Introduction
Cardiovascular disease (CVD) remains the leading
cause of mortality worldwide, accounting for ~18 million deaths
annually (1,2). This broad category includes
coronary artery disease, myocardial infarction (MI),
cerebrovascular disease (stroke), heart failure (HF) and valvular
disorders, all of which impose health and economic burdens
(3). Despite advances in
pharmacological therapies and interventional procedures (stents,
bypass surgery and mechanical valves), conventional treatments
primarily manage symptoms without fully restoring damaged cardiac
tissue. A challenge is that the adult human heart and vasculature
possess limited intrinsic regenerative capacity (4). Following MI, lost cardiac muscle is
replaced by non-contractile fibrotic scar tissue rather than newly
formed myocardium. This impairs cardiac function and often leads to
adverse remodeling and chronic HF (5-7).
Traditional therapies, such as reperfusion through percutaneous
coronary intervention, pharmacotherapy with β-blockers and
angiotensin-converting enzyme (ACE) inhibitors and mechanical
circulatory support devices, improve acute survival but do not
restore lost myocardium (8).
Heart transplantation remains the gold-standard treatment for
end-stage HF, however, it is limited by donor organ scarcity
(9,10). In vascular disease, interventions
such as angioplasty and surgery address occluded arteries but
typically fail to regenerate a functional endothelium or prevent
long-term restenosis (5).
Prosthetic heart valves and vascular grafts are lifesaving,
however, artificial materials may provoke thrombosis, necessitate
lifelong anticoagulation or cannot accommodate somatic growth
(7). There is a pressing need
for novel therapeutic strategies that repair or regenerate
cardiovascular tissue rather than merely treat symptoms.
To overcome these limitations in cardiac repair,
strategies derived from tissue engineering and regenerative
medicine have been developed (11). Hydrogels are biocompatible
three-dimensional (3D) networks composed of hydrophilic polymers,
characterized by their capacity to retain water, which results in a
soft, tissue-mimicking material (12-14). Through adjustment of their
composition and structural properties, hydrogels can be engineered
to replicate the native extracellular matrix (ECM), including its
key characteristics (high water content, biocompatibility and
elasticity), thereby providing support for cell differentiation and
maturation (15-17). Unlike rigid permanent implants,
hydrogels are typically biodegradable, which allows them to
integrate into host tissue and be replaced by native tissue. Early
generations of hydrogels [polyacrylamide or poly(2-hydroxyethyl
methacrylate) (HEMA) gels] were used in medicine as passive
materials, such as contact lenses and wound dressings, however,
other functional hydrogels extend beyond passive roles (13,14). These advanced hydrogels are
bioactive or stimuli-responsive and are designed to interact with
the biological environment in specific ways, such as delivering
drugs or cells, responding to local stimuli (pH, enzymes or
temperature) to release therapeutic agents or presenting
biochemical cues that direct cell behavior (18). Functional hydrogels can serve as
injectable scaffolds to repair infarcted myocardium, as coatings
for stents or grafts to improve performance or as engineered tissue
constructs (patches, valves or vessels) that integrate with host
tissue. Because hydrogels are typically minimally invasive
(injectable or catheter-deliverable) and highly tunable (their
mechanical properties, degradation kinetics and biofunctionality
can be precisely controlled through material design), they offer
unique solutions to challenges that traditional rigid implants or
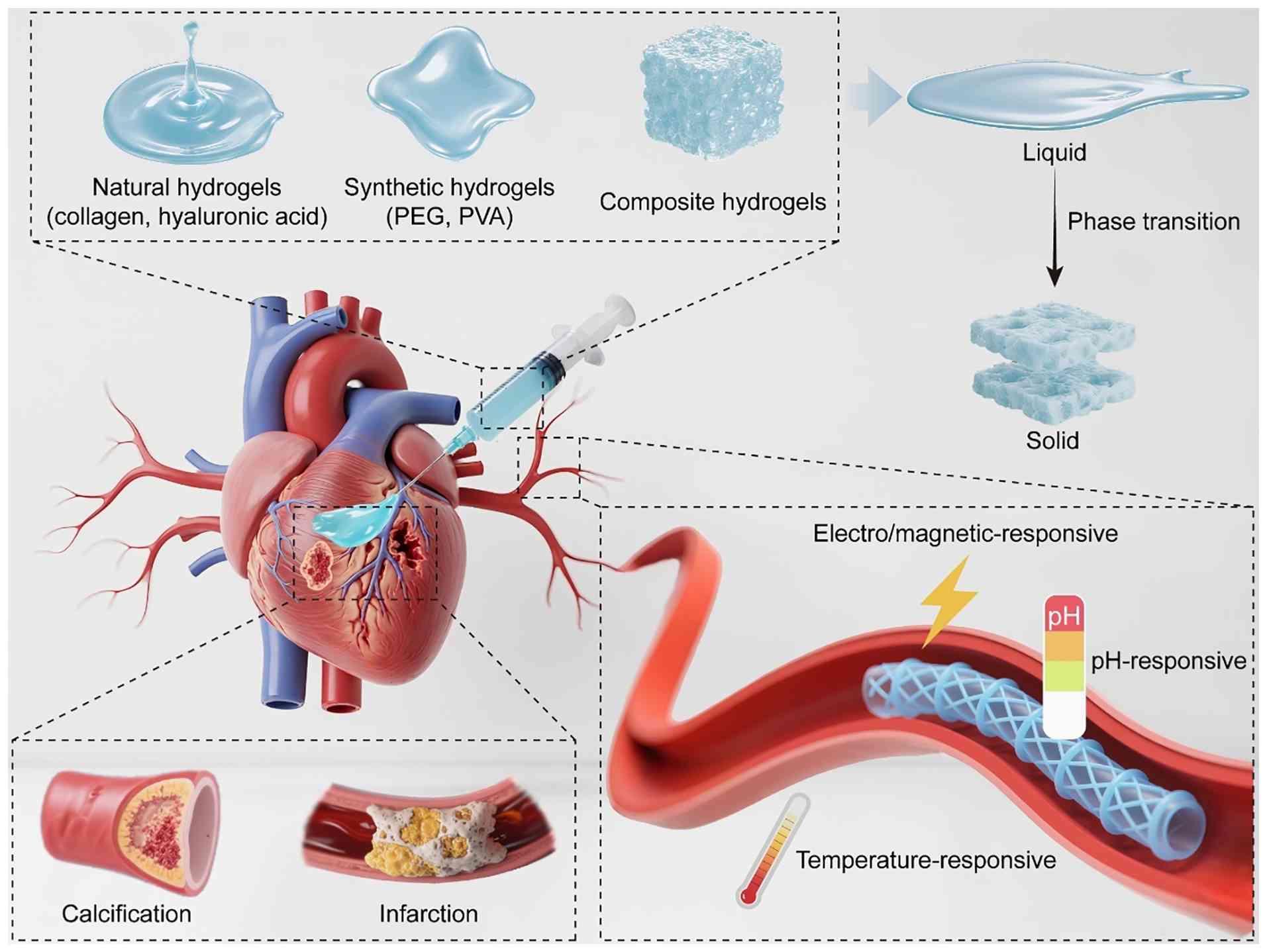
systemic drug therapy cannot adequately address (19). The present study aimed to
summarize the fabrication of functional hydrogels, along with their
intrinsic properties and therapeutic applications in CVD, the
current challenges in this field and future research directions. A
schematic overview of the synthesis and applications of functional
hydrogels in cardiovascular therapy is illustrated in Fig. 1.
Fabrication of functional hydrogels
Hydrogels used in cardiovascular applications are
formulated from a wide variety of polymers, which are broadly
classified as natural, synthetic or composite materials (20,21). Hydrogels consist of crosslinked
polymer chains that form a water-swollen network; natural polymers
offer good biocompatibility and bioactivity, synthetic polymers
provide tunable mechanical properties and reproducibility and
composite systems combine these advantages (22). Hybrid approaches and
stimuli-responsive designs are employed to achieve optimal
performance (12).
Hydrogels from natural polymers
Natural polymer hydrogels are derived from
biological macromolecules and typically resemble the composition of
the native ECM. Examples include proteins (collagen, gelatin,
fibrin and keratin) and polysaccharides [hyaluronic acid (HA),
alginate, chitosan and agarose] (23-27). These materials intrinsically
mimic the native matrix by providing ligands for cell adhesion and
enzymatic degradation sites that facilitate tissue remodeling.
Natural hydrogels are typically biocompatible and bioactive,
meaning that cells recognize and interact with them favorably.
However, they typically exhibit inferior mechanical strength
(compared with synthetic hydrogels), batch-to-batch variability and
a risk of immunogenicity if not adequately purified.
Proteins
Collagen type I, the most abundant protein in the
mammalian ECM, is found in skin, bone, tendon and myocardium and
readily forms hydrogels through the self-assembly of its
triple-helical monomers. Collagen gels exhibit intrinsic
cell-binding motifs and undergo degradation by collagenase, which
makes them cytocompatible. They have been used in tissue
engineering and 3D cell culture (19). However, their limitations include
low stiffness and the potential for xenogeneic immune responses
unless properly processed (decellularization or pepsin digestion to
decrease antigenicity) (19).
Chemical cross-linkers (such as glutaraldehyde) can reinforce
collagen gels, although this may compromise biocompatibility
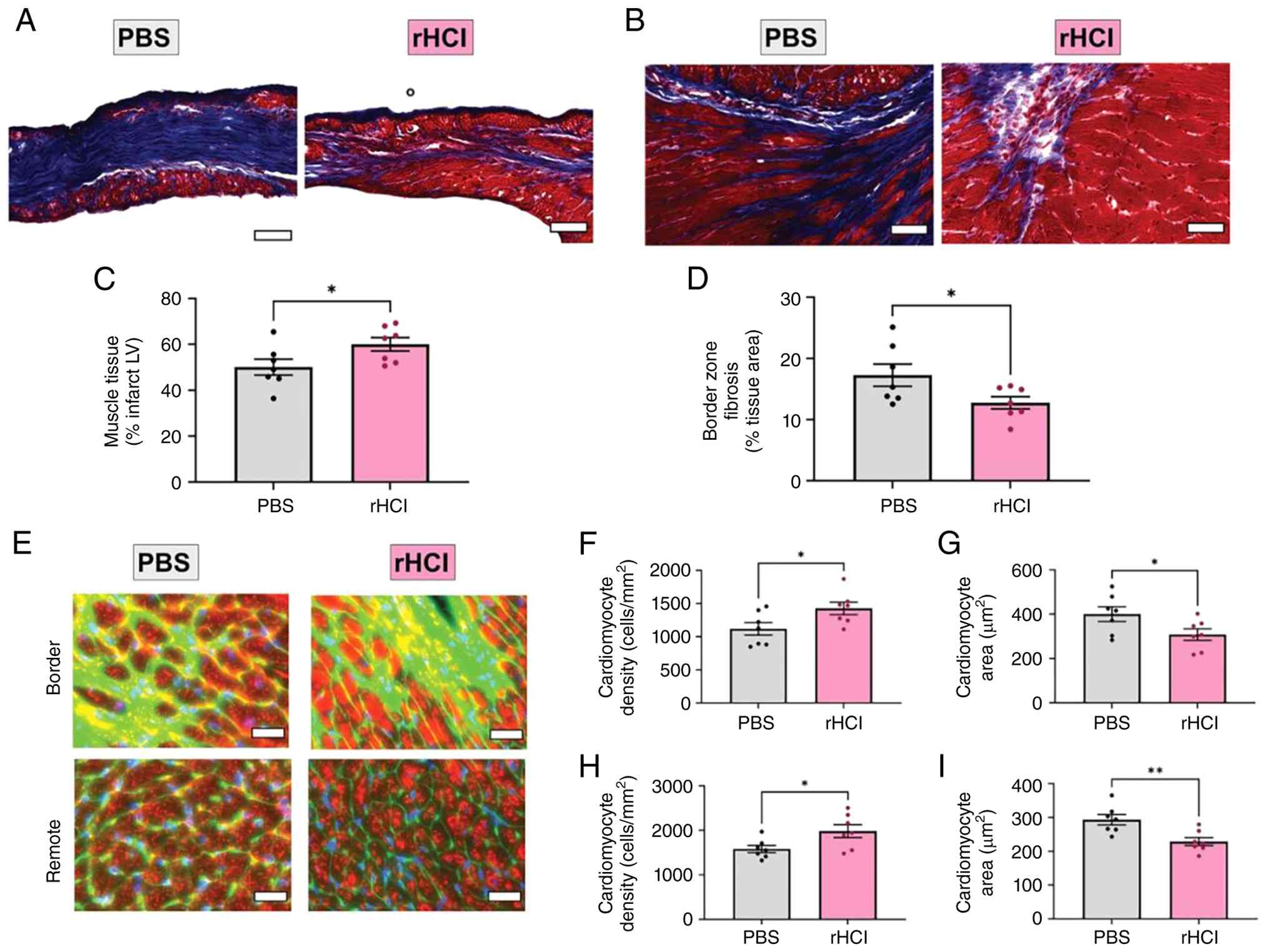
(5). Collagen hydrogels have
demonstrated efficacy in cardiac repair. McLaughlin et al
(28) demonstrated that collagen
hydrogel treatment decreases methylglyoxal adduct formation within
cardiomyocytes and enhances contractile function in the infarct
border zone in a mouse model of MI (Fig. 2A-D). Histological analysis has
revealed increased myocardial salvage and reduced fibrosis in the
border zone (Fig. 2E-I)
(28). Gelatin is a denatured
form of collagen produced through partial hydrolysis. It retains
numerous collagen bioactive sequences but is easier to handle
because it forms gels upon cooling, a property known as thermal
reversibility (13). Gelatin
hydrogels are biocompatible and can be formulated to deliver growth
factors. For example, heparin-binding growth factors can be
incorporated to promote vascularization in engineered tissue
(11). Because gelatin is
derived from collagen, it represents a promising material for
cardiac repair. Although its mechanical strength is limited,
gelatin is typically chemically modified (for example, gelatin
methacrylate) to enable cross-linking and enhance mechanical
rigidity (13).
Fibrin is a natural clotting polymer formed through
thrombin-mediated cleavage of fibrinogen. Fibrin gels polymerize
rapidly at physiological temperature and can be obtained
autologously from the patient blood plasma (5). They support cell infiltration and
ECM deposition because fibrinolytic enzymes degrade the gel
(29,30). Fibrin has clinical applications
as a surgical sealant (11).
Fibrin injection into infarcted rat hearts enhances cell
engraftment and myocardial perfusion, resulting in smaller infarct
size and improved cardiac output (31). However, fibrin has limitations,
including rapid degradation and relatively weak mechanical
strength; therefore, it may not provide sustained structural
support unless reinforced or combined with other materials
(30). Nonetheless, fibrin
exhibits good biocompatibility, as it mimics the native
wound-healing process. Fibrin-based heart valve scaffolds generated
through injection molding of cell-laden fibrin have also been
investigated (15).
Polysaccharides
HA is a glycosaminoglycan that is abundant in
connective tissue and heart valves. HA hydrogels are enzymatically
degradable by hyaluronidase and are non-immunogenic because HA is a
natural component of the human ECM. However, unmodified HA is
mechanically weak and fragile, necessitating chemical modification
(such as methacrylation or thiol modification) or cross-linking to
achieve sufficient mechanical stability for cardiovascular
application (13). HA has been
well-documented to contribute to wound healing and angiogenesis
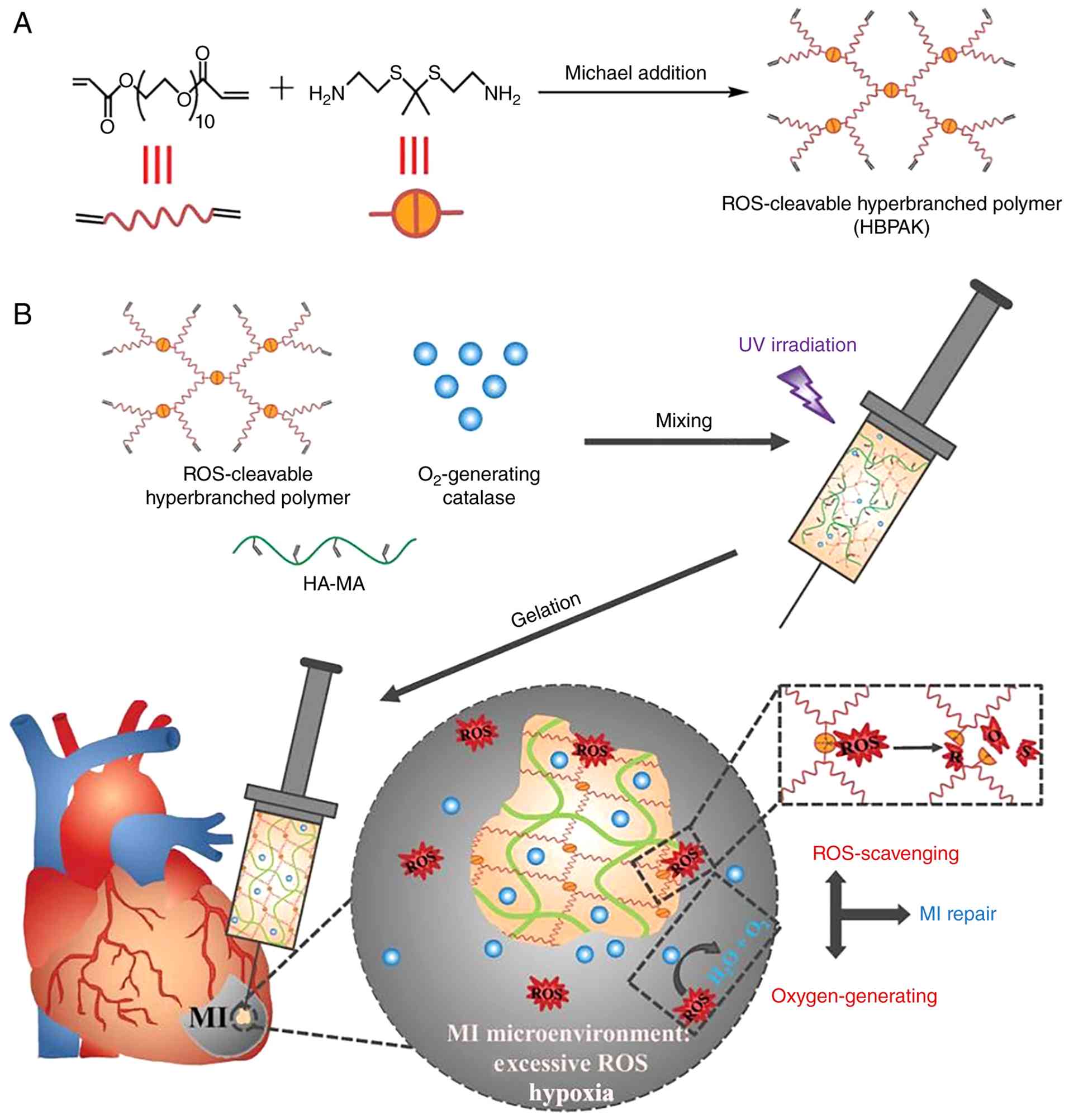
(14,18,32). Ding et al (32) developed an injectable hydrogel
based on methacrylate-modified HA, which rapidly gels following
ultraviolet irradiation via the Michael addition reaction (Fig. 3A). The aforementioned study
demonstrated that this hydrogel suppresses cell apoptosis,
increases the M2-to-M1 macrophage ratio, promotes angiogenesis,
decreases infarct size and improves cardiac function (Fig. 3B) (32). In another study, application of a
cross-linked HA patch to the heart increased ventricular wall
thickness and vascular formation, highlighting the potential of HA
hydrogels in cardiac regeneration (11).
Alginate, a polysaccharide derived from seaweed,
forms hydrogels through ionic cross-linking with divalent cations
(such as Ca2+). Alginate hydrogels are biocompatible,
inexpensive and readily gel in situ by injection of a
soluble alginate solution followed by a calcium-containing solution
(33). They are non-immunogenic
and non-thrombogenic, and their mild gelation conditions, along
with the ease of encapsulating cells or drugs, make them suitable
for cardiovascular application (33,34). Unmodified alginate is not
enzymatically degraded in humans; the gels gradually dissociate
through ion exchange of Ca2+ with the surrounding
environment, which may compromise long-term stability. To address
this limitation, alginates are partially oxidized to enable slow
hydrolytic degradation or covalently cross-linked to enhance
structural stability (34). Lee
et al (35) presented
findings from the first clinical trial evaluating the feasibility
and safety of Algisyl-LVR™, a hydrogel composed of sodium and
calcium alginate (LoneStar Heart Inc.), for the treatment of HF
associated with dilated cardiomyopathy. During injection,
mechanical stress disrupts the dynamic cross-links formed via
Ca2+ coordination, causing the hydrogel to transition
into a liquid state that facilitates catheter delivery. Once
injected into the myocardium, the stress is relieved, and dynamic
cross-linking is re-established (35).
Chitosan is derived from chitin, which is found in
crustacean shells, through deacetylation. It is a cationic
polysaccharide that forms hydrogels via ionically triggered
gelation when mixed with β-glycerophosphate. Chitosan structure
resembles that of glycosaminoglycans and it is biocompatible, with
mild antibacterial properties. It dissolves in acidic solutions and
forms gel as the pH or the temperature rises (36). For cardiac applications,
thermosensitive chitosan hydrogels (liquid formulations that remain
injectable at room temperature but solidify into a gel at body
temperature) are particularly attractive because they can be
delivered by catheter (36).
Chitosan can be chemically modified [by conjugation with
arginine-glycine-aspartic acid (RGD) peptides or growth factors] to
enhance cell adhesion and therapeutic efficacy (12).
Other natural materials
Several other natural materials have niche
applications. Agarose, an algae-derived polysaccharide, forms gels
upon cooling, and its pore size is altered by adjusting agarose
concentration. Agarose is used as a cell-encapsulation matrix and
for drug delivery (13). Kim
et al (37) developed a
low gel temperature agarose by incorporating β-cyclodextrin into
ethylenediamine-modified agarose and demonstrated that this
modified gel enables sustained release of a thermosensitive drug.
Keratin-based hydrogels, derived from hair or wool proteins,
leverage keratin self-assembling fibrous structure. They retain
bioactive motifs associated with hair follicle development and
demonstrate pro-angiogenic effects without eliciting inflammation.
Matrigel, a complex ECM extract derived from tumor cells, has been
used as an injectable scaffold for stem cell delivery to the heart
(19). Studies (17,18) have shown that it preserves
ventricular geometry and enhances vascularization. However,
Matrigel non-human origin and batch-to-batch variability preclude
its clinical use.
Overall, natural hydrogels typically exhibit
excellent bioactivity and cytocompatibility because their
biochemical components resemble those of native tissue (15). Cells typically attach, migrate
and function more readily on natural matrices. For example, a
collagen or fibrin patch applied to an infarct can recruit cells
and support novel tissue formation more effectively than numerous
synthetic materials (3).
However, purely natural hydrogels often possess limited mechanical
strength and structural stability. They tend to be soft and prone
to rapid degradation. In a beating heart or a high-pressure artery,
a mechanically weak hydrogel may not withstand physiological forces
over time (5). Thus, although
natural polymers establish a biologically favorable
microenvironment, they typically require modification or
reinforcement for load-bearing cardiovascular applications.
Synthetic polymer hydrogels
Synthetic hydrogels are formed from synthetic
polymers such as poly(ethylene glycol) (PEG), poly(vinyl alcohol)
(PVA) and polyacrylate (38-40). A key advantage of synthetic
polymers is their tunability and reproducibility: Molecular weight,
cross-link density and chemical functional groups can be precisely
controlled, resulting in consistent batch-to-batch properties
(5,15). Synthetic hydrogels can be
engineered to exhibit a range of stiffness, degradation rate and
network architectures to meet specific application requirements.
They also tend to be chemically inert and non-immunogenic in their
pure form. However, unlike natural polymers, most synthetic
polymers lack inherent bioactive cues; cells do not readily
recognize or adhere to them (13). Therefore, biofunctionalization is
typically required. For example, peptides such as RGD can be
grafted onto synthetic polymer backbones to promote cell adhesion
(13).
PEG
PEG, also known as poly(ethylene oxide), is a
hydrophilic polymer approved by the U.S Food and Drug
Administration (FDA) for medical applications (41). It resists protein adsorption and
is typically biologically inert, which decreases non-specific
immune reactions. PEG hydrogels are typically formed by
cross-linking multi-armed PEG molecules functionalized with
acrylates, thiols or other reactive groups to generate a polymeric
network. By adjusting PEG molecular weight or incorporating
degradable linkers, such as ester bonds or peptide sequences,
between PEG chains, the mechanical strength and degradation rate of
the gel can be controlled (5). A
notable advantage of PEG lies in its tunable architecture and
well-defined chemical composition. Researchers engineer PEG
hydrogels with specific pore sizes, stiffness and gelation
kinetics. In its unmodified form, PEG does not support cell
adhesion; cells typically remain rounded in pure PEG hydrogels.
However, incorporation of ECM motifs (RGD peptides or heparin to
facilitate growth factor binding) enables PEG hydrogels to become
bioactive (5). In cardiac tissue
engineering, PEG-based hydrogels have been investigated as
scaffolds for engineered heart valves and cell delivery. Crocini
et al (42) employed
photo-clickable thiol-ene PEG hydrogels for 3D cell culture of
adult mouse cardiomyocytes. These PEG hydrogels serve as versatile
and biocompatible scaffolding materials, with precisely adjustable
stiffness that enables them to mimic both physiological and
pathological microenvironmental conditions. Compared with
conventional cell culture systems, adult cardiomyocytes
encapsulated within PEG hydrogels exhibit prolonged survival and
preserved the integrity of their sarcomeric and T-tubular
structures (42). The mechanical
properties of PEG hydrogels are tunable, allowing formulations that
are very soft for injectable applications or more rigid and
elastomeric for load-bearing cardiac patches (43). Moreover, PEG can be combined with
natural polymers (for example, through PEGylation of proteins such
as fibrin or collagen) to create composite hydrogels that retain
bioactivity while improving structural stability (5).
PVA
PVA is a synthetic, water-soluble polymer that forms
hydrogels, typically through repeated freeze-thaw cycles or
chemical cross-linking (40). It
produces transparent, rubber-like hydrogels with good mechanical
integrity and was among the earliest hydrogel materials used in
medicine. PVA hydrogels are biologically inert, and few cells
adhere to them without modification, however, they are non-toxic
and chemically stable (22). PVA
is used in cardiac applications, including the fabrication of heart
valve leaflet models and vascular graft coatings, because of its
flexibility and mechanical strength. Recent studies have developed
nanocomposite PVA hydrogels reinforced with nanoparticles or
nanofibers to enhance mechanical performance (41,44). Although unmodified PVA lacks
cell-instructive cues, it can be functionalized (with gelatin or
RGD peptides) to improve cell-material interactions (5). Mannarino et al (44) developed a composite hydrogel
consisting of PVA coated with poly(acrylic acid) (PAA), which was
subjected to heat treatment to form a physically cross-linked
network. The mechanical properties and swelling behavior of the
hydrogel are modulated by adjusting the heat input and duration of
thermal exposure, thereby increasing the cross-link density of the
matrix. In an in vitro study using a simulated aging model
over 162.6 days, the composite hydrogel retained its mechanical
properties and surface functionality following accelerated aging.
When evaluated in an in vitro blood loop model, the PVA/PAA
composite hydrogel exhibited a 97% decrease in platelet adhesion
(44). Additionally, it
demonstrated a slower thrombosis-induced occlusion rate at the
catheter tip, in contrast to commercially available catheter
products. Ultimately, this thromboresistant hydrogel shows
potential as a biomaterial for vascular access application, with
the goal of improving patient outcomes. PVA hydrogels can be loaded
with drugs or growth factors and have been investigated as
drug-eluting coatings for stents or cardiac implants (45,46). Hu et al (47) developed an injectable hydrogel
composed of phenylboronic acid-grafted carboxymethyl cellulose and
PVA for the localized delivery of curcumin and recombinant human
collagen type III to the infarcted myocardium in a rat MI model.
This hydrogel improves cardiac function, increases left ventricular
(LV) wall thickness, decreases infarct size, attenuates
cardiomyocyte apoptosis and decreases inflammation.
Polyacrylates and poly(HEMA)
Hydrogels based on PAA or poly(HEMA) are classical
synthetic materials that have been widely used in contact lenses
and biomedical implants. PAA is hydrophilic and pH-responsive,
exhibiting increased swelling at higher pH due to deprotonation of
its carboxyl groups; this property has been exploited in drug
delivery systems (36). Although
these polymers are not commonly used alone in cardiac tissue
engineering because of their limited bioactivity, they demonstrate
the concept of stimuli-responsive synthetic hydrogels. By
copolymerizing acrylic monomers with other functional monomers,
responsiveness to pH or temperature can be induced (12). Poly(N-isopropylacrylamide)
(PNIPAM) is a synthetic polymer that undergoes a thermal phase
transition at ~32°C. It is soluble below this temperature and forms
a gel above it (13).
PNIPAM-based hydrogels are used to develop injectable systems that
solidify at body temperature, conceptually similar to the
chitosan/β-glycerophosphate system but fully synthetic. One
limitation of PNIPAM is that its degradation products, if the
polymer is not fully cross-linked, exhibit limited
biocompatibility; therefore, PNIPAM is often combined with
biodegradable segments or formulated as microgels to minimize
potential accumulation (13).
Self-assembling peptides and other
polymers
Certain synthetic hydrogels bridge the distinction
between natural and synthetic. For example, peptide-based hydrogels
are fabricated from short synthetic peptides that spontaneously
self-assemble into fibrous networks (such as the RADARADARADARADA
peptide forms a β-sheet hydrogel) (13). Although these materials are
synthetic in origin, they are biological in composition because
they consist of amino acids. They have been investigated for
myocardial repair because they present a nanofibrous architecture
resembling collagen and incorporate bioactive sequences (5). Polyphosphazenes, a class of
inorganic-organic polymers, can be engineered to be biodegradable
and have been evaluated as hydrogel matrices for tissue
engineering. Polyurethane and polyester urethane hybrids have also
been formulated as hydrogels, referred to as elastic hydrogels, to
provide rubber-like elasticity for cardiac patches. Synthetic
systems offers advantages, such as electrical conductivity when
doped with conductive polymers or high toughness in double-network
hydrogels composed of two interpenetrating polymer networks
(12).
In general, synthetic hydrogels provide greater
control over material properties and typically exhibit superior
mechanical robustness compared with natural hydrogels. They do not
inherently support cell attachment or tissue integration, however,
this limitation can be addressed through composite design (blending
synthetic and natural polymers) or by conjugating bioactive
molecules (5). Numerous
contemporary hydrogel systems are hybrid in composition. For
example, a PEG backbone can be functionalized with cell-adhesive
peptides or combined with collagen or chondroitin sulfate (48). Such composite hydrogels aim to
integrate the biofunctionality of the native ECM with the
mechanical tunability of synthetic polymers. An example is
PEGylated fibrin or PEG-collagen composites, in which the synthetic
component slows degradation and increases mechanical strength,
whereas the natural component preserves cytocompatibility (49,50). Table I summarizes key differences
between natural and synthetic hydrogel materials in cardiovascular
therapy.
 | Table INatural and synthetic hydrogels for
cardiovascular application. |
Table I
Natural and synthetic hydrogels for
cardiovascular application.
| Hydrogel
source | Primary
components | Strengths | Limitations | Degradation
rate | Clinical
translation status | Uses in CVD |
|---|
|
Natural-derived | Collagen, gelatin,
fibrin, hyaluronic acid, alginate, chitosan | Biocompatible;
inherent cell adhesion ligands and enzymatic degradability; promote
cell functions (migration, angiogenesis) | Lower mechanical
strength without reinforcement; batch variability (derived from
tissue); risk of immunogenicity if xenogeneic | Enzymatic
(collagenase, hyaluronidase, plasmin); typically weeks to
months | Phase I/II
(alginate, ECM hydrogels); preclinical | Collagen/gelatin
for cardiac patches; fibrin for cell delivery in MI; alginate
injectables for MI and HF; HA in tissue-engineered valves |
|
Synthetic-derived | PEG, PVA,
poly(acrylates), PNIPAM | Highly tunable
mechanical and chemical properties; reproducible and pure
(manufactured under controlled conditions); generally
non-immunogenic | Bio-inert (lack
cell recognition sites); hydrophobic degradation byproducts
possible depending on polymer (acidic monomers) | Hydrolytic or via
engineered cleavable linkers; months to years | Mostly preclinical;
PEG-based devices approved for other indications; PVA in clinical
use as coatings | PEG-based
injectable hydrogels for MI and heart valves; PVA scaffolds for
small-diameter vascular grafts; PNIPAM thermo-gels for minimally
invasive delivery |
|
Composite/hybrid | PEG-collagen
conjugates, fibrin + synthetic polymer interpenetrating
network | Improved mechanics
and stability; preserved bioactivity; versatile design to meet
complex requirements (mechanical strength and biological
function) | More complex to
manufacture (multiple components); need to balance degradation
rates of each component; regulatory approval can be harder for
multi-component products | Tunable via
component ratios; typically weeks to months | Preclinical; early
clinical (cell-loaded composites) | PEGylated collagen
hydrogels for valve engineering (retain collagen biofunction, added
strength); collagen-chitosan blends for cardiac patches (enhanced
mechanical integrity) |
Composite and stimuli-responsive
hydrogels
A trend in hydrogel research is the development of
stimuli-responsive (smart) hydrogels that undergo physicochemical
changes in response to specific environmental triggers (5,13,16). In cardiovascular therapy, dynamic
behavior is desirable because it enables minimally invasive
delivery, on-demand drug release and adaptation to the changing
post-infarction microenvironment (11). For example, a hydrogel may remain
in a liquid state during injection but undergo gelation within the
warm myocardium, or a drug-loaded matrix may release its
therapeutic payload when it detects elevated levels of inflammatory
cytokines at an injury site. By incorporating stimuli-responsive
components, hydrogels enable on-demand therapeutic delivery and
adapt to patient-specific conditions in real time (5).
Thermo-responsive hydrogels
Thermo-responsive hydrogels exploit the temperature
difference between room temperature during injection and body
temperature during gelation, enabling catheter-based delivery with
rapid in situ gelation. This temperature-triggered
transition allows therapeutic action to be aligned with the acute
to subacute phases of cardiac injury. PNIPAM is a thermo-responsive
polymer that exhibits solution-to-gel (sol-gel) transition at ~32°C
(13). By copolymerizing PNIPAM
with other monomers, the transition temperature is adjusted to
physiological temperature. Other approaches include blending
polymers that undergo temperature-induced assembly, such as
chitosan combined with β-glycerophosphate, which gels upon warming,
or Pluronic F127, a PEG-poly(propylene oxide) block copolymer that
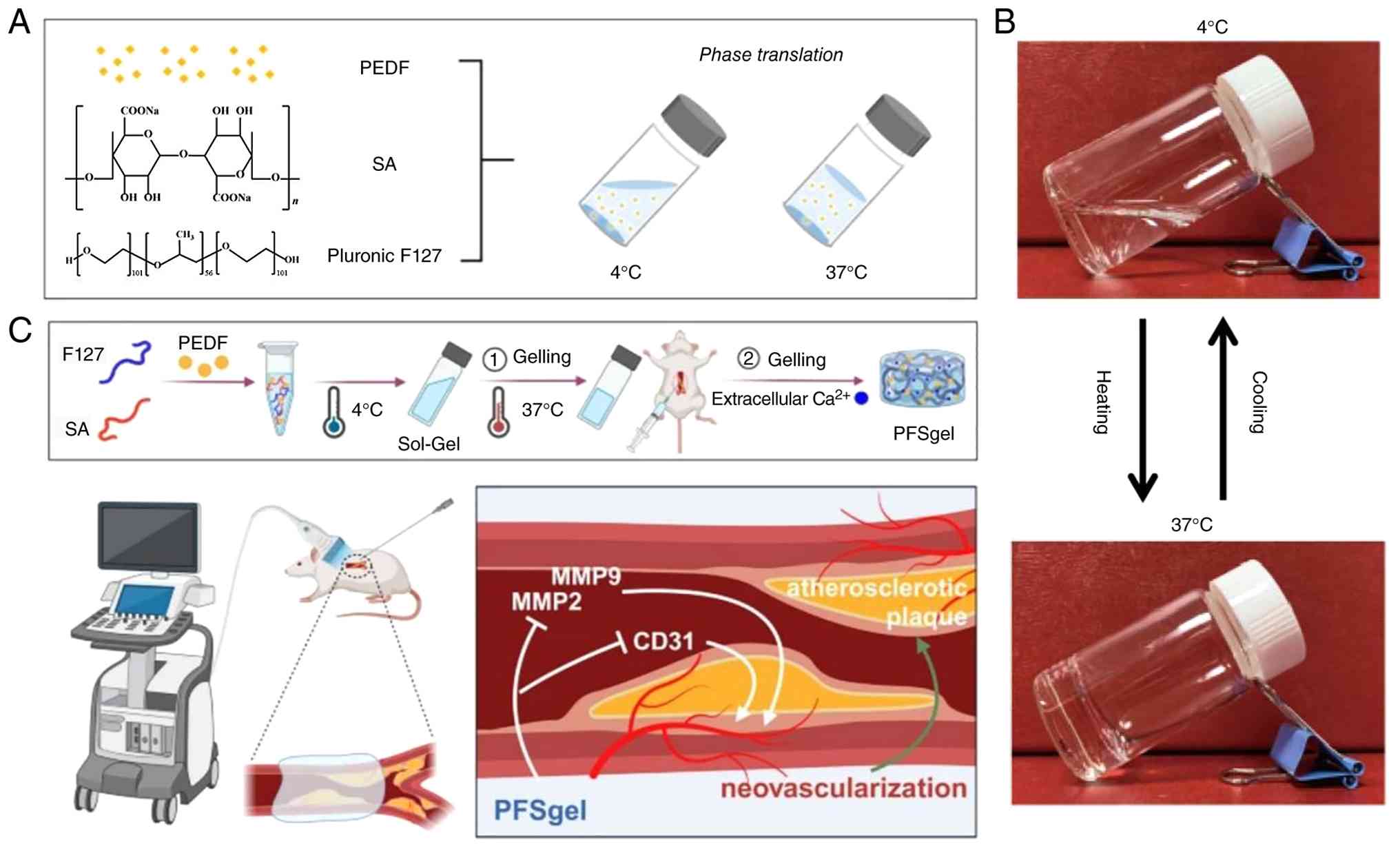
is liquid at low temperature and forms a gel at ~37°C. Duan et
al (51) prepared a
thermosensitive injectable hydrogel (PFSgel) synthesized from
Pluronic F127 and sodium alginate (Fig. 4A). The poloxamer-alginate blend
exists as a liquid solution) at room temperature and undergoes
gelation in vivo (Fig.
4C). When loaded with PEDF and injected around an
atherosclerotic arterial lesion, it forms a local depot that
gradually releases the therapeutic agent and decreases plaque
neovascularization and progression in mice by inhibiting MMP2/MMP9
and CD31 signaling pathways (Fig.
4B).
A thermo-responsive PLEL triblock copolymer hydrogel
has also been developed that undergoes rapid sol-gel transition at
body temperature. When sprayed or injected onto the injured
epicardial surface, it forms a conformal and fouling-resistant
barrier that prevents postoperative cardiac adhesion during the
critical early healing phase (52). Another thermo-responsive system
based on Pluronic F127 has been engineered to encapsulate
HA-modified zeolitic imidazolate framework-8 nanoparticles loaded
with shikonin/Cu2+ complexes, enabling sustained drug
retention at the myocardial injection site following
ischemia-reperfusion injury (53).
pH-responsive hydrogels
Following MI, sustained ischemia and hypoxia lead to
a decrease in local pH, creating a spatially and temporally defined
acidic microenvironment that evolves with disease progression
(6). pH-responsive hydrogels
exploit this dynamic change to achieve targeted, stage-specific
therapeutic delivery (3) PAA
hydrogels exhibit increased swelling at neutral-to-basic pH because
deprotonated carboxylate groups repel one another. In CVD, this
pH-responsive behavior can be harnessed because ischemic tissue
typically becomes acidic (3).
Alimirzaei et al (54)
reported the fabrication of two pH-sensitive chitosan hydrogels and
evaluated them as cell carriers and cardiac scaffold materials for
infarcted myocardial regeneration. An injectable pH-responsive
micellar system has been developed by encapsulating a
small-molecule glycogen synthase kinase-3β inhibitor
[(2'Z,3'E)-6-bromoindirubin-3'-oxime(BIO) within a
PEG-polycaprolactone (PCL) matrix and integrating it with
adipose-derived stem cells in Matrigel (55). Under acidic conditions simulating
the post-MI microenvironment, micelles undergo accelerated
degradation, triggering BIO release and mitigating reactive oxygen
species (ROS)-induced injury (55). A pH-responsive conductive
hydrogel composed of PVA, oxidized sodium alginate, borax, tannic
acid and a vanadium-based MXene (a class of 2D transition metal
carbides/nitrides) nanozyme has also been engineered. Under acidic
conditions that mimic the ischemic microenvironment, the hydrogel
exhibits enhanced nicotinamide adenine dinucleotide (NADH)
oxidation activity, enabling sustained release of the nanozyme and
restoration of the NAD+/NADH redox balance (56).
Enzyme-responsive hydrogels
MMPs, particularly MMP-2 and MMP-9, are notably
upregulated in the infarcted myocardium during the inflammatory and
early remodeling phases. Their expression peaks within days after
injury and declines as healing progresses. This positions MMPs as
ideal endogenous triggers for on-demand therapeutic delivery
aligned with the dynamic requirements of cardiac repair (57). Researchers have designed
hydrogels containing cross-links cleavable by MMP-2 or MMP-9, which
are abundant proteases in post-MI tissue (13,57,58). Such MMP-responsive hydrogels
degrade in synchrony with the remodeling process, potentially
releasing embedded therapeutics, such as growth factors or
antifibrotic agents, at sites where MMP activity is elevated
(57,58). Pereira et al (59) employed a biscysteine
MMP-cleavable peptide as a cross-linking agent and fabricated a
pectin-based hydrogel via a photo-click reaction: The fabricated
hydrogel degraded in the presence of type II collagenase,
suggesting its potential for in vivo enzymatic degradation
(59). An MMP-2-responsive
cardiac ECM (c-ECM) hydrogel has also been engineered to enable
sequential release of pro-angiogenic and vascular-stabilizing
factors (60). A
collagen-binding vascular endothelial growth factor (VEGF) is
incorporated directly into the c-ECM matrix, whereas an
angiopoietin-1 (Ang-1) mimetic peptide is conjugated through an
MMP-2-cleavable linker (60). As
MMP-2 levels progressively increase, the enzyme cleaves the peptide
linker, releasing the mimetic peptide to promote vascular
maturation. For heart valve applications, an MMP-responsive
hydrogel system encapsulating microRNA-93 (miR-93)-loaded
nanoparticles has been developed. Following MMP-mediated
degradation, the nanoparticles are released and internalized by
infiltrating macrophages, where miR-93 induces M2 polarization and
promotes constructive remodeling of decellularized valve scaffolds
(61).
Electrical, light and magnetic
responsiveness
Because the heart is an electrically active organ,
electro-responsive hydrogels that alter their properties in
response to an applied electric field represent an emerging area of
research (5). Although at an
early stage of development, conductive or piezoelectric hydrogel
composites incorporating graphene, gold nanowires or conductive
polymers such as polypyrrole have been investigated for cardiac
patch applications to enhance electrical signal propagation across
scar tissue (41,43). Light-responsive hydrogels, which
rely on photodegradable linkers or light-induced conformational
changes, are being explored for externally regulated drug release
(5,62). An injectable hydrogel containing
light-sensitive bonds and photodegradable components, composed of
PEG and heparin-derived polymers, effectively encapsulates
fibroblast growth factor-2 (FGF-2) (62). The biological activity of FGF-2
following encapsulation is comparable to that pre-encapsulation and
the hydrogel modulates its release profile. Magnetic
field-responsive hydrogels typically incorporate magnetic
nanoparticles and can be manipulated or heated under an external
magnetic field; such systems may enable targeted thrombosis therapy
or localized hyperthermia for the ablation of atherosclerotic
plaque cells (12).
Composite hydrogels
To harness the strengths of natural and synthetic
components, numerous composite hydrogels have been developed
(13,17). In composite systems, a natural
polymer, living cells or nanoparticles, may be embedded within a
synthetic polymer matrix, or a synthetic component may be
incorporated into a natural matrix (5). This strategy can produce materials
that balance biofunctionality with mechanical robustness (12). For example, combining type I
collagen with glycosaminoglycans or a synthetic polymer such as PEG
can enhance mechanical integrity while preserving cell-supportive
surfaces (16). Composite
hydrogels are applied in heart valve engineering, where a
biological scaffold, such as a decellularized valve matrix, may be
reinforced with a secondary synthetic polymer network to improve
durability (48). In vascular
graft design, the luminal surface of synthetic grafts [expanded
polytetrafluoroethylene (ePTFE) tubes) is coated with a thin
hydrogel layer to create a more biomimetic and endothelial
cell-supportive interface (63).
One study reported the bonding of a hydrogel lining to the interior
of an ePTFE graft, which promotes endothelialization without
compromising mechanical strength (63). Similarly, nanocomposite
hydrogels, in which inorganic nanoparticles or nanofibers are
dispersed within the polymer network, have attracted increasing
attention (64-66). Incorporation of silica
nanoparticles, clay nanosheets or carbon-based nanomaterials
reinforce the hydrogel matrix and, in some cases, introduce
additional functionality such as electrical conductivity or growth
factor binding (13). For
cardiac tissue engineering, embedding electrically conductive
nanomaterials, including graphene, gold nanowires or MXene
nanosheets, within a polymeric gel can generate electroconductive
hydrogels that facilitate electrical signal propagation and may
improve synchronization with myocardial contraction (64). Consequently, the incorporation of
conductive biomaterials is key for enhancing the physiological
relevance of in vitro bioengineered cardiac tissue models.
These composite systems aim to mitigate post-MI arrhythmias by
promoting integration with the cardiac electrical conduction
network (64-66).
Additional stimuli, such as oxidative stress
characterized by elevated ROS levels in infarcted regions and
alterations in mechanical strain associated with changes in loading
conditions, have also been explored (67). Overall, stimuli-responsive
hydrogels introduce an additional functional dimension by enabling
spatiotemporal control of therapeutic activity. By integrating
multiple components or incorporating distinct responsive
mechanisms, these hydrogels concurrently satisfy the mechanical
requirements of cardiac tissue and the biological requirements
necessary to support regeneration (3,11).
Application of functional hydrogels in
CVD
Hydrogels have been applied across cardiovascular
diseases, including MI, heart failure, vascular atherosclerosis and
heart valve disease, typically as components of regenerative
medicine or targeted therapeutic strategies (5,15,31,51).
Treatment of MI
MI, commonly referred to as a heart attack, results
from occlusion of a coronary artery, leading to ischemia and
necrosis of cardiac muscle tissue (68,69). The primary goals of post-MI
therapy are to preserve cardiac function, promote myocardial
regeneration and prevent adverse ventricular remodeling (3,6).
Standard post-MI management, including reperfusion therapy and
pharmacological agents such as ACE inhibitors and β-blockers, aims
to limit infarct size and decrease cardiac workload, however, these
interventions do not restore lost myocardium (7,31). Functional hydrogels have been
investigated as a multifaceted strategy for cardiac repair, serving
as structural scaffolds, therapeutic delivery platforms and
supportive biomaterials that actively promote myocardial
regeneration (5,11).
Injectable hydrogels for cardiac
repair
One of the most direct approaches involves injection
of a hydrogel or hydrogel precursor into the infarcted myocardium,
typically via intracardiac administration, either surgically or
through catheter-based delivery (33). Following administration, the
hydrogel forms a bulking scaffold within the scarred region. This
intervention confers an immediate mechanical benefit by increasing
ventricular wall thickness and decreasing wall stress on the
remaining myocardium. Finite element modeling and preclinical
animal studies have demonstrated that intramyocardial injection of
biomaterials attenuates ventricular dilation and preserves
physiological geometry, thereby improving cardiac pump function
(3). For example, an injectable
HA-based hydrogel with optimized stiffness provides mechanical
support and results in reduced infarct expansion in treated hearts
compared with controls (70).
Beyond passive mechanical reinforcement, injectable hydrogels serve
as 3D scaffolds that permit cell infiltration (13). Ideally, the material undergoes
gradual degradation and is replaced by newly formed tissue, such as
vascularized myocardium, rather than persistent fibrotic scar
tissue (16).
A variety of materials have been evaluated as
injectable cardiac hydrogels. Natural polymers, including collagen,
fibrin and alginate, were among the earliest candidates
investigated (11,17). Collagen injections in animal
models improves cardiac function, potentially by providing a
provisional matrix that facilitates cardiomyocyte alignment and
limits increases in ventricular wall stress (28). Leveraging its capacity to form
stable gels through ionic cross-linking, calcium-cross-linked
alginate injected into rat and porcine MI models increases wall
thickness and improves ejection fraction (EF) (3,34). These effects are attributed to a
combination of mechanical reinforcement and pro-angiogenic
bioactivity. This strategy has progressed to clinical evaluation as
the IK-5001 hydrogel (BioLineRx) (33). In a first-in-human study,
intracoronary administration of this alginate hydrogel shortly
following MI was demonstrated to be feasible and safe (33). Another injectable hydrogel,
VentriGel (Ventrix, Inc), is derived from decellularized porcine
c-ECM (71). It is supplied as a
lyophilized cardiac matrix powder that is reconstituted and
administered as a liquid, followed by in situ gelation
within the myocardium. VentriGel retains native cardiac ECM
biochemical cues and, in preclinical studies, recruits endogenous
cells and promotes novel myocardial tissue formation (19,71). A Phase I clinical trial
evaluating catheter-based delivery of VentriGel in patients
following MI demonstrated safety and preliminary signs of
functional improvement, including increased exercise capacity and
trends toward improved cardiac function, particularly in patients
treated >1 year after MI (71). These findings represent important
translational milestones, demonstrating that catheter-based
hydrogel therapy is feasible and safe in human patients.
Cell delivery and myocardial tissue
engineering
A notable application of hydrogels in MI therapy is
their use as cell delivery vehicles. Numerous cell types, including
mesenchymal stem cells (MSCs), adipose-derived SCs, bone
marrow-derived mononuclear cells, induced pluripotent SC
(iPSC)-derived cardiomyocytes and cardiac progenitor cells, have
been investigated for cardiac regeneration (3). Delivery of these cells within a
hydrogel enhances their retention and survival in the myocardium
compared with injection in saline alone (20). The hostile post-MI
microenvironment, characterized by inflammation, oxidative stress,
and ECM disruption, causes the majority of injected cells to
undergo apoptosis or be rapidly cleared (31). Hydrogels provide a protective and
adhesive microenvironment that promotes cell retention and supports
cell viability. For example, a chitosan-based hydrogel conjugated
with survival-promoting peptides increases the engraftment of
transplanted cardiomyocytes and enhances neovascularization in the
infarcted region (72).
Similarly, fibrin-based patches loaded with SCs demonstrated higher
cell survival rates and greater improvements in cardiac function
compared with cell transplantation alone (24). Hydrogels can be pre-seeded with
cells and implanted as cardiac patches. In this approach, cells are
cultured within or on the hydrogel scaffold in vitro,
typically under dynamic mechanical stimulation to promote tissue
maturation, and the resulting cell-laden construct is surgically
applied to the infarcted myocardium. Such tissue-engineered cardiac
patches, fabricated using scaffolds composed of collagen, fibrin or
synthetic polymers, have demonstrated partial remuscularization of
injured myocardium in animal models (64).
A study (72)
reported the development of a self-healing, electrically conductive
injectable hydrogel based on chitosan-graft-aniline tetramer for
cardiac therapy. Owing to its decreased viscosity under shear
stress, allowing easy injection) and self-healing properties, this
hydrogel enables minimally invasive administration and provides a
protective niche for transplanted cells. In a rat model, it
exhibits favorable injectability, controllable cell release and
complete biodegradation within 45 days, underscoring its potential
as a cell delivery platform for cardiovascular therapy (72).
Growth factor and drug delivery
Hydrogels serve as versatile drug delivery
platforms in the infarcted myocardium. Instead of systemic
administration, therapeutic agents are incorporated into a hydrogel
and delivered locally to the injury site, thereby achieving high
local concentrations while minimizing systemic adverse effects
(3,5). A range of cargos has been
investigated, including small-molecule agents such as
anti-inflammatory and antioxidant compounds, cytokines and growth
factors, nucleic acids and extracellular vesicles (EVs) (11). The structural characteristics of
the hydrogel regulate release kinetics, either through
diffusion-driven release mediated by water uptake and swelling or
through degradation-triggered release mechanisms (57).
Delivery of pro-angiogenic factors to promote
neovascularization within the infarcted region is key for
supporting regenerating myocardium. VEGF and basic FGF (bFGF) are
well-established angiogenic proteins with short biological
half-lives when administered in free form. Encapsulation within a
hydrogel enables sustained release over days to weeks (73). In a representative study, a
fibrin-based hydrogel patch releasing VEGF was applied to infarcted
rat hearts (51). Over a 4 week
period, it increases capillary density in the infarct border zone
and improves cardiac function compared with controls. The hydrogel
ensures prolonged local retention of VEGF, allowing it to exert
therapeutic effects during the key healing phase. Similarly, dual
delivery of an angiogenic peptide,
N-acetyl-serylaspartyl-lysyl-proline (Ac-SDKP) and the chemokine
stromal cell-derived factor-1α (SDF-1α) from an injectable hydrogel
enhances angiogenesis and promotes SC recruitment to the infarcted
myocardium, resulting in decreased infarct size and improved LV
function in a mouse MI model (73,74).
Another strategy involves modulation of
inflammation and prevention of cardiomyocyte death during the acute
phase of MI. Immediately following infarction, waves of
inflammatory cells, including neutrophils and macrophages,
infiltrate the injured myocardium and may cause collateral tissue
damage through oxidative stress and protease release (64). Hydrogels have been loaded with
anti-inflammatory agents, such as IL-10, glucocorticoids or
non-steroidal anti-inflammatory drugs (NSAIDs), to locally
attenuate this inflammatory response. For example, an injectable
peptide hydrogel carrying an NSAID and iron oxide nanoparticles has
been evaluated for targeting macrophages in atherosclerotic cardiac
tissue, demonstrating decreased inflammatory markers and promotion
of a reparative macrophage phenotype (75). In MI, a hydrogel-based platform
may similarly deliver immunomodulatory agents to promote macrophage
polarization from a pro-inflammatory M1 to a pro-reparative M2
phenotype, thereby limiting secondary tissue injury. One approach
incorporates microparticles releasing IL-10 within a cardiac patch,
resulting in decreased fibrosis and improved cardiac function in a
rat MI model (34).
Hydrogels encapsulate antifibrotic or
anti-remodeling agents. During post-infarction healing, excessive
fibrosis and ventricular dilation contribute to progressive cardiac
dysfunction (7). The peptide
Ac-SDKP inhibits cardiac fibroblast activation. Firoozi et
al (76) synthesized a
RADA-SDKP hydrogel composed of a self-assembling gel-forming core
sequence (RADA) and a bioactive motif (SDKP), providing structural
flexibility through dynamic self-assembly to facilitate
injectability. Following transplantation of the hydrogel, LVEF is
improved. This functional improvement is associated with a marked
reduction in fibrotic tissue deposition, enhanced microvascular
density and attenuation of the inflammatory response within the
infarcted region (76).
Similarly, tissue inhibitors of metalloproteinases have been
delivered via MMP-responsive hydrogels to locally counteract
MMP-mediated ECM degradation that contributes to ventricular wall
thinning (77).
Timing of therapeutic delivery can be modulated
through hydrogel design. Physiological requirements of the heart
evolve over time following MI, progressing through inflammatory,
proliferative and remodeling phases (64). Hydrogels provide the capacity for
temporally controlled release profiles (for example, immediate
release of an anti-apoptotic agent to preserve jeopardized
cardiomyocytes, followed by delayed release of a growth factor to
stimulate regenerative processes). Multiphase hydrogel systems have
been engineered to achieve sequential delivery (62). For example, a two-component
hydrogel system has been developed in which one component rapidly
releases SDF-1α to recruit progenitor cells, while the second
component enables sustained release of VEGF to promote
neovascularization (73). This
staged delivery approach enhances cardiac repair in a mouse MI
model.
Gene therapy and exosome delivery
Beyond proteins and cells, hydrogels are explored
as platforms for localized gene therapy in the myocardium (78). Plasmid DNA, mRNA or viral vectors
encoding regenerative factors can be incorporated into hydrogel
matrices to enable sustained and site-specific gene delivery
(21,78). An injectable biocompatible
hydrogel capable of facilitating efficient delivery of a
nanocomplex composed of graphene oxide (GO) and the pro-angiogenic
VEGF-165 gene demonstrates therapeutic potential for myocardial
repair (Fig. 5A) (78). Exosomes (nanoscale EVs secreted
by cells that contain miRs and proteins) have attracted attention
as cell-free therapeutic agents (79-81). Exosomes attenuate apoptosis and
promote cardiac repair in a manner comparable with their parent
cells (79-81). However, freely injected exosomes
are rapidly cleared from the myocardium. Encapsulation within
hydrogels prolongs their retention at the injury site (82). Improved retention of exosomes in
injured myocardium has been demonstrated using an injectable
shear-thinning gel (STG) loaded with EVs (82) (Fig. 5B-D). The STG shows even
distribution of EVs within the gel matrix (Fig. 5D) and sustained EV release over
21 days (Fig. 5E), which
collectively enhances myocardial function, improves hemodynamic
parameters and increases neovascularization (82). Furthermore, exosomes derived from
human adipose-derived SCs, gelatin and laponite are combined to
formulate a shear-thinning nanocomposite hydrogel (nSi Gel) as an
injectable carrier of the stem cell secretome, which increases
vascular density surrounding the myocardium, improves cardiac
function and decreases scar formation (83). These findings demonstrate how
hydrogels function as reservoirs for advanced biological agents,
such as nucleic acids or EVs, ensuring localized therapeutic
activity rather than rapid systemic dispersion.
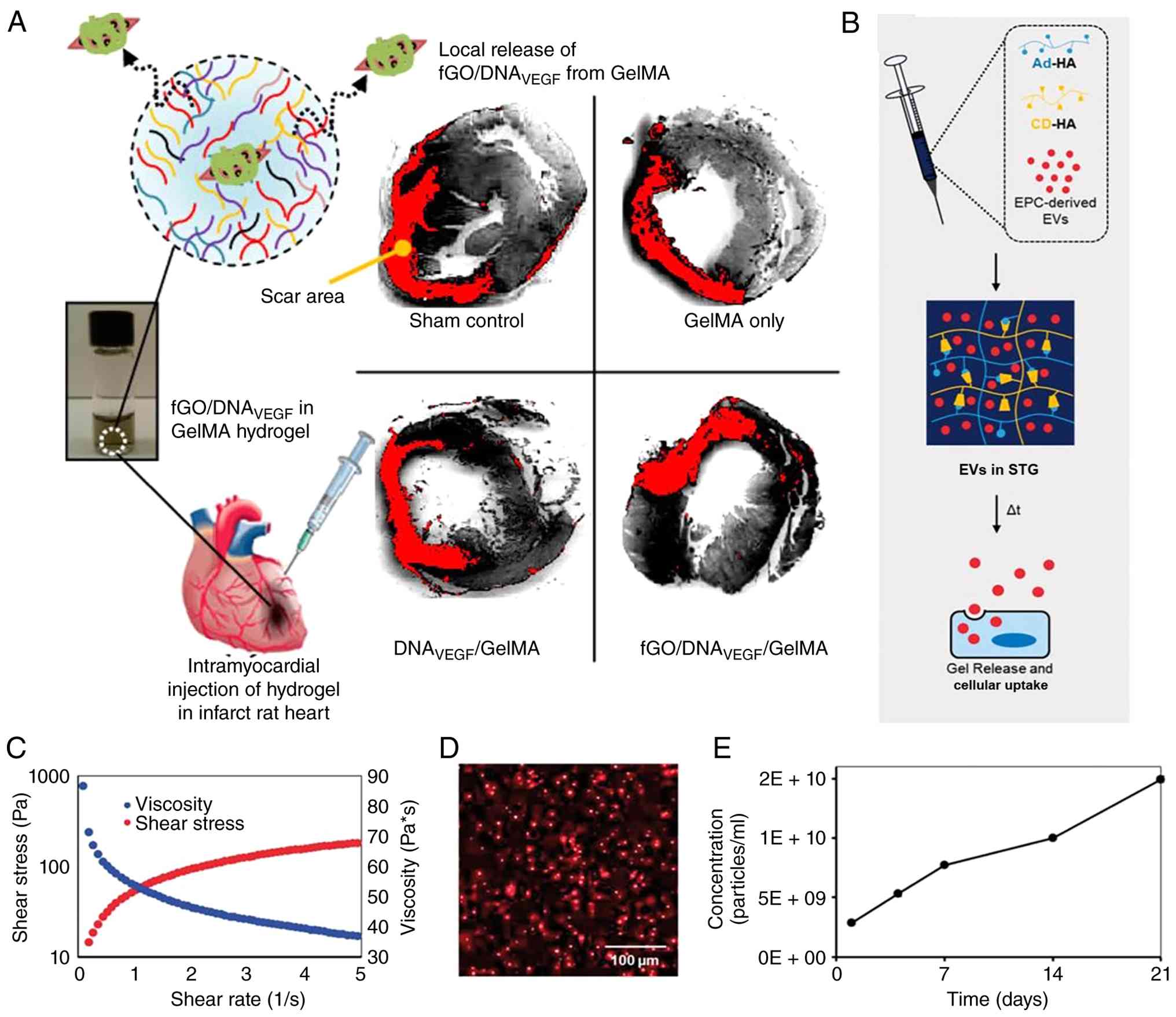 | Figure 5Hydrogel-based delivery systems for
gene and exosome therapy in myocardial repair. (A) Schematic of an
injectable GO/hydrogel-based angiogenic gene delivery system
carrying the VEGF-165 gene. The GO nanocomplex enhances
transfection efficiency and the hydrogel enables sustained local
gene release for cardiac repair. Adapted from (78) (open access). STG for EV delivery.
(B) EVs are mixed with CD-HA and Ad-HA, which form a supramolecular
gel via guest-host chemistry. (C) Under syringe shear stress, the
gel shear-thins to allow injection; upon strain cessation, it
rapidly re-assembles at the myocardial injection site, entrapping
EVs. (D) Confocal microscopy showing even distribution of
CM-DiI-labeled EVs within the STG. (E) Cumulative EV release
profile over 21 days, demonstrating steady particle release and
cellular uptake. Adapted from (82). Copyright 2018, Oxford University
Press. fGO, functionalized graphene oxide; STG, shear-thinning gel;
EV, extracellular vesicle; CD, cyclodextrin; HA, hyaluronic acid;
Ad, adamantane; GeIMA, gelatin methacryloyl; EPC, endothelial
progenitor cell. |
Epicardial patches and cardiac tissue
engineering
In addition to injectable systems, hydrogels have
been developed in patch form for application to the epicardium, the
outer surface of the heart, overlying the infarcted region
(84). These patches may be
acellular or seeded with therapeutic cells. The underlying concept
is to provide a scaffold that covers the damaged myocardium,
promotes tissue regeneration from the epicardial surface inward and
serves as a mechanical restraint to limit adverse ventricular
dilation (5). Epicardial patches
have been fabricated from synthetic polymers, such as degradable
polyester meshes embedded within hydrogel matrices, as well as from
naturally derived ECM sheets (17,64). Patch-based approaches cover a
broader area and accommodate larger numbers of cells or higher drug
loads, however, they typically require surgical implantation.
Consequently, minimally invasive strategies, including
thoracoscopic placement or catheter-based attachment techniques,
are under investigation (5). In
addition, epicardial priming through placement of bioactive
materials on the cardiac surface has been explored to stimulate
recruitment of endogenous progenitor cells from the pericardial
space (64). Hydrogels that can
be applied by painting or spraying onto the epicardium are in
development, with some formulations incorporating mucoadhesive
properties to enhance adhesion to the moist cardiac surface
(52). Furthermore,
hydrogel-based patches can be prevascularized or engineered with
microchannel architectures to facilitate oxygen and nutrient
diffusion, supporting cell survival following implantation. A 3D
bioprinted cardiac patch composed of a PEG hydrogel has been
fabricated with an internal microchannel network (64). When loaded with MSCs and
implanted in a mouse MI model, the microchannel-containing patch
results in greater vascular ingrowth and superior functional
recovery compared with a solid patch, underscoring the importance
of internal architecture (34).
Wang et al (85)
established a rabbit MI model and administered an epicardial
injection of a hydrogel incorporating bone marrow-derived
mesenchymal stem cells (BMSCs). Compared with control groups,
retention of BMSC grafts within the infarcted myocardium is
prolonged, an effect attributed to the properties of the
α-cyclodextrin (CD)/PEG-b-polycaprolactone-(dodecanedioic
acid)-polycaprolactone-PEG (MPEG-PCL-MPEG) hydrogel system. The
transplanted BMSCs contribute to restoration of cardiac function,
as evidenced by increased vascular density in the infarct border
zone (85). Although the
long-term therapeutic efficacy of this approach requires further
investigation, the α-CD/MPEG-PCL-MPEG hydrogel, characterized by
its cytoprotective properties, improves LV function and attenuates
adverse LV remodeling (85).
Vascular regeneration and repair
Vascular diseases, particularly atherosclerosis
affecting arterial vessels, contribute to life-threatening
conditions such as coronary artery and peripheral arterial disease
and stroke (1,2). Conventional treatments include
bypass graft surgery using either autologous vessels or synthetic
grafts and percutaneous angioplasty with stent implantation to
restore luminal patency in occluded arteries (5). Although these interventions are
typically effective in the short term, they present notable
limitations. Synthetic small-diameter grafts (for arteries <6
mm) exhibit high failure rates due to thrombosis or intimal
hyperplasia, defined as excessive neointimal tissue formation
(18). Stents may undergo
restenosis or induce chronic inflammatory responses. Functional
hydrogels offer strategies for engineering artificial blood
vessels, enhancing integration and healing of vascular implants and
treating vascular pathologies such as atherosclerosis (45,63).
Tissue-engineered vascular grafts
(TEVGs)
The development of TEVGs has long been an
objective, particularly for small-diameter arteries (≤6 mm), such
as coronary or peripheral vessels (86). Conventional synthetic grafts,
typically composed of PET or ePTFE, perform adequately in
large-diameter applications but demonstrate high failure rates in
small-caliber vessels due to thrombosis and intimal hyperplasia
(86). Clinical outcomes for
large-diameter grafts (>6 mm) have been satisfactory, with
reported patency rates of up to 95% at 5 years (87). By contrast, the aforementioned
study reported a patency rate of 30% for small-diameter grafts
(<6 mm) (87). Additional
investigations have documented patency rates ranging from 0 to 25%
in canine and rabbit models after implantation periods of weeks to
months (88-90).
Hydrogels serve as scaffold materials capable of
forming the structural matrix of bioengineered vascular grafts
(16). One strategy involves
fabrication of a tubular hydrogel scaffold (optionally reinforced
with supportive materials) that can be seeded with vascular cells
and matured into a functional vessel. Natural hydrogels, such as
collagen or fibrin, have been molded into tubular configurations
for this purpose (24,46). These materials provide a
favorable microenvironment for smooth muscle and endothelial cells
to deposit ECM components and organize into a vessel wall. However,
hydrogel-only tubes typically exhibit insufficient mechanical
strength, particularly in terms of burst pressure, during the early
implantation phase (63). To
address these limitations, strategies have been developed in
cardiovascular tissue engineering, including the use of diverse
scaffold types, such as natural and synthetic polymers (91-93), as well as decellularized
xenografts and homografts (94-96), in combination with different cell
sources, including valvular interstitial cells (97,98), BMSCs (99) and progenitor cells obtained from
peripheral blood or amniotic fluid (100-102). In addition, 3D bioprinting
techniques have been employed to fabricate vessel-like constructs
using hydrogel-based bioinks laden with cells, enabling the
creation of defined multilayered wall architectures (45). Another strategy involves cell
sheet engineering, in which cell monolayers cultured on
temperature-responsive hydrogel surfaces are detached as intact
sheets and wrapped into tubular structures. Although the final
graft does not contain a hydrogel component, this approach relies
on PNIPAM, a thermoresponsive hydrogel, to enable enzyme-free
harvesting of cell sheets (103). These cell sheet-based grafts
have demonstrated promising outcomes in small animal models
(45,85,103).
Hydrogels serve a more direct role in fully
synthetic TEVGs through the development of hybrid graft materials.
One design involves electrospinning a blend of biodegradable
polymer fibers with an incorporated hydrogel component to enhance
graft compliance and facilitate cell infiltration (104). Another approach involves
chemically bonding a hydrogel layer to the luminal surface of a
porous synthetic graft, thereby creating a bioactive interface that
promotes endothelialization (63). This inner hydrogel layer can be
functionalized with bioactive agents such as heparin to reduce
thrombogenicity, or VEGF to stimulate endothelial cell recruitment.
In a study by Chen et al (105), a small-diameter polyethylene
terephthalate graft was coated on its luminal surface with a
heparin-containing hydrogel. In a rabbit carotid artery
implantation model, this modification results in decreased
thrombosis and more rapid formation of a functional endothelial
lining compared with uncoated grafts (105). A key objective in TEVG
development is to promote host-mediated remodeling and repopulation
of the graft with autologous cells, effectively transforming the
construct into a living vascular tissue (86). Hydrogels, owing to their
cytocompatible and bioactive properties, are well-suited to support
this process. For example, a bioinspired small-diameter vascular
graft incorporated a hydrogel derived from decellularized arterial
matrix on the luminal surface, providing biochemical cues that
accelerate endothelial coverage following implantation (106). Establishment of a confluent
endothelium is key for long-term graft patency, as it suppresses
thrombosis and pathological smooth muscle cell proliferation
(86).
Promotion of endothelialization and
hydrogel coatings for stents
In vascular intervention, such as percutaneous
angioplasty with stent implantation, a challenge is the host
response to the implanted stent (107). Drug-eluting stents incorporate
antiproliferative agents (sirolimus or paclitaxel) within a polymer
coating to suppress excessive smooth muscle cell proliferation and
thereby prevent restenosis, however, these agents may also delay
endothelial healing (107).
Ideally, a stent should inhibit neointimal hyperplasia and rapidly
achieve coverage by a functional endothelial layer, thereby
mimicking the behavior of a native artery and decreasing the risk
of thrombosis. Hydrogel-based coatings are being investigated to
create pro-healing stent surfaces. One approach involves nitric
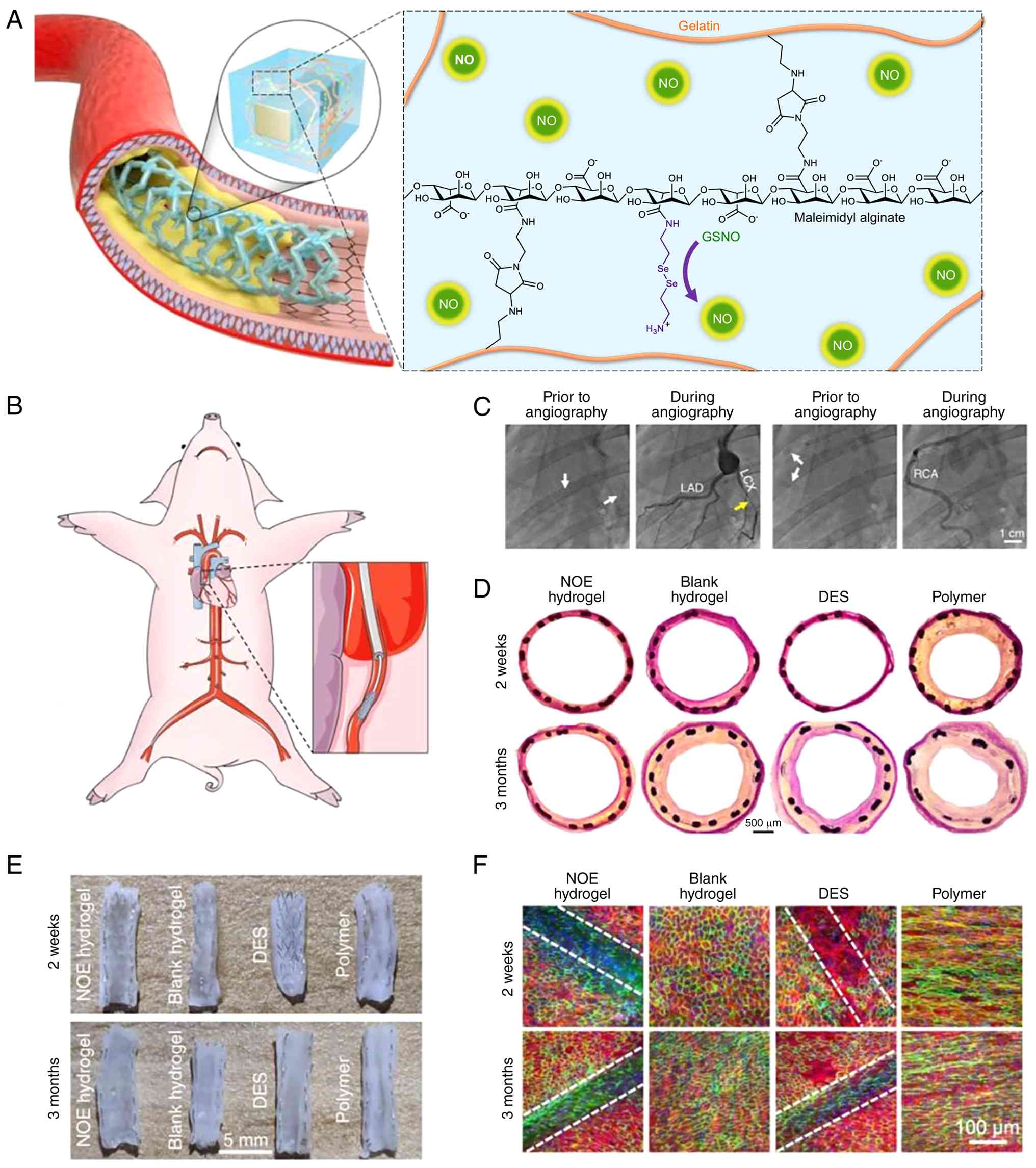
oxide (NO)-releasing hydrogel coatings applied to stents (105). A tough NO-eluting (NOE)
hydrogel coating has been designed for sustained NO release
(Fig. 6A). Following stent
deployment in porcine coronary arteries (Fig. 6B), digital subtraction
angiography shows that the NOE coating prevents severe restenosis
observed in control stents (Fig.
6C; yellow arrow). Histological analysis (Fig. 6D) and luminal surface imaging at
2 weeks and 3 months (Fig. 6E)
confirms that the NOE coating decreases neointimal hyperplasia and
thrombosis. Confocal microscopy (Fig. 6F) reveals rapid and complete
endothelialization (CD31+ cells) on the NOE-coated
stents (105). Another strategy
employs antibody-functionalized hydrogels, such as those conjugated
with anti-CD34 antibodies, to capture circulating endothelial
progenitor cells and accelerate endothelialization (106). Zwitterionic hydrogels,
characterized by resistance to non-specific protein adsorption,
have also been utilized as coatings to reduce platelet adhesion
while selectively promoting endothelial cell attachment (104). In one study, a zwitterionic
hydrogel loaded with VEGF was applied to a heart valve prosthesis
to enhance endothelialization and decrease calcification; this may
also be applicable to vascular stents (108). For bioresorbable stents
composed of biodegradable metals, such as magnesium, or
biodegradable polymers, hydrogel coatings modulate degradation
kinetics and improve the tissue-device interface. In one study,
magnesium alloy stents were coated with a fucoidan-containing
hydrogel, which enhanced hemocompatibility and promoted endothelial
cell colonization during gradual metal degradation (109). Fucoidan, a sulfated
glycosaminoglycan with anticoagulant properties, contributes to
localized inhibition of thrombosis and inflammation (109).
Hydrogel-based strategies for
atherosclerosis treatment
Atherosclerosis, characterized by the accumulation
of lipid-rich plaques within arterial walls, underlies numerous
cardiovascular events, including MI and stroke (1,2).
Although risk factor modification and systemic pharmacotherapy,
such as statins and anti-inflammatory agents, remain the
cornerstone of management, attention has been directed toward
localized therapeutic strategies aimed at stabilizing or regressing
high-risk plaques (75).
Hydrogels serve as promising platforms in this context,
particularly as injectable depots that can be delivered to
vulnerable plaque sites for localized drug release (110).
One strategy targets intraplaque
neovascularization, a hallmark of advanced atherosclerotic lesions.
Fragile microvessels that develop within plaques are prone to
rupture, leading to intraplaque hemorrhage and contributing to
plaque instability. In a recent study, a thermosensitive hydrogel
composed of poloxamer 407 and alginate was employed to deliver
PEDF, an endogenous inhibitor of pathological angiogenesis, to
atherosclerotic plaques (51).
The formulation remained in a liquid state during catheter-based
administration and gelled at physiological temperature, forming a
localized drug reservoir at the plaque site. Sustained release of
PEDF decreases intraplaque neovessel density and plaque progression
in a mouse model of atherosclerosis (51). Treated plaques exhibited smaller
lipid cores and thicker, more stable fibrous caps, indicating
enhanced lesion stabilization. This approach demonstrates how
hydrogel-based delivery systems can localize therapeutics that
would lack plaque specificity if administered systemically
(110).
Hydrogels have been investigated as vehicles for
delivering agents that modulate plaque-associated inflammation
(75). For example, an
injectable peptide hydrogel incorporating an anti-inflammatory
agent (naproxen) and a ferrofluid for magnetic targeting was
developed to treat atherosclerotic plaques by promoting macrophage
polarization toward a reparative phenotype. In principle, a
hydrogel could be directed to the lesion site using an external
magnetic field via embedded Fe3O4
nanoparticles and provide sustained local drug release (75). Similarly, another group developed
a filamentous nanofiber hydrogel depot for prolonged delivery of
anti-inflammatory nanoparticles, resulting in sustained suppression
of inflammatory markers in an experimental model of atherosclerosis
(110). Gene and RNA-based
therapeutic delivery to plaques using hydrogel systems has also
been explored (66,78). For example, administration of
small interfering RNA (siRNA) or miR targeting pro-atherogenic
genes in macrophages or vascular smooth muscle cells may modulate
plaque progression (78).
Hydrogels shield such nucleic acids from enzymatic degradation and
enhance their local retention within the plaque microenvironment
(62,78). Preliminary studies employing
DNA-loaded hydrogels to modulate macrophage signaling pathways in
arterial tissue have demonstrated decreased pro-inflammatory
cytokine expression (78,110,111).
Although these strategies remain largely at the preclinical stage,
they represent a paradigm shift toward localized resolution of
plaque pathology. While intramural hydrogel injection into the
arterial wall may appear invasive, such delivery could be
integrated into existing angioplasty procedures or implemented via
specialized catheter systems. This localized therapeutic approach
has the potential to complement systemic pharmacotherapy by
targeting high-risk plaques individually (107,110).
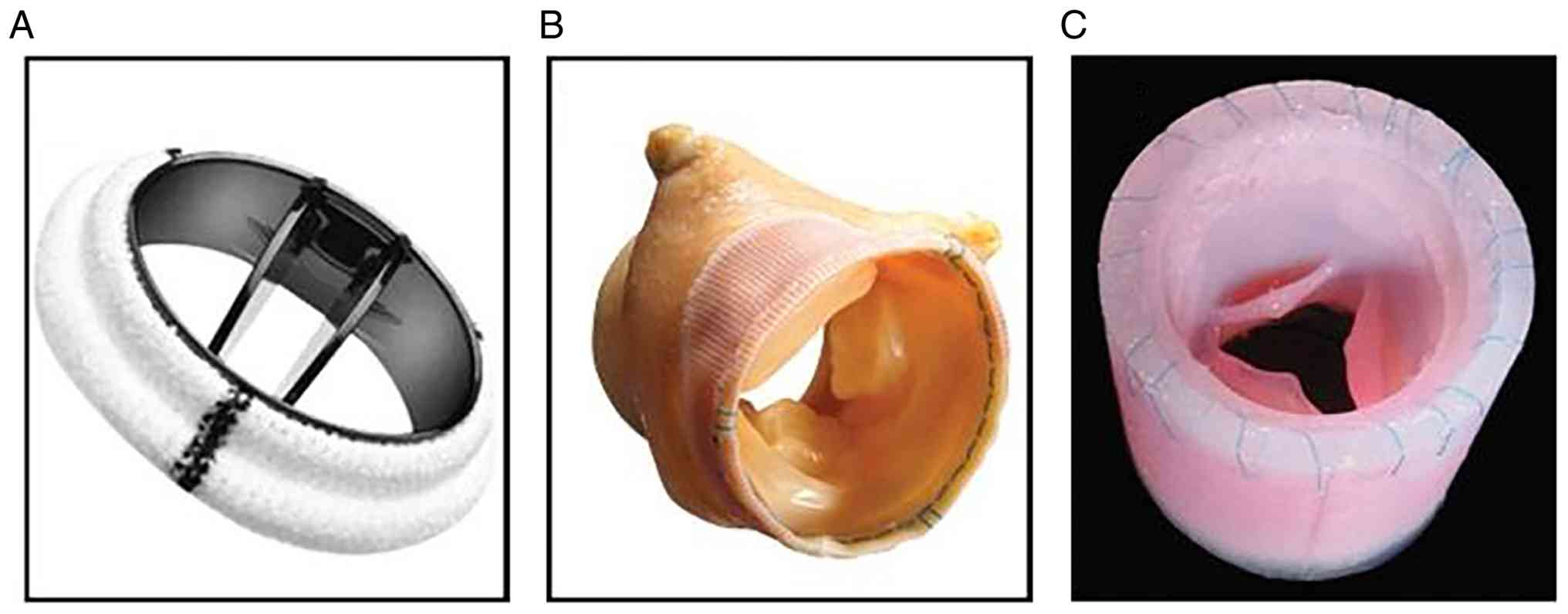
Heart valve repair and regeneration
Heart valve disease typically necessitates valve
replacement (112), with
conventional options including mechanical and bioprosthetic valves
(Fig. 7A and B). To the best of
our knowledge, however, all currently available prosthetic devices
are associated with limitations that increase the risk of morbidity
and mortality. For example, mechanical valves are associated with
thromboembolic events and hemorrhagic complications, thereby
requiring lifelong anticoagulation therapy (113). Bioprosthetic valves demonstrate
limited long-term durability due to structural degeneration,
calcification and fibrotic remodeling and they may also provoke
immunogenic responses (114-116). To the best of our knowledge, no
existing valve replacement strategy fully overcomes these
limitations, rendering tissue-engineered heart valves (TEHVs)
(Fig. 7C) an appealing
therapeutic alternative for affected patients (117-121).
Hydrogels are attractive materials in heart valve
engineering owing to their high water content, biocompatibility and
ability to mimic the compliant connective tissue of native valve
leaflets, and they can be seeded with cells capable of remodeling
the construct (122-124). Native valve leaflets exhibit a
trilayered architecture, comprising collagen fibers that provide
tensile strength, proteoglycans that confer shock absorption and
elastin that enables elastic recoil (115). Pure hydrogels, such as collagen
or fibrin, replicate certain characteristics (for example, softness
and pliability) but may lack sufficient mechanical strength to
withstand repetitive cyclic loading during valve opening and
closing (24). Consequently,
hydrogel application in TEHVs typically involves composite designs
or the use of hydrogels as cell carriers within a mechanically
robust framework (15). One
strategy employs a decellularized valve matrix as the primary
scaffold, which preserves native architecture and mechanical
integrity, followed by infusion or coating with a cell-or growth
factor-laden hydrogel (5). The
hydrogel facilitates reseeding of the decellularized scaffold with
autologous endothelial and valvular interstitial cells and can fill
microstructural defects. Hydrogels such as gelatin methacrylate or
HA-based formulations have been used to impregnate decellularized
porcine valves, generating hybrid constructs that support cellular
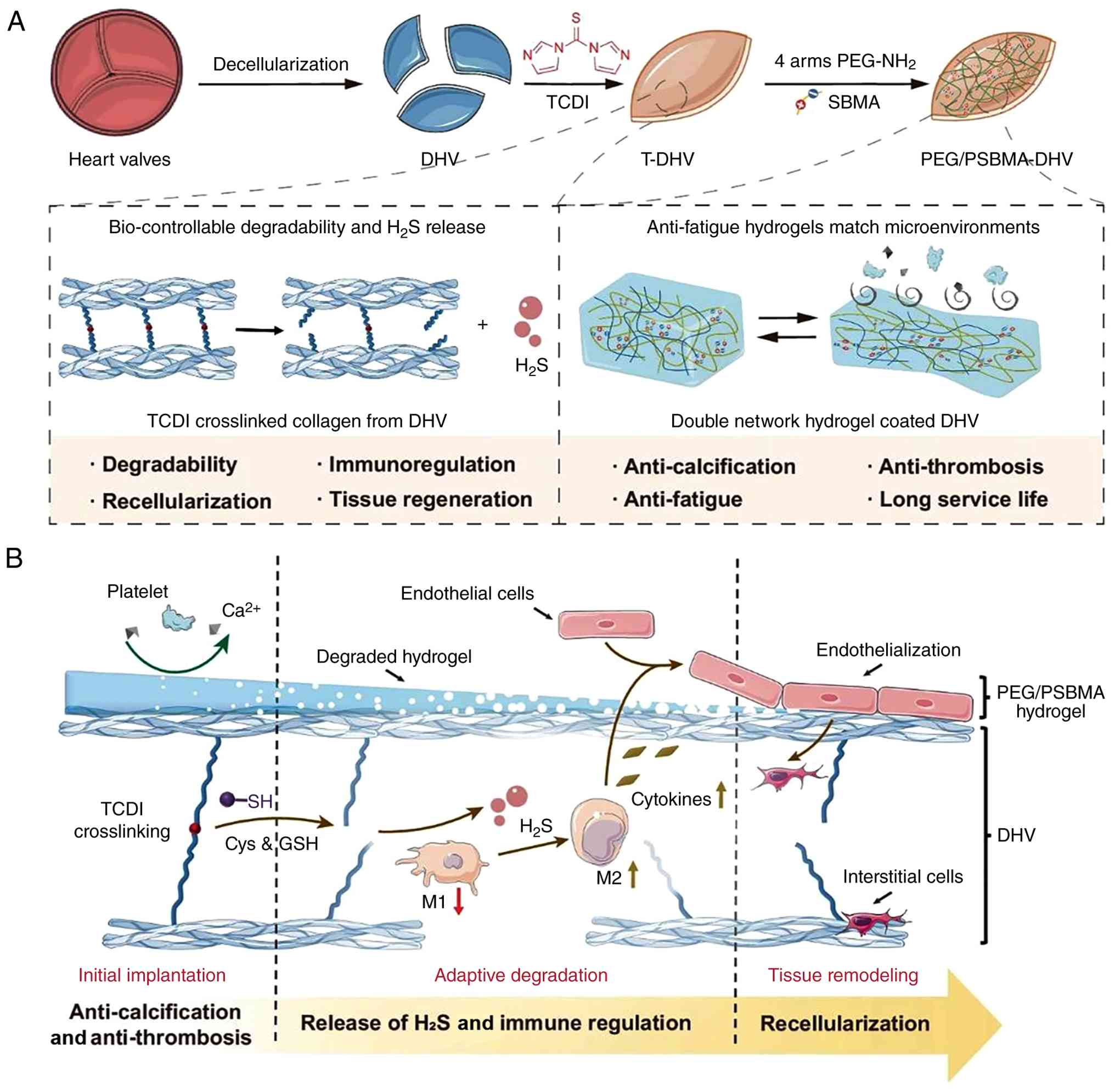
infiltration while maintaining cusp flexibility (25). Another research direction focuses
on fabricating synthetic or hybrid valve scaffolds incorporating
hydrogels. Li et al (125) developed a PEG/poly(sulfobetaine
methacrylate)] dual-network hydrogel coating on decellularized
heart valves (Fig. 8A).
Following implantation, the hydrogel coating provides sufficient
flexural stiffness and fatigue resistance to withstand mechanical
cycling, while facilitating endothelial cell coverage and ECM
remodeling (Fig. 8B) (125). Hydrogel coatings mitigate
calcification of bioprosthetic valves. For example, a zwitterionic
hydrogel coating loaded with heparin and VEGF demonstrates reduced
calcific deposition and enhanced endothelialization in a rabbit
animal model (106).
Four-dimensional (4D) bioprinting, where printed
constructs are designed to undergo controlled structural changes
over time, may enable the fabrication of hydrogel-based valves that
mature in response to physiological forces (123,124). A valve could be printed in a
predefined geometry with cells embedded within a hydrogel matrix;
as the cells synthesize ECM components and the hydrogel degrades,
the construct may transition into a mechanically functional
configuration shaped by bioreactor-mediated conditioning (121). Conditioning engineered valves
in a pulsatile flow bioreactor enhances collagen alignment and
improves mechanical strength (15). Hydrogels serve a key role in
these strategies by providing an initial structural template that
is progressively replaced by newly formed tissue.
Cell and molecular mechanisms of
hydrogel-tissue interactions in CVD
Functional hydrogels modulate cardiovascular tissue
repair through precise regulation of cell behavior and molecular
signaling pathways (5,16).
Pro-angiogenic mechanisms
Hydrogels promote vascularization through
coordinated biochemical signaling and mechanotransductive pathways
(126,127). VEGF-loaded HA
nanobubble/Pluronic F127 diacrylate) hydrogels activate PI3K/Akt
signaling, thereby enhancing endothelial cell migration and
proliferation (126). Spatially
heterogeneous platelet-rich plasma (PRP) fibrin hydrogels direct 3D
vasculogenesis via the integrin β1/phosphorylated focal adhesion
kinase/phosphorylated myosin light chain pathway and stabilize
vascular endothelial-cadherin/β-catenin junctions (127). UCL-TRO-1938, a PI3Kα activator
delivered from alginate hydrogels, stimulates angiogenesis in a
temporally controlled manner during the acute ischemic phase
(128). Moreover, c-ECM
hydrogels enable sequential release of VEGF and Ang-1 mimetic
peptides in response to MMP-2, thereby promoting the formation of
mature and functional blood vessels (60).
Anti-inflammatory mechanisms
Hydrogels reshape the cardiac immune
microenvironment through modulation of conserved anti-inflammatory
and antioxidant signaling pathways. MXene-PVA hydrogels activate
AMPK/Nrf2/Keap1 signaling to enhance ROS clearance and suppress
NF-κB activity, while promoting macrophage polarization toward a
reparative M2 phenotype (129).
Similarly, ROS-responsive adhesive hydrogels releasing
andrographolide derivatives, NLRP3 inhibitor-loaded folic
acid-HA-mesoporous silica nanoparticles and gelatin
methacrylate/gelatin norbornene hydrogel patches promote M2
polarization independent of exogenous cytokine supplementation
(130,131). MMP-responsive hydrogels enable
on-demand IL-4 plasmid delivery to suppress post-MI inflammation,
whereas p38-responsive supramolecular hydrogels inhibit p38
mitogen-activated protein kinase signaling to attenuate oxidative
stress and inflammatory responses (132,133). Furthermore, thermosensitive
hydrogels delivering thiamet-G enhance M2 polarization via signal
transducer and activator of transcription 6 O-GlcNAcylation
(134). Annexin A1-loaded
alginate hydrogels modulate macrophage polarization through the
AMPK-mTOR axis (135), while
exosome-laden hydrogels regulate PI3K/Akt/mTOR, Hippo, TGF-β, HIF-1
and FoxO signaling pathways to facilitate cardiac repair (136). Collectively, these findings
underscore the capacity of hydrogels to modulate the cardiac immune
microenvironment through multiple convergent molecular
mechanisms.
Anti-fibrotic mechanisms
Hydrogels mitigate maladaptive cardiac fibrosis
through multiple complementary mechanisms. Co-delivery of the MMP-2
inhibitor CTT (a cyclic peptide) and bFGF inhibits
fibroblast-to-myofibroblast differentiation (137). ROS-responsive hydrogels
releasing anti-IL-11 antibodies reduce scar thickness and border
zone expansion by suppressing fibroblast activation (138). Furthermore, injectable alginate
composite hydrogels enabling pH-responsive release of bone
morphogenetic protein-9 effectively suppress TGF-β mediated
fibroblast activation and myocardial fibrosis by antagonizing
maladaptive ECM deposition (128). Similarly, a ROS-responsive
hydrogel system (superoxide inhibitor, and
FT011/liposome-quercetin-thioketal ROS-responsive linker;
S1&FT/Lipo-QCFT) sequentially releases the superoxide
production inhibitor S1QEL1.1 and tannic acid to attenuate early
oxidative injury and promote M2 macrophage polarization, followed
by sustained release of the anti-fibrotic agent FT011 to counteract
TGF-β1-induced fibrosis and prevent adverse ventricular remodeling
(139). Notably, injectable
conductive hydrogel patches (GRAXe, a gelatin-base MXene-containing
ROS-responsive conductive patch with asymmetric adhesion) integrate
ROS-responsive degradation, MXene-mediated electrical conductivity
and asymmetric tissue adhesion to restore electromechanical
coupling while decreasing fibrotic remodeling (140).
Mechanisms of conductive hydrogels
regulating cardiac electrical signal propagation
Conductive hydrogels restore cardiac electrical
signal propagation by re-establishing electrophysiological
continuity, modulating connexin 43 (Cx43)-dependent gap junctions,
stabilizing ion channel function and decreasing electrical
heterogeneity across fibrotic infarcted tissue (5). Studies have demonstrated that
polypyrrole-chitosan conductive hydrogels bridge electrically
isolated cardiomyocyte clusters, synchronize calcium transients and
improve conduction velocity across cryoinfarcted myocardium
(141-147). In vivo administration
shortens QRS duration and restores longitudinal conduction, whereas
ex vivo scar tissue exhibits a three- to four-fold increase
in electrical signal amplitude compared with controls, confirming
restoration of conductive pathways (141). Injectable conductive hydrogels
composed of polypyrrole/PAA and loaded with cardiomyocyte-derived
exosomes enhance electrical coupling by upregulating Cx43
expression and improving sarcomeric organization, while
concurrently modulating SIRT1/p53 signaling to attenuate oxidative
stress and electrical instability (142). In vivo, these hydrogels
normalize action potential and calcium transient duration and
decrease arrhythmia inducibility and electrical resistivity within
infarcted tissue. MXene-based conductive hydrogel patches with
intrinsic ROS-scavenging capacity and electroconductive properties
increase Cx43 expression and enhance electrical signal amplitude in
the infarct zone, thereby synchronizing cardiomyocyte contraction
through restoration of gap junction communication (143). Their conductivity approximates
that of native myocardium, enabling physiological electroconductive
restoration. Injectable GO-based conductive hydrogels capable of
sustained NO release also provide tissue-matched electrical
conductivity. These systems preserve electrical signal propagation,
enhance endothelial network formation and maintain
electrophysiological stability by reducing ROS-mediated electrical
disruption (144). Printable
PVA-glutaraldehyde/PEDOT [poly(3,4-ethylenedioxythiophene) (PEDOT)
conductive patches efficiently transmit electrical signals to adult
cardiomyocytes without introducing notable conduction resistance,
demonstrating safe in vivo performance and preservation of
electrocardiographic parameters (145). Ionic-conductive
PEDOT/poly(ionic liquid) hydrogels enhance Cx43 and α-actinin
expression, thereby restoring intercellular electrical coupling and
decreasing infarct-associated electrical heterogeneity (146). Aniline tetramer-grafted
conductive supramolecular hydrogels preserve Cx43 expression in the
infarct border zone, maintaining gap junction integrity, improving
electrical communication and attenuating adverse ventricular
remodeling (147).
Challenges
While functional hydrogels hold promise, critical
issues must be addressed to ensure their safe and effective
translation into routine cardiovascular therapies (5). These challenges range from
material-associated concerns (biocompatibility and stability) to
practical and economic considerations (scalability and regulatory
approval) (5,13). A comprehensive understanding of
these barriers and the development of strategies to overcome them
is an active focus of ongoing research (5).
Identifying promising candidates and
their limitations
ECM-derived hydrogels represent one of the most
promising platforms owing to their intrinsic bioactivity. A
principal advantage of ECM-derived hydrogels is their capacity to
modulate the host inflammatory response and promote tissue
regeneration, rather than merely providing passive mechanical
support (71). However, their
limitations include batch-to-batch variability inherent to
biologically sourced materials, low mechanical strength compared
with synthetic counterparts and regulatory complexity associated
with xenogeneic products (60,71). Alginate-based hydrogels exhibit
good biocompatibility and have been extensively investigated for
mechanical reinforcement of the infarcted ventricle (3,8).
Preclinical studies have demonstrated increased wall thickness,
decreased wall stress, and improved cardiac function (33,35). Nevertheless, a major limitation
of alginate hydrogels is their lack of intrinsic bioactivity. As
non-degradable or slowly degrading materials, they primarily
provide mechanical support without actively stimulating tissue
regeneration (33,35). Fibrin-based hydrogels have been
employed as cell delivery vehicles because of their rapid gelation,
biocompatibility and capacity to support cell infiltration and ECM
deposition (24). Preclinical
studies have demonstrated enhanced cell engraftment and
angiogenesis (24,30,31). However, rapid degradation and
limited mechanical strength restrict their application as
standalone scaffolds in load-bearing cardiac environments (31). Collagen and gelatin-based
hydrogels support cardiomyocyte function and have demonstrated
efficacy in decreasing infarct size and improving contractility in
preclinical models (11,28,70). However, their low stiffness and
rapid enzymatic degradation necessitate chemical crosslinking or
composite formulation to achieve adequate mechanical stability,
which may compromise biocompatibility (5,28). HA hydrogels exhibit
immunomodulatory properties, including promotion of M2 macrophage
polarization and angiogenesis (32). Although promising for myocardial
repair, unmodified HA is mechanically weak and structurally
fragile, requiring chemical modification to enhance mechanical
stability, thereby increasing manufacturing complexity (32). Synthetic hydrogels offer
tunability and reproducibility, with precisely controllable
mechanical properties, degradation kinetics and network
architectures. Despite these advantages, most synthetic hydrogel
systems remain confined to preclinical development (13). Their intrinsic bioinertness
prevents effective cell recognition and adhesion, thereby limiting
tissue integration and remodeling unless biofunctionalized with
adhesive ligands, such as RGD peptides, or incorporated growth
factors (41,45). Conductive composite hydrogels
incorporating graphene, gold nanowires or MXene nanosheets
represent an emerging frontier in cardiac applications, with the
objective of enhancing electrical signal propagation across scar
tissue and decreasing arrhythmogenic susceptibility (141,143). Preclinical studies have
demonstrated improved electrical integration and synchronized
myocardial contraction (141,143). However, concerns regarding
nanomaterial-associated cytotoxicity, long-term biocompatibility
and fabrication complexity constrain their clinical
translation.
The divergent outcomes observed across hydrogel
platforms suggest that optimal cardiovascular therapy may require
integration of multiple functional attributes. This informs future
research priorities and underscores that no single platform
currently satisfies all therapeutic requirements in cardiovascular
medicine. To facilitate direct quantitative and qualitative
comparison, the key efficacy endpoints and safety outcomes of major
hydrogel platforms are summarized in Table II.
| Table IIClinical and preclinical outcomes of
hydrogel platforms. |
Table II
Clinical and preclinical outcomes of
hydrogel platforms.
| Platform | Composition | Indication | Delivery
method | Phase/status | Preclinical
findings | Clinical
findings | Safety/AEs | Discrepancy
analysis |
|---|
| Algisyl-LVR™
(LoneStar Heart Inc.) | Calcium
alginate | Advanced HF | Intramyocardial
injection | Phase II
(AUGMENT-HF) | Porcine IHF model
demonstrates increased LVEF, stroke volume and infarct wall
thickness and decreased myofiber stress; preserved sphericity
index; preserved downregulation of stress-associated miRNAs | Increased LVEF;
decreased LVEDD, KCCQ quality of life and 6MWD & peak
VO2; improved NYHA class | 30-day mortality,
0%; no device-associated SAEs; no arrhythmogenicity; decreased
NSVT; no thrombosis or immune reaction | Preclinical:
Structural and functional benefits are robust and consistent;
clinical: Clear functional improvements; modest limited improvement
in ventricular dilation and wall thickness compared with robust
preclinical findings); species difference: Preclinical studies used
healthy, genetically uniform swine with induced ischemic heart
failure, whereas clinical patients have advanced heart failure with
multiple comorbidities, which may affect the therapeutic response;
clinical delivery in advanced, chronic HF vs. preclinical in
subacute IHF; open-surgical delivery in clinical vs. preclinical
model limits comparability |
| IK-5001 (BL-1040)
(BioLineRx) | Sodium alginate +
calcium gluconate | Post-STEMI | Intracoronary
infusion | Phase II
(PRESERVATION-I) | Rat MI model:
Decreased LV dilatation, preserved scar thickness preserved,
increased LVFS/FAC; porcine MI model: Adverse LV remodeling
prevented; decreased infarct expansion; increased wall thickness;
preserved LVEF | 6 mo primary
endpoint, negative; no notable decrease in ventricular dilation;
preserved LVEF and LV volume (no further deterioration); decreased
NT-proBNP; increased 6MWD; MLHFQ improved | No
device-associated SAEs; no death, stroke, thrombosis or arrhythmia;
3.7% HF; 3.7% renal failure (not device-associated); no coronary
flow impairment | Delivery route
mismatch (preclinical, direct intramyocardial injection; clinical,
intracoronary infusion, low retention); timing difference: Clinical
delivered 2-5 d post-PCI; preclinical treated at 1-2 weeks;
revascularization effect: Clinical patients all received PCI;
preclinical models usually without reperfusion; preclinical showed
robust reverse remodeling; clinical only showed stabilization |
| VentriGel (Ventrix,
Inc) | Decellularized
porcine cardiac ECM | Post-MI | Transendocardial
injection | Phase I | Rat MI: Preserved
EF, decreased ESV/EDV, fibrosis, hypertrophy and apoptosis;
increased viable cardiomyocyte islands, angiogenesis and
c-kit+ progenitor cells; improved metabolism; modulated
immune microenvironment; Porcine MI: Increased cardiac muscle
content and global/regional function; decreased fibrosis; no
arrhythmia or embolization | Safety and
feasibility established; 3-6 mo, increased 6MWD; increased LVEF;
decreased LVESV; benefit strongest in >1 yr chronic MI | No
device-associated serious AEs, arrhythmia, thrombosis or immune
response; one case of mild transient fever | Timing mismatch:
Preclinical treated at subacute MI; clinical treated in chronic
phase (regenerative window closed); disease severity:
Rodent/porcine models uniform vs. human heterogeneous
comorbidities; Phase I underpowered; efficacy outcomes (LV
end-systolic Volume, LV end-diastolic volume) were not
statistically significant |
Translational insights from comparative
analysis
Discrepancies between preclinical and clinical
outcomes arise from multiple contributing factors. In addition to
efficacy considerations, several critical challenges must be
addressed to ensure safe and effective clinical translation,
including immune response, biodegradation control, long-term
mechanical stability, thrombogenicity and scalability (5,12,148).
Immune response
Comprehensive biocompatibility evaluation in animal
models and in vitro systems is essential prior to clinical
application (148-150). Hydrogels derived from
xenogeneic sources carry a theoretical risk of immunogenicity.
Decellularization decreases this risk by removing cell components
and debris, thereby promoting constructive tissue remodeling rather
than immune rejection (151).
VentriGel demonstrates no serious immune-associated adverse events,
supporting the biocompatibility of decellularized ECM products
&1). Nevertheless, each newly developed material must undergo
rigorous immunotoxicological assessment. Strategies include
incorporation of immunomodulatory cues within hydrogel matrices to
promote immune tolerance, as well as the use of autologous or
allogeneic sources to eliminate xenogeneic-associated risks
(132,148). Synthetic hydrogels may elicit
inflammatory responses if degradation yields irritant byproducts,
particularly in the case of certain polyester-based systems [such
as poly(lactic acid), poly(glycolic acid) and
poly(lactic-co-glycolic acid)] (13). Ensuring degradation products are
biologically inert and readily metabolized or excreted represents a
key design consideration. This challenge may be mitigated by
optimizing degradation kinetics and incorporating buffering
components, however, the balance between material persistence and
degradation must be tailored to each specific application.
Biodegradation control
Control of biodegradation is key to balance
mechanical support and tissue remodeling in cardio-vascular
hydrogels. Premature degradation leads to early loss of structural
support before myocardial repair is complete, whereas slow
degradation impedes native tissue ingrowth, disrupts
electromechanical integration and increases the risk of chronic
inflammation or foreign-body reactions. Therefore, degradation
kinetics must be tailored to align with the repair timeline of
infarcted myocardium (13,16). Recent advances (128,152) have enabled programmable
degradation through modulation of crosslinking density,
incorporation of stimuli-responsive cleavable bonds, or design of
composite networks with controlled erosion profiles. Increased
cross-linking density typically slows degradation by limiting water
penetration and enzymatic accessibility, thereby extending hydrogel
persistence (152). Degradation
byproducts must be chemically inert, non-toxic and readily
metabolized or excreted to prevent chronic inflammation, local
acidosis or tissue injury. Consequently, contemporary cardiac
hydrogels increasingly favor natural polymers or synthetic systems
engineered to yield neutral, biocompatible metabolites (13). Recent studies (138,139) emphasize the importance of
dynamic mechanical matching during degradation. Gradual decrease in
hydrogel stiffness should parallel recovery of native tissue
mechanics to prevent pathological loading or functional decline.
Collectively, rational control of degradation rate, mechanism and
byproduct biocompatibility is key for the safe and effective
application of hydrogel-based cardiac therapies (12,152).
Long-term mechanical stability under
dynamic cardiovascular conditions
The beating heart and pulsatile vasculature impose
cyclic mechanical loading that may result in material fatigue,
fracture or functional deterioration. Hydrogels must therefore
exhibit not only appropriate initial stiffness but also sufficient
fatigue resistance and viscoelastic properties that approximate
those of native tissue (5,64). Stiffness matching represents a
foundational strategy: Hydrogels can be engineered to approximate
native myocardial stiffness, thereby minimizing abnormal stress
transmission to the surrounding myocardium (153). Beyond static stiffness,
viscoelastic design is key. Hydrogels exhibiting stress relaxation
that mimics the time-dependent mechanical behavior of native tissue
promote cell spreading, proliferation and ECM deposition, which are
key for functional integration and repair (154). In addition to intrinsic
material durability, a hydrogel patch or injectable formulation
must integrate with the myocardial wall and deform synchronously
during each cardiac cycle. If the material is excessively stiff,
the adjacent myocardium may experience abnormal mechanical loading;
conversely, if it is overly compliant, it may fail to provide
adequate structural support. Achieving mechanical integration with
dynamic cardiac tissue remains challenging (64,67). Early-generation polymeric
restraint devices, for example, restricted diastolic filling.
Although hydrogels are inherently soft and deformable, offering an
advantage in this context, their mechanical contribution evolves as
degradation progresses. Designers must therefore anticipate shifts
in myocardial workload as the hydrogel resorbs. Premature
degradation may lead to loss of structural support before tissue
healing is complete, whereas excessively delayed degradation may
impede physiological remodeling. Alignment of degradation half-life
with the myocardial recovery timeline is key (155); for example, an ideal hydrogel
for MI repair may degrade over 3-6 months, coinciding with scar
maturation (31). Electrical
compatibility is also critical. An implanted hydrogel should not
interfere with cardiac electrical conduction or contractile
synchrony. Although a highly insulating hydrogel may induce a
conduction block if it forms a substantial mass, clinical
injections are typically small and distributed within native tissue
and to the best of our knowledge, no increase in arrhythmic events
has been reported to date (156). Nevertheless, studies (7,156) monitor patients for potential
proarrhythmic effects [using magnetic resonance imaging (MRI) and
electroanatomic mapping]. Conductive hydrogels incorporating
conductive nanomaterials (such as graphene, gold nanowires or
MXene) or electrically conductive polymers have been developed to
restore electrical coupling across scar tissue (141,143). Preclinical studies (141-143) have demonstrated enhanced Cx43
expression, decreased arrhythmogenic susceptibility and improved
synchronization of cardiomyocyte contraction. Collectively,
achieving long-term mechanical and electrical stability under
dynamic cardiovascular conditions requires an integrated design
strategy that balances stiffness, viscoelasticity, degradation
kinetics and electrical compatibility. By tailoring these
properties to the specific biomechanical and electrophysiological
demands of the target tissue, as well as the temporal course of
healing, functional hydrogels provide durable support that promotes
native cardiac repair.
Thrombogenicity
Thrombogenicity is a key concern for any
intravascular application of hydrogels or for materials that come
into direct contact with blood. Although numerous hydrogels
(alginate or PEG) are considered relatively hemocompatible,
clinical experience from the Humacyte human acellular vessel trial
demonstrated that even human ECM-based grafts may thrombose when
flow dynamics are disturbed (157). In the Symvess trauma study,
peri-implantation anticoagulation was administered to mitigate
thrombotic risk (158). For
future hydrogel-based vascular devices, surface modification
strategies may be necessary to maintain long-term patency. Heparin
or heparin-mimetic coatings decrease platelet adhesion and
activation, as demonstrated in heparin-coated ePTFE grafts and
stent coatings (159).
NO-eluting hydrogels and mechanically robust NO-releasing hydrogel
coatings applied to stents attenuate neointimal hyperplasia and
thrombosis in porcine models by leveraging the antiplatelet and
anti-smooth muscle proliferative effects of NO (105). Zwitterionic hydrogel coatings
exhibit enhanced antifouling properties and decrease
thrombogenicity of decellularized swim bladder matrices used for
bioprosthetic heart valves (160). Hydrogels incorporating
fucoidan, a sulfated glycosaminoglycan with anticoagulant
properties, are applied as coatings for magnesium alloy stents,
improving hemocompatibility and promoting endothelial cell
colonization (109). In cardiac
applications such as injectable hydrogels, delivery techniques must
avoid the introduction of air bubbles or particulate contaminants
that could result in embolization. Clinical protocols developed to
date, including hydrogel filtration and meticulous catheter-based
delivery techniques, have prevented embolic complications (33,71), however, these procedures require
standardization as therapies advance toward broader clinical
implementation.
Scalability and manufacturability of
hydrogel products
Complex hydrogel systems, particularly those
incorporating biological components, present challenges for
consistent large-scale production. Batch-to-batch variability in
biologically derived materials, such as differences in ECM
composition among donor lots, directly influence therapeutic
performance. For scale-up of composite and multi-component
hydrogels, advances in continuous manufacturing technology,
including microfluidic systems, automated mixing and dispensing
platforms and 3D bioprinting, are enabling reproducible large-scale
production with improved quality control (13,19). These platforms permit precise
regulation of component ratios, crosslinking kinetics and final
product homogeneity, thereby mitigating the inherent variability
associated with multi-component formulations (161-163). Sterilization constitutes a
notable translational barrier for cardiovascular hydrogels because
of their high water content, thermosensitivity and susceptibility
to structural degradation under conventional sterilization
conditions. Most hydrogels cannot tolerate autoclaving or dry-heat
sterilization, as elevated temperatures may induce premature
gelation, network disruption, polymer hydrolysis or loss of
thermoresponsive properties (164). Alternative terminal
sterilization strategies are required but must be rigorously
validated to preserve mechanical integrity, biocompatibility and
drug release characteristics (150,164). Gamma irradiation and electron
beam irradiation have been investigated for heat-sensitive
hydrogels, however, radiolysis of water generates ROS, which can
cause polymer chain scission, crosslinking imbalance, decreased
mechanical strength and accelerated degradation (164). Ethylene oxide sterilization
enables low-temperature processing; however, it requires prolonged
degassing to eliminate cytotoxic residues and is incompatible with
highly hydrated formulations. Hydrogen peroxide plasma
sterilization decreases residual toxicity but may induce oxidative
damage to polymer networks. Supercritical carbon dioxide
sterilization has emerged as a promising low-temperature,
residue-free alternative that preserves hydrogel structure,
mechanical properties and biocompatibility while achieving high
sterility assurance levels (164). For injectable and in
situ-forming hydrogels, sterile filtration of prepolymer
solutions prior to crosslinking is a practical and widely
implemented approach, provided that all components are amenable to
filtration and aseptic processing conditions are maintained.
Lyophilized (freeze-dried) hydrogel formulations enable terminal
sterilization of dry solids before reconstitution, thereby
decreasing moisture-mediated degradation during sterilization and
storage (164). No universal
sterilization strategy exists; selection must be tailored to
polymer composition, crosslinking chemistry, water content and
therapeutic payload, with rigorous validation of sterility,
structural integrity, mechanical performance and biocompatibility.
Achieving good manufacturing practice compliance is also essential.
Regulatory approval requires controlled cleanroom environments,
validated cleaning protocols and comprehensive quality control of
composition, mechanical properties, gelation behavior and
sterility. Taken together, these considerations underscore that
scalability is an integral component of hydrogel design, requiring
the integration of robust material engineering with validated
manufacturing processes to enable reproducible, off-the-shelf
production of functional hydrogels for cardiovascular
applications.
Integration with standard care
Any novel therapy must complement, rather than
replace, established treatments unless it demonstrates a clear
clinical advantage. For patients with MI, reperfusion therapy
(percutaneous coronary intervention) and contemporary
guideline-directed medical therapy are life-saving interventions
and the cornerstone of management (6,7);
hydrogel injection may serve as an adjunct strategy aimed at
improving ventricular remodeling. Accordingly, clinical trials must
demonstrate incremental benefit beyond optimal standard-of-care
therapy (8,31,37). This necessitates sufficiently
powered studies to detect, for example, additional improvements in
LVEF or decreased HF-associated hospitalizations. Similarly, in
patients with HF, hydrogel-based therapy may be administered in
combination with established pharmacological and device-based
treatments (34). The multimodal
nature of HF management complicates attribution of therapeutic
effects, making it challenging to isolate the independent
contribution of the hydrogel intervention unless trials are
rigorously designed and appropriately controlled (5,34).
Regulatory and clinical adoption
challenges
Hydrogel-based therapies typically straddle the
boundary between medical devices and biologics, rendering
regulatory classification complex (150). FDA has categorized certain
formulations (hydrogels incorporating cells such as mesenchymal
stem cells or hydrogels containing bioactive factors like growth
factors) as combination products, particularly when they
incorporate cells or bioactive factors (150). Comprehensive safety and
efficacy data are required as these therapies represent relatively
new treatment modalities. Clinicians may also exercise caution in
adopting such technologies until robust evidence from Phase III
clinical trials demonstrates clear clinical benefit (71). Practical considerations influence
adoption. Interventional cardiologists may require specialized
training to deliver hydrogels safely via catheter-based techniques
and cardiac surgeons must become familiar with handling hydrogel
materials during operative procedures. In addition, reimbursement
pathways must be defined, as these therapies may initially incur
notable costs due to manufacturing complexity (5,150).
Conclusion
Although synthetic hydrogels provide tunable
mechanical properties and high reproducibility, their long-term
in vivo fate, including degradation products, chronic
inflammatory responses, and potential toxicity, remains
insufficiently characterized. Most preclinical studies (5,13,64) have reported outcomes over weeks
to months, however, cardiovascular applications require durability
over years. Future investigations should prioritize systematic
evaluation of degradation kinetics, long-term biocompatibility and
sustained functional performance in large-animal models over
extended time-frames. Attention should be directed toward the
accumulation of degradation byproducts and their potential
off-target effects.
Current hydrogel therapies largely follow a
'one-size-fits-all' paradigm. However, patient-specific factors,
including age, comorbidity, infarct geometry, scar composition and
inflammatory status, may influence therapeutic response. Advances
in high-resolution imaging modalities (cardiac MRI and computed
tomography), biomarker profiling and 3D bioprinting may enable the
development of patient-tailored hydrogels with customized
mechanical properties, degradation rates and bioactive payloads.
Further research is required to establish rational design
algorithms that integrate patient-derived data with material
selection strategies and determine whether personalized hydrogels
confer superior outcomes compared with standardized formulations in
preclinical models.
Hydrogels represent promising platforms for
localized delivery of next-generation biologics, including mRNA,
siRNA and CRISPR-Cas9 (clustered regularly interspaced short
palindromic repeats (CRISPR)-associated protein 9) gene-editing
components (78,165). For example, hydrogel-mediated
delivery of mRNA encoding cardioprotective factors may overcome the
short half-life and off-target effects associated with systemic
administration. Similarly, hydrogels may facilitate
spatiotemporally controlled CRISPR-based genome editing to correct
disease-associated genes, such as silencing profibrotic genes in
cardiac fibroblasts, or to enhance endogenous repair pathways.
Proof-of-concept studies in clinically relevant animal models are
needed to establish safety, efficacy and optimal delivery
parameters. Addressing these knowledge gaps may accelerate the
translation of functional hydrogels and help realize their full
potential in cardiovascular regenerative medicine.
The design space for functional hydrogels,
encompassing polymer composition, crosslinking density, degradation
rate, mechanical properties and bioactive payloads, is vast and
multidimensional. Conventional trial-and-error approaches are
typically time-consuming and inefficient. Machine learning and
artificial intelligence (AI) offer transformative potential to
accelerate hydrogel development. By training algorithms on existing
datasets that associate hydrogel physicochemical properties with
biological outcomes, AI models predict optimized formulations for
specific clinical applications, propose novel polymer combinations
and elucidate structure-function relationships. When coupled with
high-throughput screening platforms and automated synthesis
technologies, AI-guided design may shorten development timelines
and reveal previously unrecognized interactions (161-163).
Advances in 3D bioprinting enable fabrication of
complex, patient-specific hydrogel constructs with precise control
over architecture, cell distribution and biomechanical properties
(45). For cardiac repair,
bioprinted patches can be designed to match individual infarct
geometry mapped using cardiac MRI and incorporate aligned
microchannels that guide cardiomyocyte orientation and vascular
ingrowth. Beyond therapeutic applications, hydrogel-based
organ-on-a-chip platforms incorporating patient-derived
iPSC-derived cardiomyocytes, endothelial cells and fibroblasts
provide powerful tools for preclinical evaluation. These
microphysiological systems recapitulate key features of the cardiac
microenvironment, enabling rapid assessment of hydrogel mechanical
behavior, drug release kinetics and cellular responses prior to
translation into animal studies (49).
Hydrogels are expected to increasingly function as
delivery platforms for next-generation therapeutics. Beyond
conventional growth factors, hydrogels encapsulate and locally
release viral vectors, such as adeno-associated virus and
lentiviral vectors encoding therapeutic genes, thereby enabling
sustained and localized transduction while minimizing systemic
exposure (66). For cell-based
therapy, hydrogels provide a protective microenvironment that
enhances survival, retention and functional integration of
transplanted cells, including MSCs, iPSC-derived cardiomyocytes and
cardiac progenitor cells (72).
Emerging strategies integrate both modalities, employing hydrogels
to deliver gene-edited cells or cells engineered to secrete
therapeutic factors. The tunable physicochemical properties of
hydrogels permit spatiotemporal control over cell release,
differentiation signals and paracrine activity, thereby maximizing
therapeutic efficacy.
The next generation of hydrogels may exhibit
enhanced responsiveness and dynamic interaction with the
physiological environment. Multi-responsive hydrogels capable of
sensing and reacting to multiple cues, including pH, enzymatic
activity, ROS and mechanical strain, may enable on-demand,
feedback-controlled therapy. 4D hydrogel materials, which undergo
programmed structural or functional changes over time, may
facilitate sequential therapeutic staging, for example, initially
promoting angiogenesis followed by stimulation of myocardial
regeneration. Such adaptive materials more closely recapitulate the
dynamic behavior of native tissue compared with conventional static
hydrogels.
Hydrogels may combine with established
cardiovascular devices to enhance therapeutic performance. For
example, hydrogel coatings applied to stents or vascular grafts can
improve hemocompatibility, promote endothelialization and enable
localized delivery of antirestenotic agents. Hydrogels incorporated
into balloon angioplasty catheters may simultaneously dilate
stenotic arteries and deliver therapeutic compounds directly into
the vessel wall. In HF management, hydrogels injected around the
inflow cannula of left ventricular assist devices may promote
myocardial recovery within the mechanically unloaded environment.
These integrated strategies leverage the complementary strengths of
biomaterials and device-based interventions while mitigating their
individual limitations.
As understanding of patient heterogeneity advances,
hydrogel-based therapies may be tailored to individual
characteristics. This personalization may involve adjusting
hydrogel composition according to inflammatory profile, selecting
degradation kinetics that correspond to individual healing dynamics
or incorporating autologous cells or PRP. With advances in imaging
technologies and 3D bioprinting, fully personalized cardiac patches
(custom-shaped to conform to infarct geometry and incorporating
patient-derived cells) may become clinically feasible. Although
technically complex, these approaches are progressing and
associated costs may decline as scalable manufacturing technologies
mature.
As clinical evidence accumulates, optimal timing
and patient selection criteria for hydrogel-based interventions may
increasingly refined. Future treatment protocols may define
specific indications, for example, hydrogel injection on day 5
post-MI in patients with infarct size exceeding a defined threshold
and inflammatory biomarkers within a specified range. Integration
of hydrogel therapy into standard-of-care algorithms requires
large-scale clinical trials demonstrating incremental benefit
beyond optimal medical management. Nevertheless, the potential
advantages, namely, true tissue regeneration rather than
symptomatic palliation, justify continued investigation.
Functional hydrogels may become a key component of
cardiovascular regenerative therapy, either as standalone
modalities or in combination with pharmacological agents,
cell-based therapy, gene-editing technologies and implantable
devices. The ongoing convergence of materials science,
bioengineering, computational modeling and clinical medicine
suggests that interventions such as myocardial regeneration,
bioengineered living valves and reversal of fibrotic remodeling may
become clinically attainable, with functional hydrogels serving as
both structural scaffolds and biological modulators. The progress
from foundational laboratory concepts to early-phase clinical
trials provides a platform for future translation. As remaining
scientific, regulatory and manufacturing challenges are
systematically addressed, hydrogel-based interventions may
transition from experimental applications to integrated components
of mainstream clinical cardiology and cardiac surgery, offering
patients restorative therapeutic options.
Availability of data and materials
Not applicable.
Authors' contributions
ZY and JL conceived the study and wrote the
manuscript. ZY edited the manuscript. ZY and LZ constructed figures
JL and DZ performed the literature review. CY, DL and YH conceived
the study and revised the manuscript. Data authentication is not
applicable. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
Not applicable.
Funding
The present study was supported by the National Natural Science
Foundation of China (grant nos. 82470303, 82570354 and 82200431),
Joint Project of Liaoning Province Science and Technology Plan
(grant nos. 2024JH2/102600272 and 2024JH2/102600279), Liaoning
Provincial Natural Science Foundation (grant nos. 2024-MSLH-534 and
2026-BS-0900) and Independent Scientific Research Project of the
General Hospital of Northern Theater Command (grant no.
ZZKY2024050).
References
|
1
|
Roth GA, Mensah GA, Johnson CO, Addolorato
G, Ammirati E, Baddour LM, Barengo NC, Beaton AZ, Benjamin EJ,
Benziger CP, et al: Global burden of cardiovascular diseases and
risk factors, 1990-2019: Update from the GBD 2019 study. J Am Coll
Cardiol. 76:2982–3021. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Li Y, Cao GY, Jing WZ, Liu J and Liu M:
Global trends and regional differences in incidence and mortality
of cardiovascular disease, 1990-2019: Findings from 2019 global
burden of disease study. Eur J Prev Cardiol. 30:276–286. 2023.
View Article : Google Scholar
|
|
3
|
Hasan A, Khattab A, Islam MA, Hweij KA,
Zeitouny J, Waters R, Sayegh M, Hossain MM and Paul A: Injectable
hydrogels for cardiac tissue repair after myocardial infarction.
Adv Sci (Weinh). 2:15001222015. View Article : Google Scholar
|
|
4
|
Klaourakis K, Vieira JM and Riley PR: The
evolving cardiac lymphatic vasculature in development, repair and
regeneration. Nat Rev Cardiol. 18:368–379. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Holme S, Richardson SM, Bella J and Pinali
C: Hydrogels for cardiac tissue regeneration: Current and future
developments. Int J Mol Sci. 26:23092025. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lüscher TF: Myocardial infarction:
Mechanisms, diagnosis, and complications. Eur Heart J. 36:947–949.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Damluji AA, van Diepen S, Katz JN, Menon
V, Tamis-Holland JE, Bakitas M, Cohen MG, Balsam LB, Chikwe J;
American Heart Association Council on Clinical Cardiology; Council
on Arteriosclerosis; et al: Mechanical complications of acute
myocardial infarction: A Scientific statement from the American
heart association. Circulation. 144:e16–e35. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mann DL, Lee RJ, Coats AJ, Neagoe G,
Dragomir D, Pusineri E, Piredda M, Bettari L, Kirwan BA, Dowling R,
et al: One-year follow-up results from AUGMENT-HF: A multicentre
randomized controlled clinical trial of the efficacy of left
ventricular augmentation with Algisyl in the treatment of heart
failure. Eur J Heart Fail. 18:314–325. 2016. View Article : Google Scholar
|
|
9
|
Nick C and John HD: Heart transplantation.
Surgery (Oxford). 41:573–579. 2023. View Article : Google Scholar
|
|
10
|
Fuchs M, Schibilsky D, Zeh W,
Berchtold-Herz M, Beyersdorf F and Siepe M: Does the heart
transplant have a future? Eur J Cardiothorac Surg. 55(Suppl 1):
i38–i48. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li P, Hu J, Wang J, Zhang J, Wang L and
Zhang C: The role of hydrogel in cardiac repair and regeneration
for myocardial infarction: Recent advances and future perspectives.
Bioengineering (Basel). 10:1652023. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dong S, An S, Saiding Q, Chen Q, Liu B,
Kong N, Chen W and Tao W: Therapeutic hydrogels: Properties and
biomedical applications. Chem Rev. 125:8835–8920. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Spicer CD: Hydrogel scaffolds for tissue
engineering: The importance of polymer choice. Polym Chem.
11:184–219. 2020. View Article : Google Scholar
|
|
14
|
Chaudhary S and Chakraborty E: Hydrogel
based tissue engineering and its future applications in
personalized disease modeling and regenerative therapy. Beni Suef
Univ J Basic Appl Sci. 11:32022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang X, Xu B, Puperi DS, Wu Y, West JL
and Grande-Allen KJ: Application of hydrogels in heart valve tissue
engineering. J Long Term Eff Med Implants. 25:105–134. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Drury JL and Mooney DJ: Hydrogels for
tissue engineering: Scaffold design variables and applications.
Biomaterials. 24:4337–4351. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gomez-Florit M, Pardo A, Domingues RMA,
Graça AL, Babo PS, Reis RL and Gomes ME: Natural-based hydrogels
for tissue engineering applications. Molecules. 25:58582020.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gutowski P, Guziewicz M, Ilzecki M,
Kazimierczak A, Lawson JH, Prichard HL, Przywara S, Samad R, Tente
W, Turek J, et al: Six-year outcomes of a phase II study of
human-tissue engineered blood vessels for peripheral arterial
bypass. JVS Vasc Sci. 4:1000922022. View Article : Google Scholar
|
|
19
|
Kafili G, Kabir H, Jalali Kandeloos A,
Golafshan E, Ghasemi S, Mashayekhan S and Taebnia N: Recent
advances in soluble decellularized extracellular matrix for heart
tissue engineering and organ modeling. J Biomater Appl. 38:577–604.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang J, Guo Y, Bai Y and Wei Y:
Application of biomedical materials in the diagnosis and treatment
of myocardial infarction. J Nanobiotechnology. 21:2982023.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hong SB, Jeong JO and Choi H: Hydrogels in
cardiac surgery: Versatile platforms for tissue repair, adhesion
prevention, and localized therapeutics. Gels. 11:5642025.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kim SJ, Park SJ and Kim SJ: Swelling
behavior of interpenetrating polymer network hydrogels composed of
poly(vinyl alcohol) and chitosan. React Funct Polym. 55:53–59.
2003. View Article : Google Scholar
|
|
23
|
Gould RA, Chin K, Santisakultarm TP,
Dropkin A, Richards JM, Schaffer CB and Butcher JT: Cyclic strain
anisotropy regulates valvular interstitial cell phenotype and
tissue remodeling in three-dimensional culture. Acta Biomater.
8:1710–1719. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mol A, van Lieshout MI, Dam-de Veen CG,
Neuenschwander S, Hoerstrup SP, Baaijens FP and Bouten CV: Fibrin
as a cell carrier in cardiovascular tissue engineering
applications. Biomaterials. 26:3113–3121. 2005. View Article : Google Scholar
|
|
25
|
Masters KS, Shah DN, Leinwand LA and
Anseth KS: Crosslinked hyaluronan scaffolds as a biologically
active carrier for valvular interstitial cells. Biomaterials.
26:2517–2525. 2005. View Article : Google Scholar
|
|
26
|
Flanagan TC, Sachweh JS, Frese J,
Schnöring H, Gronloh N, Koch S, Tolba RH, Schmitz-Rode T and
Jockenhoevel S: In vivo remodeling and structural characterization
of fibrin-based tissue-engineered heart valves in the adult sheep
model. Tissue Eng Part A. 15:2965–2976. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Rodriguez KJ, Piechura LM and Masters KS:
Regulation of valvular interstitial cell phenotype and function by
hyaluronic acid in 2-D and 3-D culture environments. Matrix Biol.
30:70–82. 2011. View Article : Google Scholar
|
|
28
|
McLaughlin S, Sedlakova V and Zhang QZ:
Recombinant human collagen hydrogel rapidly reduces methylglyoxal
adducts within cardiomyocytes and improves borderzone contractility
after myocardial infarction in mice. Adv Funct Mater.
32:22040762022. View Article : Google Scholar
|
|
29
|
Gorlatov S and Medved L: Interaction of
fibrin(ogen) with the endothelial cell receptor VE-cadherin:
Mapping of the receptor-binding site in the NH2-terminal portions
of the fibrin beta Chains. Biochemistry. 41:4107–4116. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ahmed TA, Griffith M and Hincke M:
Characterization and inhibition of fibrin hydrogel-degrading
enzymes during development of tissue engineering scaffolds. Tissue
Eng. 13:1469–1477. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hu W, Yang C, Guo X, Wu Y, Loh XJ, Li Z,
Wu YL and Wu C: Research advances of injectable functional hydrogel
materials in the treatment of myocardial infarction. Gels.
8:4232022. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Ding J, Yao Y, Li J, Duan Y, Nakkala JR,
Feng X, Cao W, Wang Y, Hong L, Shen L, et al: A reactive oxygen
species scavenging and O2 generating injectable hydrogel
for myocardial infarction treatment in vivo. Small.
16:e20050382020. View Article : Google Scholar
|
|
33
|
Frey N, Linke A, Süselbeck T,
Müller-Ehmsen J, Vermeersch P, Schoors D, Rosenberg M, Bea F, Tuvia
S and Leor J: Intracoronary delivery of injectable bioabsorbable
scaffold (IK-5001) to treat left ventricular remodeling after
ST-elevation myocardial infarction: A first-in-man study. Circ
Cardiovasc Interv. 7:806–812. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wan H, Sun CW and Zhang JY: Recent
advances in implantable hydrogels for treating heart failure. J
Appl Polym Sci. 139:531562022. View Article : Google Scholar
|
|
35
|
Lee RJ, Hinson A, Bauernschmitt R,
Matschke K, Fang Q, Mann DL, Dowling R, Schiller N and Sabbah HN:
The feasibility and safety of Algisyl-LVR™ as a method of left
ventricular augmentation in patients with dilated cardiomyopathy:
Initial first in man clinical results. Int J Cardiol. 199:18–24.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chaturvedi K, Ganguly K, Nadagouda MN and
Aminabhavi TM: Polymeric hydrogels for oral insulin delivery. J
Control Release. 165:129–138. 2013. View Article : Google Scholar
|
|
37
|
Kim C, Jeong D, Kim S, Kim Y and Jung S:
Cyclodextrin functionalized agarose gel with low gelling
temperature for controlled drug delivery systems. Carbohydr Polym.
222:1150112019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tseng H, Cuchiara ML, Durst CA, Cuchiara
MP, Lin CJ, West JL and Grande-Allen KJ: Fabrication and mechanical
evaluation of Anatomically-inspired quasilaminate hydrogel
structures with Layer-specific formulations. Ann Biomed Eng.
41:398–407. 2013. View Article : Google Scholar
|
|
39
|
Durst CA, Cuchiara MP, Mansfield EG, West
JL and Grande-Allen KJ: Flexural characterization of cell
encapsulated PEGDA hydrogels with applications for tissue
engineered heart valves. Acta Biomater. 7:2467–2476. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Jiang H, Campbell G, Boughner D, Wan WK
and Quantz M: Design and manufacture of a polyvinyl alcohol (PVA)
cryogel tri-leaflet heart valve prosthesis. Med Eng Phys.
26:269–277. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Xue F, Zhao S, Tian H, Qin H, Li X, Jian
Z, Du J, Li Y, Wang Y, Lin L, et al: Two way workable
microchanneled hydrogel Suture to diagnose, treat and monitor the
infarcted heart. Nat Commun. 15:8642024. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Crocini C, Walker CJ, Anseth KS and
Leinwand LA: Three-dimensional encapsulation of adult mouse
cardiomyocytes in hydrogels with tunable stiffness. Prog Biophys
Mol Biol. 154:71–79. 2020. View Article : Google Scholar
|
|
43
|
Zou Y, Li L, Li Y, Chen S, Xie X, Jin X,
Wang X, Ma C, Fan G and Wang W: Restoring cardiac functions after
myocardial infarction-ischemia/reperfusion via an exosome anchoring
conductive hydrogel. ACS Appl Mater Interfaces. 13:56892–56908.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Mannarino MM, Bassett M, Donahue DT and
Biggins JF: Novel high-strength thromboresistant poly(vinyl
alcohol)-based hydrogel for vascular access applications. J
Biomater Sci Polym Ed. 31:601–621. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Matějková J, Kaňoková D and Matějka R:
Current status of bioprinting using polymer hydrogels for the
production of vascular grafts. Gels. 11:42024. View Article : Google Scholar
|
|
46
|
López-Gutierrez J, Ramos-Payán R,
Ayala-Ham A, Romero-Quintana JG, Castillo-Ureta H, Villegas-Mercado
C, Bermúdez M, Sanchez-Schmitz G and Aguilar-Medina M:
Biofunctionalization of hydrogel-based scaffolds for vascular
tissue regeneration. Front Mater. 10:11686162023. View Article : Google Scholar
|
|
47
|
Hu C, Liu W, Long L, Wang Z, Zhang W, He
S, Lu L, Fan H, Yang L and Wang Y: Regeneration of infarcted hearts
by myocardial infarction-responsive injectable hydrogels with
combined anti-apoptosis, anti-inflammatory and pro-angiogenesis
properties. Biomaterials. 290:1218492022. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Wang K, Zhang J, Li H, Wu J, Wan Q, Chen
T, Liu W, Peng H, Zhang H and Luo Y: Smart hydrogel sensors for
health monitoring and early warning. Adv Sensor Res. 3:24000032024.
View Article : Google Scholar
|
|
49
|
Lu J, Pan X, Zhang W, Han J, Chen J, Song
M, Xu C, Li X, Wang J and Wang L: Hydrogel sensing platforms for
monitoring contractility in in vitro cardiac models. Nanoscale.
17:8436–8452. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Xu Q, Xiao Z, Yang Q, Yu T, Deng X, Chen
N, Huang Y, Wang L, Guo J and Wang J: Hydrogel-based cardiac repair
and regeneration function in the treatment of myocardial
infarction. Mater Today Bio. 25:1009782024. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Duan Y, Lin J, Yue J, Li Y, Liao J, Sun Y,
Wang Q, Duan Y and Li Z: Temperature-sensitive hydrogel inhibits
VEGFA-dependent neovascularization in atherosclerosis progression.
Sci China Mater. 68:280–291. 2025. View Article : Google Scholar
|
|
52
|
Shi K, Li T, Hu X, Chen W, Yu Y, Bei Z,
Yuan L, Tong Q, Liu J, Fan Q, et al: Injectable and sprayable
thermoresponsive hydrogel with Fouling-Resistance as an effective
barrier to prevent postoperative cardiac adhesions. Adv Sci
(Weinh). 12:e25007312025. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Tang J, Li T, He X, Liu Y, Zhou M, Wu M,
Li Y, Lan Y, Tan X, Tian J and Li C: A shikonin/Cu2+ coordination
complex-encapsulated hydrogel drug depot alleviates myocardial
ischemia-reperfusion injury by disrupting energy
metabolism-mediated intercellular crosstalk. J Colloid Interface
Sci. 706:1395802026. View Article : Google Scholar
|
|
54
|
Alimirzaei F, Vasheghani FE, Ghiaseddin A,
Soleimani M, Pouri and Zeinab NG: pH-sensitive chitosan hydrogel
with instant gelation for myocardial regeneration. J Tissue Sci
Eng. 8:32017.
|
|
55
|
Kong Y, Wang L, Duan F, Huang C, Qiu Z, Ji
RJ, Qiao L, Zhou Y, Cai T, Li YQ, et al: Injectable and
pH-activated Self-feedback hydrogel encapsulating stem cells for
augmented acute myocardial infarction therapy. Adv Healthc Mater.
15:e033242026. View Article : Google Scholar
|
|
56
|
Chen Y, Liang Y, Shen J, Wang Y, Qiu B,
Hou H and Qiu X: A NADH oxidase nanozyme restores redox homeostasis
to ameliorate Multi-organ aging and ischemic cardiomyopathy.
Research (Wash D C). 8:09732025.PubMed/NCBI
|
|
57
|
Wu TL and Liu WG: Functional hydrogels for
the treatment of myocardial infarction. NPG Asia Mater. 14:92022.
View Article : Google Scholar
|
|
58
|
Sullivan HL, Liang Y, Worthington K, Luo
C, Gianneschi NC and Christman KL: Enzyme-Responsive nanoparticles
for the targeted delivery of an MMP inhibitor to acute myocardial
infarction. Biomacromolecules. 24:4695–4704. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Pereira RF, Barrias CC, Bártolo PJ and
Granja PL: Cell-instructive pectin hydrogels crosslinked via
thiol-norbornene photo-click chemistry for skin tissue engineering.
Acta Biomater. 66:282–293. 2018. View Article : Google Scholar
|
|
60
|
Song S, Yang L, Su K, Wu G, Li N, Wang J,
Yu Z and Shi C: Bioactive cardiac ECM hydrogel sequentially
released VEGF and Ang-1 mimic peptides to promote the recovery of
myocardial infarction. Biomater Adv. 180:2146172026. View Article : Google Scholar
|
|
61
|
Chen X, Wu Y, Song P, Feng L, Zhou Y, Shi
J, Dong N and Qiao W: Matrix Metalloproteinase-responsive
controlled release of Self-assembly nanoparticles accelerates heart
valve regeneration in situ by orchestrating immunomodulation. Adv
Sci (Weinh). 12:e24033512025. View Article : Google Scholar :
|
|
62
|
Kharkar PM, Scott RA, Olney LP, LeValley
PJ, Maverakis E, Kiick KL and Kloxin AM: Controlling the release of
small, bioactive proteins via dual mechanisms with therapeutic
potential. Adv Healthc Mater. 6:102017. View Article : Google Scholar
|
|
63
|
Li Z, Chen E, Parsons J and Turng LS:
Design, synthesis, and characterization of polymer-hydrogel
composite vascular grafts using double-expanded
polytetrafluoroethylene to achieve enhanced mechanical and
biological properties. Polym Eng Sci. 65:2893–2908. 2025.
View Article : Google Scholar
|
|
64
|
Liu Z, Zheng Z, Xie J, Wei H and Yu CY:
Hydrogel-based cardiac patches for myocardial infarction therapy:
Recent advances and challenges. Mater Today Bio. 29:1013312024.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Walker BW, Lara RP, Yu CH, Sani ES,
Kimball W, Joyce S and Annabi N: Engineering a naturally-derived
adhesive and conductive cardiopatch. Biomaterials. 207:89–101.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Wu C, Zhang Y, Xu Y, Long L, Hu X, Zhang J
and Wang Y: Injectable polyaniline nanorods/alginate hydrogel with
AAV9-mediated VEGF overexpression for myocardial infarction
treatment. Biomaterials. 296:1220882023. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Alvarez-Lorenzo C, Grinberg VY, Burova TV
and Concheiro A: Stimuli-sensitive cross-linked hydrogels as drug
delivery systems: Impact of the drug on the responsiveness. Int J
Pharm. 579:1191572020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Streian CG, Novaconi RC, Munteanu IR,
Manzur AR, Merce AG, Boca MI, Falnita LS, Dima CN, Merce AP,
Pescariu SA, et al: Mechanical complications after acute myocardial
infarction: A Shock-Stage and Timing-based management framework. J
Clin Med. 15:23992026. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Bi S, Yu L and Gu Y: Inflammatory
signalling pathways and non-coding RNAs in myocardial infarction:
Insights into pathogenesis and therapeutic opportunities. Folia
Morphol (Warsz). 84:816–839. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Young JL and Engler AJ: Hydrogels with
time-dependent material properties enhance cardiomyocyte
differentiation in vitro. Biomaterials. 32:1002–1009. 2011.
View Article : Google Scholar
|
|
71
|
Traverse JH, Henry TD, Dib N, Patel AN,
Pepine C, Schaer GL, DeQuach JA, Kinsey AM, Chamberlin P and
Christman KL: First-in-Man study of a cardiac extracellular matrix
hydrogel in early and late myocardial infarction patients. JACC
Basic Transl Sci. 4:659–669. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Dong R, Zhao X, Guo B and Ma PXL:
Self-Healing conductive injectable hydrogels with antibacterial
activity as cell delivery carrier for cardiac cell therapy. ACS
Appl Mater Interfaces. 8:17138–17150. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Song M, Jang H, Lee J, Kim JH, Kim SH, Sun
K and Park Y: Regeneration of chronic myocardial infarction by
injectable hydrogels containing stem cell homing factor SDF-1 and
angiogenic peptide Ac-SDKP. Biomaterials. 35:2436–2445. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Yi B, Xu Y, Wang X, Wang G, Li S, Xu R,
Liu X and Zhou Q: Overview of injectable hydrogels for the
treatment of myocardial infarction. Cardiovasc Innov Appl.
9:2024.
|
|
75
|
Xing M, Bian S, Li B, Yang Z and Li J:
Functional peptide hydrogel for the synergistic treatment of
atherosclerosis based on macrophage autophagy induction and
Anti-inflammation. ACS Materials Lett. 6:384–399. 2024. View Article : Google Scholar
|
|
76
|
Firoozi S, Pahlavan S, Ghanian MH, Rabbani
S, Tavakol S, Barekat M, Yakhkeshi S, Mahmoudi E, Soleymani M and
Baharvand H: A cell-free SDKP-conjugated Self-assembling peptide
hydrogel sufficient for improvement of myocardial infarction.
Biomolecules. 10:2052020. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Purcell BP, Barlow SC, Perreault PE,
Freeburg L, Doviak H, Jacobs J, Hoenes A, Zellars KN, Khakoo AY,
Lee T, et al: Delivery of a matrix metalloproteinase-responsive
hydrogel releasing TIMP-3 after myocardial infarction: Effects on
left ventricular remodeling. Am J Physiol Heart Circ Physiol.
315:H814–H825. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Paul A, Hasan A, Kindi HA, Gaharwar AK,
Rao VT, Nikkhah M, Shin SR, Krafft D, Dokmeci MR, Shum-Tim D and
Khademhosseini A: Injectable graphene oxide/hydrogel-based
angiogenic gene delivery system for vasculogenesis and cardiac
repair. ACS Nano. 8:8050–8062. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Davidson SM, Takov K and Yellon DM:
Exosomes and cardiovascular protection. Cardiovasc Drugs Ther.
31:77–86. 2017. View Article : Google Scholar :
|
|
80
|
Emanueli C, Shearn AI, Angelini GD and
Sahoo S: Exosomes and exosomal miRNAs in cardiovascular protection
and repair. Vascul Pharmacol. 71:24–30. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Zhang Y, Hu YW, Zheng L and Wang Q:
Characteristics and roles of exosomes in cardiovascular disease.
DNA Cell Biol. 36:202–211. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Chen CW, Wang LL, Zaman S, Gordon J, Arisi
MF, Venkataraman CM, Chung JJ, Hung G, Gaffey AC, Spruce LA, et al:
Sustained release of endothelial progenitor cell-derived
extracellular vesicles from shear-thinning hydrogels improves
angiogenesis and promotes function after myocardial infarction.
Cardiovasc Res. 114:1029–1040. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Waters R, Alam P, Pacelli S, Chakravarti
AR, Ahmed RPH and Paul A: Stem cell-inspired secretome-rich
injectable hydrogel to repair injured cardiac tissue. Acta
Biomater. 69:95–106. 2018. View Article : Google Scholar
|
|
84
|
Sharma V, Manhas A, Gupta S, Dikshit M,
Jagavelu K and Verma RS: Fabrication, characterization and in vivo
assessment of cardiogel loaded chitosan patch for myocardial
regeneration. Int J Biol Macromol. 222:3045–3056. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Wang T, Jiang XJ, Tang QZ, Li XY, Lin T,
Wu DQ, Zhang XZ and Okello E: Bone marrow stem cells implantation
with alpha-cyclodextrin/MPEG-PCL-MPEG hydrogel improves cardiac
function after myocardial infarction. Acta Biomater. 5:2939–2944.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Melchiorri AJ, Hibino N and Fisher JP:
Strategies and techniques to enhance the in situ endothelialization
of small-diameter biodegradable polymeric vascular grafts. Tissue
Eng Part B Rev. 19:292–307. 2013. View Article : Google Scholar
|
|
87
|
Abbott WM, Callow A, Moore W, Rutherford
R, Veith F and Weinberg S: Evaluation and performance standards for
arterial prostheses. J Vasc Surg. 17:746–756. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Budd JS, Allen KE, Hartley G and Bell PR:
The effect of preformed confluent endothelial cell monolayers on
the patency and thrombogenicity of small calibre vascular grafts.
Eur J Vasc Surg. 5:397–405. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Pasic M, Müller-Glauser W, von Segesser
LK, Lachat M, Mihaljevic T and Turina MI: Superior late patency of
small-diameter Dacron grafts seeded with omental microvascular
cells: An experimental study. Ann Thorac Surg. 58:677–683. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Demiri EC, Iordanidis SL and Mantinaos CF:
Experimental use of prosthetic grafts in microvascular surgery.
Handchir Mikrochir Plast Chir. 31:102–106. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Ciolacu DE, Nicu R and Ciolacu F: Natural
polymers in heart valve tissue engineering: Strategies, advances
and challenges. Biomedicines. 10:10952022. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Coenen AMJ, Bernaerts KV, Harings JAW,
Jockenhoevel S and Ghazanfari S: Elastic materials for tissue
engineering applications: Natural, synthetic, and hybrid polymers.
Acta Biomater. 79:60–82. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Taghizadeh B, Ghavami L, Derakhshankhah H,
Zangene E, Razmi M, Jaymand M, Zarrintaj P, Zarghami N, Jaafari MR,
Moallem Shahri M, et al: Biomaterials in valvular heart diseases.
Front Bioeng Biotechnol. 8:5292442020. View Article : Google Scholar
|
|
94
|
Lee JM, Courtman DW and Boughner DR: The
glutaraldehyde-stabilized porcine aortic valve xenograft. I.
Tensile viscoelastic properties of the fresh leaflet material. J
Biomed Mater Res. 18:61–77. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Spina M, Ortolani F, El Messlemani A,
Gandaglia A, Bujan J, Garcia-Honduvilla N, Vesely I, Gerosa G,
Casarotto D, Petrelli L, et al: Isolation of intact aortic valve
scaffolds for heart-valve bioprostheses: Extracellular matrix
structure, prevention from calcification, and cell repopulation
features. J Biomed Mater Res A. 67:1338–1350. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Steinhoff G, Stock U, Karim N, Mertsching
H, Timke A, Meliss RR, Pethig K, Haverich A and Bader A: Tissue
engineering of pulmonary heart valves on allogenic acellular matrix
conduits: In vivo restoration of valve tissue. Circulation.
102:III50–III55. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Kniebs C, Kreimendahl F, Köpf M, Fischer
H, Jockenhoevel S and Thiebes AL: Influence of different cell types
and sources on Pre-Vascularisation in fibrin and Agarose-collagen
gels. Organogenesis. 16:14–26. 2020. View Article : Google Scholar :
|
|
98
|
Shah DN, Recktenwall-Work SM and Anseth
KS: The effect of bioactive hydrogels on the secretion of
extracellular matrix molecules by valvular interstitial cells.
Biomaterials. 29:2060–2072. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Ku CH, Johnson PH, Batten P, Sarathchandra
P, Chambers RC, Taylor PM, Yacoub MH and Chester AH: Collagen
synthesis by mesenchymal stem cells and aortic valve interstitial
cells in response to mechanical stretch. Cardiovasc Res.
71:548–556. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Sales VL, Mettler BA, Engelmayr GC Jr,
Aikawa E, Bischoff J, Martin DP, Exarhopoulos A, Moses MA, Schoen
FJ, Sacks MS and Mayer JE Jr: Endothelial progenitor cells as a
sole source for ex vivo seeding of tissue-engineered heart valves.
Tissue Eng Part A. 16:257–267. 2010. View Article : Google Scholar
|
|
101
|
Cebotari S, Lichtenberg A, Tudorache I,
Hilfiker A, Mertsching H, Leyh R, Breymann T, Kallenbach K, Maniuc
L, Batrinac A, et al: Clinical application of tissue engineered
human heart valves using autologous progenitor cells. Circulation.
114(1 Suppl): I132–I137. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Petsche Connell J, Camci-Unal G,
Khademhosseini A and Jacot JG: Amniotic fluid-derived stem cells
for cardiovascular tissue engineering applications. Tissue Eng Part
B Rev. 19:368–379. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Choi A, Seo KD, Yoon H, Han SJ and Kim DS:
Bulk poly(N-isopropylacrylamide) (PNIPAAm) thermoresponsive cell
culture platform: Toward a new horizon in cell sheet engineering.
Biomater Sci. 7:2277–2287. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Wen C, Zhang J, Li Y, Zheng W, Liu M, Zhu
Y, Sui X, Zhang X, Han Q, Lin Y, et al: A zwitterionic hydrogel
coated titanium surface with high-efficiency endothelial cell
selectivity for rapid re-endothelialization. Biomater Sci.
8:5441–5451. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Chen Y, Gao P, Huang L, Tan X, Zhou N,
Yang T, Qiu H, Dai X, Michael S, Tu Q, et al: A tough nitric
oxide-eluting hydrogel coating suppresses neointimal hyperplasia on
vascular stent. Nat Commun. 12:70792021. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Peng X, Wang X, Cheng C, Zhou X, Gu Z, Li
L, Liu J and Yu X: Bioinspired, artificial, small-diameter vascular
grafts with selective and rapid endothelialization based on an
amniotic Membrane-derived hydrogel. ACS Biomater Sci Eng.
6:1603–1613. 2020. View Article : Google Scholar
|
|
107
|
Kang MK, Heo SH and Yoon JK: In-Stent
Re-Endothelialization Strategies: Cells, extracellular matrix, and
extracellular vesicles. Tissue Eng Part B Rev. 31:317–330.
2025.
|
|
108
|
Tong Q, Sun A, Wang Z, Li T, He X, Qian Y
and Qian Z: Hybrid heart valves with VEGF-loaded zwitterionic
hydrogel coating for improved anti-calcification and
re-endothelialization. Mater Today Bio. 17:1004592022. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Wang L, Xu R, Meng L, Zhang Q, Qian Z,
Chen J and Pan C: A fucoidan-loaded hydrogel coating for enhancing
corrosion resistance, hemocompatibility and endothelial cell growth
of magnesium alloy for cardiovascular stents. Biomater Adv.
163:2139602024. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Yi S, Karabin NB, Zhu J, Bobbala S, Lyu H,
Li S, Liu Y, Frey M, Vincent M and Scott EA: An Injectable hydrogel
platform for sustained delivery of Anti-inflammatory nanocarriers
and induction of regulatory T cells in atherosclerosis. Front
Bioeng Biotechnol. 8:5422020. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Sayegh MN, Cooney KA, Han WM, Wang L,
Strobel F, Hansen LM, García AJ and Levit RD: A hydrogel strategy
to augment tissue adenosine to improve hindlimb perfusion.
Arterioscler Thromb Vasc Biol. 41:e314–e324. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Zhang Y, Xiong TY and Feng Y: Current
status and challenges of valvular heart disease interventional
therapy. Cardiol Discovery. 2:97–113. 2022. View Article : Google Scholar
|
|
113
|
Cannegieter SC, Rosendaal FR and Briët E:
Thromboembolic and bleeding complications in patients with
mechanical heart valve prostheses. Circulation. 89:635–641. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Fann JI, Miller DC, Moore KA, Mitchell RS,
Oyer PE, Stinson EB, Robbins RC, Reitz BA and Shumway NE:
Twenty-year clinical experience with porcine bioprostheses. Ann
Thorac Surg. 62:1301–1311. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Schoen FJ and Levy RJ: Tissue heart
valves: Current challenges and future research perspectives. J
Biomed Mater Res. 47:439–465. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Siddiqui RF, Abraham JR and Butany J:
Bioprosthetic heart valves: Modes of failure. Histopathology.
55:135–144. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Yacoub MH and Takkenberg JJ: Will heart
valve tissue engineering change the world? Nat Clin Pract
Cardiovasc Med. 2:60–61. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Masoumi N, Johnson KL, Howell MC and
Engelmayr GC Jr: Valvular interstitial cell seeded poly(glycerol
sebacate) scaffolds: Toward a biomimetic in vitro model for heart
valve tissue engineering. Acta Biomater. 9:5974–5988. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Neuenschwander S and Hoerstrup SP: Heart
valve tissue engineering. Transpl Immunol. 12:359–365. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Vesely I: Heart valve tissue engineering.
Circ Res. 97:743–755. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Flanagan TC, Cornelissen C, Koch S,
Tschoeke B, Sachweh JS, Schmitz-Rode T and Jockenhoevel S: The in
vitro development of autologous fibrin-based tissue-engineered
heart valves through optimised dynamic conditioning. Biomaterials.
28:3388–3397. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Green JJ and Elisseeff JH: Mimicking
biological functionality with polymers for biomedical applications.
Nature. 540:386–394. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Burdick JA and Murphy WL: Moving from
static to dynamic complexity in hydrogel design. Nat Commun.
3:12692012. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Seliktar D: Designing cell-compatible
hydrogels for biomedical applications. Science. 336:1124–1128.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Li J, Qiao W, Liu Y, Lei H, Wang S, Xu Y,
Zhou Y, Wen S, Yang Z, Wan W, et al: Facile engineering of
interactive double network hydrogels for heart valve regeneration.
Nat Commun. 15:74622024. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
He L, Wang W, Li Q, Jiang Y, Xia Z, Xia Z,
Li J and Dong Q: VEGF-loaded HANB/F127DA photosensitive hydrogel in
combination with exercise training: For improving post-myocardial
infarction myocardial remodeling. Biomater Adv. 183:2147672026.
View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Huangfu Y, Zhang Y, Zhang Y, Wang S, Ding
S, Gao R, Li H, Ju W, Zhang C, Huang P, et al: Spatially
heterogeneous microgel-annealed PRP-derived fibrin hydrogel
promotes coordinated vasculogenesis and angiogenesis after
myocardial infarction. Acta Biomater. 213:182–199. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Jia Y, Yin T, Wang Z, Chen L, Fan H, Wu J,
Yu Q, Zhang Y and Shen Z: Injectable alginate composite hydrogel
with spatiotemporal codelivery of pro-angiogenic and anti-fibrotic
agents for synergistic myocardial repair. Mater Today Bio.
37:1028542026. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Tong J, Sun D, Sun J, Zhang J, Chen M, Liu
X, Zhang R, Zhang F, Zheng C, Wei Y, et al: Intelligent responsive
PVA hydrogel loaded with composite MXene nanozyme enables efficient
myocardial infarction repair by disrupting the oxidative
stress-inflammation cascade. Mater Today Bio. 35:1025562025.
View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Fan P, Liu Y, Qian X, Li J, Xu Y, Qiu X,
Tong L, Tong F, Fan Z, Zheng Y, et al: An intelligent nanoreservoir
system promotes heart valve regeneration via ROS scavenging and
immunomodulation. Bioact Mater. 55:205–223. 2026.
|
|
131
|
Wang W, He L, Li X, Zhou Z, Xia Z, Xia Z,
Dong Q and Li J: Gelatin-based hydrogel patch by promoting M2
macrophage polarization to reduce inflammation and fibrosis
alleviate post-myocardial infarction ventricular remodeling. Int J
Biol Macromol. 322:1466522025. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Chen W, Wang C, Liu W, Zhao B, Zeng Z,
Long F, Wang C, Li S, Lin N and Zhou J: A
Matrix-Metalloproteinase-Responsive hydrogel system for modulating
the immune microenvironment in myocardial infarction. Adv Mater.
35:e22090412023. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Wang D, Xu A, Su H and Zhang Y, Jiang L,
Wang Y, Liang G and Zhang Y: Sustained release of dual p38
inhibitors via supramolecular hydrogels to enhance cardiac repair
after MI/R injury. Biomaterials. 326:1236702026. View Article : Google Scholar
|
|
134
|
Zhou W, Tang Q, Wang S, Ding L, Chen M,
Liu H, Wu Y, Xiong X, Shen Z and Chen W: Local thiamet-G delivery
by a thermo-sensitive hydrogel confers ischemic cardiac repair via
myeloid M2-like activation in a STAT6 O-GlcNAcylation-dependent
manner. Int Immunopharmacol. 131:1118832024. View Article : Google Scholar
|
|
135
|
Zhang L, Shao L, Li J, Zhang Y and Shen Z:
Annexin A1-Loaded alginate hydrogel promotes cardiac repair via
modulation of macrophage phenotypes after myocardial infarction.
ACS Biomater Sci Eng. 10:3232–3241. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Yuan L, Hu Z, Peng S, Li N, Wu H and Wang
Y: Molecular mechanisms of myocardial repair and cardiac function
improvement with Hydrogel-mediated Macrophage-derived exosome
delivery. FASEB J. 39:e709772025. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Niu H, Liu Z, Guan Y, Wen J, Dang Y and
Guan J: Harnessing synergistic effects of MMP-2 Inhibition and bFGF
to simultaneously preserve and vascularize cardiac extracellular
matrix after myocardial infarction. Acta Biomater. 191:189–204.
2025. View Article : Google Scholar :
|
|
138
|
You T, Zhang Y, Su H, Wang N, Zhang X,
Anwaier S, Long X, Han L, Wu Y, Liang J, et al: Ameliorating
post-infarction myocardial fibrosis and cardiac function via
ROS-responsive hydrogel-mediated IL-11 antibody delivery. Bioact
Mater. 60:527–538. 2026.PubMed/NCBI
|
|
139
|
Luo Q, Cheng N, Yang Y, Shao N, Nie T,
Chen J, Huang C, Zhang S, Huang Y, Ieong CM, et al: Multi-stage
cooperative ROS-responsive hydrogel platform for drug delivery in
myocardial ischemia-reperfusion injury repair. Mater Today Bio.
32:1018542025. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Zhang Y, Xu Y, Wu C, Chen S, Chen Z, Qin
F, Hu X, Zhang J and Wang Y: Injectable conductive hydrogel patch
with spatiotemporally tailored asymmetric adhesion for myocardial
infarction repair. Adv Mater. 38:e108242026. View Article : Google Scholar
|
|
141
|
Cui Z, Ni NC, Wu J, Du GQ, He S, Yau TM,
Weisel RD, Sung HW and Li RK: Polypyrrole-chitosan conductive
biomaterial synchronizes cardiomyocyte contraction and improves
myocardial electrical impulse propagation. Theranostics.
8:2752–2764. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Xu Z, Li X, Mi X and Lin Y: Exosomes
loaded stimuli responsive conductive hydrogel restores cardiac
function post-myocardial infarction via SIRT1/p53-mediated
anti-inflammatory mechanism: Mechanistic insights into
cardioprotection. Biomater Adv. 180:2146102026. View Article : Google Scholar
|
|
143
|
Wang S, Zhao X, Zhan Y, Liang J, Shi J, Gu
J and Wang H: A ROS-Scavenging and Conductive Hydrogel-based
cardiac patch with controlled release of edaravone for myocardial
infarction treatment assisted by electrical stimulation.
Biomacromolecules. 26:7930–7943. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Tran DL, Phan HN, Nguyen HTA, Nguyen HT,
Nguyen LM, Phung VT and Nguyen DH: An injectable conductive
hydrogel enabling sustained nitric oxide generation for cardiac
tissue regeneration. J Mater Chem B. 14:4330–4345. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Luque GC, Picchio ML, Daou B,
Lasa-Fernandez H, Criado-Gonzalez M, Querejeta R, Filgueiras-Ramas
D, Prato M, Mecerreyes D, Ruiz-Cabello J, et al: Printable
Poly(3,4-ethylen edioxythiophene)-based conductive patches for
cardiac tissue remodeling. ACS Appl Mater Interfaces.
16:34467–34479. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Xu Z, Chen J, Shu L, Hong W, Mo Y, Wang J,
Liu Y, Wong WT, Tsang SY, Tan N, et al: Fabrication of a
conductive, ionic liquid functionalized, oxygen-generating hydrogel
loaded with ADSC-derived exosomes to enhance angiogenesis and
cardiac repair after acute myocardial infarction. Theranostics.
16:1997–2018. 2026. View Article : Google Scholar :
|
|
147
|
Yu R, Zhao R, Guo D, Shi M, Wen H, Niu X,
Ni P, Liu M, Luo H, Qi B, et al: Supramolecular antioxidant
conductive injectable hydrogel encapsulating L-arginine for
synergistic modulation of myocardial infarction. J Control Release.
390:1145522026. View Article : Google Scholar
|
|
148
|
Abdollahiyan P, Baradaran B, de la Guardia
M, Oroojalian F and Mokhtarzadeh A: Cutting-edge progress and
challenges in stimuli responsive hydrogel microenvironment for
success in tissue engineering today. J Control Release.
328:514–531. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Sood N, Bhardwaj A, Mehta S and Mehta A:
Stimuli-responsive hydrogels in drug delivery and tissue
engineering. Drug Deliv. 23:758–780. 2016. View Article : Google Scholar
|
|
150
|
Xue K, Wang X, Yong PW, Young DJ, Wu YL,
Li Z and Loh XJ: Hydrogels as emerging materials for translational
biomedicine. Adv Therap. 2:18000882019. View Article : Google Scholar
|
|
151
|
Zhao XY, Li PC, Chen YM, Cao K, Wei W,
Aziz Y and Zrínyi M: Adipose tissue engineering biomaterials: Smart
scaffolds, vascularization, and clinical frontiers. Biomolecules.
16:3622026. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Tong S, Chen J, Li Y and Zhao W: Emerging
gel technologies for atherosclerosis research and intervention.
Gels. 12:802026. View Article : Google Scholar : PubMed/NCBI
|
|
153
|
Felisbino MB, Rubino M, Travers JG,
Schuetze KB, Lemieux ME, Anseth KS, Aguado BA and McKinsey TA:
Substrate stiffness modulates cardiac fibroblast activation,
senescence, and proinflammatory secretory phenotype. Am J Physiol
Heart Circ Physiol. 326:H61–H73. 2024.
|
|
154
|
Shayan M, Huang MS, Navarro R, Chiang G,
Hu C, Oropeza BP, Johansson PK, Suhar RA, Foster AA, LeSavage BL,
et al: Elastin-like protein hydrogels with controllable stress
relaxation rate and stiffness modulate endothelial cell function. J
Biomed Mater Res A. 111:896–909. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Krebs C, Macara LM, Leiser R, Bowman AW,
Greer IA and Kingdom JC: Intrauterine growth restriction with
absent end-diastolic flow velocity in the umbilical artery is
associated with maldevelopment of the placental terminal villous
tree. Am J Obstet Gynecol. 175:1534–1542. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Page G, Ratchada P, Miron Y, Steiner G,
Ghetti A, Miller PE, Reynolds JA, Wang K, Greiter-Wilke A,
Polonchuk L, et al: Human ex-vivo action potential model for
pro-arrhythmia risk assessment. J Pharmacol Toxicol Methods.
81:183–195. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
Nash KM, Boe BA, Carrillo SA, Harrison A,
Iwaki R, Kelly J, Kirkton RD, Krishnamurthy R, Lawson JH, Matsuzaki
Y, et al: Evaluation of tissue-engineered human acellular vessels
as a Blalock-Taussig-Thomas shunt in a juvenile primate model.
JTCVS Open. 15:433–445. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Kelsey LJ, Fry DM and VanderKolk WE:
Thrombosis risk in the trauma patient. Prevention and treatment.
Hematol Oncol Clin North Am. 14:417–430. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
159
|
Cutiongco MF, Anderson DE, Hinds MT and
Yim EK: In vitro and ex vivo hemocompatibility of off-the-shelf
modified poly(vinyl alcohol) vascular grafts. Acta Biomater.
25:97–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Ren H, Pan Z, Yuan J and Liu J:
Zwitterionic hydrogel coatings enhance anti-fouling and
anti-thrombogenicity of decellularized swim bladder for
bioprosthetic heart valves. Colloids Surf B Biointerfaces.
260:1153492026. View Article : Google Scholar
|
|
161
|
Liu Y, Zhang J, Zhang Y, Yoon HY, Jia X,
Roman M and Johnson BN: Accelerated engineering of optimized
functional composite hydrogels via High-throughput experimentation.
ACS Appl Mater Interfaces. 15:52908–52920. 2023.PubMed/NCBI
|
|
162
|
Pleshakov PS, Shmakov SV, Filatov NA and
Bukatin AS: Negative pressure actuated microfluidic droplet
generation enables High-throughput and robust synthesis of
cell-laden alginate microgels. ACS Biomater Sci Eng. 12:180–189.
2026. View Article : Google Scholar
|
|
163
|
Zheng F, Tian R, Lu H, Liang X, Shafiq M,
Uchida S, Chen H and Ma M: Droplet microfluidics powered hydrogel
microparticles for stem Cell-mediated biomedical applications.
Small. 20:e24014002024. View Article : Google Scholar : PubMed/NCBI
|
|
164
|
SA Bento C, Gaspar MC, Coimbra P, de Sousa
HC and EM Braga M: A review of conventional and emerging
technologies for hydrogels sterilization. Int J Pharm.
634:1226712023. View Article : Google Scholar
|
|
165
|
Gil-Cabrerizo P, Simon-Yarza T, Garbayo E
and Blanco-Prieto MJ: Navigating the landscape of RNA delivery
systems in cardiovascular disease therapeutics. Adv Drug Deliv Rev.
208:1153022024. View Article : Google Scholar : PubMed/NCBI
|