Introduction
Hyposalivation is affected by multiple factors and
usually follows head and neck cancer therapy. Head and neck cancer
is the fifth most common type of cancer, and represents
approximately 6% of all cases and accounts for an estimated 650,000
new cancer diagnoses and 350,000 cancer-related deaths worldwide
annually (1). Radiotherapy plays
an important role in conventional therapy, either independently or
combined with surgery, which results in a 5-year survival rate of
approximately 50% for non-metastatic and locally advanced disease
(2).
However, the salivary glands, which are frequently
included in the radiation field, are severely damage by this
approach. A large number of affected patients suffer from
xerostomia, dysphagia, dental caries, fungal infection and
malnutrition that consequently and severely compromise their
quality of life. The irreversible salivary gland dysfunction has
been attributed to a noticeable lose of acinar cells and the
sterilization of primitive glandular stem cells (3). Artificial saliva substitutes and
sialogogues represent the main clinical strategies used to relieve
oral dryness; however, tehse strategies require frequent
administration and are unpredictable in their efficacy (2,4).
Therefore, studies have sought to regenerate irradiation-injured
glands. Stem cell-based therapy is considered as a feasible
approach to restore radiation-damaged salivary glands. Bone
marrow-derived cells (BMDCs) may also hold promise for repairing
the irradiation-damaged salivary gland (5,6).
Nevertheless, there are unavoidable clinical issues associated with
transplanting BMDCs, due in part to painful procurement, low yield
rates and relatively low proliferation rates. Another source
suggested as a candidate for the treatment of irradiation-induced
hyposalivation includes cells derived from salivary glands. The
function of irradiated mouse salivary glands can be rescued by an
intra-glandular injection of primitive salivary gland stem cells
(7). However, the self-renewal
capacity of salivary gland stem cells is restricted in
vitro, and as most patients treated for head and neck cancer
are elderly, obtaining a sufficient amount of primitive salivary
gland stem cells for clinical use is challenging.
Human adipose tissue-derived stem cells (hADSCs) are
pluripotent stem cells obtained from human adipose tissue, and
similar to BMDCs, they have the multipotential to differentiate
toward osteogenic, adipogenic, myogenic and chondrogenic lineages
(8). Moreover, hADSCs can be
easily obtained from human adipose tissue or lipoaspirates, which
cause little discomfort to the donor and have gained significant
attention as a source of cell-based therapy. hADSCs have been
investigated for the possible treatment of tissue defects and organ
dysfunction in diabetes, pancreatitis, cardiac and neurological
diseases (9–11). Furthermore, in a previous study,
the potential toxicity and tumorigenicity of hADSCs was
investigated in animals and humans and the hADSCs were found to be
both non-toxic and non-tumorigenic (12). Based on the above study, we
speculated that hADSC transplantation may be a promising strategy
for stem cell-based treatment to alleviate xerostomia. This study
aimed to determine whether hADSCs possess the ability to restore
radiation-induced salivary gland dysfunction by local engraftment
in a Sprague-Dawley (SD) rat model of irradiation-induced
hyposalivation. The data presented in this study provide important
new information for the potential application of hADSCs in the
treatment of salivary gland dysfunction.
Materials and methods
hADSC ZsGreen labeling, flow cytometry
and differentiation
The cells were seeded into T75 flasks and grown to
20% confluence. The medium was changed to Dulbecco’s modified
Eagle’s medium (DMEM) with F12 (Gibco, Grand Island, NY, USA) that
was supplemented with 10% FBS and the cells were incubated for 4 h.
The purified lentiviral vector, ZsGreen, was added to the medium at
a multiplicity of infection (MOI) of 20. The medium was changed to
mesenchymal stem cell medium (MSCM; BioWit Technologies, Shenzhen,
China) 8 h after infection. ZsGreen expression was examined by
fluorescence microscopy 48 h after infection. The ratio of
ZsGreen-positive cells in the infected hADSCs was determined using
the captured images. Flow cytometry, as well as the adipogenic and
chondrogenic differentiation of ADSCs were carried out as
previously described (13). The
cells were dissociated using 0.25% trypsin-EDTA and washed twice
with PBS. The cells were then incubated with anti-human CD36
(eBioscience, Inc., San Diego, CA, USA), anti-human CD44
(eBioscience, Inc.) and corresponding isotype control antibody at
4°C for 30 min. Following incubation, PBS with 0.5% bovine serum
albumin (BSA) was utilized to wash the cells 3 times. Flow
cytometric analysis was performed using a FACSCalibur flow
cytometer (FACSAria III; BD Biosciences, Franklin Lakes, NJ, USA),
and the data were analyzed using FlowJo software (TreeStar Inc.,
Ashland, OR, USA). When the confluence of the cells reached 80%,
the differentiation experiments were performed. For adipogenic
differentiation, the medium was changed to adipogenic
differentiation medium (DMEM/F12 supplemented with 10% FBS, 1 μM
dexamethasone, 0.5 mM isobutyl-methylxanthine and 60 μM
indomethacin). Adipogenic differentiation was examined by Oil Red O
staining 14 days after induction. To induce chondrogenic
differentiation, the cells grown in DMEM medium containing 500
ng/ml BMP-6, 10 ng/ml TGF-β3, 0.1 μM dexamethasone, 0.17 mM
ascorbate-2 phosphate, 50 mg/ml ITS+ premix (BD Biosciences: 6.25
μg/ml insulin, 6.25 μg/ml transferrin, 6.25 ng/ml selenous acid,
1.25 mg/ml bovine serum albumin and 5.35 mg/ml linoleic acid).
Chondrogenic differentiation was examined by Alcian blue staining
21 days after induction.
Animals
Twelve-week-old male SD rats were purchased from
Sino-British SIPPR/BK Laboratory Animal Co., Ltd. (Shanghai, China)
and were used for the experiments. The rats were kept in a specific
pathogen-free, micro-isolated environment at the Institute of
Laboratory Animals, Tongji University, Shanghai, China, and allowed
access to water and chow ad libitum. The rats were divided
randomly into 3 groups as follows: group 1 (normal, n=30), group 2
(18 Gy irradiation, n=30), and group 3 (18 Gy + hADSCs, n=30). The
Animal Research Committee of Tongji University approved the study
and all the procedures that involved rats.
Irradiation of the salivary gland
Prior to irradiation, all the rats were weighed and
anesthetized using sodium pentobarbital (4.5 mg/100 g body weight).
Subsequently, the rats in groups 2 and 3 were fixed on a special
apparatus, with the head and neck exposed and other parts of the
body protected. Single-dose irradiation at 18 Gy was administered
using a 6-MV X-ray linear accelerator (2100C/D; Varian Medical
Systems, Inc., Palo Alto, CA, USA) at a dose rate of 300 cGy/min at
a focus to skin distance of 100 cm. Group 1 rats did not receive
any irradiation.
Transplantation of hADSCs
Immediately following irradiation, 1x106
hADSCs in 0.1 ml PBS were adoptively transferred by subcutaneous
injection into the submandibular glands of the rats in group 3
under anesthesia. Additionally, the same volume of PBS was injected
into the glands of the group 2 control rats. Group 1 rats received
anesthesia but no treatment or PBS.
Saliva collection
One PE-10 tube (outer diameter, 1.00 mm; inner
diameter, 0.65 mm) was inserted into the duct opening of the
submandibular gland of the rats after receiving anesthesia.
Salivary output was collected following stimulation with
subcutaneous injections of pilocarpine (0.06 mg/100 g body weight)
and placed in pre-weighed 0.5 ml microcentrifuge tubes. Saliva was
collected for a period of 10 min, and the volume was estimated by
weight, which assumed a specific gravity of 1.0 g/cm. The salivary
flow rate (SFR) was assessed at 8, 16 and 24 weeks
post-irradiation.
Histological and morphological
examination
At 24 weeks post-irradiation, the submandibular
glands were harvested and washed for 30 sec in PBS and fixed with
4% paraformaldehyde (PFA) at 4°C overnight and embedded in
paraffin. The paraffin-embedded glands were cut into 5-μm-thick
sections and subjected to hematoxylin and eosin (H&E) or
periodic acid-Schiff (PAS) staining. TdT-mediated dUTP nick
end-labeling (TUNEL) staining (In Situ Cell Death Detection kit;
Roche Diagnostic Corp., Indianapolis, IN, USA) was performed as
previously described (14). The
sections were ice-bathed in 0.1% Triton X-100 for permeation for 5
min and washed twice with PBS for 5 min. The sections were then
incubated with a TUNEL reaction mixture for 60 min at 37°C in the
dark. After the reaction, the sections were washed in PBS and
stained with hematoxylin. The sections were then mounted with
neutral gum before being examined under a light microscopy.
Paraffin sections were stained by an immunohistochemical method
using the blood vessel staining kit (Chemicon International, Inc.,
Billerica, MA, USA) following a previously published protocol
(6). The sections were
deparaffinized, rehydrated and rinsed with 10 mM sodium citrate (pH
6.0) solution 3 times in a 600-W microwave and cooled to room
temperature. After blocking overnight at 4°C, the sections were
incubated in 1:200 diluted rabbit anti-vWF polyclonal antibody at
room temperature. After secondary antibody incubation and HRP
reaction, the sections were examined under a light microscope. The
percentage of surface occupied by blood vessels was counted under
x400 magnification using 100 squares of 0.25 mm2 each.
Five squares were scored from each gland, and subsequently the data
were assessed using NIH ImageJ software (NIH, Bethesda,
MD,USA).
Quantitative reverse transcription PCR
(RT-qPCR
Total RNA was extracted from the fresh enucleated
salivary glands using TRIzol reagent (Invitrogen Life Technologies,
Carlsbad, CA, USA), and cDNA was synthesized using the PrimeScript™
RT reagent kit (Takara Bio, Inc., Shiga, Japan). The relative
expression levels of vascular endothelial growth factor (VEGF),
hepatocyte growth factor (HGF), cyclooxygenase-2 (COX-2) and matrix
metalloproteinase-2 (MMP-2) were determined using SYBR Premix Ex
Taq (Takara Bio, Inc.) and an Applied Biosystems 7900HT device
(Life Technologies, Inc., Grand Island, NY, USA). The primer
sequences are presented in Table
I. The average threshold cycles were determined from triplicate
PCR cycle assays, and the relative expression levels were
normalized to the endogenous control GAPDH.
 | Table ISpecific gene primers used for
RT-qPCR. |
Table I
Specific gene primers used for
RT-qPCR.
| Gene | Sense | Antisense | Annealing temperature
(°C) | Product size
(bp) |
|---|
| VEGF |
5′-CAAACCTCACCAAAGCCAGC-3′ |
5′-ACGCGAGTCTGTGTTTTTGC-3′ | 59.97 | 187 |
| HGF |
5′-ACCCTGGTGTTTCACAAGCA-3′ |
5′-GCAAGAATTTGTGCCGGTGT-3′ | 59.97 | 182 |
| COX-2 |
5′-GTGGAAAAGCCTCGTCCAGA-3′ |
5′-TCCTCCGAAGGTGCTAGGTT-3′ | 60.25 | 132 |
| MMP-2 |
5′-CCCCATGTGTCTTCCCCTTC-3′ |
5′-TGGGCTGCCACAAGGAATAG-3′ | 60.03 | 169 |
| GAPDH |
5′-AATGCATCCTGCACCACCAA-3′ |
5′-GATGGCATGGACTGTGGTCA-3′ | 60.04 | 99 |
Immunohistochemical analysis
The freshly isolated glands were fixed in 4% PFA,
embedded in optimal cutting temperature medium and sectioned at a
thickness of 8 μm. The cryostat sections were air-dried at room
temperature, post-fixed in 1% PFA and blocked in blocking buffer
consisting of 5% normal goat serum (Gibco), 0.1% Tween-20, 3% BSA
in PBS for 1 h at room temperature. The blocked sections were
incubated with antibodies (diluted in blocking buffer) targeted
against the following proteins overnight at 4°C: cytokeratin 7
(CK7, 1:250; Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA),
cytokeratin 14 (CK14, 1:50; R&D Systems, Minneapolis, MN, USA),
Na+-K+-Cl− co-transporter type 1
(NKCC1, 1:250; Abcam, Cambridge, MA, USA) and α-smooth muscle actin
(α-SMA, 1:50; R&D Systems). The slides were then washed in PBS
prior to incubation with secondary antibodies that were conjugated
to Cy-3. The slides were then washed in PBS and counterstained with
4′,6-diamidino-2-phenylindole (DAPI), and then mounted using 50%
glycerol-PBS before being examined under a fluorescence microscope
(IX71; Olympus Corp., Tokyo, Japan)..
Statistical analysis
All data are expressed as the means ± SD. To
determine statistical significance, one-way factorial analysis of
variance (ANOVA) and Student-Newman-Keuls (SNK) analysis were
conducted using SPSS version 17.0 software. A value of p<0.05
was considered to indicate a stastistically signficant
difference.
Results
Characterization of hADSCs
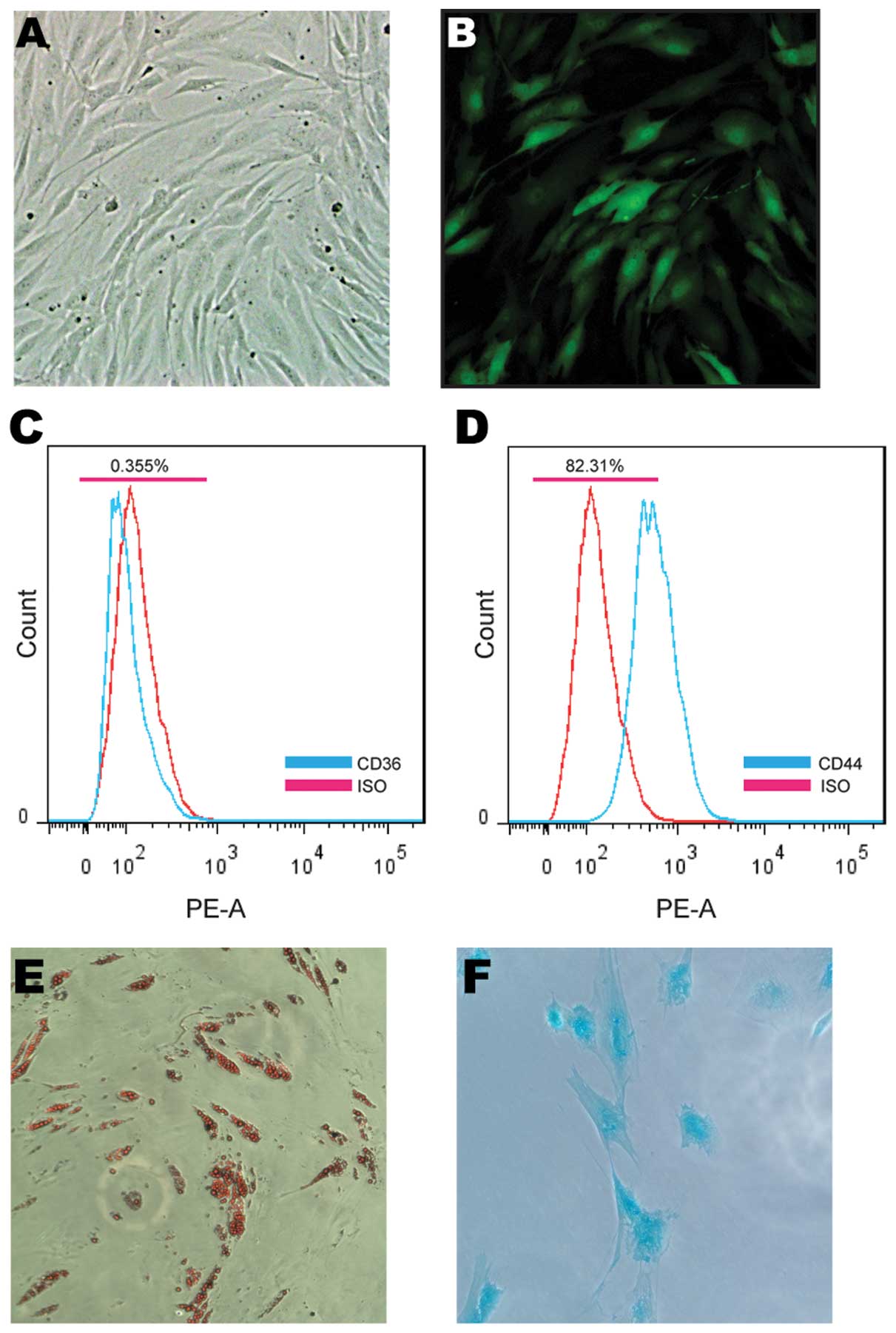
The morphology of the hADSCs [passage 3 (P3)] was
fibroblast-like and the hADSCs were effectively infected with the
lentivirus expressing ZsGreen (Fig.
1A and B). Flow cytometry was performed for the hADSC cell
lineage classification prior to transplantation (Fig. 1C and D). Chondrogenic and
adipogenic differentiation was also used to verify the
multipotential differentiation capacity of the hADSCs used in this
study (Fig. 1E and F).
Functional improvement of hyposalivation
by SFR detection
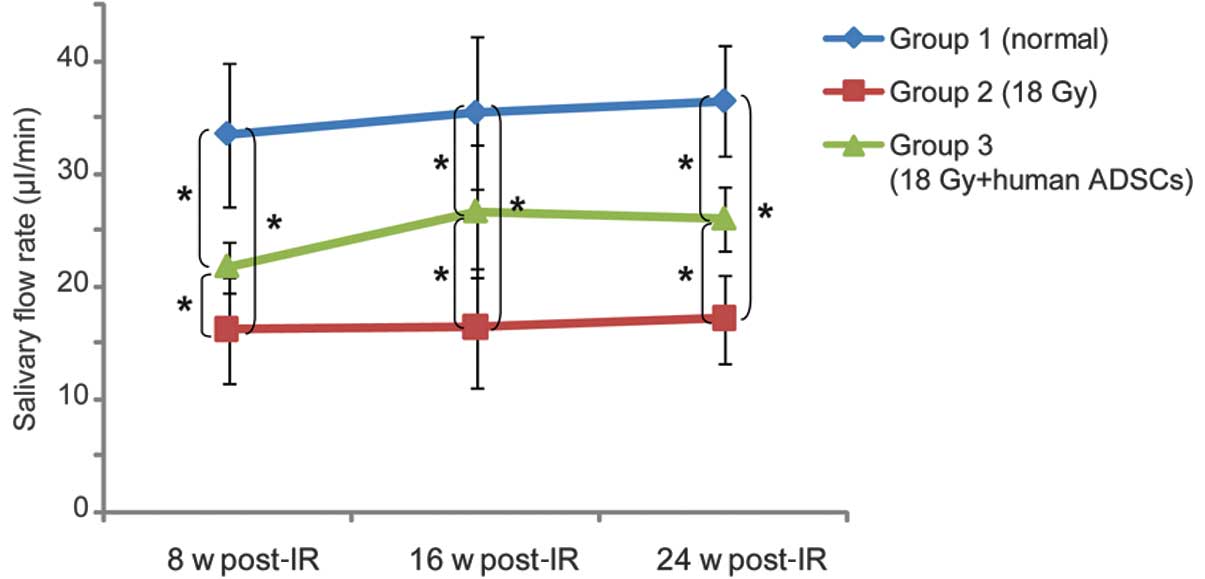
To assay the functional improvement in
radiation-induced hyposalivation, the SFR was measured at 8, 16 and
24 weeks post-irradiation. The SFR of the rats in group 2 sharply
decreased by 48.27% of the SFR of the rats in group 1 at 8 weeks
after radiography. Group 2 rats also showed persistent
hyposalivation throughout the experiment, and maintained only
approximately 50% of the SFR of the rats in group 1 at 24 weeks
(p<0.05). At 8 weeks post irradiation, a decrease in SFR was
also observed in the rats in group 3; however, this decrease was
not as significant as that of the one of the rats in group 2 at 8
weeks after irradiation (p<0.05). In addition, the output for
group 3 was 1.51-fold higher compared to that for group 2, and the
SFR recovered to 71.45% of the SFR of the rats in group 1 at 24
weeks (p<0.05, Fig. 2).
Injury tissue improvement and blood
vessel regeneration following hADSC transplantation
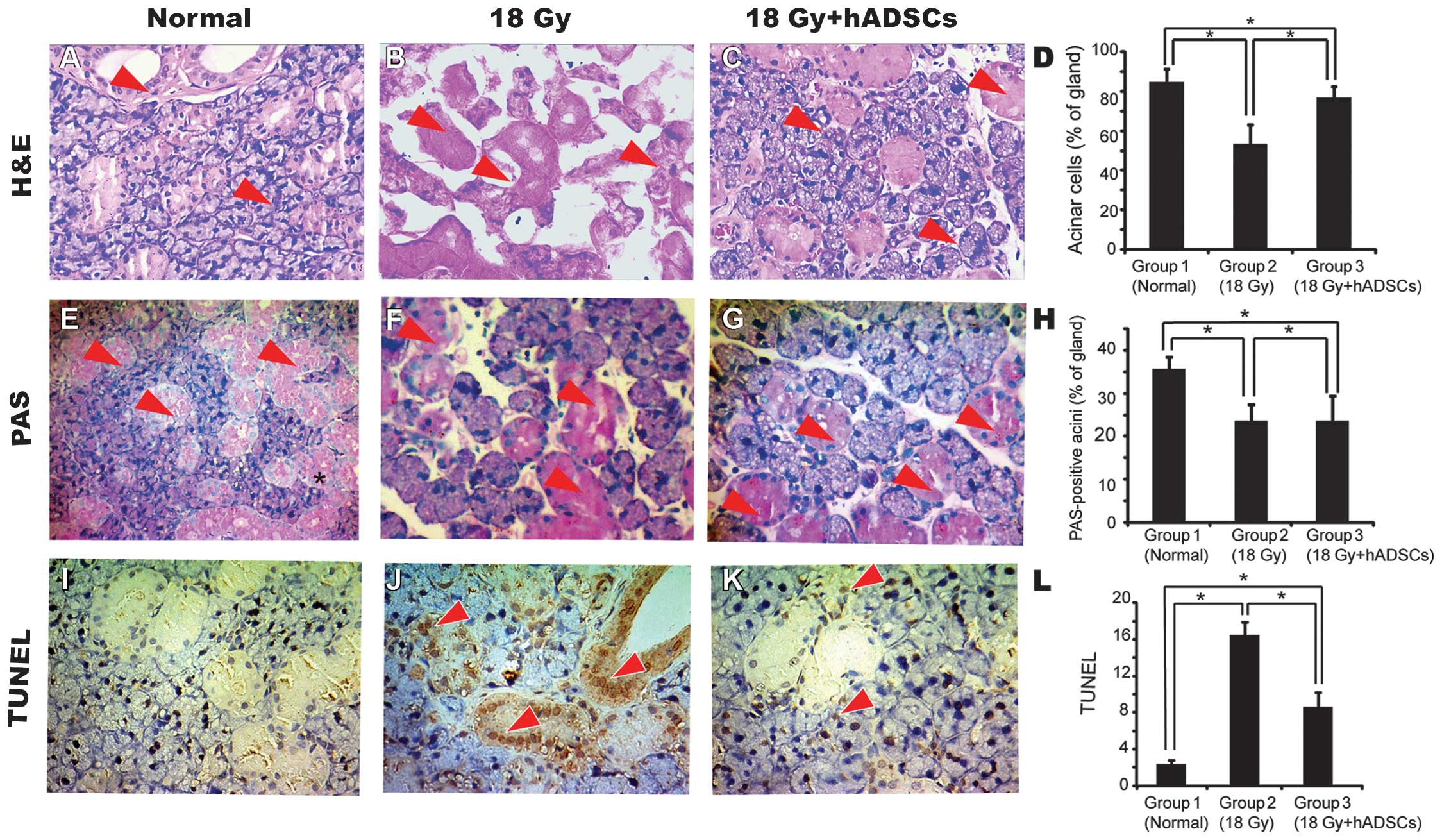
Pronounced acinar loss occurred in the rats in group
2 by 24 weeks post-irradiation as compared to the rats in group 1.
Extensive cellular and interstitial edema, cellular necrosis and
blood vessel congestion were observed in the rats in group 2.
Moreover, edema, blood vessel congestion, coagulative necrosis and
fibrosis were observed in the irradiated glands. By contrast, the
hADSC-treated salivary glands had a greater number of acinar cells
that displayed a normal morphology. In addition, swelling of the
parenchymal and mesenchymal cells, congestion and duct dilation
were observed in the rats in group 3. No inflammatory cells were
detected in group 3 by H&E staining (Fig. 3A–C). Additionally, PAS staining
revealed a greater number of PAS-positive acini in group 3 compared
to group 2 (p<0.05, Fig.
3E–G). An increased number of apoptotic cells was observed in
group 2 based on the observations derived from TUNEL assay, which
involved acinar and duct cells, while a sporadic pattern of
apoptotic cells was observed in group 3 (p<0.05, Fig. 3I–K).
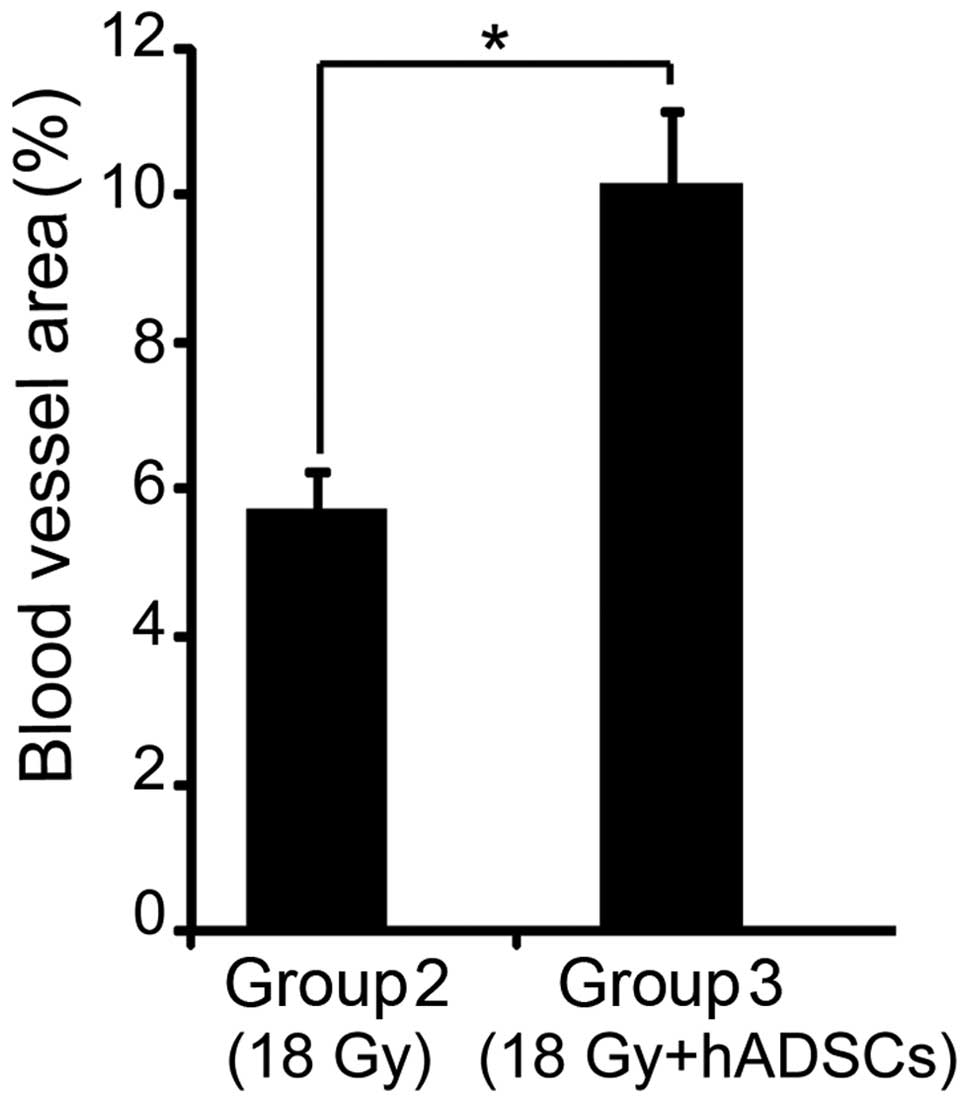
The frequency of the surface area occupied by the
blood vessels in each gland was calculated by blood vessel
staining. The area percentage in the hADSC-treated glands was
1.59-fold higher than that of the non-treated glands (p<0.05,
Fig. 4).
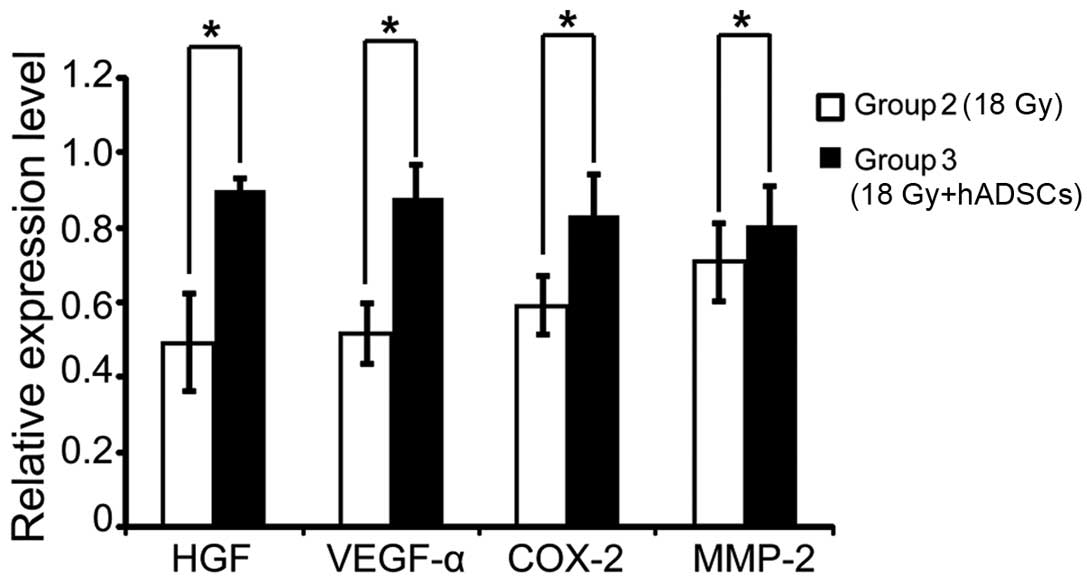
Paracrine effect of hADSCs
hADSCs secrete multiple cytokines and growth factors
that may contribute to the functional reconstruction of injured
organs (15). At 24 weeks
following hADSC engraftment, total RNA was extracted from the
freshly enucleated salivary glands, and RT-qPCR indicated that the
mRNA levels of VEGF, HGF and COX-2 increased significantly in the
rats in group 3 as compared to the rats in group 2. Moreover, MMP-2
expression showed no significant increment in expression (Fig. 5).
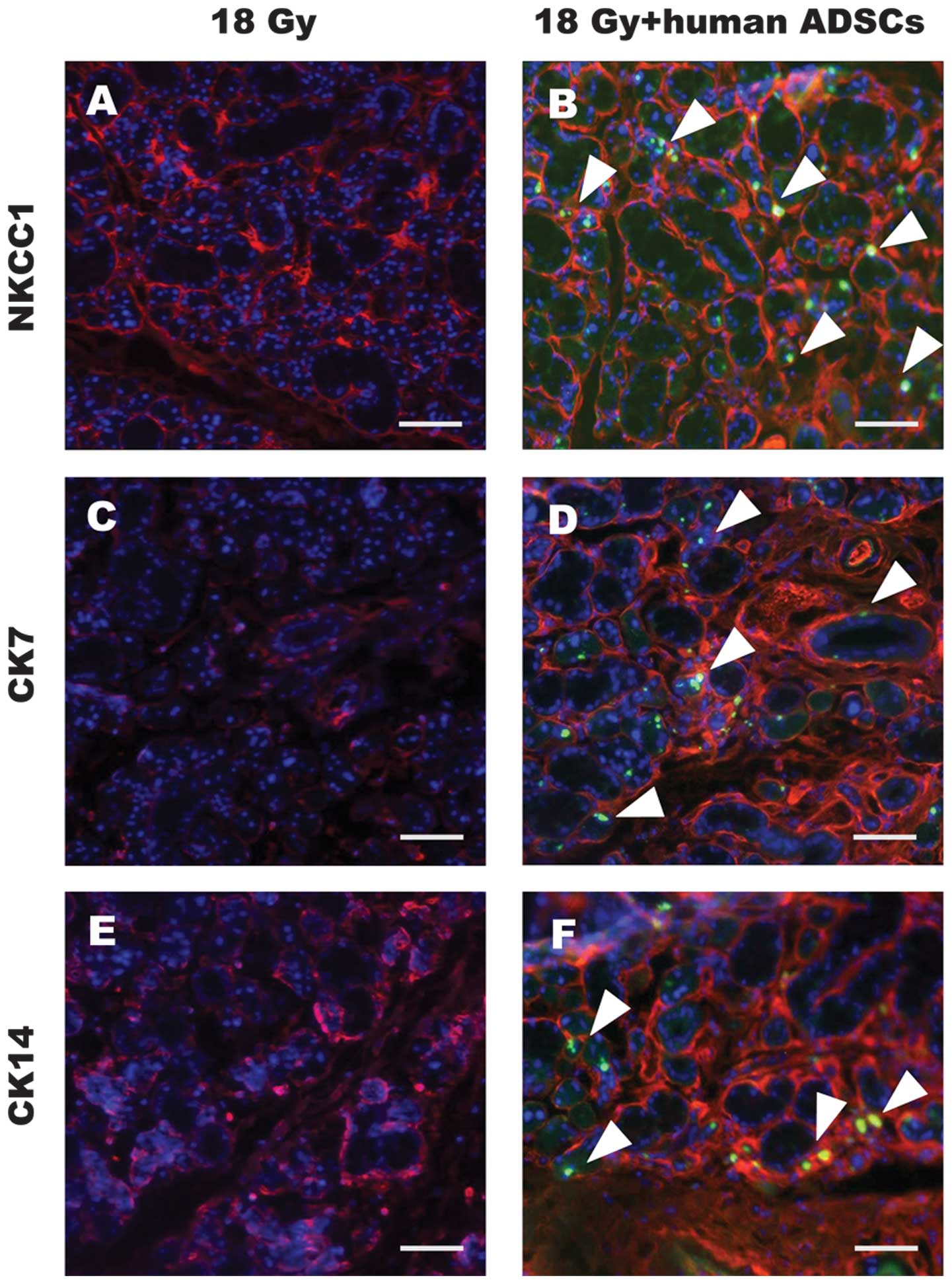
hADSC differentiation into acinar and
duct cells in the submandibular glands
Markers of the 3 main parenchymal cells in the
salivary gland, including acinar, ductal and myoepithelial cells,
were assayed by double immunostaining. At 24 weeks
post-transplantation, ZsGreen-positive cells could still be
observed in the submandibular glands from the rats in group 3.
Moreover, ZsGreen-positive cells were located in cells that
expressed NKCC1 (an acinar cell marker), CK7 and CK14 (duct cell
markers), but they did not express the myoepithelial cell marker,
α-SMA, Fig. 6).
Discussion
Xerostomia remains a major challenge and
complication of radiotherapy for head and neck cancer. In this
study, we demonstrate the potential of hADCSs for rescuing
radiation-damaged rat submandibular glands by intra-glandular
transplantation. Our findings showed that engrafted hADSCs survived
in the submandibular glands, and played a role in the protection
against irradiation-induced cellular apoptosis, and promoted
angiogenic activity. Moreover, a small proportion of hADSCs that
expressed salivary gland cell makers was also detected.
Mesenchymal stem cells (MSCs) are found in a variety
of tissues, including BMDCs (16), umbilical cord blood placenta
(17) and fat (18). MSCs derived from human adipose
tissue are referred to as hADSCs in this study, which present an
accessible and available source for stem cell therapy, and have
been applied in numerous animal and clinical trials (9). The application of MSCs for tissue
repair can be systematically or site-directed. It has been reported
that systemically infused MSCs localize within injured, inflamed
and cancerous tissues. However, their efficiency of homing as a
function of local tissue properties is unclear (19). The risk of intravascular
transplantation of cultured MSCs should also be taken into
consideration (20,21). MSCs can be delivered by
site-directed approaches in the treatment of impaired tissue
(22). Since the submandibular
glands of SD rats are substantially larger than those found in
mice, and they can be targeted subcutaneously near the inferior
border of the mandible, we elected to perform the transplantation
of the hADSCs through an intraglandular route.
The SFR is one of the most visual indices for
evaluating salivary gland function. A higher SFR was detected in
the hADSC-injected group during the experimental period, as
compared to the uninjected controls. However, a slight decline in
the SFR in the hADSC-injected group was observed after 16 weeks,
which may be attributed to a peak in the therapeutic effect.
Although the salivary output of the submandibular gland in the
hADSC treated group failed to recover competence to that of normal
levels, an increase would be helpful for patients who suffer from
dry mouth, and would alleviate symptoms and discomfort following
xerostomia. The main reason for this is that the submandibular
gland produces up to 90% of the salivary volume at rest and 40%
under stimulation in humans (23).
ADSCs also have a multi-lineage differentiation
potential (24). In a previous
study, when hADSCs were co-cultured with murine salivary gland
cells in vitro, only a low number of co-cultured hADSCs
(13–18%) was observed to transdifferentiate into amylase-producing
salivary gland epithelial cells, which represent acinar cells
(25). In this study,
ZsGreen-labeled hADSCs survived in the salivary glands of rats at
24 weeks post-irradiation, and a small proportion was observed as
positive for the expression of NKCC-1, CK7 and CK14, which
indicated transdifferentiation into acinar and ductal cells.
Moreover, hADSCs produce multiple cytokines and chemokines,
angiogenic and anti-apoptotic factors at bioactive levels (15). Additionally, saliva secretion is
highly relevant to blood flow in the gland as the fluid component
of saliva is derived from the local vascular bed in the gland
(26). Our results showed
enhanced angiogenesis and decreased apoptosis in the salivary
glands of the hADSC-treated rats when compared to those of the
untreated rats. In addition, both VEGF and HGF are factors
considered to be important for the improvement of salivary glands.
The expression of VEGF and HGF significantly increased 24 weeks
post-irradiation, as shown by RT-qPCR. These results suggest that
the paracrine effect of hADSCs participated in the protection
against irradiation and improved the microstructure of rat
submandibular glands.
In the present study, we injected hADSCs into the
submandibular glands of SD rats. We found that the hADSCs survived
in the salivary glands, and underwent differentiation into salivary
epithelial cells in the xenogeneic environment. Surviving
xenogeneic engrafted MSCs in fully immunocompetent adult recipients
without immunosuppression have been suggested to be related to the
immunoprivileged properties of MSCs (27). MSCs can avoid immunological
rejection in humans and in animal models, and the mechanisms
involved, while perplexing, remain poorly understood. Three broad
mechanisms that may contribute to this effect are being considered
and these include hypoimmunogenicity, the prevention of T cell
responses and the induction of an immunosuppressive local
microenvironment (28). Our
results showing that long-term hADSC engraftment occurs in
xenogeneic recipients without evidence of immunocompromise, and
that hADSCs take part in tissue repair, are consistent with those
of a previous study (22).
Overall, the present study demonstrates that the
intraglandular transplantation of hADSCs can alleviate
radiation-induced xerostomia, and our data may provide a reference
suitable for subsequent clinical applications.
Acknowledgements
We would like to thank Professor Xiaoqing Liu
(Medical School, Tongji University, Shanghai, China) for the
generous gift of the hADSCs and the other colleagues in the
laboratory for technically supporting our experiments. This study
was supported by grants from the National Natural Science
Foundation of China (nos. 81170942 and 81100673), the National
Science Foundation 973 program (nos. 2010CB945600 and 2011CB965100)
and the Natural Science Foundation of Shanghai (no.
10JC1415500).
References
|
1
|
Baum BJ and Tran SD: Synergy between
genetic and tissue engineering: creating an artificial salivary
gland. Periodontol 2000. 41:218–223. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vissink A, Jansma J, Spijkervet FK,
Burlage FR and Coppes RP: Oral sequelae of head and neck
radiotherapy. Crit Rev Oral Biol Med. 14:199–212. 2003. View Article : Google Scholar
|
|
3
|
Konings AW, Coppes RP and Vissink A: On
the mechanism of salivary gland radiosensitivity. Int J Radiat
Oncol Biol Phys. 62:1187–1194. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nieuw Amerongen AV and Veerman EC: Current
therapies for xerostomia and salivary gland hypofunction associated
with cancer therapies. Support Care Cancer. 11:226–231.
2003.PubMed/NCBI
|
|
5
|
Lombaert IM, Wierenga PK, Kok T, Kampinga
HH, deHaan G and Coppes RP: Mobilization of bone marrow stem cells
by granulocyte colony-stimulating factor ameliorates
radiation-induced damage to salivary glands. Clin Cancer Res.
12:1804–1812. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sumita Y, Liu Y, Khalili S, Maria OM, Xia
D, Key S, Cotrim AP, Mezey E and Tran SD: Bone marrow-derived cells
rescue salivary gland function in mice with head and neck
irradiation. Int J Biochem Cell Biol. 43:80–87. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lombaert IM, Brunsting JF, Wierenga PK,
Faber H, Stokman MA, Kok T, Visser WH, Kampinga HH, de Haan G and
Coppes RP: Rescue of salivary gland function after stem cell
transplantation in irradiated glands. PloS One. 3:e20632008.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zuk PA, Zhu M, Mizuno H, Huang J, Futrell
JW, Katz AJ, Benhaim P, Lorenz HP and Hedrick MH: Multilineage
cells from human adipose tissue: implications for cell-based
therapies. Tissue Eng. 7:211–228. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schäffler A and Büchler C: Concise review:
adipose tissue-derived stromal cells-basic and clinical
implications for novel cell-based therapies. Stem Cells.
25:818–827. 2007.PubMed/NCBI
|
|
10
|
Wen Z, Liao Q, Hu Y, Liu S, You L and Zhao
Y: Human adipose-derived stromal/stem cells: a novel approach to
inhibiting acute pancreatitis. Med Hypotheses. 80:598–600. 2013.
View Article : Google Scholar
|
|
11
|
Kim JM, Lee ST, Chu K, Jung KH, Song EC,
Kim SJ, Sinn DI, Kim JH, Park DK, Kang KM, et al: Systemic
transplantation of human adipose stem cells attenuated cerebral
inflammation and degeneration in a hemorrhagic stroke model. Brain
Res. 1183:43–50. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ra JC, Shin IS, Kim SH, Kang SK, Kang BC,
Lee HY, Kim YJ, Jo JY, Yoon EJ, Choi HJ and Kwon E: Safety of
intravenous infusion of human adipose tissue-derived mesenchymal
stem cells in animals and humans. Stem Cells Dev. 20:1297–1308.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen G, Shi X, Sun C, Li M, Zhou Q, Zhang
C, Huang J, Qiu Y, Wen X, Zhang Y, et al: VEGF-mediated
proliferation of human adipose tissue-derived stem cells. PloS One.
8:e736732013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Labat-Moleur F, Guillermet C, Lorimier P,
Robert C, Lantuejoul S, Brambilla E and Negoescu A: TUNEL apoptotic
cell detection in tissue sections: critical evaluation and
improvement. J Histochem Cytochem. 46:327–334. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rehman J, Traktuev D, Li J, Merfeld-Clauss
S, Temm-Grove CJ, Bovenkerk JE, Pell CL, Johnstone BH, Considine RV
and March KL: Secretion of angiogenic and antiapoptotic factors by
human adipose stromal cells. Circulation. 109:1292–1298. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Friedenstein AJ, Chailakhjan RK and
Lalykina KS: The development of fibroblast colonies in monolayer
cultures of guinea-pig bone marrow and spleen cells. Cell Tissue
Kinet. 3:393–403. 1970.PubMed/NCBI
|
|
17
|
Erices A, Conget P and Minguell JJ:
Mesenchymal progenitor cells in human umbilical cord blood. Br J
Haematol. 109:235–242. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zuk PA, Zhu M, Ashjian P, et al: Human
adipose tissue is a source of multipotent stem cells. Mol Biol
Cell. 13:4279–4295. 2002.PubMed/NCBI
|
|
19
|
Karp JM and Leng Teo GS: Mesenchymal stem
cell homing: the devil is in the details. Cell Stem Cell.
4:206–216. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Freyman T, Polin G, Osman H, Crary J, Lu
M, Cheng L, Palasis M and Wilensky RL: A quantitative, randomized
study evaluating three methods of mesenchymal stem cell delivery
following myocardial infarction. Eur Heart J. 27:1114–1122. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Furlani D, Ugurlucan M, Ong L, Bieback K,
Pittermann E, Westien I, Wang W, Yerebakan C, Li W, Gaebel R, et
al: Is the intravascular administration of mesenchymal stem cells
safe? Mesenchymal stem cells and intravital microscopy. Microvasc
Res. 77:370–376. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rodriguez AM, Pisani D, Dechesne CA,
Turc-Carel C, Kurzenne JY, Wdziekonski B, Villageois A, Bagnis C,
Breittmayer JP, Groux H, Ailhaud G and Dani C: Transplantation of a
multipotent cell population from human adipose tissue induces
dystrophin expression in the immunocompetent mdx mouse. J Exp Med.
201:1397–1405. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Saarilahti K, Kouri M, Collan J,
Kangasmäki A, Atula T, Joensuu H and Tenhunen M: Sparing of the
submandibular glands by intensity modulated radiotherapy in the
treatment of head and neck cancer. Radiother Oncol. 78:270–275.
2006. View Article : Google Scholar
|
|
24
|
Nakagami H, Morishita R, Maeda K, Kikuchi
Y, Ogihara T and Kaneda Y: Adipose tissue-derived stromal cells as
a novel option for regenerative cell therapy. J Atheroscler Thromb.
13:77–81. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lim J-Y, Ra JC, Choi J-S, Jang YH, Lee S,
Kim WC and Kim Y-M: OP061: Adipose tissue-derived mesenchymal stem
cells for regeneration of irradiation-induced salivary gland
damage. Oral Oncology. 49(Suppl 1): S28–S29. 2013. View Article : Google Scholar
|
|
26
|
Baum BJ: Principles of saliva secretion.
Ann N Y Acad Sci. 694:17–23. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Saito T, Kuang JQ, Bittira B, Al-Khaldi A
and Chiu RC: Xenotransplant cardiac chimera: immune tolerance of
adult stem cells. Ann Thorac Surg. 74:19–24. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ryan JM, Barry FP, Murphy JM and Mahon BP:
Mesenchymal stem cells avoid allogeneic rejection. J Inflamm
(Lond). 2:82005. View Article : Google Scholar : PubMed/NCBI
|