Coronavirus disease 2019 (COVID-19) is an illness
resulting from the novel severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2). COVID-19 often begins with respiratory
symptoms, such as cough, fever and fatigue, and develops into acute
respiratory distress syndrome (ARDS) at the later stages of the
disease. However, some patients also exhibit neurological symptoms,
including headaches, dizziness, fatigue, a disruption of
consciousness, insomnia, anosmia and ischemic stroke (1,2).
Ischemic stroke secondary to severe COVID-19 is common and fatal
once it appears. Mao et al demonstrated that patients with
severe COVID-19 were more likely to have complications with
ischemic stroke and this was associated with higher mortality rates
(3). Research on the mechanisms
through which SARS-CoV-2 induces ischemic stroke has become a
popular research topic. It has been demonstrated that SARS-CoV-2
leads to systemic hypercoagulability, namely, to elevated levels of
D-dimer and fibrinogen, as the inducing factor of ischemic stroke
(4). Consequently, some
researchers have postulated that COVID-19 induces ischemic stroke
by promoting a hypercoagulable state in affected patients. However,
the mechanisms through which COVID-19 induces hypercoagulability
remain unclear, and are crucial for the targeted therapy for
ischemic stroke induced by COVID-19. The present review summarizes
the current status of research on COVID-19, hypercoagulability and
ischemic stroke. Subsequently, the underlying mechanisms through
which COVID-19 induces hypercoagulability are summarized. Moreover,
the present review provides therapies that target different
mechanisms for different stages of SARS-CoV-2-induced acute
ischemic stroke (AIS) and for the prevention of AIS in patients
with SARS-CoV-2 infection.
As the COVID-19 pandemic progresses, there is
increasing evidence to indicate that patients with COVID-19 present
hypercoagulability and hyperfibrinolysis, particularly those with
severe COVID-19; this mainly manifests as increased levels of
D-dimer and fibrinogen, a low platelet count, and a prolonged
coagulation time (4). Studies
have suggested that an increased level of D-dimer in patients with
COVID-19 is closely associated with a poor prognosis and a high
mortality rate (5), and heparin
anticoagulant therapy can effectively reduce the mortality rate of
patients with COVID-19 with a D-dimer level >3.0 µg/ml
(6). In addition, the levels of
Von Willebrand factor (VWF) and FXIII are considerably increased in
patients with COVID-19 (7).
Although the level of plasminogen activator inhibitor 1 (PAI-1) in
patients with severe COVID-19 has not yet been investigated, it has
been found to be increased in patients with severe acute
respiratory syndrome; thus, an increased level of PAI-1 would not
be unanticipated (8). The
coagulation indexes of patients with severe infection exhibit
obvious changes compared with those of non-severely infected
patients (Table I).
A number of patients with COVID-19 have developed
venous and arterial thrombosis, which is often associated with high
mortality rates. The autopsy analysis of 12 deceased patients at a
research center in Germany revealed that 7 patients had venous
thrombosis, and 4 had pulmonary embolism (9). A study from Tongji Hospital revealed
71.4% of non-survivors had disseminated intravascular coagulation
(DIC), while 0.6% survivors had DIC (5). Xiong et al demonstrated that
compared with those in patients with moderate COVID-19, the D-dimer
and PT levels were significantly increased in patients with severe
COVID-19, suggesting that DIC was common in patients with severe
COVID-19 (10). A study on 388
patients demonstrated that 26 had thromboembolic events, including
16 with venous thromboembolism, 10 with pulmonary embolism; in
addition, 8 patients had with overt DIC, 9 with ischemic stroke and
4 with myocardial infarction in Italy (11). Further reports of thromboembolic
events in patients with COVID-19 are presented in Table II.
AIS during the COVID-19 outbreak remains a disabling
and lethal disease that cannot be ignored. The main symptoms of
COVID-19 involve fever, cough, and other respiratory symptoms.
However, it has been indicated that AIS can also be the primary
symptom of COVID-19, which is highly suggested to be induced by
SARS-CoV-2 infection (12). As
the COVID-19 pandemic progresses, increasing numbers of research
groups have focused on the association between COVID-19 and AIS.
Fara et al reported cases of AIS in the early stages of
COVID-19 (13). Mao et al
demonstrated that 18.7% of patients with COVID-19 needed to be
transferred to the ICU for treatment due to severe neurological
symptoms, and 5.7% of patients with severe COVID-19 had AIS
(3). Beyrouti et al
analyzed patients with COVID-19 with AIS and found that AIS
occurred at 8-24 days following the onset of COVID-19 symptoms; an
analysis of the laboratory tests revealed that lactate
dehydrogenase, fibrinogen, D-dimer, and C-reactive protein levels
were significantly increased in these patients (14). In addition, Li et al found
the presence of SARS-CoV-2 in the cerebrospinal fluid of patients,
suggesting that this type of virus can penetrate the blood-brain
barrier and damage brain tissue (15).
The pathogenesis of AIS includes thrombosis,
artery-to-artery embolization and hypoperfusion. However, the
pathogenesis of AIS secondary to COVID-19 remains to be
investigated. It has been demonstrated that patients with COVID-19
with secondary AIS had an elevated National Institutes of Stroke
Scale score at admission, an elevated D-dimer level and a poor
prognosis compared to those of non-COVID-19 patients with stroke,
suggesting that blood coagulation plays an essential role in AIS
secondary to COVID-19 (16).
Oxley et al reported cases of secondary AIS in young
patients with COVID-19 with elevated levels of D-dimer and
fibrinogen, and some of these patients did not have risk factors
for stroke, suggesting that COVID-19 induces AIS by promoting
hypercoagulability (17).
Nevertheless, the exact mechanisms through which COVID-19 induces a
hypercoagulable state in patients remain unclear. The following
sections focus on possible procoagulant mechanisms of COVID-19.
More importantly, therapies that target the specific mechanisms for
the more effective treatment of patients with COVID-19 with AIS are
discussed.
Previous studies on patients with severe COVID-19
have demonstrated elevated levels of pro-inflammatory cytokines
(IL-1, IL-2, IL-6, IL-8, IL-10, IL-17 and TNF-α) (18,19). Elevated levels of cytokines cause
inflammation and hypercoagulability in patients with COVID-19,
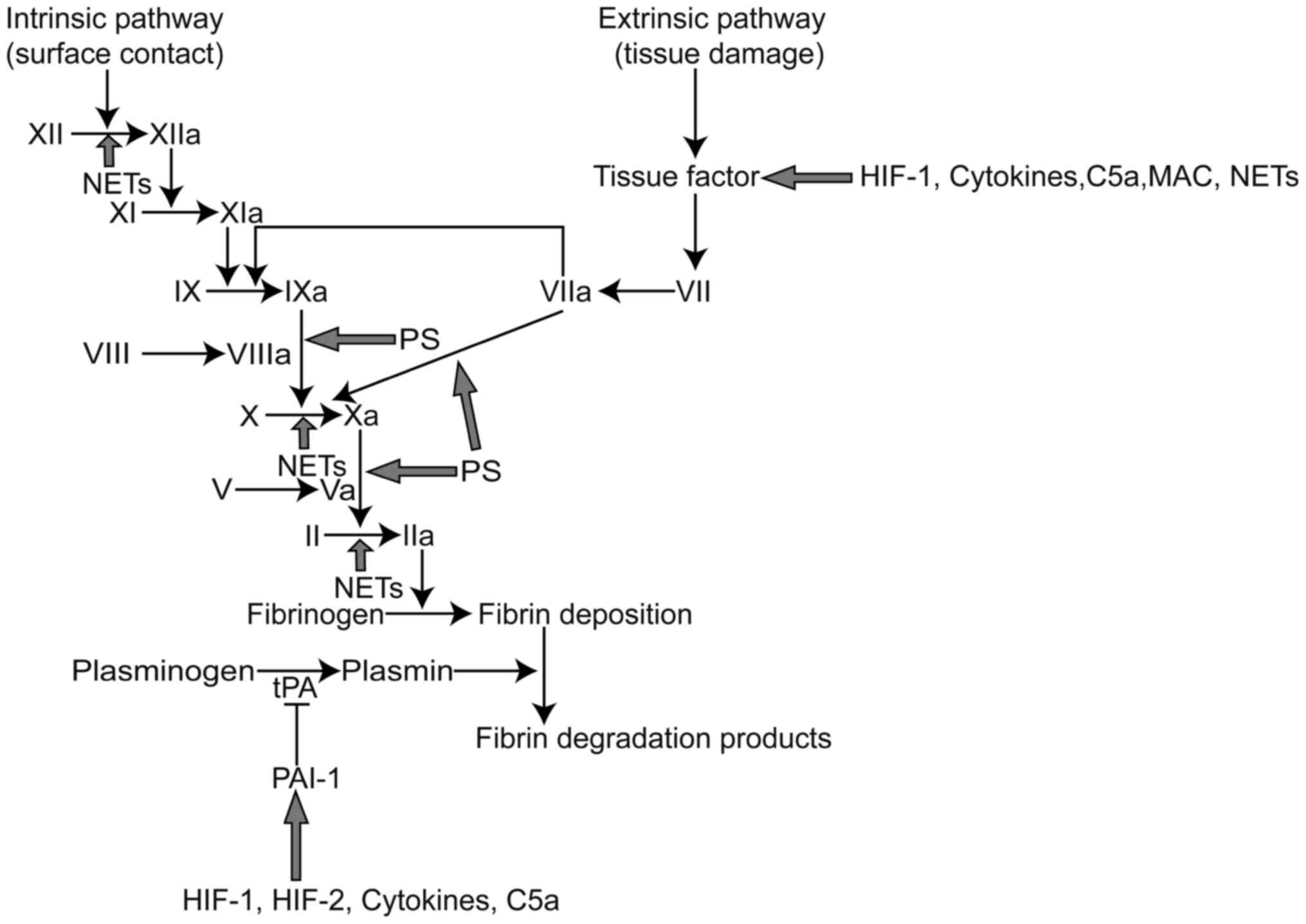
which may be ascribed to several reasons. First, cytokines interact
with the coagulation system. Cytokines, such as IL-1, IL-6 and
TNF-α facilitate the release of tissue factor (TF), which activates
the extrinsic coagulation pathway. Moreover, they promote the
expression of PAI-1, which results in the inhibition of the
fibrinolysis system (Fig. 1)
(20). Beyond that, the levels of
TF pathway inhibitors and antithrombin are decreased in an
inflammatory environment, which causes the activation of the
coagulation system (21). It
should be noted that the activation of thrombin can induce the
overproduction of pro-inflammatory cytokines through PAR-1, while
FXa can activate PAR-1 and PAR-2 to enhance the inflammatory
response (22). Second, cytokines
interact with NETs. Previous studies have indicated that cytokines
promote NET formation, which triggers the extrinsic and intrinsic
coagulation pathways, resulting in thrombin generation.
Correspondingly, NETs also promote the release of inflammatory
cytokines to cause cytokine storms (23). Third, when promoted by IL-1β, IL-8
and TNF-α, blood cells (erythrocytes, leukocytes, and lymphocytes)
expose phosphatidylserine (PS) to their outer membrane, which leads
to a hypercoagulable state (24).
In summary, it is inferred that the elevated levels of cytokines in
COVID-19 patients and the subsequent activation of the coagulation
system leads to AIS.
The majority of patients with severe COVID-19 have
abnormal laboratory data, including low platelet and lymphocyte
counts and increased levels of neutrophils, D-dimer and C-reactive
protein (30). Among these, a low
platelet count has attracted increasing attention. Xu et al
hypothesized that there were 3 main reasons for platelet reduction:
First, viruses may cause decreased platelet synthesis; second,
viruses may lead to increased platelet destruction; and third,
viruses may contribute to thrombosis, which results in platelet
consumption (31). Although
platelet counts are reduced in patients with COVID-19, platelets
are actually activated as reduced platelets are used to form
microthrombi, which may adhere to the endothelium of blood vessels
damaged by the virus (32). Thus,
it is reasonable to believe that activated platelets promote
hypercoagulability. On the one hand, activated platelets release
microparticles (MPs), VWF and PAI to promote coagulation (27), and promote the generation of NETs
that participate in the formation of hypercoagulability (33). Moreover, platelet activation is a
prominent feature of AIS. Therefore, platelet activation in
patients with COVID-19 may promote hypercoagulability and induce
AIS.
Under inflammatory conditions, neutrophils catch
bacteria by extruding neutrophil extracellular traps (NETs), which
are composed of DNA, histones and other active proteins (34). However, NETs are associated with
hypercoagulable states of disease and even promote thrombosis
(Fig. 1) (35). Patients with COVID-19 are in a
state of inflammation, which is advantageous for the generation of
NETs. Some patients with COVID-19 already have elevated neutrophil
counts (14). Moreover, the
inflammatory response triggered by excessive NET formation is
directly related to the destruction of surrounding tissues and
microthrombosis and plays an important role in organ damage. The
above 3 points have been proven to be essential causes of
multiorgan failure in patients with severe COVID-19 (36). Zuo et al found that the
plasma levels of cell free DNA (cf-DNA), myeloperoxidase (MPO)-DNA
and citrullinated histone H3 (CitH3) were significantly elevated in
patients with COVID-19, thereby confirming the presence of NETs in
these patients (37). Their study
also found that plasma cf-DNA levels were positively associated
with plasma D-dimer levels, suggesting that NETs were associated
with hypercoagulability in patients (37). Previous research has demonstrated
the presence of NETs in thrombi and the peripheral blood of
patients with AIS, and the NET content in peripheral blood is
associated with the hypercoagulability of patients with AIS
(33). Based on the
above-mentioned studies, it can be hypothesized that NETs in
patients with COVID-19 lead to a hypercoagulable state that induces
AIS (Fig. 2).
MPs are vesicles (100-1,000 nm) in diameter derived
from the shedding of the cellular membrane of activated or
apoptotic cells. Circulating MPs are produced by a variety of
cells, such as erythrocytes, granulocytes, monocytes, platelets,
and endothelial cells (38). In
recent years, studies have found that MPs induce hypercoagulability
in a number of diseases, such as sepsis, stroke and nephrotic
syndrome (39,40). The expression of
phosphatidylserine (PS) is the underlying cause of MP-induced
coagulation. Cell membrane PS can provide a catalytic surface for
coagulation factors, promoting intrinsic and extrinsic FXa and
thrombin production (Fig. 1)
(41). In addition, Wang et
al found that neutrophil extracellular trap-MP complexes can
promote the intrinsic pathway of coagulation in a sepsis mouse
model; they subsequently found that neutrophil extracellular
trap-MP complexes can trigger inflammation by mediating neutrophil
aggregation through HMGB1-TLR2/TLR4 signaling (42,43). Damaged endothelial cells and
epithelial cells are also found to release MPs in a number of
respiratory diseases, such as chronic obstructive pulmonary
disease, asthma, pulmonary fibrosis and pulmonary hypertension
(44). However, whether MPs play
roles in COVID-19 has not yet been determined. Previous research
has indicated that the systemic inflammatory response syndrome
leads to the activation or apoptosis of blood cells throughout the
body, resulting in the production of MPs (45). Systemic inflammatory response
syndrome is the main cause of multiple organ failure in patients
with severe COVID-19 (19).
Therefore, there is reason to believe that MPs play a procoagulant
role in patients with severe COVID-19.
The complement system plays a major role in
regulating the immune system to protect against viruses. However,
inadequate complement activation may also cause a systemic
inflammatory response that leads to tissue damage. In addition,
complement activation is also associated with coagulation and
microthrombosis (Fig. 1).
Complement activation contributes to membrane attack complex
formation, which drives neutrophil activation and endothelial
damage (46). Cugno et al
demonstrated that the plasma levels of C5a and sC5b-9 were
significantly higher in patients with COVID-19 compared with
healthy subjects, suggesting the activation of the complement
system in patients with COVID-19 (47). Magro et al suggested that
complement system activation was associated with thrombosis in
patients with severe COVID-19 (48). Complement activation may be caused
by the following 2 mechanisms (49): i) The antigen-antibody complexes
formed by antibodies combined with viral antigens initiate
complement activation; and ii) viral invasion results in damage to
endothelial cells, which leads to the activation of the complement
system. Strategies targeting the complement system have been exert
protective effects against brain ischemia-reperfusion injury,
indirectly reflecting that complement activation plays an important
role in the development of AIS (50). Therefore, it is feasible to
believe that the activation of the complement system in COVID-19
contributes to hypercoagulability, which induces AIS.
ARDS, the most common symptom of patients with
severe COVID-19, contributes to hypoxia in the entire body, playing
an essential role in regulating thrombosis by triggering a number
of molecular signaling pathways (51). Platelets are more likely to be
activated in low oxygen environments (52). Moreover, hypoxia prompts the
generation of hypoxia inducible factor (HIF)-1 and HIF-2, leading
to the activation of the coagulation system and impairment of the
fibrinolysis system. More precisely, HIF-1α increases the
expression of TF, which activates extrinsic blood coagulation,
while HIF-1 and HIF-2 promote the expression of PAI-1, which
impairs fibrinolysis (Fig. 1)
(53). Additionally, HIF-1α
induces the formation of NETs (54). NET formation released by activated
neutrophils promotes a hypercoagulable state in the
circulation.
It has previously been reported that bacteria or
viruses can induce antiphospholipid antibodies. A recent article in
the New England Journal of Medicine demonstrated that
antiphospholipid antibody in patients with COVID-19 was associated
with hypercoagulability and the onset of AIS (55). Although only 3 patients were
discussed in that article, sufficient attention should be paid.
Subsequently, Beyrouti et al also found that patients with
COVID-19 with AIS had positive antiphospholipid antibodies, which
were suspected to be related to the onset of stroke (14). It has been demonstrated that
antiphospholipid antibodies initiate coagulation by activating the
TF signaling pathway (56). It
has also been proven that positive antiphospholipid antibodies are
a risk factor for AIS (57).
Therefore, it is considered that the antiphospholipid antibody in
COVID-19 activates the coagulation system and contributes to the
onset of AIS. However, there are no drugs that target
antiphospholipid antibodies in COVID-19. Further research into this
matter is required in the future.
Currently, traditional antithrombotic treatments for
COVID-19 with coagulopathy include anticoagulant therapy and
thrombolytic therapy. Heparin, an anticoagulant and
anti-inflammatory drug, has been used in the treatment of the
hypercoagulable state of COVID-19. Tang et al demonstrated
that COVID-19-induced mortality was reduced by heparin treatment
(58). Compared with heparin, low
molecular weight heparin (LMWH) has a long half-life, is associated
with less bleeding and there is no need for routine coagulation
monitoring. Oudkerk et al suggested that patients with
COVID-19 should be treated with prophylactic LMWH as soon as they
are admitted to the hospital (59). Klok et al found that
despite the prevention of systemic thrombosis with a low dose of
LMWH, a number of patients with COVID-19 still developed thrombotic
events; therefore, a high dose of LMWH was recommended for
anticoagulation in patients with COVID-19 admitted to the ICU
(60). However, has not been
determined which dose of LMWH should be used and this remains
controversial. A previous study found that 31.6% of subjects
supported an intermediate dose for moderate or severe COVID-19,
while 5.2% of subjects supported a therapeutic dose, and the rest
supported a prophylactic dose (61). New oral anticoagulants were also
recommended during the COVID-19 pandemic due to their safety,
convenience, and strong anticoagulant effects (62). SARS-CoV-2 infection not only
activates the coagulation system but also inhibits the fibrinolytic
system. Tissue plasminogen activator (tPA), a thrombolytic drug for
AIS, has been reported to be effective for COVID-19 patients
complicated with ARDS (63).
However, the risk of bleeding should also be evaluated. In
addition, chloroquine, which has been widely used in the treatment
of COVID-19, can also play an antithrombotic role by inhibiting
NETs and interfering with platelet aggregation (64). Statins can prevent the virus from
infecting cells and inhibit the inflammatory response and
coagulation activation, so they could be used to treat thrombosis
in patients with COVID-19 (65).
Further information on the antithrombotic therapy of COVID-19 is
presented in Table III. In
addition, some recommendations for antithrombotic therapy are
presented in Table IV. Although
anticoagulant therapy and thrombolytic therapy have been shown to
be effective, a number of patients with COVID-19 develop thrombotic
complications. Therefore, it is necessary to explore novel methods
of anti-thrombotic therapy. Below, antithrombotic therapy targeting
different mechanisms for coagulation is discussed.
Considering the crucial role of cytokines in leading
to tissue damage and a hypercoagulable state, targeting cytokines
in patients with COVID-19 has become an inevitable trend. It has
been proven that IL-6 initiates the inflammatory response in
patients with COVID-19. Tocilizumab, sarilumab and siltuximab, as
inhibitors of IL-6 and its receptor, have been approved by the Food
and Drug Administration for the treatment of rheumatic and
lymphoproliferative diseases. Importantly, tocilizumab has been
approved for the treatment of patients with COVID-19 with elevated
levels of IL-6 (66,67). IL-17, which acts upstream of
IL-1β, IL-6 and TNF-α, should attract increasing attention.
Secukinumab, ixekizumab and brodalumab, as inhibitors of IL-17 and
its receptor, have been shown to be effective in the treatment of
psoriasis (18); however, their
effects on COVID-19 need to be further investigated.
Preventing viruses from entering cells has become a
novel method for the treatment of COVID-19. Human recombinant
soluble angiotensin-converting enzyme 2 (hrsACE2), currently being
studied, can competitively bind to viruses to inhibit viruses from
being able to invade into cells (68). Fortunately, hrsACE2 has been
approved for the treatment of ARDS (68-70). Given the damage exerted by
cytokines to endothelial cells, anti-inflammatory treatment such as
with tocilizumab may also protect endothelial cells (18,66). Additionally, colchicine,
azithromycin and famotidine have also been proven to reduce
endothelial injury (71).
Previous studies have demonstrated that aspirin is
effective in patients with pneumonia, particularly in those with
severe pneumonia complicated by ARDS or sepsis (72). In animal experiments, the
combination of clopidogrel and oseltamivir has been shown to
effectively inhibit the inflammatory response induced by influenza
pneumonia and can thus improve the survival rate of mice (73). Furthermore, aspirin and
clopidogrel can efficiently prevent the occurrence of
cardiovascular and cerebrovascular diseases.
The targeting of NETs for the treatment of
inflammatory diseases and thrombotic diseases has improved. Thus,
there is reason to believe that therapies that target NETs are of
vital importance for COVID-19 treatment. Currently, there are 3
main mechanisms against NETs: The inhibition of NET formation, the
direct degradation of NETs and the inhibition of upstream
regulatory molecules of NETs. The histone inhibitor, activated
protein C and the neutrophil elastase inhibitor, sivelestat, have
been shown to reduce hypercoagulability in AIS by inhibiting the
generation of NETs (33). BWA3,
an anti-histone H4 antibody, can effectively reduce infarct size in
t-MACO mice (74). Recombinant
DNase I (dornase alfa) can directly degrade NETs in the airway of
patients with cystic fibrosis, relieving patient symptoms (75). In addition, recombinant DNase I
has been shown to improve the efficiency of tPA thrombolysis in
vitro (76) and reduced
hypercoagulability in patients with AIS (33). IL-1β and HMGB1 have been reported
to mediate the generation of NETs in various diseases. Targeting
IL-1β or HMGB1 can inhibit the generation of NETs, thereby
improving multiorgan functions (77,78).
The inhibition of the complement system may be an
underlying treatment for patients with severe COVID-19 with
coagulopathy. In a virus-infected mouse model, the inhibition of C3
or C5 was shown to reduce the inflammatory response by attenuating
the release of cytokines (81).
The C5 inhibitor eculizumab may treat COVID-19 by hampering the
amplification of the complement cascade (47). The C3 inhibitor, AMY-101, which
can effectively inhibit the production of C3a and C5a and inhibit
the release of IL-6, is currently undergoing clinical trials for
the treatment of periodontal disease (NCT03694444) (82).
Mechanical ventilation is a key treatment for
patients with severe COVID-19 with ARDS. Hyperbaric oxygen therapy
has been shown to improve neurological function in patients with
stroke (83). Extracorporeal
membrane oxygenation has been used in the treatment of
COVID-19-related ARDS (84).
However, whether oxygen therapy or extracorporeal membrane
oxygenation is effective for COVID-19 patients with AIS needs to be
studied further.
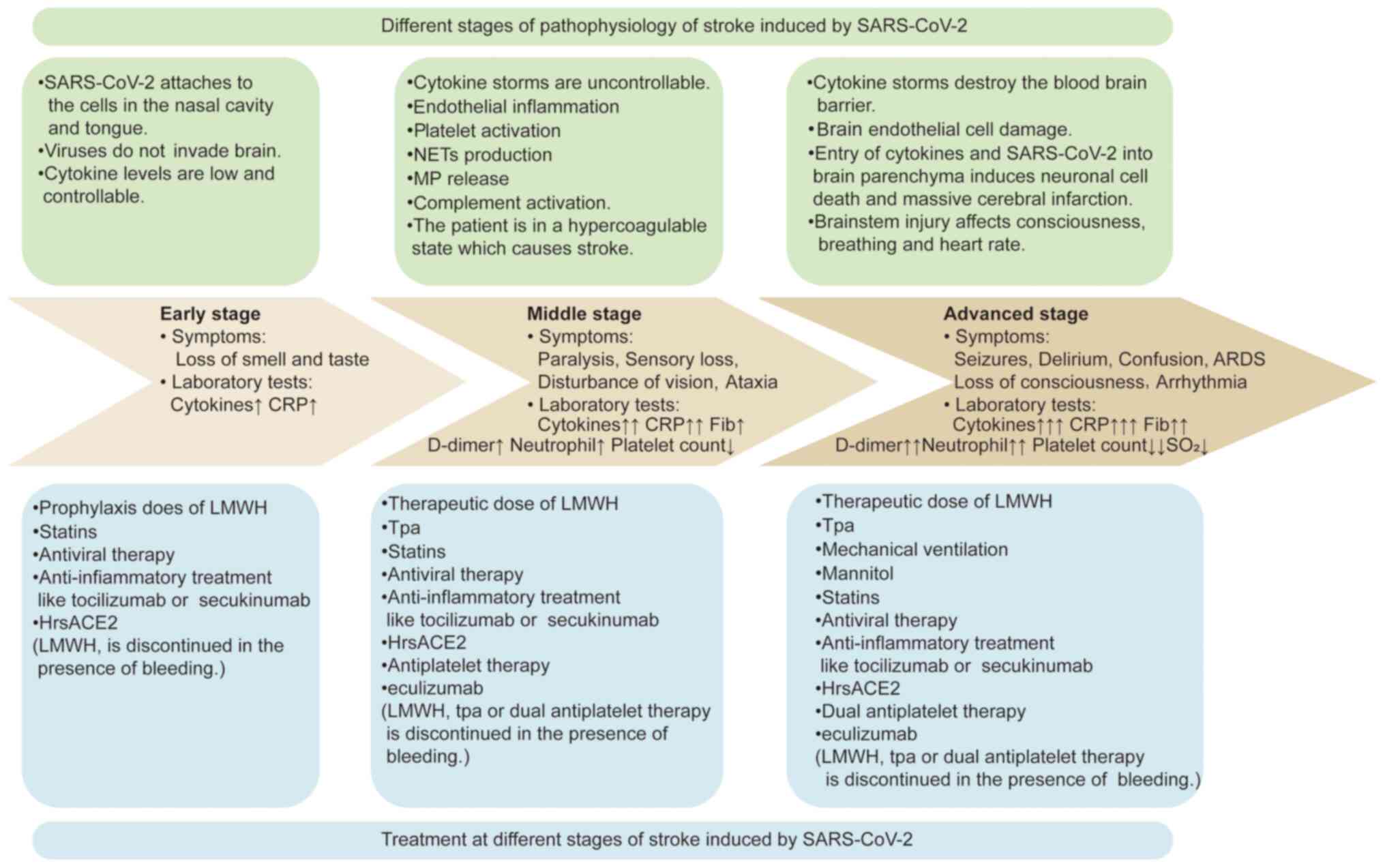
SARS-CoV-2-induced AIS encompasses 3 main stages: An
early stage that involves controllable levels of cytokines with
mild symptoms, a middle stage that is characterized by the
activation of the coagulation system and occurrence of AIS, and an
advanced stage that involves the progression to massive cerebral
infarction. The present review summarized the pathophysiology,
symptoms and laboratory tests at different stages of
SARS-CoV-2-induced AIS. More importantly, antithrombotic strategies
are suggested for different stages of SARS-CoV-2-induced AIS
(Fig. 3).
Various methods are proposed for the prevention of
AIS according to the different states of patients with SARS-CoV-2
infection (Table V).
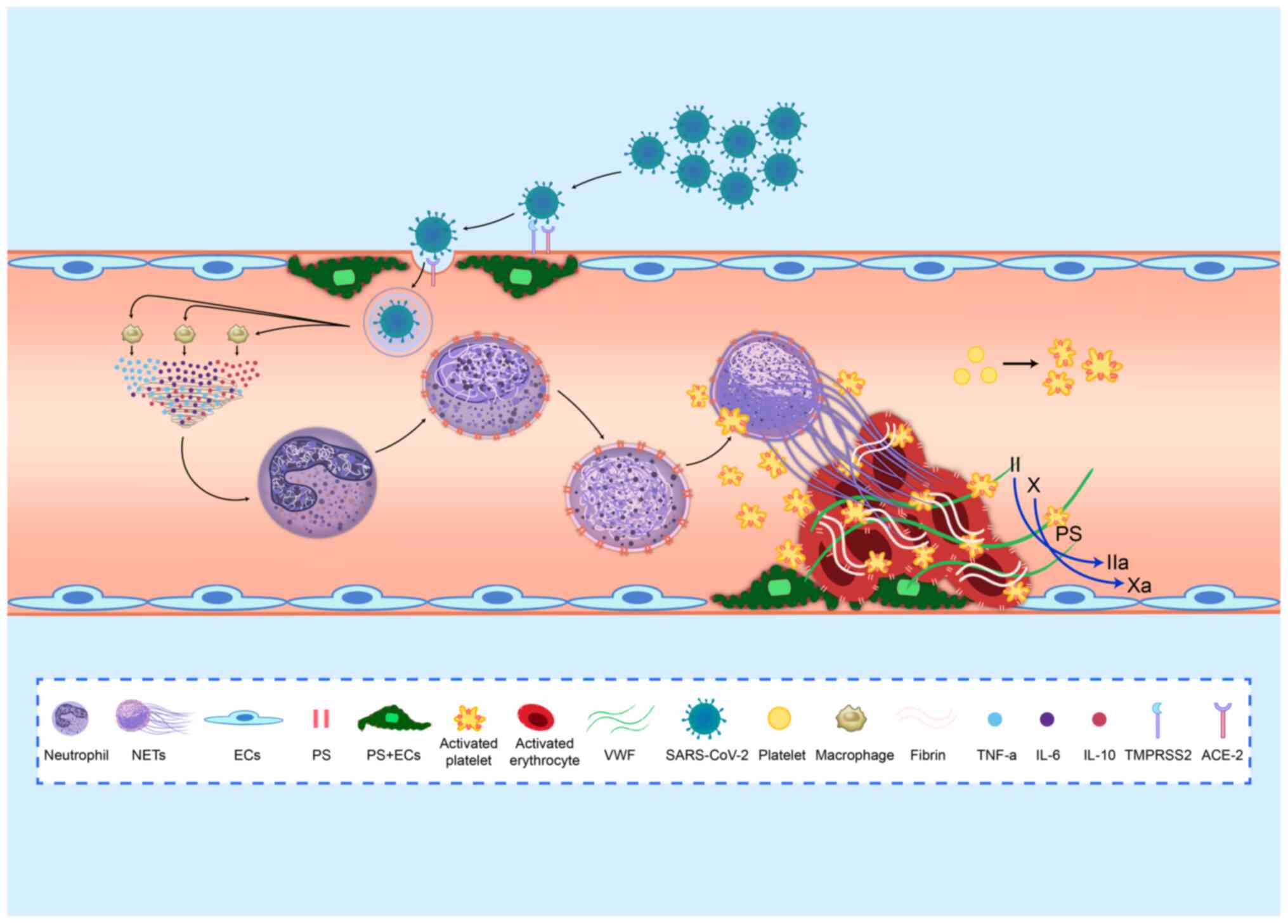
Although various components, including cytokines,
damaged endothelial cells, activated platelets, NETs, MPs, the
activated complement system, hypoxia and the antiphospholipid
antibody, are believed to activate the coagulation system during
the development of COVID-19, it is considered that cytokines play a
predominant role in COVID-19-associated hypercoagulability. The
invasion of SARS-CoV-2 activates the immune system and produces a
large number of cytokines. Cytokines and the invasion of SARS-CoV-2
result in the injury of endothelial cells, which then leads to the
generation of NETs, the release of MPs, the activation of platelets
and the activation of the complement system. Given that brain
tissue is highly sensitive to hypoxia, hypoxia plays an essential
role in COVID-19-associated stroke. Hypoxia can not only lead to
brain interstitial edema but also activate the coagulation
system.
Antithrombotic therapy is often overlooked in the
treatment of COVID-19. Antithrombotic therapy can not only treat
thrombosis in COVID-19 but can also increase the blood oxygen
saturation level in patients with COVID-19. However, traditional
antithrombotic therapy fails to treat COVID-19 with coagulopathy. A
more comprehensive antithrombotic therapy targeting different
mechanisms should be given to COVID-19 patients who develop
thrombosis, such as stroke. We believe that traditional
antithrombotic therapy plus anti-inflammatory therapy should be
used as the basis of comprehensive antithrombotic therapy.
The present review focused on the mechanisms that
lead to the hypercoagulable state in patients with COVID-19 and the
association between AIS and these mechanisms. A more comprehensive
treatment method was also provided to complement traditional
antithrombotic therapy. In addition, methods for the prevention of
AIS were discussed. Since patients with severe COVID-19 are prone
to complications with AIS, antithrombotic therapy should be given
in the early stages of COVID-19 to prevent the occurrence of
AIS.
The present study was supported by grants from the
National Science Foundation of China (81670128 and 81873433) and
the Graduate Innovation Fund of Harbin Medical University
(YJSSJCX2019-07HYD).
Not applicable.
SZ designed the review, prepared the tables and
figures, and wrote the manuscript. JZ and XC were involved in the
conception and design of the study. CW and XZ searched the
literature and wrote the manuscript. HJ, HL and ZL provided helpful
comments and acquired data. LW was involved in the conception and
design of the study and revised the manuscript. JS designed the
study and revised the manuscript. All authors read and approved the
final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
Not applicable.
|
1
|
Jamwal S, Gautam A, Elsworth J, Kumar M,
Chawla R and Kumar P: An updated insight into the molecular
pathogenesis, secondary complications and potential therapeutics of
COVID-19 pandemic. Life Sci. 257:1181052020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nalleballe K, Reddy Onteddu S, Sharma R,
Dandu V, Brown A, Jasti M, Yadala S, Veerapaneni K, Siddamreddy S,
Avula A, et al: Spectrum of neuropsychiatric manifestations in
COVID-19. Brain Behav Immun. 88:71–74. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mao L, Jin H, Wang M, Hu Y, Chen S, He Q,
Chang J, Hong C, Zhou Y, Wang D, et al: Neurologic manifestations
of hospitalized patients with coronavirus disease 2019 in Wuhan,
China. JAMA Neurol. 77:683–690. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Han H, Yang L, Liu R, Liu F, Wu KL, Li J,
Liu XH and Zhu CL: Prominent changes in blood coagulation of
patients with SARS-CoV-2 infection. Clin Chem Lab Med.
58:1116–1120. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tang N, Li D, Wang X and Sun Z: Abnormal
coagulation parameters are associated with poor prognosis in
patients with novel coronavirus pneumonia. J Thromb Haemost.
18:844–847. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yin S, Huang M, Li D and Tang N:
Difference of coagulation features between severe pneumonia induced
by SARS-CoV2 and non-SARS-CoV2. J Thromb Thrombolysis. 1–4.
2020.
|
|
7
|
Helms J, Tacquard C, Severac F,
Leonard-Lorant I, Ohana M, Delabranche X, Merdji H, Clere-Jehl R,
Schenck M, Fagot Gandet F, et al: High risk of thrombosis in
patients with severe SARS-CoV-2 infection: A multicenter
prospective cohort study. Intensive Care Med. 46:1089–1098. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Whyte CS, Morrow GB, Mitchell JL, Chowdary
P and Mutch NJ: Fibrinolytic abnormalities in acute respiratory
distress syndrome (ARDS) and versatility of thrombolytic drugs to
treat COVID-19. J Thromb Haemost. 18:1548–1555. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wichmann D, Sperhake JP, Lütgehetmann M,
Steurer S, Edler C, Heinemann A, Heinrich F, Mushumba H, Kniep I,
Schröder AS, et al: Autopsy findings and venous thromboembolism in
patients With COVID-19: A prospective cohort study. Ann Intern Med.
173:268–277. 2020. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xiong M, Liang X and Wei YD: Changes in
blood coagulation in patients with severe coronavirus disease 2019
(COVID-19): A meta-analysis. Br J Haematol. 189:1050–1052. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lodigiani C, Iapichino G, Carenzo L,
Cecconi M, Ferrazzi P, Sebastian T, Kucher N, Studt JD, Sacco C,
Bertuzzi A, et al: Venous and arterial thromboembolic complications
in COVID-19 patients admitted to an academic hospital in Milan,
Italy. Thromb Res. 191:9–14. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Avula A, Nalleballe K, Narula N,
Sapozhnikov S, Dandu V, Toom S, Glaser A and Elsayegh D: COVID-19
presenting as stroke. Brain Behav Immun. 87:115–119. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fara MG, Stein LK, Skliut M, Morgello S,
Fifi JT and Dhamoonr MS: Macrothrombosis and stroke in patients
with mild Covid-19 infection. J Thromb Haemost. 18:2031–2033. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Beyrouti R, Adams ME, Benjamin L, Cohen H,
Farmer SF, Goh YY, Humphries F, Jäger HR, Losseff NA, Perry RJ, et
al: Characteristics of ischaemic stroke associated with COVID-19. J
Neurol Neurosurg Psychiatry. 91:889–891. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li YC, Bai WZ and Hashikawa T: The
neuroinvasive potential of SARS-CoV2 may play a role in the
respiratory failure of COVID-19 patients. J Med Virol. 92:552–555.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yaghi S, Ishida K, Torres J, Mac Grory B,
Raz E, Humbert K, Henninger N, Trivedi T, Lillemoe K, Alam S, et
al: SARS-CoV-2 and stroke in a New York healthcare system. Stroke.
51:2002–2011. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Oxley TJ, Mocco J, Majidi S, Kellner CP,
Shoirah H, Singh IP, De Leacy RA, Shigematsu T, Ladner TR, Yaeger
KA, et al: Large-vessel stroke as a presenting feature of Covid-19
in the young. N Engl J Med. 382:e602020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pacha O, Sallman MA and Evans SE:
COVID-19: A case for inhibiting IL-17? Nat Rev Immunol. 20:345–346.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mehta P, McAuley DF, Brown M, Sanchez E,
Tattersall RS and Manson JJ; HLH Across Speciality Collaboration
UK: COVID-19: Consider cytokine storm syndromes and
immunosuppression. Lancet. 395:1033–1034. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Sawdey MS and Loskutoff DJ: Regulation of
murine type 1 plasminogen activator inhibitor gene expression in
vivo. Tissue specificity and induction by lipopolysaccharide, tumor
necrosis factor-alpha, and transforming growth factor-beta. J Clin
Invest. 88:1346–1353. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fourrier F, Chopin C, Goudemand J,
Hendrycx S, Caron C, Rime A, Marey A and Lestavel P: Septic shock,
multiple organ failure, and disseminated intravascular coagulation.
Compared patterns of antithrombin III, protein C, and protein S
deficiencies. Chest. 101:816–823. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jose RJ and Manuel A: COVID-19 cytokine
storm: The interplay between inflammation and coagulation. Lancet
Respir Med. 8:e46–e47. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hudock KM, Collins MS, Imbrogno M,
Snowball J, Kramer EL, Brewington JJ, Gollomp K, McCarthy C,
Ostmann AJ, Kopras EJ, et al: Neutrophil extracellular traps
activate IL-8 and IL-1 expression in human bronchial epithelia. Am
J Physiol Lung Cell Mol Physiol. 319:L137–L147. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pliyev BK and Menshikov M: Differential
effects of the autophagy inhibitors 3-methyladenine and chloroquine
on spontaneous and TNF-α-induced neutrophil apoptosis. Apoptosis.
17:1050–1065. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Varga Z, Flammer AJ, Steiger P, Haberecker
M, Andermatt R, Zinkernagel AS, Mehra MR, Schuepbach RA, Ruschitzka
F and Moch H: Endothelial cell infection and endotheliitis in
COVID-19. Lancet. 395:1417–1418. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Leisman DE, Deutschman CS and Legrand M:
Facing COVID-19 in the ICU: Vascular dysfunction, thrombosis, and
dysregulated inflammation. Intensive Care Med. 46:1105–1108. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Li T, Wang C, Liu Y, Li B, Zhang W, Wang
L, Yu M, Zhao X, Du J, Zhang J, et al: Neutrophil extracellular
traps induce intestinal damage and thrombotic tendency in
inflammatory bowel disease. J Crohns Colitis. 14:240–253. 2020.
View Article : Google Scholar
|
|
28
|
Zubair AS, McAlpine LS, Gardin T,
Farhadian S, Kuruvilla DE and Spudich S: Neuropathogenesis and
neurologic manifestations of the coronaviruses in the age of
coronavirus disease 2019: A review. JAMA Neurol. 77:1018–1027.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Al Saiegh F, Ghosh R, Leibold A, Avery MB,
Schmidt RF, Theofanis T, Mouchtouris N, Philipp L, Peiper SC, Wang
ZX, et al: Status of SARS-CoV-2 in cerebrospinal fluid of patients
with COVID-19 and stroke. J Neurol Neurosurg Psychiatry.
91:846–848. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han
Y, Qiu Y, Wang J, Liu Y, Wei Y, et al: Epidemiological and clinical
characteristics of 99 cases of 2019 novel coronavirus pneumonia in
Wuhan, China: A descriptive study. Lancet. 395:507–513. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Xu P, Zhou Q and Xu J: Mechanism of
thrombocytopenia in COVID-19 patients. Ann Hematol. 99:1205–1208.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hottz ED, Bozza FA and Bozza PT: Platelets
in immune response to virus and immunopathology of viral
infections. Front Med (Lausanne). 5:1212018. View Article : Google Scholar
|
|
33
|
Zhou P, Li T, Jin J, Liu Y, Li B, Sun Q,
Tian J, Zhao H, Liu Z, Ma S, et al: Interactions between neutrophil
extracellular traps and activated platelets enhance procoagulant
activity in acute stroke patients with ICA occlusion. EBioMedicine.
53:1026712020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Brinkmann V, Reichard U, Goosmann C,
Fauler B, Uhlemann Y, Weiss DS, Weinrauch Y and Zychlinsky A:
Neutrophil extracellular traps kill bacteria. Science.
303:1532–1535. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Martinod K and Wagner DD: Thrombosis:
Tangled up in NETs. Blood. 123:2768–2776. 2014. View Article : Google Scholar :
|
|
36
|
Barnes BJ, Adrover JM, Baxter-Stoltzfus A,
Borczuk A, Cools-Lartigue J, Crawford JM, Dassler-Plenker J, Guerci
P, Huynh C, Knight JS, et al: Targeting potential drivers of
COVID-19: Neutrophil extracellular traps. J Exp Med.
217:e202006522020. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zuo Y, Yalavarthi S, Shi H, Gockman K, Zuo
M, Madison JA, Blair C, Weber A, Barnes BJ, Egeblad M, et al:
Neutrophil extracellular traps in COVID-19. JCI Insight.
5:e1389992020.
|
|
38
|
Hargett LA and Bauer NN: On the origin of
microparticles: From 'platelet dust' to mediators of intercellular
communication. Pulm Circu. 3:329–340. 2013. View Article : Google Scholar
|
|
39
|
Yao Z, Wang L, Wu X, Zhao L, Chi C, Guo L,
Tong D, Yang X, Dong Z, Deng R, et al: Enhanced procoagulant
activity on blood cells after acute ischemic stroke. Transl Stroke
Res. 8:83–91. 2017. View Article : Google Scholar
|
|
40
|
Yu M, Xie R, Zhang Y, Liang H, Hou L, Yu
C, Zhang J, Dong Z, Tian Y, Bi Y, et al: Phosphatidylserine on
microparticles and associated cells contributes to the
hypercoagulable state in diabetic kidney disease. Nephrol Dial
Transplant. 33:2115–2127. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Vance JE and Steenbergen R: Metabolism and
functions of phosphatidylserine. Prog Lipid Res. 44:207–234. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wang Y, Du F, Hawez A, Mörgelin M and
Thorlacius H: Neutrophil extracellular trap-microparticle complexes
trigger neutrophil recruitment via high-mobility group protein 1
(HMGB1)-toll-like receptors(TLR2)/TLR4 signalling. Br J Pharmacol.
176:3350–3363. 2019.PubMed/NCBI
|
|
43
|
Wang Y, Luo L, Braun OÖ, Westman J, Madhi
R, Herwald H, Mörgelin M and Thorlacius H: Neutrophil extracellular
trap-microparticle complexes enhance thrombin generation via the
intrinsic pathway of coagulation in mice. Sci Rep. 8:40202018.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Nieri D, Neri T, Petrini S, Vagaggini B,
Paggiaro P and Celi A: Cell-derived microparticles and the lung.
Eur Respir Rev. 25:266–277. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Balvers K, Curry N, Kleinveld DJ, Böing
AN, Nieuwland R, Goslings JC and Juffermans NP: Endogenous
microparticles drive the proinflammatory host immune response in
severely injured trauma patients. Shock. 43:317–321. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Riedl M, Fakhouri F, Le Quintrec M, Noone
DG, Jungraithmayr TC, Fremeaux-Bacchi V and Licht C: Spectrum of
complement-mediated thrombotic microangiopathies: Pathogenetic
insights identifying novel treatment approaches. Semin Thromb
Hemost. 40:444–464. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Cugno M, Meroni PL, Gualtierotti R,
Griffini S, Grovetti E, Torri A, Panigada M, Aliberti S, Blasi F,
Tedesco F and Peyvandi F: Complement activation in patients with
COVID-19: A novel therapeutic target. J Allergy Clin Immunol.
146:215–217. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Magro C, Mulvey JJ, Berlin D, Nuovo G,
Salvatore S, Harp J, Baxter-Stoltzfus A and Laurence J: Complement
associated microvascular injury and thrombosis in the pathogenesis
of severe COVID-19 infection: A report of five cases. Transl Res.
220:1–13. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Stites E, Renner B, Laskowski J, Le
Quintrec M, You Z, Freed B, Cooper J, Jalal D and Thurman JM:
Complement fragments are biomarkers of antibody-mediated
endothelial injury. Mol Immunol. 118:142–152. 2020. View Article : Google Scholar
|
|
50
|
Heydenreich N, Nolte MW, Göb E, Langhauser
F, Hofmeister M, Kraft P, Albert-Weissenberger C, Brede M,
Varallyay C, Göbel K, et al: C1-inhibitor protects from brain
ischemia-reperfusion injury by combined antiinflammatory and
antithrombotic mechanisms. Stroke. 43:2457–2467. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Pugh CW and Ratcliffe PJ: New horizons in
hypoxia signaling pathways. Exp Cell Res. 356:116–121. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Cameron SJ, Mix DS, Ture SK, Schmidt RA,
Mohan A, Pariser D, Stoner MC, Shah P, Chen L, Zhang H, et al:
Hypoxia and ischemia promote a maladaptive platelet phenotype.
Arterioscler Thromb Vasc Biol. 38:1594–1606. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Gupta N, Zhao YY and Evans CE: The
stimulation of thrombosis by hypoxia. Thromb Res. 181:77–83. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Frangou E, Chrysanthopoulou A, Mitsios A,
Kambas K, Arelaki S, Angelidou I, Arampatzioglou A, Gakiopoulou H,
Bertsias GK, Verginis P, et al: REDD1/autophagy pathway promotes
thromboinflammation and fibrosis in human systemic lupus
erythematosus (SLE) through NETs decorated with tissue factor (TF)
and inter-leukin-17A (IL-17A). Ann Rheum Dis. 78:238–248. 2019.
View Article : Google Scholar
|
|
55
|
Zhang Y, Xiao M, Zhang S, Xia P, Cao W,
Jiang W, Chen H, Ding X, Zhao H, Zhang H, et al: Coagulopathy and
antiphospholipid antibodies in patients with Covid-19. N Engl J
Med. 382:e382020. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Müller-Calleja N, Hollerbach A, Ritter S,
Pedrosa DG, Strand D, Graf C, Reinhardt C, Strand S, Poncelet P,
Griffin JH, et al: Tissue factor pathway inhibitor primes monocytes
for antiphospholipid antibody-induced thrombosis. Blood.
134:1119–1131. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Gašperšič N, Zaletel M, Kobal J, Žigon P,
Čučnik S, Šemrl SS, Tomšič M and Ambrožič A: Stroke and
antiphospholipid syndrome-antiphospholipid antibodies are a risk
factor for an ischemic cerebrovascular event. Clin Rheumatol.
38:379–384. 2019. View Article : Google Scholar
|
|
58
|
Tang N, Bai H, Chen X, Gong J, Li D and
Sun Z: Anticoagulant treatment is associated with decreased
mortality in severe coronavirus disease 2019 patients with
coagulopathy. J Thromb Haemost. 18:1094–1099. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Oudkerk M, Buller HR and Kuijpers D:
Diagnosis, prevention, and treatment of thromboembolic
complications in COVID-19: Report of the National Institute for
Public Health of the Netherlands. Radiology. 297:E216–E222. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Klok FA, Kruip MJHA, van der Meer NJM,
Arbous MS, Gommers DAMPJ, Kant KM, Kaptein FHJ, van Paassen J,
Stals MAM, Huisman MV and Endeman H: Incidence of thrombotic
complications in critically ill ICU patients with COVID-19. Thromb
Res. 191:145–147. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Bikdeli B, Madhavan MV, Jimenez D, Chuich
T, Dreyfus I, Driggin E, Nigoghossian C, Ageno W, Madjid M, Guo Y,
et al: COVID-19 and thrombotic or thromboembolic disease:
Implications for prevention, antithrombotic therapy, and follow-up.
J Am Coll Cardiol. 75:2950–2973. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Hermans C and Lambert C: Impact of the
COVID-19 pandemic on therapeutic choices in thrombosis-hemostasis.
J Thromb Haemost. 18:1794–1795. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Wang J, Hajizadeh N, Moore EE, McIntyre
RC, Moore PK, Veress LA, Yaffe MB, Moore HB and Barrett CD: Tissue
plasminogen activator (tPA) treatment for COVID-19 associated acute
respiratory distress syndrome (ARDS): A case series. J Thromb
Haemost. 18:1752–1755. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Quiros Roldan E, Biasiotto G, Magro P and
Zanella I: The possible mechanisms of action of 4-aminoquinolines
(chloroquine/hydroxychloroquine) against Sars-Cov-2 infection
(COVID-19): A role for iron homeostasis? Pharmacol Res.
158:1049042020. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Rodrigues-Diez RR, Tejera-Muñoz A,
Marquez-Exposito L, Rayego-Mateos S, Sanchez LS, Marchant V,
Santamaria LT, Ramos AM, Ortiz A, Egido J and Ruiz-Ortega M:
Statins: Could an old friend help the fight against COVID-19? Br J
Pharmacol. 177:4873–4886. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Ascierto PA, Fox BA, Urba WJ, Anderson AC,
Atkins MB, Borden EC, Brahmer JR, Butterfield LH, Cesano A, Chen
DC, et al: Insights from immuno-oncology: The Society for
Immunotherapy of Cancer Statement on access to IL-6-targeting
therapies for COVID-19. J Immunother Cancer. 8:e0008782020.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Paniri A and Akhavan-Niaki H: Emerging
role of IL-6 and NLRP3 inflammasome as potential therapeutic
targets to combat COVID-19: Role of lncRNAs in cytokine storm
modulation. Life Sci. 118114:2020.
|
|
68
|
Alhenc-Gelas F and Drueke TB: Blockade of
SARS-CoV-2 infection by recombinant soluble ACE2. Kidney Int.
97:1091–1093. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Haschke M, Schuster M, Poglitsch M,
Loibner H, Salzberg M, Bruggisser M, Penninger J and Krähenbühl S:
Pharmacokinetics and pharmacodynamics of recombinant human
angiotensin-converting enzyme 2 in healthy human subjects. Clin
Pharmacokinet. 52:783–792. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Khan A, Benthin C, Zeno B, Albertson TE,
Boyd J, Christie JD, Hall R, Poirier G, Ronco JJ, Tidswell M, et
al: A pilot clinical trial of recombinant human
angiotensin-converting enzyme 2 in acute respiratory distress
syndrome. Crit Care. 21:2342017. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Sardu C, Gambardella J, Morelli MB, Wang
X, Marfella R and Santulli G: Hypertension, thrombosis, kidney
failure, and diabetes: Is COVID-19 an endothelial disease? A
comprehensive evaluation of clinical and basic evidence. J Clin
Med. 9:14172020. View Article : Google Scholar :
|
|
72
|
Fan E, Brodie D and Slutsky AS: Acute
respiratory distress syndrome: Advances in diagnosis and treatment.
JAMA. 319:698–710. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Pulavendran S, Rudd JM, Maram P, Thomas
PG, Akhilesh R, Malayer JR, Chow VTK and Teluguakula N: Combination
therapy targeting platelet activation and virus replication
Protects mice against lethal influenza pneumonia. Am J Respir Cell
Mol Biol. 61:689–701. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
De Meyer SF, Suidan GL, Fuchs TA,
Monestier M and Wagner DD: Extracellular chromatin is an important
mediator of ischemic stroke in mice. Arterioscler Thromb Vasc Biol.
32:1884–1891. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Papayannopoulos V, Staab D and Zychlinsky
A: Neutrophil elastase enhances sputum solubilization in cystic
fibrosis patients receiving DNase therapy. PLoS One. 6:e285262011.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Laridan E, Denorme F, Desender L, François
O, Andersson T, Deckmyn H, Vanhoorelbeke K and De Meyer SF:
Neutrophil extracellular traps in ischemic stroke thrombi. Ann
Neurol. 82:223–232. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Mistry P, Carmona-Rivera C, Ombrello AK,
Hoffmann P, Seto NL, Jones A, Stone DL, Naz F, Carlucci P,
Dell'Orso S, et al: Dysregulated neutrophil responses and
neutrophil extracellular trap formation and degradation in PAPA
syndrome. Ann Rheum Dis. 77:1825–1833. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Kim SW, Lee H, Lee HK, Kim ID and Lee JK:
Neutrophil extracellular trap induced by HMGB1 exacerbates damages
in the ischemic brain. Acta Neuropathol Commun. 7:942019.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Neri T, Scalise V, Passalacqua I,
Sanguinetti C, Lombardi S, Pergoli L, Bollati V, Pedrinelli R,
Paggiaro P and Celi A: Tiotropium inhibits proinflammatory
microparticle generation by human bronchial and endothelial cells.
Sci Rep. 9:116312019. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Neri T, Lombardi S, Faìta F, Petrini S,
Balìa C, Scalise V, Pedrinelli R, Paggiaro P and Celi A:
Pirfenidone inhibits p38-mediated generation of procoagulant
microparticles by human alveolar epithelial cells. Pulm Pharmacol
Ther. 39:1–6. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Gralinski LE, Sheahan TP, Morrison TE,
Menachery VD, Jensen K, Leist SR, Whitmore A, Heise MT and Baric
RS: Complement activation contributes to severe acute respiratory
syndrome coronavirus pathogenesis. mBio. 9:e01753–18. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Mastellos DC, Ricklin D and Lambris JD:
Clinical promise of next-generation complement therapeutics. Nat
Rev Drug Discov. 18:707–729. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Hadanny A, Rittblat M, Bitterman M,
May-Raz I, Suzin G, Boussi-Gross R, Zemel Y, Bechor Y, Catalogna M
and Efrati S: Hyperbaric oxygen therapy improves neurocognitive
functions of post-stroke patients-a retrospective analysis. Restor
Neurol Neurosci. 38:93–107. 2020.
|
|
84
|
Beyls C, Huette P, Abou-Arab O, Berna P
and Mahjoub Y: Extracorporeal membrane oxygenation for
COVID-19-associated severe acute respiratory distress syndrome and
risk of thrombosis. Br J Anaesth. 125:e260–e262. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Fan H, Zhang L, Huang B, Zhu M, Zhou Y,
Zhang H, Tao X, Cheng S, Yu W, Zhu L and Chen J: Cardiac injuries
in patients with coronavirus disease 2019: Not to be ignored. Inter
J Infect Dis. 96:294–297. 2020. View Article : Google Scholar
|
|
86
|
Zou Y, Guo H, Zhang Y, Zhang Z, Liu Y,
Wang J, Lu H and Qian Z: Analysis of coagulation parameters in
patients with COVID-19 in Shanghai, China. Biosci Trends.
14:285–289. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Fogarty H, Townsend L, Ni Cheallaigh C,
Bergin C, Martin-Loeches I, Browne P, Bacon CL, Gaule R, Gillett A,
Byrne M, et al: COVID19 coagulopathy in Caucasian patients. Br J
Haematol. 189:1044–1049. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirus in Wuhan, China. Lancet.
395:497–506. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S,
Huang H, Zhang L, Zhou X, Du C, et al: Risk factors associated with
acute respiratory distress syndrome and death in patients with
coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern
Med. 180:934–943. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Cui S, Chen S, Li X, Liu S and Wang F:
Prevalence of venous thromboembolism in patients with severe novel
coronavirus pneumonia. J Thromb Haemost. 18:1421–1424. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Stoneham SM, Milne KM, Nuttall E, Frew GH,
Sturrock BR, Sivaloganathan H, Ladikou EE, Drage S, Phillips B,
Chevassut TJ and Eziefula AC: Thrombotic risk in COVID-19: A case
series and case-control study. Clin Med (Lond). 20:e76–e81. 2020.
View Article : Google Scholar
|
|
92
|
Léonard-Lorant I, Delabranche X, Séverac
F, Helms J, Pauzet C, Collange O, Schneider F, Labani A, Bilbault
P, Molière S, et al: Acute pulmonary embolism in COVID-19 patients
on CT angiography and relationship to D-Dimer levels. Radiology.
296:E189–E191. 2020. View Article : Google Scholar
|
|
93
|
Llitjos JF, Leclerc M, Chochois C,
Monsallier JM, Ramakers M, Auvray M and Merouani K: High incidence
of venous thromboembolic events in anticoagulated severe COVID-19
patients. J Thromb Haemost. 18:1743–1746. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Poillon G, Obadia M, Perrin M, Savatovsky
J and Lecler A: Cerebral venous thrombosis associated with COVID-19
infection: Causality or coincidence? J Neuroradiol.
S0150-986:30167–X. 2020.
|
|
95
|
Paranjpe I, Fuster V, Lala A, Russak AJ,
Glicksberg BS, Levin MA, Charney AW, Narula J, Fayad ZA, Bagiella
E, et al: Association of treatment dose anticoagulation with
in-hospital survival among hospitalized patients with COVID-19. J
Am Coll Cardiol. 76:122–124. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
White D, MacDonald S, Bull T, Hayman M, de
Monteverde-Robb R, Sapsford D, Lavinio A, Varley J, Johnston A,
Besser M and Thomas W: Heparin resistance in COVID-19 patients in
the intensive care unit. J Thromb Thrombolysis. 50:287–291. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Arachchillage DJ, Remmington C, Rosenberg
A, Xu T, Passariello M, Hall D, Laffan M and Patel BV:
Anticoagulation with argatroban in patients with acute antithrombin
deficiency in severe COVID-19. Br J Haematol. 190:e286–e288. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Ranucci M, Ballotta A, Di Dedda U,
Bayshnikova E, Dei Poli M, Resta M, Falco M, Albano G and Menicanti
L: The procoagulant pattern of patients with COVID-19 acute
respiratory distress syndrome. J Thromb Haemost. 18:1747–1751.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Thachil J, Tang N, Gando S, Falanga A,
Cattaneo M, Levi M, Clark C and Iba T: ISTH interim guidance on
recognition and management of coagulopathy in COVID-19. J Thromb
Haemost. 18:1023–1026. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Connors JM and Levy JH: COVID-19 and its
implications for thrombosis and anticoagulation. Blood.
135:2033–2040. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Thachil J, Tang N, Gando S, Falanga A,
Cattaneo M, Levi M, Clark C and Iba T: DOACs and 'newer'
haemophilia therapies in COVID-19. J Thromb Haemost. 18:1795–1796.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Bikdeli B, Madhavan MV, Gupta A, Jimenez
D, Burton JR, Der Nigoghossian C, Chuich T, Nouri SN, Dreyfus I,
Driggin E, et al: Pharmacological agents targeting
thromboinflammation in COVID-19: Review and implications for future
research. Thromb Haemost. 120:1004–1023. 2020. View Article : Google Scholar : PubMed/NCBI
|