Introduction
Adriamycin (ADM) is a potent anthracycline chemotherapeutic agent with proven clinical efficacy, used in the treatment of various malignancies, including hematologic cancers and breast cancer (1-3). In gynecological oncology, ADM is a key drug for treating endometrial cancer and uterine leiomyosarcoma (4-6).
Despite its therapeutic efficacy, ADM causes dose-dependent cardiotoxicity. Previous studies indicated that cumulative doses above 400-550 mg/m2 significantly increased the risk of congestive heart failure (HF) (7,8). ADM-induced cardiomyopathy has traditionally been regarded as irreversible and often leads to progressive HF and death. In contrast, recent studies have suggested that early detection and timely management might allow partial or complete recovery of cardiac function (9). However, in patients who begin HF treatment more than two months after the completion of ADM therapy, the rate of left ventricular ejection fraction (LVEF) recovery markedly decreases. The rate of LVEF recovery when HF therapy is initiated between two and four months after the completion of chemotherapy has been reported to be as low as 28%. Moreover, in patients who experienced partial or complete recovery from ADM-induced cardiomyopathy, LVEF values prior to the initiation of HF therapy have been reported to range from 30 to 40% (10). In a prospective cohort study by Cardinale et al (9), anthracycline-related cardiotoxicity was most commonly detected within one year after treatment, with a median time to onset of approximately 3-6 months following completion of chemotherapy. Therefore, even when LVEF appears to be within the ‘normal range’ at the end of chemotherapy, a delayed decline in cardiac function may still occur after treatment cessation. Although recovery of LVEF with HF therapy has been reported, most recovery cohorts primarily include patients with mild-to-moderate left ventricular dysfunction (9). Reports on recovery from severe cardiac dysfunction remain limited. Furthermore, to the best of our knowledge, reports are extremely limited about the recovery of cardiac function in patients with LVEF <20% complicated by cardiogenic shock and multiorgan failure, particularly after prolonged intensive care management. Here, we report a case of recovery from severe ADM-induced cardiomyopathy presenting with an LVEF of 15%, with onset occurring three months after the completion of chemotherapy. The patient subsequently developed cardiogenic shock and multiorgan failure but ultimately improved following prolonged, multidisciplinary intensive care and successfully returned to work.
Case report
A 40-year-old woman presented to Jichi Medical University Hospital (Shimotsuke, Japan) with abdominal distension in November 2019. Contrast-enhanced magnetic resonance imaging revealed a uterine mass measuring 210x166x98 mm, with multiple cystic components and dilated intratumoral vessels. The tumor exhibited high signal intensity on T1-weighted imaging. Computed tomography showed no evidence of distant or lymph node metastases. Electrocardiography, spirometry, and chest radiography were unremarkable. Laboratory findings included carbohydrate antigen 19-9 of 15 U/ml (reference range, <36 U/ml), carbohydrate antigen 125 of 18 U/ml (<35 U/ml), and lactate dehydrogenase of 478 U/l (124-222 U/l). Preoperative examination suggested uterine leiomyosarcoma, and the patient underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy. Pathological examination confirmed a uterine leiomyosarcoma composed of spindle-shaped atypical cells positive for α-SMA and desmin. According to the International Federation of Gynecology and Obstetrics staging system, the clinical stage was classified as IB (pT1bNXM0). Adjuvant chemotherapy with ADM (75 mg/m2 every three weeks for six cycles; cumulative dose, 450 mg/m2) was administered. Echocardiography revealed a gradual decline in LVEF from 63% at baseline to 56% at the end of chemotherapy, although the patient remained asymptomatic.
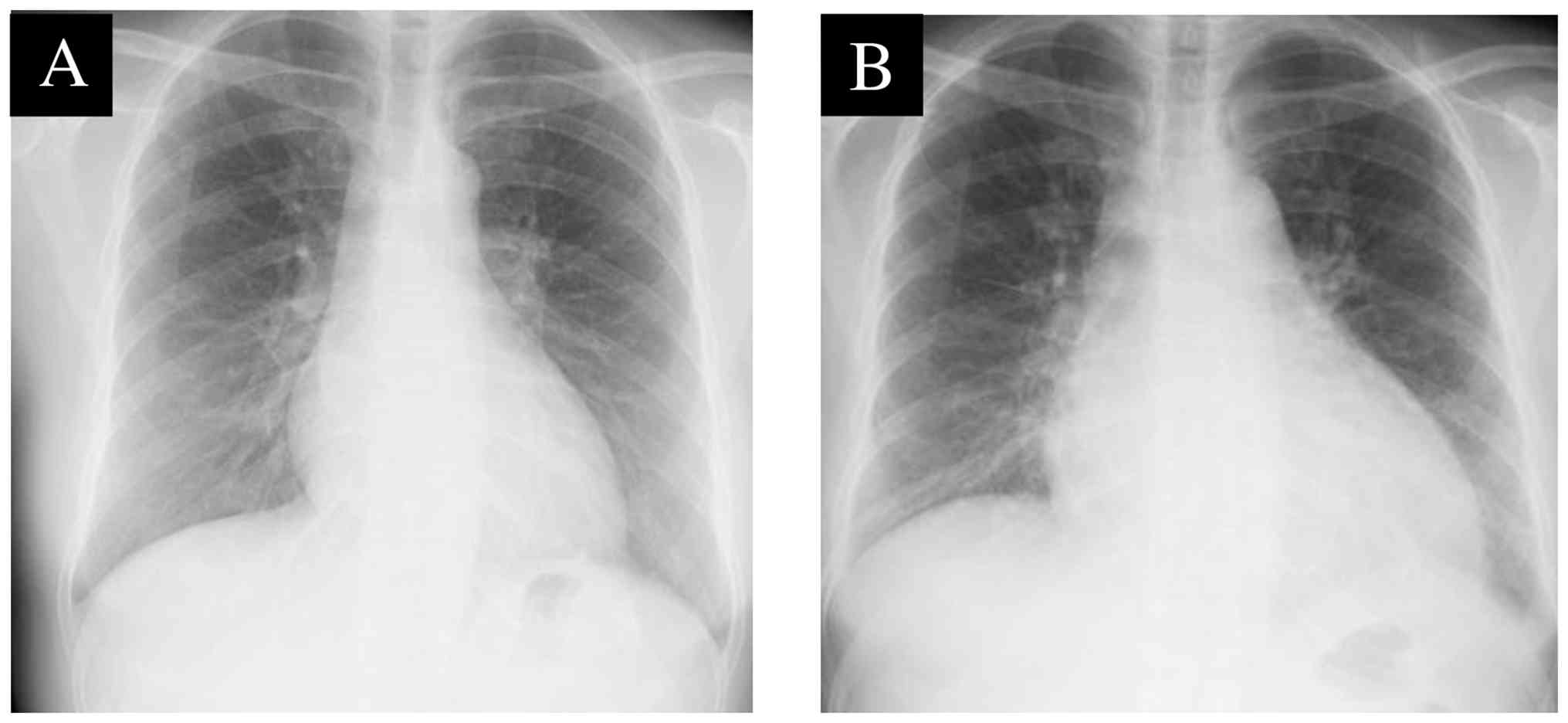
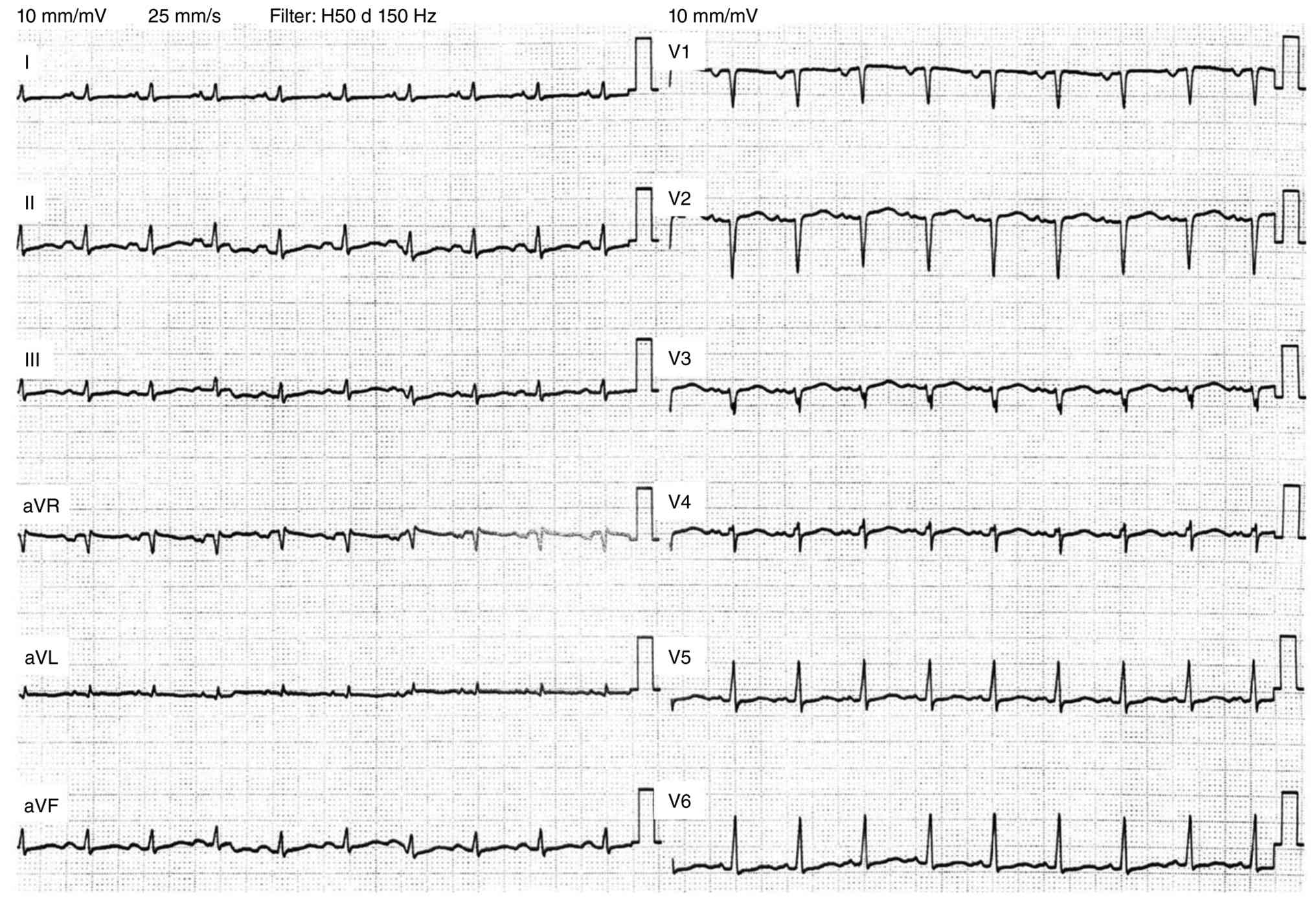
Three months after completing chemotherapy, the patient experienced epigastric discomfort, dyspnea, and general fatigue. She initially regarded it as a common cold and opted for observation; however, her symptoms worsened within a week, prompting her to visit the emergency department of Jichi Medical University Hospital in August 2020. On admission, vital signs were as follows: body temperature, 35.7˚C; blood pressure, 108/86 mmHg; pulse rate, 120 beats/minute; and peripheral oxygen saturation, 96% on room air. Blood tests revealed a markedly elevated NT-proBNP level (9,801 pg/ml; reference range, <121 pg/ml), a slightly elevated troponin T level (0.157 ng/ml; reference range, <0.014 ng/ml) and C-reactive protein (CRP) (0.31 mg/dl; reference range, <0.15 mg/dl), mild hepatic dysfunction, and preserved renal function. Chest radiography revealed cardiomegaly with a cardiothoracic ratio of 63.8% (baseline, 50.2%; reference range, <50%) and mild pulmonary congestion (Fig. 1A and B). Electrocardiography showed low voltage in the limb leads and decreased R-wave amplitude in V3-V4 (Fig. 2).
Echocardiography revealed diffuse hypokinesis with a severely reduced LVEF of 15% and left atrial and left ventricular dilatation, as shown in Video S1. Before establishing the diagnosis of ADM-induced cardiomyopathy, a systematic differential diagnosis was undertaken for the acute severe left ventricular dysfunction. Based on the clinical history and comprehensive evaluation, she was ultimately diagnosed with ADM-induced cardiomyopathy. Ischemic cardiomyopathy was considered unlikely because there was no chest pain and no ischemic ST-T changes on electrocardiography (Fig. 2). Myocarditis was also included in the differential diagnosis; however, it was deemed less likely due to the absence of fever or clear preceding viral symptoms, lack of suggestive inflammatory markers, and no evidence of sustained ventricular arrhythmias. Septic cardiomyopathy was also considered unlikely because there was no fever, no clinical findings suggestive of an infectious focus, and inflammatory markers, including CRP, did not support systemic infection. Thus, these alternative etiologies were systematically excluded based on the overall clinical, laboratory, and electrocardiographic findings.
Cardiac magnetic resonance imaging and endomyocardial biopsy, which are important investigations for differential diagnosis, could not be performed because of hemodynamic instability and renal dysfunction, representing a limitation of the diagnostic evaluation. In such critically ill patients, the risks of these procedures may outweigh their diagnostic benefits during the acute phase.
The patient was admitted to the coronary care unit (CCU) for advanced management. She required continuous oxygen therapy, intravenous cardiotonic drugs, and vasopressors, including dobutamine, milrinone, and norepinephrine. Oral HF pharmacotherapy with an angiotensin II receptor blocker, a β-blocker, and a loop diuretic was also initiated. Hemodynamic agents were titrated according to predefined perfusion and blood pressure targets. Dobutamine was initiated at 3 µg/kg/min on the day of admission and was gradually increased up to 8 µg/kg/min to maintain adequate peripheral perfusion. From day 9 of hospitalization, milrinone was started at 0.2 µg/kg/min and titrated to 0.5 µg/kg/min under strict monitoring for hypotension and arrhythmias. From day 13, norepinephrine was initiated at 0.02 µg/kg/min and adjusted up to 0.05 µg/kg/min to maintain a mean arterial pressure ≥65 mmHg or systolic blood pressure ≥90 mmHg, thereby ensuring adequate organ perfusion. Dose adjustments and weaning were guided by serial assessments of hemodynamics, lactate levels, urine output, and organ function, with careful balancing of therapeutic efficacy against adverse events (e.g., tachyarrhythmia, hypotension, and renal deterioration). The drug names, routes of administration, initial doses, titration strategies, maximum doses, and duration of administration are summarized in Table I.
 |
Table I
Detailed pharmacological and hemodynamic management during hospitalization.
|
Table I
Detailed pharmacological and hemodynamic management during hospitalization.
| Drug |
Route of administration |
Initial dose |
Titration strategies |
Maximum dose |
Duration of administration |
| Dobutamine |
Continuous intravenous infusion |
3 µg/kg/min |
Gradually increased to maintain adequate peripheral perfusion |
8 µg/kg/min |
Days 0-118 |
| Milrinone |
Continuous intravenous infusion |
0.2 µg/kg/min |
Gradually increased to maintain cardiac output |
0.5 µg/kg/min |
Days 9-62 |
| Norepinephrine |
Continuous intravenous infusion |
0.02 µg/kg/min |
Gradually increased to maintain mean arterial pressure ≥65 mmHg |
0.05 µg/kg/min |
Days 13-102 |
| Loop diuretic |
Switched from intravenous administration to oral administration |
20 mg/day (intravenous); 30 mg/day (oral) |
Continuously adjusted to optimize volume status |
80 mg/day (intravenous); 30 mg/day (oral) |
Days 0-Post-discharge |
| Angiotensin receptor blockers |
Oral administration |
1 mg/day |
Gradually titrated according to blood pressure, heart rate, renal function, and clinical status |
2 mg/day |
Days 0-post-discharge |
| β-blocker |
Oral administration |
0.625 mg/day |
Gradually titrated based on hemodynamic tolerance |
1.25 mg/day |
Days 0-post-discharge |
The fluid status was managed based on a multimodal assessment that incorporated body weight, chest radiography, echocardiography, and clinical symptoms. Ultimately, dobutamine, milrinone, and norepinephrine were discontinued on days 118, 62, and 102 of hospitalization, respectively. From a pharmacodynamic perspective, norepinephrine was primarily used to restore arterial pressure and end-organ perfusion in cardiogenic shock, whereas inotropes (dobutamine and/or milrinone) were used to augment cardiac output. Dobutamine provides β-adrenergic inotropy and is often favored when rapid titration is required; milrinone provides PDE3 inhibition with inotropy and vasodilation, but may worsen hypotension (11,12). For hemodynamic monitoring, continuous electrocardiographic and oxygen saturation monitoring were performed, along with frequent blood pressure measurements using an arterial line or cuff. Organ perfusion was comprehensively assessed based on trends in lactate levels, urine output, and mental status. Lactate levels were measured serially using standard blood tests, urine output was continuously monitored via a urinary catheter, and mental status was evaluated clinically through regular neurological assessments using the Glasgow Coma Scale. Volume status was evaluated using physical examination, daily body weight measurements, chest radiography, and repeated focused echocardiography. When feasible, cardiac output was estimated using echocardiography based on the left ventricular outflow tract velocity-time integral (13). A pulmonary artery catheter was used between days 10 and 20 of hospitalization. Management was conducted based on this multimodal monitoring approach. Despite intensive support, escalation of cardiotonic drugs and vasopressors failed to elevate blood pressure on the 11th day of hospitalization. On the 12th day, elevated liver enzyme levels [aspartate aminotransferase 332 U/l (reference range, 10-40 U/l), alanine aminotransferase 421 U/l (reference range, 10-45 U/l)] and serum creatinine [0.97 mg/dl (reference range, 0.47-0.79 mg/dl)] were observed, indicating the development of multiple-organ dysfunction. Moreover, the HF symptoms worsened to the extent that the patient was unable to engage in daily activities, such as eating. Therefore, heart transplantation remains the only curative treatment option available. However, heart transplantation was not feasible in this case, as it required a confirmed tumor-free status for a minimum of five years. Uterine leiomyosarcoma has a poor prognosis even at stage I, with reported 5-year progression-free survival and overall survival rates of 28 and 57%, respectively (14). Long-term ventricular assist device support, typically employed as a bridge to transplantation, was also deemed not feasible, as heart transplantation would not be eligible for consideration for at least four years; furthermore, the risks of infection and bleeding associated with device implantation were considered substantial following multidisciplinary discussion involving gynecology, cardiology, cardiac surgery, and oncology. Following a thorough explanation of the benefits and risks to the patient, the decision was made not to proceed with ventricular assist device implantation. Given this clinical course, the possibility of HF improvement was considered low, and a do-not-attempt resuscitation (DNAR) order was obtained. Concurrently, the palliative care team intervened and commenced morphine treatment to alleviate symptoms.
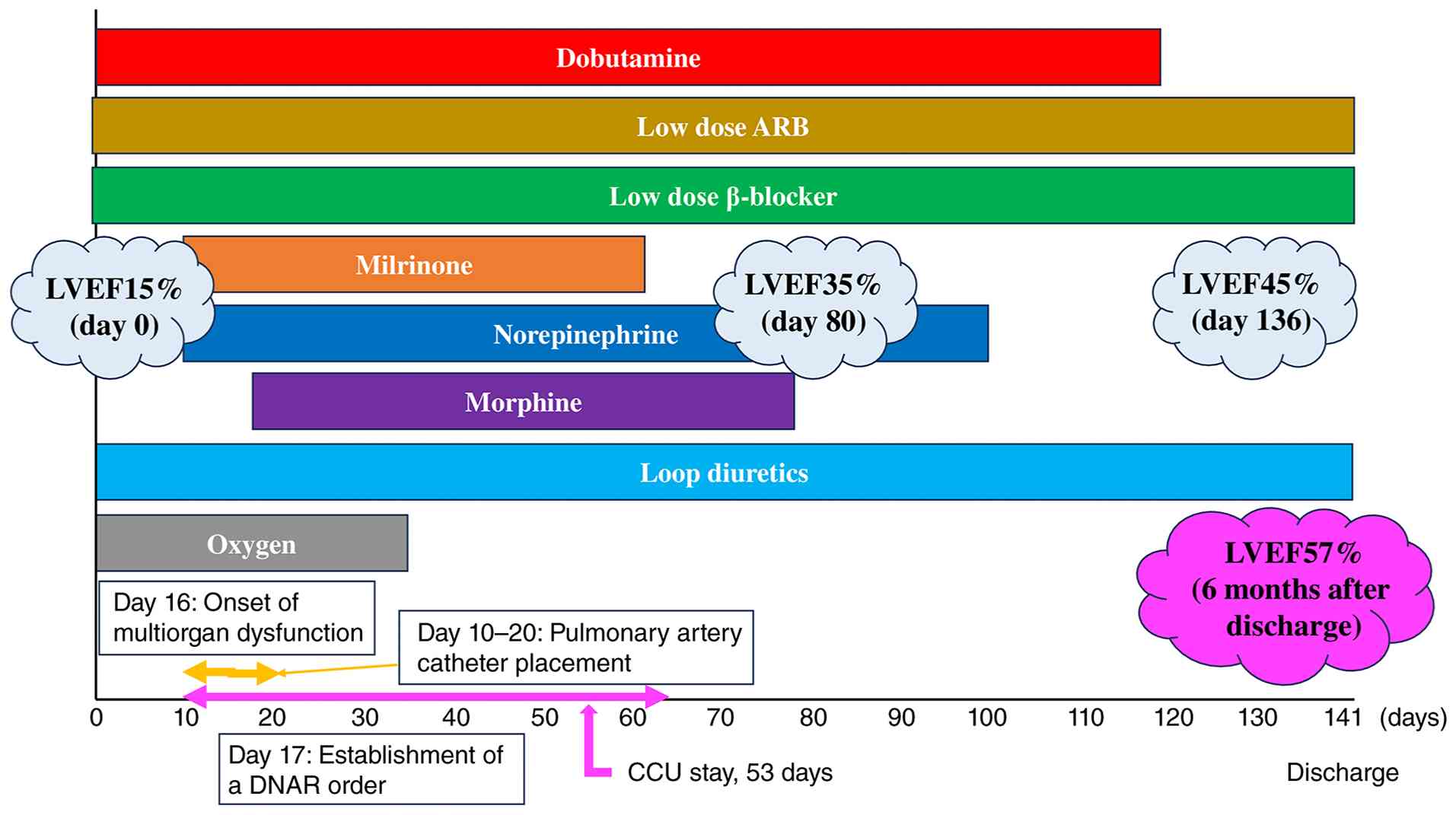
Interestingly, over the weeks of CCU management, HF progressively improved. Intravenous cardiotonic drugs and vasopressors were tapered off, and the patient was switched to oral medications, including bisoprolol, candesartan, and diuretics. After hemodynamic stabilization, defined as i) no requirement for intravenous inotropes or vasopressors for ≥24 h, ii) systolic blood pressure ≥90 mmHg (or mean arterial pressure ≥65 mmHg) without clinical signs of hypoperfusion, iii) down-trending lactate to ≤2.0 mmol/l, and iv) stable or improving renal/hepatic function, we initiated oral guideline-directed medical therapy in a stepwise manner (15). Escalation of vasoactive support is triggered by hypotension with hypoperfusion (e.g., rising lactate and oliguria), whereas de-escalation is performed once perfusion targets are sustained without dose increases (11). An angiotensin receptor blocker was first introduced at a low dose once congestion was controlled, followed by cautious initiation of a β-blocker after confirming the absence of low-output symptoms. The doses were gradually titrated according to the blood pressure, heart rate, renal function, and clinical status. Loop diuretics were continuously adjusted to optimize the volume status throughout this transition. This sequential approach, based on contemporary HF guidelines, aims to promote reverse remodeling while minimizing hemodynamic deterioration (16,17). Oxygen was subsequently discontinued, and the patient was discharged from the CCU on the 35th day. She was able to walk without fatigue on the 94th day, and her systolic blood pressure stabilized at approximately 90 mmHg on the 118th day. The patient was discharged on day 141 (January 2021). Cardiac function improved progressively, with LVEF increasing from 15% at admission to 35% at CCU discharge, 45% at hospital discharge, and 57% at the six-month follow-up; representative serial echocardiographic images are shown in Video S2. The overall clinical course, including changes in LVEF, major therapeutic interventions, and key clinical events, is summarized (Fig. 3). Serial measurements of NT-proBNP and troponin T levels decreased in parallel with clinical improvement, and the patient eventually reintegrated into society. In addition, the patient remained free of uterine leiomyosarcoma recurrence. As of the end of 2025, the patient had a performance status of 0 and no symptoms of HF. Planned long-term follow-up by the cardiology team will include blood tests for HF biomarkers every one to two months and echocardiography every three to six months; gynecological surveillance will include pelvic ultrasonography every three months, blood tests with measurement of tumor markers, and annual CT examination. This case was managed through a multidisciplinary collaboration between gynecology, cardiology, cardiac surgery, and oncology. A dedicated cardio-oncology consultation was also obtained; however, treatment decisions were made collaboratively, considering the balance between oncologic prognosis and therapeutic options for severe HF.
Discussion
We present the case of a patient who recovered from severe ADM-induced cardiomyopathy and successfully returned to work following long-term intensive care. This case illustrates several important clinical considerations. ADM-induced cardiomyopathy shows substantial inter-individual variability in onset and trajectory, ranging from transient early dysfunction to late-onset progressive cardiomyopathy (9,18,19). This heterogeneity should be considered when interpreting a single-case course. To improve clarity, we structured the following discussion around i) the atypical nature of this recovery, ii) potential contributors to reverse remodeling, iii) implications for surveillance and early detection, and iv) mechanistic considerations and limitations.
Cardinale et al reported that cardiac function did not recover in patients with an LVEF of 33±9% at HF therapy initiation (9), and the recovery rate fell below 30% two months post-chemotherapy (10). Thus, the presence of severe left ventricular dysfunction at the initiation of therapy and a longer interval between the completion of ADM treatment and the onset of cardiomyopathy are both associated with a lower likelihood of recovery.
In this case, the patient differed from the majority of previously reported recovery cases in several clinically important aspects: i) an extremely low LVEF of 15% at presentation, ii) delayed onset occurring three months after completion of chemotherapy, iii) progression to cardiogenic shock with multiorgan dysfunction requiring inotropes and vasopressors, iv) prolonged critical care and hospitalization (35 days in the CCU; 141 days total), and v) limited feasibility of advanced therapies such as heart transplantation or long-term mechanical circulatory support due to the oncological context, as active or recently treated malignancy is generally considered a contraindication or major limitation for heart transplantation and may also affect eligibility for durable mechanical circulatory support (20,21). Despite these unfavorable features, factors generally associated with poor recovery rates, she achieved near-normal LVEF (57%) and returned to normal life after months of intensive supportive care and a stepwise transition to oral HF therapy. Given the presence of multiple adverse prognostic factors, including severely reduced LVEF, delayed onset after chemotherapy, and progression to cardiogenic shock, this favorable outcome should be considered highly atypical. This clinical course suggests that recovery can occur, albeit rarely, even in extremely severe ADM-induced cardiomyopathy in selected patients; therefore, it should be interpreted cautiously and not generalized as a typical clinical course. When recovery occurs, improvement in LVEF can be delayed and may unfold over several months after the initiation of HF therapy, rather than immediately. This delayed recovery pattern supports sustained follow-up before concluding irreversibility. In the existing literature, presentations as severe as anthracycline-related cardiomyopathy complicated by cardiogenic shock have been reported mainly as case reports/series and in advanced HF registries, frequently requiring temporary mechanical circulatory support, durable left ventricular assist device therapy, or both; however, reports of near-complete recovery remain limited (22,23).
Despite these unfavorable indicators, cardiac function showed a gradual recovery, and one possible contributing factor may have been the early timing of HF intervention. Earlier initiation of HF treatment relative to the onset of symptoms is associated with a more favorable prognosis, as some patients may be identified before overt clinical deterioration occurs. Therefore, early detection strategies are essential, with the goal of identifying HF prior to the onset of overt symptoms and marked LVEF reduction, thereby enabling treatment initiation at the earliest possible opportunity. Recent studies have identified new prognostic factors for ADM-induced cardiomyopathy. A prospective study demonstrated that elevated troponin I (TnI) levels following chemotherapy identified patients at higher risk of LVEF reduction compared with those with undetectable TnI (24). Changes in global longitudinal strain (GLS) have emerged as valuable early markers for the detection of chemotherapy-induced cardiotoxicity. Furthermore, a systematic review of 1,504 patients indicated that a relative reduction of 10-15% in GLS from baseline during chemotherapy appears to be a clinically useful parameter that may precede overt LVEF reduction (25). Most studies support GLS as a better early indicator than LVEF (26,27). Moreover, some studies have indicated that the combination of GLS and TnI may serve as a superior predictive tool compared with either parameter alone (28-30). In addition, these studies suggest that combining multiple assessments may better predict the onset of ADM-induced cardiomyopathy, identify high-risk patients, optimize surveillance intervals for cardiac function monitoring, and enable early intervention. We acknowledge that GLS data during ADM therapy were not available in our case, which limited our ability to characterize the earliest phase of myocardial injury. At that time, GLS assessment had not yet been routinely implemented at our institution, and cardiac monitoring relied primarily on LVEF. Given the accumulating evidence that GLS changes can precede overt LVEF decline (21,31), we strongly recommend that oncology centers implement standardized baseline and serial GLS surveillance together with cardiac biomarkers when feasible as part of routine ADM cardiotoxicity monitoring. This is aligned with contemporary cardio-oncology guidance recommending a structured, risk-stratified surveillance program during anthracycline therapy and throughout the first 12 months after completion, integrating echocardiography (including GLS when feasible) and cardiac biomarkers to enable earlier cardioprotective intervention when subclinical injury is detected (21,31,32). In this case, although the LVEF at the end of chemotherapy remained within the normal range (63-56%), this absolute decline should not be dismissed, particularly in the setting of a high cumulative ADM dose (450 mg/m2). Contemporary cardio-oncology guidance emphasizes that clinically meaningful myocardial injury may develop before overt symptoms or a marked reduction in LVEF becomes apparent; therefore, even ‘small’ LVEF declines during ADM therapy warrant intensified surveillance, including GLS and cardiac biomarkers, and early consideration of cardioprotective therapy when subclinical dysfunction is suspected. In retrospect, earlier cardio-oncology intervention during this warning window may have been an opportunity to mitigate progression to severe cardiomyopathy. At the time of chemotherapy completion, the patient was asymptomatic and the LVEF remained within the normal range. In standard clinical practice at that time, routine initiation of cardioprotective therapy in such patients was not universally recommended, although it could be considered in selected high-risk individuals. In the absence of overt HF symptoms or hemodynamic compromise, pharmacological intervention was not initiated. Therefore, the management in this phase was consistent with standard clinical practice. However, in retrospect, earlier cardiology consultation and closer surveillance might have been beneficial.
In the present case, morphine was initiated by the palliative care team solely for the relief of refractory dyspnea and distress following a DNAR order, and was not intended as disease-modifying HF therapy. The symptom-relieving effects of morphine should be clearly distinguished from its hemodynamic or disease-modifying effects. In the context of HF, morphine is not considered a therapeutic agent and should be interpreted solely as supportive care for symptom relief rather than a contributor to cardiac recovery. Because the clinical benefit of morphine in acute HF is uncertain and observational data have suggested worse outcomes in some settings (33-35), we interpret morphine use in this case as supportive, not causal, with respect to LV functional recovery. For the management of refractory dyspnea, options other than opioids, such as benzodiazepines, may also be considered. However, in patients with advanced HF, opioids represent the most evidence-supported pharmacological therapy for refractory dyspnea, and in this case, low-dose morphine was selected for symptom relief. Observational studies have suggested that morphine use in acute HF is associated with worse outcomes; however, this association may be confounded by indication. Specifically, morphine is preferentially administered to more severely ill patients.
Importantly, despite the presence of multiple adverse prognostic factors, including severely reduced LVEF, delayed onset after completion of ADM therapy, and progression to cardiogenic shock, the patient ultimately recovered. We speculate that this recovery was facilitated by the patient's preserved myocardial reserve, as evidenced by maintained cardiac function prior to chemotherapy, combined with several months of intensive supportive care, which collectively outweighed these negative prognostic indicators. Notably, she was relatively young, had preserved pre-chemotherapy cardiac function, and had no major cardiovascular or systemic comorbidities, suggesting preserved physiological and myocardial reserves that may have enabled tolerance to prolonged intensive care and facilitated reverse remodeling. However, this report represents a single-case observation and does not establish a causal relationship between prolonged intensive care and partial recovery of LVEF. The observed association may reflect the natural course of ADM-induced cardiomyopathy, as well as the combined effects of supportive therapy and the passage of time. This natural course may include variability in the clinical trajectory, delayed recovery patterns, and partial spontaneous reversibility reported in ADM-induced cardiotoxicity. Partial and occasionally full reversibility has been demonstrated in ADM-induced cardiomyopathy, implying that time-dependent reverse remodeling may contribute (10,36). Therefore, our single case cannot separate the effect of prolonged intensive care from spontaneous partial reversibility over time.
Contemporary HF management is now based on four foundational drug classes (renin-angiotensin system inhibition with angiotensin-converting enzyme inhibitors/angiotensin receptor blockers (ACE-I/ARB), or preferably angiotensin receptor-neprilysin inhibitors (ARNI), evidence-based β-blockers, mineralocorticoid receptor antagonists, and sodium-glucose cotransporter-2 (SGLT2) inhibitors) (16). In cardio-oncology, the 2022 European Society of Cardiology cardio-oncology guidelines similarly recommend guideline-based HF therapy, including an ACE-I/ARB or ARNI, a β-blocker, an SGLT2 inhibitor, and a mineralocorticoid receptor antagonist (MRA), for symptomatic anthracycline-related cancer therapy-related cardiac dysfunction unless contraindicated or not tolerated (37). In our patient, early initiation of ARNI, SGLT2 inhibitors, and MRA was judged unsafe because she remained in prolonged cardiogenic shock with persistent hypotension and fluctuating end-organ dysfunction. Although SGLT2 inhibitors generally have a minimal blood pressure-lowering effect, evidence supporting their in-hospital initiation is derived mainly from patients who had achieved hemodynamic stabilization (16). In the EMPULSE trial, empagliflozin was initiated in patients hospitalized for acute HF after clinical stabilization, and in-hospital initiation of sacubitril/valsartan in PIONEER-HF was similarly evaluated after hemodynamic stabilization (15,38). Therefore, in the present case, initiation of additional guideline-directed medical therapy (GDMT) during the unstable acute phase was deferred to avoid worsening hypotension, renal dysfunction, or further impairment of organ perfusion. Although earlier initiation of GDMT might theoretically have promoted reverse remodeling, the impact of delayed initiation on clinical outcome cannot be determined from a single case. Notably, in-hospital initiation trials of ARNI (PIONEER-HF) and SGLT2 inhibitor (EMPULSE) after acute HF required hemodynamic stability (e.g., systolic blood pressure ≥100 mmHg without symptomatic hypotension and no IV inotropes), which was not met for an extended period in this case (15,38). In addition, MRA initiation is generally avoided when eGFR, a marker of renal function, is ≤30 ml/min/1.73 m2 or when serum potassium is ≥5.0 mEq/l because of the increased risk of hyperkalemia and renal dysfunction. Accordingly, we introduced HF pharmacotherapy in a stepwise manner, prioritizing decongestion and perfusion, followed by low-dose ARB and cautious β-blocker initiation once low-output symptoms were absent. The pharmacological management strategy, including the use of inotropes and vasopressors, was based on contemporary evidence and guideline recommendations for cardiogenic shock and acute HF management (11,12,15,16,38). We acknowledge that full contemporary GDMT was not achieved; therefore, we have clarified this as a limitation. Overall, the patient was managed according to standard clinical practice. However, some components of GDMT could not be implemented due to clinical limitations, including prolonged hemodynamic instability. Importantly, eligibility for full GDMT should be reassessed repeatedly during recovery, and earlier introduction of each drug class should be considered as soon as the stability criteria are satisfied.
In retrospect, there may have been an opportunity for transition from vasoactive agents to oral GDMT during the later phase of treatment. In this case, prolonged cardiogenic shock physiology and persistent hypotension limited the feasibility of the early introduction of additional agents. However, this experience highlights the importance of repeatedly reassessing eligibility for GDMT during the recovery phase and considering its introduction as soon as the stability criteria are met.
The key clinical lessons regarding the timing of GDMT initiation derived from this case are summarized as follows: i) GDMT should not be permanently withheld due to initial hypotension; ii) reassessment is essential after hemodynamic stabilization; iii) SGLT2 inhibitors may be considered early, given their minimal effect on blood pressure; and iv) stepwise initiation after vasopressor withdrawal is recommended.
Mechanistically, ADM-induced cardiotoxicity is mediated by multiple pathways, including oxidative stress, mitochondrial dysfunction, and Top2β-mediated DNA damage in cardiomyocytes (39). The gradual and delayed recovery observed in this case raises the possibility that the myocardial injury was at least partially reversible (e.g., myocardial stunning/edema) and not dominated by extensive replacement fibrosis (39,40). Another limitation is the absence of cardiac magnetic resonance (CMR) and histopathological evaluation, which precluded tissue-level assessment, including differentiation between myocardial edema and fibrosis, thereby limiting mechanistic interpretation (41). In severe cases of progressive cardiogenic shock and multiorgan dysfunction, gadolinium-enhanced CMR and endomyocardial biopsy may be difficult to perform or inappropriate from a safety perspective. Follow-up imaging after clinical stabilization may allow further evaluation, including the assessment of residual fibrosis after recovery of cardiac function. This case demonstrates that even extremely severe ADM-induced cardiomyopathy can achieve substantial recovery under intensive, guideline-directed management. Despite the presence of multiple adverse prognostic factors, including markedly reduced LVEF and prolonged cardiogenic shock, recovery was achieved without precipitating further hemodynamic deterioration. These findings suggest that the careful and sustained application of contemporary HF treatment strategies may significantly improve outcomes even in critically severe cases of chemotherapy-induced cardiomyopathy, thereby expanding the evidence supporting current therapeutic approaches.
In conclusion, even extremely severe ADM-induced cardiomyopathy may not be irreversible; long-term intensive management incorporating pharmacological therapy, supportive care, and rehabilitation may contribute to the recovery of cardiac function. Clinically, this case highlights that recovery is possible but appears uncommon; therefore, it should not alter standard prognostic expectations or clinical decision-making in similar severe presentations without broader evidence (18,42).
Supplementary Material
Supplementary Data.
Echocardiography after administering adriamycin. Echocardiography revealed diffuse hypokinesis with a left ventricular ejection fraction of 15%, left atrial dilatation, and left ventricular dilatation, indicative of cardiomyopathy. LA, left atrium; LV, left ventricle.
Serial echocardiography from CCU discharge to 6 months after discharge. (A) LVEF was 35% at CCU discharge. (B) LVEF was 45% at discharge. (C) LVEF was 57% at 6 months after discharge. LVEF, left ventricular ejection fraction; CCU, coronary care unit.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be requested from the corresponding author.
Authors' contributions
KT, YuT, TK and HF conceived and designed the study. KT, YuT and TK were major contributors to the writing of the manuscript. MT, YaS, ES, KY, MS, YoT, AT and YuS acquired the data and interpreted the results. HF critically revised the manuscript for important intellectual content. KT and TK confirm the authenticity of all the raw data. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Patient consent to participate
The patient provided written informed consent for participation in this case report after receiving a full explanation.
Competing interests
The authors declare that they have no competing interests.
References
|
1
|
Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, Morel P, Van Den Neste E, Salles G, Gaulard P, et al: CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 346:235–242. 2002.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Boleti E and Mead GM: ABVD for Hodgkin's lymphoma: Full-dose chemotherapy without dose reductions or growth factors. Ann Oncol. 18:376–380. 2007.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Jones SE, Savin MA, Holmes FA, O'Shaughnessy JA, Blum JL, Vukelja S, McIntyre KJ, Pippen JE, Bordelon JH, Kirby R, et al: Phase III trial comparing doxorubicin plus cyclophosphamide with docetaxel plus cyclophosphamide as adjuvant therapy for operable breast cancer. J Clin Oncol. 24:5381–5387. 2006.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Randall ME, Filiaci VL, Muss H, Spirtos NM, Mannel RS, Fowler J, Thigpen JT and Benda JA: Gynecologic Oncology Group Study. Randomized phase III trial of whole-abdominal irradiation versus doxorubicin and cisplatin chemotherapy in advanced endometrial carcinoma: A Gynecologic Oncology Group Study. J Clin Oncol. 24:36–44. 2006.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Nomura H, Aoki D, Michimae H, Mizuno M, Nakai H, Arai M, Sasagawa M, Ushijima K, Sugiyama T, Saito M, et al: Effect of taxane plus platinum regimens vs doxorubicin plus cisplatin as adjuvant chemotherapy for endometrial cancer at a high risk of progression: A Randomized clinical trial. JAMA Oncol. 5:833–840. 2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Pautier P, Italiano A, Piperno-Neumann S, Chevreau C, Penel N, Firmin N, Boudou-Rouquette P, Bertucci F, Balleyguier C, Lebrun-Ly V, et al: Doxorubicin alone versus doxorubicin with trabectedin followed by trabectedin alone as first-line therapy for metastatic or unresectable leiomyosarcoma (LMS-04): A Randomised, multicentre, open-label phase 3 trial. Lancet Oncol. 23:1044–1054. 2022.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Von Hoff DD, Layard MW, Basa P, Davis HL Jr, Von Hoff AL, Rozencweig M and Muggia FM: Risk factors for doxorubicin-induced congestive heart failure. Ann Intern Med. 91:710–717. 1979.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Swain SM, Whaley FS and Ewer MS: Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer. 97:2869–2879. 2003.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Cardinale D, Colombo A, Bacchiani G, Tedeschi I, Meroni CA, Veglia F, Civelli M, Lamantia G, Colombo N, Curigliano G, et al: Early detection of anthracycline cardiotoxicity and improvement with heart failure therapy. Circulation. 131:1981–1988. 2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Cardinale D, Colombo A, Lamantia G, Colombo N, Civelli M, De Giacomi G, Rubino M, Veglia F, Fiorentini C and Cipolla CM: Anthracycline-induced cardiomyopathy: Clinical relevance and response to pharmacologic therapy. J Am Coll Cardiol. 55:213–220. 2010.PubMed/NCBI View Article : Google Scholar
|
|
11
|
van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al: Contemporary management of cardiogenic shock: A scientific statement from the American Heart Association. Circulation. 136:e232–e268. 2017.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Mathew R, Di Santo P, Jung RG, Marbach JA, Hutson J, Simard T, Ramirez FD, Harnett DT, Merdad A, Almufleh A, et al: Milrinone as compared with dobutamine in the treatment of cardiogenic shock. N Engl J Med. 385:516–525. 2021.PubMed/NCBI View Article : Google Scholar
|
|
13
|
VanDyck TJ and Pinsky MR: Hemodynamic monitoring in cardiogenic shock. Curr Opin Crit Care. 27:454–459. 2021.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Zivanovic O, Leitao MM, Iasonos A, Jacks LM, Zhou Q, Abu-Rustum NR, Soslow RA, Juretzka MM, Chi DS, Barakat RR, et al: Stage-specific outcomes of patients with uterine leiomyosarcoma: A comparison of the International Federation of gynecology and obstetrics and American joint committee on cancer staging systems. J Clin Oncol. 27:2066–2072. 2009.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Voors AA, Angermann CE, Teerlink JR, Collins SP, Kosiborod M, Biegus J, Ferreira JP, Nassif ME, Psotka MA, Tromp J, et al: The SGLT2 inhibitor empagliflozin in patients hospitalized for acute heart failure: A multinational randomized trial. Nat Med. 28:568–574. 2022.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Heidenreich PA, Bozkurt B, Aguilar D, Allen LA, Byun JJ, Colvin MM, Deswal A, Drazner MH, Dunlay SM, Evers LR, et al: 2022 AHA/ACC/HFSA guideline for the management of heart failure: Executive summary: A report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 145:e876–e894. 2022.PubMed/NCBI View Article : Google Scholar
|
|
17
|
McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, Burri H, Butler J, Čelutkienė J, Chioncel O, et al: 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 42:3599–3726. 2021.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Cardinale D, Iacopo F and Cipolla CM: Cardiotoxicity of anthracyclines. Front Cardiovasc Med. 7(26)2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Zamorano JL, Lancellotti P, Rodriguez Muñoz D, Aboyans V, Asteggiano R, Galderisi M, Habib G, Lenihan DJ, Lip GYH, Lyon AR, et al: 2016 ESC position paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC committee for practice guidelines: The task force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur Heart J. 37:2768–2801. 2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Velleca A, Shullo MA, Dhital K, Azeka E, Colvin M, DePasquale E, Farrero M, García-Guereta L, Jamero G, Khush K, et al: The International Society for Heart and Lung Transplantation (ISHLT) guidelines for the care of heart transplant recipients. J Heart Lung Transplant. 42:e1–e141. 2023.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, Boriani G, Cardinale D, Cordoba R, Cosyns B, et al: 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 43:4229–4361. 2022.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Freilich M, Stub D, Esmore D, Negri J, Salamonsen R, Bergin P, Leet A, Richardson M, Taylor A, Woodard J, et al: Recovery from anthracycline cardiomyopathy after long-term support with a continuous flow left ventricular assist device. J Heart Lung Transplant. 28:101–103. 2009.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Guha A, Caraballo C, Jain P, Miller PE, Owusu-Guha J, Clark KAA, Velazquez EJ, Ahmad T, Baldassarre LA, Addison D, et al: Outcomes in patients with anthracycline-induced cardiomyopathy undergoing left ventricular assist devices implantation. ESC Heart Fail. 8:2866–2875. 2021.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Cardinale D, Sandri MT, Colombo A, Colombo N, Boeri M, Lamantia G, Civelli M, Peccatori F, Martinelli G, Fiorentini C and Cipolla CM: Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation. 109:2749–2754. 2004.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Thavendiranathan P, Poulin F, Lim KD, Plana JC, Woo A and Marwick TH: Use of myocardial strain imaging by echocardiography for the early detection of cardiotoxicity in patients during and after cancer chemotherapy: A systematic review. J Am Coll Cardiol. 63 (25 Pt A):2751–2768. 2014.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Cocco LD, Chiaparini AF, Saffi MAL and Leiria TLL: Global longitudinal strain for the early detection of chemotherapy-induced cardiotoxicity: A systematic review and meta-analysis. Clin Oncol (R Coll Radiol). 34:514–525. 2022.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Gripp EA, Oliveira GE, Feijó LA, Garcia MI, Xavier SS and Sousa AS: Global longitudinal strain accuracy for cardiotoxicity prediction in a cohort of breast cancer patients during anthracycline and/or trastuzumab treatment. Arq Bras Cardiol. 110:140–150. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Sawaya H, Sebag IA, Plana JC, Januzzi JL, Ky B, Tan TC, Cohen V, Banchs J, Carver JR, Wiegers SE, et al: Assessment of echocardiography and biomarkers for the extended prediction of cardiotoxicity in patients treated with anthracyclines, taxanes, and trastuzumab. Circ Cardiovasc Imaging. 5:596–603. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Sawaya H, Sebag IA, Plana JC, Januzzi JL, Ky B, Cohen V, Gosavi S, Carver JR, Wiegers SE, Martin RP, et al: Early detection and prediction of cardiotoxicity in chemotherapy-treated patients. Am J Cardiol. 107:1375–1380. 2011.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Kang Y, Xu X, Cheng L, Li L, Sun M, Chen H, Pan C and Shu X: Two-dimensional speckle tracking echocardiography combined with high-sensitive cardiac troponin T in early detection and prediction of cardiotoxicity during epirubicine-based chemotherapy. Eur J Heart Fail. 16:300–308. 2014.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Plana JC, Galderisi M, Barac A, Ewer MS, Ky B, Scherrer-Crosbie M, Ganame J, Sebag IA, Agler DA, Badano LP, et al: Expert consensus for multimodality imaging evaluation of adult patients during and after cancer therapy: A report from the American society of echocardiography and the European association of cardiovascular imaging. J Am Soc Echocardiogr. 27:911–939. 2014.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Cardinale D, Colombo A, Sandri MT, Lamantia G, Colombo N, Civelli M, Martinelli G, Veglia F, Fiorentini C and Cipolla CM: Prevention of high-dose chemotherapy-induced cardiotoxicity in high-risk patients by angiotensin-converting enzyme inhibition. Circulation. 114:2474–2481. 2006.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Peacock WF, Hollander JE, Diercks DB, Lopatin M, Fonarow G and Emerman CL: Morphine and outcomes in acute decompensated heart failure: An ADHERE analysis. Emerg Med J. 25:205–209. 2008.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Miró Ò, Gil V, Martín-Sánchez FJ, Herrero-Puente P, Jacob J, Mebazaa A, Harjola VP, Ríos J, Hollander JE, Peacock WF, et al: Morphine use in the ED and outcomes of patients with acute heart failure: A propensity score-matching analysis based on the EAHFE registry. Chest. 152:821–832. 2017.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Witharana TN, Baral R and Vassiliou VS: Impact of morphine use in acute cardiogenic pulmonary oedema on mortality outcomes: A systematic review and meta-analysis. Ther Adv Cardiovasc Dis. 16(17539447221087587)2022.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Saini J, Rich MW and Lyss AP: Reversibility of severe left ventricular dysfunction due to doxorubicin cardiotoxicity. Report of three cases. Ann Intern Med. 106:814–816. 1987.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Lyon AR, López-Fernández T, Couch LS, Asteggiano R, Aznar MC, Bergler-Klein J, Boriani G, Cardinale D, Cordoba R, Cosyns B, et al: 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J Cardiovasc Imaging. 23:e333–e465. 2022.PubMed/NCBI View Article : Google Scholar
|
|
38
|
Velazquez EJ, Morrow DA, DeVore AD, Duffy CI, Ambrosy AP, McCague K, Rocha R and Braunwald E: PIONEER-HF Investigators. Angiotensin-neprilysin inhibition in acute decompensated heart failure. N Engl J Med. 380:539–548. 2019.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Zhang S, Liu X, Bawa-Khalfe T, Lu LS, Lyu YL, Liu LF and Yeh ET: Identification of the molecular basis of doxorubicin-induced cardiotoxicity. Nat Med. 18:1639–1642. 2012.PubMed/NCBI View Article : Google Scholar
|
|
40
|
Octavia Y, Tocchetti CG, Gabrielson KL, Janssens S, Crijns HJ and Moens AL: Doxorubicin-induced cardiomyopathy: From molecular mechanisms to therapeutic strategies. J Mol Cell Cardiol. 52:1213–1225. 2012.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Mabudian L, Jordan JH, Bottinor W and Hundley WG: Cardiac MRI assessment of anthracycline-induced cardiotoxicity. Front Cardiovasc Med. 9(903719)2022.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Itzhaki Ben Zadok O, Simitsis P and Nohria A: Recovery of left ventricular ejection fraction in patients with anthracycline-induced cardiomyopathy: A contemporary cohort study. J Card Fail. 31:1379–1389. 2025.PubMed/NCBI View Article : Google Scholar
|