Introduction
Spontaneous dural arteriovenous fistula (DAVF) is a
relatively rare pathological condition, representing 10-15% of all
intracranial arteriovenous malformations, including ~6% of
supratentorial and 35% of infratentorial vascular malformations
(1). The reported annual incidence
is ~0.15 per 100,000 individuals, and DAVFs are most frequently
diagnosed in patients aged 40-60 years (2). DAVF is primarily characterized by
arterial blood flow that drains directly into the cavernous sinus
(CS) via an abnormal arteriovenous fistula. This abnormal drainage
may lead to increased intracranial pressure and various cerebral
complications (3). This condition
exhibits a predilection for middle-aged men and is often associated
with hypertension, trauma or other vascular pathologies.
Epidemiological data on DAVF indicate a low incidence rate, and its
clinical symptoms are complex and varied, which increases the
difficulty of diagnosis (2).
Typical clinical manifestations include ocular symptoms, such as
exophthalmos and conjunctival congestion, as well as neurological
symptoms. In the early stages, these symptoms may be atypical and
are easily misdiagnosed as common ocular diseases, such as
conjunctivitis (4). The current
study reports a case of spontaneous CS-DAVF complicated by remote
cerebellar hemorrhage. The study highlights the potential
complications and diagnostic challenges associated with this
condition, offering valuable insights for similar cases.
Case report
A 52-year-old man presented to The Second People's
Hospital of Liao Cheng (Linqing, China) in December 2023 with
nausea, vomiting and decreased appetite. A total of 10 days prior
to this, the patient had developed redness of the left conjunctiva
accompanied by a foreign body sensation in the left eye and was
initially diagnosed with conjunctivitis. Oral antibiotic therapy
with amoxicillin was administered and yielded poor results, with
persisting symptoms; the exact dose and duration are not available.
The patient had a history of hypertension and denied any trauma. On
admission, a physical examination revealed the following:
Temperature, 36.5˚C (normal range, 36.0-37.3˚C); pulse, 64
beats/min (normal range, 60-100 beats/min); respiratory rate, 16
breaths/minute (normal range, 12-20 breaths/min); and blood
pressure, 154/104 mmHg (normal range, <140/90 mmHg for an adult
male). No facial weakness, sensory disturbance, dysarthria, ataxia
or gait instability was observed. Bilateral pupillary light
reflexes were intact, and no visual acuity deterioration, proptosis
or tinnitus was noted. The patient was conscious and oriented, with
left conjunctival congestion and mild limitation of the abduction
of the left eye. An abdominal examination revealed a soft abdomen
without tenderness or rebound pain. No hepatic or renal percussion
tenderness was elicited. Bowel sounds were normal, and the lower
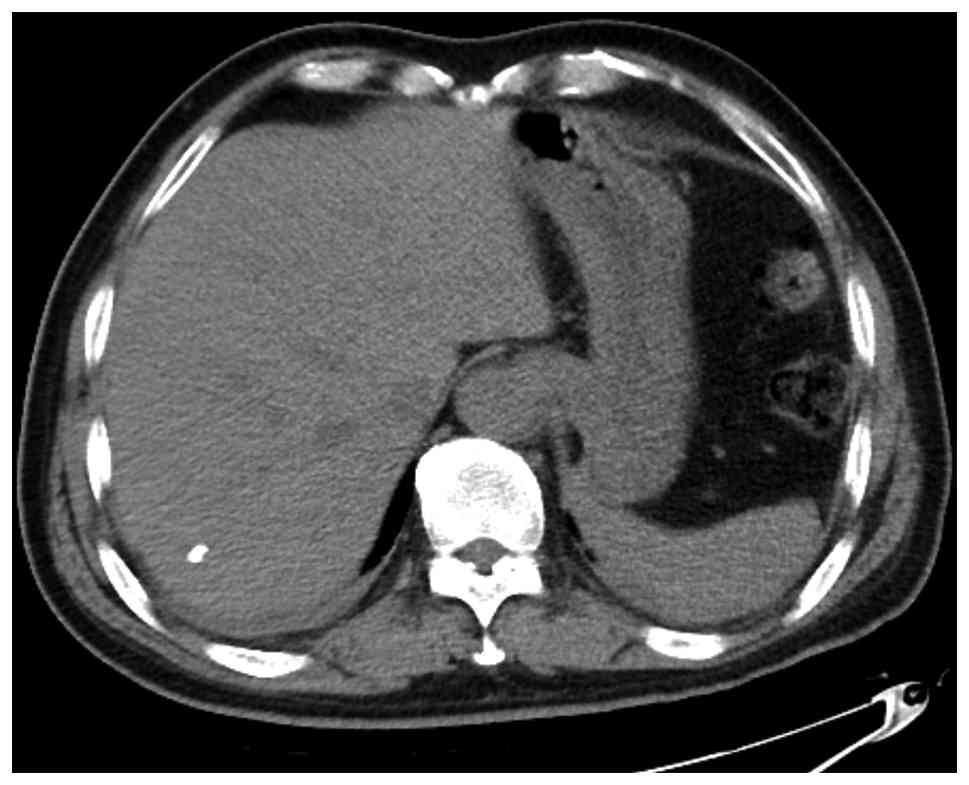
extremities were free of edema. Routine laboratory investigations,
including coagulation function, were unremarkable. Further workup
with a non-contrast computed tomography scan of the whole abdomen
demonstrated hepatic calcifications (Fig. 1). Despite symptomatic supportive
treatment, including antiemetics and hydration, which yielded mild
improvement in the vomiting, the left conjunctival congestion
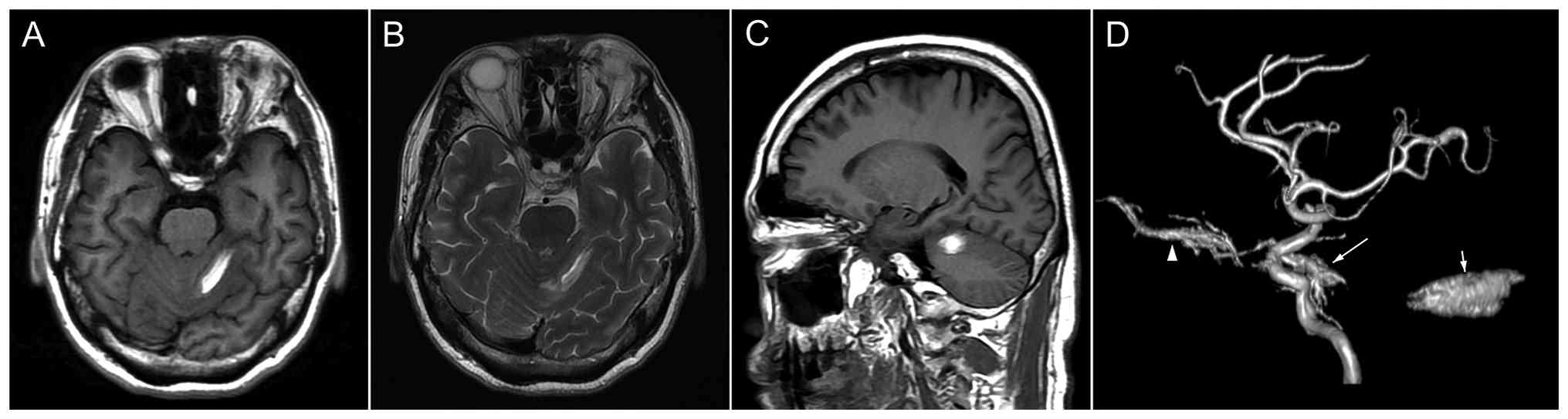
persisted severely. Further head magnetic resonance imaging
demonstrated a subacute intracerebral hemorrhage in the left
cerebellar hemisphere (Fig. 2A-C),
and magnetic resonance angiography revealed a left CS fistula
(Fig. 2D). Therefore, the patient
was transferred to the Department of Neurosurgery for further
management.
After the exclusion of surgical contraindications,
the patient underwent a diagnostic angiography in January 2024, for
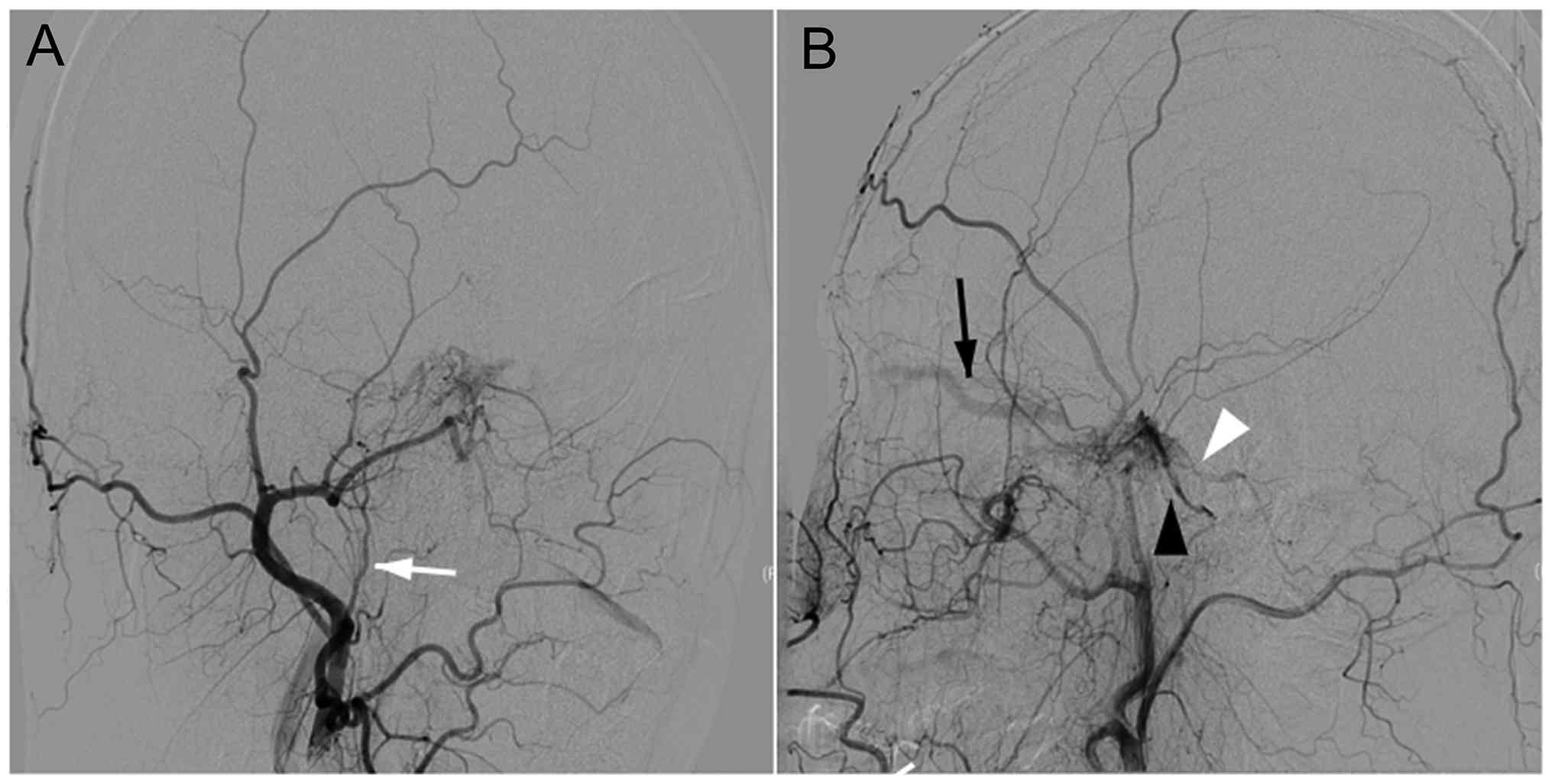
a comprehensive assessment of the vascular pathology. Selective
angiography of the left external carotid artery revealed a vascular
network arising from the distal branches of the ascending
pharyngeal artery and supplying the CS. Drainage was observed into
the ophthalmic vein, inferior petrosal sinus and superior petrosal
sinus, confirming the presence of a CS-DAVF (Fig. 3).
The patient underwent an interventional embolization
for the DAVF on day 6 post-presentation. During the procedure, a 5F
single-curve angiographic catheter was selectively advanced into
the left internal jugular vein over a Glidewire® (Terumo
Medical Corporation), with the tip positioned at the junction of
the inferior petrosal sinus and jugular vein. The patency of the
inferior petrosal sinus was confirmed by Glidewire exploration,
which successfully accessed the CS. A pre-shaped Echelon-10
(Medtronic plc) microcatheter was then navigated over a microwire
into the anterior CS, adjacent to the origin of the ophthalmic
vein. Microcatheter angiography confirmed the intracavernous
position. Multiple coils were deployed in a basket configuration,
embolizing the ophthalmic vein origin and anterior CS. After
preparing the microcatheter with a dimethyl sulfoxide flush,
Onyx-18 (Medtronic plc) was slowly injected through the
microcatheter, permeating the ophthalmic vein origin, CS
compartments and fistula sites.
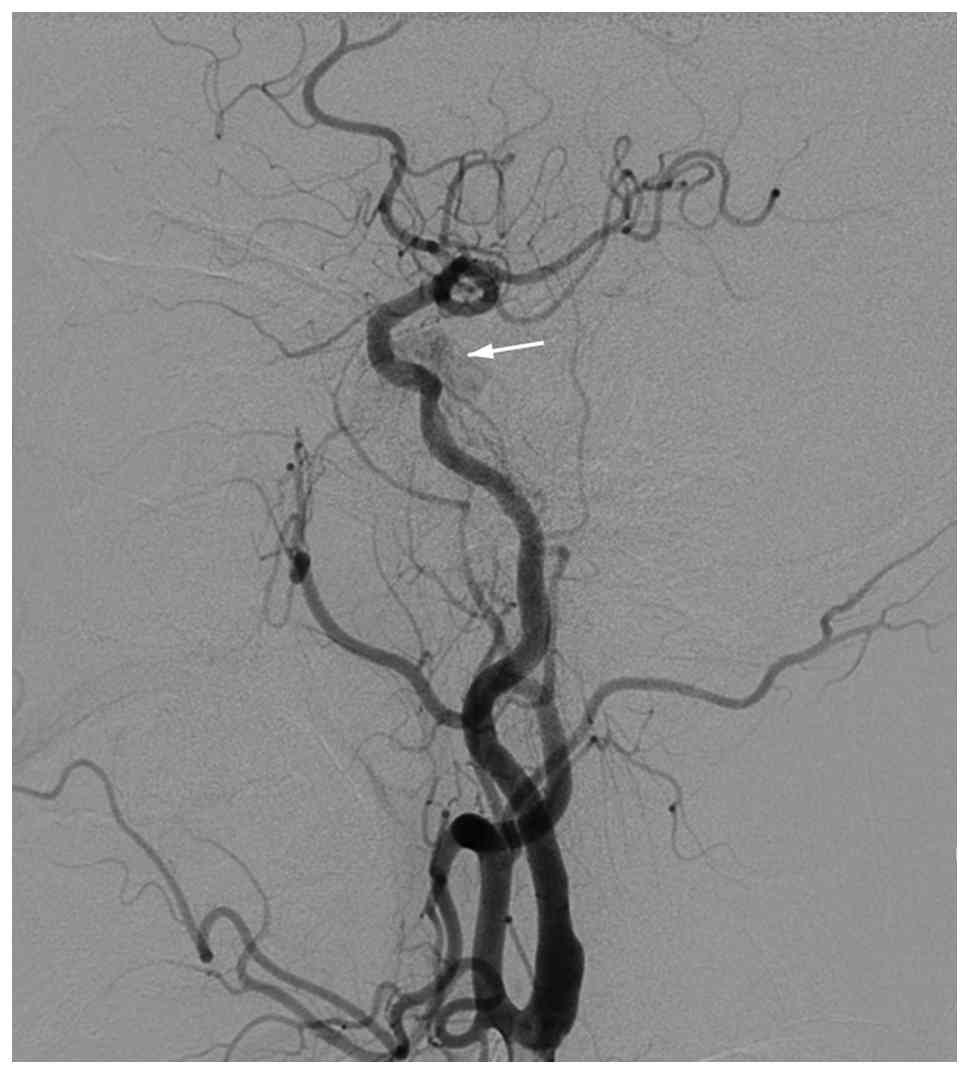
Post-embolization bilateral common carotid
angiography revealed complete occlusion of the left CS, with
visible coil mesh and Onyx cast. No opacification was identified in
the ophthalmic vein and superior petrosal sinus, while the delayed
venous phase showed minimal faint opacification in the
posterosuperior CS draining into the inferior petrosal sinus
(Fig. 4). The procedure was
successfully completed with adequate anesthesia. Postoperatively,
the patient received nutritional support, dexamethasone (5 mg,
intravenous, stat), glycerol fructose (250 ml, intravenous drip,
every 12 h) to reduce intracranial pressure, and vitamin B6 (0.2 g,
intravenous drip, once daily) for neurotrophic support. At the
1-week follow-up, the left conjunctival edema had improved compared
with the preprocedural status, with mild restriction of left ocular
movement and preserved limb mobility, muscle strength and muscle
tone. No postoperative hemorrhagic, ischemic or infectious
complications were observed during hospitalization. At the 1-month
follow-up, the patient showed marked improvement in conjunctival
congestion and ocular motility, without evidence of recurrent
hemorrhage or neurological deficits. The patient is scheduled for
regular clinical and imaging follow-up every 3 months to monitor
for recurrence. The prognosis of the patient is considered
favorable based on the complete occlusion of the fistula and the
progressive resolution of symptoms.
Discussion
Spontaneous DAVF in the CS region is an uncommon
vascular malformation, typically characterized by ophthalmic and
neurological symptoms, such as ocular motility disorders, elevated
intraocular pressure and headaches (4). Current literature indicates that
patients are frequently misdiagnosed with mild ocular conditions,
such as conjunctivitis, at the initial presentation, leading to a
delay in appropriate treatment (3,5). In
the current case, the patient presented with remote cerebellar
hemorrhage, an atypical manifestation that may be attributed to
hemodynamic changes in the CS, especially in cases of obstructed
venous drainage of the orbit (6,7).
This unusual manifestation underscores the complexity of DAVF and
the severity of its associated symptoms.
Clinically, the diagnosis of DAVF often faces
challenges, as early symptoms can easily be confused with other
diseases. Patients may seek medical attention due to ocular
symptoms such as conjunctival congestion, and the preliminary
diagnosis is often misidentified as conjunctivitis (4). Therefore, in radiological evaluation,
it is crucial to pay close attention to the abnormal signals on
cranial MR and the manifestations of cerebral hemorrhage,
particularly in patients presenting with concomitant ocular and
neurological signs. Therapeutically, interventional embolization
has demonstrated favorable outcomes in managing DAVF, effectively
alleviating symptoms and improving quality of life (8,9). The
treatment plan for the present case was determined through a
multidisciplinary consultation, considering the patient's high-risk
factors, particularly hypertension, emphasizing the necessity of
early recognition and intervention (10). Future research should further
explore the optimal management strategies and epidemiological
characteristics of different DAVF subtypes, thereby optimizing
clinical outcomes and mitigating complications (11,12).
From the pathological perspective, the development
of CS arteriovenous fistula is closely associated with
hypertension, particularly in non-traumatic cases. The etiology of
DAVF is likely multifactorial, involving hypertension, chronic
venous obstruction and other vascular lesions. Arteriovenous
fistulas in non-traumatic patients usually occur in the setting of
elevated venous pressure. Long-term venous hypertension may lead to
vascular wall fragility and pathological remodeling, thereby
promoting the formation of fistulas, resulting in the direct
shunting of arterial blood into the venous system (13,14).
This abnormal blood flow pattern may lead to venous hypertension,
especially in cases where venous drainage from the eye is
obstructed. When the pressure within the CS increases, it may
induce hemodynamic alterations at distant sites. Common causes of
distant cerebellar hemorrhage include arterial embolism and
ischemia, lesions of the venous system, traumatic factors, tumors,
cerebral infections or inflammation (15). At presentation, the current patient
lacked common precipitating factors, such as arterial embolism,
ischemia or trauma. Therefore, the condition was attributed to the
DAVF-induced abnormal hemodynamics.
The clinical significance of the present case lies
in the accompanying remote cerebellar hemorrhage, underscoring the
intricate pathological mechanisms associated with DAVF. Through
detailed analysis, the case reminds clinicians to maintain a high
level of vigilance for similar symptoms to prevent a misdiagnosis
and delays in treatment. Imaging studies play a key role in the
diagnosis of DAVF, especially when the patient presents with ocular
and neurological symptoms (4).
There are certain limitations to the present study.
Firstly, this is a single-case report describing a rare
presentation of CS-DAVF associated with remote cerebellar
hemorrhage. Therefore, the findings may not be generalizable to all
patients with DAVF. Secondly, the retrospective nature of this
report may have introduced incomplete clinical information and
potential publication bias related to the rarity of the condition.
Thirdly, the follow-up period was relatively short, limiting
comprehensive evaluation of the long-term prognosis and recurrence
risk after endovascular treatment. In addition, the diagnostic
evaluation and treatment strategy were based on single-center
clinical experience, which may differ across institutions. Further
multicenter studies with larger sample sizes are needed to better
clarify the clinical characteristics, pathophysiological mechanisms
and optimal management strategies of DAVF. Despite the inherent
limitations of this study, it offers valuable insights for clinical
practice and emphasizes the importance of early recognition and
intervention for DAVF. This report paves the way for further
investigations, aiming to improve the understanding of DAVF and
subsequently enhance the overall prognosis for patients.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
TJB and JL contributed to the conception and design
of the case report, analysis and interpretation of the clinical
data, and critical revision of the manuscript for important
intellectual content. YZS and SLZ acquired and organized the
clinical data, including laboratory results, medical images and
follow-up information, and participated in the analysis and
interpretation of the patient's clinical course. YHW contributed to
the study design, data acquisition and interpretation, performed
the literature review, and drafted the manuscript. All authors have
read and approved the final manuscript. TJB, JL, YZS, SLZ and YHW
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient in this study received standard clinical
practice and provided written informed consent for the publication
of any medical data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Rhim JK, Cho YD, Yoo DH, Kang HS, Cho WS,
Kim JE, Cho MJ, Hwang G, Kwon OK and Han MH: Endovascular treatment
of bilateral cavernous sinus dural arteriovenous fistula:
Therapeutic strategy and follow-up outcomes. Korean J Radiol.
19:334–341. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Maciejewski K, Pinkiewicz M, Mruk B, Knap
D, Zaczyński A, Walecki J and Zawadzki M: A practical approach to
intracranial dural arteriovenous fistulas: Pathogenesis,
classification and management. J Clin Med. 14(6895)2025.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Roy T, van den Berg R, Brandsen RP and
Saeed PO: Likelihood of spontaneous closure of cavernous sinus
dural arteriovenous fistulas based on clinical and radiological
findings. Interv Neuroradiol. 31:344–351. 2023.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Thiyagarajam K, Chong MF and Mohd Khialdin
S: The diagnostic challenges in carotid cavernous fistula: A case
series. Cureus. 13(e19696)2021.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Kato M, Maki Y, Nakada Y, Shirai S and Ono
Y: Three cases of spontaneous bilateral external carotid-cavernous
sinus fistula (dural arteriovenous shunts in the region of the
cavernous sinus). No Shinkei Geka (Japanese). 3:607–613.
1975.PubMed/NCBI
|
|
6
|
Moster ML, Sergott RC and Grossman RI:
Dural carotid-cavernous sinus vascular malformation with facial
nerve paresis. Can J Ophthalmol. 23:27–29. 1988.PubMed/NCBI
|
|
7
|
Dixit N, Sharma A and Hosur B: Remote
cerebellar hemorrhage: A bleed not too far! Neurol. India.
71:1088–1089. 2023.PubMed/NCBI View Article : Google Scholar
|
|
8
|
He HW, Jiang CH, Wu ZX, Li YX, Lü XL and
Wang ZC: Transvenous embolization with a combination of detachable
coils and onyx for a complicated cavernous dural arteriovenous
fistula. Chin Med J (Engl). 121:1651–1655. 2008.PubMed/NCBI
|
|
9
|
Kato S, Ishihara H, Nakayama H, Fujii M,
Fujisawa H, Kajiwara K, Nomura S, Sadanaga H and Suzuki M:
Transvenous embolization for dural arteriovenous shunt of the
cavernous sinus. Comparison of multi-staged transvenous
embolization and transvenous embolization with sinus packing.
Interv Neuroradiol. 13:353–358. 2007.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Nakagawa H, Kubo S, Nakajima Y, Izumoto S
and Fujita T: Shifting of dural arteriovenous malformation from the
cavernous sinus to the sigmoid sinus to the transverse sinus after
transvenous embolization. A case of left spontaneous
carotid-cavernous sinus fistula. Surg Neurol. 37:30–38.
1992.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Komiyama M, Nishikawa M and Yasui T:
Transient monocular blindness during manual carotid compression for
carotid-cavernous sinus fistulas-Two case reports. Neurol Med Chir
(Tokyo). 36:805–807. 1996.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Li W, Liu Y, Chu F and Wang YL:
Interventional embolization of unilateral cavernous sinus with onxy
glue combined with coils for the treatment of bilateral dural
arteriovenous fistula. J Craniofac Surg. 35:e451–e454.
2024.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Li H, Wang Y, Li L, Niu X and Zhang J:
Clinical characteristics, imaging, treatment, and prognosis of
dural arteriovenous fistula presented with parkinsonism-A
systematic review. Neurosurg Rev. 48(625)2025.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Shapiro M, Raz E, Litao M, Becske T, Riina
H and Nelson PK: Investigating the pathophysiology of intracranial
dural arteriovenous fistulas with associated cerebellar hemorrhage.
Stroke. 52:1381–1387. 2021.
|
|
15
|
Arismendi Morillo GJ, Fernández Abreu MC,
Cardozo Sosa DP and Cardozo JJ: Lesiones ocupantes de espacio no
neoplasicas que simulan tumores del sistema nervioso central. Rev
Neurol. 38:427–430. 2004.PubMed/NCBI
|