduction
Painless gastroscopy is commonly used for diagnosing
and treating gastrointestinal diseases (1). However, hypoxemia is a frequent
complication with reported incidences ranging from 1.8 to 69%
(2). This variation is influenced
by factors such as sedation depth, patient risk profiles,
oxygenation strategies and monitoring practices (3). Several factors contribute to the risk
of hypoxemia, including respiratory depression caused by sedatives,
pharyngeal airway obstruction, reduced chest wall compliance in
obesity and airway obstruction from the endoscope (4). Severe or prolonged hypoxemia can lead
to serious complications, such as myocardial ischemia, arrhythmias
and cerebral hypoxia (5). As a
result, assessing hypoxemia risk before the procedure is essential
for enabling early interventions such as optimal patient
positioning, airway management, tailored oxygen delivery and
precise sedative titration, all of which improve procedural safety
and patient outcomes.
Ultrasonography has become an important tool in
clinical airway evaluation due to its real-time imaging
capabilities, dynamic airway monitoring, and operator-independent
measurements (6,7). Ultrasound can also capture dynamic
airway changes under sedation, which are closely linked to
desaturation during procedures (8). Consequently, ultrasound has gained
prominence in pre-anesthesia difficult-airway assessment (9-10). A
growing body of evidence supports the diagnostic utility of
sonographic upper-airway parameters, such as distance from the skin
to the hyoid bone (DSH), distance from the skin to the epiglottis
(DSE), distance from the skin to the anterior commissure of the
vocal cords (DSAC), tongue thickness (TT), hyoid-mental distance
(HMD) and anterior condylar translation (ACT, a functional
surrogate of mandibular mobility), for predicting difficult
laryngoscopy or intubation (11-13).
Notwithstanding these strengths, to the best of our knowledge, the
direct application of airway ultrasound to predict hypoxemia during
painless gastroscopy has been insufficiently explored, and robust,
endoscopy-specific predictive models remain scarce.
The present study aimed to determine whether
sonographic measurements can serve as reliable predictors of
hypoxemia risk. We hypothesize that integrating multiple ultrasound
parameters with clinical variables into a prediction model will
offer a more accurate assessment, ultimately improving safety and
guiding individualized oxygenation management during painless
gastroscopy.
Materials and methods
Patient cohort and protocol
The present study was registered at the China
Clinical Trial Registry (trial no. ChiCTR2500109627) on September
23 of 2025. The present study was reviewed and approved by the
Medical Ethics Committee of Jiangnan University Medical Center
(Wuxi, China; approval no. 2024Y329), and all participants gave
informed consent. This prospective observational study was
conducted at the Second People's Hospital (Wuxi, China) from
October 2025 to January 2026. Consecutive adult patients aged 20-65
years who were scheduled for painless gastroscopy during the
recruitment window were screened for eligibility. After confirming
eligibility and obtaining written informed consent, 218 patients
were enrolled. No interim analyses or protocol deviations that
could affect patient safety or data integrity occurred during the
study period.
Exclusion criteria were prespecified to minimize
confounding from anatomical or physiological conditions that could
independently alter airway dynamics. Patients were excluded if they
had: Restricted neck movement (for example due to rheumatic
disease, cervical masses or severe cervical spondylosis); upper
respiratory tract anomalies or acute trauma (including
maxillofacial trauma, cervical spine fractures or intraoral/airway
masses); prior neck radiotherapy; single- or double-lumen tracheal
intubation at presentation; known respiratory dysfunction (for
example chronic respiratory failure, severe chronic obstructive
pulmonary disease/asthma exacerbation or home oxygen use); or were
pregnant. Where exclusion status was uncertain, supervising
anesthesiologists adjudicated eligibility based on clinical records
and examination.
After written informed consent was obtained, a
standardized preoperative assessment was conducted by trained
research staff using a predefined case report form. Demographic and
anthropometric data included sex, age, body mass index (BMI,
kg·m-²), neck circumference (measured at the level of
the cricothyroid membrane at end-expiration) and sternomental
distance (SMD; measured from the upper border of the manubrium to
the mentum with the head fully extended and the mouth closed). All
measurements were performed twice and averaged; if two readings
differed by >5%, a third measurement was obtained and the median
recorded. Comorbidities, medication history and prior
anesthesia/sedation tolerance were documented to contextualize
risk.
Upper-airway ultrasonography was performed using a
GE ultrasound platform (GE HealthCare) equipped with a
low-frequency convex probe and a high-frequency linear probe.
Patients were positioned supine with the head in a neutral sniffing
position; a thin pillow (3-5 cm) was used to align the external
auditory meatus with the sternal notch when feasible. A liberal
amount of gel was applied, and sonographers were instructed to use
minimal transducer pressure to avoid compressing superficial soft
tissues. The linear probe was the default for superficial
structures; the convex probe was used in patients with large neck
habitus or suboptimal acoustic windows. Measurements were acquired
at end-expiration to reduce respiratory motion artifacts. Each
parameter was measured three times, and the mean value was used for
analysis.
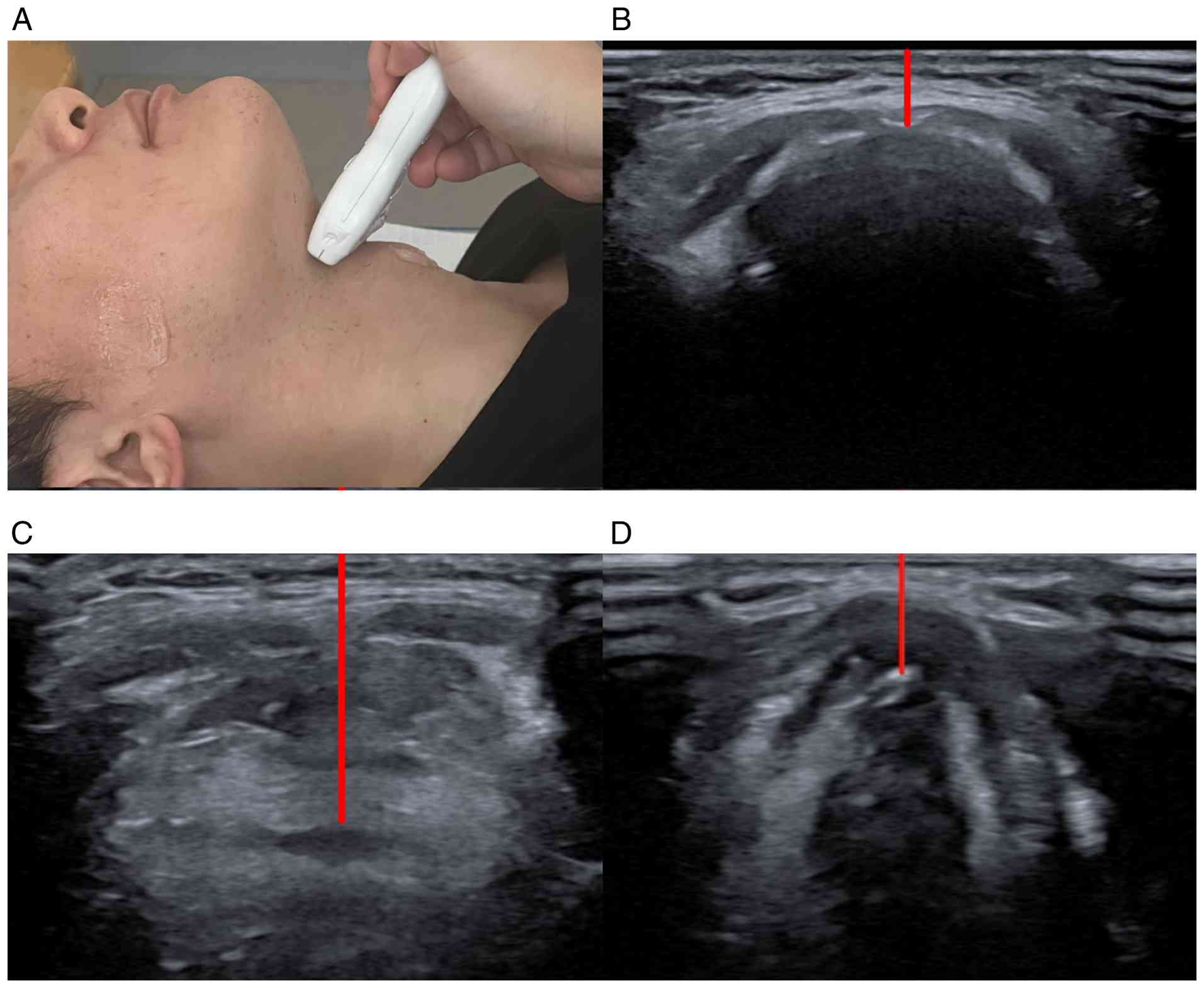
The measured parameters are delineated as follows:
i) DSH, distance in millimeters measured in a straight line from
the cutaneous surface to the midline of the hyoid bone (Fig. 1); ii) DSE, distance in millimeters
measured from the cutaneous surface to the middle axis of the
highest part of epiglottis detected, through the thyrohyoid
membrane (Fig. 1); iii) DSAC,
distance in millimeters measured from the cutaneous surface to the
midline of the anterior commissure of the vocal cords through the
cricothyroid membrane (Fig. 1);
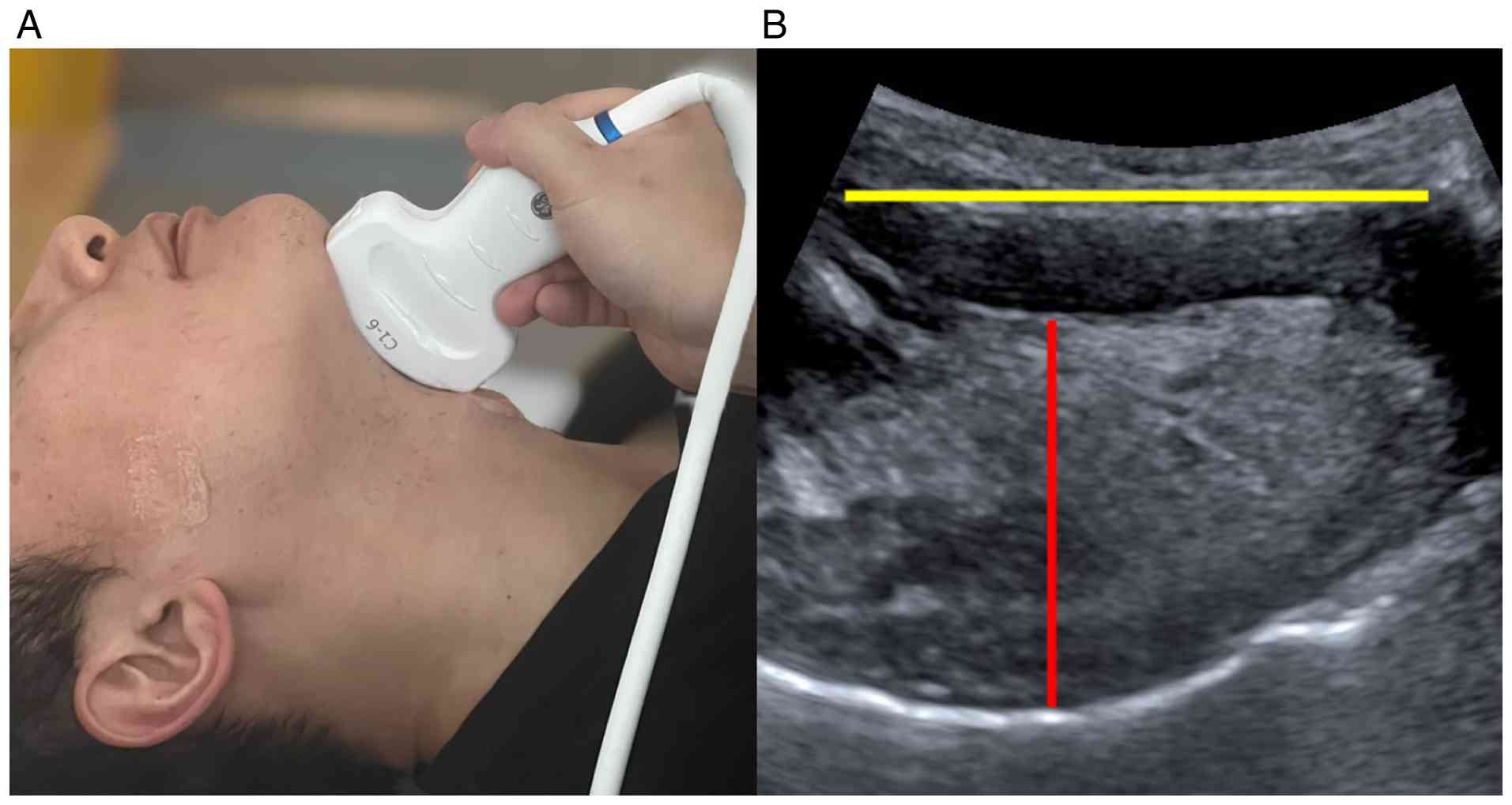
iv) TT, the maximum vertical distance in millimeters measured from
mylohyoid raphe to the surface of tongue (Fig. 2); v) HMD, distance in millimeters
measured from the lower border of the mentum of the mandible to the
upper border of the hyoid bone (Fig.
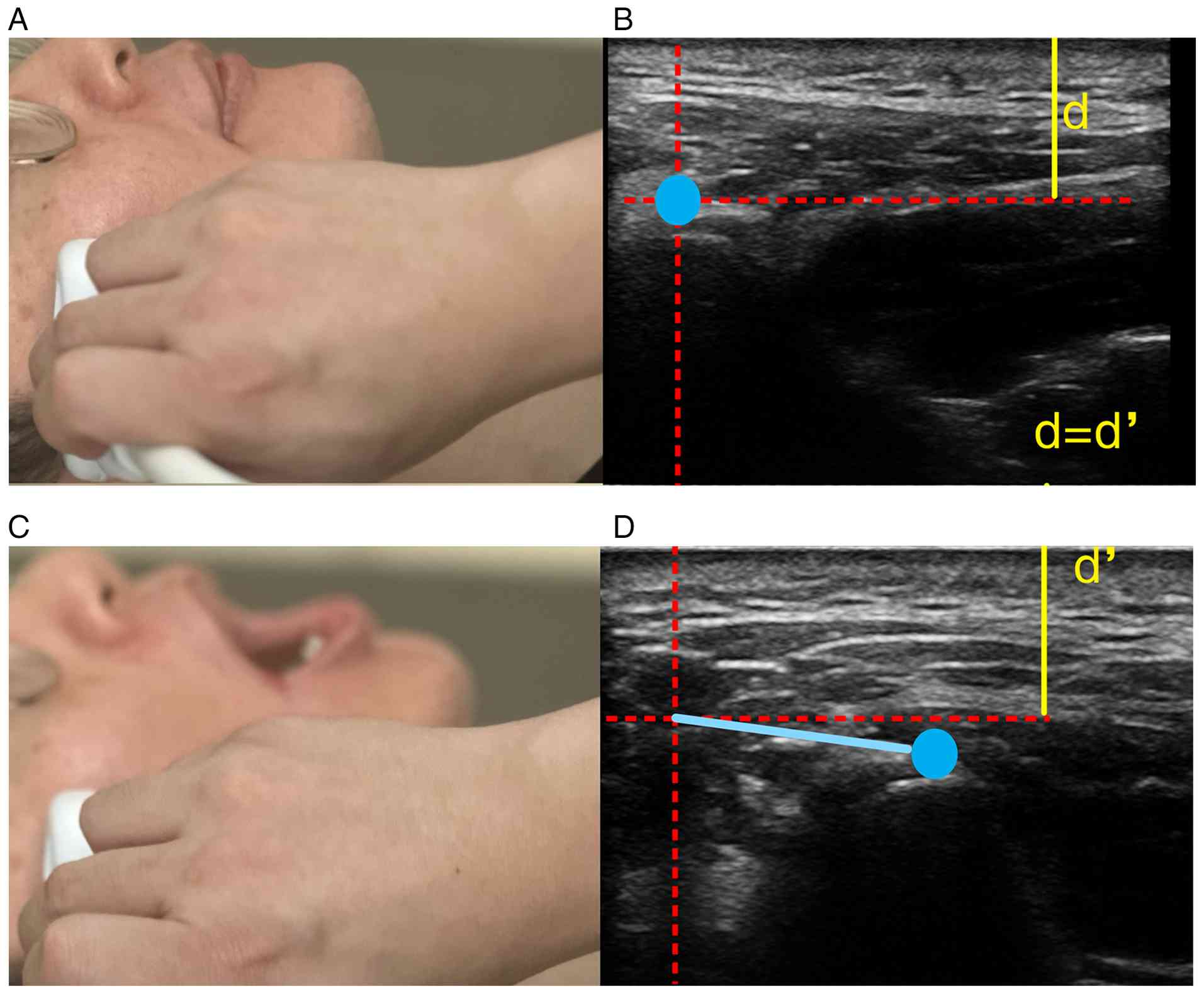
2); vi) ACT, distance that the anterior condyle moves
horizontally after opening the mouth, measured in millimeters
(Fig. 3).
After ultrasound assessment, all patients proceeded
to painless gastroscopy under standardized sedation procedure. All
patients received 5 µg sufentanil followed by propofol (1.5 mg/kg)
over a time period of 60 sec. An endoscopist started examination
when the MOAA/S score was ≤1 and the MOAA/S score was evaluated
every 30 sec. A dose of 0.5 mg/kg propofol was administered when
the MOAA/S score >1. Supplemental oxygen at 3 l·min-1
via standard nasal cannula was applied before induction.
Physiologic monitoring included continuous pulse
oximetry (SpO2), non-invasive blood pressure every 3-5
min, and electrocardiogram. Respiratory rate and chest excursion
were observed throughout. An escalation algorithm for desaturation
was predefined: i) Optimize head and neck position and reduce
propofol infusion if SpO2 trended downward; ii) initiate
chin lift and/or jaw thrust for SpO2 <90%; iii)
increase oxygen flow to 5-8 l·min-1 and provide assisted
ventilation via mask if recovery was not immediate; iv) for severe
or persistent hypoxemia, suspend propofol infusion, perform
bag-mask ventilation with 100% oxygen and insert an
oral/nasopharyngeal airway as indicated. All hypoxemic events
(threshold SpO2 <90% for ≥10 sec) were prospectively
recorded, including lowest SpO2, duration, interventions
and recovery time, using standardized forms by trained staff
blinded to ultrasound measurements.
To ensure data quality, all measurements and
intra-procedural events were double-entered into a secure database
with real-time range checks. A 10% random sample of ultrasound
images was re-evaluated by a senior reviewer; discrepancies >2
mm triggered consensus review and operator feedback. Where
feasible, inter-operator reliability was assessed on a pilot
subset, targeting intraclass correlation coefficients ≥0.80 for key
parameters (DSH, DSE, DSAC, TT, HMD, ACT). Outcome adjudication
(occurrence of hypoxemia) was independently verified by two
investigators based on monitor trends and intervention logs.
Statistical analysis
Statistical analyses were performed using SPSS 27.0
software (IBM Corp.). Categorical data are expressed as cases (%),
and differences between groups were analyzed using the
χ2 test. Measurement data that did not conform to a
normal distribution are expressed as median (lower quartile-upper
quartile), and the non-parametric Mann-Whitney U test was used to
compare hypoxemia and non-hypoxemia groups. Multiple index joint
diagnosis was achieved using binary logistic regression analysis to
calculate odds ratios (ORs) and confidence intervals (CIs). A novel
combined predictive model was developed, and its predictive value
was evaluated using the area under the receiver operating
characteristic (ROC) curve (AUC). The combined predictive model
equation was established according to the regression coefficients
of the independent predictors retained in the multivariate logistic
regression analysis. The nomogram was constructed based on this
final logistic regression model. The Hosmer-Lemeshow
goodness-of-fit test was used to assess the calibration of the
model. The efficiency of diagnosing hypoxemia was analyzed using
ROC curves. Calibration curves were constructed to assess the
consistency between predicted and observed probabilities. Decision
curve analysis (DCA) was performed to evaluate the clinical utility
of the model. All tests for statistical significance were
two-tailed, and P<0.05 was considered to indicate a
statistically significant difference. The adequacy of the sample
size for multivariable modeling was assessed according to the
events-per-variable criterion.
Results
Clinical characteristics and
laboratory data of patients
A total of 218 patients were included in the present
study (Table I). The median age
was 45.00 (36.00-57.00) years in the non-hypoxemia group and 34.50
(28.00-56.00) years in the hypoxemia group. In the hypoxemia group,
28 (56.00%) were female, while in the non-hypoxemia group, 115
(68.45%) were female. Compared with the non-hypoxemia group,
patients in the hypoxemia group had higher BMI (P<0.001), neck
circumference (P=0.018), DSH (P<0.001), DSE (P<0.001), DSAC
(P<0.001), TT (P<0.001), and HMD (P=0.001), but lower ACT
(P<0.001). No significant differences were observed in sex
(P=0.104), age (P=0.055) or SMD (P=0.405).
 | Table IComparison of clinical
characteristics between hypoxemia and non-hypoxemia groups. |
Table I
Comparison of clinical
characteristics between hypoxemia and non-hypoxemia groups.
| Variable | Non-hypoxemia
(n=168) | Hypoxemia
(n=50) | P-value |
|---|
| Sex (female %) | 115 (68.45) | 28 (56.00) | 0.104 |
| Age, years | 45.00
(36.00-57.00) | 34.50
(28.00-56.00) | 0.055 |
| BMI,
kg·m-2 | 23.80
(21.75-25.40) | 27.10
(25.40-29.33) | <0.001 |
| Neck circumference,
cm | 32.00
(30.00-35.00) | 35.00
(29.00-37.00) | 0.018 |
| SMD, cm | 12.00
(12.00-13.00) | 13.00
(11.00-13.00) | 0.405 |
| DSH, mm | 0.85
(0.79-0.94) | 1.02
(0.97-1.22) | <0.001 |
| DSE, mm | 2.13
(2.01-2.54) | 2.78
(2.63-2.82) | <0.001 |
| DSAC, mm | 0.79
(0.71-0.85) | 0.95
(0.83-1.07) | <0.001 |
| TT, cm | 5.09
(4.75-5.19) | 6.11
(5.28-6.27) | <0.001 |
| HMD, cm | 4.91
(4.69-5.24) | 5.24
(4.86-5.28) | 0.001 |
| ACT, cm | 1.21
(1.15-1.27) | 1.00
(0.99-1.12) | <0.001 |
Univariate and multivariate logistic
regression analyses for predicting hypoxemia
Univariate analysis showed that BMI (P<0.001),
neck circumference (P=0.013), DSH (P<0.001), DSE (P<0.001),
DSAC (P<0.001), TT (P<0.001), HMD (P=0.002) and ACT
(P<0.001) were significantly associated with hypoxemia (Table II). Multivariate logistic
regression analysis identified BMI (OR=2.867; 95% CI: 1.257-6.539;
P=0.012), DSH (OR=5.251; 95% CI: 1.892-14.572; P=0.001), DSE
(OR=3.907; 95% CI: 1.534-9.949; P=0.004), DSAC (OR=6.289; 95% CI:
2.601-15.205; P<0.001), TT (OR=2.929; 95% CI: 1.281-6.696;
P=0.011) and ACT (OR=0.409; 95% CI: 0.184-0.909; P=0.028) as
independent predictors of hypoxemia. By contrast, neck
circumference (P=0.309) and HMD (P=0.063) were not significant in
the multivariable model.
| Table IIUnivariate and multivariate logistic
regression analysis. |
Table II
Univariate and multivariate logistic
regression analysis.
| Variable | Univariate OR (95%
CI) | P-value | Multivariate OR
(95% CI) | P-value | VIF |
|---|
| BMI | 2.573
(1.806-3.667) | <0.001 | 2.867
(1.257-6.539) | 0.012 | 1.165 |
| Neck
circumference | 1.509
(1.089-2.091) | 0.013 | 1.496
(0.689-3.247) | 0.309 | 1.145 |
| DSH | 3.924
(2.512-6.129) | <0.001 | 5.251
(1.892-14.572) | 0.001 | 1.575 |
| DSE | 7.287
(3.919-13.55) | <0.001 | 3.907
(1.534-9.949) | 0.004 | 1.040 |
| DSAC | 4.299
(2.738-6.750) | <0.001 | 6.289
(2.601-15.205) | <0.001 | 1.809 |
| TT | 3.208
(2.227-4.622) | <0.001 | 2.929
(1.281-6.696) | 0.011 | 1.234 |
| HMD | 1.639
(1.205-2.229) | 0.002 |
2.353(0.954-5.804) | 0.063 | 1.362 |
| ACT | 0.218
(0.136-0.349) | <0.001 | 0.409
(0.184-0.909) | 0.028 | 1.131 |
To assess multicollinearity, variance inflation
factors (VIFs) were calculated. All predictors showed low VIF
values (1.040-1.809), below the threshold of 5.0, indicating no
significant multicollinearity and good stability of the
multivariate model.
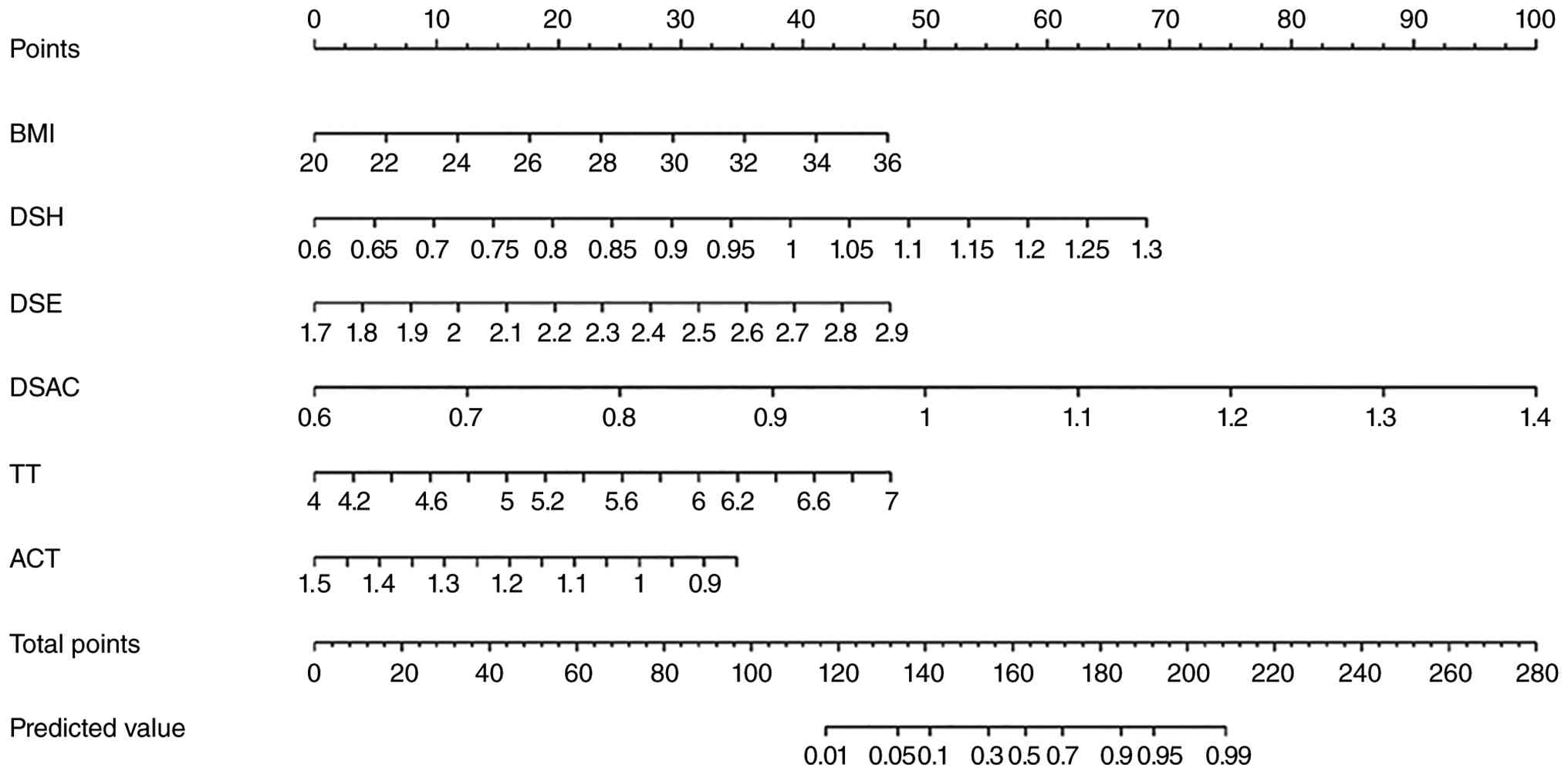
The combined predictive model equation is:
logit(P)=1.053 x BMI + 1.363 x DSH + 1.658 x DSE + 1.839 x DSAC +
1.075 x TT-0.894 x ACT. The nomogram provides a visual tool for
estimating this probability based on the individual contributions
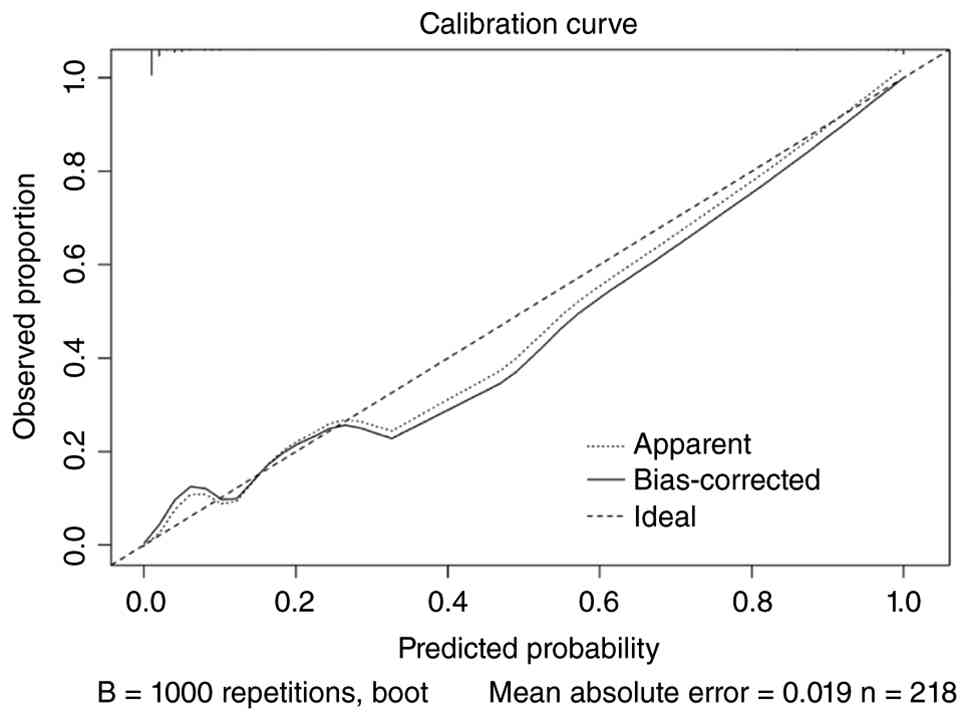
of these factors (Fig. 4). The
calibration curve demonstrates good agreement between the predicted
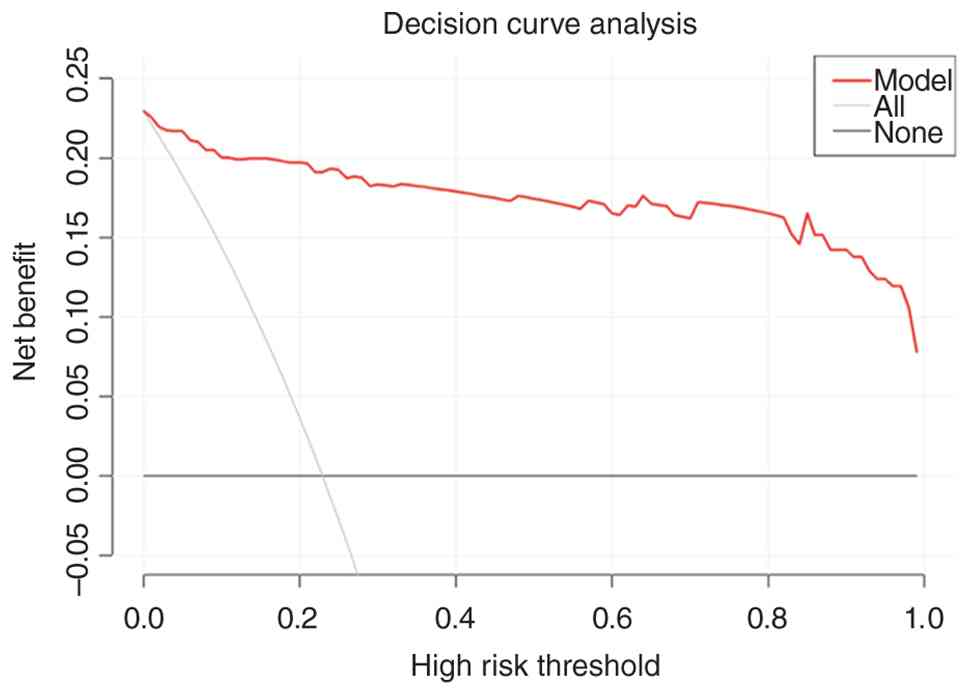
and observed probabilities of hypoxemia (Fig. 5). Finally, the DCA indicates that
the combined predictive model has clinical utility, showing a net
benefit over assuming all or no patients will experience hypoxemia
across a range of risk thresholds (Fig. 6).
Predicting hypoxemia status
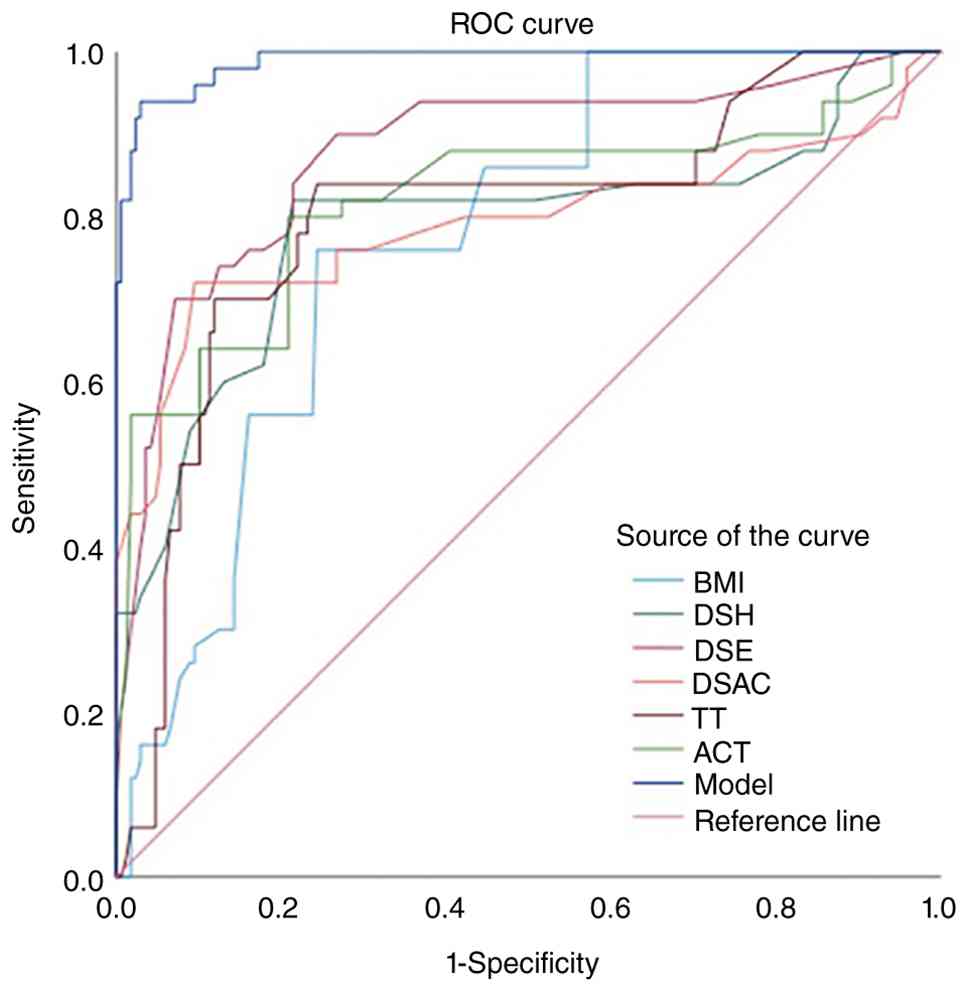
In the ROC curve analysis, the AUC values for
different variables in predicting hypoxemia were all >0.7,
indicating good discriminative ability (Table III and Fig. 7). Among them, DSE (AUC=0.879; 95%
CI: 0.818-0.940) and ACT (AUC=0.821; 95% CI: 0.740-0.901) performed
best in independently predicting hypoxemia. BMI (AUC=0.775; 95% CI:
0.710-0.840), DSH (AUC=0.789; 95% CI: 0.703-0.875), DSAC
(AUC=0.791; 95% CI: 0.700-0.883) and TT (AUC=0.800; 95% CI:
0.724-0.876) also demonstrated good predictive efficacy. In terms
of sensitivity and specificity, DSE had the highest sensitivity
(0.900), meaning this indicator can more effectively identify
hypoxemia positive cases, while DSAC had the highest specificity
(0.905), indicating its stronger ability to distinguish hypoxemia
negative cases. Regarding the best thresholds, the optimal cut-off
for BMI is 25.600, for DSH is 0.955, for DSE is 2.525, for DSAC is
0.905, for TT is 5.200 and for ACT is 1.130. The AUC of the
combined model reached 0.989 (95% CI: 0.979-0.999), which is
significantly higher than individual indicators, indicating that
combining multiple variables can further improve the accuracy of
hypoxemia prediction. The sensitivity of the combined model is
0.940, and the specificity is 0.970, balancing the stability and
reliability of the prediction.
| Table IIIReceiver operating characteristic
curve analysis for predicting hypoxemia. |
Table III
Receiver operating characteristic
curve analysis for predicting hypoxemia.
| Variable | AUC (95%CI) | Cut-off value | P-value | Sensitivity | Specificity |
|---|
| BMI | 0.775
(0.710-0.840) | 25.600 | <0.001 | 0.760 | 0.756 |
| DSH | 0.789
(0.703-0.875) | 0.955 | <0.001 | 0.820 | 0.786 |
| DSE | 0.879
(0.818-0.940) | 2.525 | <0.001 | 0.900 | 0.732 |
| DSAC | 0.791
(0.700-0.883) | 0.905 | <0.001 | 0.720 | 0.905 |
| TT | 0.800
(0.724-0.876) | 5.200 | <0.001 | 0.840 | 0.756 |
| ACT | 0.821
(0.740-0.901) | 1.130 | <0.001 | 0.800 | 0.792 |
| Model | 0.989
(0.979-0.999) | - | <0.001 | 0.940 | 0.970 |
Discussion
The present prospective observational study analyzed
clinical and ultrasonographic data from 218 patients undergoing
painless gastroscopy. Analysis revealed significant differences in
BMI, neck circumference, DSH, DSE, DSAC, TT, HMD and ACT between
the hypoxemia and non-hypoxemia groups. The relevance of these
upper-airway ultrasonographic parameters in airway assessment has
also been reported in previous studies (14-16).
Multivariate analysis identified BMI, DSH, DSE, DSAC, TT and ACT as
independent predictors of hypoxemia. A novel combined predictive
model was constructed based on logistic regression analysis. ROC
analysis demonstrated that the combined prediction model had an AUC
of 0.989, which was significantly superior compared with individual
parameters, indicating that the integration of ultrasonographic
parameters can significantly improve the accuracy of preoperative
hypoxemia prediction; the evaluation methods used were consistent
with previous methodological studies (17-19).
The high incidence of hypoxemia during painless
gastroscopy poses a notable clinical challenge (20-22).
As gastroscopy is a valuable tool for diagnosing and treating
gastrointestinal diseases, the associated hypoxemia can lead to
severe adverse events, including myocardial ischemia, arrhythmias,
neurological damage and even death (23,24).
Systematic pre-procedural assessment of hypoxemia risk in patients
undergoing painless gastroscopy may enable early intervention and
markedly reduce its incidence (25). This approach allows clinicians to
formulate individualized oxygenation-management strategies in
advance, thereby enhancing peri-procedural oxygenation stability,
improving procedural safety, minimizing adverse events and
ultimately optimizing both diagnostic quality and patient outcomes
(26-29).
In the present study, the incidence of hypoxemia was
22.9% (50/218). The present findings demonstrated that specific
ultrasonographic measurements, such as DSH, DSE, DSAC and TT, are
independently associated with hypoxemia during painless
gastroscopy, which is consistent with previous studies on airway
ultrasound assessment (13-16).
Specifically, a higher DSH, DSE and DSAC were associated with
increased risk of hypoxemia (30-32).
These parameters provide valuable information about the upper
airway anatomy and potential airway obstruction, which can
contribute to respiratory compromise during sedation (33-35).
Notably, ACT, reflecting mandibular mobility, was also identified
as an independent predictor of hypoxemia, where a lower ACT was
associated with hypoxemia. This suggests that limited mandibular
movement may contribute to airway obstruction and increase the risk
of hypoxemia during painless gastroscopy, which is supported by
previous studies on mandibular movement and airway patency
(36-38).
Several studies have demonstrated that ultrasound
measurement of upper airway anatomical parameters can accurately
assess difficult airways, including parameters such as DSH, DSE,
DSAC, TT and ACT. In line with prior studies, the present results
highlight the importance of upper airway assessment in predicting
hypoxemia (16,34,35).
The strength of the present study lies in its prospective design
and comprehensive data collection. The prospective nature minimized
recall bias and allowed for standardized data acquisition.
Comprehensive preoperative assessments were undertaken, and
demographic and anthropometric data were recorded including sex,
age, BMI and neck circumference. To obtain a series of upper
respiratory tract anatomical parameters, ultrasound measurements
were performed utilizing the convex and linear probes of the GE
ultrasound system (39,40).
The combined predictive model, incorporating BMI,
DSH, DSE, DSAC, TT and ACT, demonstrated excellent predictive
accuracy (AUC=0.989), surpassing the predictive ability of
individual parameters. The novel combined predictive model equation
was derived: logit(P)=1.053 x BMI + 1.363 x DSH + 1.658 x DSE +
1.839 x DSAC + 1.075 x TT-0.894 x ACT. This highlights the value of
integrating multiple ultrasonographic parameters to create a more
robust and reliable risk assessment tool (13-16).
The nomogram based on the predictive model offers a user-friendly
method for clinicians to estimate the probability of hypoxemia,
facilitating individualized management strategies. The calibration
curve further validates the reliability of the model. The DCA
(19,41) also showed that the combined
predictive model has clinical utility, showing a net benefit across
a range of risk thresholds (18).
In the present study, the findings were partly
consistent with previous studies, but some differences were also
observed. Similar to earlier reports, BMI was a notable predictor
of hypoxemia. Previous studies mainly focused on conventional
clinical variables or limited ultrasound indicators (2,42,43).
For example, an earlier artificial neural network (ANN) model
included BMI, habitual snoring and neck circumference (42), whereas a recent nomogram study
included BMI, propofol dose, Mallampati score and TT (43). Machine-learning studies also showed
that integrating more peri-procedural variables could improve
predictive performance (2,44). Different from these studies, the
present study systematically evaluated multiple upper-airway
ultrasound parameters, including DSH, DSE, DSAC, TT, HMD and ACT,
and found that DSH, DSE, DSAC, TT and ACT were independent
predictors of hypoxemia. These results indicate that hypoxemia
during painless gastroscopy may be associated not only with general
clinical factors, but also with multidimensional upper-airway
anatomical characteristics. This may provide additional information
for pre-procedural risk assessment in clinical practice.
Some limitations should be acknowledged. First, this
was a single-center study, which may limit the generalizability of
the present findings (41).
Second, while comprehensive data on upper airway anatomical
parameters were collected, other potential contributing factors to
hypoxemia (such as sedative dosage and endoscope insertion
technique) were not fully evaluated. Specifically, anesthesia was
induced and maintained via continuous intravenous infusion of
propofol, and prior to the administration of propofol for sedation,
all patients received oxygen at 3 l min-1 via standard
nasal cannula. The dose of sufentanil was predetermined at a
concentration of 5 µg (25).
Future studies should consider incorporating these variables to
refine the predictive model (17,41).
Third, although the present study was conducted prospectively, the
sample size could be larger to enhance statistical power (41). Despite these limitations, the
present study provides valuable insights into the use of
ultrasonography for predicting hypoxemia during painless
gastroscopy. The identified ultrasonographic parameters and the
developed combined predictive model hold promise for improving
patient safety and optimizing oxygenation management during these
procedures.
Future research should focus on validating the
present findings in larger, multi-center studies (41). Furthermore, investigating the
impact of targeted interventions based on ultrasonographic risk
assessment on hypoxemia incidence and patient outcomes would be
beneficial (26). With the
increasing use of point-of-care ultrasound, further studies could
explore the role of machine learning and artificial intelligence
for automated analysis and prediction of hypoxemia risk, improving
diagnostic efficiency and accuracy (17).
In conclusion, the present study supports the use of
ultrasonography as a valuable tool for predicting hypoxemia during
painless gastroscopy and provides a foundation for future research
in this area.
Acknowledgements
The authors would like to acknowledge Dr Shanshan
Zhou and Dr Linlin Cai (Department of Anesthesiology, Jiangnan
University Medical Center, Wuxi No. 2 People's Hospital, Wuxi,
Jiangsu 214000, P.R. China) for the collection and organization of
the experimental data.
Funding
Funding: Funding support for the present study was received from
the Construction Project of the High-end Clinical Science and
Technology Platform and Transformation Base of Soochow University
(grant no. ML12202723), and Top Talent Support Program for Young
and Middle-aged People of Wuxi Health Committee (grant no.
HB2023025).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YZ was responsible for the conceptualization and
methodology of the study, led the investigation and formal analysis
and wrote the original draft; LL contributed to clinical data
collection, organization and checking of the dataset, and reviewed
and edited the manuscript; JL contributed to statistical analysis,
construction and assessment of the prediction model, and
preparation of the figures; JX contributed to patient recruitment,
data acquisition and interpretation of clinical data; AW
contributed to the study design, patient recruitment, data
acquisition and interpretation of clinical data; FD led the
conceptualization and supervision of the research, was responsible
for funding acquisition, project administration and reviewed and
edited the entire manuscript and handled all correspondence. DH
contributed to the interpretation of clinical data and critical
revision of the manuscript. YZ and LL confirm the authenticity of
all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
The present research was carried out after receiving
approval from the Ethics Committee of Jiangnan University Medical
Center (approval no. 2024Y329). The present study was performed in
accordance with The Declaration of Helisinki (2013) and registering
on Clinical Trials (ChiCTR2500109627, Chinese Clinical Trial
Registry), and all participants gave written informed consent.
Patient consent for publication
Written informed consent for publication of
identifiable personal/face images shown in Figs. 1, 2 and 3
was obtained from the patients.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Beaton DR, Sharp L, Lu L, Trudgill NJ,
Thoufeeq M, Nicholson BD, Rogers P, Docherty J, Jenkins A, Morris
AJ, et al: Diagnostic yield from symptomatic gastroscopy in the UK:
British society of gastroenterology analysis using data from the
national endoscopy database. Gut. 73:1421–1430. 2024.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Zheng L, Wu X, Gu W, Wang R, Wang J, He H,
Wang Z, Yi B and Zhang Y: Development and validation of a hypoxemia
prediction model in middle-aged and elderly outpatients undergoing
painless gastroscopy. Sci Rep. 15(17965)2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Lin Y, Zhang X, Li L, Wei M, Zhao B, Wang
X, Pan Z, Tian J, Yu W and Su D: High-flow nasal cannula oxygen
therapy and hypoxia during gastroscopy with propofol sedation: A
randomized multicenter clinical trial. Gastrointest Endosc.
90:591–601. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Yan L, Wang X, Du K and Liang Y: Effect of
inspiratory muscle training on hypoxemia in obese patients
undergoing painless gastroscopy: Protocol for a single-center,
double-blind, randomized controlled trial. Front Med (Lausanne).
10(1269486)2023.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bach J: A quick reference on hypoxemia.
Vet Clin North Am Small Anim Pract. 47:175–179. 2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Sikha SB, Prakash NB, Thomas NC, John JA,
Mathews SS, Mannam P and George P: Role of ultrasonography in upper
airway assessment for decannulating tracheostomy in acquired brain
injury-a pilot study. Arch Phys Med Rehabil. 103:2174–2179.
2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Singh M, Chin KJ, Chan VWS, Wong DT,
Prasad GA and Yu E: Use of sonography for airway assessment: An
observational study. J Ultrasound Med. 29:79–85. 2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Osman A and Sum KM: Role of upper airway
ultrasound in airway management. J Intensive Care.
4(52)2016.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Reddy PB, Punetha P and Chalam KS:
Ultrasonography-a viable tool for airway assessment. Indian J
Anaesth. 60:807–813. 2016.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Zetlaoui PJ: Ultrasonography for airway
management. Anaesth Crit Care Pain Med. 40(100821)2021.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Carsetti A, Sorbello M, Adrario E, Donati
A and Falcetta S: Airway ultrasound as predictor of difficult
direct laryngoscopy: A systematic review and meta-analysis. Anesth
Analg. 134:740–750. 2022.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Martínez-García A, Guerrero-Orriach JL and
Pino-Gálvez MA: Ultrasonography for predicting a difficult
laryngoscopy. Getting closer. J Clin Monit Comput. 35:269–277.
2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Fulkerson JS, Moore HM, Anderson TS and
Lowe RF Jr: Ultrasonography in the preoperative difficult airway
assessment. J Clin Monit Comput. 31:513–530. 2017.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Yadav NK, Rudingwa P, Mishra SK and
Pannerselvam S: Ultrasound measurement of anterior neck soft tissue
and tongue thickness to predict difficult laryngoscopy-an
observational analytical study. Indian J Anaesth. 63:629–634.
2019.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Yao W and Wang B: Can tongue thickness
measured by ultrasonography predict difficult tracheal intubation?
Br J Anaesth. 118:601–609. 2017.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Kristensen MS, Teoh WH, Graumann O and
Laursen CB: Ultrasonography for clinical decision-making and
intervention in airway management: From the mouth to the lungs and
pleurae. Insights Imaging. 5:253–279. 2014.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Steyerberg EW: Clinical prediction models:
A practical approach to development, validation, and updating. 2nd
edition. Springer, 2019.
|
|
18
|
Vickers AJ and Elkin EB: Decision curve
analysis: A novel method for evaluating prediction models. Med
Decis Making. 26:565–574. 2006.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Van Calster B, McLernon DJ, van Smeden M,
Wynants L and Steyerberg EW: Topic Group ‘Evaluating diagnostic
tests and prediction models’ of the STRATOS initiative.
Calibration: The Achilles heel of predictive analytics. BMC Med.
17(230)2019.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Qadeer MA, Vargo JJ, Dumot JA, Lopez R,
Trolli PA, Stevens T, Parsi MA, Sanaka MR and Zuccaro G:
Capnographic monitoring of respiratory activity improves safety of
sedation for endoscopic cholangiopancreatography and
ultrasonography. Gastroenterology. 136:1568–1576, 1819-1820.
2009.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Beitz A, Riphaus A, Meining A, Kronshage
T, Geist C, Wagenpfeil S, Weber A, Jung A, Bajbouj M, Pox C, et al:
Capnographic monitoring reduces the incidence of arterial oxygen
desaturation and hypoxemia during propofol sedation for
colonoscopy: A randomized, controlled study (ColoCap study). Am J
Gastroenterol. 107:1205–1212. 2012.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Vargo JJ, Cohen LB, Rex DK and Kwo PY:
American Association for the Study of Liver Diseases; American
College of Gasteroenterology; American Gastroenterological
Association; American Society for Gastrointestinal Endoscopy.
Position statement: Nonanesthesiologist administration of propofol
for GI endoscopy. Gastroenterology. 137:2161–2167. 2009.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Wani S, Azar R, Hovis CE, Hovis RM, Cote
GA, Hall M, Waldbaum L, Kushnir V, Early D, Mullady DK, et al:
Obesity as a risk factor for sedation-related complications during
propofol-mediated sedation for advanced endoscopic procedures.
Gastrointest Endosc. 74:1238–1247. 2011.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Qadeer MA, Rocio Lopez A, Dumot JA and
Vargo JJ: Risk factors for hypoxemia during ambulatory
gastrointestinal endoscopy in ASA I-II patients. Dig Dis Sci.
54:1035–1040. 2009.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Wernli KJ, Brenner AT, Rutter CM and
Inadomi JM: Risks associated with anesthesia services during
colonoscopy. Gastroenterology. 150:888–894, e18. 2016.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Tao Y, Sun M, Miao M, Han Y, Yang Y, Cong
X and Zhang J: High flow nasal cannula for patients undergoing
bronchoscopy and gastrointestinal endoscopy: A systematic review
and meta-analysis. Front Surg. 9(949614)2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Douglas N, Ng I, Nazeem F, Lee K, Mezzavia
P, Krieser R, Steinfort D, Irving L and Segal R: A randomised
controlled trial comparing high-flow nasal oxygen with standard
management for conscious sedation during bronchoscopy. Anaesthesia.
73:169–176. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Patel A and Nouraei SAR: Transnasal
humidified rapid-insufflation ventilatory exchange (THRIVE): A
physiological method of increasing apnoea time in patients with
difficult airways. Anaesthesia. 70:323–329. 2015.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Petkar S, Wanjari D and Priya V: A
comprehensive review on high-flow nasal cannula oxygen therapy in
critical care: Evidence-based insights and future directions.
Cureus. 16(e66264)2024.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Wojtczak JA: Submandibular sonography:
Assessment of hyomental distances and ratio, tongue size, and floor
of the mouth musculature using portable sonography. J Ultrasound
Med. 31:523–528. 2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Pinto J, Cordeiro L, Pereira C, Gama R,
Fernandes HL and Assunção J: Predicting difficult laryngoscopy
using ultrasound measurement of distance from skin to epiglottis. J
Crit Care. 33:26–31. 2016.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Zheng Z, Wang X, Du R, Wu Q, Chen L and Ma
W: Effectiveness of ultrasonic measurement for the hyomental
distance and distance from skin to epiglottis in predicting
difficult laryngoscopy in children. Eur Radiol. 33:7849–7856.
2023.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Wang B, Wang M, Yang F, Zheng C, Yu T, Xu
J, Chen Y and Yao W: Predicting difficult intubation: The hyomental
distance ultrasound evaluation is superior to the thyromental
distance. Anaesth Crit Care Pain Med. 41(101144)2022.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Komatsu R, Sengupta P, Wadhwa A, Akça O,
Sessler DI, Ezri T and Lenhardt R: Ultrasound quantification of
anterior soft tissue thickness fails to predict difficult
laryngoscopy in obese patients. Anaesth Intensive Care. 35:32–37.
2007.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Altınsoy KE and Bayhan BU:
Ultrasound-measured skin-to-epiglottis distance as a predictor of
difficult intubation in obese patients: A prospective observational
study. J Clin Med. 14(2092)2025.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Claudino LV, Mattos CT, Mota-Júnior SL,
Coser RC, Silveira HMD and Franzotti Sant'Anna E: Upper airway
changes after mandibular advancement surgery combined with minimal
maxillary displacement: A preliminary cone-beam computed tomography
12 month minimum follow-up controlled study. J Am Dent Assoc.
156:398–407. 2025.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Isono S, Tanaka A, Sho Y, Konno A and
Nishino T: Advancement of the mandible improves velopharyngeal
airway patency. J Appl Physiol (1985). 79:2132–2138.
1995.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Chung F, Abdullah HR and Liao P: STOP-bang
questionnaire: A practical approach to screen for obstructive sleep
apnea. Chest. 149:631–638. 2016.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Moons KGM, Altman DG, Reitsma JB,
Ioannidis JPA, Macaskill P, Steyerberg EW, Vickers AJ, Ransohoff DF
and Collins GS: Transparent reporting of a multivariable prediction
model for individual prognosis or diagnosis (TRIPOD): Explanation
and elaboration. Ann Intern Med. 162:W1–W73. 2015.PubMed/NCBI View
Article : Google Scholar
|
|
40
|
Collins GS, Reitsma JB, Altman DG and
Moons KGM: Transparent reporting of a multivariable prediction
model for individual prognosis or diagnosis (TRIPOD): The TRIPOD
statement. BMJ. 350(g7594)2015.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Snell KIE, Archer L, Ensor J, Bonnett LJ,
Debray TPA, Phillips B, Collins GS and Riley RD: External
validation of clinical prediction models: Simulation-based sample
size calculations were more reliable than rules-of-thumb. J Clin
Epidemiol. 135:79–89. 2021.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Geng W, Tang H, Sharma A, Zhao Y, Yan Y
and Hong W: An artificial neural network model for prediction of
hypoxemia during sedation for gastrointestinal endoscopy. J Int Med
Res. 47:2097–2103. 2019.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Wu H, Chen X, Hou G, Zhang X, Zhang W,
Wang S and Chen L: Development of a tongue ultrasound-based
predictive model for hypoxemia during painless gastroscopy in ASA
I-II patients. PeerJ. 14(e20634)2026.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Zhao R, Chen Z, Teng Q, Xu T, Li Q, Gong
H, Ji H and Zhang H: Hypoxemia prediction model based on XGBoost
during sedation for gastrointestinal endoscopy. Front Med
(Lausanne). 12(1714512)2026.PubMed/NCBI View Article : Google Scholar
|