Introduction
Hepatocellular carcinoma (HCC) has become the second
leading cause of cancer-associated death, which affects patients
worldwide, and is associated with early recurrence and a poor
response to chemotherapy (1,2). As
our understanding of the roles of immune checkpoints in tumor cells
and the surrounding non-tumor cells in the cancer microenvironment
has advanced, novel technologies, such as Chimeric antigen receptor
T-cell therapy and PD-1/PD-L1 checkpoint inhibition therapy, have
been developed to target the immune environment of HCC to improve
the prognosis of patients following HCC resection (3-6).
However, the overall responses rates of patients treated with
specific checkpoint blockers in HCC, such as those targeting PD-1
or CTLA-4, are not favorable, possibly due to unknown changes to
the immune microenvironment (7).
The emergence of high-throughput nucleotide
sequencing analysis provides new perspectives to understand the
genomic changes in tumors, revealing the differentially expressed
genetic signatures between tumor tissues and normal tissues
(8,9). Several studies in
different types of cancer, including breast cancer, thyroid cancer,
non-squamous non-small cell lung cancer and colorectal carcinoma,
have examined differences in the patterns of immune signatures to
improve our understanding of the immune environment and the
mechanisms underlying tumor development and progression (10-14).
However, the specific immune genetic changes in HCC have not been
extensively studied, although one study found that the levels of
immune cells infiltration, specifically by T-cells, cytotoxic
cells, Th2 cells and macrophages, in HCC were associated with
improved survival in patients based on n silico analysis,
suggesting that the type of immune cells present in HCC tissues
were different from the immune cell profile of the normal liver
(15). As the liver is now
considered to a 'immune associated organ', the presence of immune
cells in HCC should be taken into consideration as a leading factor
for predicting prognosis following resection, and should not be
restricted to specific types of immune cells (16-18).
In the present study, the changes in expression of
immune related genes in HCC tissues were compared with the adjacent
healthy matching tissues, using bioinformatics analysis. The
immune-associated genes identified was derived from a comprehensive
study of the immune landscape of 20 solid tumors, which allowed for
evaluation of relevant immune functions and the immune status of
solid tumors in a simplified manner (19,20).
The aim of the present study was to identify the immune-related
genetic changes between HCC tissues and normal liver tissues, to
understand the effects of immune regulation of HCC, and the effect
on progression of HCC. Additionally, an immune evaluating model for
prognostic evaluation in HCC patients was constructed, with the aim
of differentiating patients into sub-populations for more
personalized clinical treatment to maximize the efficacy of
therapies used, particularly for treatment with immune checkpoint
inhibition.
Materials and methods
Datasets
Data on patients with HCC were obtained from The
Cancer Genome Atlas (TCGA; cancer.gov/tcga)
and ICGC (icgc.org), which are publicly available databases
(21,22). The databases contained information
on 370 (TCGA) and 232 cases (ICGC) of HCC, which included RNA
sequencing information and the clinical characteristics (Table I). In the data obtained from TCGA,
there were 249 men and 121 women with a median age of 61 (range,
16-85). In the ICGC dataset, there were 171 men and 61 women with a
median age of 69 (range, 31-89). The list of immune-related genes
for analysis was obtained from previous studies (19,20)
which contained a total of 821 immune related genes.
 | Table IClinicopathological characteristics
of patients in TCGA and ICGC. |
Table I
Clinicopathological characteristics
of patients in TCGA and ICGC.
| TCGA. n=370 |
|---|
| Clinical
characteristics | n | % |
| Survival
status |
| Survived | 244 | 6555 |
| Died | 126 | 34.05 |
| Age |
| ≤65 years | 232 | 62.70 |
| >65 years | 138 | 37.30 |
| Sex |
| Male | 249 | 67.30 |
| Female | 121 | 32.70 |
| Histological
grade |
| G1 | 55 | 14.86 |
| G2 | 177 | 47.84 |
| G3 | 121 | 32.70 |
| G4 | 12 | 3.24 |
| Stage |
| I | 171 | 46.22 |
| II | 85 | 22.57 |
| III | 85 | 22.57 |
| IV | 5 | 1.35 |
| T
classification |
| T1 | 181 | 4852 |
| T2 | 93 | 25.14 |
| T3 | 80 | 21.62 |
| T4 | 13 | 3.51 |
| TX | 1 | 0.27 |
| M
classification |
| M0 | 266 | 71.89 |
| Ml | 4 | 1.08 |
| MX | 100 | 27.03 |
| N
classification |
| N0 | 252 | 68.11 |
| NI | 4 | 1.08 |
| NX | 113 | 30.54 |
| ICGC, n=232 |
| Clinical
characteristics | n | % |
| Survival
status |
| Survived | 189 | 81.47 |
| Died | 43 | 18.53 |
| Age |
| ≤65 years | 90 | 38.79 |
| >65 years | 142 | 61.21 |
| Sex |
| Male | 171 | 73.71 |
| Female | 61 | 26.29 |
| Clinical
characteristics | n | % |
| Stage |
| I | 36 | 15.52 |
| II | 106 | 45.69 |
| III | 71 | 30.60 |
| IV | 19 | 8.19 |
| Prior
malignancy |
| No | 202 | 87.07 |
| Yes | 30 | 12.93 |
Differential expression analysis
DEIGs between adjacent and HCC tissues were analyzed
using the limma package on the cohort from TCGA (23). The raw data were normalized and
log2(x+1) transformed. Genes with a fold change >1 and an
adjusted P-value <0.05 were considered significant (based on
false discovery rates using the Benjamini-Hochberg approach)
(24). A heatmap of significantly
up or downregu-lated immune-associated genes was plotted using the
heatmap package version 1.8.0 (git.bioconductor.org/packages/heat-maps), and these
genes were used for further prognostic analysis.
Gene ontology annotation and pathway
enrichment
Immune genes determined to be significantly
differentially expressed were functionally annotated using the
clusterProfiler package (25),
which stratified pathways according to one of the following
categories: Cellular compartment, biological process or molecular
function, and Kyoto Encyclopedia of Genes and Genomes (KEGG)
analysis was performed to enrich the pathways associated with the
identified genes (26).
Construction of the immune risk score
(IRS) model
The entire cohort of patients with HCC from TCGA
were randomly divided into a training set and a testing set to
construct and assess the prognostic model. The DEIGs were evaluated
using a univariate Cox model for individual risk factors affecting
OS of the training set (P<0.05), and the associated genes were
analyzed together using a Lasso penalty linear regression model,
which were subsequently used to construct a multivariate Cox model.
In Lasso regression, the patients were subsampled 1,000 times, and
the genes with an occurrence >900 instances were selected. In
multivariate Cox regression analysis, a stepwise method is used,
where all combinations of the identified genes are assessed to
construct the best combination of the immune associated gene set.
The prognostic value of the linear IRS model was validated in the
testing set, the entire TCGA cohort and the independent cohort from
the ICGC database separately, with patients divided into high- and
low- risk sub-populations according to the median IRS. Kaplan-Meier
survival curves and time-dependent receiver operating
characteristic curves (ROC) were used to demonstrate the prognostic
value of the 5-gene IRS model, using the R packages of survival
(rdocumentation.org/packages/survival)
and survivalROC (27).
Independent prognostic value of IRS and
the construction of a nomogram
The independent prognostic value of IRS was further
examined through univariate and multivariate Cox regression
analysis in combination with the clinical characteristics, such as
age, sex, tumor grade and tumor stages. Following evaluation of the
risk effect of clinical characteristics and IRS, a nomogram model
was constructed for prognostic prediction, which included the IRS
and tumor stage. The predictive value of the nomogram was further
confirmed using ROC curves for prediction of the 1, 3 and 5 year OS
rates, in which the predictive value of the single risk factors
were also assessed independently. The C-index of the nomogram was
calculated with a bootstrap of 1,000 resamples, and the results
ranged between 0.5-1.0, where 0.5 indicated a random chance and 1.0
indicated perfect separation of the outcomes. Calibration curves
were also plotted to demonstrate the precision of the nomogram,
contrasting the predictive probability with the actual
incidence.
Tumor infiltrating immune cells and their
correlation with IRS
The calculation of tumor infiltrating immune cells
in patients with HCC from TCGA was performed using Tumor IMmune
Estimation Resource (TIMER), an online tool which contains the
reanalyzed genomic expression data across 32 types of cancer,
including over 10,897 samples from TCGA (28,29).
The online portal calculates the abundance of 6 types of
infiltrating immune cells; B cells, CD4+ T cells, CD8+ T cells,
neutrophils, dendritic cells and macrophages. The abundance of
infiltrating immune cells was correlated with IRS, and significance
was examined using a Pearson's correlation test. P<0.05 was
considered to indicate a statistically significant difference. The
degree of correlation between immune cell abundance and IRS was
defined as follows: Very low, 0.0-0.2; low, 0.2-0.4; medium,
0.4-0.6; high, 0.6-0.8; and very high, 0.8-1.0.
Statistical analysis
Statistical analysis was performed in R (version
3.6.1), using R studio (version 1.2.1335) (30,31).
DEIGs between adjacent and HCC tissues were analyzed using a
Wilcoxon Signed-rank test. Univariate Cox regression, Lasso
regression and multivariate Cox regression analysis were performed
to construct the IRS model. The infiltration levels of different
immune cells between HCC and para-tumor tissues were compared using
Pearson's correlation coefficients. P<0.05 was considered to
indicate a statistically significant difference.
Results
Analysis strategy and overview of the
DEIGs
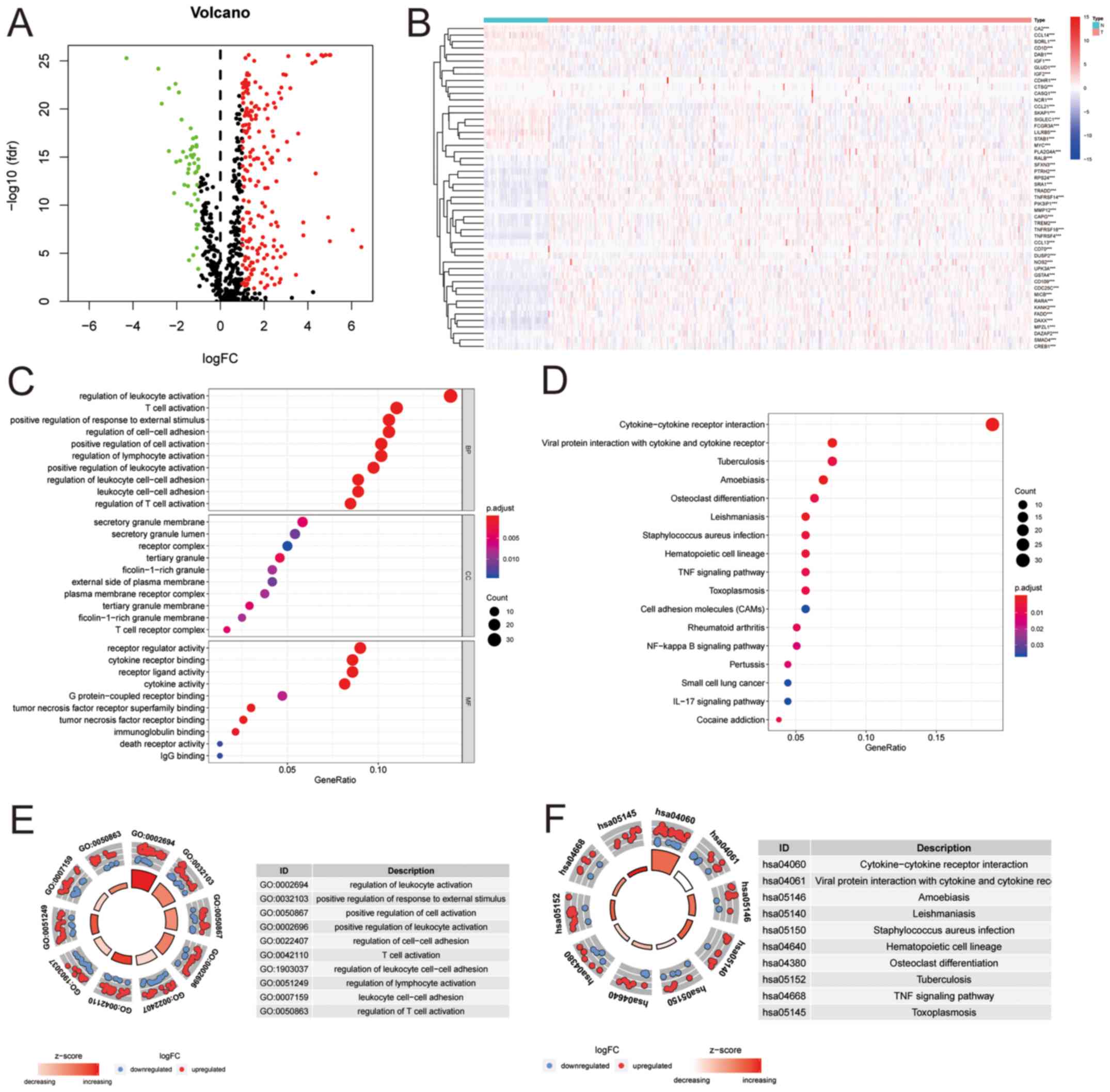
Analysis of the TCGA dataset identified 247
significantly differently expressed genes, of which 200 were
upregulated and 47 were downregulated (Fig. 1A and B). Gene ontology of the DEIGs
were primarily associated with immune cell activation, adhesion or
responses to stimuli (Fig. 1C and
E). The enriched pathways for those DEIGs were primarily
enriched in cytokine and cytokine receptor interactions between
cells, in which the cytokine-cytokine receptor interaction pathways
had the highest counts of associated genes and significance.
Additionally, the z-score of the cytokine-cytokine receptor
interaction pathways was the highest ranked amongst all enriched
pathways (Fig. 1D and F).
Relative risk effect of the immune
associated genes and construction of the IRS based
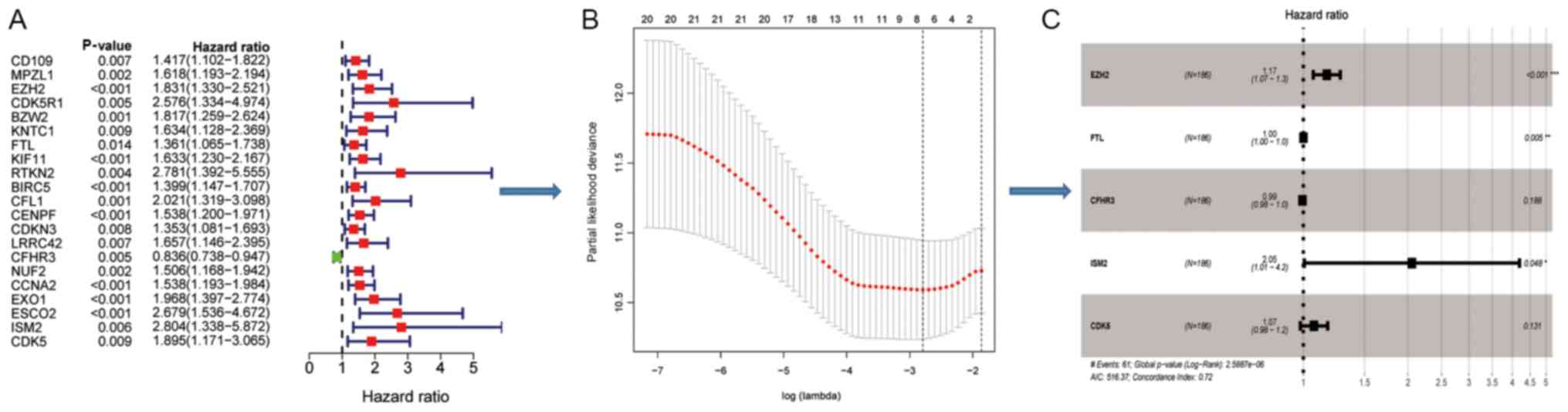
Patients from TCGA were divided into two sets; a
training set and an internal test set. In the training set,
significant DEIGs (P<0.05) associated with OS in the Cox model
(Fig. 2A), were further analyzed
using a Lasso penalty linear regression model (Fig. 2B). The final multivariate Cox model
was constructed using 5 genes [Enhancer of zest homology 2 (EZH2),
ferritin light chain (FTL), complement factor H related 3 (CFHR3),
isthmin 2 (ISM2), cyclin dependent kinase 5 (CDK5)], of which EZH2
and ISM2 still significant and had high risk effect following
adjustment (Fig. 2C).
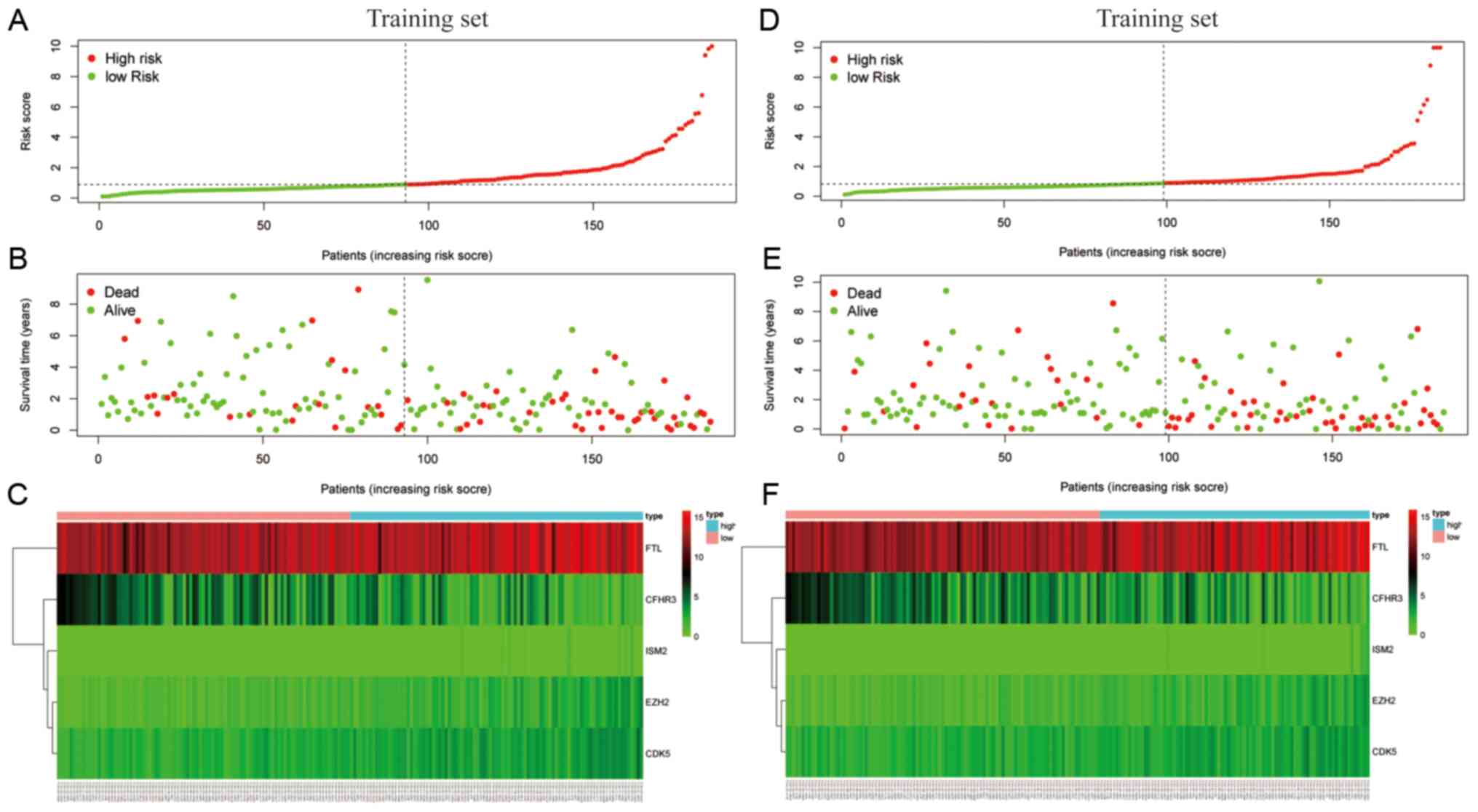
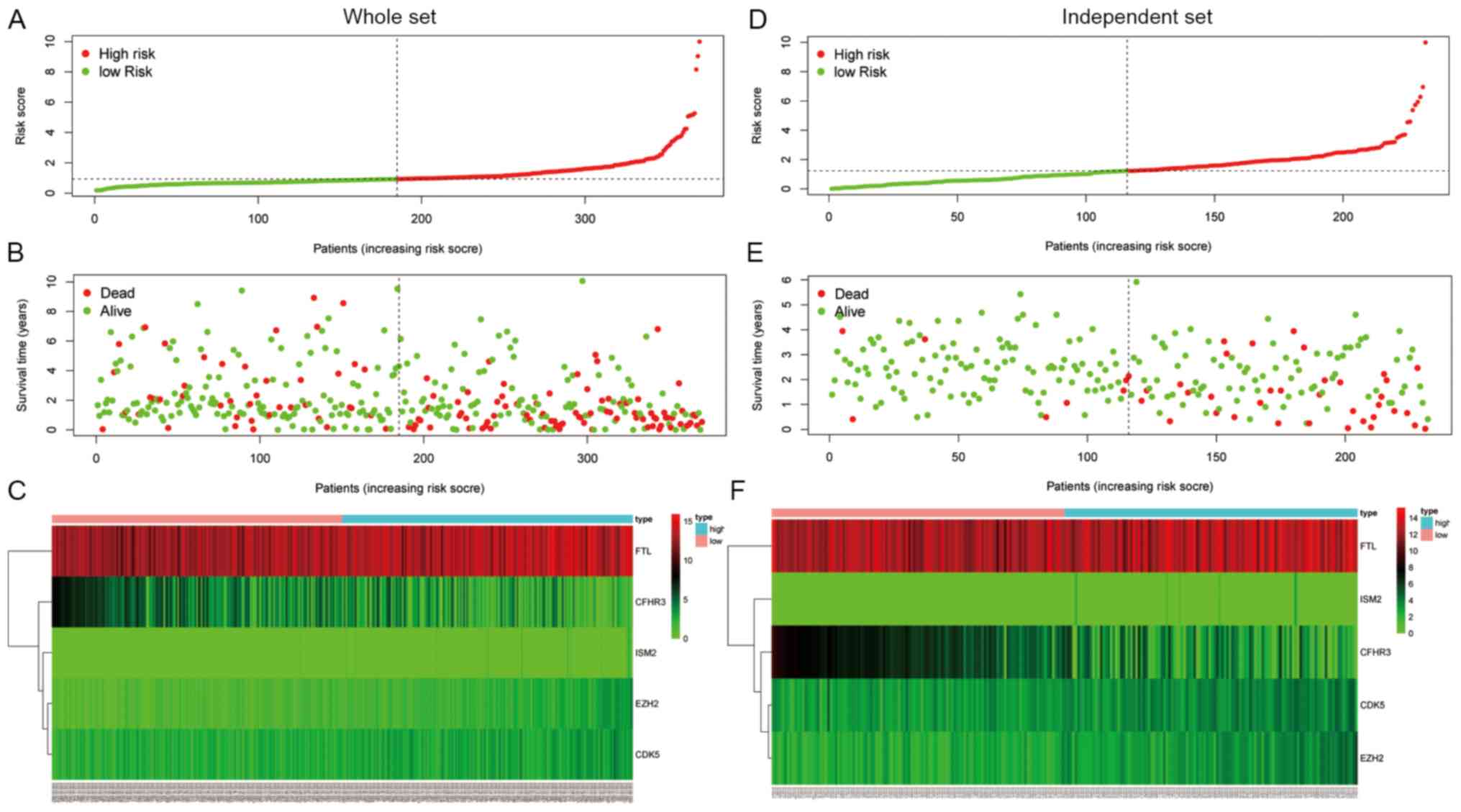
The final model was then used to calculate the IRS
of patients for prognostic evaluation in four separate cohorts: The
training cohort from TCGA (Fig.
3A-C), the test cohort from TCGA (Fig. 3D-F), the entire TCGA cohort
(Fig. 4A-C) and the independent
cohort from ICGC (Fig. 4D-F). The
median IRSs of the four cohorts were used to stratify patients into
high- and low-score groups.
Survival validation of the IRS model
The IRS model, based on the 5 significantly changed
immune associated genes, was able to divide the patients with HCC
into high- and low-risk sub-groups based on the corresponding score
levels. Patients with higher scores had a worse prognosis in all
four cohorts (Fig. 5A-D). The area
under the curve (AUC) values of the model for 0.5, 1, 2, 3 and 5
year survival in all four cohorts were all ~0.7, with a lowest
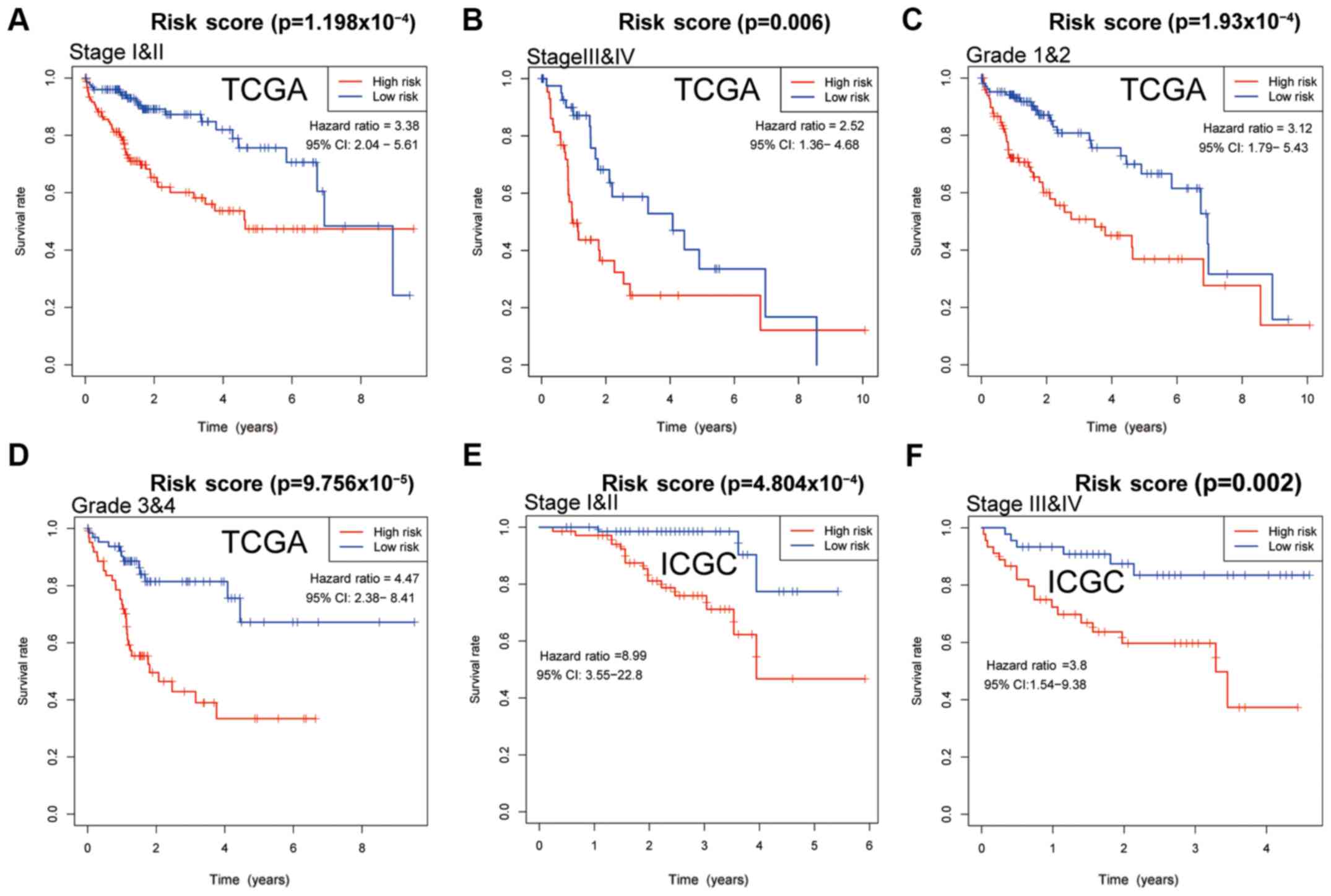
value of 0.643 for 5 year survival in the test cohort (Fig. 5E-H) Further analysis of patients
with different tumor stages and grades, showed that a high IRS
predicted worse survival in both datasets from TCGA and ICGC
(P<0.05), demonstrating the independent prognostic value of IRS
for clinical use. In patients with stage I & II, III & IV
and grade 1 & 2 cancer in TCGA, the curves for high- and
low-IRS showed notable differences in the 6 year survival, whereas
after 6 years of follow-up, the curves nearly overlapped (Fig. 6A-C). In patients with grade 3 &
4 cancer from TCGA, and stage I & II, and III & IV patients
from ICGC, the curves of patients with high- and low-IRS diverted
with no overlap (Fig. 6D-F).
Regarding disease free survival, patients with a high IRS also
exhibited worse outcomes compared with patients with a low IRS, and
this difference was significant in the entire TCGA cohort, in
patients with stage I & II, and grade 1 & 2 cancer from
TCGA (Fig. S1).
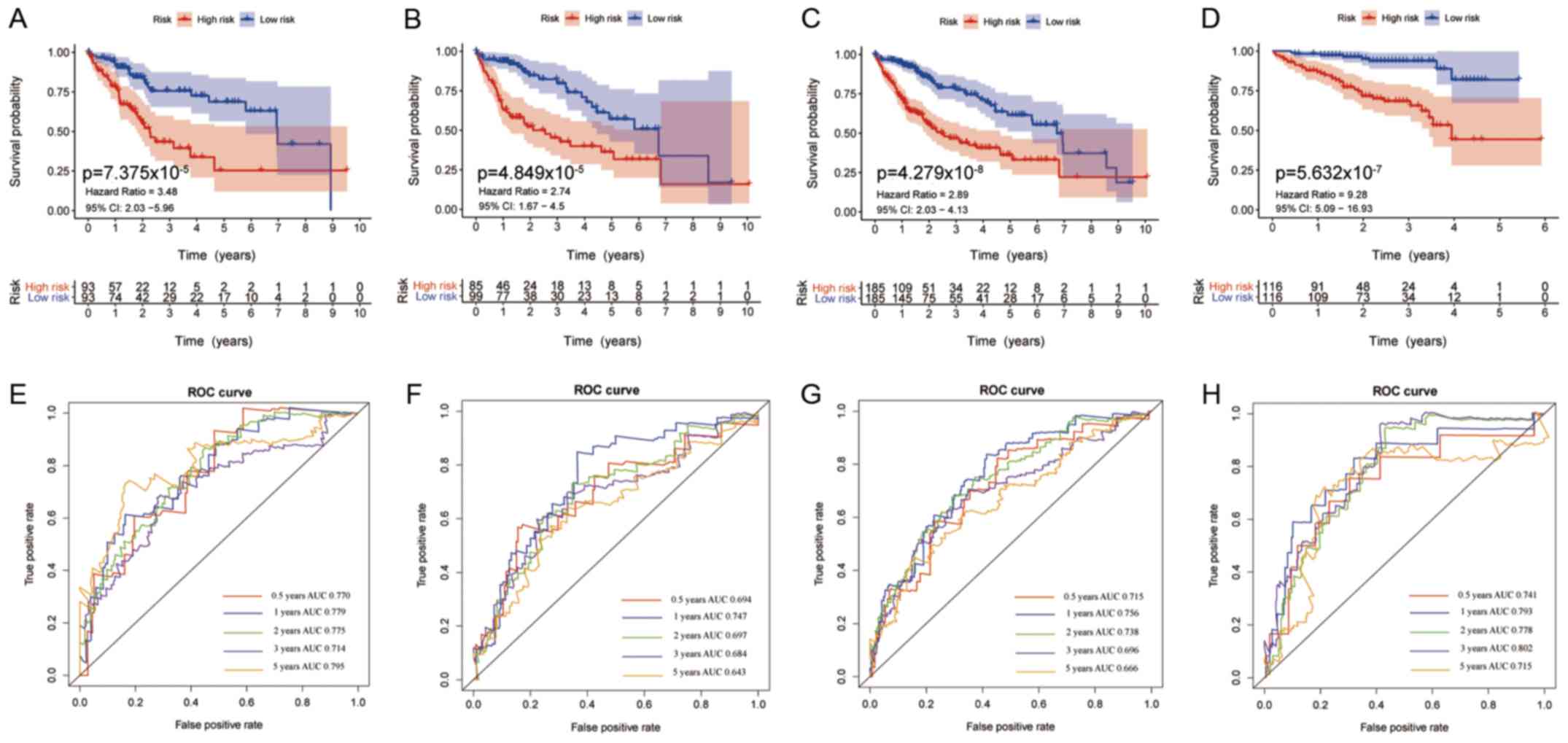 | Figure 5Survival curves of patients with
different IRS and the predictive value of the IRS for 0.5, 1, 2, 3
and 5 year survival. Survival curves of patients stratified by the
IRS in the (A) training set, (B) testing set, (C) entire TCGA
cohort and the (D) external International Cancer Gene Consortium
cohort. Survival was compared using a log-rank test; P<0.05 was
considered to indicate a statistically significant difference. ROC
curves for 0.5, 1, 2, 3 and 5 year survival in the (E) training
set, (F) testing set, (G) entire TCGA cohort and (H) ICGC cohort.
IRS, immune risk score; TCGA, The Cancer Genome Atlas; ICGC,
International Cancer Gene Consortium; ROC, receiver operating
characteristic curve; AUC, area under the curve; CI, confidence
interval. |
Nomogram of IRS and other associated
clinical factors
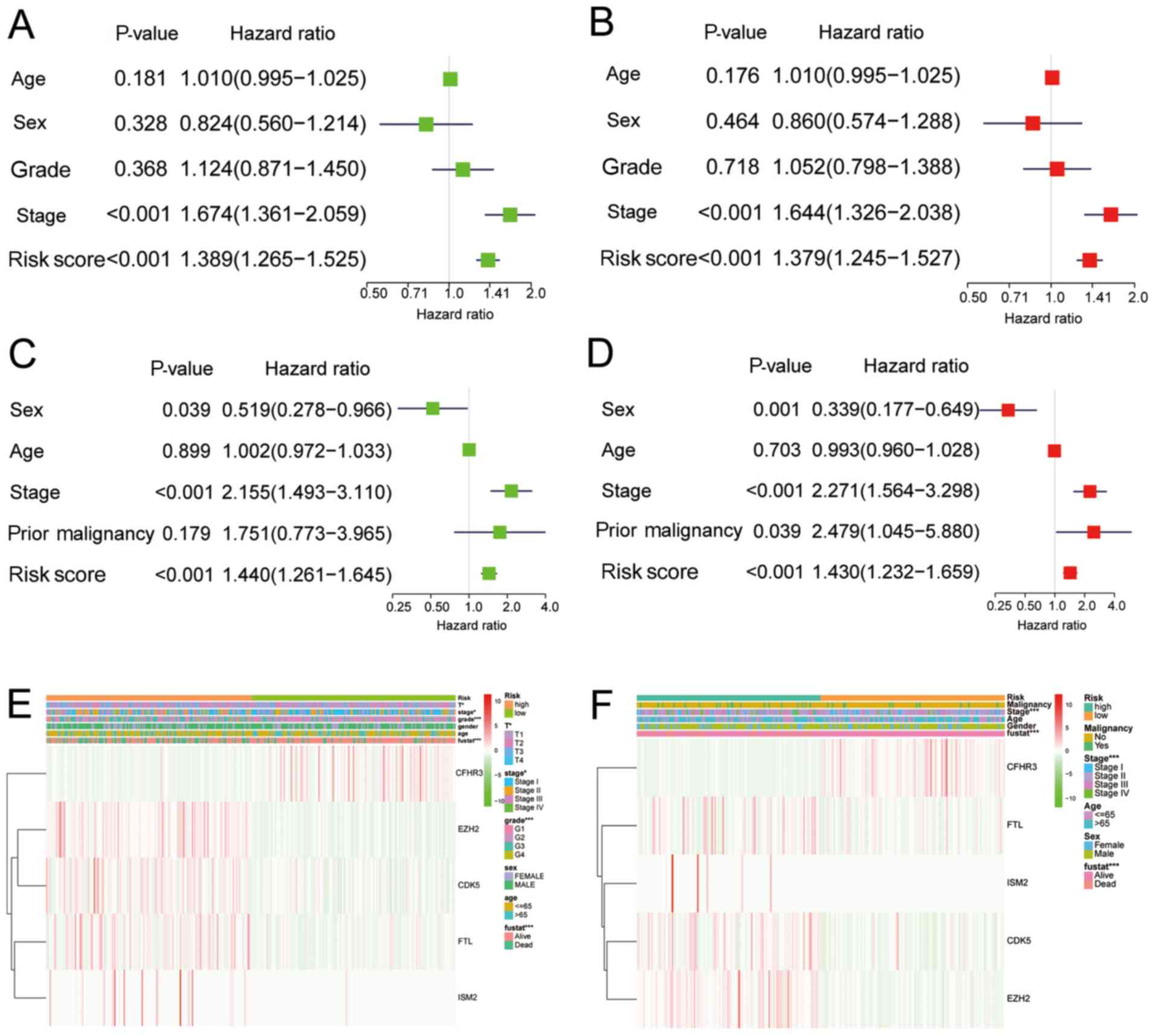
To assess the clinical relevance and significance of
the IRS model, the IRS model was combined with the clinical
characteristics for prognostic prediction of the data obtained from
TCGA and ICGC. In univariate and multivariate analysis of patients
from TCGA, cancer stage and IRS were significantly associated with
survival, with or without adjustment (Fig. 7A and B). In the ICGC dataset, in
addition to cancer stage and IRS, the presence of a previous
malignancy was also significantly associated with survival
following adjustment (Fig. 7C and
D). The correlations between the 5-gene model and clinical
characteristics are presented in Fig.
7E and F.
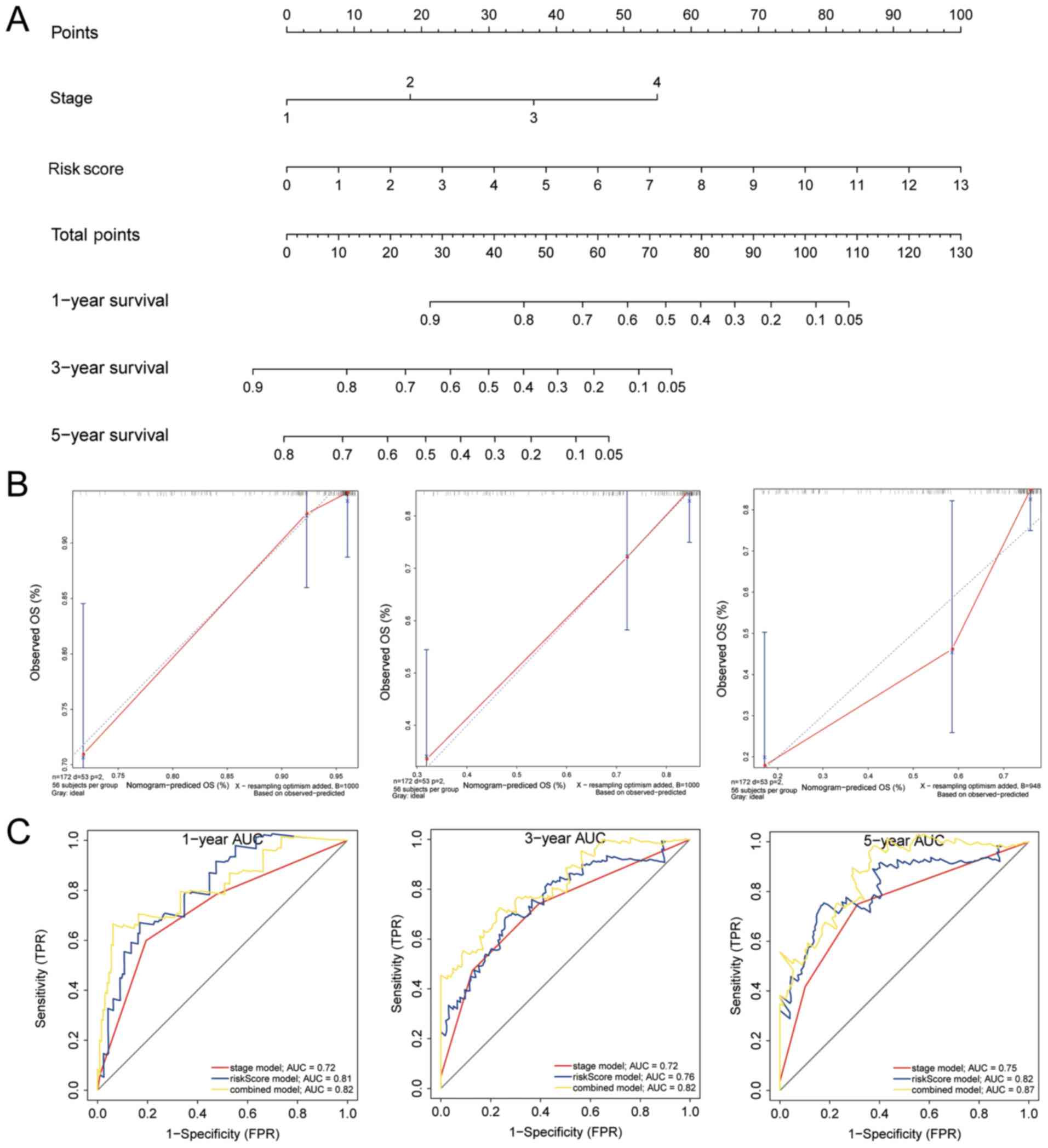
For clinical use, a nomogram was constructed for all
the significant factors, including clinical tumor stage and IRS,
using the entire TCGA cohort. (Fig.
8A) The AUCs for 1, 3 and 5 year survival were higher in the
nomogram compared with IRS or tumor stage (Fig. 8C) The C-index for the
nomogram-predicted OS was 0.749, with 1,000 cycles of bootstrapping
(Table II). Calibration graphs
were drawn to evaluate the corresponding performance of the
nomogram for predicting 1, 3 and 5 year OS, and the lines almost
overlapped, suggesting its accuracy (Fig. 8B). These results all show the value
of the nomogram for predicting OS in patients following resection,
and was shown to be more accurate than tumor stage or IRS, for both
short- and long-term.
| Table IIC-index analysis of models. |
Table II
C-index analysis of models.
| Model | C-index |
|---|
| Stage model | 0.654 |
| Prognostic
model | 0.746 |
| Nomogram model | 0.749 |
Potential roles of immune infiltrating
cells in prognostic prediction
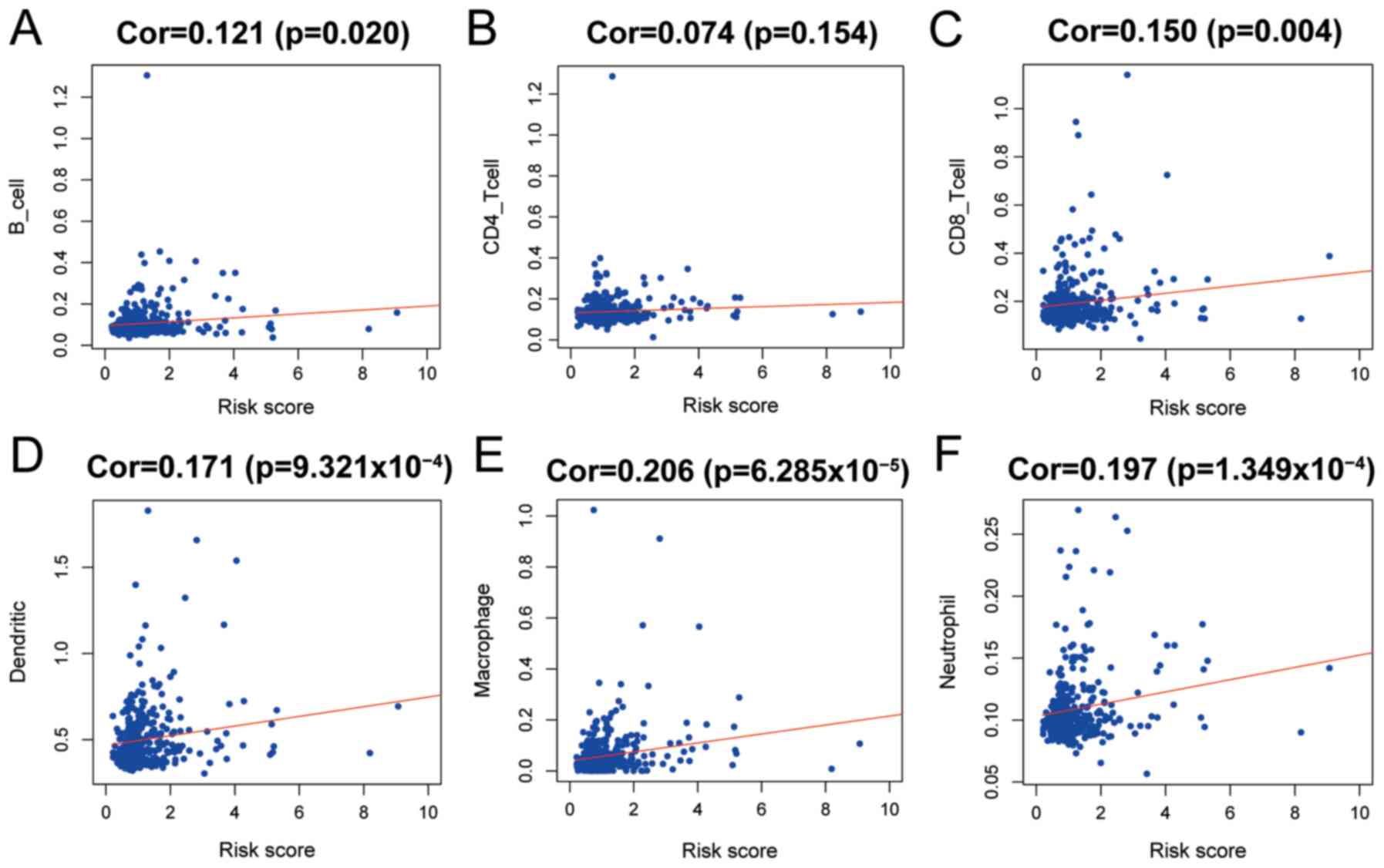
Using the evaluation scores of six common types of
immune infiltrating cells from TIMER, the abundance of immune-cells
in HCC tissue was estimated. Patients in TCGA were used to
calculate the abundance of infiltration, and a score was generated
by the tool. The correlation between the scores of B cells, CD8+ T
cells, dendritic cells, macrophages, neutrophils and IRS were
significant and positive, suggesting an association between
increased infiltration and IRS (Fig.
9). However, five types of infiltrating immune cells had very
low correlation coefficients with IRS, and macrophages had a low
correlation, suggesting that the IRS based on the five-gene model
was primarily dependent on change sin expression of
immune-associated genes in HCC tissues, as opposed to infiltration
of immune cells.
Discussion
Malignant HCC is associated with poor outcomes and
with high recurrence rates following resection (1,2). In
addition, a growing body of evidence highlights the vital value of
immune regulation in HCC, and poor responses to treatment with
chemotherapy highlight the need for drugs with greater specificity
for immune targets (3-6). The development of immune checkpoint
blockers, such as nivolumab and pembrolizumab have not yielded
optimistic results for patients with HCC, and this may be
associated with the immune microenvironment of HCC tissues, as
patients with a high degree of immune cell infiltration often
exhibit more favorable outcomes (3). Understanding the immune environment
and immune status of HCC may result in improved strategies for
treatment of patients, resulting in improved prognosis.
In the present study, the differentially expressed
immune associated genes between HCC and adjacent tissues were
identified, and following Lasso regression and multivariate Cox
analysis, 5 significantly differentially expressed OS-related
immune associated genes (EZH2, FTL, CFHR3, ISM2, CDK5) were used to
build a prognostic nomogram in combination with clinical
characteristics. The prognostic values of the nomogram for 1, 3 and
5 year survival achieved was >0.8, and performed better compared
with the individual clinical risk factors, and may thus be used to
stratify patients with HCC in clinical practice, preventing early
recurrence.
EZH2 is expression is low in the normal liver, and
is associated with methylation of histone H3K27 and recruitment of
methyltransferases, which are involved in DNA replication for
cancer progression, and stem cell maintenance and differentiation
of other cell lineages, such as immune cells (32,33).
Several studies have confirmed its prognostic value and importance
in various types of cancer, including lymphoma, glioma, head and
neck carcinoma, and cervical neoplasia (34-38).
Novel therapeutic methods have been developed to target EZH2,
although high expression of EZH2 is not always correlated with the
malignancy of a cancer, such as in colorectal cancer (39-41).
In the present study, it was shown that high expression of EZH2 was
significantly associated with poor OS in patients in the univariate
analysis, including after adjustment, highlighting the prognostic
value of high EZH2 expression in patients with HCC. EZH2 may
promote the development and proliferation of HCC, and may thus
result in recurrence following tumor resection.
Ferritin light chain (FTL) is the light subunit of
the ferritin protein, which is involved in iron release and uptake
in tissues. Several allergic diseases, inflammation status and
oxidative damage are associated with the roles of FTL, including
systemic lupus erythematosus, cataracts, hepatitis E virus
infection and Alzheimer's disease (42-47).
FTL also serves a role in cancer, where the dysfunction of iron
metabolism is a hallmark of various types of cancer, and is
involved drug resistance and malignant progression (48-50).
Although the risk effect of FTL was small following adjustment in
the multivariate Cox model, the potential role of changes to iron
metabolism in the progression of HCC should not be ignored.
CFHR3 was demonstrated to exert a protective effect
in patients with HCC, and physiologically, CFHR3 is exclusively
expressed in normal liver (51).
CFHR3 is associated with compliment factor H, which can bind to the
C3d region of C3b, regulating the function of compliment system
(52). The loss of CFHR3 results
in age-related macular degeneration, and high expression levels of
CFHR3 may result in atypical hemolytic-uremic syndrome (53-54).
There are no published articles regarding the expression of CFHR3
in cancer, and the protective role of CFHR3 observed in the present
study may highlight a potential change in the expression profile
that may be used for improving the prognosis of patients with
HCC.
In both univariate and multivariate analysis, ISM2
was significantly associated with poor outcomes and was considered
a high risk factor in patients with HCC. ISM2 is a component of
thrombospondin (THBS), which promotes the activity of mesenchymal
and stromal cells through TGF-β, and regulates secretion of
inflammatory cytokines through the NF-κB signaling pathway
(55,56). THBS promotes
epithelial-to-mesenchymal transition in melanoma, and exacerbates
the progression of prostate cancer to more advanced stages
(57,58). Additionally, THBS may serve a role
in gastric carcinogenesis, and invasiveness of breast cancer and
nodal metastasis (59-62). The role of ISM2 or THBS in HCC has
not been explored to the best of our knowledge, and further
analysis is required to understand their potential roles and
effects.
CDK5 has been extensively studied as an important
factor in tumor development and metastasis (63-65).
Although CDK5 shares homologous structure with other CDKs, it is
not cyclin-dependent and does not need to be phosphorylated in the
T-loop for activation (66). CDK5
expression is upregulated in several types of cancer, and
inhibition induces cancer cell death through a FOXO1-Bim pathway or
mitochondrial dysfunction (67-73).
Ehrlich et al (74) showed
that expression of CDK5 was increased in HCC tissues, and was
correlated with malignant phenotypes. Additionally, CDK5 was most
active in the G2/M phase of cancer cells in the nucleus, and
regulated DNA damage response through phosphorylation of ataxia
telangiectasia mutated kinase, validating the prognostic role of
CDK5 in the present study.
Infiltration of immune cells in HCC tissues was
assessed, and 5 of the 6 common types of immune cells were
significantly associated with IRS; however the correlation
coefficients for all 6 types of cells were either low or very low.
Thus, although patients with a high degree of immune cell
infiltration may have a high IRS, the IRS based on the five immune
associated genes primarily accounted for the functional status of
the microenvironment in HCC tissues. Recent studies have focused on
the roles of infiltrating immune cells in the tumor
microenvironment, to explain the mechanisms underlying immune
evasion and to predict drug response or prognosis (75-77).
Further analysis of the sub-types of immune cells in HCC may
improve our understanding of immune function in tumor, and with
advances in technologies, changing the types of immune cells
present may be considered as a potential treatment strategy,
emphasizing the importance of restoring immune function in HCC
(78-80).
The IRS model and the nomogram developed in the
present study may exhibit value in clinical practice for prognostic
prediction. Based on the IRS model and nomogram, it may be possible
to tailor therapeutic regimens to each specific patient, or they
may be useful for predicting/detecting early recurrence, and to
evaluate immune function in HCC to optimize the benefits of
monoclonal targeting therapies.
The present study has some limitations. First, the
cohorts from TCGA and ICGA are primarily from several local
populations, and thus may not be applicable to all ethnicities.
Second, the DEIGs in this analysis may not reveal the holistic
changes in the immune microenvironment in HCC. Third, the present
study focused primarily on overall survival of patients following
tumor resection, and disease-free survival was not assessed as this
information was not contained in the data-sets. Furthermore,
experimental validation of the prognostic signatures in HCC cell
lines and human tissues is required to validate their relevance and
improve our understanding of their respective roles, and will be
performed in future experiments.
In conclusion, a 5-gene model was constructed from
differentially expressed immune associated genes to evaluate the
IRS of patients for independent prognostic prediction. By combining
IRS with clinical tumor stage, a nomogram was constructed with
efficient predictive value for 1, 3 and 5 year OS for patients with
HCC. This nomogram may be used clinically for monitoring early
recurrence and prognostic prediction.
Supplementary Data
Funding
The present study was supported by the Education and
Scientific Research Project of Middle and Young Teachers in Fujian
Province (grant no. JAT170245).
Availability of data and materials
The datasets analyzed during the present study are
available from The Cancer Genome Atlas (portal.gdc.cancer.gov/) and International Cancer
Genome Consortium (icgc.org/) repository.
Authors' contributions
WL and CF designed the study and participated in
data collection. RH, ZC and JL analyzed and interpreted the data,
and wrote the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests
Acknowledgements
Not applicable.
References
|
1
|
Singal AG, Lampertico P and Nahon P:
Epidemiology and surveillance for hepatocellular carcinoma: New
trends. J Hepatol. 72:250–261. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer sta-tistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA-Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar
|
|
3
|
Chen L and Han X: Anti-PD-1/PD-L1 therapy
of human cancer: Past, present, and future. J Clin Invest.
125:3384–3391. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sun C, Mezzadra R and Schumacher TN:
Regulation and function of the PD-L1 checkpoint. Immunity.
48:434–452. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liu G, Rui W, Zheng H, Huang D, Yu F,
Zhang Y, Dong J, Zhao X and Lin X: CXCR2-modified CAR-T cells have
enhanced trafficking ability that improves treatment of
hepatocellular carcinoma. Eur J Immunol. Jan 24–2020.Epub ahead of
print. View Article : Google Scholar
|
|
6
|
Batra SA, Rathi P, Guo L, Courtney AN,
Fleurence J, Balzeau J, Shaik RS, Nguyen TP, Wu MF, Bulsara S, et
al: Glypican-3-specific CAR T cells co-expressing IL15 and IL21
have superior expansion and antitumor activity against
hepato-cellular carcinoma. Cancer Immunol Res. Jan 17–2020.Epub
ahead of print. View Article : Google Scholar
|
|
7
|
Jindal A, Thadi A and Shailubhai K:
Hepatocellular carcinoma: Etiology and current and future drugs. J
Clin Exp Hepatol. 9:221–232. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zucman-Rossi J, Villanueva A, Nault JC and
Llovet JM: Genetic landscape and biomarkers of hepatocellular
carcinoma. Gastroenterology. 149:1226–1239.e4. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cancer Genome Atlas Research Network:
Electronic address simplewheeler@bcm.edu; Cancer
Genome Atlas Research Network: Comprehensive and integrative
genomic characterization of hepatocellular carcinoma. Cell.
169:1327–1341.e23. 2017. View Article : Google Scholar
|
|
10
|
Li B, Cui Y, Diehn M and Li R: Development
and validation of an individualized immune prognostic signature in
early-stage nonsquamous non-small cell lung cancer. JAMA Oncol.
3:1529–1537. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen CH, Lu YS, Cheng AL, Huang CS, Kuo
WH, Wang MY, Chao M, Chen IC, Kuo CW, Lu TP and Lin CH: Disparity
in tumor immune microenvironment of breast cancer and prognostic
impact: Asian versus Western populations. Oncologist. 25:e16–e23.
2020. View Article : Google Scholar :
|
|
12
|
Ge P, Wang W, Li L, Zhang G, Gao Z, Tang
Z, Dang X and Wu Y: Profiles of immune cell infiltration and
immune-related genes in the tumor microenvironment of colorectal
cancer. Biomed Pharmacother. 118:1092282019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lin P, Guo YN, Shi L, Li XJ, Yang H, He Y,
Li Q, Dang YW, Wei KL and Chen G: Development of a prognostic index
based on an immunogenomic landscape analysis of papillary thyroid
cancer. Aging (Albany NY). 11:480–500. 2019. View Article : Google Scholar
|
|
14
|
Wang J, Li Y, Fu W, Zhang Y, Jiang J,
Zhang Y and Qi X: Prognostic nomogram based on immune scores for
breast cancer patients. Cancer Med. 8:5214–5222. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Foerster F, Hess M, Gerhold-Ay A,
Marquardt JU, Becker D, Galle PR, Schuppan D, Binder H and Bockamp
E: The immune contexture of hepatocellular carcinoma predicts
clinical outcome. Sci Rep. 8:53512018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zheng M and Tian Z: Liver-mediated
adaptive immune tolerance. Front Immunol. 10:25252019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lu LC, Hsu C, Shao YY, Chao Y, Yen CJ,
Shih IL, Hung YP, Chang CJ, Shen YC, Guo JC, et al: Differential
differential organ-specific tumor response to immune checkpoint
inhibitors in hepatocellular carcinoma. J Liver Cancer. 8:480–490.
2019. View Article : Google Scholar
|
|
18
|
Keenan BP, Fong L and Kelley RK:
Immunotherapy in hepatocel-lular carcinoma: The complex interface
between inflammation, fibrosis, and the immune response. J
Immunother Cancer. 7:2672019. View Article : Google Scholar
|
|
19
|
Charoentong P, Finotello F, Angelova M,
Mayer C, Efremova M, Rieder D, Hackl H and Trajanoski Z: Pan-cancer
immunoge-nomic analyses reveal genotype-immunophenotype
relationships and predictors of response to checkpoint blockade.
Cell Rep. 18:248–262. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Rooney MS, Shukla SA, Wu CJ, Getz G and
Hacohen N: Molecular and genetic properties of tumors associated
with local immune cytolytic activity. Cell. 160:48–61. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
International Cancer Genome Consortium;
Hudson TJ, Anderson W, Aretz A, Barker AD, Bell C, Bernabé RR, Bhan
MK, Calvo F, Eerola I, et al: International network of cancer
genome projects. Nature. 464:993–998. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tomczak K, Czerwinska P and Wiznerowicz M:
The cancer genome atlas (TCGA): An immeasurable source of
knowledge. Contemp Oncol (Pozn). 19:A68–A77. 2015.
|
|
23
|
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW,
Shi W and Smyth GK: limma powers differential expression analyses
for RNA-sequencing and microarray studies. Nucleic Acids Res.
43:e472015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hu J, Koh H, He L, Liu M, Blaser MJ and Li
H: A two-stage microbial association map-ping framework with
advanced FDR control. Microbiome. 6:1312018. View Article : Google Scholar
|
|
25
|
Yu G, Wang LG, Han Y and He QY:
clusterProfiler: An R package for comparing biological themes among
gene clusters. OMICS. 16:284–287. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kanehisa M: Post-genome Informatics.
Oxford University Press; 2000
|
|
27
|
Heagerty PJ: Compute time-dependent ROC
curve from censored survival data using Kaplan-Meier (KM) or
Nearest Neighbor Estimation (NNE) method of Heagerty, Lumley &
Pepe. Biometrics. 56:337–344. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Li B, Severson E, Pignon JC, Zhao H, Li T,
Novak J, Jiang P, Shen H, Aster JC, Rodig S, et al: Comprehensive
analyses of tumor immunity: Implications for cancer immunotherapy.
Genome Biol. 17:1742016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Li T, Fan J, Wang B, Traugh N, Chen Q, Liu
JS, Li B and Liu XS: TIMER: A web server for comprehensive analysis
of tumor-infiltrating immune cells. Cancer Res. 77:e108–e110. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Team RC: R: A language and environment for
statistical computing. R Foundation for Statistical Computing;
Vienna, Austria: 2012
|
|
31
|
Team RS: RStudio: Integrated Development
for R. RStudio, Inc; Boston, MA: 2015
|
|
32
|
A P, Xu X, Wang C, Yang J, Wang S, Dai J
and Ye L: EZH2 promotes DNA replication by stabilizing interaction
of POLδ and PCNA via methylation-mediated PCNA trimerization.
Epigenetics Chromatin. 11:442018. View Article : Google Scholar
|
|
33
|
Batool A, Jin C and Liu YX: Role of EZH2
in cell lineage determination and relative signaling pathways.
Front Biosci (Landmark Ed). 24:947–960. 2019. View Article : Google Scholar
|
|
34
|
Cheng T and Xu Y: Effects of enhancer of
zeste homolog 2 (EZH2) expression on brain glioma cell
proliferation and tumori-genesis. Med Sci Monit. 24:7249–7255.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mochizuki D, Misawa Y, Kawasaki H, Imai A,
Endo S, Mima M, Yamada S, Nakagawa T, Kanazawa T and Misawa K:
Aberrant epigenetic regulation in head and neck cancer due to
distinct EZH2 overexpression and DNA hypermethylation. Int J Mol
Sci. 19:pii: E3707. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Karlowee V, Amatya VJ, Takayasu T, Takano
M, Yonezawa U, Takeshima Y, Sugiyama K, Kurisu K and Yamasaki F:
Immunostaining of increased expression of enhancer of zeste homolog
2 (EZH2) in diffuse midline glioma H3K27M-mutant patients with poor
survival. Pathobiology. 86:152–161. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Makk E, Bálint L, Cifra J, Tornóczky T,
Oszter A, Tóth A, Kálmán E and Kovács K: Robust expression of EZH2
in endocervical neoplastic lesions. Virchows Arch. 475:95–104.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Romanchikova N and Trapencieris P:
Wedelolactone targets EZH2-mediated Histone H3K27 methylation in
mantle cell lymphoma. Anticancer Res. 39:4179–4184. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhou L, Wei E, Zhou B, Bi G, Gao L, Zhang
T, Huang J, Wei Y and Ge B: Anti-proliferative benefit of curcumol
on human bladder cancer cells via inactivating EZH2 effector.
Biomed Pharmacother. 104:798–805. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Böhm J, Muenzner JK, Caliskan A,
Ndreshkjana B, Erlenbach-Wünsch K, Merkel S, Croner R, Rau TT,
Geppert CI, Hartmann A, et al: Loss of enhancer of zeste homologue
2 (EZH2) at tumor invasion front is correlated with higher
aggressiveness in colorectal cancer cells. J Cancer Res Clin Oncol.
145:2227–2240. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Natsumeda M, Liu Y, Nakata S, Miyahara H,
Hanaford A, Ahsan S, Stearns D, Skuli N, Kahlert UD, Raabe EH, et
al: Inhibition of enhancer of zest homologue 2 is a potential
therapeutic target for high-MYC medulloblastoma. Neuropathology.
39:71–77. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Cozzi A, Rovelli E, Frizzale G, Campanella
A, Amendola M, Arosio P and Levi S: Oxidative stress and cell death
in cells expressing L-ferritin variants causing
neuroferritinopathy. Neurobiol Dis. 37:77–85. 2010. View Article : Google Scholar
|
|
43
|
Vanarsa K, Ye Y, Han J, Xie C, Mohan C and
Wu T: Inflammation associated anemia and ferritin as disease
markers in SLE. Arthritis Res Ther. 14:R1822012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kwiatek-Majkusiak J, Dickson DW, Tacik P,
Aoki N, Tomasiuk R, Koziorowski D and Friedman A: Relationships
between typical histopathological hallmarks and the ferritin in the
hippocampus from patients with Alzheimer's disease. Acta Neurobiol
Exp (Wars). 75:391–398. 2015.
|
|
45
|
Döring M, Cabanillas Stanchi KM, Feucht J,
Queudeville M, Teltschik HM, Lang P, Feuchtinger T, Handgretinger R
and Müller I: Ferritin as an early marker of graft rejection after
allogeneic hematopoietic stem cell transplantation in pediatric
patients. Ann Hematol. 95:311–323. 2016. View Article : Google Scholar
|
|
46
|
Ojha NK and Lole KS: Hepatitis E virus
ORF1 encoded macro domain protein interacts with light chain
subunit of human ferritin and inhibits its secretion. Mol Cell
Biochem. 417:75–85. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Yazar S, Franchina M, Craig JE, Burdon KP
and Mackey DA: Ferritin light chain gene mutation in a large
Australian family with hereditary hyperferritinemia-cataract
syndrome. Ophthalmic Genet. 38:171–174. 2017. View Article : Google Scholar
|
|
48
|
Chekhun VF, Lukyanova NY, Burlaka CA,
Bezdenezhnykh NA, Shpyleva SI, Tryndyak VP, Beland FA and Pogribny
IP: Iron metabolism disturbances in the MCF-7 human breast cancer
cells with acquired resistance to doxorubicin and cisplatin. Int J
Oncol. 43:1481–1486. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wu T, Li Y, Liu B, Zhang S, Wu L, Zhu X
and Chen Q: Expression of ferritin light chain (FTL) is elevated in
glioblastoma, and FTL silencing inhibits glioblastoma cell
proliferation via the GADD45/JNK pathway. PLoS One.
11:e01493612016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Khanna V, Karjodkar F, Robbins S, Behl M,
Arya S and Tripathi A: Estimation of serum ferritin level in
potentially malignant disorders, oral squamous cell carcinoma, and
treated cases of oral squamous cell carcinoma. J Cancer Res Ther.
13:550–555. 2017.PubMed/NCBI
|
|
51
|
Liu J, Li W and Zhao H: CFHR3 is a
potential novel biomarker for hepatocellular carcinoma. J Cell
Biochem. Nov 10–2019.Epub ahead of print.
|
|
52
|
Hellwage J, Jokiranta TS, Koistinen V,
Vaarala O, Meri S and Zipfel PF: Functional properties of
complement factor H-related proteins FHR-3 and FHR-4: Binding to
the C3d region of C3b and differential regulation by heparin. FEBS
Lett. 462:345–352. 1999. View Article : Google Scholar
|
|
53
|
Spencer KL, Hauser MA, Olson LM, Schmidt
S, Scott WK, Gallins P, Agarwal A, Postel EA, Pericak-Vance MA and
Haines JL: Deletion of CFHR3 and CFHR1 genes in age-related macular
degeneration. Hum Mol Genet. 17:971–977. 2008. View Article : Google Scholar
|
|
54
|
Pouw RB, Gómez Delgado I, López Lera A,
Rodríguez de Córdoba S, Wouters D, Kuijpers TW and Sánchez-Corral
P: High complement factor H-related (FHR)-3 levels are associated
with the atypical hemolytic-uremic syndrome-risk allele CFHR3*B.
Front Immunol. 9:8482018. View Article : Google Scholar
|
|
55
|
Belotti D, Capelli C, Resovi A, Introna M
and Taraboletti G: Thrombospondin-1 promotes mesenchymal stromal
cell functions via TGFβ and in cooperation with PDGF. Matrix Biol.
55:106–116. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Xing T, Wang Y, Ding WJ, Li YL, Hu XD,
Wang C, Ding A and Shen JL: Thrombospondin-1 production regulates
the inflammatory cytokine secretion in THP-1 cells through NF-κB
signaling pathway. Inflammation. 40:1606–1621. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Firlej V, Mathieu JR, Gilbert C, Lemonnier
L, Nakhlé J, Gallou-Kabani C, Guarmit B, Morin A, Prevarskaya N,
Delongchamps NB and Cabon F: Thrombospondin-1 triggers cell
migration and development of advanced prostate tumors. Cancer Res.
71:7649–7658. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Jayachandran A, Anaka M, Prithviraj P,
Hudson C, McKeown SJ, Lo PH, Vella LJ, Goding CR, Cebon J and
Behren A: Thrombospondin 1 promotes an aggressive phenotype through
epithelial-to-mesenchymal transition in human melanoma. Oncotarget.
5:5782–5797. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Ioachim E, Damala K, Tsanou E, Briasoulis
E, Papadiotis E, Mitselou A, Charhanti A, Doukas M, Lampri L and
Arvanitis DL: Thrombospondin-1 expression in breast cancer:
Prognostic significance and association with p53 alterations,
tumour angiogenesis and extracellular matrix components. Histol
Histopathol. 27:209–216. 2012.
|
|
60
|
Lin XD, Chen SQ, Qi YL, Zhu JW, Tang Y and
Lin JY: Overexpression of thrombospondin-1 in stromal
myofibroblasts is associated with tumor growth and nodal metastasis
in gastric carcinoma. J Surg Oncol. 106:94–100. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Horiguchi H, Yamagata S, Rong Qian Z,
Kagawa S and Sakashita N: Thrombospondin-1 is highly expressed in
desmo-plastic components of invasive ductal carcinoma of the breast
and associated with lymph node metastasis. J Med Invest. 60:91–96.
2013. View Article : Google Scholar
|
|
62
|
Kashihara H, Shimada M, Yoshikawa K,
Higashijima J, Tokunaga T, Nishi M, Takasu C and Ishikawa D:
Correlation between thrombospondin-1 expression in non-cancer
tissue and gastric carcinogenesis. Anticancer Res. 37:3547–3552.
2017.PubMed/NCBI
|
|
63
|
Pozo K and Bibb JA: The emerging role of
Cdk5 in cancer. Trends Cancer. 2:606–618. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Lopes JP and Agostinho P: Cdk5:
Multitasking between physiological and pathological conditions.
Prog Neurobiol. 94:49–63. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Liebl J, Weitensteiner SB, Vereb G, Takács
L, Fürst R, Vollmar AM and Zahler S: Cyclin-dependent kinase 5
regulates endothelial cell migration and angiogenesis. J Biol Chem.
285:35932–35943. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Shupp A, Casimiro MC and Pestell RG:
Biological functions of CDK5 and potential CDK5 targeted clinical
treatments. Oncotarget. 8:17373–17382. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Liang Q, Li L, Zhang J, Lei Y, Wang L, Liu
DX, Feng J, Hou P, Yao R, Zhang Y, et al: CDK5 is essential for
TGF-β1-induced epithelial-mesenchymal transition and breast cancer
progression. Sci Rep. 3:29322013. View Article : Google Scholar
|
|
68
|
Yushan R, Wenjie C, Suning H, Yiwu D,
Tengfei Z, Madushi WM, Feifei L, Changwen Z, Xin W, Roodrajeetsing
G, et al: Insights into the clinical value of cyclin-dependent
kinase 5 in glioma: A retrospective study. World J Surg Oncol.
13:2232015. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Zhang X, Zhong T, Dang Y, Li Z, Li P and
Chen G: Aberrant expression of CDK5 infers poor outcomes for
nasopharyngeal carcinoma patients. Int J Clin Exp Pathol.
8:8066–8074. 2015.PubMed/NCBI
|
|
70
|
Pan DH, Zhu ML, Lin XM, Lin XG, He RQ,
Ling YX, Su ST, Wickramaarachchi MM, Dang YW, Wei KL and Chen G:
Evaluation and clinical significance of cyclin-dependent kinase5
expression in cervical lesions: A clinical research study in
Guangxi, China. Eur J Med Res. 21:282016. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Wei K, Ye Z, Li Z, Dang Y, Chen X, Huang
N, Bao C, Gan T, Yang L and Chen G: An immunohistochemical study of
cyclin-dependent kinase 5 (CDK5) expression in non-small cell lung
cancer (NSCLC) and small cell lung cancer (SCLC): A possible
prognostic biomarker. World J Surg Oncol. 14:342016. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Mandl MM, Zhang S, Ulrich M, Schmoeckel E,
Mayr D, Vollmar AM and Liebl J: Inhibition of Cdk5 induces cell
death of tumor-initiating cells. Br J Cancer. 116:912–922. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
73
|
NavaneethaKrishnan S, Rosales JL and Lee
KY: Loss of Cdk5 in breast cancer cells promotes ROS-mediated cell
death through dysregulation of the mitochondrial permeability
transition pore. Oncogene. 37:1788–1804. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Ehrlich SM, Liebl J, Ardelt MA, Lehr T, De
Toni EN, Mayr D, Brandl L, Kirchner T, Zahler S, Gerbes AL and
Vollmar AM: Targeting cyclin dependent kinase 5 in hepatocellular
carcinoma-A novel therapeutic approach. J Hepatol. 63:102–113.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Chen QF, Li W, Wu PH, Shen LJ and Huang
ZL: Significance of tumor-infiltrating immunocytes for predicting
prognosis of hepatitis B virus-related hepatocellular carcinoma.
World J Gastroenterol. 25:5266–5282. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Lu J, Xu Y, Wu Y, Huang XY, Xie JW, Wang
JB, Lin JX, Li P, Zheng CH, Huang AM and Huang CM:
Tumor-infiltrating CD8+ T cells combined with tumor-associated
CD68+ macrophages predict postoperative prognosis and adjuvant
chemotherapy benefit in resected gastric cancer. BMC Cancer.
19:9202019. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Wang J, Li Z, Gao A, Wen Q and Sun Y: The
prognostic landscape of tumor-infiltrating immune cells in cervical
cancer. Biomed Pharmacother. 120:1094442019. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Kobayashi N, Hiraoka N, Yamagami W, Ojima
H, Kanai Y, Kosuge T, Nakajima A and Hirohashi S: FOXP3+ regulatory
T cells affect the development and progression of
hepatocarcino-genesis. Clin Cancer Res. 13:902–911. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Mathai AM, Kapadia MJ, Alexander J,
Kernochan LE, Swanson PE and Yeh MM: Role of Foxp3-positive
tumor-infiltrating lymphocytes in the histologic features and
clinical outcomes of hepatocellular carcinoma. Am J Surg Pathol.
36:980–986. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Brunner SM, Rubner C, Kesselring R, Martin
M, Griesshammer E, Ruemmele P, Stempfl T, Teufel A, Schlitt HJ and
Fichtner-Feigl S: Tumor-infiltrating, interleukin-33-producing
effector-memory CD8(+) T cells in resected hepatocellular carcinoma
prolong patient survival. Hepatology. 61:1957–1967. 2015.
View Article : Google Scholar : PubMed/NCBI
|