Introduction
The liver is a vital and intricate organ within the
human body, undertaking several important physiological functions,
including metabolizing carbohydrates and lipids, detoxifying drugs,
secreting bile, and synthesizing plasma proteins, which are
irreplaceable for maintaining homeostasis in the body's internal
environment and overall health (1,2).
Liver disease is characterized by injury to hepatocytes,
infiltration by inflammatory cells, and activation of hepatic
stellate cells (HSCs). It covers an extensive range of conditions,
ranging from acute liver damage and chronic liver conditions to
end-stage liver disease (ESLD). In clinical settings, the prevalent
types of liver disease consist of viral hepatitis, non-alcoholic
fatty liver disease (NAFLD), liver injury, liver fibrosis (LF),
liver cirrhosis (LC) and liver cancer (3,4).
In modern society, the global number of liver
disease patients continues to rise, imposing a heavy economic
burden worldwide (5-7). According to the global
epidemiological statistics of liver disease in 2023, more than 2
million individuals perish annually because of liver-related
conditions, representing 4% of the total number of deaths in the
world, and ranking 11th among the causes of death in the world. LC
and liver cancer account for the highest proportion of deaths
(8). However, a large number of
the early manifestations of liver disease lack specificity. The
diagnosis of liver disease is highly dependent on liver biopsy.
Given that an invasive approach is inappropriate for widespread
screening, the disease often progresses to the ESLD stage (9). Despite the use of a range of drugs,
such as antioxidant medications, including glutathione (GSH),
choleretic agents, including ursodeoxycholic acid (10), and statins, including simvastatin
(11), and corticosteroids
(12) in current treatments,
most patients ultimately and inevitably progress to ESLD.
Traditional treatments, such as resection, transplantation and
systemic chemotherapy, have certain limitations. For example, liver
transplantation, a treatment for ESLD, faces the dual challenges of
high cost and a shortage of donor organs (13-15). Transplantation therapy involving
mesenchymal stem cells (MSCs) has undergone assessment in numerous
clinical trials. To a certain extent, it has demonstrated safety
and is considered a promising avenue for cellular therapy of liver
disease (16). However,
transplanted MSCs are at risk of unintended differentiation, may
impair antitumor immune responses, and even have a tendency to form
new arteries and thus promote tumor development and spread
(17). Therefore, developing
new, highly effective, and low-toxicity drugs for liver disease
intervention remains an important task for the medical community in
the modern healthcare system.
Various factors, including viruses, alcohol,
metabolites, toxins and other pathogens, predispose individuals to
liver diseases. Metabolic dysfunction, assessed using different
indicators such as insulin resistance, disturbances in bile acid
metabolism, imbalances in the intestinal flora, and elevated uric
acid levels, can lead to metabolic-associated steatohepatitis
(18,19). NAFLD is characterized by the
abnormal accumulation of fat within hepatocytes, accompanied with
the abnormal inactivation of adenosine monophosphate-activated
protein kinase (AMPK) and abnormal activation of nuclear factor κB
(NF-κB) (20,21). This phenomenon further
exacerbates hepatic inflammatory responses and induces oxidative
damage to the liver. The key pathogenic mechanism of LF is abnormal
HSC activation. Upon activation, these cells trigger the excessive
deposition of extracellular matrix (ECM) proteins such as collagen
and fibronectin (FN), subsequently inducing hepatocyte apoptosis
and cellular senescence and ultimately leading to LF development
(22). The pathogenesis of
hepatocellular carcinoma (HCC) is more complex than that of liver
injury. HCC primarily manifests through the proliferation of cancer
cells and the apoptosis of normal cells, while liver injury
involves pathological processes such as oxidative stress,
inflammatory responses and cellular apoptosis (23,24).
Chinese medicines have garnered significant
attention on account of their minimal toxicity and side effects,
and excellent tolerability. Radix Astragali (RA),
predominantly sourced from the dried root of Astragalus
membranaceous (A. membranaceous), a plant belonging to
the legume family, has been used in pharmacological studies or as a
dietary supplement in some countries (25). Astragaloside IV (AS-IV), a
natural saponin obtained from RA, possesses low toxicity and
various bioactivities, including anti-inflammatory, antioxidant,
antiapoptotic and anticancer. These activities are important in
treating neurological, cardiovascular and metabolic diseases, and
cancer (26). These
comprehensive summaries and exploratory research findings have
substantially reinforced the medicinal value and attention from
investigators of AS-IV. In recent years, the therapeutic potential
of AS-IV in liver diseases has gradually attracted widespread
attention from researchers. A number of in vivo and in
vitro studies have confirmed that AS-IV can exert
hepatoprotective effects in liver diseases via multiple signaling
pathways.
Consequently, the present study conducts a
comprehensive review of the hepatoprotective effects of AS-IV in
various diseases, deeply analyzes the molecular mechanism
underlying its role in liver disease, and summarizes the measures
to improve its bioavailability. The aim is to provide innovative
insights and rationale for the future development of AS-IV as a
prospective new drug for treating liver diseases. In contrast to
recently published reviews (27), the present review systematically
summarizes the chemical structure, physicochemical properties and
extraction methods of AS-IV. Regarding hepatoprotective mechanisms,
liver injury was classified into four types, providing an updated
analysis of iron overload-induced liver damage, and the synergistic
antifibrotic effects of AS-IV combined with ferulic acid were
reviewed. Moreover, the pharmacokinetics, toxicology and
nano-delivery systems of AS-IV were comprehensively discussed,
focusing on translational applications.
Overview of AS-IV
Sources and background
A. membranaceous, a common qi-tonifying herb,
has had its medicinal use documented since 'Shen Nong's Herbal
Classic,' written over 2,000 years ago in China (28). It is a member of the legume
family and has a wide geographical distribution across the Northern
Hemisphere, South America and Africa, featuring a distinctive plant
morphology with erect and well-branched stems and neatly arranged
leaflets on pinnately compound leaves (29). AS-IV is a natural saponin
extracted from the root of A. membranaceous, also known as
RA. The composition of RA varies by region and country. Its main
components include astragali polysaccharides, saponins and
flavonoids (25). AS-IV serves
as a marker substance for one of the aspects of quality control for
RA and its products in the Chinese Pharmacopoeia (2020 edition)
(30).
RA is used in the field of ethnopharmacology in
several countries in Asia, North America and Europe, such as China,
the United States and Russia (31). In clinical practice, numerous
proprietary and patented Chinese medicines and injections are
formulated using or contain RA, including Astragalus injection,
Astragalus polysaccharide injection, Yupingfeng Powder, Xuefu Zhuyu
Decoction and Huangqi Siwu Decoction (32,33). These preparations have shown
favorable application prospects in treating neurological,
cardiovascular, renal, gynecological and pulmonary disorders, and
organ injuries (26). RA is used
as a dietary product in China and is also classified as a legal
dietary supplement in the United States (34).
Chemical and physical properties
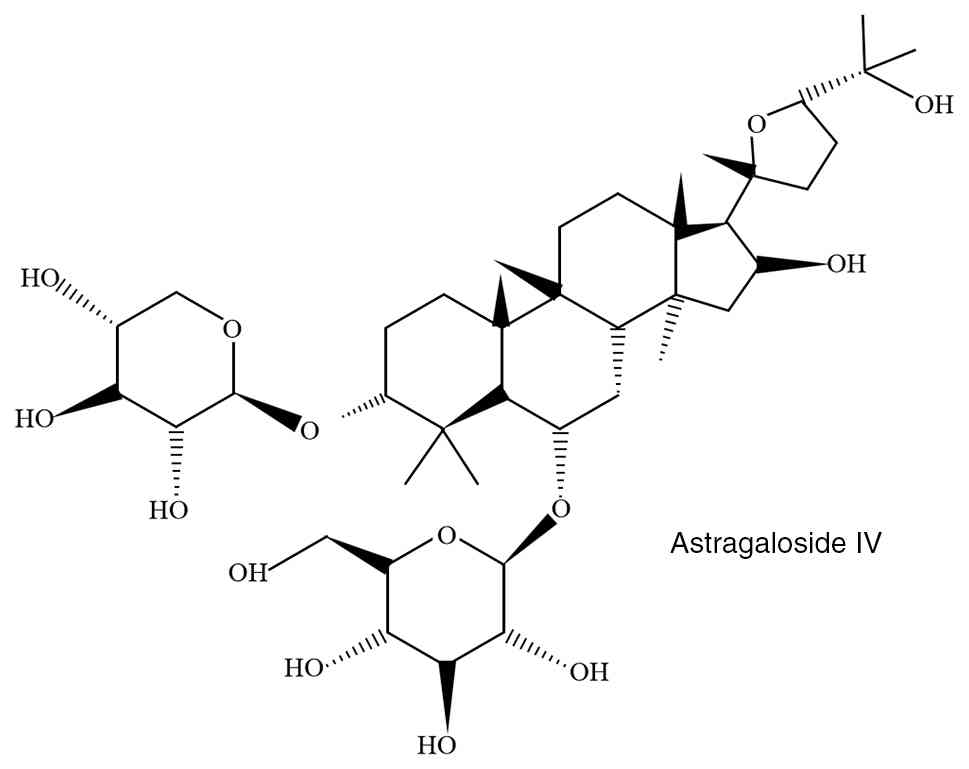
AS-IV appears as a white to yellow crystalline
powder (35) and has a chemical
name of 3-O-β-d-xylopyranosyl-6-O-β-glucopyranosyl-cyclostelli
feryl alcohol, molecular formula of
C41H68O14, and a relative
molecular mass of 784.97 g/mol (36). This compound has a high melting
point, ranging from 295-296°C. It is insoluble in water but
displays solubility in certain organic solvents such as ethanol,
methanol and acetone (37).
AS-IV belongs to the category of triterpenoid saponins and
pentacyclic triterpenoids, featuring a tetracyclic triterpenoid
saponin in the form of lanolin ester alcohol. This structural
configuration is vital because it underlies the manifestation of
its anti-inflammatory and antioxidant effects and ability to
improve lipid metabolism, thereby potentially exerting
hepatoprotective effects (38,39). The commonly employed extraction
methods include solvent extraction, ultrasound-assisted extraction,
microwave-assisted extraction, enzyme-assisted extraction,
supercritical fluid extraction and rapid extraction techniques
(40) [Fig. 1 (37)].
Pharmacological effects
AS-IV, an emerging natural compound in the medical
realm, is a highly promising nutritional therapeutic agent. It
displays an array of advantageous biological functions, such as
anti-inflammatory, antioxidant (41), antiapoptotic (42), anticancer (43) and antitumor (44). These properties hold promise for
its applications in neurological disorders such as stroke,
dementia, epilepsy and Alzheimer's disease (29). AS-IV is also of great
significance in cardioprotection. It may play a role, either
directly or indirectly, in the treatment of cardiac disorders. It
controls myocardial hypertrophy and fibrosis processes and
effectively reduces cardiomyocyte apoptosis (45-47). In addition, AS-IV shows
remarkable efficacy in combating diabetes and its complications
(48), along with certain
viruses (49). In the area of
intestinal health, it modulates intestinal function, alleviates
intestinal inflammation, and effectively restores damaged
intestinal barrier function (50,51). In the treatment of kidney and
gynecological diseases, AS-IV can ameliorate chronic
glomerulonephritis and triple-negative breast cancer by
participating in autophagy inhibition (52,53). Owing to its powerful antioxidant
and anti-inflammatory characteristics, AS-IV exhibits significant
protective effects against various lung diseases (54,55). These properties provide a strong
rationale for the evaluation of AS-IV as a potential therapeutic
option for various liver ailments.
Hepatoprotective effect of AS-IV
NAFLD
NAFLD belongs to the category of metabolic
syndromes. It is triggered by well-defined liver-damaging factors.
A prominent feature of NAFLD is the over-accumulation of fat in
hepatocytes, which is evident in conditions such as non-alcoholic
fatty liver, non-alcoholic steatohepatitis (NASH) and associated LC
(56). In general, non-alcoholic
fatty liver may progress to NASH, which in turn may eventually
progress to LC and liver cancer (57). NAFLD development is associated
with a variety of factors. The currently widely recognized
'multiple strike' hypothesis takes into account the synergistic
effects of fat build-up, lipotoxicity, inflammation, oxidative
stress, mitochondrial impairment, gut microbiota and genetic
elements (58). As shown in
NAFLD models, a diet rich in fat can trigger hepatic steatosis and
inflammation, which subsequently lead to significant oxidative
damage in the liver (59).
Palmitic acid, the most prevalent free fatty acid (FFA) in dietary
sources and the serum, contributes to hepatic steatosis and
exacerbates insulin resistance (60).
Zhai et al (61) successfully established a cellular
model of hepatic steatosis using FFA. They discovered that
FFA-induced lipid accumulation led to endoplasmic reticulum (ER)
stress, and triggered autophagy and inflammation. This ER stress
was significantly alleviated by AS-IV treatment. It reduced the
elevated expression of ER stress markers, such as glucose-regulated
protein 78, protein kinase R-like ER kinase, and C/EBP homologous
protein, and mitigated the increased nuclear translocation of these
markers (21,62). Liu et al (63) discovered that FFA induced the
blockage of autophagic fluxes, attenuating lipophagy. AS-IV
triggered autophagy within HepG2 cells by inhibiting the activation
of protein kinase B (Akt)/mammalian target of rapamycin (mTOR)
pathway, effectively attenuating FFA-induced lipid accumulation in
HepG2 cells and degrading excess intracellular lipids. Moreover,
AS-IV alleviates oxidative stress in hepatocytes. It reduces the
elevated levels of reactive oxygen species (ROS) and
malondialdehyde (MDA) and mitigates the significant decrease in GSH
peroxidase (Px) activity. And, AS-IV plays a role in hepatocyte
apoptosis inhibition by downregulating the mRNA and protein
expression levels of B-cell lymphoma/leukemia-2-associated X
protein (Bax) and upregulating the mRNA and protein expression
levels of B-cell lymphoma 2 (Bcl-2) (64). NAFLD is marked by the deposition
of hepatic fat within the liver, and prolonged deposition can give
rise to hepatic inflammation. AS-IV can mitigate the inflammatory
response by inhibiting the generation of inflammatory cytokines
such as interleukin-1β (IL-1β), interleukin-6 (IL-6) and tumor
necrosis factor-α (TNF-α). Toll-like receptor 4 (TLR4) can initiate
a series of injury-related immune responses. However, the
overexpression of the TLR4 signaling pathway leads to the
occurrence of immune-inflammatory responses, and AS-IV can inhibit
the overexpression of this pathway (64-67). AMPK functions as a crucial
regulator in hepatic lipogenesis, and acetyl-CoA carboxylase
phosphorylation is a direct target of AMPK. AS-IV dose-dependently
increased the phosphorylation of acetyl-CoA carboxylase (ACC) by
AMPK activation. The presence of adipogenic genes such as acc1,
scd1 and fas in sterol regulatory element-binding protein-1c
(SREBP-1c) reduces the accumulation of mature SREBP-1c in HepG2
cells exposed to FFA. It also inhibits the enhanced nuclear
translocation of SREBP-1c and downregulates adipogenic gene mRNA.
Co-processing with 5-amino-4-imidazolecarboxamide ribonucleotide
can further enhance this effect (68). The intestinal flora is essential
for maintaining physiological balance in the human body (69). When the population of bile salt
hydrolase flora decreases, AS-IV can inhibit diet-induced metabolic
damage, especially hepatic steatosis. AS-IV can also inhibit
intestinal farnesoid receptor (FXR) signaling, and this inhibition
is accompanied with a reduction in intestinal fibroblast growth
factor expression. Subsequently, hepatic FXR is activated. AS-IV
increases glucagon-like peptide-1 and promotes ceramide production.
All these effects collaborate to suppress the progression of
hepatic steatosis (61). In a
mouse model study of NAFLD, AS-IV reduced body weight gain in NAFLD
mice without reducing food intake. It also decreased the levels of
NAFLD markers aspartate aminotransferase (AST) and alanine
aminotransferase (ALT), eliminated the tendency of elevated
triglyceride (TG) and total cholesterol, and significantly reduced
the release of aminotransferases due to hepatocellular injury
(64,70).
All the aforementioned molecular effects of AS-IV
have been validated across heterogeneous experimental systems,
including in vitro fatty liver cell models, HepG2 cell
lines, primary mouse hepatocytes, and in vivo NAFLD mouse
and rat models. Comprehensive analysis of current evidence
demonstrates that, despite variations in experimental conditions,
these regulatory effects maintain an overall consistent trend.
AS-IV directly reduces fat accumulation, facilitates excess fat
degradation, and inhibits steatosis by regulating autophagy,
promoting AMPK activation, and synergizing with the gut microbiota.
Furthermore, it suppresses oxidative stress and hepatic
inflammation in hepatocytes, thereby alleviating NAFLD.
LF
LF is the outcome of a continuous wound-healing
response to chronic liver injury, and its main causes include
chronic hepatitis C virus (HCV) and hepatitis B virus (HBV)
infections, alcohol abuse that results in alcoholic liver disease
(ALD), NASH, and autoimmune diseases (71). The distinguishing feature of LF
is HSC activation, which subsequently triggers excessive ECM
accumulation, leading to fibrous scarring. If the disease
progresses further, fibrous scarring can transform into LC and
ESLD. LC is defined as the presence of regenerating hepatocellular
nodules in the liver, accompanied with a reduced hepatic blood
supply. Oxidative stress and inflammation are as important factors
in LF development (72,73).
Chen et al (74) revealed the protective effects of
AS-IV on LF, it downregulated collagen type I alpha 1 chain,
α-smooth muscle actin (α-SMA) and FN, thereby reducing the
excessive secretion and accumulation of ECM. AS-IV can also inhibit
the excessive pathological activation of the NF-κB signaling
pathway, thereby exerting antifibrotic effects. It can enhance the
expression levels of p65, p52 and p50, thus promoting the
senescence and apoptosis of activated HSC-T6 cells. Moreover, AS-IV
reduces the protein and mRNA expression of α-SMA, collagen
synthesis, and FN through mediated p38 MAPK. In turn, this process
inhibits HSC activation. AS-IV exhibits antioxidant properties and
could decrease the levels of ROS and lipid peroxide (75). Hydroxyproline content, one of the
indicators of LF, initially showed a decreasing trend after AS-IV
treatment. In vitro studies showed that the platelet-derived
growth factor-bb stimulated proliferation of HSC was significantly
inhibited by AS-IV (76). In the
bile duct ligation-induced LF model, the combined treatment of
AS-IV and ferulic acid (FA) effectively alleviated LF,
significantly reduced collagen deposition, and greatly improved the
pathological changes in the liver. Compared with AS-IV or FA alone,
the combination therapy was more effective in inhibiting HSC
activation and significantly enhanced the body's capacity to resist
oxidative stress. The reduction in MDA levels, elevation in GSH-Px,
and enhancement of superoxide dismutase (SOD) enzyme activity are
all attributed to AS-IV rather than FA. In addition, AS-IV
activates antioxidant defense mechanisms via the nuclear factor
erythroid 2-related factor 2 (Nrf2) signaling pathway and promotes
the phosphorylation of glycogen synthase kinase 3β (GSK-3β) at the
Ser9 site (77).
All the aforementioned molecular effects of AS-IV
have been validated across heterogeneous experimental systems,
including in vitro HSC-T6 cells and HCC cell lines, in
vivo models of the PS-induced LF rat model, the bile duct
ligation rat model, and the PSmad3C and Nrf2 mouse models.
Comprehensive analysis of current evidence demonstrates that,
despite variations in experimental conditions, these regulatory
effects maintain an overall consistent trend. AS-IV exerts
antifibrotic effects in vivo by inhibiting oxidative stress
and inflammation via the NF-κB and Nrf2 pathways. It also
suppresses the proliferation of HSC in vitro, and its
combined treatment with FA synergistically enhances the
anti-fibrotic effect. Compared with other antiviral drugs,
corticosteroids, immunosuppressive and antifibrotic agents, AS-IV
exhibits significant advantages, including a broad application
spectrum, high safety, multi-target regulation and low cost
(78,79) (Fig. 2).
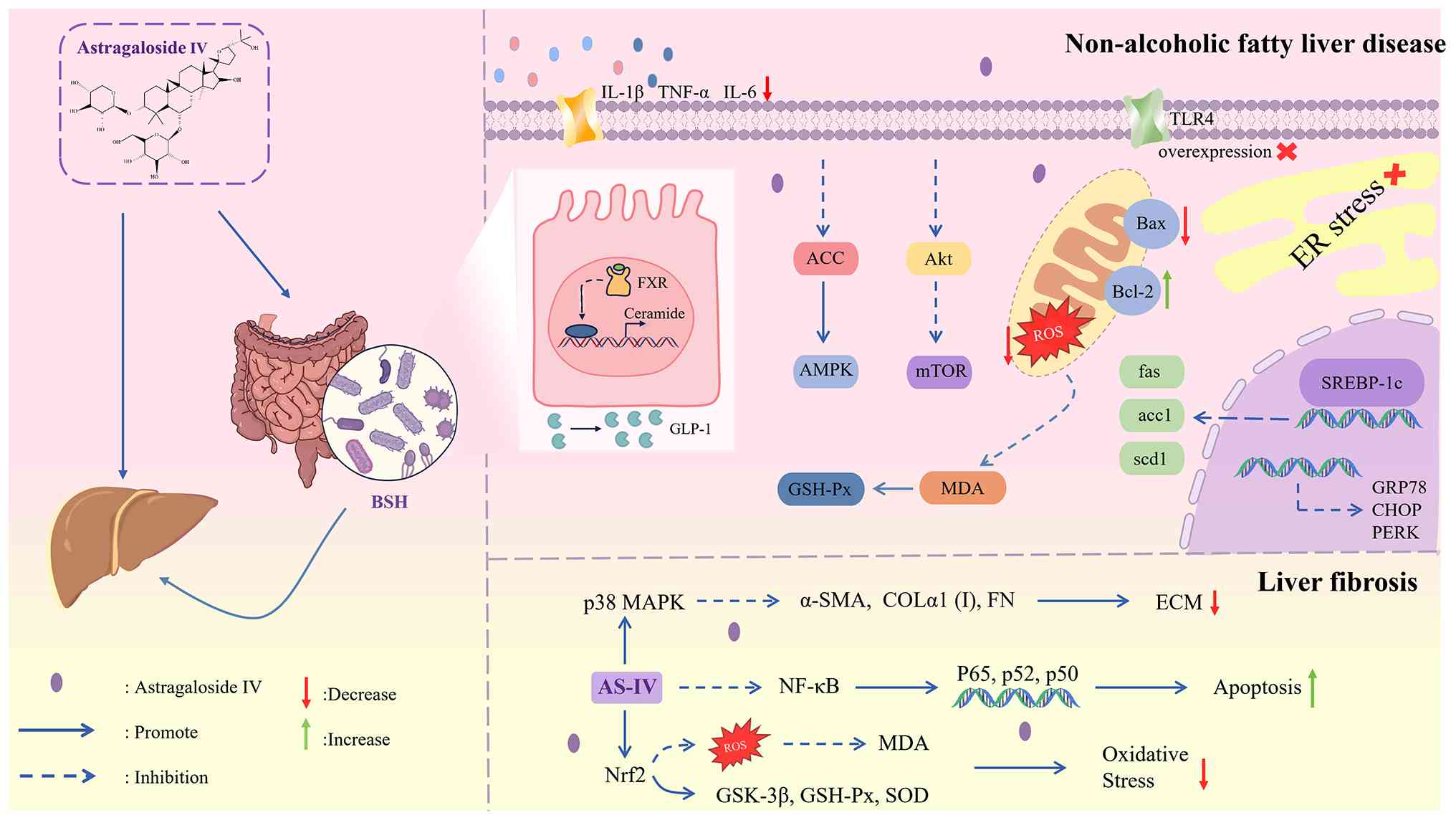 | Figure 2Mechanisms by which AS-Ⅳ ameliorates
non-alcoholic fatty liver disease and liver fibrosis. BSH, bile
salt hydrolase; IL-1β, interleukin-1β; TNF-α, tumor necrosis
factor-α; IL-6, interleukin-6; TLR4, toll-like receptor 4; FXR,
farnesoid x receptor; GLP-1, glucagon-like peptide-1; ACC,
acetyl-CoA carboxylase; AMPK, adenosine monophosphate-activated
protein kinase; GSH-Px, glutathione peroxidase; Akt, protein kinase
B; mTOR, mammalian target of rapamycin; MDA, malondialdehyde; Bax,
b-cell lymphoma/leukemia-2-associated X protein; Bax, B cell
lymphoma 2; ROS, reactive oxygen species; ER, endoplasmic
reticulum; SREBP-1c, sterol regulatory element-binding protein-1c;
GRP78, glucose-regulated protein 78; CHOP, c/edp homologous
protein; PERK, phosphorylated protein kinase-like ER kinase; MAPK,
mitogen-activated protein kinase; AS-IV, Astragaloside IV; Nrf2,
nuclear factor erythroid 2-related factor 2; α-SMA, α-smooth muscle
actin; COLα1 (I), collagen type I alpha 1 chain; FN, fibronectin;
NF-κB, nuclear factor κB; GSK-3β, glycogen synthase kinase 3β; SOD,
superoxide dismutase; ECM, extracellular matrix. |
HCC
Liver cancer, a common solid malignancy arising from
the liver, is the sixth most common type of cancer and the fourth
leading cause of cancer-related deaths worldwide (80). It encompasses HCC, intrahepatic
cholangiocarcinoma and fibrous laminar carcinoma. Among them, HCC
is the most common type of primary liver cancer, accounting for 90%
of all liver cancer cases (81-83). Numerous factors, including HBV
and HCV infections (84), NAFLD
(85), alcohol abuse (86) and exposure to aflatoxin (87,88), elevate the risk of developing
HCC. The common symptoms of HCC are abdominal pain, abdominal
distension, weight loss, fatigue, jaundice and vomiting (89). Its pathogenesis is intricate and
may involve alterations in the tumor microenvironment, inflammatory
response, oxidative stress, tissue hypoxia, hepatocyte necrosis,
regeneration related to fibrosis, and numerous molecular-level
changes (90,91). At present, surgical resection
remains the preferred treatment for HCC (92). AS-IV, a typical natural
antioxidant, exerts potential pharmacological effects against
various malignancies. It influences the development of HCC via four
principal mechanisms: (i) metabolic regulation, (ii)
immunomodulatory mechanism, (iii) apoptosis induction, and (iv)
inhibition of epithelial-mesenchymal transition (EMT). The specific
mechanisms are described below:
First, AS-IV can inhibit the malignant proliferation
of hepatoma cells by regulating glycolipid metabolism, thereby
breaking the abnormal metabolic homeostasis of tumor cells. A
recent study showed that AS-IV decreased glucose consumption,
lactate production and extracellular acidification rate (93). It also inhibits phosphoglycerate
mutase 1 (PGAM1) succinylation levels and lysine acetyltransferase
2A (KAT2A) protein levels in SNU182 and Huh7 cell lines.
Overexpressing KAT2A counteracted the reduction in cell viability
and glycolysis brought about by AS-IV treatment in the SNU182 and
Huh-7 cell lines. Meanwhile, KAT2A increases the succinylation of
PGAM1, and AS-IV appeared to inhibit tumor growth by blocking the
KAT2A-mediated succinylation of PGAM1 (93). Fang Gong et al (94) and Li et al (95) revealed that AS-IV significantly
reduces the proliferation, migration and invasion in Huh-7 cells
and suppresses ROS production. These effects were achieved via
multiple pathways, including the TGF β1/mothers against
decapentaplegic homolog (Smad) and Nrf2/heme oxygenase 1 (HO-1)
pathway; upregulated expression of pSmad3C, pNrf2, HO-1 and
DT-diaphorase (NQO1); and decreased expression of pSmad2C, pSmad2L,
pSmad3L, plasminogen activator inhibitor-1 and α-SMA. The
inhibitory impact of AS-IV on HCC in vivo was further
corroborated in a mouse subcutaneous tumor model, in which AS-IV
suppressed the proliferation, migration and invasive capacity of
Huh-7 cells by inhibiting macrophage M2 polarization and reducing
the expression of M2 macrophage-stimulated phosphorylated signal
transducer and activator of signal transducer and activator of
transcription (STAT) 3, p-NF-κB and TLR4 expression (94,96). In a mouse model of HCC, Li et
al (95) analyses further
verified the reversibility and antagonism of AS-IV in regulating
pSmad3C/3L and the phosphorylated expression of the Nrf2/HO-1
pathway in TGF β1-activated HSC-T6 and HepG2 cells. All these
results indicated that AS-IV can effectively inhibit HCC
progression by suppressing the proliferation, migration and
invasion of liver cancer cells.
AS-IV exerts indirect anti-hepatoma effects by
regulating the tumor immune microenvironment and enhancing
antitumor immune responses. Yang et al (97) and Cui et al (98) uncovered the underlying mechanism:
AS-IV could target the miR-135b-5p signaling pathway of
carboxypeptidase n domain-containing protein 1, alleviating the
immunosuppression caused by programmed death-ligand 1 (PD-L1) and
accelerating apoptosis. In addition, AS-IV exhibited a
dose-dependent inhibitory impact on the proliferation of Huh-7 and
SMMC-7721 cell lines. It suppressed the interferon-γ-induced
expression of PD-L1, thereby weakening PD-L1-mediated
immunosuppression and immune cell cytotoxicity, and strengthening
the antitumor immune response (96). Guo et al (99) demonstrated that AS-IV facilitated
dendritic cell maturation and enhanced antigen presentation. It
also increased the release of the functional cytokine
interleukin-12 (IL-12) by upregulating various surface markers,
namely, cluster of differentiation (CD)14, CD40, CD80, CD83, CD86
and human leukocyte antigen-DR. As a consequence, dendritic
cell-induced specific cytotoxic T lymphocyte responses against the
HCC cell line SMMC-7721 were enhanced. IL-12 is regarded as a
natural immune booster in dendritic cell-mediated anti-HCC therapy.
In a study by Qi et al (100), AS-IV exhibited anticancer
activity by downregulating oncogenes such as vav guanine
nucleotide exchange factor 3.1 and inhibiting the
non-adherent-dependent growth of HepG2 cells. Another study showed
that AS-IV inhibited the phosphorylation of c-Jun-terminal kinase
and p-c-Jun and downregulated multidrug resistance gene 1 in
Bel-7402 and Bel-7402/FU cells in a dose-dependent manner (101). It achieved this feature by
decreasing the expression levels of multidrug resistance gene 1
mRNA and p-glycoprotein, thus reversing the resistance of
Bel-7402/FU cells to 5-FU. Therefore, AS-IV can reverse multidrug
resistance in a mouse model of HCC (101). Meanwhile, Qu et al
(102) discovered that AS-IV
enhanced the antitumor effect of cisplatin by inhibiting the
expression of certain factors in HepG2 cells and multidrug
resistance-associated protein 2. It also enhanced the
responsiveness of HCC to cisplatin-based chemotherapy.
Inducing the apoptosis of hepatoma cells is one of
the core antitumor mechanisms of AS-IV. Cui et al (98) revealed that AS-IV negatively
regulated CTNNB1 levels through the binding of miR-150-5p to the
untranslated region of CTNNB1. In addition, CTNNB1 overexpression
partially reversed the tumor growth inhibition and apoptosis
effects induced by miR-150-5p upregulation. Meanwhile, miR-150-5p
upregulation suppressed β-catenin expression, thereby promoting
apoptosis and inhibiting tumor growth. Furthermore, Su et al
(103) showed that AS-IV could
induce SK-Hep1 and Hep3B cells to halt the cell cycle in the G1
phase and activate the caspase-8-dependent exogenous and
caspase-9-dependent endogenous apoptotic pathways. As a result, it
suppressed the expression of apoptotic signal proteins such as
myeloid cell leukemia-1 protein, x-linked inhibitor of apoptosis
protein, cellular fas-associated death domain-like
interleukin-1β-converting enzyme inhibitory protein, and survivin
in HCC cells.
AS-IV significantly inhibits EMT in hepatoma cells.
EMT is a key process for the migration, invasion and distant
metastasis of hepatoma cells. Qin et al (104) reported that AS-IV could
mitigate the inhibitory effect on GSK-3β by reducing Akt
phosphorylation. As a consequence, the expression of the
wingless-type MMTV integration site family (Wnt)/β-catenin
signaling pathway is suppressed, and the EMT signaling pathway is
regulated, resulting in the downregulation of N-catenin, vimentin
and α-SMA. In addition, AS-IV reduces the expression of zinc finger
protein transcription factor and promotes the transcription of
E-cadherin to some extent, thereby weakening the invasion and
migration abilities of HCC cells. Li et al (15) demonstrated that AS-IV inhibited
the EMT and migration of HCC cells by downregulating long
non-coding RNA-activated transcript in breast cancer. Jiang and Mao
(105) demonstrated that AS-IV
reduced the expression of N-calmodulin, E-calmodulin and vimentin
in HepG2 and Hep3B cell lines by influencing their EMT. As a
consequence, the proliferative capacity of these HCC cell lines
HepG2 and Hep3B was diminished. Moreover, the enhanced apoptotic
capacity was manifested by a substantial elevation in the protein
amounts of caspase-3 and caspase-9, effectively inhibited tumor
invasion and migration. In a mouse model of HCC, AS-IV induced the
apoptosis of tumor cells by blocking the activation of the Wnt/β
catenin/T cell factor-4 signaling pathway and reducing the protein
expression of vascular endothelial growth factor.
All the aforementioned molecular effects of AS-IV
have been validated across heterogeneous experimental systems,
including in vitro HCC cell lines, in vivo nude mouse
xenograft models, H22 tumor-bearing mouse models, HepG2 xenograft
tumor models, and HCC rat models. Comprehensive analysis of current
evidence demonstrates that, despite variations in experimental
conditions, these regulatory effects maintain an overall consistent
trend. AS-IV exerts a pivotal function in HCC development. It curbs
the proliferation, migration, and invasion of cancer cells;
restrains tumor growth; promotes apoptosis; and improves the
treatment outcome by enhancing the antitumor immune response
(Fig. 3).
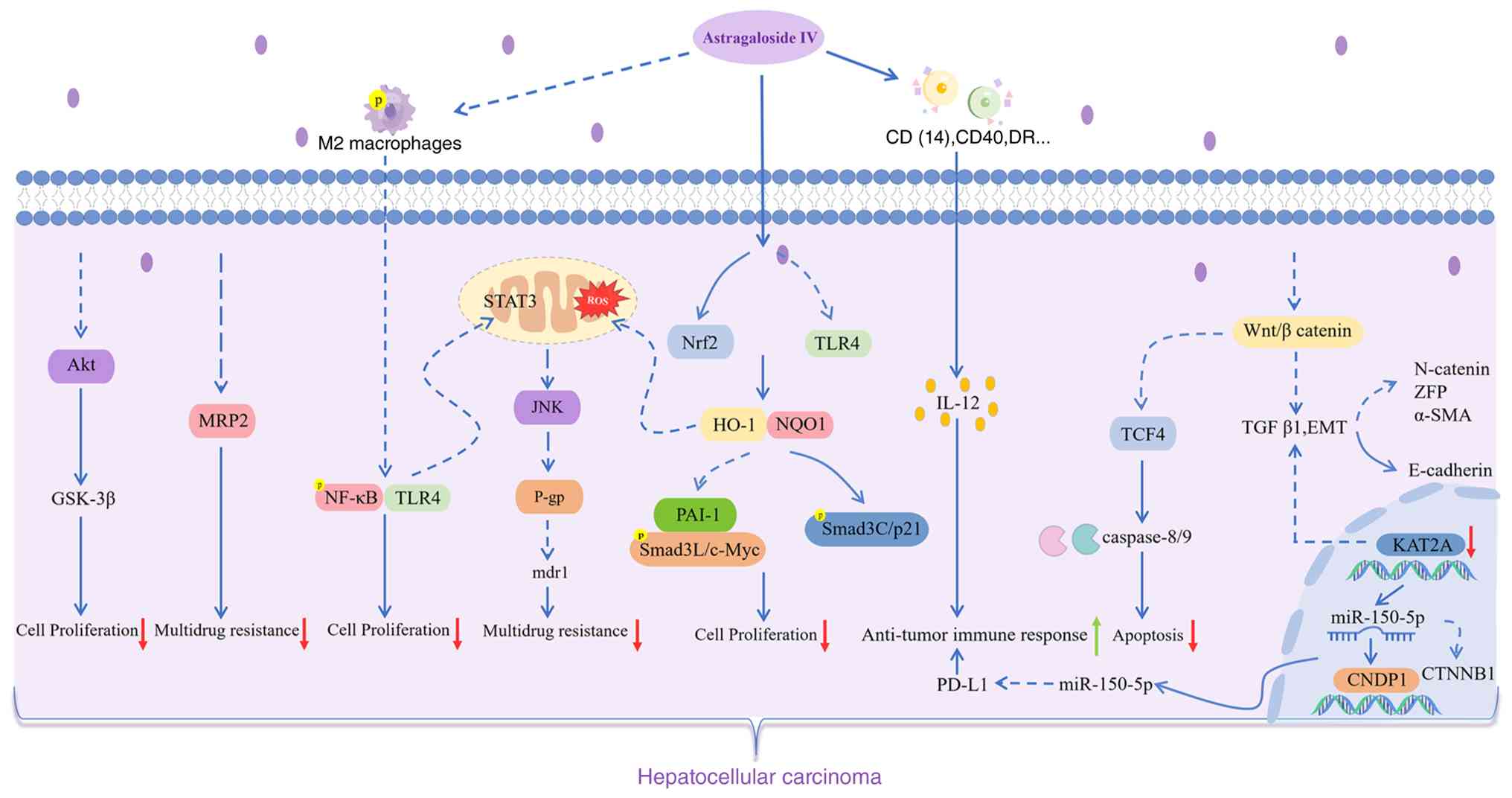 | Figure 3Mechanisms by which Astragaloside Ⅳ
ameliorate hepatocellular carcinoma. MRP2, multidrug
resistance-associated protein 2; HO-1, heme oxygenase 1; NQO1,
DT-diaphorase; PAI-1, plasminogen activator inhibitor-1; Smad,
mothers against decapentaplegic homolog; STAT, signal transducer
and activator of transcription; p-gp, p-glycoproterin; IL-12,
interleukin-12; PD-L1, programmed death-ligand 1; Wnt,
wingless-type mmtv integration site family; TGF4, T cell factor-4;
TGF, transforming growth factor; EMT, epithelial-mesenchymal
transition; ZFP, zinc finger protein transcription; KAT2A, lysine
acetyltransferase 2A; CNDP1, carboxypeptidase n domain containing
protein 1; miR, microRNA. |
Liver injury
Liver injury refers to a series of
pathophysiological alterations induced by diverse internal and
external factors, with significant manifestations of liver
dysfunction (106). If this
condition remains inadequately controlled, then it has a high
probability of further progressing to LF or LC, and may even
deteriorate into acute liver failure (107). Liver injury has numerous
causes, including toxins, inflammation, metabolic disorders and
ischemia-reperfusion. In the present treatment of liver injury,
synthetic drugs such as corticosteroids and IFN are commonly
employed to manage the progression of this condition (108). When liver injury is exacerbated
and progresses to liver failure, liver transplantation emerges as
one of the limited therapeutic alternatives. This approach faces
numerous challenges, with the low graft success rate being a
prominent issue (109). Natural
compounds with anti-inflammatory and antioxidant properties offer
significant protection against liver injury (110,111). Among them, AS-IV, a typical
natural compound, possesses strong anti-inflammatory and
antioxidant activity and shows great potential for use in liver
injury prevention (112).
Toxin-induced liver injury
Iron serves as a vital biological catalyst for
cellular redox reactions and is essential for life. However,
excessive iron absorption in the gut can lead to abnormal iron
deposition within the parenchymal cells of various organs,
including the liver, heart and pancreas, resulting in cytotoxicity,
tissue damage and organ fibrosis. The liver is the primary site of
iron storage and plays a central role in regulating iron
homeostasis. Iron-induced cellular damage is caused by the
oxygen-free radicals generated by iron and lipid membrane
peroxidation. In the liver, particularly within the mitochondria
and lysosomes, this condition is considered a factor in hepatocyte
necrosis and apoptosis, ultimately leading to LF and liver damage
(113-115). In a related study, Lo2 cells
were continuously cultured in a medium containing iron dextrose to
construct an iron overload model (116). The results revealed decreased
Lo2 cell viability and increased autophagy and apoptosis, which
were reversed by AS-IV. Excessive autophagy damages the cell
structure, which was significantly alleviated by AS-IV. This effect
manifested as a marked elevation in p62 expression and a
significant decline in the microtubule-associated protein light
chain 3 (LC3) Ⅱ/Ⅰ ratio in the cells treated with AS-IV. Meanwhile,
the cell morphology and structure gradually returned to the normal
state. Hepcidin is a well-recognized iron modulator that plays a
crucial part in regulating plasma iron concentration by modulating
iron release from the circulatory system or from the cells that
store iron. The same study found that AS-IV dose-dependently
increased the expression level of hepcidin, thus effectively
inhibiting iron-induced apoptosis and autophagy in hepatocytes.
Cisplatin, a highly potent chemotherapeutic agent
widely employed in the treatment of numerous cancers, exhibits
remarkable anticancer effects. However, it is accompanied with
severe issues of nephrotoxicity and hepatotoxicity (117,118). Cisplatin nephrotoxicity at
standard clinical doses is one of the most common side effects.
Although the incidence of hepatotoxicity is relatively low, it may
still occur following exposure to high cisplatin doses.
Hepatotoxicity occurs primarily because the liver is the main organ
responsible for metabolizing a wide range of drugs and chemicals.
After the kidneys, the liver is the organ in which cisplatin
accumulates to the greatest extent; this is the key reason
high-dose cisplatin induces hepatotoxicity. Prolonged or high-dose
exposure to cisplatin may lead to hepatic necrosis, and apoptotic
lesions may be observed in liver tissue. At present, research on
the hepatotoxicity of cisplatin remains limited, and the potential
mechanisms have not been fully elucidated (119,120). Several studies investigated
cisplatin-induced toxicity and corresponding coping strategies. For
instance, an experimental study using rats discovered that the
hepatotoxic injury caused by cisplatin was significantly mitigated
when the rats treated with cisplatin were administered AS-IV
(121). In particular, the
hepatic/body mass index of the rats returned to normal. The levels
of ALT and AST, which had been elevated by cisplatin, showed a
downward trend. This finding demonstrated that AS-IV could
effectively alleviate cisplatin-induced hepatic injury in a
dose-dependent manner (121).
In another study, cisplatin induced an inflammatory response and
autophagy in hepatocytes. AS-IV reversed this process, thereby
offering protection against cisplatin-mediated liver injury in rats
(122). Cisplatin-induced
abnormal cellular function frequently triggers ferroptosis, a
crucial type of programmed cell death in cisplatin-induced acute
liver injury (123-125). Guo et al (122) distinctly demonstrated that
AS-IV could inhibit excessive lipid peroxidation and iron induced
cell death by targeting the peroxisome proliferator-activated
receptor α (PPARα) pathway. It also restored the expression of
GSH-Px 4 and ferroptosis suppressor protein 1, ultimately
ameliorating cisplatin-induced liver injury.
Acetaminophen (APAP) is a well-known antipyretic and
analgesic widely used in daily life. If overdosed, excessive APAP
promotes high ROS generation, which induces oxidative damage and
ultimately leads to liver injury (126,127). AS-IV demonstrates a positive
intervention in this process. It can effectively reduce the
inflammatory response and inhibit APAP-induced oxidative stress.
Its mechanism of action is mainly based on the regulation of the
Nrf2 pathway. AS-IV can activate Nrf2, resulting in a significant
enhancement of nuclear Nrf2 expression. As a crucial transcription
factor, Nrf2 governs the expression of downstream genes HO-1
and NQO1, both of which encode important antioxidant
enzymes. Meanwhile, AS-IV inhibits the expression of Kelch-like
ECH-associated protein 1, which is involved in the ubiquitination
and degradation of Nrf2 within cells and exerts a negative
regulatory influence on Nrf2 activity. These findings suggest that
AS-IV alleviates liver damage caused by excess APAP (128,129).
Atorvastatin (ATO) is commonly utilized in clinical
practice for its effects of lowering blood lipids and preventing
atherosclerosis. However, its excessive use can give rise to
hepatotoxicity (130). From a
pathological perspective, an ATO overdose can trigger a series of
pathological alterations in liver tissues, including inflammatory
cell infiltration and apoptosis. Qin et al (131) reported that AS-IV could
remarkably mitigate these adverse pathological changes. In
particular, AS-IV alleviates the LF and inflammatory responses
induced by ATO and activates the phosphorylation of AMPK. It also
inhibits hepatocyte apoptosis by upregulating sirtuin 1 in the
liver tissues of rats. As a result, AS-IV significantly reduces the
hepatotoxicity caused by ATO.
Chronic excessive alcohol intake is a primary factor
contributing to the development of ALD, a condition that can
severely damage the liver. Regarding its pathogenesis, the
metabolic process of ethanol in the body disrupts normal FA
oxidation, leading to a substantial buildup of fat within the liver
(132). In clinical settings,
this phenomenon is demonstrated by a significant elevation in ALT
and AST concentrations. In addition, the liver tissue exhibits
notable pathological changes, such as cellular degeneration,
hepatocellular necrosis and nuclear condensation. Treatment with
AS-IV can effectively reverse these adverse conditions. It
ameliorates pathological damage in ALD rats, reduces lipid
accumulation in hepatocytes, and plays a positive role in repairing
the damaged liver (133).
Oxidative stress is a crucial indicator for evaluating the severity
of alcoholic liver injury (134). AS-IV treatment effectively
reverses the inhibition of SOD activity and GSH-Px content and
blocks the increase in 4-hydroxy-2-nonenal and MDA levels, thereby
suppressing oxidative stress. Acute alcohol stimulation prompts an
upsurge in the production of macrophages and neutrophils in the
liver, leading to systemic and hepatic inflammation. In this
regard, AS-IV has demonstrated excellent anti-inflammatory
properties. It inhibits the upregulation of F4/80 protein,
effectively reduces the levels of pro-inflammatory factors,
including TNF-α, IL-1β, IL-6 and myeloperoxidase; and prevents the
activation of nod-like receptor protein 3 inflammatory vesicles
(135). In addition, alcohol
stimulation impairs the intestinal barrier function, resulting in a
leaky gut and endotoxemia (136). AS-IV can significantly reduce
the elevated levels of LPS, LPS-binding protein and diamine
oxidase. The changes in the levels of these three indicators can
effectively reflect the severity of the leaky gut. Moreover, AS-IV
prevents the decrease in the expression of tight junction proteins,
such as occludin and claudin 4, within the small intestine
(133), thereby preserving the
integrity of the intestinal barrier and lessening the harm
inflicted on organs such as the liver when endotoxins infiltrate
the circulatory system. Furthermore, Hao et al (137) indicated that AS-IV could
improve the metabolic disorders of linoleic acid, sphingolipid and
glycerophospholipid in rats with ALD through the core targets of
phosphorylated receptor-interacting protein kinase 3,
phosphorylated mixed lineage kinase domain-like protein, cytochrome
p450 family 2 subfamily c member 19, cytochrome p450 family 1
subfamily a member 2, PPARα and proprotein convertase
subtilisin/kexin type 9. It alleviates liver injury in rats with
ALD at the metabolic level. Their study provided an in-depth
theoretical basis for the treatment of ALD with AS-IV.
Inflammatory liver injury
In the pathology of sepsis/septic shock,
lipopolysaccharide (LPS), an immunostimulatory molecule located in
the outer membrane of Gram-negative bacteria, is a major causative
factor for inducing organ failure, including liver injury (138). When LPS enters the liver, it
induces an immune response, triggering the release of
pro-inflammatory cytokines (such as TNF-α, IL-6 and IL-1β), ROS and
nitrosamines, thereby significantly increasing inflammation
(139). Hepatic injury is a
crucial component of this inflammatory response. LPS significantly
increases the mRNA expression levels of inflammatory cytokines,
including IL-1β, TNF-α and IL-6, triggering a series of
pathological reactions. AS-IV has demonstrated remarkable efficacy
in countering LPS-induced hepatic injury. It can directly decrease
ALT and AST levels in LPS-induced liver injury, a reduction in
these levels directly reflects a decrease in hepatic cell damage
degree. Moreover, AS-IV improves the pathological changes in liver
tissue and repairs the damaged liver at the histological level.
Regarding apoptosis regulation, AS-IV reduces the expression of
pro-apoptotic proteins via downregulating the mRNA expression of
Bax and augments the expression of anti-apoptotic proteins
by upregulating the mRNA expression of Bcl-2. As a
consequence, the LPS-induced apoptosis of hepatic tissues is
inhibited, thereby maintaining the normal survival and function of
liver cells. Oxidative stress has a crucial impact on liver injury
induced by LPS. AS-IV protects liver cells from oxidative damage by
reducing the MDA content and lipid peroxidation products in
LPS-stimulated mice. It also elevates the levels of SOD and
catalase, which bolster the antioxidant ability of liver cells. As
a result, it effectively inhibits oxidative stress and ROS within
liver cells. In addition, LPS induces a robust inflammatory
response. AS-IV can reverse this outcome by significantly
decreasing the mRNA expression levels of these inflammatory
factors, thus effectively alleviating the generation of the
inflammatory response and further mitigating inflammatory injury in
the liver (140).
Metabolic liver injury
Type 2 diabetes mellitus (T2DM) is a serious
lifelong metabolic disease. Among the numerous complications
associated with T2DM, liver injury is one of the major ones and is
triggered by multiple factors (141,142). Long-term chronic hyperglycemia
leads to glycotoxicity. The insulin resistance associated with T2DM
impairs insulin signaling in the liver, disrupting gluconeogenesis
and glycogen synthesis, and directly damaging the normal metabolism
and structure of liver cells. A large influx of FFAs into the liver
leads to abnormal lipid accumulation, which activates inflammatory
signaling pathways, induces oxidative stress and ER stress, and
exacerbates inflammation, apoptosis and damage to liver cells.
Liver damage further exacerbates hepatic insulin resistance,
leading to an increase in the conversion of glucose into
triglycerides and worsening of hepatic steatosis; in turn, the
accumulation of hepatic fat further exacerbates insulin resistance
and hyperglycemia, creating a vicious cycle that accelerates the
progression of T2DM and liver damage (143-145). In the synergistic treatment
with AS-IV and metformin, the abnormally elevated liver indices
(which are important indicators for evaluating liver function) in
patients with diabetes were significantly suppressed. As shown in
the T2DM rat model, T2DM is often accompanied with dyslipidemia,
characterized by significantly elevated levels of TG and IL and
markedly reduced levels of high-density lipoprotein cholesterol.
These manifestations can be mitigated by AS-IV treatment. Moreover,
AS-IV and Met inhibited the conversion of LC3I to LC3II (a marker
of autophagy) and the reduction of beclin 1 (an Essen autophagy
protein at the initial stage of autophagy) accumulation. They also
reduced the expression level of P62 and facilitated the generation
of autophagosomes, thereby enhancing hepatic autophagy. The
mechanism further involves enhancing autophagy by activating the
AMPK/mTOR pathway, which helps ameliorate IR, dyslipidemia,
oxidative stress and inflammation (146).
Ischemic liver injury
Ischemia-reperfusion injury mainly occurs during
liver transplantation, an effective treatment for ESLD (147). According to Cheng et al
(148), AS-IV pretreatment
could significantly ameliorate hepatic parenchymal cell injury. It
improves hepatocyte survival and liver function by downregulating
TNF-α levels and NF-κB expression and transcriptional activity, and
upregulating glucocorticoid receptor.
All the aforementioned molecular effects of AS-IV
have been validated across heterogeneous experimental systems,
including in vitro models of iron overload-induced liver
injury, HepG2 cells, Bel-7402 cells, and others, in vivo
models such as cisplatin-induced liver injury in rats,
paracetamol-induced liver injury in mice, atorvastatin-induced
liver injury in rats, and the ALD rat model. Comprehensive analysis
of current evidence demonstrates that, despite variations in
experimental conditions, these regulatory effects maintain an
overall consistent trend.
Overall, AS-IV frequently exhibits pronounced
therapeutic efficacy in oxidative stress-related liver injury.
Specifically, its protective effects have been consistently
demonstrated across multiple studies on toxin-induced and metabolic
liver injury, where it exerts hepatoprotection mainly by activating
the Nrf2 signaling pathway to exert antioxidant effects and
modulating the AMPK/PPARα signaling pathway to maintain metabolic
homeostasis. In inflammatory liver injury, AS-IV exerts a marked
anti-inflammatory effect by inhibiting the NF κB signaling pathway.
In ischemic liver injury, AS-IV confers protection by ameliorating
hepatocellular damage via modulation of the AMPK/mTOR signaling
pathway. However, its mechanism of action in ischemic liver injury
is relatively limited (Fig.
4).
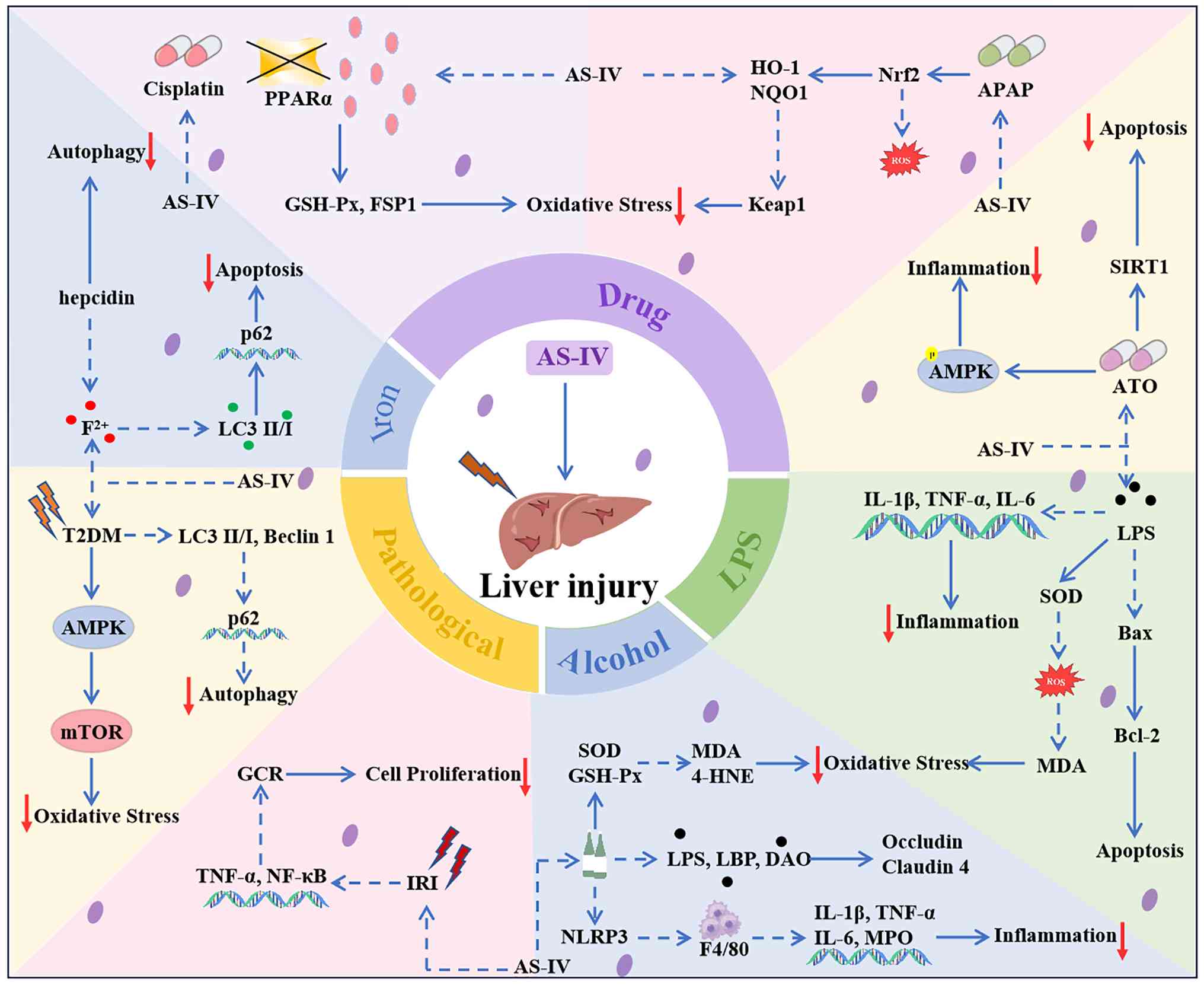 | Figure 4Mechanism of AS-Ⅳ amelioration of
liver injury induced by various hepatotoxin substances. PPARα,
peroxisome proliferator-activated receptor α; FSP1, ferroptosis
suppressor protein 1; APAP, acetaminophen; SIRT1, sirtuin 1; ATO,
atorvastatin; LPS, lipopolysaccharide; 4-HNE, 4-hydroxy-2-nonena;
LBP, lipopolysaccharide-binding protein; DAO, diamine oxidase; NLRP
3, nod-like receptor protein 3; MPO, myeloperoxidase; IRI,
ischemia-reperfusion injury; GCR, glucocorticoid receptor; AS-IV,
Astragaloside IV; MDA, malondialdehyde; SOD, superoxide dismutase;
GSH-Px, glutathione peroxidase; ROS, reactive oxygen species. |
Pharmacokinetics, toxicity and nanoscale
application of AS-Ⅳ
Pharmacokinetics
As a discipline focusing on drug absorption,
distribution and metabolism excreted in living organisms,
pharmacokinetics is crucial for understanding drug action and
efficacy. AS-IV presents a unique pharmacokinetic profile because
of its own characteristics, such as low intestinal permeability, a
relatively high molecular weight, and limited lipophilicity, which
is associated with paracellular transport.
The oral bioavailability of AS-IV remains low across
different species. When orally given to rats and beagles at 10
mg/kg dose, its in vivo bioavailability was only 3.66 and
7.4%, respectively. The low oral bioavailability substantially
limits systemic drug exposure, making it challenging to reach
therapeutically effective concentrations in target tissues.
Therefore, intravenous injection is generally adopted for AS-IV
administration in clinical settings. However, when the drug
concentration in various tissues was measured subsequent to the
intravenous injection of AS-IV to rats, the liver and kidneys
exhibited the highest levels of AS-IV, followed by the lungs, heart
and spleen. By contrast, the limited distribution of AS-IV to the
brain indicates that it might encounter challenges in crossing the
blood-brain barrier. Within the concentration range of 250-1,000
ng/ml, ~90% of AS-IV was bound to plasma proteins. In plasma, AS-IV
primarily exists in a bound state, with relatively low free drug
concentrations (149,150).
The elimination of AS-IV exhibits certain
variations across different species yet displays overall linear
kinetic characteristics. For instance, following the intravenous
injection of 0.5, 1 and 2 mg/kg of AS-IV in beagles, the plasma
t1/2 was 177.18, 196.58 and 241.59 min, respectively,
and the area under the curve (AUC) was 126.24, 276.28 and 724.51
µg h/ml respectively (149). By contrast, when AS-IV was
administered intravenously only to healthy volunteers, the mean
maximum plasma concentration (Cmax) values were 2.12,
3.59, 3.71 and 5.17 g/ml at single doses of 200, 300, 400 and 500
ml (contained 27, 36, 45 and 54 mg AS-IV, respectively),
respectively. The corresponding mean values of AUC were 4.38, 9.75,
13.59 and 18.22 µg h/ml, respectively, and the mean values
of elimination t1/2 were 2.14, 2.59, 2.62 and 2.69 h,
respectively (151).
In terms of excretion, AS-IV is primarily
eliminated via feces and bile, with urinary excretion accounting
for a relatively minor proportion. For male rats, the excretion
rates of the substance in feces, urine and bile within 24 h were
31.41, 13.43 and 31.92%, respectively. For female rats, the
corresponding excretion rates in feces, urine and bile over the
same 24-h period were 31.84, 21.77 and 36.20%, respectively
(150). In healthy volunteers,
the cumulative urinary excretion of AS-IV over 24 h after
administration of 500 ml was 3.91% (151). However, in rat models, only 50%
of AS-IV was metabolized in vivo via urine and feces, 30%
was recovered in bile, and metabolism was virtually non-existent in
the liver, suggesting that first-pass elimination does not occur
(47,152).
Toxicity
Understanding the toxic impacts of AS-IV is
essential for the development of AS-IV-related drugs. For
therapeutic applications, AS-IV has a high safety profile, with low
levels of toxicity at standard doses that do not induce significant
adverse effects. Oral administration of AS-IV at a daily dose of
1.0 mg/kg for 14 weeks did not cause adverse effects on hepatic and
renal function (153). Animal
studies also confirmed that AS-IV treatment does not lead to
toxicity or side effects in adult animals. The safe doses for rats
and beagles are equivalent to 70 or 35-fold the human dose,
respectively, such as 0.57 g/kg (154). When AS-IV was administered
intravenously at a daily dose of 1.0 mg/kg, it caused maternal
toxicity in rats, and doses >0.5 mg/kg led to fetal toxicity. By
contrast, when AS-IV was administered intravenously daily from 4
weeks before mating until day 6 of pregnancy in rats, no maternal
toxicity was observed at doses ranging from 0.25-1.0 mg/kg.
However, at the highest dose of 1.0 mg/kg, suppression of female
fertility and delayed hair growth and neurological development in
the offspring were observed. These findings indicate that while the
toxic effects of AS-IV vary markedly with the stage of pregnancy,
the compound consistently lacks teratogenic effects, underscoring
the need for caution in its clinical use during pregnancy (155,156). Therefore, caution should be
exercised when applying AS-IV treatment in the pregnant
population.
However, current research on the adverse reactions
and toxic side effects of AS-IV remains limited. Most findings are
based on preliminary observations, and the underlying mechanisms of
its potential toxicity have not been fully elucidated. Notably,
long-term human clinical data are still lacking, rendering it
difficult to confirm its long-term safety profile in chronic
conditions such as viral liver disease. Therefore, clinical studies
on the toxicity of AS-IV in liver disease are urgently needed to
facilitate its development and application in the therapeutic field
of liver disease.
Nanoscale application
AS-IV suffers from poor permeability and low oral
bioavailability. Nanocapsules and nanocarriers have been effective
in enhancing drug bioavailability (157). In terms of brain-targeted
delivery, the use of the ion cross-linking method for
β-asarone-modified asi-loaded chitosan nanoparticles with 120 nm
size and favorable uniformity led to ~20% cumulative release in
vitro over 48 h, demonstrating sustained-release properties.
Compared with unmodified nanoparticles, DiR-βCS-NP exhibited
1.52-fold enhanced uptake in 16HBE cells and 2.49-fold increased
fluorescence intensity in the brain, significantly improving nasal
brain targeting efficiency. ASI-βCS-NP reduced clinical scores in
EAE mice by ~60%, inhibited glial cell activation, mitigated myelin
loss and promoted myelin regeneration, demonstrating superior
nasal-brain delivery and neuroprotective effects (158). In terms of stability and
hydrophilicity, encapsulation in liposomes and loading them onto
PVA nanofibers yielded particles with an average diameter of
143.23±3.25 nm and a polydispersity index of 0.11±0.048. The zeta
potential was -11.2±1.35 mV, indicating uniform particle
distribution without significant aggregation. The ASL/APS/PVA
nanofiber surface exhibited smoothness and structural stability,
protecting AS-IV from degradation while enhancing its storage and
in vivo transport stability. Furthermore, the liposomes
encapsulated the hydrophobic AS-IV, enabling its stable dispersion
in the aqueous phase. The PVA nanofibers demonstrated excellent
hydrophilicity, adsorbing bodily fluids to promote AS-IV dispersion
and sustained release within aqueous environments, and
significantly improving its hydrophilic properties (159). In tumor-targeted drug delivery,
nanomicelles efficiently encapsulate AS-IV with a 90.92%
encapsulation efficiency and 12.48% loading capacity, significantly
enhancing its water solubility and dispersibility. This
nanomedicine exhibited stable particle size in serum and at 4°C
storage conditions, demonstrating favorable biosafety. Following
PDL1 modification, the tumor-targeting capability was enhanced,
enabling the precise delivery of AS-IV and inhibition of the
STAT3/NF-κB pathway, substantially boosting antitumor efficacy
(160). In addition, AS-IV can
enhance ocular delivery. AS-IV-loaded lipid nanocapsules (LNCs)
with uniform particle sizes of 19.88, 49.39 and 92.89 nm showed an
encapsulation efficiency of over 90%. AS-IV-LNCs-20 also markedly
reduced retinal apoptosis rate from 5.12 to 0.533% and alleviated
ROS accumulation, while showing no ocular irritation and excellent
biocompatibility (161).
Nanoparticles, nanomicelles and LNCs are excellent in
tissue-targeted delivery; and the liposome-PVA nanofiber system has
advantages in improving stability and water solubility. These
results demonstrate that nanotechnology greatly enhances the
solubility, stability, ocular penetration and retinal targeting
efficiency of AS-IV, providing new ideas and ways to improve the
pharmacokinetic properties of AS-IV.
Conclusions and future perspectives
Liver disease has become one of the major perils to
global public health, significantly influencing patient morbidity
and mortality worldwide. At present, the issue of diverse
side-effects associated with existing therapeutic drugs is
prominent. Traditional Chinese medicine has garnered substantial
attention mainly because of its features such as low toxicity, few
side effects and favorable tolerability. AS-IV is the key active
component derived from the root of A. membranaceous, a
traditional Chinese herb renowned for qi-tonifying. In the present
study, a comprehensive review of the hepatoprotective effects of
AS-IV in NAFLD, liver injury, LF and liver cancer was conducted.
Its potential hepatoprotective mechanisms encompass a wide
spectrum, including attenuation of fat accumulation, modulation of
apoptosis, activation of autophagy, inhibition of fibrosis,
regulation of the inflammatory response, alleviation of oxidative
stress, anticancer effects, and combined therapeutic effects
related to intestinal microbiota. These effects are mediated
through signaling pathways such as Akt/mTOR, TLR4, NF-κB, PPARα,
TGF β/Smad, Wnt/β catenin and Nrf2/HO-1. Notwithstanding the
extensive potential of AS-IV in liver disease treatment, current
research exhibits notable limitations. Most studies remained
confined to in vitro cell and animal experiments, lacking
high-quality, large-scale human clinical trial evidence. As a
consequence, the systematic elucidation of its overall regulatory
network and underlying interactive mechanisms remains insufficient.
The inherent issues with AS-IV, including its low water solubility,
poor oral bioavailability, and insufficient hepatic targeting,
remain key bottlenecks constraining its druggability and clinical
translation. Furthermore, the process scale-up, long-term
stability, and in vivo long-term safety of existing
nano-delivery systems require further systematic validation. Novel
drug delivery systems such as liposomes, nanoparticles and micelles
have significantly enhanced the solubility and tissue distribution
of AS-IV, offering viable strategies to overcome its translational
barriers. Therefore, large-scale randomized clinical trials and
comprehensive and in-depth scientific research are urgently
required to accurately assess the safety and efficacy of AS-IV
(Table I).
 | Table ISummary of the protective effect of
Astragaloside IV in various liver diseases. |
Table I
Summary of the protective effect of
Astragaloside IV in various liver diseases.
| Authors, year | Dosage | In vivo, in
vitro | Model | Observed
effects | (Refs.) |
|---|
NAFLD
|
| Zhai et al,
2022 | 12.5, 25, 50
mg/kg | In vivo | Mouse model of
NAFLD | AS-IV inhibits
intestinal FXR through intestinal microbiota remodeling and
improves dietinduced hepatic steatosis in obese mice | (61) |
| Liu et al,
2024 | 0.25, 0.5, 1, 5,
10, 20, 40 µg/ml | In
vitro | Fatty liver cell
model | AS-IV promotes
autophagy and improves cellular lipid deposition through the
Akt/mTOR pathway | (63) |
| Liang et al,
2021 | 0, 20, 40, 80 mg/kg
and 20, 60, 100 µg/ml | In vivo, in
vitro | Mouse model of
NAFLD and fatty liver cell model | AS-IV reduces liver
inflammation, oxidative stress, and apoptosis | (64) |
| Liu et al,
2020 | 0, 20, 40, 80
mg/kg | In vivo | NAFLD rat
model | AS-IV regulates
inflammatory factor levels via the TLR4/NF-κB signaling
pathway | (67) |
| Zhou et al,
2017 | 0, 50, 100, 200,
400 µg/ml | In
vitro | HepG2 cells and
Primary mouse hepatocytes | AS-IV alleviates
free fatty acid-induced ER stress and lipid accumulation in
hepatocytes through AMPK activation | (68) |
| Chen et al,
2019 | 0, 20, 40
µg/ml | In
vitro | HSC-T6 cells | AS-IV regulates
NF-κB-mediated hepatic stellate cell senescence and apoptosis to
inhibit PDGF BB-induced activation | (74) |
|
| Liver fibrosis |
|
| Li et al,
2013 | 0, 1, 3, 10, 30,
100 µM | In
vitro | HSC-T6 cells | AS-IV inhibits
collagen production in activated hepatic stellate cells via the p38
MAPK pathway | (75) |
| Liu et al,
2009 | 0, 1.5, 3, 6, 12,
24 mg/kg | In vivo | PS-induced LF rat
model | AS-IV delayed the
formation of liver fibrosis | (76) |
| Zhao et al,
2020 | 0, 4.8, 10.8
mg/kg | In vivo | BDL rat model | AS-IV in
collaboration with FA induced hepatic stellate cell inactivation by
activating the Nrf2 pathway | (77) |
| Zhu and Lu,
2024 | 0, 10, 20, 40
µg/ml | In
vitro | HCC cell lines
(SNU-18 and Huh-7) | AS-IV inhibits HCC
by regulating KAT2A-mediated PGAM1 succinylation | (93) |
| Fang Gong et
al, 2023 | 40 mg/kg | In vivo, in
vitro | PSmad3C and Nrf2
mice and HepG2 cells | The ameliorative
effect of AS-IV on HCC through Nrf2-mediated pSmad3C/3L
transformation | (94) |
| Li et al,
2022 | 5, 10, 20
µM | In
vitro | HCC cell lines
(Huh-7) | The AS-IV by
regulating Nrf2/HO-1 and TGF beta inhibition of migration and
invasion of cancer of the liver | (95) |
|
| HCC |
|
| Min et al,
2022 | 0, 40, 80, 100
mg/kg and 0, 50, 80, 100, 120, 150 µM | In vivo, in
vitro | Mouse model of
subcutaneous tumor and HCC cell lines (Huh-7), THP-1 | AS-IV regulates
macrophage polarization through the TLR4/ NF-κB/STAT3 signaling
pathway | (96) |
| Yang et al,
2023 | 0, 50, 100, 150
mg/kg and 0, 10, 20, 40, 80 µg/ml | In vivo, in
vitro | HCC rat model and
HCC cell lines (Huh-7 and SMMC-7721), THP-1 | AS-IV alleviates
PD-L1-induced immunosuppression by modulating the miR-135b-5p/CNDP1
pathway | (97) |
| Cui et al,
2020 | 0, 5, 10, 20, 40,
80, 100, 120, 160, 200 µg/ml | In vivo, in
vitro | Xenotransplantation
model of nude mouse and HCC cell lines (Huh-7 and SMMC-7721) | AS-IV-induced
up-regulation of miR-150-5p inhibits HCC progression by inhibiting
β catenin | (98) |
| Qi et al,
2010 | 0, 150, 200
µg/ml | In
vitro | HepG2 cells | As-iv induces
anticancer activity by downregulating the expression of oncogenes
such as Vav3.1 | (100) |
| Wang et al,
2014 | 0.04, 0.08
mg/ml | In
vitro | Bel-7402 cells,
Bel-7402/FU cells | AS-IV reversed drug
resistance in Bel-7402/FU cells by downregulating mdr1
expression | (101) |
| Qu et al,
2020 | 40, 60, 80
µM and 0.4, 4, 40 µM | In vivo, in
vitro | H22 tumor-bearing
mice and HepG2 cells | AS-IV enhances
cisplatin chemotherapy sensitivity in HCC by inhibiting MRP2 | (102) |
| Su et al,
2020 | 0, 100, 150, 200,
300, 400 µM | In
vitro | HCC cell lines
(SK-Hep1 and Hep3) | AS-IV induced G1
block and apoptosis of HCC cells | (103) |
| Qin et al,
2017 | 0, 0.5, 1, 5, 10,
50, 100 µg/ml | In
vitro | HCC cell lines
(Huh-7 and MHCC97-H) | AS-IV inhibits EMT
by targeting the Akt/GSK-3β/β catenin pathway, thereby reducing the
invasion and migration of HCC cells | (104) |
| Jiang and Mao,
2019 | 25, 50, 100
nmol/l | In vivo, in
vitro | HepG2 xenograft
tumor model and HCC cell lines (HepG2 and Hep3B) | AS-IV alleviates
HCC via the Wnt/β catenin signaling pathway | (105) |
| Xie et al,
2019 | 2.5, 5, 10, 20, 40,
80, 160 µM | In
vitro | Liver injury
induced by iron loading | AS-IV protects the
liver by inhibiting excessive autophagy and apoptosis | (116) |
|
| Liver injury |
|
| Qu et al,
2019 | 40, 80 mg/kg | In vivo | Cisplatin-induced
liver injury in rats | AS-IV protects the
liver by inhibiting NLRP3 through autophagy | (121) |
| Guo et al,
2024 | 40,80 mg/kg | In vivo | Cisplatin induced
liver injury in rats Cisplatin induced liver injury in rats | AS-IV protects the
liver by inhibiting PPARα/FSP1 signaling | (122) |
| Li et al,
2018 | 20,40 mg/kg | In vivo | Acetaminophen in
mice | AS-IV alleviates
liver damage by activating the Nrf2 signaling pathway | (129) |
| Qin et al,
2023 | 0,60 mg/kg | In vivo | Atorvastatin in
rats | AS-IV alleviates
liver damage through the AMPK/SIRT1 pathway | (131) |
| Wu et al,
2023 | 50, 150, 500
mg/kg | In vivo | Rat model of
ALD | AS-IV protects the
liver by regulating intestinal flora imbalance and regulating the
NLRP3/Caspase-1 signaling pathway | (133) |
| Han et al,
2014 | 0.1, 1, 10, 50
mg/l | In
vitro | Alcoholic and
non-alcoholic oxidative damage models | AS-IV had
protective effects on both alcoholic and non-alcoholic oxidative
damage of Chang's liver cells | (135) |
| Hao et al,
2024 | 50, 100, 200
mg/kg | In vivo | Rat model of
ALD | AS-IV reduces liver
damage by regulating oxidative stress and inflammation | (137) |
| Sun et al,
2023 | 0, 80 mg/kg | In vivo |
Lipopolysaccharide-induced liver
injury | AS-IV reduces liver
damage by regulating oxidative stress and inflammation | (140) |
| Zhu et al,
2021 | 0, 80 mg/kg | In vivo | Type 2 diabetes
mellitus rat model | AS-IV alleviates
liver damage by promoting AMPK/mTOR-mediated autophagy | (146) |
| Cheng et al,
2011 | 100 g/ml | In vivo | Mouse orthotopic
liver transplantation model | AST-IV alleviates
hepatic ischemia-reperfusion injury by inhibiting NF-κB
transcriptional activity | (148) |
In summary, AS-IV demonstrates clear anti-liver
disease activity and holds potential for clinical application.
Nevertheless, rigorous, standardized clinical trials are required
for further validation. Future research should focus on optimizing
liver-targeted nano-delivery systems to enhance drug accumulation
efficiency and potency within the liver. High-quality clinical
studies should be conducted to systematically elucidate its
efficacy, safety profile and optimal dosing regimen, thereby
advancing AS-IV from basic research toward clinical application.
The present review may serve as a theoretical reference for the
pharmacological research and subsequent development of AS-IV in
liver diseases.
Availability of data and materials
Not applicable.
Authors' contributions
JS conceptualized the study, curated data and wrote
the original draft. XZ validated and curated data. JW conducted
investigation and data curation. LZ conducted investigation. XW
curated data. WL supervised the study. XH acquired funding,
conducted project administration and supervised the study. XD
supervised the study and conducted project administration. WW
acquired funding and conducted project administration. XZ, LZ, XW,
WL, XH, XD and WW wrote, reviewed and edited the manuscript. All
authors read and approved the final version of the manuscript. Data
authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this work, artificial
intelligence tools were used to improve the readability and
language of the manuscript or to generate images, and subsequently,
the authors revised and edited the content produced by the
artificial intelligence tools as necessary, taking full
responsibility for the ultimate content of the present
manuscript.
Abbreviations:
|
AMPK
|
adenosine monophosphate-activated
protein kinase
|
|
MAPK
|
mitogen-activated protein kinase
|
|
Akt
|
protein kinase B
|
|
AS-IV
|
astragaloside IV
|
|
mTOR
|
mammalian target of rapamycin
|
|
SREBP-1c
|
sterol regulatory element-binding
protein-1c
|
|
ALT
|
alanine aminotransferase
|
|
AST
|
aspartate aminotransferase
|
|
TG
|
triglyceride
|
|
IL-1β
|
interleukin-1β
|
|
IL-6
|
interleukin-6
|
|
TNF-α
|
tumor necrosis factor-α
|
|
TLR4
|
toll-like receptor 4
|
|
ROS
|
reactive oxygen species
|
|
Bax
|
b-cell lymphoma/leukemia-2-associated
X protein
|
|
α-SMA
|
α-smooth muscle actin
|
|
NF-κB
|
nuclear factor κB
|
|
Nrf2
|
nuclear factor erythroid 2-related
factor 2
|
|
HO-1
|
heme oxygenase 1
|
|
IL-12
|
interleukin-12
|
|
LC3
|
microtubule-associated protein light
chain 3
|
Acknowledgments
Not applicable.
Funding
The present study was supported by the Outstanding Youth Project
of Department of Education of Hunan (grant nos. 24B1079 and
24B1077).
References
|
1
|
Núñez M: Hepatotoxicity of
antiretrovirals: Incidence, mechanisms and management. J Hepatol.
44(1 Suppl): S132–S139. 2006. View Article : Google Scholar
|
|
2
|
Sun L and Hui L: Progress in human liver
organoids. J Mol Cell Biol. 12:607–617. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Xiao J, Wang F, Wong NK, He J, Zhang R,
Sun R, Xu Y, Liu Y, Li W, Koike K, et al: Global liver disease
burdens and research trends: Analysis from a Chinese perspective. J
Hepatol. 71:212–221. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Han H, Desert R, Das S, Song Z, Athavale
D, Ge X and Nieto N: Danger signals in liver injury and restoration
of homeostasis. J Hepatol. 73:933–951. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Terrault NA, Francoz C, Berenguer M,
Charlton M and Heimbach J: Liver transplantation 2023: Status
report, current and future challenges. Clin Gastroenterol Hepatol.
21:2150–2166. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wong MCS, Huang JLW, George J, Huang J,
Leung C, Eslam M, Chan HLY and Ng SC: The changing epidemiology of
liver diseases in the Asia-Pacific region. Nat Rev Gastroenterol
Hepatol. 16:57–73. 2019. View Article : Google Scholar
|
|
7
|
Chen J, Ruan X, Fu T, Lu S, Gill D, He Z,
Burgess S, Giovannucci EL, Larsson SC, Deng M, et al: Sedentary
lifestyle, physical activity, and gastrointestinal diseases:
Evidence from mendelian randomization analysis. EBioMedicine.
103:1051102024. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Devarbhavi H, Asrani SK, Arab JP, Nartey
YA, Pose E and Kamath PS: Global burden of liver disease: 2023
update. J Hepatol. 79:516–537. 2023. View Article : Google Scholar
|
|
9
|
Li JZ, Cai XB and Lu LG: Endoscopic
ultrasound-guided liver biopsy: Current status and prospects).
Zhonghua Gan Zang Bing Za Zhi. 32:572–576. 2024.In Chinese.
PubMed/NCBI
|
|
10
|
Li M, Luo Q, Tao Y, Sun X and Liu C:
Pharmacotherapies for drug-induced liver injury: A current
literature review. Front Pharmacol. 12:8062492021. View Article : Google Scholar
|
|
11
|
Pose E, Napoleone L, Amin A, Campion D,
Jimenez C, Piano S, Roux O, Uschner FE, de Wit K, Zaccherini G, et
al: Safety of two different doses of simvastatin plus rifaximin in
decompensated cirrhosis (LIVERHOPE-SAFETY): A randomised,
double-blind, placebo-controlled, phase 2 trial. Lancet
Gastroenterol Hepatol. 5:31–41. 2020. View Article : Google Scholar
|
|
12
|
Bataller R, Arab JP and Shah VH:
Alcohol-Associated hepatitis. N Engl J Med. 387:2436–2448. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang L, Deng Y, Bai X, Wei X, Ren Y, Chen
S and Deng H: Cell therapy for end-stage liver disease: Current
state and clinical challenge. Chin Med J (Engl). 137:2808–2820.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Artru F, Trovato F, Morrison M, Bernal W
and McPhail M: Liver transplantation for acute-on-chronic liver
failure. Lancet Gastroenterol Hepatol. 9:564–576. 2024. View Article : Google Scholar
|
|
15
|
Li Y, Ye Y and Chen H: Astragaloside IV
inhibits cell migration and viability of hepatocellular carcinoma
cells via suppressing long noncoding RNA ATB. Biomed Pharmacother.
99:134–141. 2018. View Article : Google Scholar
|
|
16
|
Yao L, Hu X, Dai K, Yuan M, Liu P, Zhang Q
and Jiang Y: Mesenchymal stromal cells: Promising treatment for
liver cirrhosis. Stem Cell Res Ther. 13:3082022. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Volarevic V, Markovic BS, Gazdic M,
Volarevic A, Jovicic N, Arsenijevic N, Armstrong L, Djonov V, Lako
M and Stojkovic M: Ethical and safety issues of stem cell-based
therapy. Int J Med Sci. 15:36–45. 2018. View Article : Google Scholar :
|
|
18
|
Arab JP, Karpen SJ, Dawson PA, Arrese M
and Trauner M: Bile acids and nonalcoholic fatty liver disease:
Molecular insights and therapeutic perspectives. Hepatology.
65:350–362. 2017. View Article : Google Scholar :
|
|
19
|
Tilg H, Adolph TE, Dudek M and Knolle P:
Non-alcoholic fatty liver disease: The interplay between
metabolism, microbes and immunity. Nat Metab. 3:1596–1607. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ghazanfar H, Javed N, Qasim A, Zacharia
GS, Ghazanfar A, Jyala A, Shehi E and Patel H: Metabolic
dysfunction-associated steatohepatitis and progression to
hepatocellular carcinoma: A literature review. Cancers (Basel).
16:12142024. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nassir F: NAFLD: Mechanisms, treatments,
and biomarkers. Biomolecules. 12:8242022. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Akkız H, Gieseler RK and A Canbay A: Liver
fibrosis: From basic science towards clinical progress, focusing on
the central role of hepatic stellate cells. Int J Mol Sci.
25:78732024. View Article : Google Scholar
|
|
23
|
Malhi H and Gores GJ: Cellular and
molecular mechanisms of liver injury. Gastroenterology.
134:1641–1654. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hu X, Jiang J, Xu Q, Ni C, Yang L and
Huang D: A systematic review of long noncoding RNAs in
hepatocellular carcinoma: Molecular mechanism and clinical
implications. Biomed Res Int. 2018:81262082018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhou L, Li M, Chai Z, Zhang J, Cao K, Deng
L, Liu Y, Jiao C, Zou GM, Wu J and Han F: Anticancer effects and
mechanisms of astragaloside-IV. Oncol Rep. 49:52022. View Article : Google Scholar
|
|
26
|
Yang Y, Hong M, Lian WW and Chen Z: Review
of the pharmacological effects of astragaloside IV and its
autophagic mechanism in association with inflammation. World J Clin
Cases. 10:10004–10016. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chen C, Bu X, Deng L, Xia J, Wang X, Chen
L, Li W, Huang J, Chen Q and Wang C: Astragaloside IV as a
promising therapeutic agent for liver diseases: Current landscape
and future perspectives. Front Pharmacol. 16:15741542025.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wang T, Chen X, Gao Q, Huang C, Wang K and
Qiu F: Herb-drug interaction potential of Astragali Radix: A
metabolic perspective. Drug Metab Rev. 57:9–25. 2025. View Article : Google Scholar
|
|
29
|
Zhang J, Wu C, Gao L, Du G and Qin X:
Astragaloside IV derived from Astragalus membranaceus: A research
review on the pharmacological effects. Adv Pharmacol. 87:89–112.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Gu Y, Wang G, Pan G, Fawcett JP, J A and
Sun J: Transport and bioavailability studies of astragaloside IV,
an active ingredient in Radix Astragali. Basic Clin Pharmacol
Toxicol. 95:295–298. 2004. View Article : Google Scholar
|
|
31
|
Salehi B, Carneiro JNP, Rocha JE, Coutinho
HDM, Morais Braga MFB, Sharifi-Rad J, Semwal P, Painuli S, Moujir
LM, de Zarate Machado V, et al: Astragalus species: Insights on its
chemical composition toward pharmacological applications. Phytother
Res. 35:2445–2476. 2021. View Article : Google Scholar
|
|
32
|
Lu S, Chen KJ, Yang QY and Sun HR:
Progress in the research of Radix Astragali in treating chronic
heart failure: Effective ingredients, dose-effect relationship and
adverse reaction. Chin J Integr Med. 17:473–477. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Fu S, Zhang J, Menniti-Ippolito F, Gao X,
Galeotti F, Massari M, Hu L, Zhang B, Ferrelli R, Fauci A, et al:
Huangqi injection (a traditional Chinese patent medicine) for
chronic heart failure: A systematic review. PLoS One. 6:e196042011.
View Article : Google Scholar :
|
|
34
|
Ziyang T, Xirong H, Chongming A and
Tingxin L: The potential molecular pathways of Astragaloside-IV in
colorectal cancer: A systematic review. Biomed Pharmacother.
167:1156252023. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Xu Z, Zhou H, Zhang Y, Cheng Z, Wan M, Qin
W, Li P, Feng J, Shao S, Xue W, et al: Recent pharmacological
advances in the treatment of cardiovascular events with
Astragaloside IV. Biomed Pharmacother. 168:1157522023. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yuan F, Yang Y, Liu L, Zhou P, Zhu Y, Chai
Y, Chen K, Tang W, Huang Q and Zhang C: Research progress on the
mechanism of astragaloside IV in the treatment of asthma. Heliyon.
9:e221492023. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Tan YQ, Chen HW and Li J: Astragaloside
IV: An effective drug for the treatment of cardiovascular diseases.
Drug Des Devel Ther. 14:3731–3746. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Liang Y, Chen B, Liang D, Quan X, Gu R,
Meng Z, Gan H, Wu Z, Sun Y, Liu S and Dou G: pharmacological
effects of astragaloside IV: A review. Molecules. 28:61182023.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yu Y, Zhou L, Yang Y and Liu Y:
Cycloastragenol: An exciting novel candidate for age-associated
diseases. Exp Ther Med. 16:2175–2182. 2018.PubMed/NCBI
|
|
40
|
Monschein M, Ardjomand-Woelkart K, Rieder
J, Wolf I, Heydel B, Kunert O, Heuberger H and Bauer R: Accelerated
sample preparation and formation of astragaloside IV in astragali
radix. Pharm Biol. Oct 30–2013.Epub ahead of print.
|
|
41
|
Chen Q, Su Y, Ju Y, Ma K and Li W and Li
W: Astragalosides IV protected the renal tubular epithelial cells
from free fatty acids-induced injury by reducing oxidative stress
and apoptosis. Biomed Pharmacother. 108:679–686. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Huang XP, Tan H, Chen BY and Deng CQ:
Astragalus extract alleviates nerve injury after cerebral ischemia
by improving energy metabolism and inhibiting apoptosis. Biol Pharm
Bull. 35:449–454. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Xia D, Li W, Tang C and Jiang J:
Astragaloside IV, as a potential anticancer agent. Front Pharmacol.
14:10655052023. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhou R, Chen H, Chen J, Chen H, Wen Y and
Xu L: Extract from Astragalus membranaceus inhibit breast cancer
cells proliferation via PI3K/AKT/mTOR signaling pathway. BMC
Complement Altern Med. 18:832018. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zang Y, Wan J, Zhang Z, Huang S, Liu X and
Zhang W: An updated role of astragaloside IV in heart failure.
Biomed Pharmacother. 126:1100122020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yao M, Zhang L and Wang L: Astragaloside
IV: A promising natural neuroprotective agent for neurological
disorders. Biomed Pharmacother. 159:1142292023. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zhang WD, Zhang C, Liu RH, Li HL, Zhang
JT, Mao C, Moran S and Chen CL: Preclinical pharmacokinetics and
tissue distribution of a natural cardioprotective agent
astragaloside IV in rats and dogs. Life Sci. 79:808–815. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Li L, Zhang Y, Luo Y, Meng X, Pan G, Zhang
H, Li Y and Zhang B: The molecular basis of the anti-inflammatory
property of astragaloside IV for the treatment of diabetes and its
complications. Drug Des Devel Ther. 17:771–790. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Huang X, Zhou Y, Li Y, Wang T, Chen Y,
Zhou Y, Zhou X and Liu Q: Astragaloside IV inhibits inflammation
caused by influenza virus via reactive oxygen species/NOD-like
receptor thermal protein domain associated protein 3/Caspase-1
signaling pathway. Immun Inflamm Dis. 12:e13092024. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zhang X, Zhang F, Li Y, Fan N, Zhao K,
Zhang A, Kang J, Lin Y, Xue X and Jiang X: Blockade of PI3K/AKT
signaling pathway by Astragaloside IV attenuates ulcerative colitis
via improving the intestinal epithelial barrier. J Transl Med.
22:4062024. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Sun Q, Hu M, Yuan C, Ren B, Zhong M, Zhou
S, Wang X, Gao Q, Zeng M, Cai X and Song H: Astragaloside IV
ameliorates indomethacin-induced intestinal inflammation in rats
through inhibiting the activation of NLRP3 inflammasome. Int
Immunopharmacol. 135:1122812024. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lu R, Chen J, Liu B, Lin H, Bai L, Zhang
P, Chen D, Li H, Li J, Pang Y, et al: Protective role of
Astragaloside IV in chronic glomerulonephritis by activating
autophagy through PI3K/AKT/AS160 pathway. Phytother Res.
34:3236–3248. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wang X, Gao Y, Tian N, Zhu Z, Wang T, Xu
J, Wu B and Zhang N: Astragaloside IV represses high
glucose-induced mesangial cells activation by enhancing autophagy
via SIRT1 deacetylation of NF-κB p65 subunit. Drug Des Devel Ther.
12:2971–2980. 2018. View Article : Google Scholar
|
|
54
|
Wang Z, Wu Y, Pei C, Wang M, Wang X, Shi
S, Huang D, Wang Y, Li S, Xiao W, et al: Astragaloside IV
pre-treatment attenuates PM2.5-induced lung injury in rats: Impact
on autophagy, apoptosis and inflammation. Phytomedicine.
96:1539122022. View Article : Google Scholar
|
|
55
|
Yang B, Yang N, Chen Y, Zhu M, Lian Y,
Xiong Z, Wang B, Feng L and Jia X: An integrated strategy for
effective-component discovery of astragali radix in the treatment
of lung cancer. Front Pharmacol. 11:5809782021. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Guo X, Yin X, Liu Z and Wang J:
Non-Alcoholic fatty liver disease (NAFLD) pathogenesis and natural
products for prevention and treatment. Int J Mol Sci. 23:154892022.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Grgurevic I, Podrug K, Mikolasevic I,
Kukla M, Madir A and Tsochatzis EA: Natural history of nonalcoholic
fatty liver disease: Implications for clinical practice and an
individualized approach. Can J Gastroenterol Hepatol.
2020:91813682020. View Article : Google Scholar :
|
|
58
|
Buzzetti E, Pinzani M and Tsochatzis EA:
The multiple-hit pathogenesis of non-alcoholic fatty liver disease
(NAFLD). Metabolism. 65:1038–1048. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Wardani HA, Rahmadi M, Ardianto C, Balan
SS, Kamaruddin NS and Khotib J: Development of nonalcoholic fatty
liver disease model by high-fat diet in rats. J Basic Clin Physiol
Pharmacol.
30:/j/jbcpp.2019.30.issue-6/jbcpp-2019-0258/jbcpp-2019-0258.xml.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Puri P, Wiest MM, Cheung O, Mirshahi F,
Sargeant C, Min HK, Contos MJ, Sterling RK, Fuchs M, Zhou H, et al:
The plasma lipidomic signature of nonalcoholic steatohepatitis.
Hepatology. 50:1827–1838. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Zhai Y, Zhou W, Yan X, Qiao Y, Guan L,
Zhang Z, Liu H, Jiang J, Liu J and Peng L: Astragaloside IV
ameliorates diet-induced hepatic steatosis in obese mice by
inhibiting intestinal FXR via intestinal flora remodeling.
Phytomedicine. 107:1544442022. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Chen CL and Lin YC: Autophagy
dysregulation in metabolic associated fatty liver disease: A new
therapeutic target. Int J Mol Sci. 23:100552022. View Article : Google Scholar :
|
|
63
|
Liu G, Wang YH, Zhang T, Li YQ, Chen XY,
Dong W, Li W, Miao QX, Qiao WB, Tian HQ and Yin SL:
Astragaloside-IV promotes autophagy via the Akt/mTOR pathway to
improve cellular lipid deposition. Medicine (Baltimore).
103:e378462024. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Liang XY, Hong FF and Yang SL:
Astragaloside IV alleviates liver inflammation, oxidative stress
and apoptosis to protect against experimental non-alcoholic fatty
liver disease. Diabetes Metab Syndr Obes. 14:1871–1883. 2021.
View Article : Google Scholar :
|
|
65
|
Snyder GA and Sundberg EJ: Molecular
interactions in interleukin and toll-like receptor signaling
pathways. Curr Pharm Des. 20:1244–1258. 2014. View Article : Google Scholar
|
|
66
|
Erridge C: Endogenous ligands of TLR2 and
TLR4: Agonists or assistants? J Leukoc Biol. 87:989–999. 2010.
View Article : Google Scholar
|
|
67
|
Liu YL, Zhang QZ, Wang YR, Fu LN, Han JS,
Zhang J and Wang BM: Astragaloside IV improves high-fat
diet-induced hepatic steatosis in nonalcoholic fatty liver disease
rats by regulating inflammatory factors level via TLR4/NF-κB
signaling pathway. Front Pharmacol. 11:6050642021. View Article : Google Scholar
|
|
68
|
Zhou B, Zhou DL, Wei XH, Zhong RL, Xu J
and Sun L: Astragaloside IV attenuates free fatty acid-induced ER
stress and lipid accumulation in hepatocytes via AMPK activation.
Acta Pharmacol Sin. 38:998–1008. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Asadi A, Shadab Mehr N, Mohamadi MH,
Shokri F, Heidary M, Sadeghifard N and Khoshnood S: Obesity and
gut-microbiota-brain axis: A narrative review. J Clin Lab Anal.
36:e244202022. View Article : Google Scholar :
|
|
70
|
Zhang Y, Du M, Wang J and Liu P:
Astragaloside IV relieves atherosclerosis and hepatic steatosis via
MAPK/NF-κB signaling pathway in LDLR-/- Mice. Front Pharmacol.
13:8281612022. View Article : Google Scholar
|
|
71
|
Li Z, Zhu JF and Ouyang H: Progress on
traditional Chinese medicine in improving hepatic fibrosis through
inhibiting oxidative stress. World J Hepatol. 15:1091–1108. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Cheung F, Feng Y, Wang N, Yuen MF, Tong Y
and Wong VT: Effectiveness of Chinese herbal medicine in treating
liver fibrosis: A systematic review and meta-analysis of randomized
controlled trials. Chin Med. 7:52012. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Bataller R and Brenner DA: Liver fibrosis.
J Clin Invest. 115:209–218. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Chen Z, Yao L, Liu Y, Pan Z, Peng S, Wan
G, Cheng J, Wang J and Cao W: Astragaloside IV regulates
NF-κB-mediated cellular senescence and apoptosis of hepatic
stellate cells to suppress PDGF-BB-induced activation. Exp Ther
Med. 18:3741–3750. 2019.PubMed/NCBI
|
|
75
|
Li X, Wang X, Han C, Wang X, Xing G, Zhou
L, Li G and Niu Y: Astragaloside IV suppresses collagen production
of activated hepatic stellate cells via oxidative stress-mediated
p38 MAPK pathway. Free Radic Biol Med. 60:168–176. 2013. View Article : Google Scholar
|
|
76
|
Liu H, Wei W, Sun WY and Li X: Protective
effects of astragaloside IV on porcine-serum-induced hepatic
fibrosis in rats and in vitro effects on hepatic stellate cells. J
Ethnopharmacol. 122:502–508. 2009. View Article : Google Scholar
|
|
77
|
Zhao XM, Zhang J, Liang YN and Niu YC:
Astragaloside IV synergizes with ferulic acid to alleviate hepatic
fibrosis in bile duct-ligated cirrhotic rats. Dig Dis Sci.
65:2925–2936. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Bansal MB and Chamroonkul N: Antifibrotics
in liver disease: Are we getting closer to clinical use? Hepatol
Int. 13:25–39. 2019. View Article : Google Scholar
|
|
79
|
Odagiri N, Matsubara T, Sato-Matsubara M,
Fujii H, Enomoto M and Kawada N: Anti-fibrotic treatments for
chronic liver diseases: The present and the future. Clin Mol
Hepatol. 27:413–424. 2021. View Article : Google Scholar :
|
|
80
|
Siegel RL, Giaquinto AN and Jemal A:
Cancer statistics, 2024. CA Cancer J Clin. 74:12–49.
2024.PubMed/NCBI
|
|
81
|
Baecker A, Liu X, La Vecchia C and Zhang
ZF: Worldwide incidence of hepatocellular carcinoma cases
attributable to major risk factors. Eur J Cancer Prev. 27:205–212.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Llovet JM, Kelley RK, Villanueva A, Singal
AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J and
Finn RS: Hepatocellular carcinoma. Nat Rev Dis Primers. 7:62021.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Zhang Y, Zhang C, Wu N, Feng Y, Wang J, Ma
L and Chen Y: The role of exosomes in liver cancer: Comprehensive
insights from biological function to therapeutic applications.
Front Immunol. 15:14730302024. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Kalantari L, Ghotbabadi ZR, Gholipour A,
Ehymayed HM, Najafiyan B, Amirlou P, Yasamineh S, Gholizadeh O and
Emtiazi N: A state-of-the-art review on the NRF2 in Hepatitis
virus-associated liver cancer. Cell Commun Signal. 21:3182023.
View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Pugliese N, Alfarone L, Arcari I,
Giugliano S, Parigi TL, Rescigno M, Lleo A and Aghemo A: Clinical
features and management issues of NAFLD-related HCC: What we know
so far. Expert Rev Gastroenterol Hepatol. 17:31–43. 2023.
View Article : Google Scholar
|
|
86
|
Jacob R, Prince DS, Kench C and Liu K:
Alcohol and its associated liver carcinogenesis. J Gastroenterol
Hepatol. 38:1211–1217. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Jin J, Kouznetsova VL, Kesari S and
Tsigelny IF: Synergism in actions of HBV with aflatoxin in cancer
development. Toxicology. 499:1536522023. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Hamid AS, Tesfamariam IG, Zhang Y and
Zhang ZG: Aflatoxin B1-induced hepatocellular carcinoma in
developing countries: Geographical distribution, mechanism of
action and prevention. Oncol Lett. 5:1087–1092. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Pathomjaruwat T, Matchim Y and Armer JM:
Symptoms and symptom clusters in patients with hepatocellular
carcinoma and commonly used instruments: An integrated review. Int
J Nurs Sci. 11:66–75. 2023.
|
|
90
|
Xue Y, Ruan Y, Wang Y, Xiao P and Xu J:
Signaling pathways in liver cancer: Pathogenesis and targeted
therapy. Mol Biomed. 5:202024. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Chan YT, Zhang C, Wu J, Lu P, Xu L, Yuan
H, Feng Y, Chen ZS and Wang N: Biomarkers for diagnosis and
therapeutic options in hepatocellular carcinoma. Mol Cancer.
23:1892024. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Mehta N, Dodge JL, Roberts JP and Yao FY:
Validation of the prognostic power of the RETREAT score for
hepatocellular carcinoma recurrence using the UNOS database. Am J
Transplant. 18:1206–1213. 2018. View Article : Google Scholar
|
|
93
|
Zhu Y and Lu F: Astragaloside IV inhibits
cell viability and glycolysis of hepatocellular carcinoma by
regulating KAT2A-mediated succinylation of PGAM1. BMC Cancer.
24:6822024. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Fang Gong Y, Hou S, Xu JC, Chen Y, Zhu LL,
Xu YY, Chen YQ, Li MM, Li LL, Yang JJ and Yang Y: Amelioratory
effects of astragaloside IV on hepatocarcinogenesis via
Nrf2-mediated pSmad3C/3L transformation. Phytomedicine.
117:1549032023. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Li L, Wang Q, He Y, Sun L, Yang Y and Pang
X: Astragaloside IV suppresses migration and invasion of
TGF-β1-induced human hepatoma HuH-7 cells by regulating Nrf2/HO-1
and TGF-β1/Smad3 pathways. Naunyn Schmiedebergs Arch Pharmacol.
395:397–405. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Min L, Wang H and Qi H: Astragaloside IV
inhibits the progression of liver cancer by modulating macrophage
polarization through the TLR4/NF-κB/STAT3 signaling pathway. Am J
Transl Res. 14:1551–1566. 2022.
|
|
97
|
Ma Y, Li Y, Wu T, Li Y and Wang Q:
Astragaloside IV attenuates programmed death-ligand 1-mediated
immunosuppression during liver cancer development via the
miR-135b-5p/CNDP1 Axis. Cancers (Basel). 15:50482023. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Cui X, Jiang X, Wei C, Xing Y and Tong G:
Astragaloside IV suppresses development of hepatocellular carcinoma
by regulating miR-150-5p/β-catenin axis. Environ Toxicol Pharmacol.
78:1033972020. View Article : Google Scholar
|
|
99
|
Guo H, Zhao J and Wu C: Astragaloside
IV-enhanced anti-hepatocarcinoma immunity of dendritic cells. Asian
J Surg. 45:1216–1218. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Qi H, Wei L, Han Y, Zhang Q, Lau AS and
Rong J: Proteomic characterization of the cellular response to
chemopreventive triterpenoid astragaloside IV in human
hepatocellular carcinoma cell line HepG2. Int J Oncol. 36:725–735.
2010.PubMed/NCBI
|
|
101
|
Wang PP, Xu DJ, Huang C, Wang WP and Xu
WK: Astragaloside Ⅳ reduces the expression level of P-glycoprotein
in multidrug-resistant human hepatic cancer cell lines. Mol Med
Rep. 9:2131–2137. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Qu X, Gao H, Zhai J, Sun J, Tao L, Zhang
Y, Song Y and Hu T: Astragaloside IV enhances cisplatin
chemosensitivity in hepatocellular carcinoma by suppressing MRP2.
Eur J Pharm Sci. 148:1053252020. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Su CM, Wang HC, Hsu FT, Lu CH, Lai CK,
Chung JG and Kuo YC: Astragaloside IV induces apoptosis, G1-Phase
arrest and inhibits anti-apoptotic signaling in hepatocellular
carcinoma. In Vivo. 34:631–638. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Qin CD, Ma DN, Ren ZG, Zhu XD, Wang CH,
Wang YC, Ye BG, Cao MQ, Gao DM and Tang ZY: Astragaloside IV
inhibits metastasis in hepatoma cells through the suppression of
epithelial-mesenchymal transition via the Akt/GSK-3β/β-catenin
pathway. Oncol Rep. 37:1725–1735. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Jiang Z and Mao Z: Astragaloside IV
(AS-IV) alleviates the malignant biological behavior of
hepatocellular carcinoma via Wnt/beta-catenin signaling pathway.
RSC Adv. 9:35473–35482. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Dai S, Fu K, Liu Y, Yao Y, Zhang F, Wu R,
Guo Y, Yao C and Li Y: Vitexin: A dietary flavonoid with potential
protective effects against liver diseases. Food Rev Int.
40:3254–3290. 2024. View Article : Google Scholar
|
|
107
|
Ko S, Russell JO, Molina LM and Monga SP:
Liver progenitors and adult cell plasticity in hepatic injury and
repair: Knowns and unknowns. Annu Rev Pathol. 15:23–50. 2020.
View Article : Google Scholar
|
|
108
|
Hu PF and Xie WF: Corticosteroid therapy
in drug-induced liver injury: Pros and cons. J Dig Dis. 20:122–126.
2019. View Article : Google Scholar
|
|
109
|
Stravitz RT and Lee WM: Acute liver
failure. Lancet. 394:869–881. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Dossi CG, Vargas RG, Valenzuela R and
Videla LA: Beneficial effects of natural compounds on experimental
liver ischemia-reperfusion injury. Food Funct. 12:3787–3798. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Rani J, Dhull SB, Rose PK and Kidwai MK:
Drug-induced liver injury and anti-hepatotoxic effect of herbal
compounds: A metabolic mechanism perspective. Phytomedicine.
122:1551422024. View Article : Google Scholar
|
|
112
|
Cengiz M, Cetik Yildiz S, Demir C, Şahin
IK, Teksoy O and Ayhanci A: Hepato-preventive and anti-apoptotic
role of boric acid against liver injury induced by
cyclophosphamide. J Trace Elem Med Biol. 53:1–7. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Liu C, Wang R, Zhang B, Hu C and Zhang H:
Protective effects of lycopene on oxidative stress, proliferation
and autophagy in iron supplementation rats. Biol Res. 46:189–200.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Ramm GA and Ruddell RG: Hepatotoxicity of
iron overload: Mechanisms of iron-induced hepatic fibrogenesis.
Semin Liver Dis. 25:433–449. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Corradini E, Ferrara F and Pietrangelo A:
Iron and the liver. Pediatr Endocrinol Rev. 2(Suppl 2) (2004):
S245–S248. 2004.
|
|
116
|
Xie D, Zhou P, Liu L, Jiang W, Xie H,
Zhang L and Xie D: Protective effect of astragaloside IV on hepatic
injury induced by iron overload. Biomed Res Int. 2019:31039462019.
View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Gao Y, Chu S, Shao Q, Zhang M, Xia C, Wang
Y, Li Y, Lou Y, Huang H and Chen N: Antioxidant activities of
ginsenoside Rg1 against cisplatin-induced hepatic injury through
Nrf2 signaling pathway in mice. Free Radic Res. 51:1–13. 2017.
View Article : Google Scholar
|
|
118
|
Romani AMP: Cisplatin in cancer treatment.
Biochem Pharmacol. 206:1153232022. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Pezeshki Z, Khosravi A, Nekuei M,
Khoshnood S, Zandi E, Eslamian M, Talebi A, Emami SN and
Nematbakhsh M: Time course of cisplatin-induced nephrotoxicity and
hepatotoxicity. J Nephropathol. 6:163–167. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Tarladacalisir YT, Uygun M, Akpolat M and
UZ YH: Histologic examination of the protective effect of vitamin E
and C in cisplatin-induced hepatotoxicity. Trakya Univ Tip Fak
Derg. 22:124–131. 2005.
|
|
121
|
Qu X, Gao H, Tao L, Zhang Y, Zhai J, Sun
J, Song Y and Zhang S: Astragaloside IV protects against
cisplatin-induced liver and kidney injury via autophagy-mediated
inhibition of NLRP3 in rats. J Toxicol Sci. 44:167–175. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Guo J, Le Y, Yuan A, Liu J, Chen H, Qiu J,
Wang C, Dou X, Yuan X and Lu D: Astragaloside IV ameliorates
cisplatin-induced liver injury by modulating ferroptosis-dependent
pathways. J Ethnopharmacol. 328:1180802024. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Dixon SJ, Lemberg KM, Lamprecht MR, Skouta
R, Zaitsev EM, Gleason CE, Patel DN, Bauer AJ, Cantley AM, Yang WS,
et al: Ferroptosis: An iron-dependent form of nonapoptotic cell
death. Cell. 149:1060–1072. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Chen J, Li X, Ge C, Min J and Wang F: The
multifaceted role of ferroptosis in liver disease. Cell Death
Differ. 29:467–480. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
125
|
Guo J, Yin J, Liu P, Zhang X, Wei J, Wang
M, Xiao Y, Zhen Y, Lin Y and Li J: Glycyrrhizin arginine salt
protects against cisplation-induced acute liver injury by
repressing BECN1-mediated ferroptosis. Front Pharmacol.
14:12194862023. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Saito C, Zwingmann C and Jaeschke H: Novel
mechanisms of protection against acetaminophen hepatotoxicity in
mice by glutathione and N-acetylcysteine. Hepatology. 51:246–254.
2010. View Article : Google Scholar
|
|
127
|
Kim SJ, Kim KM, Yang JH, Cho SS, Kim JY,
Park SJ, Lee SK, Ku SK, Cho IJ and Ki SH: Sestrin2 protects against
acetaminophen-induced liver injury. Chem Biol Interact. 269:50–58.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Bunchorntavakul C and Reddy KR:
Acetaminophen (APAP or N-Acetyl-p-Aminophenol) and acute liver
failure. Clin Liver Dis. 22:325–346. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Li L, Huang W, Wang S, Sun K, Zhang W,
Ding Y, Zhang L, Tumen B, Ji L and Liu C: Astragaloside IV
attenuates acetaminophen-induced liver injuries in mice by
activating the Nrf2 signaling pathway. Molecules. 23:20322018.
View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Perez-Calahorra S, Laclaustra M,
Marco-Benedi V, Pinto X, Sanchez-Hernandez RM, Plana N, Ortega E,
Fuentes F and Civeira F: Comparative efficacy between atorvastatin
and rosuvastatin in the prevention of cardiovascular disease
recurrence. Lipids Health Dis. 18:2162019. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Qin L, Wang Y, Liang Y, Li Q, Xie X and
Zhang H: Astragaloside IV alleviates atorvastatin-induced
hepatotoxicity via AMPK/SIRT1 pathway. Pharmacology. 108:74–82.
2023. View Article : Google Scholar
|
|
132
|
Osna NA, Donohue TM Jr and Kharbanda KK:
Alcoholic liver disease: Pathogenesis and current management.
Alcohol Res. 38:147–161. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Wu S, Wen F, Zhong X, Du W, Chen M and
Wang J: Astragaloside IV ameliorate acute alcohol-induced liver
injury in mice via modulating gut microbiota and regulating
NLRP3/caspase-1 signaling pathway. Ann Med. 55:22169422023.
View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Wu D and Cederbaum AI: Oxidative stress
and alcoholic liver disease. Semin Liver Dis. 29:141–154. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Han L, Li J, Lin X, Ma YF and Huang YF:
(Protective effect of astragaloside IV on oxidative damages of
chang liver cell induced by ethanol and H2O2). Zhongguo Zhong Yao
Za Zhi. 39:4430–4435. 2014.In Chinese.
|
|
136
|
Albillos A, de Gottardi A and Rescigno M:
The gut-liver axis in liver disease: Pathophysiological basis for
therapy. J Hepatol. 72:558–577. 2020. View Article : Google Scholar
|
|
137
|
Hao J, Hu R, Zhao J, Li Y, Li Q and Zhang
X: Metabolomics combined with network pharmacology reveals the
protective effect of astragaloside IV on alcoholic liver disease.
Phytomedicine. 135:1560322024. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Ingawale DK, Mandlik SK and Naik SR:
Models of hepatotoxicity and the underlying cellular, biochemical
and immunological mechanism(s): A critical discussion. Environ
Toxicol Pharmacol. 37:118–133. 2014. View Article : Google Scholar
|
|
139
|
Zhang G, Li J, Xu Z, Zhou K, Zhao X, Wu X,
Liang C, Lai Z, Cheng Y, Meng C, Huang J and Deng Z: Exocarpium
citri grandis attenuates lipopolysaccharide-induced acute liver
injury through suppression of inflammatory, apoptotic, oxidative,
and ferroptotic pathways. Food Sci Nutr. 13:e710122025. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Sun Y, Ma Y, Sun F, Feng W, Ye H, Tian T
and Lei M: Astragaloside IV attenuates lipopolysaccharide induced
liver injury by modulating Nrf2-mediated oxidative stress and
NLRP3-mediated inflammation. Heliyon. 9:e154362023. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Shima T, Uto H, Ueki K, Takamura T, Kohgo
Y, Kawata S, Yasui K, Park H, Nakamura N, Nakatou T, et al:
Clinicopathological features of liver injury in patients with type
2 diabetes mellitus and comparative study of histologically proven
nonalcoholic fatty liver diseases with or without type 2 diabetes
mellitus. J Gastroenterol. 48:515–525. 2013. View Article : Google Scholar
|
|
142
|
Tan SY, Mei Wong JL, Sim YJ, Wong SS,
Mohamed Elhassan SA, Tan SH, Ling Lim GP, Rong Tay NW, Annan NC,
Bhattamisra SK and Candasamy M: Type 1 and 2 diabetes mellitus: A
review on current treatment approach and gene therapy as potential
intervention. Diabetes Metab Syndr. 13:364–372. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Kumar V, Xin X, Ma J, Tan C, Osna N and
Mahato RI: Therapeutic targets, novel drugs, and delivery systems
for diabetes associated NAFLD and liver fibrosis. Adv Drug Deliv
Rev. 176:1138882021. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Targher G, Corey KE, Byrne CD and Roden M:
The complex link between NAFLD and type 2 diabetes
mellitus-mechanisms and treatments. Nat Rev Gastroenterol Hepatol.
18:599–612. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Stefan N and Cusi K: A global view of the
interplay between non-alcoholic fatty liver disease and diabetes.
Lancet Diabetes Endocrinol. 10:284–296. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Zhu Y, Su Y, Zhang J, Zhang Y, Li Y, Han
Y, Dong X and Li W and Li W: Astragaloside IV alleviates liver
injury in type 2 diabetes due to promotion of AMPK/mTOR-mediated
autophagy. Mol Med Rep. 23:4372021. View Article : Google Scholar
|
|
147
|
Liu J and Man K: Mechanistic insight and
clinical implications of ischemia/reperfusion injury post liver
transplantation. Cell Mol Gastroenterol Hepatol. 15:1463–1474.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Cheng MX, Chen ZZ, Cai YL, Liu CA and Tu
B: Astragaloside IV protects against ischemia reperfusion in a
murine model of orthotopic liver transplantation. Transplant Proc.
43:1456–1461. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Zhang Q, Zhu LL, Chen GG and Du Y:
Pharmacokinetics of astragaloside iv in beagle dogs. Eur J Drug
Metab Pharmacokinet. 32:75–79. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Chang YX, Sun YG, Li J, Zhang QH, Guo XR,
Zhang BL, Jin H and Gao XM: The experimental study of Astragalus
membranaceus on meridian tropsim: The distribution study of
astragaloside IV in rat tissues. J Chromatogr B Analyt Technol
Biomed Life Sci. 911:71–75. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Xu M, Yin J, Xie L, Zhang J, Zou C, Zou J,
Liu F, Ju W and Li P: Pharmacokinetics and tolerance of toal
astragalosides after intravenous infusion of astragalosides
injection in healthy Chinese volunteers. Phytomedicine.
20:1105–1111. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Du Y, Zhang Q, Chen GG, Wei P and Tu CY:
Pharmacokinetics of Astragaloside IV in rats by liquid
chromatography coupled with tandem mass spectrometry. Eur J Drug
Metab Pharmacokinet. 30:269–273. 2005. View Article : Google Scholar
|
|
153
|
Gui D, Guo Y, Wang F, Liu W, Chen J, Chen
Y, Huang J and Wang N: Astragaloside IV, a novel antioxidant,
prevents glucose-induced podocyte apoptosis in vitro and in vivo.
PLoS One. 7:e398242012. View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Yu SY, Ouyang HT, Yang JY, Huang XL, Yang
T, Duan JP, Cheng JP, Chen YX, Yang YJ and Qiong P: Subchronic
toxicity studies of Radix Astragali extract in rats and dogs. J
Ethnopharmacol. 110:352–355. 2007. View Article : Google Scholar
|
|
155
|
Jiangbo Z, Xuying W, Yuping Z, Xili M,
Yiwen Z and Tianbao Z: Effect of astragaloside IV on the
embryo-fetal development of Sprague-Dawley rats and New Zealand
White rabbits. J Appl Toxicol. 29:381–385. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Xuying W, Jiangbo Z, Yuping Z, Xili M,
Yiwen Z, Tianbao Z and Weidong Z: Effect of astragaloside IV on the
general and peripartum reproductive toxicity in Sprague-Dawley
rats. Int J Toxicol. 29:505–516. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
Singh R and Lillard JW Jr:
Nanoparticle-based targeted drug delivery. Exp Mol Pathol.
86:215–223. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Zhao X, Sun L, Wang J, Xu X, Ni S, Liu M
and Hu K: Nose to brain delivery of Astragaloside IV by β-Asarone
modified chitosan nanoparticles for multiple sclerosis therapy. Int
J Pharm. 644:1233512023. View Article : Google Scholar
|
|
159
|
Yue Y, Liu X, Pang L, Liu Y, Lin Y, Xiang
T, Li J, Liao S and Jiang Y: Astragalus polysaccharides/PVA
nanofiber membranes containing astragaloside IV-Loaded liposomes
and their potential use for wound healing. Evid Based Complement
Alternat Med. 2022:97162712022. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Kong C, Sun J, Hu X, Li G and Wu S: A
tumor targeted nano micelle carrying astragaloside IV for
combination treatment of bladder cancer. Sci Rep. 14:177042024.
View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Sun R, Zhang A, Ge Y, Gou J, Yin T, He H,
Wang Y, Zhang G, Kong J, Shang L, et al: Ultra-small-size
Astragaloside-IV loaded lipid nanocapsules eye drops for the
effective management of dry age-related macular degeneration.
Expert Opin Drug Deliv. 17:1305–1320. 2020. View Article : Google Scholar : PubMed/NCBI
|