Introduction
Acute respiratory distress syndrome (ARDS) is a
medical condition that is characterized by non-cardiogenic
pulmonary edema and acute hypoxemic respiratory failure with
diffuse lung inflammation (1).
ARDS was first reported by Ashbaugh et al (2) in 1967. Since then, numerous revisions
have been made to its definition and diagnostic criteria (3). Acute lung injury (ALI) represents a
milder form of ARDS that progresses through a complex and stepwise
process that frequently culminates in fulminant respiratory failure
and patient mortality (4). In a
study reported by Bellani et al (5), ARDS was observed in 10.4% patients
with acute hypoxemic respiratory failure in intensive care units,
demonstrating a mortality rate of ~40%. Therefore, understanding of
the pathophysiology of ALI and ARDS is important for their
effective management and for developing potential future
therapies.
ALI is characterized by pulmonary edema caused by
the dysregulation of inflammation and disruption of the
alveolocapillary barrier (3). A
number of risk factors, such as pneumonia, thoracic trauma
(pulmonary contusion), sepsis and blood transfusions, have been
shown to trigger dysregulated inflammatory responses, as well as
excessive leukocyte and platelet activation and increased
permeability of the alveolar-capillary barrier, ultimately leading
to ALI or ARDS (6). The
progression of ARDS has been proposed to consist of three distinct
phases: i) The acute/exudative phase; ii) the
organized/proliferative phase; and iii) the late/fibrotic phase
(7). The acute phase of ARDS is
characterized by the presence of notable hyaline membranes that
line the alveolar spaces, which frequently exhibit edemas and acute
alveolar hemorrhages (7).
Concurrently, the necrosis of endothelial cells and pneumocytes is
observed (7). Granulation tissue
proceeds to develop within the alveolar spaces of patients with
acute-phase ARDS and type II pneumocytes exhibit notable reactivity
and hyperplasia toward the end of the early phase (7). These characteristics have also been
shown to persist throughout the proliferative phase (7). At this stage, dense squamous
metaplasia may be observed (7). As
the proliferative phase progresses, granulation tissue extends into
the alveolar septa, resulting in notable levels of fibrosis in the
alveoli (7). During the fibrotic
phase, the alveolar walls exhibit dense collagen fibrosis and
hyalinization (7).
The cornerstone of current ARDS management is the
identification and treatment of its underlying cause. In addition
to treating its underlying causes, ARDS is clinically managed with
supportive therapies, which primarily entail ventilator strategies.
However, to the best of our knowledge, an effective targeted
treatment for ARDS beyond supportive therapies has remained elusive
(1,6).
As the incidence of ALI and ARDS has notably
increased following the coronavirus disease 2019 (COVID-19)
pandemic, awareness of these conditions has notably increased the
importance of their prevention, early diagnosis and treatment
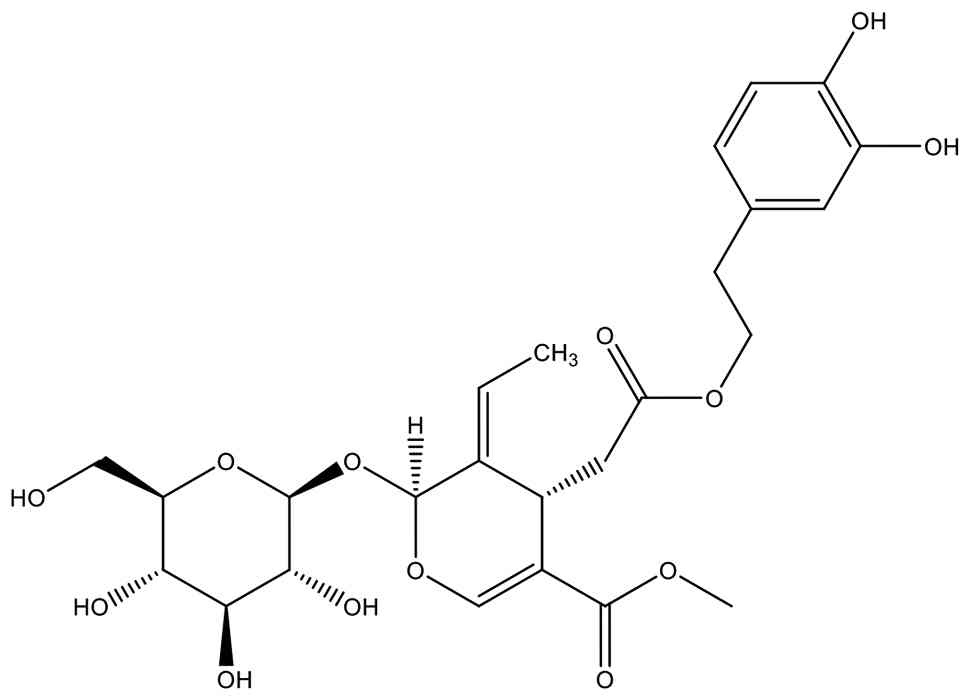
(8). Oleuropein (OLE) is a
secoiridoid compound that is extracted from unprocessed olive
fruits and leaves (9) (Fig. 1). It is the predominant phenolic
component found in olive leaves and has demonstrated
anti-inflammatory, antioxidant and anti-apoptotic activities in
multiple ischemia models; therefore, OLE has been shown to exhibit
notable potential therapeutic functions (10). The present study aimed to
investigate the protective and therapeutic effects of OLE in an ALI
model induced by oleic acid (OA).
Materials and methods
Animals
Ethical approval for the present study was obtained
from the Local Ethics Committee for Animal Experiments at Mersin
University (Mersin, Turkey; approval no. 2024/25; September 27,
2024). In total, 30 adult female Wistar Albino rats (weight,
200-300 g; age, 3-4 months) obtained from the Experimental Animal
Production and Research Center of the Mersin University Faculty of
Medicine were included. All experimental procedures were performed
in accordance with the Guidelines for the Care and Use of
Laboratory Animals. During the experiment, rats were provided with
standard pellet feed and tap water ad libitum and were
housed under a 12-h light/dark cycle, 60% humidity and at a
temperature of 21±1˚C. To induce lung injury, an OA solution was
prepared by dissolving OA in 75 mg/ml ethanol and diluting it with
saline. OA was purchased from Sigma-Aldrich (cat. no. O1008; Merck
KGaA. An OLE solution was prepared by dissolving OLE in 100 mg/ml
DMSO. To establish a model of ALI, rats were injected with 60 mg/kg
OA solution through the tail vein using a 26-g syringe.
The rats were randomly divided into the following
six groups (n=5/group): i) Group 1, which received intravenous (IV)
administration of an ethanol control; ii) group 2, which received
60 mg/kg OA by IV administration; iii) group 3, the prophylactic
group, which first received 100 mg/kg OLE by intraperitoneal (IP)
injection, followed ~30 min later by IV administration of 60 mg/kg
OA; iv) group 4, the therapeutic group, which received 60 mg/kg OA
by IV administration followed by 100 mg/kg OLE by IP injection ~15
min later; v) group 5, the OLE control, which received 100 mg/kg
OLE via IP administration; and vi) group 6, which received DMSO
administered via IP injection.
In total, 4 h after the administration of OA to rats
in all treatment groups and solvent to rats in the control groups,
rats were anesthetized via IP administration of 90 mg/kg ketamine
and 10 mg/kg xylazine. Subsequently, 4-5 ml blood samples were
taken from the inferior vena cava of rats by laparotomy. Rats were
then euthanized by exsanguination under anesthesia. Lung tissues
were subsequently collected and divided for tissue homogenization,
histopathological and immunohistochemical analyses. Blood samples
were centrifuged at 4,000 x g for 10 min at room temperature and
the sera were extracted and stored at -80˚C for biochemical
analysis.
Biochemical analysis
In serum and tissue homogenates of the collected
samples, malondialdehyde (MDA), lipid peroxide (LPO), surfactant
protein-D (SP-D), total antioxidant status (TAS) and total oxidant
status (TOS) were analyzed biochemically. For biochemical analyses,
the serum concentrations of MDA (cat. no. E0156Ra), LPO (cat. no.
E0285Ra) and SP-D (cat. no. E1072Hu) were determined using ELISA
kits from Shanghai Korain Biotech Co., Ltd. according to the
manufacturer's protocols. The TAS (cat. no. RL0024) and TOS (cat.
no. RL0017) of samples were analyzed using kits from Rel Assay
Diagnostics (MEGA TIP San. Tic. Ltd. Sti.) according to the
manufacturer's protocol. For tissue homogenization, 25-50 mg lung
tissue was collected, 500 µl PBS was added and tissues were
homogenized for 1 min. The tubes were centrifuged at 12,000 x g
(4˚C) for 2 min, and the supernatant was collected and analyzed
biochemically using the aforementioned commercial kits.
Histopathological and
immunohistochemical analysis
Lung tissues were evaluated histopathologically
using hematoxylin and eosin (H&E) staining. Tissue samples were
fixed in 10% neutral buffered formalin at room temperature for 24
h. Following paraffin embedding, specimens were sectioned at a
thickness of 4-5 µm and mounted on glass slides. Sections were
deparaffinized in xylene and rehydrated through a graded ethanol
series. Slides were stained with hematoxylin for 5 min at room
temperature, rinsed in running tap water, differentiated and blued
and then counterstained with Eosin for 2 min at room temperature
(20-25˚C). After dehydration and clearing, slides were coverslipped
using a permanent mounting medium. Histological examination was
performed using a light microscope (Olympus BX53, Olympus
Corporation, Tokyo, Japan). Histomorphometric and image analyses
were conducted using Stream Basic image acquisition and analysis
software version 2.4 (Olympus Corporation).
The immunoreactivity of lung tissues for TNF-α and
nuclear factor erythroid 2-related factor 2 (Nrf-2) were analyzed
immunohistochemically. Paraffin-embedded tissue sections (5 µm)
were used for immunohistochemical analysis. Following
deparaffinization and rehydration, antigen retrieval was performed
in 10 mM citrate buffer (pH 6.0) by heating at 95-100˚C for 20 min.
The sections were washed three times with PBS, pH 7.4). Endogenous
peroxidase activity was blocked using 3% hydrogen peroxide for 10
min, followed by blocking with a protein blocking solution (Abcam,
ab64226), supplied as a ready-to-use (undiluted) reagent, for 20
min at room temperature. Sections were 1/200 diluted incubated with
primary antibodies against monoclonal Anti-TNF-alpha (Abcam- cat.
No. ab220210) and Polyclonal Nrf2 (Abcam, cat. no. ab137550) at 4˚C
overnight. Sections were incubated with HRP Polymer Quanto
secondary antibody (ready-to-use; Thermo Fisher Scientific™,
UltraVision™ Quanto Detection System HRP DAB, Cat. No. TL-125-QHD)
for 30 min at room temperature. Immunoreactivity was visualized
using a DAB chromogen system and counterstained with hematoxylin.
Slides were examined using a light microscope, and images were
captured and analyzed using Stream Basic software (versions
1.6-1.8, Olympus Corporation, Tokyo, Japan).
Lung tissue sections were stained with H&E and
evaluated under a light microscope. Images of stained samples were
captured at x20 and x40 magnification. Lung damage was assessed
using a ‘Total Damage score’ based on the presence of interstitial
edema, alveolar congestion, alveolar septa thickness, and
inflammatory cell infiltration. Each parameter was rated on a scale
of 0 to 3 (0: normal, 1: mild, 2: moderate, 3: severe). The total
lung damage score was calculated by evaluating 6 areas for each
sample and taking the arithmetic mean of the scores for these
parameters. Furthermore, for the semi-quantitative analysis of
immunoreactivity, signal intensity and antibody distribution were
analyzed by a histologist blinded to the experimental groups of
samples. An overall immunohistochemistry composite score (H-score)
was generated by categorizing the staining intensity (range, 0-3)
of sections across all 6 fields observed per slide using the
following criteria: i) Fields with negative staining were scored 0;
ii) weak staining was assigned a score of 1; iii) areas of moderate
staining were scored 2; and iii) fields with strong staining
intensity were assigned a score of 3. The results of
semi-quantitative analyses were calculated using the formula:
H-score=ΣPi (i + 1), with i indicating staining intensity and Pi
representing the percentage of stained cells. The Pi-value ranged
from 0-100% and each field of view received a maximum H-score
between 0 and 400.
Purification of OLE from olive
leaves
OLE was isolated by Dr Tuba Aydın (Department of
Pharmacognosy of Ağrı Ibrahim Çeçen University (Ağrı, Türkiye)..
The isolation procedure was performed as described in a previous
study by Aggul et al (11).
Olive tree (Olea europaea) leaves (500 g) that were
collected from Yusufeli (Artvin; Turkey) in 2021 were dried, ground
and powdered. Leaves were first macerated with ethanol (5 l) at
room temperature for 24 h and filtered. Ethanol was removed under
reduced pressure using a rotary evaporator (42˚C, 90 rpm) for ~40
min. Ethyl acetate (500 ml) was then added to the concentrated
ethanol extract until precipitation occurred. The precipitate was
separated, and the remaining solvent was removed under reduced
pressure using a rotary evaporator (35˚C, 90 rpm) for ~30 min, As a
result of these processes, 78 g ethanol extract was obtained (15.6%
yield). The ethanol extract (10 g) was subsequently fractionated by
silica gel column chromatography. Silica gel 60 (70-230 mesh,
TEKKİM, Türkiye) was suspended in a dichloromethane:methanol
(80:20, v/v) solvent mixture and loaded onto the column (40x3 cm,
Çalışkan Lab). Fractions (40 ml) were analyzed by thin-layer
chromatography and OLE-containing subfractions 7-9 (1.7 g) were
combined. To isolate OLE, subfractions 7-9 were subjected to a
second silica gel column chromatography under the same conditions,
which improved the enrichment and recovery of OLE, resulting in a
higher isolated yield. The chemical structure was determined by
1H and 13C nuclear magnetic resonance
spectroscopic methods. The purity of the isolated OLE was
determined by High-performance liquid chromatography analysis to be
84.19%. A stock solution of oleuropein was prepared in methanol at
a concentration of 500 µg/ml. Chromatographic analysis was
performed using a C18 (ODS-3V) column. The mobile phase consisted
of solvent A (0.1% formic acid in water) and solvent B (100%
methanol) in an isocratic ratio of 60:40 (v/v). The flow rate was
maintained at 1.0 ml/min, and the column oven temperature was set
at 30˚C. The injection volume was 10 µl. Detection was carried out
using a photodiode array detector at 280 nm. The total run time was
30 min. Oleuropein concentration was determined from the
corresponding peak area using an external standard calibration
method.Statistical analysis. Statistical analysis was
performed using GraphPad Prism (version 9.0; Dotmatics). The
Shapiro-Wilk test was applied to assess the normality of data, and
the distribution of data was normal. Data are presented as the mean
and standard deviation of 5 independent experimental repeats/group.
Comparisons between group means of the parameter values were
analyzed via one-way ANOVA. Post hoc pairwise comparisons were
performed using the Tukey test. P<0.05 was considered to
indicate a statistically significant difference.
Results
H&E total damage score
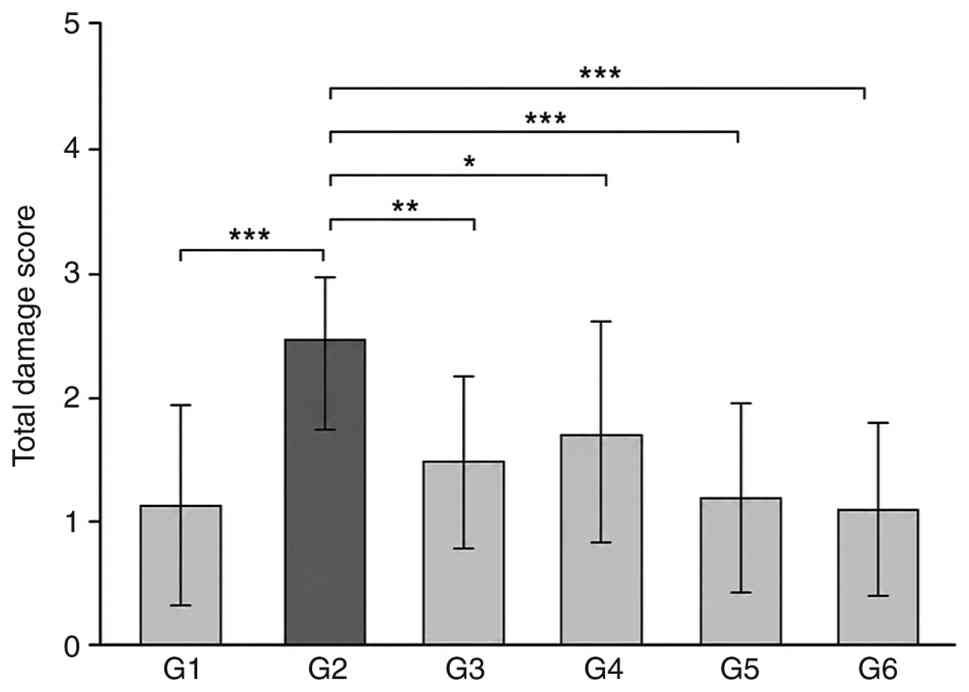
Total damage scores were evaluated
histopathologically in rat lung tissues using H&E staining
(Fig. 2). The total damage scores
of each group were compared with those of group 2 (Table I). In group 2, the lung tissue
architecture was markedly disrupted compared with that in group 1;
notable hemorrhagic foci were observed in the pleural and
subpleural spaces. Alveolar septal thickening, widespread edema,
alveolar collapse and peribronchial inflammatory-cell infiltration
were also observed in the lung tissue of rats in group 2. (Fig. 3) The highest total
histopathological damage score of lung tissues was observed in
group 2 (2.50±0.88), and this increase was significantly higher
compared with the scores of all other groups (Fig. 2 and Table I). In group 3, alveolar structures
demonstrated improved preservation compared with those in group 2.
Although hemorrhagic and edematous areas remained present in the
lung tissues of group 3, the presence of these features was notably
reduced compared with those in group 2. The lung tissues of rats in
group 3 also demonstrated milder inflammatory-cell infiltration
than in group 2 (Fig. 3). The
total damage score was significantly lower in group 3 lung tissues
compared with that in group 2 (mean ± SD, 1.47±0.74; Fig. 2; Table
I). In group 4, lung damage was moderately reduced compared
with the lung tissues of rats in group 2: Alveolar structures were
partially preserved, hemorrhagic foci were limited and moderate
inflammatory infiltration was observed (Fig. 3). The total damage score of lung
tissues from rats in group 4 was significantly reduced compared
with that of group 2 rats (mean ± SD, 1.71±0.86; Fig. 2; Table
I).
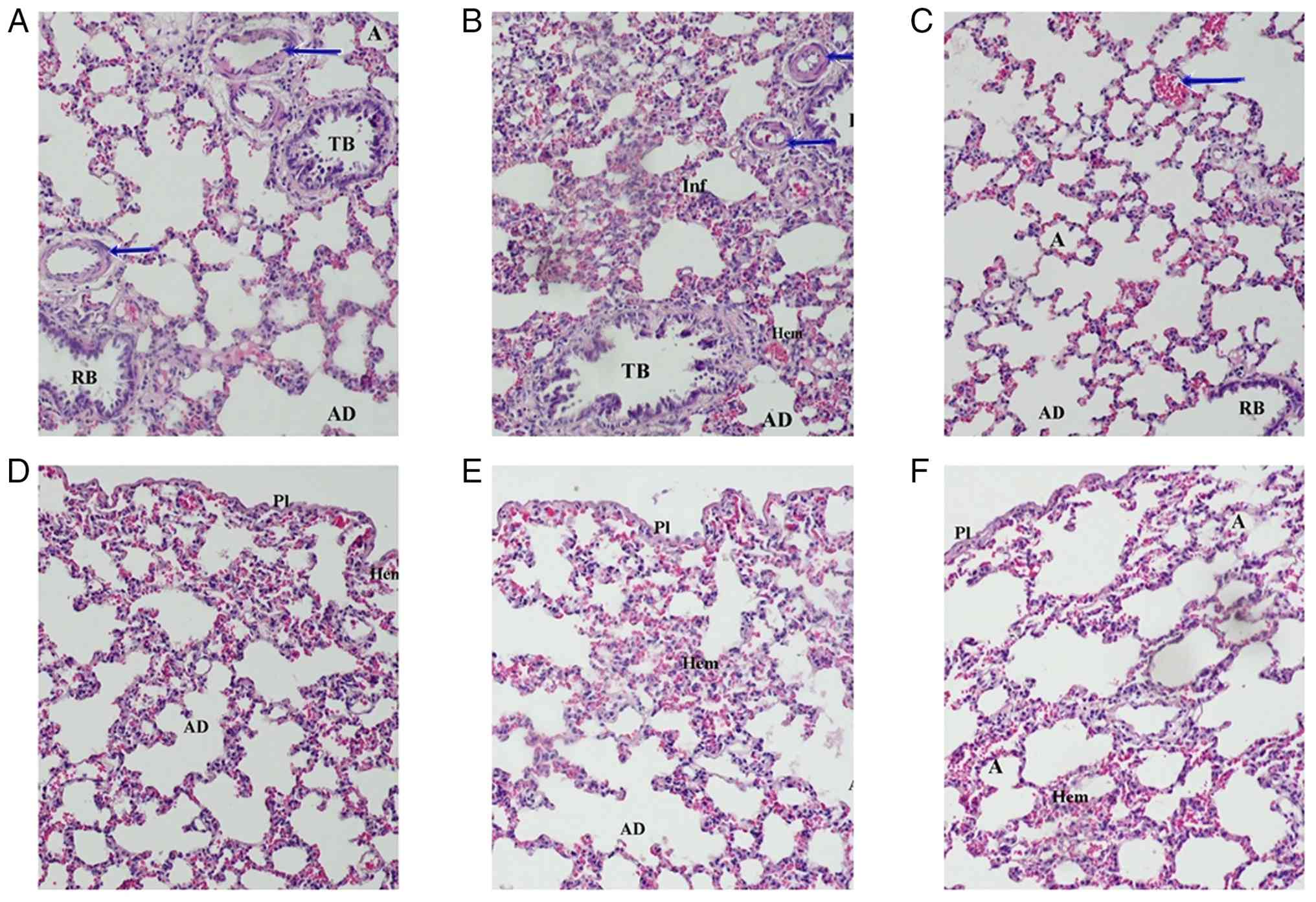 | Figure 3Histopathological examination of rat
lung tissue was performed via H&E staining. Representative
images of rat lung tissues stained with H&E in the (A) ethanol
control, (B) OA, (C) prophylactic OLE, (D) therapeutic OLE, (E) OLE
control and (F) DMSO control groups (x20 magnification). Arrows
indicate arterioles. Notable hemorrhage, edema and inflammatory
cell infiltration were observed in the OA group, whereas reduced
damage was observed in the lung tissues of rats in the prophylactic
and therapeutic OLE groups. A, alveolus; AD, alveolar duct; RB,
respiratory bronchiole; TB, terminal bronchiole; Pl, pleura; Hem,
hemorrhage; Inf, infiltration; H&E, hematoxylin and eosin; OA,
oleic acid; OLE, oleuropein. |
 | Table IComparison of the total damage score
of the oleic acid model group with other groups. |
Table I
Comparison of the total damage score
of the oleic acid model group with other groups.
| Comparison | Mean difference | Adjusted P-value | 95% CI |
|---|
| G2 vs. G1 | +1.42 | <0.001 | (0.75, 2.09) |
| G3 vs. G2 | -1.03 | 0.002 | (-1.80, -0.26) |
| G4 vs. G2 | -0.79 | 0.012 | (-1.47, -0.12) |
| G5 vs. G2 | -1.33 | <0.001 | (-2.01, -0.66) |
| G6 vs. G2 | -1.41 | <0.001 | (-2.10, -0.72) |
TNF-α immunoreactivity
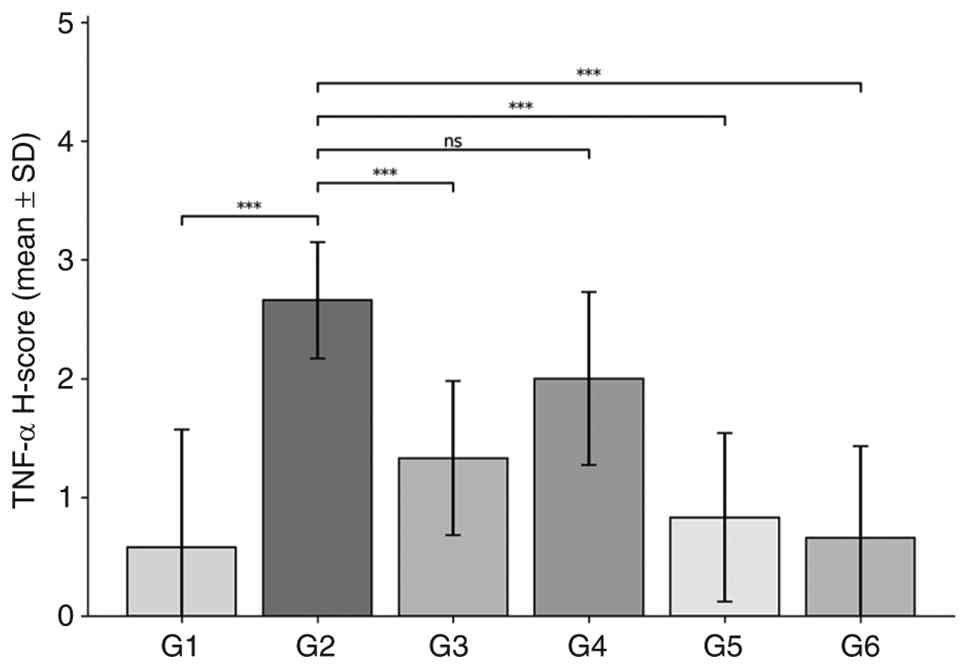
The immunohistochemical levels of TNF-α
immunoreactivity were examined across experimental groups and
statistically compared using H-score values (Figs. 4 and 5). Group 2 exhibited the highest level of
TNF-α expression; this increase in immunoreactivity compared with
all other groups was statistically significant. Notable positive
staining for TNF-α was observed in the alveolar epithelial cells,
interstitial spaces and peribronchiolar regions of tissues in group
2. However, in the lung tissues of rats in group 3, TNF-α
expression significantly decreased compared with that in group 2.
Positive staining in group 3 was more limited to specific areas
compared with the staining distribution in group 2. Furthermore, in
group 4, TNF-α expression was decreased compared with that in group
2, but was markedly higher compared with TNF-α expression levels in
group 3 (Fig. 5).
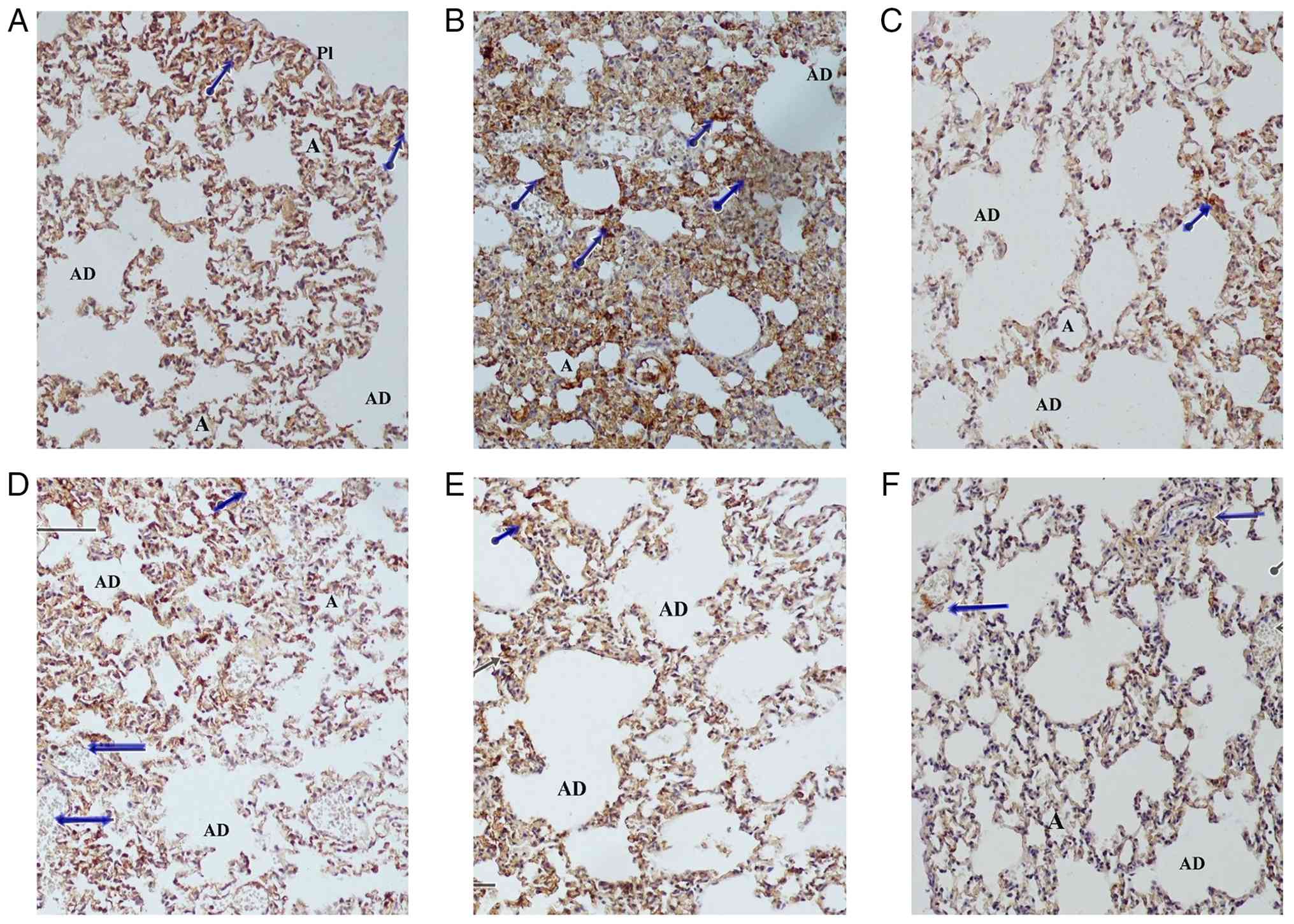 | Figure 5Immunohistochemical examination of
TNF-α immunoreactivity levels in the lung tissues of acute lung
injury model rats. Representative images of immunohistochemical
staining for TNF-α in rat lung tissues in (A) ethanol control, (B)
OA, (C) prophylactic OLE, (D) therapeutic OLE, (E) OLE control and
(F) DMSO control groups (x20 magnification). Left-facing arrows
indicate arterioles and shorter arrows with a circular base
indicate areas of notable immunoreactivity. The OA group
demonstrated the strongest immunostaining against TNF-α, whereas
immunostaining notably decreased in the lung tissues of rats in the
prophylactic and therapeutic OLE groups. A, alveolus; AD, alveolar
duct; Pl, pleura; OA, oleic acid; OLE, oleuropein. |
Nrf-2 immunoreactivity
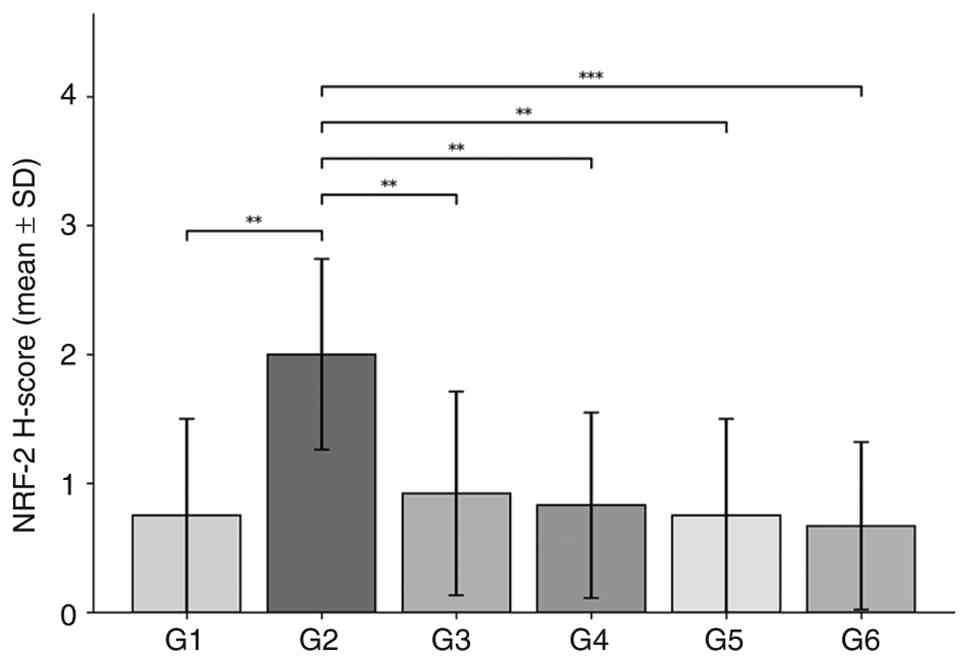
The immunohistochemical levels of Nrf-2
immunoreactivity were examined across the experimental groups and
resulting H-score values were compared (Figs. 6 and 7). In group 2, Nrf-2 expression was
significantly increased as a result of the oxidative stress
response induced by OA. Notable immunoreactivity was observed in
the alveolar epithelium and interstitial regions of lung tissue in
group 2. The mean immunoreactivity score in group 2 was
significantly higher compared with that in all other experimental
groups. In the lung tissues of rats in treatment group 3, Nrf-2
expression was significantly decreased compared with those in group
2. This indicated that OLE suppressed the oxidative stress response
and exhibited a protective effect against lung damage. In group 4,
Nrf-2 expression was decreased compared with that in group 2, but
slightly higher compared with that in the prophylactic group.
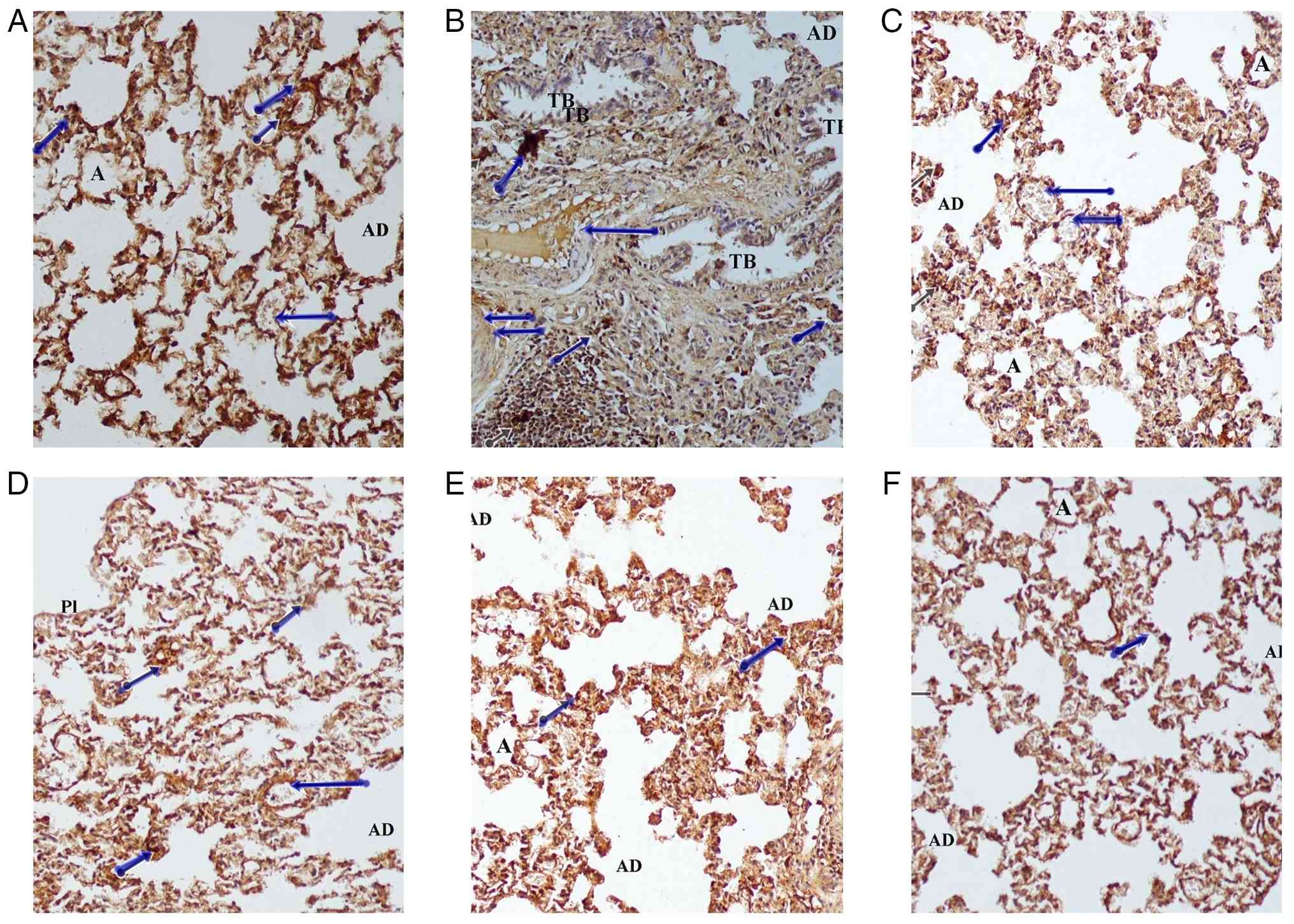 | Figure 7Immunohistochemical examination of
Nrf-2 immunoreactivity levels in acute lung injury model rats.
Representative images of immunohistochemical staining for Nrf-2 in
rat lung tissues in the (A) ethanol control, (B) OA, (C)
prophylactic OLE, (D) therapeutic OLE, (E) OLE control and (F) DMSO
control groups (x20 magnification). Left-facing arrows indicate
arterioles and shorter arrows with a circular base indicate areas
of notable immunoreactivity. The strongest Nrf-2 immunostaining
signals were observed in the lung tissues of rats in the OA group,
whereas immunostaining intensity decreased in the lung tissues of
rats in the prophylactic and therapeutic OLE groups. A, alveolus;
AD, alveolar duct; TB, terminal bronchiole; Pl, pleura; OA, oleic
acid; OLE, oleuropein; Nrf-2, nuclear factor erythroid 2-related
factor 2. |
Biochemical analysis
Blood samples and lung-tissue homogenates were
biochemically analyzed to determine MDA, LPO and SP-D concentration
in each experimental group, and TAS and TOS parameters were
measured. Intergroup comparisons for all analyzed biomarkers
demonstrated no significant differences (data not shown).
Discussion
ARDS is a condition that is characterized by acute
hypoxemic respiratory failure and the presence of bilateral
pulmonary infiltrates that cannot be explained by cardiac failure
or fluid overload (3). In a study
reported by Bellani et al (5), ARDS development was observed in 10.4%
of patients in intensive care units that exhibited acute hypoxemic
respiratory failure, demonstrating a mortality rate of ~40%
(5). In addition to these notable
mortality rates, the prevention and treatment of ARDS have become
more important due to notable morbidity rates, high intensive care
costs and the increasing number of ARDS cases associated with the
COVID-19 pandemic (8).
Supportive therapies remain the primary approach to
managing ARDS, specifically ventilator strategies (1). However, despite advances in intensive
care facilities, mortality rates remain high, as there are no
effective, targeted therapies for ARDS beyond supportive treatment
(1). This lack of effective ARDS
treatment has driven the search for targeted therapies, which has
been exemplified by previous studies (1,6). The
majority of these studies have focused on developing prophylactic
treatments aimed at preventing the development of ARDS (1,6).
Although these targeted therapies for ARDS prophylaxis appear
theoretically successful, the practical application of prophylactic
treatments remains limited due to the acute nature of ARDS
(1,6). Therefore, the present study compared
two different treatments: One treatment aimed at preventing the
development of ARDS and another aimed at reducing the severity of
ARDS after its development.
In the present study, OA was used to establish a rat
model of ARDS, as OA administration has been shown to rapidly cause
ARDS-like lung damage. Histological changes in the lungs during
this OA-induced damage are similar to the pathological changes
observed in the exudative phase of ARDS and manifest as edemas in
the interstitial and intra-alveolar regions, intra-alveolar
hemorrhages, intravascular coagulation and vascular congestion,
which can be observed minutes after IV administration of OA
(12). In the present study, these
pathological changes were also found to be notably more prominent
in the lung tissues of rats in the OA-induced ARDS model group
compared with those in the other groups. In addition, the present
study used OLE as a treatment to prevent and reduce the severity of
lung damage. The protective effect of OLE on OA-induced lung damage
was assessed by comparing the prophylactic administration of OLE,
which involved OLE treatment prior to inducing lung injury with OA,
with the therapeutic group, for which lung damage was induced
initially with OA and followed by OLE treatment.
OLE is the predominant phenolic compound present in
olive leaves and has notable anti-inflammatory, antioxidant and
anti-apoptotic activities. In a previous study by Xu et al
(10), OLE was shown to markedly
ameliorate lung ischemia-reperfusion injury by reducing the
activity of the toll-like receptor 4 signaling cascade in alveolar
macrophages (10). Caglayan et
al (13) demonstrated that OLE
can exert anti-inflammatory effects through lipoxygenase and
leukotriene B4 inhibition (13).
In a study reported by Dikmen et al (14), OLE was administered
prophylactically to rats by oral gavage for 20 days, demonstrating
that OLE reduced lipopolysaccharide-induced ALI. Based on the
aforementioned findings, a 20-day treatment period was deemed
impractical for the present study, which employed an ARDS disease
model; as ARDS demonstrates an acute and subtle disease onset, the
present study required a study plan that established prophylactic
and therapeutic treatment groups treated with a single dose of OLE.
To permit more rapid observations of treatment efficacy, OLE was
administered intraperitoneally rather than orally through gavage.
In the present study, a single dose of OLE (100 mg/kg) was selected
for use in treatments based on previous studies that have
demonstrated the biological efficacy and safety of OLE in
experimental models (10,13,14).
However, the absence of a dose-response analysis for OLE represents
a notable limitation of the present study. As such, further studies
involving multiple dose levels of OLE are required to determine the
optimal therapeutic range and dose-dependent effects.
In the present study, the lung tissues of rats were
examined via H&E staining; this primarily involved comparisons
between the lung tissues of rats in group 2 and other experimental
groups. The present study observed that the total damage score was
significantly reduced in rats treated with prophylactic OLE
compared with that of the model group. Compared with the model
group, a significant reduction in total damage score was also
observed in the group administered therapeutic OLE, but this
improvement was notably milder compared with that in the
prophylactic group. This difference may have been attributed to the
rapid and effective lung injury-inducing effect of OA and the short
duration before euthanasia in the present experimental model.
TNF-α was shown to serve a key role in regulating
the pathophysiology of ARDS. In a number of medical conditions,
such as sepsis, infection and tissue damage that causes ARDS, TNF-α
has been shown to activate various signaling pathways that: i)
Initiate early inflammation; ii) affect intercellular tight
junction proteins; iii) increase permeability in the
alveolo-capillary membrane; iv) decrease alveolar fluid clearance
capacity; and v) increase neutrophil infiltration, coagulation and
fibrin deposition (15-17).
Therefore, TNF-α immunoreactivity levels were assessed
immunohistochemically in the present study. TNF-α expression was
highest in the OA-induced ARDS model group. When compared with the
ARDS model group, TNF-α expression was significantly decreased in
rats receiving prophylactic or therapeutic OLE, although this
improvement was superior in the prophylactic OLE group.
Nrf-2 serves an important role in maintaining the
balance of antioxidants and regulating various forms of cell death,
such as ferroptosis and apoptosis, in the pathophysiology of ARDS
(18,19). In addition, a previous study
reported by Wei et al (20)
showed that tert-butylhydroquinone, an Nrf-2 activator, exerts a
protective effect on ARDS. In the present study, Nrf-2
immunoreactivity levels were evaluated immunohistochemically. The
OA-induced ARDS model group was shown to demonstrate the highest
Nrf-2 expression levels across all treatment groups. Compared with
the ARDS model group, Nrf-2 expression significantly decreased in
the groups receiving prophylactic or therapeutic OLE; this decrease
in Nrf-2 expression was notably larger in the prophylactic OLE
group than the therapeutic OLE group.
The present study aimed to contribute to the
development of targeted therapies for ARDS by using two different
compounds derived from the same raw material, namely olive fruit
and leaves (9,21). As such, lung damage was induced
with OA and the efficacy of subsequent treatments with OLE was
evaluated. Based on the histopathological and immunohistochemical
findings of the present study, OLE demonstrated the ability to
exert both protective and therapeutic effects in the targeted
treatment of ARDS. Notably, the prophylactic effects of OLE
administration on ARDS were found to be more potent than its
therapeutic effects. This may have been due to the rapid and potent
injury-inducing effects of OA after IV injection.
No statistically significant differences were
observed in the biochemical parameters evaluated in the serum and
lung-tissue homogenates of rats across treatment groups. Notably,
the majority of the biochemical parameters evaluated in ARDS
studies, such as TAS, TOS and MDA and LPO concentrations, have been
used to measure oxidant/antioxidant molecule regulation. The role
of free oxygen radicals remains controversial in OA-induced models
of lung injury. SP-D has been evaluated as an important indicator
of alveolar epithelial integrity and lung damage (22). The aim of the present study was to
analyze the levels of this molecule to determine the degree of
damage in ARDS/ALI models; no significant difference (P>0.05)
was observed in SP-D levels between groups. McGuigan et al
(23) demonstrated that OA-induced
ARDS models did not exhibit notable free oxygen radical levels.
OA-induced ARDS animal models mimic the early/exudative phase of
ARDS, in which free oxygen radicals do not contribute to lung
injury (23). The lack of
statistically significant biochemical differences between treatment
groups, despite distinct histopathological and immunohistochemical
findings, may be explained by this underlying mechanism of ARDS
pathophysiology. Additionally, OA has been shown to induce the
rapid development of lung injury, with structural and inflammatory
changes occurring within minutes of administration, whereas
systemic oxidative stress markers may require a longer time to
reach detectable levels (10,19).
This temporal mismatch may further explain the absence of
significant differences in biochemical parameters despite clear
histopathological and immunohistochemical findings; the relatively
short experimental duration of the present study (4 h) may have
limited the detectability of systemic biochemical alterations. In
addition, although the OA-induced ARDS model has been shown to
reproduce key features of early-phase ARDS, this model does not
fully reflect the complex and heterogeneous nature of this disease
in humans (12). Therefore, the
findings of the present study should be interpreted as preclinical
evidence; further studies, including dose-optimization studies,
pharmacokinetic analyses and clinical trials, are required before
clinical application of OLE can be considered.
In conclusion, additional studies are required to
develop targeted therapies for ARDS. The present study demonstrated
that OLE exhibited notable potential for both protective and
therapeutic effects on ARDS. The present study, alongside similar
future studies, will further elucidate potential targeted
therapeutic agents for ARDS and therefore guide more comprehensive
research in the future.
Acknowledgements
Not applicable.
Funding
Funding: The present study was funded by the Scientific Research
Project Unit of Mersin University Rectorate (grant no.
2025-TP3-5282).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TUK, KB and MOK were responsible for the
experimental design and conceptualization of the study. TUK, KB, TA
and MOK performed literature searches. TUK, LB, ÇÇ, KB, TA and MOK
were responsible for performing the animal experiments. TUK and LB
contributed towards data collection and processing. TUK, LB and MOK
confirm the authenticity of all the raw data. TUK, LB, ÇÇ and KB
were responsible for the analysis and interpretation of results.
TUK, LB, TA and MOK wrote the original draft of the manuscript. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Ethical approval for the present study was obtained
from the Local Ethics Committee for Animal Experiments at Mersin
University (Mersin, Türkiye; approval no. 2024/25; dated September
27, 2024).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gorman EA, O'Kane CM and McAuley DF: Acute
respiratory distress syndrome in adults: Diagnosis, outcomes,
long-term sequelae, and management. Lancet. 400:1157–1170.
2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Ashbaugh DG, Bigelow DB, Petty TL and
Levine BE: Acute respiratory distress in adults. Lancet. 2:319–323.
1967.PubMed/NCBI View Article : Google Scholar
|
|
3
|
ARDS Definition Task Force. Ranieri VM,
Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E,
Camporota L and Slutsky AS: Acute respiratory distress syndrome:
The Berlin Definition. JAMA. 307:2526–2533. 2012.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Butt Y, Kurdowska A and Allen TC: Acute
lung injury: A clinical and molecular review. Arch Pathol Lab Med.
140:345–350. 2016.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Bellani G, Laffey JG, Pham T, Fan E,
Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley
DF, et al: Epidemiology, patterns of care, and mortality for
patients with acute respiratory distress syndrome in intensive care
units in 50 countries. JAMA. 315:788–800. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Mokrá D: Acute lung injury - from
pathophysiology to treatment. Physiol Res. 69 (Suppl 3):S353–S366.
2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Unruh HW: Katzenstein and Askin's surgical
pathology of non-neoplastic lung disease. Can J Surg.
40(394)1997.
|
|
8
|
Hussain M, Khurram Syed S, Fatima M,
Shaukat S, Saadullah M, Alqahtani AM, Alqahtani T, Bin Emran T,
Alamri AH, Barkat MQ and Wu X: Acute respiratory distress Syndrome
and COVID-19: A literature review. J Inflamm Res. 14:7225–7242.
2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Ahamad J, Toufeeq I, Khan MA, Ameen MSM,
Anwer ET, Uthirapathy S, Mir SR and Ahmad J: Oleuropein: A natural
antioxidant molecule in the treatment of metabolic syndrome.
Phytother Res. 33:3112–3128. 2019.PubMed/NCBI View
Article : Google Scholar
|
|
10
|
Xu Z, Sun X, Ding B, Zi M and Ma Y:
Oleuropein ameliorated lung ischemia-reperfusion injury by
inhibiting TLR4 signaling cascade in alveolar macrophages. Transpl
Immunol. 74(101664)2022.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Aggul AG, Gulaboglu M, Cetin M, Ozakar E,
Ozakar RS and Aydin T: Effects of emulsion formulations of
oleuropein isolated from ethanol extract of olive leaf in diabetic
rats. An Acad Bras Cienc. 92(e20190810)2020.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Dickey BF, Thrall RS, McCormick JR and
Ward PA: Oleic-acid-induced lung injury in the rat. Failure of
indomethacin treatment or complement depletion to ablate lung
injury. Am J Pathol. 103:376–383. 1981.PubMed/NCBI
|
|
13
|
Caglayan K, Güngör B, Cinar H, Avci B, Gur
S and Arslan N: Effects of oleuropein on serum inflammatory
cytokines and histopathological changes in rats with pancreatitis.
Adv Clin Exp Med. 24:213–218. 2015.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Dikmen N, Cellat M, Etyemez M, İşler CT,
Uyar A, Aydın T and Güvenç M: Ameliorative effects of oleuropein on
lipopolysaccharide-induced acute lung injury model in rats.
Inflammation. 44:2246–2259. 2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Huang Q, Le Y, Li S and Bian Y: Signaling
pathways and potential therapeutic targets in acute respiratory
distress syndrome (ARDS). Respir Res. 25(30)2024.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Mazzon E and Cuzzocrea S: Role of
TNF-alpha in lung tight junction alteration in mouse model of acute
lung inflammation. Respir Res. 8(75)2007.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Patel BV, Wilson MR, O'Dea KP and Takata
M: TNF-induced death signaling triggers alveolar epithelial
dysfunction in acute lung injury. J Immunol. 190:4274–4282.
2013.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Liu Q, Gao Y and Ci X: Role of Nrf2 and
its activators in respiratory diseases. Oxid Med Cell Longev.
2019(7090534)2019.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Deng J, Li N, Hao L, Li S, Aiyu N, Zhang J
and Hu X: Transcription factor NF-E2-related factor 2 plays a
critical role in acute lung injury/acute respiratory distress
syndrome (ALI/ARDS) by regulating ferroptosis. PeerJ.
12(e17692)2024.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Wei J, Chen G, Shi X, Zhou H, Liu M, Chen
Y, Feng D, Zhang P, Wu L and Lv X: Nrf2 activation protects against
intratracheal LPS induced mouse/murine acute respiratory distress
syndrome by regulating macrophage polarization. Biochem Biophys Res
Commun. 500:790–796. 2018.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Lopez S, Bermudez B, Montserrat-de la Paz
S, Jaramillo S, Varela LM, Ortega-Gomez A, Abia R and Muriana FJ:
Membrane composition and dynamics: A target of bioactive virgin
olive oil constituents. Biochim Biophys Acta. 1838:1638–1656.
2014.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Peukert K, Seeliger B, Fox M, Feuerborn C,
Sauer A, Schuss P, Schneider M, David S, Welte T, Putensen C, et
al: SP-D serum levels reveal distinct epithelial damage in direct
human ARDS. J Clin Med. 10(737)2021.PubMed/NCBI View Article : Google Scholar
|
|
23
|
McGuigan RM, Mullenix P, Norlund LL, Ward
D, Walts M and Azarow K: Acute lung injury using oleic acid in the
laboratory rat: Establishment of a working model and evidence
against free radicals in the acute phase. Curr Surg. 60:412–417.
2003.PubMed/NCBI View Article : Google Scholar
|