1. Introduction
Celiac disease (CD) is a chronic T-cell mediated
intestinal inflammatory condition, caused by the ingestion of
gluten in genetically susceptible individuals who carry the human
leukocyte antigen (HLA)-DQ2 and HLA-DQ8 haplotypes (1,2).
Gluten is a storage protein of wheat and is also found in related
grains, such as rye, barley and spelt. CD affects ~1% of the
population worldwide. The HLA-DQ haplotype is strongly associated
with the development of CD. CD is an interplay between the adaptive
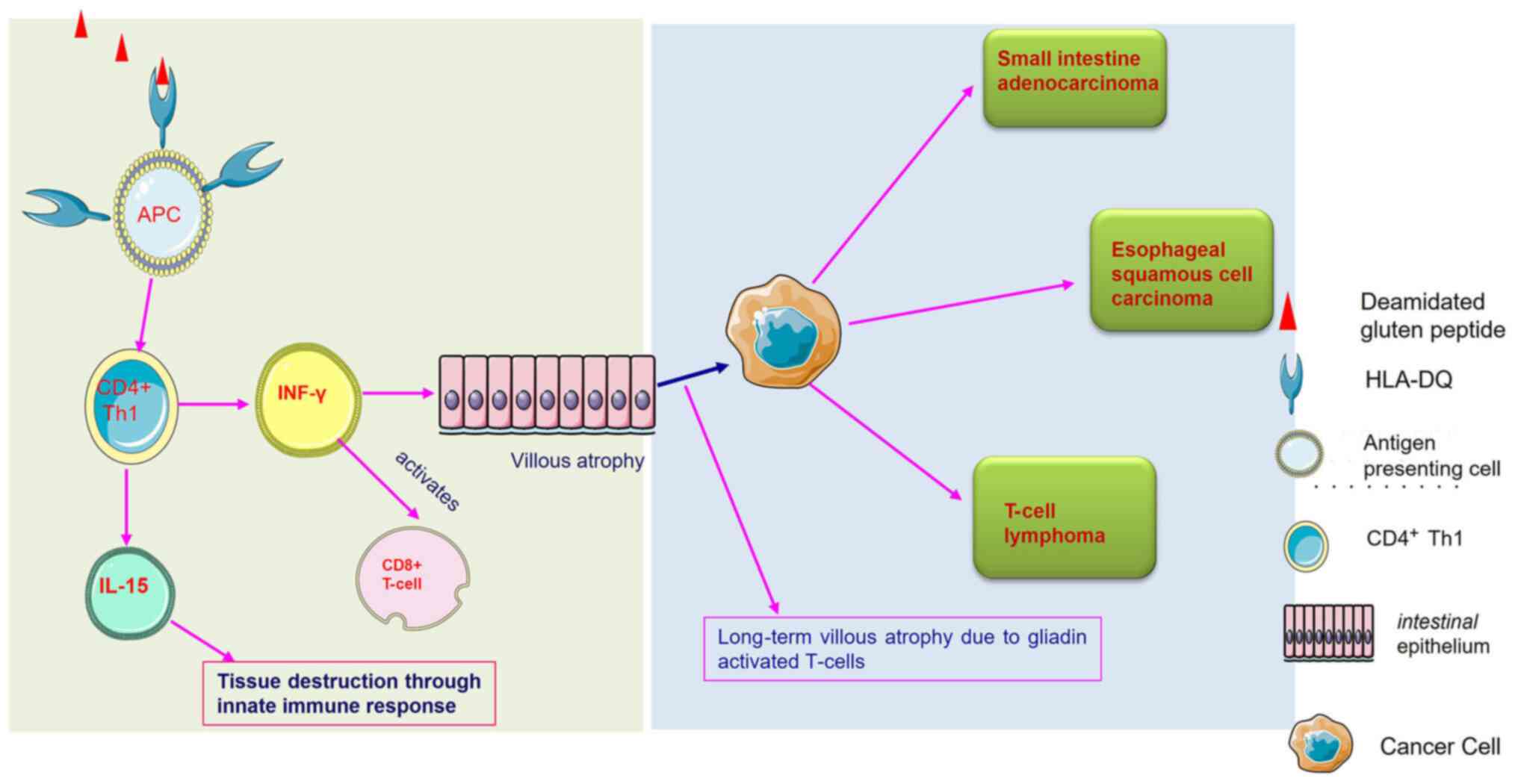
and innate immune systems. The gluten peptide is deamidated by the
tissue transglutaminase (tTG) enzyme on gluten consumption in
patients with CD. Deamidated gluten protein is recognized by the
HLA-DQ molecules that activate CD4+ T lymphocytes that
secrete interferon (IFN)-γ, causing the destruction of the small
intestinal mucosa. Gliadin peptide can also trigger innate immune
components (e.g., IL-15), leading to intestinal tissue damage.
Hence, the elimination of gluten is strongly recommended in CD, and
a strict and life-long gluten-free diet (GFD) is the only accepted
treatment (3). Complete adherence
to a GFD heals the mucosal injury and leads to the remission of
celiac-related symptoms (e.g., frequent diarrhoea) (4) Daily exposure to even a minor amount
of gluten traces is able to restore chronic inflammation and
CD-related symptoms (5). Hence,
complete gluten elimination is strictly required to heal the
damaged intestinal mucosa. As gluten is a pervasive molecule, it is
challenging to eliminate gluten from the diet. Several other
factors, such as availability, cost and product labelling prevent
the adherence to a GFD (6).
Continuous exposure to gluten severely affects CD management and
may cause a complex condition known as a refractory CD, in which
patients do not respond to a GFD (7).
Cancer is a life-threatening disease marked by
uncontrollable, disorganized and undesired cell division. Cancer
encompasses >200 diseases, and according to the World Health
Organization (WHO), cancer is one of the most severe medical issues
confronting humanity in the 21st century. In 2019, the WHO placed
cancer in the first or second position as the cause of mortality
for individuals <70 years of age in 112 countries (8). Cancer is likely to become the most
prevalent cause of mortality due to increased diagnostics,
insufficient health care, and poor lifestyle habits and diet
(9). Based on a study involving
over 7,000 tumour samples and 29 cancer types, it was found that 1
to 10 mutations are required for cancer to grow (10). Hereditary cancers are caused by a
prior family history of the disease. By contrast, sporadic cancer
is caused by environmental factors, such as comorbidities,
lifestyle habits, or the use of specific medicines, such as
immunosuppressants (10).
In recent decades, several studies have confirmed
that the long-term constant exposure to gluten traces is associated
with an increased risk of developing certain types of cancer. In
the first set of studies, Green et al (11) in 2003 reported a connection between
cancer and CD. Later on, various studies demonstrated that the risk
of developing certain types of cancer, such as lymphoma and
oropharyngeal cancer increased at alarming rates in patients with
CD (12-14).
There is also evidence to indicate an association between CD and
cancer development, primarily intestinal cancer (13-16).
In a recent nationwide cohort study, Lebwohl et al (17) reported that patients with CD were
at an increased risk of developing cancer, particularly those
diagnosed with CD after the age of 40.
The present review article addresses the prominent
link between CD and certain types of cancer, and the role of a GFD.
Furthermore, the present review also discusses whether a strict GFD
increases or decreases the risk of developing CD-associated
cancer.
2. Celiac disease: Pathophysiology
Celiac disease occurs upon exposure to gluten in
susceptible individuals. Gluten protein contains a 33-mer protein
sequence rich in the repetitive sequence of proline and glutamine,
which develops due to the partial digestion of wheat molecules;
this specific sequence remains highly stable toward the breakdown
by all gastric, pancreatic and intestinal brush border membrane
endoprotease (18). Hence, when a
CD-affected individual consumes wheat, the wheat peptides are
partially digested, and relatively large gluten peptides are
transported across the mucosal epithelium (19), where tTG enzymes are entangled with
processed gluten peptides and deamidated glutamine into negatively
charged glutamic acid. These negatively charged glutamic acid
residues increase the binding affinity for the disease-relevant
HLA-DQ2/-DQ8 molecules. Once bound to the HLA-DQ2/8 molecule, this
gluten-HLA-DQ complex activates the CD4 T-helper 1 (Th1) cells
(20). The gluten-reactive CD4
T-cells produce IFN-γ upon activation. T-cells also stimulate the
production of IFN-γ in the epithelium. T-cells migrate to the
epithelium and facilitate the killing of enterocytes that
eventually damages the intestinal mucosa, leading to partial/total
villous atrophy (21).
CD is a systemic disease. It is associated with
other similar autoimmune diseases. HLA-DQ molecules that cause
susceptibility to CD also play a role in type 1 diabetes mellitus
(T1DM), the pathophysiology of which is identical to CD (22). HLA-DQ molecules bind and present
β-cell autoantigen derived peptides in T1DM. CD exhibits genetic
similarity with another autoimmune diseases, such as rheumatoid
arthritis (RA). Hence, patients with CD remain at risk of
developing T1DM and RA (23,24).
Furthermore, gluten has been shown to be frequently associated with
neurological disorders, such as cerebellar ataxia, peripheral
neuropathy, seizures, headaches, cognitive impairment and
neuropsychiatric diseases (25).
However, a relief in the symptoms has been reported upon the
implementation of a GFD in such conditions (26).
3. Role of the gut microbiota in celiac
disease
According to increasing evidence, changes in gut
microbiome composition and function are linked to various chronic
inflammatory diseases, including obesity, diabetes, inflammatory
bowel disease and cancer (27).
This may also be the case with CD. Gluten metabolism is aided by
the gut bacteria found in the human colon. Lactobacilli and
Bifidobacterium spp. may play a role in modifying the
immunogenic potential of gluten and its peptides (28). Patients implementing a long-term
GFD who have persistent symptoms of CD have an altered microbial
gut composition, with significant differences between patients with
classic gastrointestinal symptoms (such as weight loss and
diarrhoea) and patients with extraintestinal manifestations (such
as anaemia, malabsorption of iron, folate, Vitamin D, calcium and
short stature) (29). Intestinal
dysbiosis has been documented in patients with CD, whether
untreated or treated with a GFD, compared with healthy
participants. Recent investigations on patients with CD have found
an increase in the relative amounts of Gram-negative bacterial
genera, including Bacteroides, Prevotella and
Escherichia, and a decrease in the relative amounts of
beneficial anti-inflammatory bacteria, such as
Bifidobacteria and lactobacilli. Dysbiotic microbiota can
cause a dysregulated immunological response, contributing to CD
pathogenesis. Antibiotic usage and certain feeding habits during
infancy may also lead to changes in the developing gut microbiota,
affecting immunological maturation and predisposing the individual
to CD. De Palma et al (30)
found that the milk-feeding style, in combination with the HLA-DQ
genotype, affected the gut microbiota of newborns in a study
involving 164 healthy newborns with one first-degree relative with
CD. The discovery of the role of intestinal bacteria in the
development of CD opens up new avenues for treatment with
probiotics. However, further research is required in this field
(28).
4. Association between celiac disease and an
increased risk of cancer
Chronic inflammation is one of the hallmarks of
cancer, and chronic intestinal inflammation remains associated with
the development of CD (16,31,32).
Therefore, it can be considered that CD can lead to the development
of certain types of cancer, particularly cancers related to the
gastrointestinal tract (Fig.
1).
Cancer is a manifestation of immune system
abnormalities, since malignant cells avoid detection and removal by
the immune system. Tumour growth is further aided by chronic
infections and inflammation associated with polarised or limited
immune responses. The tumour immune environment refers to the
conditions and factors that enable malignant cells to survive
(9). In the case of CD, it is most
likely related to how the human body reacts to the inflammation,
intestinal damage and nutritional deficits caused by villous
atrophy (33). T-cells in the
bowel are generally ‘tissue-healing’ cells that protect the body.
T-cells, on the other hand, generate inflammation in patients with
CD when they are exposed to gluten. This inflammation damages the
gut lining, resulting in acute symptoms in patients with CD
following the consumption of gluten (34). Patients with CD primarily develop
an adaptive T-cell-mediated immune response. However, in cancer
development, apart from T-cells, natural killer (NK) T-cells also
play an essential role. These cells are a subset of T-cells
involved indirectly, inducing the death of tumour cells when
activated. In patients with CD, the NK T-cell count remains low
compared with healthy subjects. The loss of these immunoregulatory
cells may lead to the improper activation of gluten-sensitive
T-cells, resulting in intestinal damage (35). The association between different
types of cancer and CD is summarised in the following sections, and
a summary of their association is presented in Table I and Fig. 1.
 | Table IAssociation between celiac disease
and various types of cancer. |
Table I
Association between celiac disease
and various types of cancer.
| No. | Cancer type | Risk | Mechanism | Author/(Refs.),
Year |
|---|
| 1. | Oesophageal | High | Due to GERD damage
to the tissue lining | Green et al,
2003(11) |
| | | | | Askling et
al, 2002(12) |
| | | | | Souza,
2010(38) |
| 2. | Colorectal | High | Lower count of
Bifidobacterium in the jejunum | Green et al,
2003(11) |
| | | | | Lasa et al,
2018(42) |
| | | | | Golfetto et
al, 2014(43) |
| | | Low | Lower absorption of
fat | Pereyra et
al, 2013(45) |
| | | | | Lebwohl et
al, 2010(46) |
| | | | | Kabbani et
al, 2012(47) |
| | | | | Volta et al,
2014(48) |
| | | | | Delaunoit et
al, 2005(49) |
| 3. | Small intestinal
adenocarcinoma | High | Gliadin disrupts
the gut barrier and alters cell polarity, a major driver of
oncogenesis | Askling et
al, 2002(12) |
| | | | | Dunne et al,
2020(51) |
| | | | | Shin et al,
2006(52) |
| | | | | Lee and Vasioukhin,
2008(53) |
| 4. | Lymphoma | High | Less specific
pro-proliferative effects of chronic inflammation | Askling et
al, 2002(12) |
| | | | | Marušić et
al, 2011(57) |
| 5. | Primary liver cell
cancer | High | Chronic
inflammation A shift from normal in
Bifidobacterium/Enterobacteriaceae ratio | Askling et
al, 2002(12) |
| | | | | Rubio-Tapia and
Murray, 2008(61) |
| | | | | Fang et al,
2017(62) |
| 6. | Oropharyngeal | High | Largely
unknown | Askling et
al, 2002(12) |
| 7. | Ovarian | Low | Low exposure to
oestrogen in lifetime due to inflammation-induced hormonal
disbalance | Ludvigsson et
al, 2012(67) |
| 8. | Breast cancer | Low | Lower consumption
of milk products reduces exposure to insulin-like growth factors,
low exposure to the hormone oestrogen | Furnari et
al, 2013(66) |
| | | | | Ludvigsson et
al, 2012(67) |
| | | | | Ugalde-Morales
et al, 2017(68) |
| | | | | Olén et al,
2009(69) |
| 9. | Endometrial
cancer | Low | Early menopause in
women due to celiac disease | Santonicola et
al, 2011(74) |
5. Celiac disease and its association with
various types of cancer
CD and oesophageal cancer
Oesophageal cancer is the seventh most common cause
of cancer-related mortality among males, thus exhibiting a strong
male predominance attributed to environmental factors, such as
alcohol consumption, cigarette smoking, nutrition and socioeconomic
status (36). Apart from the
environmental factors, the risk of developing this type of cancer
can increase due to underlying disorders, such as gastroesophageal
reflux disease (GERD), CD, Barrett's oesophagus, achalasia and
obesity. Cancer generally develops in the inner layer of the
oesophageal wall and continues to spread to the outer layers.
According to the cancer statistics, the prevalence of oesophageal
cancer is more common in Iran, India, Northern China and South
Africa than in Western countries, such as the USA (37).
In GERD, the acid from the stomach rises to the
oesophagus and damages the oesophageal tissue, causing a scar in
the oesophagus. This constant insult and injury to the lower
oesophageal cell lining and tissues can ultimately increase the
proliferation of cells (38). A
change in cell shape from squamous to columnar following GERD
indicates the disruption of cell polarity, which marks the onset of
cancer (39).
Patients with CD have been observed to have a high
risk of developing oesophageal malignancies. It has been found that
in patients with untreated CD, the delayed emptying of the stomach
is quite common, and this may be an essential factor that can be
linked to gastroesophageal reflux (23). The abnormal concentrations of a
number of hormones related to the GIT have also been observed in
untreated patients with CD. This causes a disbalance in upper
gastrointestinal function controlled by neuroendocrine factors
(40). Constant acid reflux from
the stomach manifests Barrett's oesophagus. GFD has been shown as a
valuable approach to reduce GERD symptoms (41).
CD and colorectal cancer
Colorectal cancer is a cancer of the colon or
rectum. It is the third most common type of cancer in males and the
second most prevalent among females in the USA (42). The risk of developing colorectal
cancer increase with age, diet and lifestyle. Apart from age, a
family history also contributes to an increased risk of this type
of cancer. It begins with the loss of the adenomatous polyposis
coli (APC) gene present on chromosome 5q21 and the
subsequent activation of the KRAS oncogene and mutations in
the TP53 gene (42,43).
A previous study by Lasa et al (42) demonstrated that patients with CD
have an increased risk of developing colorectal cancer. Consistent
gluten exposure in individuals with CD may increase their risk of
developing colorectal neoplasia (42). Golfetto et al (43) compared the count of
Bifidobacterium in faecal matter and reported that patients
with CD had a lower Bifidobacterium count.
Bifidobacterium metabolites exhibit anticancer activity, as
previously observed using the SW742 colon cancer cell line
(44). This may be one of the
probable causes of the increased incidence of colon cancer among
patients with CD. Contrary to previous reports, other studies have
not found any direct link between CD and an increased risk of
colorectal neoplasia (45,46). It is crucial to note that these
studies all involved patients with CD on a GFD and were compared to
non-celiac, otherwise healthy controls (42,45,46).
The simple fact may explain this as a high-fat, low-fibre diet has
been associated with an increased risk of colorectal cancer, and
celiac-associated intestinal damage may aid to reduce that risk by
preventing the body from absorbing fat. Alternatively,
immunological changes in the small intestine may prevent colon
cancer from developing (46). Body
mass index (BMI) is also a crucial factor when assessing the risk
of developing colorectal cancer. Patients with CD are generally
found to have a low BMI compared to healthy individuals (47,48),
which acts as a protective factor when measuring the risk of CD
(48). In addition, the lack of an
increased risk of colorectal cancer in population research is due
to a genuine average risk of colorectal neoplasia, not to greater
colonoscopy and concomitant polypectomies in the celiac community
(46).
CD and small intestine adenocarcinoma
(SBA)
SBA, also known as small bowel adenocarcinoma, is a
rare form of neoplasm that accounts for <5% of all
gastrointestinal malignancies (15). This type of cancer can affect all
three parts of the small intestine, i.e., the duodenum, jejunum and
ileum (49). Often, SBA is
attributed as the ‘sibling’ of colorectal cancer due to
epidemiological and clinical similarities between both types of
cancers (49). This type of cancer
arises first from the glandular cells on the small intestine lining
and then spreads to deeper layers. Genes commonly mutated in this
type of cancer include TP53, KRAS, APC,
SMAD4, BRAF, SOX9, ATM, ARID2, ACVR2A, ACVR1B, BRCA2
and SMARCA4 (50).
The risk factors for SBA can range from the consumption of sugar,
red meat, alcohol, smoking and underlying diseases, such as Crohn's
disease and CD. The main trigger factor for SBA arises due to
inflammation in the small intestinal walls, which occurs following
gluten consumption. This leads to damage in the villi of the small
intestine. It has been reported that during the course of CD, γ-δ-
and T-cell expansion increases in the small intestinal epithelium,
which plays an active role in pathogenic inflammation (51).
Inflammation promotes the development of tumours.
Gliadin peptides trigger the excessive release of zonulin (the
protein that modulates tight intercellular junctions), leading to
the disruption of the gut barrier and the disassembly of tight
junctions (51). Tight junction
proteins play an essential role in establishing and maintaining the
apicobasal cell polarity (52),
leading to alterations in cell polarity, a major driver and
hallmark of oncogenesis (53).
Zona occludens 1 (ZO-1) expression has been shown to be
significantly reduced in patients with CD (54). ZO-1 is a tight junction protein
that, along with occludin, helps maintain the barrier function.
However, this downregulation has been shown to be reversed by
following a GFD (54). Thus,
persistent inflammation and alterations in cell morphology due to
severe insults to cells increases the risk of SBA.
CD and lymphoma
Lymphomas begin in the lymphatic system, where white
blood cells proliferate uncontrollably. Although the disease is
rare in children <5 years of age, it is the most commonly
diagnosed type of cancer in teens aged between 15 to 19 years. The
disease accounts for 12% of all cancer cases in this age group
(55).
This is a rare type of aggressive-cell lymphoma that
accounts for <5% of all GIT lymphomas, with an annual incidence
rate of 0.5-1 per million subjects in Western countries (13). The incidence and temporal trend
patterns differ by age, sex, race/ethnicity and geography, implying
that infectious agents, environmental variables and lifestyle
factors, in addition to the genetic status of the host, may play a
role in the development of lymphoma. Immune modulation and
persistent antigen activation are two critical pathogenetic
pathways (56).
Patients with CD have a high risk of developing
lymphoma. Patients with untreated CD often have a high risk of
developing enteropathy-associated T-cell lymphoma (EATL) (57). Based on appearance,
immunohistochemistry and genetic profile, it is divided into two
types. However, type I is more frequent and strongly linked to CD,
particularly when the condition becomes refractory to gluten
withdrawal. The molecular mechanisms that cause EATL in the
gluten-sensitive atrophic intestinal mucosa have been thoroughly
investigated. Classic EATL frequently exhibits chromosomal gains at
9q33-34, 7q, 5q34-35 and 1q21-23, and losses at 8p, 13q21 and
9p21(58). Cellier et al
(14) proposed that cryptic
enteropathy-related T-cell lymphoma represents a transitory stage
of gluten refractory disease with aberrant intraepithelial
T-lymphocyte clones. The adjacent small bowel usually shows villous
atrophy associated with CD (14).
The use of a GFD to treat CD effectively inhibits the development
of EATL. The mechanisms underlying the strong link between EATL and
CD are unknown; antigen-driven T-cell proliferation and less
specific pro-proliferative effects of chronic inflammation are both
potential candidates (57).
CD and primary liver cell cancer
Hepatocellular carcinoma is the most common form of
primary liver cell cancer due to liver disease. It is the fifth
most common type of cancer in males and seventh most common cancer
in females, and ranks second as regards cancer-related mortality
(59). The risk factors include
heavy alcohol consumption, hepatitis B and C infection, diabetes
mellitus and fatty liver disease (60). Celiac hepatitis is the most common
form of liver abnormality in patients with CD (61). Untreated CD can lead to a
disbalance between liver enzyme levels, ultimately increasing the
risk of liver cancer. The mechanisms through which patients with CD
develop liver cancer remain unknown. One proposition may be gut
microbiota alterations (62). CD
causes a decrease in the numbers of Bifidobacterium; as a
result, the Bifidobacterium/Enterobacteriaceae ratio
is altered, which then causes liver disease (62). Liver disease can be a threat that
can lead to cirrhosis of the liver and, ultimately, cancer and
gluten consumption by patients with CD can cause an inflammatory
response, leading to liver scarring. The scar tissues hinder the
flow of blood through that region of the liver, and eventually, the
scars lead to cirrhosis of the liver, leading to cancer onset.
Hence, untreated CD can increase the risk of primary liver cell
carcinoma (61).
CD and breast cancer
According to the WHO and the statistics released by
the International Agency for Research on Cancer (IARC), as of
December 2020, breast cancer is the most commonly diagnosed cancer
among females (8). It has
surpassed lung cancer, which used to have the highest incidence
worldwide. Breast cancer remains the most common form of cancer in
females in the USA, with 1 out of 8 women bearing the risk of
developing breast cancer at some point in their lives (63). In breast cancer, the epithelial
cells residing in the breast (preferably in the lobules) lead to
the formation of a tumour. The risk factors for breast cancer
include age, sex, lifestyle, food, sleep patterns, hormone status
(oestrogen and progesterone), and inherited genetic mutations from
family members. Breast cancer comprises four types, namely invasive
ductal carcinoma, invasive lobular carcinoma, Paget's disease and
inflammatory breast cancer. The genes associated with breast cancer
include BRCA1 and BRCA2. Other than these two genes,
BRCA3, located on chromosome 8p11-21, exhibits mutations
that give rise to sporadic disease. Inactivating mutations in
TP53 are also associated with breast cancer. The
inactivation of TP53 occurs not only in breast cancer, but
also in all cancer types, as this tumour suppressor gene is mainly
involved in the suppression of cancer cell growth (64). Other genetic mutations associated
with breast cancer include the PTEN, CDH1,
PALB2, CHEK2 and STK11 genes (65).
As demonstrated in the study by Askling et al
(12), patients with CD have a low
risk of developing breast cancer. Patients with CD often have
lactose intolerance, which occurs due to a deficiency in the
lactase enzyme. Lactase deficiency can lead to CD demonstrated by
the H2 lactose breath test, as previously demonstrated in a
retrospective study involving 54 subjects (66). Milk products contain insulin-like
growth factor 1 (IGF-1) (43),
which facilitates tumour growth through angiogenesis, low rates of
apoptosis (a process where the damaged cells destroy themselves and
macrophages eat away the debris), and a high proliferative
potential leading to a higher risk of breast cancer (43). Therefore, the possible reason for
the low risk of breast cancer in patients with CD is that they
consume fewer dairy products due to lactose intolerance.
Additionally, women with CD have a low nutritional
status due to malabsorption by villi, leading to weight loss. This
can be another factor for the reduced risk of breast cancer
(67). Ugalde-Morales et al
(68) demonstrated the association
between common shared single nucleotide polymorphisms between the
two diseases mapped onto genes enriched for immunoregulatory and
apoptotic processes behind the decreased risk of breast cancer in
celiac disease. Another study suggested that the reduced risk may
be attributed to the lower BMI in individuals with CD, as reported
in anorexia nervosa (69).
CD and oropharyngeal cancer
According to the American Cancer Society statistics,
oropharyngeal cancer, commonly known as head and neck cancer, is
the eighth most common type of cancer among males (70). The majority of oropharyngeal
cancers arise in the squamous. Risk factors include human papilloma
virus infection, smoking and alcohol consumption. In a previous
study on Swedish patients, it was found that the risk of developing
oropharyngeal cancer increased to a moderate amount in patients
with CD (12). Another study
reported several oral health issues, such as canker sores,
xerostomia (dry mouth), dental discoloration and enamel defects in
patients with CD (71). The study
by Askling et al (12)
employed a population cohort of 11,019 patients with CD. They
reported that patients with CD were at a higher risk of developing
both oropharyngeal and oesophageal cancers by 2.3- and 4.2-fold,
respectively (12). Thus, one
answer for the risk of oropharyngeal cancer in CD is oesophageal
cancer manifestation. The radiotherapy involved in treating cancer
(preferably oesophageal cancer in this case) damages the salivary
glands and thickens saliva, thus leading to dry mouth disease.
However, the exact reason for the increased risk remains unknown. A
two-fold relative risk of cancer was found due to an increased risk
of cancer of the mouth and pharynx. However, the risk was increased
in those taking reduced gluten, or a normal diet, with an excess of
cancers of the mouth, pharynx, and oesophagus (12). Holmes et al (72) reported a significant decrease in
the morbidity rate of patients with CD adhering to the GFD diet;
the results of their study suggest a protective role for a GFD
against malignancy in CD (72).
CD and endometrial cancer
Endometrial cancer is a type of cancer that forms in
the tissues of the endometrium (lining of the uterus).
Female-related cancer begins in the hollow, pear-shaped
baby-bearing organ, and the uterus is the fourth most common type
of cancer among females in the USA (73). Endometrial cancers are of two
types, i.e., type I, which exhibits a dependency on oestrogen, and
type II, which is oestrogen-independent. (73) Type I is most common, with an
occurrence rate of 85% and generally harbours mutations in KRAS,
PTEN and β-catenin (73). It also
exhibits microsatellite instability. Type II endometrial cancer
exhibits p53 mutation and HER-2 amplification (73). The risk factors for endometrial
cancer include age, tamoxifen consumption, oestrogen treatment,
obesity, menstrual factors and underlying disorders, such as
diabetes mellitus (73).
This type of has been found to have an inverse
association with CD. The risk for female hormone-related cancers is
generally reported to be low in patients with CD (67). One reason for this may be the low
exposure to oestrogen, which acts as a protective shield for these
types of cancer in women with CD (67). A previous study reported that
untreated CD can lead to early menopause in women, which eventually
leads to low oestrogen levels in the body as ovaries begin to lose
their ability to produce this hormone (74). Endometrial cancer generally occurs
in females >50 years of age, i.e., after menopause. The risk
increases if oestrogen pills are administered post-menopause
without maintaining a balance with progesterone (75). Hence, a burst in oestrogen hormone
levels following menopause may be the primary reason for developing
this type of cancer.
Thus, untreated CD clearly explains the negative
association with endometrial cancer. However, with a proper GFD,
the timing of menopause becomes normal compared to celiac-free
subjects (74).
CD and ovarian cancer
In ovarian cancer, ovarian cells divide
uncontrollably, leading to the formation of tumours. Ovarian cancer
is the seventh most common type of cancer among females. This
cancer has a high mortality rate (76). Mutations in the BRCA1 and
BRCA2 genes are responsible for this type of cancer. Apart
from these genes, mutations in other genes, such as CHEK2,
RAD51, BRIP1 and PIK3CA have also been observed. The
risk of developing ovarian cancer increases if an individual has a
family history of breast or ovarian cancer (77).
Women with CD have a lower risk of developing
ovarian cancer, as reported by a study carried out in Sweden, in
which 17,825 women with CD were diagnosed between the years 1969
and 2007(67). It has been
observed that patients with CD have a reduced risk of developing
female hormone-related cancer. A possible explanation for the
reduction in ovarian cancer is that women with CD may be less
exposed to oestrogen in their lifetime (67). Oestrogen displays a close
association with ovarian cancer along with endometrial and breast
cancer (67). The inflammation
that generally arises due to this disease can cause hormonal
disbalance. This condition later gives rise to issues regarding
pregnancy and menopause.
6. The gluten-free diet
A GFD implies avoiding any gluten sources containing
wheat, rye and barley, as well as their derivatives in any form
(3). Other foods that do not
contain gluten naturally, such as vegetables, fruits and
animal-derived food (fish, poultry and meats) are permitted in
their natural state. Naturally, gluten-free grains, such as rice,
corn and potatoes are widely used to substitute gluten-containing
grains.
Of note, even though grains naturally lack gluten,
they are considered suspicious. Oats are such a grain that has been
excluded from CD dietary advice for several years, as avenin (the
storage protein found in oats) is also toxic to patients with CD.
However, it has been demonstrated that the oat grain is safe for
patients with CD. In a previous study, Gatti et al (78) reported that gluten-uncontaminated
oats were safe.
7. Role of a gluten-free diet in the
prevention of cancer risk
Several studies have explored the effects of a GFD
on the healing of CD-related mucosal tissue damage. It has been
found that following a strict GFD causes complete mucosal healing
in a large number of patients with CD (79-82).
However, only a limited number of studies have explored the effects
of a GFD in reducing celiac-associated cancer types. In a critical
study conducted in 1989, Holmes et al (72) investigated the effects of GD
adherence in patients with CD related to cancers of the mouth,
pharynx and oesophagus. They found that patients with CD following
a GFD ≥5 five years had a reduced risk of developing cancer
compared to the general population. The study concluded that the
GFD plays a protective role; hence, a strict GFD must be followed
by patients with CD (72). Another
study found that the GFD was indeed helpful for preventing certain
aggressive forms of cancer (13).
Pereyra et al (45)
suggested that patients with CD with a poor GFD compliance had a
higher risk of colorectal adenomas. Even though the proportion of
such patients who did not adhere to a GFD was small, this finding
suggests that untreated CD patients may have a higher risk of
colorectal neoplasia (45). They
further investigated whether the lack of a GFD among patients with
CD could be a trigger for the development of colorectal lesions.
This theory was supported by evidence indicating an increased risk
of mortality among patients with CD. On the other hand, in
refractory CD, continuous gluten exposure causes histopathological
lesions (83). Gluten exposure
induces a toxic and immunological response in patients with CD
(84). Hence, it is possible that
a nutritional element plays a role in the development of neoplasms
in patients with CD, including colorectal neoplasia. It may also
emphasize the need of adhering to a GFD as a possible preventive
factor against the development of colon cancer (45). In a recent study, Um et al
investigated an association between whole-grain intake with lower
risk of colorectal cancer among older US men (84). The authors of that study found that
men who ate more whole grains had a decreased risk of colorectal
cancer, while women did not (85).
As per a recent report, there has been an increase in cancer risk
among individuals diagnosed with CD >40 year of age, and this
risk is predominantly prevalent within the first year of diagnosis
(17). Thus far, the majority of
studies investigating the risk of cancer in patients with CD have
been conducted before CD serologic testing, and a GFD was generally
available. Thus, the GFD may reduce cancer risk in CD (17). Silano et al (86) emphasized the early diagnosis of CD
and the importance of a GFD and its protection against the
development of malignancies in patients with CD. A GFD has been
demonstrated to reduce inflammatory markers, such as antibody
levels (87). Hence, it is
possible that a GFD minimizes the risk of cancer where inflammation
is a major trigger. The number of prospective studies investigating
the effects of a GFD on cancer in patients with CD is still limited
in the literature (72,88). The effects of a GFD in
preventing/reducing the risk of developing malignancies in patients
with CD is still under debate. As non-adherence and/or
non-responsiveness to a GFD can result in chronic inflammation of
the small bowel, it is tempting to speculate that a
gluten-containing diet in patients with CD may promote the
activation of immune/inflammatory signals, eventually leading to
the onset/progression of lymphomas and other cancer types (16).
8. Conclusions
A long-term failure to adherence to a GFD increases
the risk of developing different types of malignancies. It has been
found that a strict GFD reduces the risk of developing colon
cancer, oropharyngeal cancer and intestine adenocarcinoma in
patients with CD. Although a GFD minimizes the risk of certain
types of cancer, this fact has not yet been fully explored however.
Thus, there is a need for studies investigating the role of a GFD
in decreasing cancer risk in CD.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
NK was involved in the study design, analysis and
interpretation of the data to be included in the review (literature
search), as well as in the writing and preparation of the original
draft, in the drafting of the manuscript, and in the critical
revision of the manuscript for important intellectual content. AM
contributed to acquiring the data for inclusion in the review
(literature search), as well as in the writing and preparation of
the original draft, and in designing the figure. SS and VM
contributed to the acquisition of data for inclusion in the review
(literature search), and in the writing and preparation of the
original draft. YS was involved in the writing and reviewing of the
manuscript, as well as in the drafting the manuscript. AT
contributed to the critical revision of the manuscript. AKV
contributed to the conception and design of the study, and in the
critical revision of the manuscript. All authors have read and
approved the final manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Verma AK, Singh A, Gatti S, Lionetti E,
Galeazzi T, Monachesi C, Franceschini E, Ahuja V, Catassi C and
Makharia GK: Validation of a novel single-drop rapid human
leukocyte antigen-DQ2/-DQ8 typing method to identify subjects
susceptible to celiac disease. JGH Open. 2:311–316. 2018.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Megiorni F, Mora B, Bonamico M, Barbato M,
Nenna R, Maiella G, Lulli P and Mazzilli MC: HLA-DQ and risk
gradient for celiac disease. Hum Immunol. 70:55–59. 2009.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Ciacci C, Ciclitira P, Hadjivassiliou M,
Kaukinen K, Ludvigsson JF, McGough N, Sanders DS, Woodward J,
Leonard JN and Swift GL: The gluten-free diet and its current
application in coeliac disease and dermatitis herpetiformis. United
European Gastroenterol J. 3:121–135. 2015.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Parzanese I, Qehajaj D, Patrinicola F,
Aralica M, Chiriva-Internati M, Stifter S, Elli L and Grizzi F:
Celiac disease: From pathophysiology to treatment. World J
Gastrointest Pathophysiol. 8:27–38. 2017.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Catassi C, Fabiani E, Iacono G, D'Agate C,
Francavilla R, Biagi F, Volta U, Accomando S, Picarelli A, De Vitis
I, et al: A prospective, double-blind, placebo-controlled trial to
establish a safe gluten threshold for patients with celiac disease.
Am J Clin Nutr. 85:160–166. 2007.PubMed/NCBI View Article : Google Scholar
|
|
6
|
MacCulloch K and Rashid M: Factors
affecting adherence to a gluten-free diet in children with celiac
disease. Paediatr Child Health. 19:305–309. 2014.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Soldera J, Salgado K and Pêgas KL:
Refractory celiac disease type 2: How to diagnose and treat? Rev
Assoc Med Bras (1992). 67:168–172. 2021.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA A Cancer J Clin. 71:209–249.
2021.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Shurin MR: Cancer as an immune-mediated
disease. Immunotargets Ther. 1:1–6. 2012.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Martincorena I, Raine KM, Gerstung M,
Dawson KJ, Haase K, Van Loo P, Davies H, Stratton MR and Campbell
PJ: Universal patterns of selection in cancer and somatic tissues.
Cell. 171:1029–1041.e21. 2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Green PH, Fleischauer AT, Bhagat G, Goyal
R, Jabri B and Neugut AI: Risk of malignancy in patients with
celiac disease. Am J Med. 115:191–195. 2003.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Askling J, Linet M, Gridley G, Halstensen
TS, Ekström K and Ekbom A: Cancer incidence in a population-based
cohort of individuals hospitalized with celiac disease or
dermatitis herpetiformis. Gastroenterology. 123:1428–1435.
2002.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Catassi C, Bearzi I and Holmes GKT:
Association of celiac disease and intestinal lymphomas and other
cancers. Gastroenterology. 128 (4 Suppl 1):S79–S86. 2005.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Cellier C, Delabesse E, Helmer C, Patey N,
Matuchansky C, Jabri B, Macintyre E, Cerf-Bensussan N and Brousse
N: Refractory sprue, coeliac disease, and enteropathy-associated
T-cell lymphoma. Lancet. 356:203–208. 2000.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Barsouk A, Rawla P, Barsouk A and Thandra
KC: Epidemiology of cancers of the small intestine: Trends, risk
factors, and prevention. Med Sci (Basel). 7(46)2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Marafini I, Monteleone G and Stolfi C:
Association between celiac disease and cancer. Int J Mol Sci.
21(4155)2020.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Lebwohl B, Green PHR, Emilsson L, Mårild
K, Söderling J, Roelstraete B and Ludvigsson JF: Cancer risk in
47,241 individuals with celiac disease: A nationwide cohort study.
Clin Gastroenterol Hepatol. 20:e111–e131. 2022.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Sharma N, Bhatia S, Chunduri V, Kaur S,
Sharma S, Kapoor P, Kumari A and Garg M: Pathogenesis of celiac
disease and other gluten related disorders in wheat and strategies
for mitigating them. Front Nutr. 7(6)2020.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Balakireva AV and Zamyatnin AA: Properties
of gluten intolerance: Gluten structure, evolution, pathogenicity
and detoxification capabilities. Nutrients. 8(644)2016.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Meresse B, Malamut G and Cerf-Bensussan N:
Celiac disease: An immunological jigsaw. Immunity. 36:907–919.
2012.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Jabri B and Sollid LM: T cells in celiac
disease. J Immunol. 198:3005–3014. 2017.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Bhatia E: Celiac disease & type 1
diabetes: A double burden. Indian J Med Res. 149:5–7.
2019.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Lerner A and Matthias T: Rheumatoid
arthritis-celiac disease relationship: Joints get that gut feeling.
Autoimmun Rev. 14:1038–1047. 2015.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Kostopoulou E, Lagadinou M, Avgeri A and
Varvarigou A: Delayed presentation of seropositivity in
pre-existent coeliac disease in patients with Type 1 diabetes
mellitus: A possible co-occurrence? Eur Rev Med Pharmacol Sci.
25:7093–7096. 2021.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Casella G, Bordo BM, Schalling R,
Villanacci V, Salemme M, Di Bella C, Baldini V and Bassotti G:
Neurological disorders and celiac disease. Minerva Gastroenterol
Dietol. 62:197–206. 2016.PubMed/NCBI
|
|
26
|
Campagna G, Pesce M, Tatangelo R, Rizzuto
A, La Fratta I and Grilli A: The progression of coeliac disease:
Its neurological and psychiatric implications. Nutr Res Rev.
30:25–35. 2017.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Valitutti F, Cucchiara S and Fasano A:
Celiac disease and the microbiome. Nutrients.
11(2403)2019.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Pecora F, Persico F, Gismondi P, Fornaroli
F, Iuliano S, de'Angelis Gl and Esposito S: Gut microbiota in
celiac disease: Is there any role for probiotics? Front Immunol.
11(957)2020.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Akobeng AK, Singh P, Kumar M and Al Khodor
S: Role of the gut microbiota in the pathogenesis of coeliac
disease and potential therapeutic implications. Eur J Nutr.
59:3369–3390. 2020.PubMed/NCBI View Article : Google Scholar
|
|
30
|
Palma GD, Capilla A, Nova E, Castillejo G,
Varea V, Pozo T, Garrote JA, Polanco I, López A, Ribes-Koninckx C,
et al: Influence of milk-feeding type and genetic risk of
developing coeliac disease on intestinal microbiota of infants: The
PROFICEL study. PLoS One. 7(e30791)2012.PubMed/NCBI View Article : Google Scholar
|
|
31
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011.PubMed/NCBI View Article : Google Scholar
|
|
32
|
Maluf SW, Wilhelm Filho D, Parisotto EB,
Medeiros GDS, Pereira CHJ, Maraslis FT, Dornelles Schoeller CC,
Rosa JSD and Fröde TS: DNA damage, oxidative stress, and
inflammation in children with celiac disease. Genet Mol Biol.
43(e20180390)2020.PubMed/NCBI View Article : Google Scholar
|
|
33
|
Lebwohl B, Blaser MJ, Ludvigsson JF, Green
PH, Rundle A, Sonnenberg A and Genta RM: Decreased risk of Celiac
disease in patients with Helicobacter Pylori Colonization. Am J
Epidemiol. 178:1721–1730. 2013.PubMed/NCBI View Article : Google Scholar
|
|
34
|
Mayassi T, Ladell K, Gudjonson H, McLaren
JE, Shaw DG, Tran MT, Rokicka JJ, Lawrence I, Grenier JC, van Unen
V, et al: Chronic inflammation permanently reshapes tissue-resident
immunity in celiac disease. Cell. 176:967–981.e19. 2019.PubMed/NCBI View Article : Google Scholar
|
|
35
|
Grose RH, Cummins AG and Thompson FM:
Deficiency of invariant natural killer T cells in coeliac disease.
Gut. 56:790–795. 2007.PubMed/NCBI View Article : Google Scholar
|
|
36
|
Zhang Y: Epidemiology of esophageal
cancer. World J Gastroenterol. 19:5598–5606. 2013.PubMed/NCBI View Article : Google Scholar
|
|
37
|
Howlader N, Noone AM, Krapcho M, Miller D,
Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR (eds), et
al: SEER Cancer Statistics Review, 1975-2018. National Cancer
Institute. Bethesda, MD, 2021. https://seer.cancer.gov/csr/1975_2018/. Based on
November 2020 SEER data submission, posted to the SEER web site,
April 2021.
|
|
38
|
Souza RF: The role of acid and bile reflux
in oesophagitis and Barrett's metaplasia. Biochem Soc Trans.
38:348–352. 2010.PubMed/NCBI View Article : Google Scholar
|
|
39
|
Daum O, Kokošková B and Švajdler M:
Morphology of the gastroesophageal reflux disease. Cesk Patol.
52:15–22. 2016.PubMed/NCBI(In Czech).
|
|
40
|
Reimer C, Søndergaard B, Hilsted L and
Bytzer P: Proton-pump inhibitor therapy induces acid-related
symptoms in healthy volunteers after withdrawal of therapy.
Gastroenterology. 137:80–87, 87.e1. 2009.PubMed/NCBI View Article : Google Scholar
|
|
41
|
Usai P, Manca R, Cuomo R, Lai MA, Russo L
and Boi MF: Effect of gluten-free diet on preventing recurrence of
gastroesophageal reflux disease-related symptoms in adult celiac
patients with nonerosive reflux disease. J Gastroenterol Hepatol.
23:1368–1372. 2008.PubMed/NCBI View Article : Google Scholar
|
|
42
|
Lasa J, Rausch A, Bracho LF, Altamirano J,
Speisky D, de Dávila MTG, Iotti A and Zubiaurre I: Colorectal
adenoma risk is increased among recently diagnosed adult celiac
disease patients. Gastroenterol Res Pract.
2018(6150145)2018.PubMed/NCBI View Article : Google Scholar
|
|
43
|
Golfetto L, de Senna FD, Hermes J, Beserra
BT, França Fda S and Martinello F: Lower bifidobacteria counts in
adult patients with celiac disease on a gluten-free diet. Arq
Gastroenterol. 51:139–143. 2014.PubMed/NCBI View Article : Google Scholar
|
|
44
|
Bahmani S, Azarpira N and Moazamian E:
Anti-colon cancer activity of Bifidobacterium metabolites on colon
cancer cell line SW742. Turk J Gastroenterol. 30:835–842.
2019.PubMed/NCBI View Article : Google Scholar
|
|
45
|
Pereyra L, Gonzalez R, Mohaidle A, Fischer
C, Mella JM, Panigadi GN, Manazzoni D, Matoso MD, Lasa JS, Novillo
A, et al: Risk of colorectal neoplasia in patients with celiac
disease: A multicenter study. J Crohns Colitis. 7:e672–e677.
2013.PubMed/NCBI View Article : Google Scholar
|
|
46
|
Lebwohl B, Stavsky E, Neugut AI and Green
PH: Risk of colorectal adenomas in patients with coeliac disease:
Aliment Pharmacol. Ther. 32:1037–1043. 2010.PubMed/NCBI View Article : Google Scholar
|
|
47
|
Kabbani TA, Goldberg A, Kelly CP, Pallav
K, Tariq S, Peer A, Hansen J, Dennis M and Leffler DA: Body mass
index and the risk of obesity in coeliac disease treated with the
gluten-free diet. Aliment Pharmacol Ther. 35:723–729.
2012.PubMed/NCBI View Article : Google Scholar
|
|
48
|
Volta U, Vincentini O, Quintarelli F,
Felli C and Silano M: Collaborating Centres of the Italian Registry
of the Complications of Celiac Disease. Low risk of colon cancer in
patients with celiac disease. Scand J Gastroenterol. 49:564–568.
2014.PubMed/NCBI View Article : Google Scholar
|
|
49
|
Delaunoit T, Neczyporenko F, Limburg PJ
and Erlichman C: Pathogenesis and risk factors of small bowel
adenocarcinoma: A colorectal cancer sibling? Am J Gastroenterol.
100:703–710. 2005.PubMed/NCBI View Article : Google Scholar
|
|
50
|
Hänninen UA, Katainen R, Tanskanen T,
Plaketti RM, Laine R, Hamberg J, Ristimäki A, Pukkala E, Taipale M,
Mecklin JP, et al: Exome-wide somatic mutation characterization of
small bowel adenocarcinoma. PLoS Genet. 14(e1007200)2018.PubMed/NCBI View Article : Google Scholar
|
|
51
|
Dunne MR, Byrne G, Chirdo FG and Feighery
C: Coeliac Disease Pathogenesis: The uncertainties of a well-known
immune mediated disorder. Front Immunol. 11(1374)2020.PubMed/NCBI View Article : Google Scholar
|
|
52
|
Shin K, Fogg VC and Margolis B: Tight
junctions and cell polarity. Annu Rev Cell Dev Biol. 22:207–235.
2006.PubMed/NCBI View Article : Google Scholar
|
|
53
|
Lee M and Vasioukhin V: Cell polarity and
cancer-cell and tissue polarity as a non-canonical tumor
suppressor. J Cell Sci. 121 (Pt 8):1141–1150. 2008.PubMed/NCBI View Article : Google Scholar
|
|
54
|
Pizzuti D, Bortolami M, Mazzon E, Buda A,
Guariso G, D'Odorico A, Chiarelli S, D'Incà R, De Lazzari F and
Martines D: Transcriptional downregulation of tight junction
protein ZO-1 in active coeliac disease is reversed after a
gluten-free diet. Dig Liver Dis. 36:337–341. 2004.PubMed/NCBI View Article : Google Scholar
|
|
55
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2021. CA A Cancer J Clin. 71:7–33.
2021.PubMed/NCBI View Article : Google Scholar
|
|
56
|
Chiu BC and Hou N: Epidemiology and
etiology of non-hodgkin lymphoma. Cancer Treat Res. 165:1–25.
2015.PubMed/NCBI View Article : Google Scholar
|
|
57
|
Marušić M, Gulić S, Gašparov S, Bilić A,
Jurčić D, Vučković B, Stanić G, Luetić K, Dominković A and Sučić T:
Celiac disease and fulminant T lymphoma detected too late in a
35-year-old female patient: Case report. Bosn J Basic Med Sci.
11:190–193. 2011.PubMed/NCBI View Article : Google Scholar
|
|
58
|
Zettl A, Lee SS, Rüdiger T, Starostik P,
Marino M, Kirchner T, Ott M, Müller-Hermelink HK and Ott G:
Epstein-Barr virus-associated B-cell lymphoproliferative disorders
in angioimmunoblastic T-cell lymphoma and peripheral T-cell
lymphoma, unspecified. Am J Clin Pathol. 117:368–379.
2002.PubMed/NCBI View Article : Google Scholar
|
|
59
|
Mittal S and El-Serag HB: Epidemiology of
hepatocellular carcinoma: Consider the population. J Clin
Gastroenterol. 47 (Suppl):S2–S6. 2013.PubMed/NCBI View Article : Google Scholar
|
|
60
|
Janevska D, Chaloska-Ivanova V and
Janevski V: Hepatocellular carcinoma: Risk factors, diagnosis and
treatment. Open Access Maced J Med Sci. 3:732–736. 2015.PubMed/NCBI View Article : Google Scholar
|
|
61
|
Rubio-Tapia A and Murray JA: Liver
involvement in celiac disease. Minerva Med. 99:595–604.
2008.PubMed/NCBI
|
|
62
|
Fang D, Shi D, Lv L, Gu S, Wu W, Chen Y,
Guo J, Li A, Hu X, Guo F, et al: Bifidobacterium pseudocatenulatum
LI09 and Bifidobacterium catenulatum LI10 attenuate
D-galactosamine-induced liver injury by modifying the gut
microbiota. Sci Rep. 7(8770)2017.PubMed/NCBI View Article : Google Scholar
|
|
63
|
Feuer EJ, Wun LM, Boring CC, Flanders WD,
Timmel MJ and Tong T: The lifetime risk of developing breast
cancer. J Natl Cancer Inst. 85:892–897. 1993.PubMed/NCBI View Article : Google Scholar
|
|
64
|
de Jong MM, Nolte IM, te Meerman GJ, van
der Graaf WT, Oosterwijk JC, Kleibeuker JH, Schaapveld M and de
Vries EG: Genes other than BRCA1 and BRCA2 involved in breast
cancer susceptibility. J Med Genet. 39:225–242. 2002.PubMed/NCBI View Article : Google Scholar
|
|
65
|
Wood ME, McKinnon W and Garber J: Risk for
breast cancer and management of unaffected individuals with
non-BRCA hereditary breast cancer. Breast J. 26:1528–1534.
2020.PubMed/NCBI View Article : Google Scholar
|
|
66
|
Furnari M, Bonfanti D, Parodi A, Franzè J,
Savarino E, Bruzzone L, Moscatelli A, Di Mario F, Dulbecco P and
Savarino V: A comparison between lactose breath test and quick test
on duodenal biopsies for diagnosing lactase deficiency in patients
with self-reported lactose intolerance. J Clin Gastroenterol.
47:148–152. 2013.PubMed/NCBI View Article : Google Scholar
|
|
67
|
Ludvigsson JF, West J, Ekbom A and
Stephansson O: Reduced risk of breast, endometrial and ovarian
cancer in women with celiac disease. Int J Cancer. 131:E244–E250.
2012.PubMed/NCBI View Article : Google Scholar
|
|
68
|
Ugalde-Morales E, Li J, Humphreys K,
Ludvigsson JF, Yang H, Hall P and Czene K: Common shared genetic
variation behind decreased risk of breast cancer in celiac disease.
Sci Rep. 7(5942)2017.PubMed/NCBI View Article : Google Scholar
|
|
69
|
Olén O, Montgomery SM, Marcus C, Ekbom A
and Ludvigsson JF: Coeliac disease and body mass index: A study of
two Swedish general population-based registers. Scand J
Gastroenterol. 44:1198–1206. 2009.PubMed/NCBI View Article : Google Scholar
|
|
70
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2013. CA Cancer J Clin. 63:11–30. 2013.PubMed/NCBI View Article : Google Scholar
|
|
71
|
de Carvalho FK, de Queiroz AM, Bezerra da
Silva RA, Sawamura R, Bachmann L, Bezerra da Silva LA and
Nelson-Filho P: Oral aspects in celiac disease children: Clinical
and dental enamel chemical evaluation. Oral Surg Oral Med Oral
Pathol Oral Radiol. 119:636–643. 2015.PubMed/NCBI View Article : Google Scholar
|
|
72
|
Holmes GK, Prior P, Lane MR, Pope D and
Allan RN: Malignancy in coeliac disease-effect of a gluten free
diet. Gut. 30:333–338. 1989.PubMed/NCBI View Article : Google Scholar
|
|
73
|
Lucas WE and Yen SS: A study of endocrine
and metabolic variables in postmenopausal women with endometrial
carcinoma. Am J Obstet Gynecol. 134:180–186. 1979.PubMed/NCBI
|
|
74
|
Santonicola A, Iovino P, Cappello C,
Capone P, Andreozzi P and Ciacci C: From menarche to menopause: The
fertile life span of celiac women. Menopause. 18:1125–1130.
2011.PubMed/NCBI View Article : Google Scholar
|
|
75
|
Bharatnur S, Kustagi P and Krishnamohan D:
Endometrial carcinoma in a young woman: ‘30 is not immune.’. J
Obstet Gynecol India. 61:686–688. 2011.PubMed/NCBI View Article : Google Scholar
|
|
76
|
Momenimovahed Z, Tiznobaik A, Taheri S and
Salehiniya H: Ovarian cancer in the world: Epidemiology and risk
factors. Int J Womens Health. 11:287–299. 2019.PubMed/NCBI View Article : Google Scholar
|
|
77
|
Toss A, Tomasello C, Razzaboni E, Contu G,
Grandi G, Cagnacci A, Schilder RJ and Cortesi L: Hereditary ovarian
cancer: Not only BRCA 1 and 2 genes. Biomed Res Int.
2015(341723)2015.PubMed/NCBI View Article : Google Scholar
|
|
78
|
Gatti S, Caporelli N, Galeazzi T,
Francavilla R, Barbato M, Roggero P, Malamisura B, Iacono G,
Budelli A, Gesuita R, et al: Oats in the diet of children with
celiac disease: Preliminary results of a double-blind, randomized,
placebo-controlled multicenter Italian study. Nutrients.
5:4653–4664. 2013.PubMed/NCBI View Article : Google Scholar
|
|
79
|
Rubio-Tapia A, Rahim MW, See JA, Lahr BD,
Wu TT and Murray JA: Mucosal recovery and mortality in adults with
celiac disease after treatment with a gluten-free diet. Am J
Gastroenterol. 105:1412–1420. 2010.PubMed/NCBI View Article : Google Scholar
|
|
80
|
Wahab PJ, Meijer JW and Mulder CJ:
Histologic follow-up of people with celiac disease on a gluten-free
diet: Slow and incomplete recovery. Am J Clin Pathol. 118:459–463.
2002.PubMed/NCBI View Article : Google Scholar
|
|
81
|
Collin P, Mäki M and Kaukinen K: Complete
small intestinal mucosal recovery is obtainable in the treatment of
celiac disease. Gastrointest Endosc. 59:158–159; author reply
159-60. 2004.PubMed/NCBI View Article : Google Scholar
|
|
82
|
Szakács Z, Mátrai P, Hegyi P, Szabó I,
Vincze Á, Balaskó M, Mosdósi B, Sarlós P, Simon M, Márta K, et al:
Younger age at diagnosis predisposes to mucosal recovery in celiac
disease on a gluten-free diet: A meta-analysis. PLoS One.
12(e0187526)2017.PubMed/NCBI View Article : Google Scholar
|
|
83
|
Ciccocioppo R, Di Sabatino A and Corazza
GR: The immune recognition of gluten in coeliac disease. Clin Exp
Immunol. 140:408–416. 2005.PubMed/NCBI View Article : Google Scholar
|
|
84
|
Silano M, Vincentini O and De Vincenzi M:
Toxic, immunostimulatory and antagonist gluten peptides in celiac
disease. Curr Med Chem. 16:1489–1498. 2009.PubMed/NCBI View Article : Google Scholar
|
|
85
|
Um CY, Campbell PT, Carter B, Wang Y,
Gapstur SM and McCullough ML: Association between grains, gluten
and the risk of colorectal cancer in the cancer prevention study-II
nutrition cohort. Eur J Nutr. 59:1739–1749. 2020.PubMed/NCBI View Article : Google Scholar
|
|
86
|
Silano M, Volta U, Mecchia AM, Dessì M, Di
Benedetto R and De Vincenzi M: Collaborating centers of the Italian
registry of the complications of coeliac disease. Delayed diagnosis
of coeliac disease increases cancer risk. BMC Gastroenterol.
7(8)2007.PubMed/NCBI View Article : Google Scholar
|
|
87
|
Midhagen G, Aberg AK, Olcén P, Jarnerot G,
Valdimarsson T, Dahlbom T, Hansson T and Ström M: Antibody levels
in adult patients with coeliac disease during gluten-free diet: A
rapid initial decrease of clinical importance. J Intern Med.
256:519–524. 2004.PubMed/NCBI View Article : Google Scholar
|
|
88
|
Elfström P, Granath F, Ye W and Ludvigsson
JF: Low risk of gastrointestinal cancer among patients with celiac
disease, inflammation, or latent celiac disease. Clin Gastroenterol
Hepatol. 10:30–36. 2012.PubMed/NCBI View Article : Google Scholar
|