Introduction
Pancreatic cancer is known to be one of the most
severe malignant tumors in humans and is the fourth-leading cause
of cancer-related mortality in the USA (1). Due to the rapidly aging population,
much of which is due to aging baby boomers, it is predicted that
pancreatic cancer will be the second-leading cause of
cancer-related mortality among the elderly, particularly those
>65 years of age, by 2030 (2).
This global trend has continued, leading to >200,000 deaths due
to pancreatic cancer each year (3). Due to its local advancement or
multiple metastasis, approximately 80% of patients with pancreatic
cancer are diagnosed at an advanced stage where surgical resection
of the tumor cannot be performed (4), leading to a 5-year overall survival
(OS) rate of 6% (5). Moreover, the
median survival time is reportedly <2 years for surgically
treated patients (6).
Pancreatic cancer has not exhibited a significant
improvement in OS over the past 30 years and has maintained similar
mortality and incidence rates. The mortality rate has remained high
as several patients are diagnosed at an advanced and unresectable
stage, where current treatment procedures have limited therapeutic
efficacy (7). Resistance to
chemotherapy is another reason for the high mortality rate
(3,8). Gemcitabine (GEM) is a typical
chemotherapeutic drug used in the treatment of advanced-stage
pancreatic cancer based on randomized trials (9-11),
indicating an improvement in the 1-year survival rate when using
GEM compared to when using 5-fluorouracil (5-FU) (12). However, systemic chemotherapy for
patients with pancreatic cancer has limited effects on the OS due
not only to low response rates, but also to chemoresistant
abilities generated by unknown mechanisms underlying the mode of
action of GEM. On the other hand, nab-paclitaxel co-administered
with GEM, another standard chemotherapeutic regimen, has been shown
to improve OS and progression-free survival (PFS) compared to GEM
monotherapy, based on a randomized trial for advanced pancreatic
cancer (10). Currently, patients
with advanced disease have an abysmal prognosis; therefore,
effective screening methods and early diagnosis, along with the
development of novel therapeutics, are essential for a more
comprehensive management of the disease. Thus, the present study
aimed to identify novel molecules related to chemoresistance in
pancreatic cancer using patient-derived xenografts (PDXs). The
present study identified a molecule, human epididymis protein 4
(HE4), that was associated with a poor prognosis and
chemoresistance in pancreatic cancer.
In 1991, the HE4 gene was cloned from human
epididymis by Kirchhoff et al for the first time (13). As HE4 was identified in the
epithelium of the distal epididymis, it was considered to act as a
protease inhibitor during the process of sperm maturation (13,14).
From structural analysis, HE4 is a member of the
whey-acidic-protein (WAP) family consisting of 2 WAP-type
4-disulfide core (WFDC) domains (15,16).
HE4 has a molecular weight of approximately 25 kDa and is a
secretory glycosylated protein encoded by the WAP 4-disulfide core
domain 2 (WFDC2) gene (17). The
genomic location of HE4 is chromosome 20, which often
undergoes amplification and, as a result, has a high gene
expression level in a number of types of cancer (15). Recently, HE4 has attracted
attention as a biomarker in various types of neoplasia, such as
ovarian (18,19), endometrial (20,21),
lung (22-24), breast (25), gastric (26) and colorectal (27) cancers; its clinicopathological
significance, cellular function and mechanisms of action, however,
remain unknown. While some normal tissues and various malignant
tissues exhibit HE4 expression, low levels have been observed in
the epithelium of some normal tissues (28,29).
Recent studies have demonstrated that HE4 is
expressed in several pancreatic carcinomas (30-33)
and that the normal pancreas does not generally express HE4
(17,30). Although HE4 seems to be associated
with pancreatic cancer, the association between HE4 and resistance
to anticancer drugs or prognosis remains unclear. The present study
aimed to reveal the mechanisms underling chemoresistance or the
poor prognosis of pancreatic cancer, and to determine the roles of
HE4 expression in these mechanism in vitro and ex
vivo.
Materials and methods
Establishment of pancreatic cancer
PDXs
All experiments involving laboratory animals were
performed in accordance with the care and use guidelines and
approved by the Ethics Committee of the Kanagawa Cancer Center
Research Institute (approval no. 176).
The establishment of the PDX model has been
previously described by the authors (34). A total of 1,204 NSG mice were
obtained from the Jackson Laboratory. Briefly, fresh tumor tissues
excised from 36 patients with pancreatic cancer; 18 males and 18
females, aged 48-69 years, with stage I-II disease [for human
research, the study protocol was approved by the Ethics Committee
of the Showa University School of Medicine (Tokyo, Japan); approval
no. 2611; consent was not obtained from the individual patients;
however, the patients were notified of the details of the study
using an opt-out form and were given the right to refuse study
participation. This is a method widely used in Japan] were minced
into small sections. They were then subcutaneously implanted into
the dorsal upper part of the backs of 40 NSG mice (12 weeks old;
female, weighing 20-30 g), as previously described (35,36).
For the induction of anesthesia, all mice were exposed to 4%
isoflurane at a 400 ml/min airflow in a chamber. Anesthesia was
then maintained with 1-2% isoflurane at a 200 ml/min airflow. The
mice were euthanized by cervical dislocation prior to the excision
of the tumor tissues. The first 140 PDXs established through
implantation were labeled as generation 1 (G1). When the tumor
volume reached 1,000 mm3 in this group, the tumor was
once excised and re-implanted into other mice following the same
procedure and in total, 160 mice were used to re-implant the tumor
tissues in each passage. This passage process was repeated and PDXs
up to G7 were successfully generated. A total of 1,140 mice were
used to establish each generation of PDXs.
Characteristics of pancreatic cancer
PDXs
Immunohisto-chemistry (IHC) and gene analysis were
conducted to confirm whether PDXs retained the histological and
genetic characteristics of the original patient tissues even
following repeated passaging. For the methodology in this section,
the same procedures we used as described in a previous study by the
authors (34).
Designation of chemoresistance-related
molecules in the PDXs from pancreatic cancer
Anticancer drugs (GEM as monotherapy or GEM and
nab-paclitaxel as combination therapy) or saline as an untreated
control were intraperitoneally injected into the PDXs as described
in a previous study by the authors (34). In brief, chemotherapeutic drugs or
saline were administered to the PDX models by an intra-abdominal
injection on days 1, 4 and 7; no injection was performed on day 10.
The tumor volume was measured each week for both the chemotherapy
(treatment) and saline (non-treatment) groups. Each group included
32 PDXs.
Tumor tissues from PDXs of both the treatment and
non-treatment groups were implanted when the tumor volume surpassed
1,500 mm3 in the non-treatment group. Tissue DNA and RNA
were extracted and subjected to NGS by Illumina HiSeq 4000
system.
Transcriptome analysis
For the methodology for transcriptome analysis, the
same methods and procedures were used as previously described
(34). Paired-end reads were
mapped to all or any human RefSeq transcripts (hg38 coordinates)
and mouse RefSeq transcripts (mm 10 coordinates) by bowtie 1.1.2
(37), with one mismatch at most.
When the mapped reads belonged to both species or more than one
gene was found, they were removed. The primary 100 bp of every read
for samples with 150-bp read length were applied to mapping to
avoid bias from the difference in read length. Since reads mapped
to noncoding transcripts were discarded, the remaining reads were
suitable for estimating the overview of organic phenomenon of human
cancer cells and mouse stromal cells, consistent with strategies
that have been previously described (34,38).
Bioinformatics analysis
The TCGA database of the National Cancer Institute
has published a huge number of RNA sequencing data from pancreatic
adenocarcinoma patients. The database is available to all
researchers. These data were retrieved and used for Kaplan-Meier
analysis based on HE4 expression.
Cells and cell culture
Various cell lines were prepared, including 293
(permanent primary cell line), SK-N-AS (human neuroblastoma),
KATOIII (human gastric cancer), AsPC-1 (human pancreatic ductal
cell carcinoma), PANC-1 (human pancreatic ductal cell carcinoma),
SUIT-2 (human pancreatic ductal cell carcinoma), MIA PaCa-2 (human
pancreatic ductal cell carcinoma), IMR-32 (human neuroblastoma),
HCT116 (human colon cancer) and HeLa (human cervical epithelioid
carcinoma); in addition, 3 non-cancerous cell lines were prepared,
namely human umbilical vein endothelial cells (HUVECs), human renal
glomerular endothelial cells (HRGEC) and H6c7 (human pancreatic
duct epithelial cell line). The SK-N-AS, IMR-32 and HCT116 cell
lines were obtained from Chiba Cancer Center Research Institute.
The other tumor cell lines were obtained from the Department of
Cancer Immunotherapy at the Kanagawa Cancer Center. The HUVEC and
HRGEC cell lines were obtained from the Department of Anatomy at
Showa University School of Medicine. The H6c7 cell line was
purchased from Kerafast. The 293, KATOIII, AsPC-1, MIA PaCa-2,
HCT116 and HeLa cells were grown in Dulbecco's modified Eagle's
medium (Thermo Fisher Scientific, Inc.), and the PANC-1, SUIT-2,
SK-N-AS and IMR-32 cells were grown in Roswell Park Memorial
Institute medium (Thermo Fisher Scientific, Inc.). The HUVECs were
cultured in endothelial cell growth medium-2 (EGM-2; PromoCell),
while the HRGECs were cultured in endothelial cell medium
(ScienCell Research Laboratories, Inc.). Each medium was
supplemented with 10% heat-inactivated fetal bovine serum (FBS;
Cytiva), 100 µg/ml streptomycin and 100 U/ml penicillin. The
H6c7 cells were cultured in keratinocyte-SFM supplemented with
human recombinant epidermal growth factor (EGF), bovine pituitary
extract (Invitrogen; Thermo Fisher Scientific, Inc.) and 1X
antibiotic-antimycotic (Invitrogen; Thermo Fisher Scientific,
Inc.). Each cell line was cultured at 37°C in 5%
CO2.
Reverse transcription-quantitative PCR
(RT-qPCR)
HE4 expression levels were determined in each
cell line. After collecting cultured cells, total RNA was prepared
with an RNeasy Mini kit (Qiagen GmbH) and subsequently reverse
transcribed with Superscript IV VILO Master Mix (Invitrogen; Thermo
Fisher Scientific, Inc.) according to the manufacturers' protocol.
The cDNA was then amplified using the StepOnePlus Real-Time PCR
System (Applied Biosystems; Thermo Fisher Scientific, Inc.) with
TaqMan Fast Advanced Master Mix (Applied Biosystems; Thermo Fisher
Scientific, Inc.) to quantify the mRNA expression of HE4 and
ACTB. The optimal thermal cycling conditions for the master
mix were as follows: 40 cycles of a two-step PCR (95°C for 1 sec
and 60°C for 20 sec) after the initial enzyme activation (50°C for
2 min and 95°C for 2 min). The quantification cycle (Cq) values
were determined using StepOne Software v2.0 yielding amplification
plots. The ΔΔCq method was then used to calculate relative gene
expression, as previously described (39). The specific TaqMan probes were as
follows: HE4, Hs00197437_m1; ACTB, Hs01060665_g1
(Applied Biosystems; Thermo Fisher Scientific, Inc.).
Cell viability assay of tumor cell lines
treated with anticancer drugs
Cell viability assays of various malignant tumor
cell lines (SK-N-AS, KATOIII, AsPC-1, PANC-1, SUIT-2, MIA PaCa-2,
IMR-32, HCT116 and HeLa) treated with GEM were performed as
previously described (34). After
examining cell viability, endogenous HE4 gene expression
levels were measured in these cell lines by RT-qPCR. First, each
cell line was inoculated at 1×104 cells/well in a
96-well plate and cultured for 24 h GEM was then added at varying
concentrations (0-10,000 nM). Following a 72-h culture, the cell
viability under each condition was measured using MTT Reagent
(Thermo Fisher Scientific, Inc.), according to the manufacturer's
instructions. The relative cell number was then determined by
calculating the rate of change, where the cell number of untreated
cells (0 nm GFM) was set as 100%. For transient overexpression
experiments, an expression plasmid vector for HE4 (pCMV6-AC-HE4-GFP
tag plasmid, NM_006418) was obtained from OriGene Technologies,
Inc. and an empty vector (pCMV6-AC-GFP) was adopted for control
transfection. The 293 cells were seeded at 3×105
cells/well in 6-well plates for transfection. Following a 24-h
culture, transfection was performed using 6 µl FuGENE 6
(Promega Corporation) with 2 µg the expression plasmid for
GFP-tagged HE4 or with the empty plasmid, based on the
manufacturer's protocol. At 24 h following transfection, the cells
were suspended and seeded in a 96-well plate with or without GEM.
Following a 48-h culture, cell viability was measured as described
above.
Immunohistological analysis of pancreatic
cancer tissues
The present study comprised a successive cohort of
80 patients with histopathologically-confirmed pancreatic cancer
who had undergone surgical excision at the Showa University
Hospital), from January 1, 2008 to December 31, 2017. The patient
cohort of the present study is identical to that of a previous
study by the authors (34). The
study protocol was approved by the Ethics Committee of the Showa
University School of Medicine (approval no. 2611), and all study
procedures abided by the principles of the Declaration of Helsinki.
Consent was not obtained from the individual patients. However, the
patients were notified of the details of the study using an opt-out
form and were given the right to refuse study participation. This
is a method widely used in Japan. Patients had no history of
chemotherapy prior to surgical excision. For further stratification
to analyze the clinicopathological factors, invasive factors were
assessed according to the classification of pancreatic cancer by
the Japan Pancreas Society.
By using a Leica Bond system, HE4 protein expression
in patient tissues was evaluated immunohistologically. Briefly,
formalin-fixed, paraffin-embedded tissue sections were
deparaffinized and pretreated with heat-mediated antigen retrieval
solution with sodium citrate buffer for 20 min. The sections were
then incubated with a primary antibody against HE4 (cat. no.
ab200828; Abcam) for 15 min at 25±1°C. Bond™ Primary Antibody
Diluent (cat. no. AR9352; Leica Biosystems, Bannockburn, IL) was
used to dilute the antibody (1:1,000 dilution). HE4 detection was
carried out using a horseradish peroxidase-conjugated compact
polymer system (HRP-polymer secondary antibody; goat anti-rabbit
IgG H&L (HRP polymer); product code ab214880; pre-diluted;
Abcam). And DAB was applied as the chromogen and incubated for 5
min at 25±1°C. Counterstaining was performed with hematoxylin for 5
min at 25±1°C, and the sections were mounted for microscopic
observation.
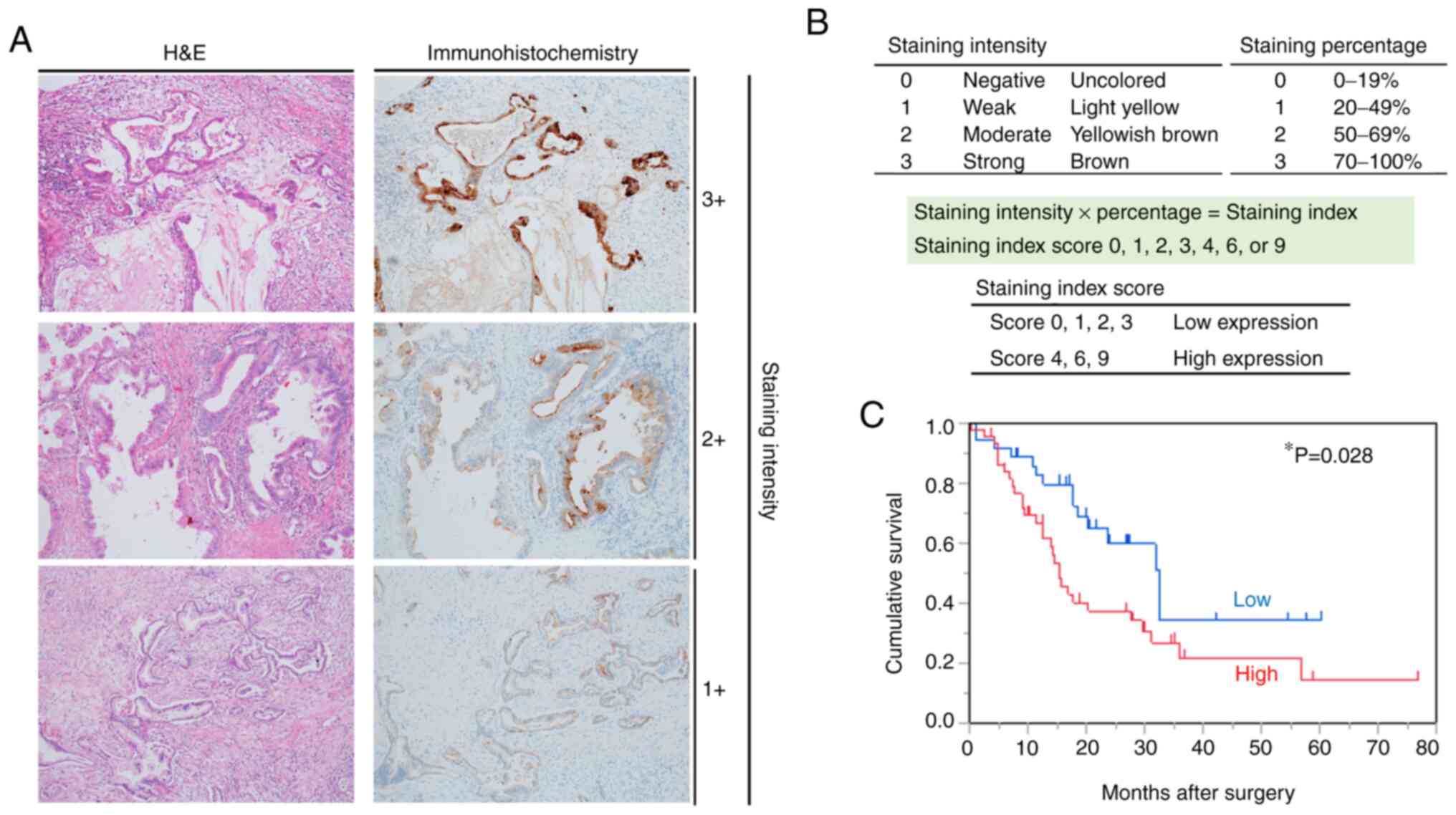
The immunostained tissue sections were assessed by
two pathologists who had no clinical information of the patients.
The degree of positiveness was evaluated by the staining intensity
and the percentage of positively stained cells. The criteria for
the staining intensity grade were as follows: 0, negative
(uncolored); 1, weak (light yellow); 2, moderate (yellowish brown);
and 3, strong (brown). Based on the relative number of stained
tumor cells, staining percentages were graded as follows: 0
(<19% positive tumor cells), 1 (20-49% positive tumor cells), 2
(50-69% positive tumor cells) and 3 (≥70% positive tumor cells).
HE4 expression was classified referring to the staining index
(scored as 0, 1, 2, 3, 4, 6, or 9). The staining index scores of
<3 (low HE4 expression) and >4 (high HE4 expression) were
regarded as the optimal cut-off values.
Statistical analysis
All statistical analyses were carried out using JMP
Pro 14.0 software (SAS Institute Inc.). HE4 gene expression
in 9 cell lines was statistically analyzed using one-way analysis
of variance (ANOVA) and subsequently by the Tukey-Kramer post-hoc
test. The difference in cell viability between the control 293
cells, which had been transfected with an empty vector, and the
HE4-expressing 293 cells, which had been transfected with the HE4
expression vector, at each concentration of GEM, was statistically
analyzed by two-way ANOVA with the Bonferroni post hoc test for
multiple comparisons. In addition, associations between the IHC
status of HE4 expression and various clinical and pathological
parameters were assessed using the Student's t-test or Fisher's
exact test. In this study, OS was defined as the interval time from
the first surgery to either patients' decease or last observation.
Kaplan-Meier analysis and log-rank tests were adopted to estimate
the difference in OS due to high or low HE4 expression level. Using
the Cox proportional hazards regression model, univariate and
multivariate analyses were performed. All statistical tests were
two-tailed, and a value of P<0.05 was considered to indicate a
statistically significant difference.
Results
Establishment of a PDX model from
pancreatic cancer
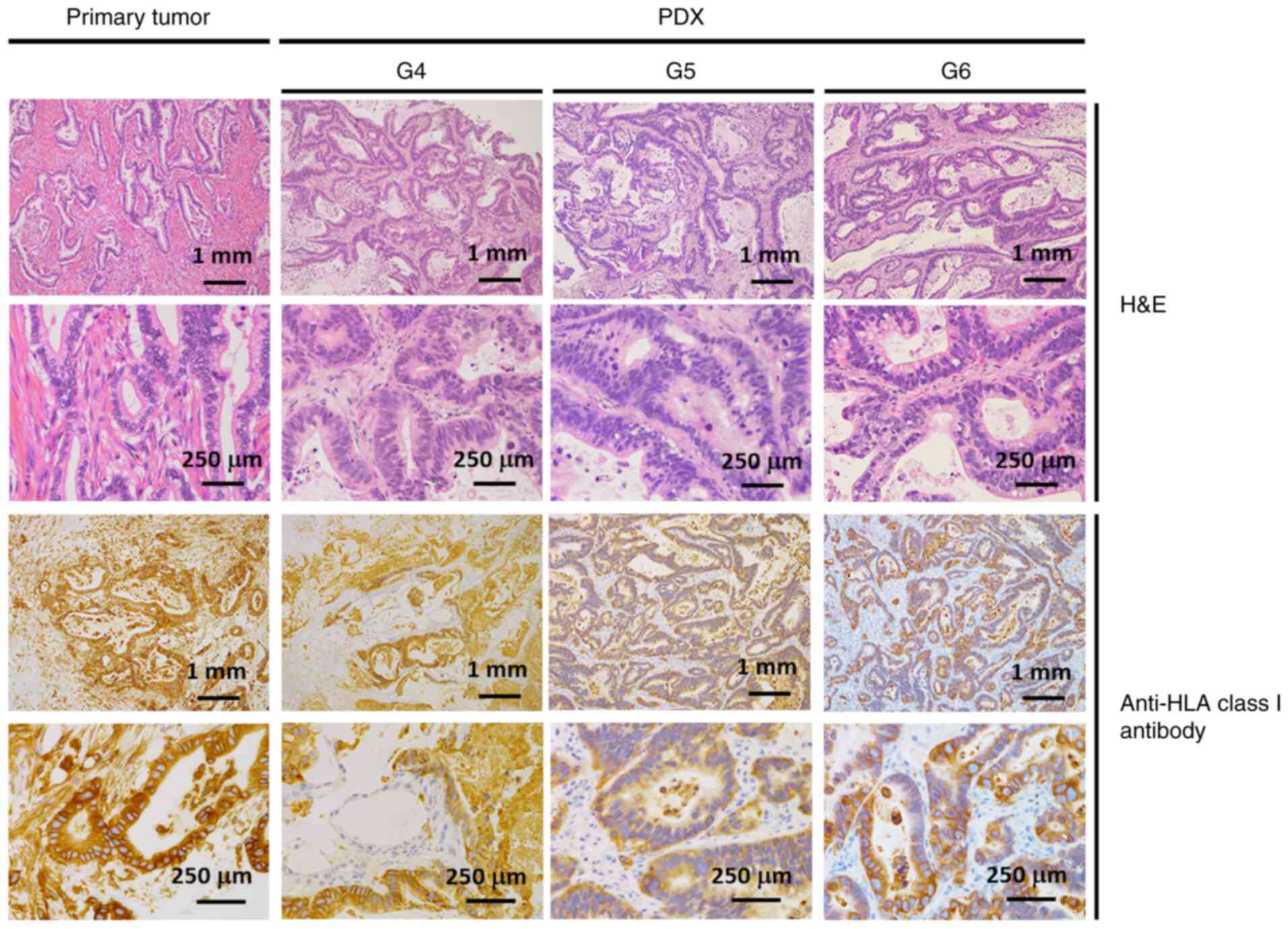
A total of 10 PDX lines of pancreatic cancer were
established. By histopathological observation, it was found that
the PDXs had identical histological characteristics to the patient
specimens, even following repeated PDX passaging procedures. In
addition, it was found that the expression of HLA class I molecules
in PDX specimens was maintained even after passaging (Fig. 1). Thus, the PDXs established in the
present study retained the pathological characteristics of the
original patient tissues. Furthermore, gene mutation
characteristics were investigated by DNA/RNA extraction and
high-throughput sequencing. In addition to the pathological
features, the tumor cells of PDXs retained the genetic
characteristics of the original pancreatic tissues from the
patients (data not shown).
Designation of a chemoresistance-related
molecule
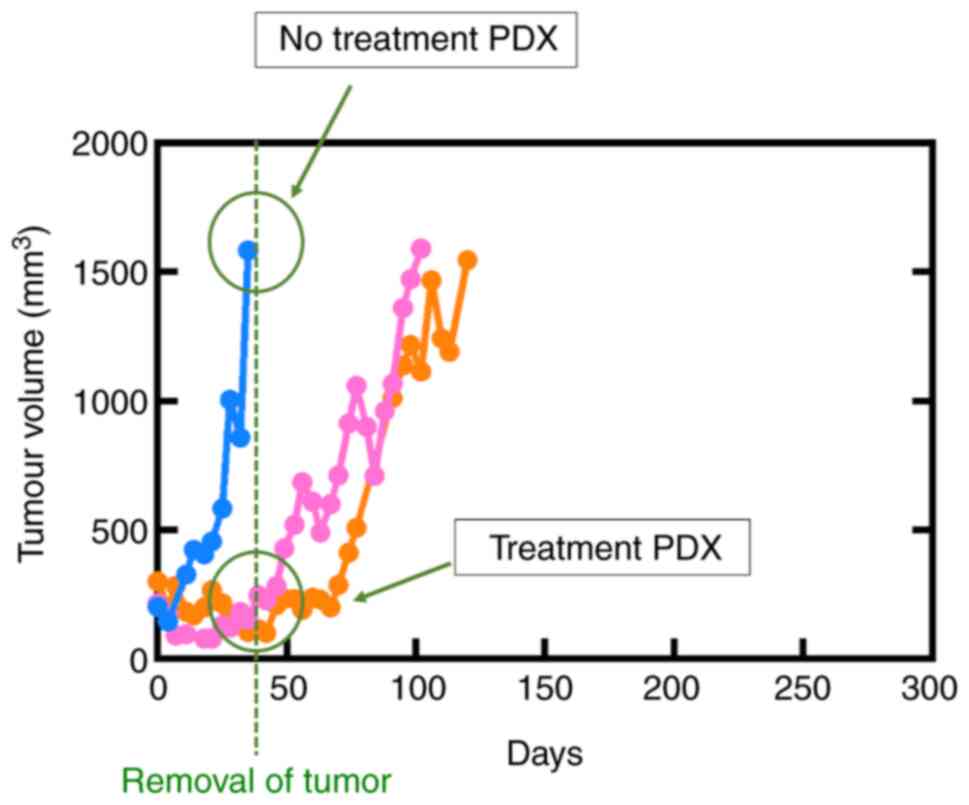
The anti-tumor effects of GEM monotherapy or GEM and
nab-paclitaxel combination therapy were examined using the PDX
model to identify a molecule related to chemoresistance, and tumor
growth was analyzed following antitumor treatment. The curve of the
tumor volume of a typical PDX is shown in Fig. 2.
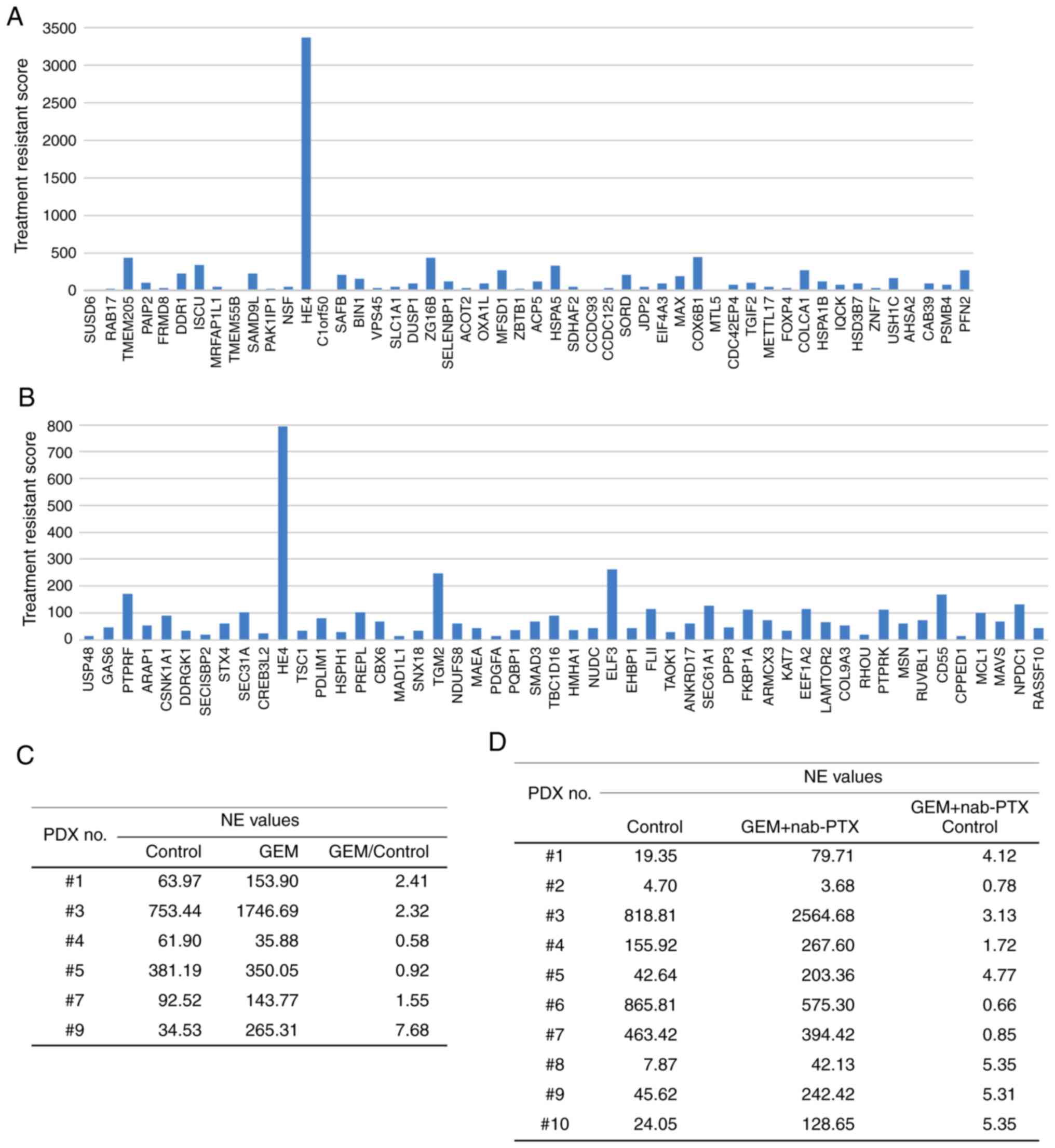
The mRNA expression level in the tumor tissues was
then assessed by NGS analysis. The ratio of the control to treated
PDXs was calculated by referring to the data for normalized
expression (NE) values. In total, 6 PDX lines were examined for GEM
monotherapy, as well as 10 PDX lines for GEM and nab-paclitaxel
combination therapy; genes with NE values >10 and NE ratios
(treated group to control group) >2 were selected (Fig. 3A and B). HE4 was identified
as having a robust expression in the treatment group. The ratio of
the NE values for HE4 expression (Fig. 3C and D) between the
chemotherapy-treated and untreated groups tended to be >1.0 for
some PDXs treated with GEM or GEM and nab-paclitaxel. The results
revealed that the mRNA expression level of HE4 increased
when PDXs were treated with anticancer drugs.
Analysis of pancreatic cancer prognosis
using the TCGA database
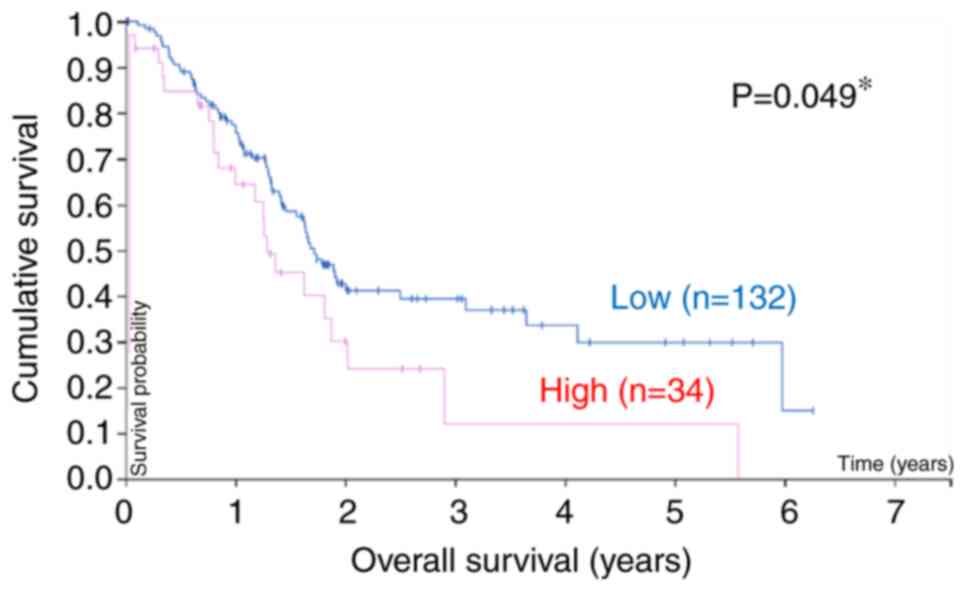
The association between HE4 expression and OS
in 166 pancreatic cancer samples from the TCGA database was
analyzed, and the association between the mRNA expression level of
HE4 and patient survival was also assessed (Fig. 4). As a result, it was found that
patients with a higher HE4 expression level exhibited lower
survival rates than those with a low HE4 expression level
(P=0.049).
In vitro confirmation of HE4
function
To investigate the specific role of HE4 in
chemoresistance, the gene expression levels of endogenous
HE4 were examined in various tumor cell lines (SK-N-AS,
KATOIII, AsPC-1, PANC-1, SUIT-2, MIA PaCa-2, IMR-32, HCT116 and
HeLa) and 2 non-cancerous cell lines (HUVECs and HRGECs) by
RT-qPCR. It was found that the endogenous HE4 levels
differed between the cell lines (Fig.
5A). As the HeLa cells exhibited the lowest HE4
expression levels, they were used as the controls. In addition, the
2 non-cancerous cell lines, HUVECs and HRGECs, also exhibited a
significantly low expression of HE4, similar to that in the
HeLa cells, and were also considered as controls. As a result,
HE4 expression was significantly higher in the SK-N-AS,
KATOIII and ASPC-1 cell lines than in the others (Table SI). Moreover, in the non-cancerous
pancreatic cell line, H6c7, the HE4 expression level was
relatively high compared to that in the HeLa cell line (Fig. S1). Subsequently, cell viability
assays were performed on these cell lines treated with various
concentrations of GEM (Fig. 5B). A
statistically significant difference in cell numbers was observed
among the 9 cell lines at the GEM concentrations of 100, 1,000 and
10,000 nM. It was found that the 3 cell lines with a relatively
high HE4 expression (SK-N-AS, KATOIII and ASPC-1) exhibited
higher cell survival rates than the 4 cell lines with a low
HE4 expression (HeLa, HCT116, IMR-32 and MIA PaCa-2) at GEM
concentrations of 1,000 and 10,000 nM (Table SII). As regards the pancreatic
cancer cell lines, the AsPC-1 cells, which exhibited a
significantly high expression of HE4, had higher viable cell
numbers than did the SUIT-2 and MIA PaCa-2 cells at GEM
concentrations of 1,000 and 10,000 nM (Fig. 5B). These results suggest that HE4
expression is partially associated with resistance to GEM.
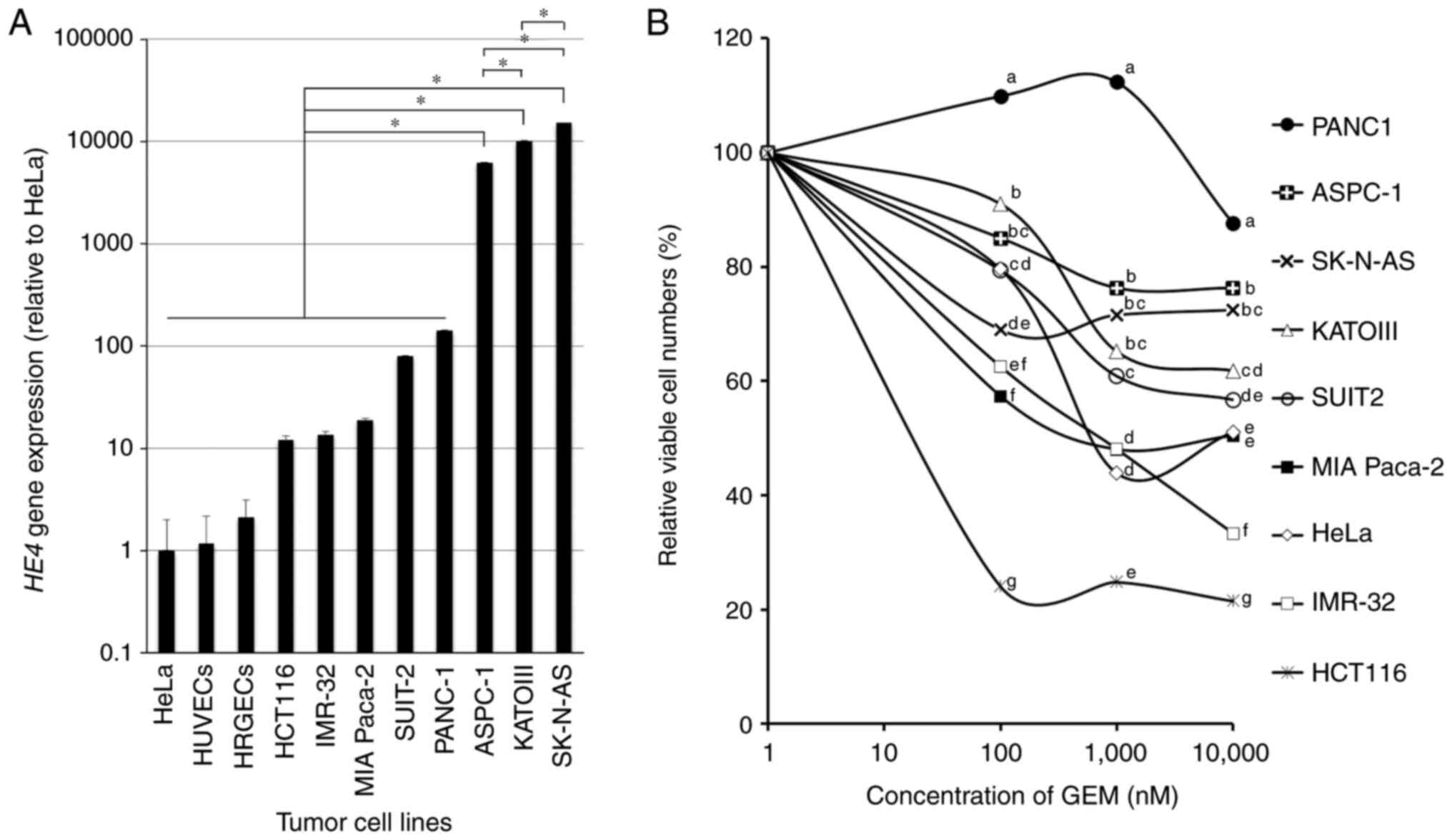 | Figure 5Expression of HE4 and cell viability
assays of cell lines. (A) The levels of HE4 gene expression
in 9 tumor cell lines (SK-N-AS, KATOIII, ASPC-1, PANC-1, SUIT-2,
MIA-Paca2, IMR-32, HCT116 and HeLa) and 2 non-cancerous cell lines
(HUVECs and HRGECs) measured by RT-qPCR. Endogenous HE4 expression
levels differed among cell lines. *P<0.05. (B) Cell
viability assays of tumor cell lines in response to GEM treatment.
When the concentration of GEM was increased, the relative viable
cell numbers tended to be higher in the cell lines in which
expression of endogenous HE4 was relatively higher. Cell lines with
different lowercase letters (a-g) indicate statistically
significant differences at each GEM concentration.
aP<0.05 vs. b-g; bP<0.05 vs. c-g;
cP<0.05 vs. d-g; dP<0.05 vs. e-g;
eP<0.05 vs. f and g; and fP<0.05 vs. g.
HE4, human epididymis protein 4; GEM, gemcitabine; HUVECs, human
umbilical vein endothelial cells; HRGECs, human renal glomerular
endothelial cells. |
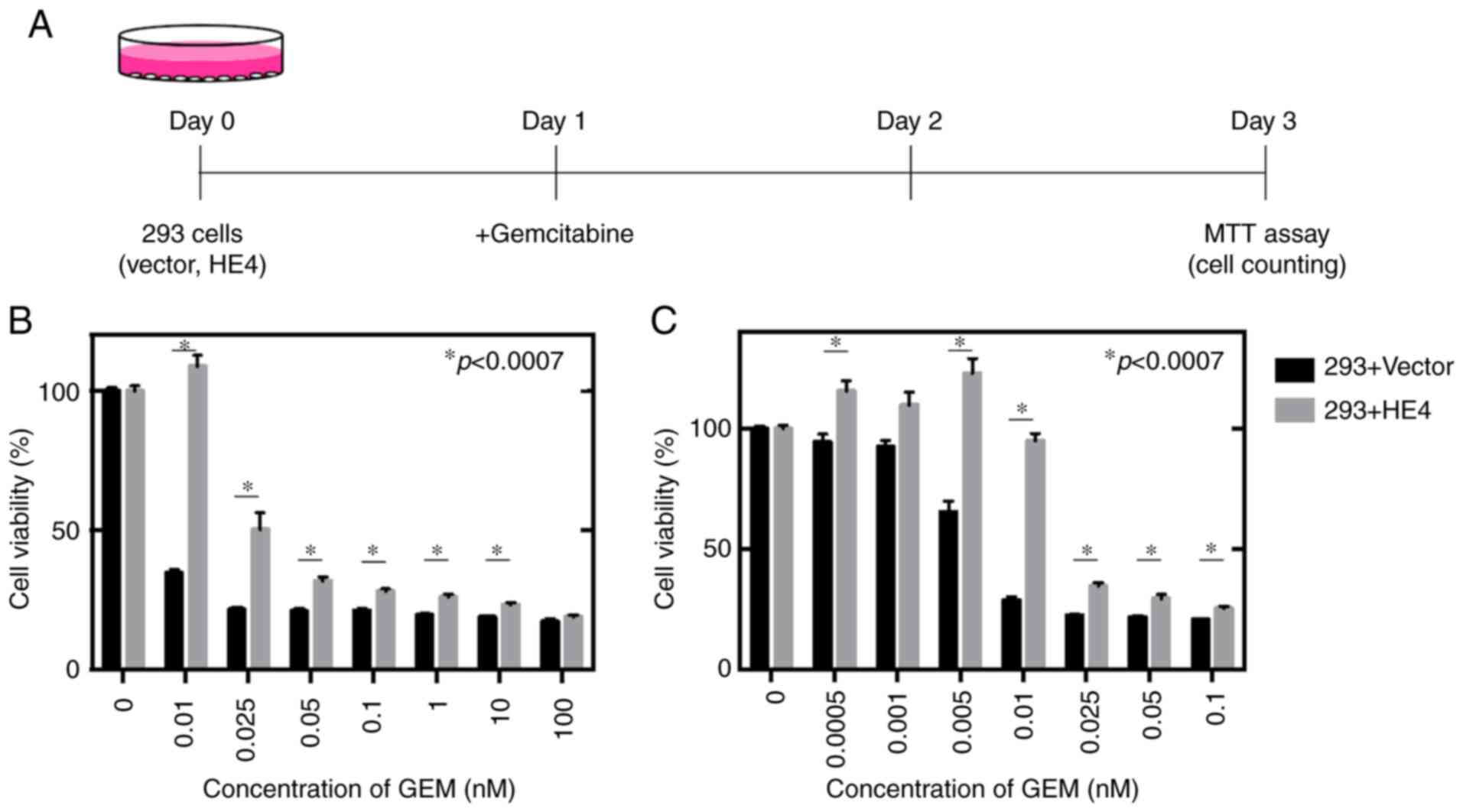
The 293 cells were prepared for the induction of
exogeneous HE4 expression, and an MTT cell viability assay for the
293 cells treated with GEM was conducted (Fig. 6A). With the increased GEM
concentration, the number of tumor cells decreased in the control
group; in the HE4-expressing cells, however, a partial decrease in
tumor cell growth was observed following GEM treatment. At each GEM
concentration, apart from those of 0.001 and 100 nM, the viability
of the HE4-expressing cells was significantly higher than that of
the controls (Fig. 6B and C),
suggesting that HE4 partially contributes to chemoresistance in
vitro.
Immunohistological and prognostic
analyses in patients with pancreatic cancer
To corroborate the discoveries on HE4 expression in
the current PDX model with that in clinical specimens, IHC was
performed and HE4-positive tumor cells were found (Fig. 7A). The samples were then divided
into 2 groups as follows: High HE4 expression [55.0% (44/80)] group
and low HE4 expression [45.0% (36/80)] group, as described in
Fig. 7B. No obvious associations
were found between the 2 groups in each category, including age
(P=0.46), sex (P=0.26), tumor location (head or body/tail,
P=0.059), histological type (adenocarcinoma or others, P=0.62), TNM
stage (IIA or IIB, P=0.999), lymphatic invasion (P=0.999), venous
invasion (P=0.50) and the presence of adjuvant chemotherapy
(P=0.82; Table I). The
associations between the expression level of HE4 and survival rate
were examined by Kaplan-Meier analysis and log-rank tests (Fig. 7C). From the results presented in
Fig. 7C, the higher HE4 expression
was, the poorer the survival rate (P=0.028) in the current cohort
of 80 patients with pancreatic cancer. In total, 3 prognostic
parameters were identified from the univariate analysis of OS: Sex
(P=0.033), adjuvant chemotherapy (P=0.037) and HE4 expression
(P=0.031), while the multivariate analysis revealed that sex
(P=0.045), adjuvant chemotherapy (P=0.020) and HE4 expression
(P=0.029) were independent factors of a poor prognosis (Table II). The data for age in Table I and sex in Table II are similar to those of a
previous study by the authors (34) as the same patient cohort was used
in both studies.
 | Table IAssociation between HE4 expression
and clinicopathological features in 80 cases of pancreatic
cancer. |
Table I
Association between HE4 expression
and clinicopathological features in 80 cases of pancreatic
cancer.
|
Characreristics | HE4 expression
| P-value |
|---|
Low
n=36 | High
n=44 |
|---|
| Age, years (mean ±
SD) | 72.00±9.38 | 71.75±12.49 | 0.46a |
| Sex | | | 0.26b |
| Male | 15 | 25 | |
| Female | 21 | 19 | |
| Tumor location | | | 0.059b |
| Head | 19 | 33 | |
| Body/tail | 17 | 11 | |
| Histological
type | | | 0.62b |
|
Adenocarcinoma | 35 | 41 | |
| Others | 1 | 3 | |
| TNM (UICC 7th) | | | 0.999b |
| IIA | 9 | 11 | |
| IIB | 27 | 33 | |
| Lymphatic
invasion | | | 0.999b |
| ly0, ly1 | 14 | 17 | |
| ly2, ly3 | 22 | 27 | |
| Venous
invasion | | | 0.50b |
| v0, v1 | 3 | 6 | |
| v2, v3 | 33 | 38 | |
| Adjuvant
chemotherapy | | | 0.82b |
| Absent | 23 | 26 | |
| Present | 13 | 18 | |
| Table IIUnivariate and multivariate analyses
of prognostic factor for overall survival in 80 pancreatic cancer
patients. |
Table II
Univariate and multivariate analyses
of prognostic factor for overall survival in 80 pancreatic cancer
patients.
| Clinicopathological
factors | Univariate analysis
| Multivariate
analysis
|
|---|
| HR | 95% CI | P-valuea | HR | 95% CI | P-valuea |
|---|
| Age, years (≤71 vs.
>71) | 1.1 | 0.60-2.09 | 0.76 | - | - | - |
| Sex (Male vs.
female) | 0.52 | 0.28–0.95 | 0.033b | 0.54 | 0.29–0.97 | 0.045b |
| TNM stage UICC 7th
(IIA vs. IIB) | 0.55 | 0.25–1.12 | 0.12 | - | - | - |
| Tumor location
(Body/tail vs. head) | 1.68 | 0.90–3.31 | 0.12 | - | - | - |
| Histological type
(Adeno vs. others) | 0.6 | 0.10–1.20 | 0.48 | - | - | - |
| Lymphatic invasion
(ly0, ly1 vs. ly2, ly3) | 1.4 | 0.77–2.62 | 0.28 | - | - | - |
| Venous invasion
(v0, v1 vs. v2, v3) | 1.13 | 0.51–3.00 | 0.78 | - | - | - |
| Adjuvant
chemotherapy (Absent vs. present) | 0.49 | 0.25–0.93 | 0.037b | 0.45 | 0.22–0.86 | 0.020b |
| HE4 (Low vs.
high) | 1.98 | 1.08–3.80 | 0.031b | 2.01 | 1.09–3.86 | 0.029b |
Discussion
The distinctive features of pancreatic cancer, known
as one of the lethal malignancies, are a delay in making the
diagnosis, the metastatic progression of cancer in the early stages
and chemoresistance. Thus, it is imperative to discover novel and
effective prognostic markers as well as targets for anticancer
therapy. In a previous study by the authors, it was found that HE4
expression increased in chemotherapy-treated PDXs compared with
that in untreated PDXs, suggesting that chemotherapy treatment may
have induced the expression of HE4 or that the increased expression
of HE4 may be involved in the mechanisms of chemoresistance. The
present study also investigated HE4 gene expression levels
and cell viability in various tumor cell lines, including
pancreatic cancer cells. From the results, the cell lines with a
relatively higher expression of HE4 tended to have a higher cell
viability than did those with a lower HE4 expression when the GEM
concentration was increased. Of note, the viability of
HE4-overexpressing 293 cells largely increased in response to GEM
treatment compared to that in non-treated cells. Furthermore, it
was demonstrated that a high HE4 expression was an independent
prognostic factor, which is in association with the survival rate
of pancreatic cancer. The current discoveries for pancreatic cancer
were supported by an analysis of TCGA data that highlighted the use
of HE4 expression as a prognostic factor.
The present study generated numerous PDX models;
herein, pancreatic cancer PDXs were established in order to
understand the mechanisms of chemoresistance and develop a novel
biomarker. Several types of tumor cell lines and mouse tumor models
have been applied in a number of experiments to determine the
effects and potential toxicities of anticancer agents in cancer
patients (35,40). The results of this research,
however, do not always represent the data from human clinical
trials (41). Furthermore, mouse
studies are not always translatable to human cases (42,43).
As a result, substantial mouse models that are applicable to the
pathology in human clinical trials are required.
In recent years, drug screening using the latest
animal models, including PDXs that are produced by transplanting
tiny pieces of human tumors into mice, have been drawing attention;
with these techniques, the environment inside the human body has
been mimicked in host sites (44).
As the noble PDX methods have been established by grafting freshly
resected samples directly into immunodeficient mice, relevant and
effective in vivo models for human tumors have been
developed (45). Thus, PDX models
that retained the molecular signatures and morphology of the
resected original tumors were established for the speedy screening
of latent therapy (46,47). In the present study, PDXs that were
generated from pancreatic cancer were established and it was proven
that they preserved the pathological features of human tumor
tissues. It was confirmed that the PDXs maintained the specific
histological features of their donor tumors, which were stable
throughout the repeated passaging. The amount of sample tissue
collected from pancreatic cancer is limited due to the condition of
the disease; PDX models are, therefore, considered ideal animal
models to investigate the pathology of pancreatic cancer.
PDX experiments revealed that the mRNA expression of
HE4 increased in the chemotherapy-treated group compared
with that in the untreated group, indicating that the elevation of
mRNA expression of HE4 elicited the chemoresistance.
Nevertheless, variations in mRNA expression do not necessarily
reflect an alteration in protein expression, as it may be affected
by a variety of post-transcriptional regulations (48-50);
therefore, mRNA levels do not necessarily reflect protein
abundance. The proteomics of rectal and colon cancers formerly
qualified in the TCGA database were analyzed, and it was revealed
that the difference in protein expression could not be estimated
from the quantity of mRNA transcripts between these cancers
(51). To confirm the concordance
between mRNA and protein levels of HE4, we examined whether there
is a relationship between HE4 protein and clinicopathological
factors by evaluating HE4 expression in 80 pancreatic cancer
patient tissues. As a result, it was regarded that the increased
expression level of HE4 as a prognostic factor that caused poor
survival in patients with pancreatic cancer.
A better understanding of the association between
HE4 expression and a poor prognosis is provided by reviews of the
literature in this field; the cellular and molecular mechanisms may
be proven by the role of HE4 in the progression of ovarian cancer
(52,53). Recent studies have inferred that
HE4 may play a pivotal role in the occurrence and development of
tumors. They provide sufficient evidence that HE4, when
overexpressed in cancer cells localized in the ovary or
endometrium, is capable of improving cell proliferation, adhesion
and invasion (54-56). There are a few reports on the
functions of HE4 in pancreatic cancer. Lu et al demonstrated
that extracellular recombinant HE4 protein purified from human
cells was able to enhance the proliferation of pancreatic cancer
cell lines (33). They also
observed that extracellular HE4 increased DNA synthesis and
modulated the expression of cell cycle regulators, such as p21 and
PCNA. Therefore, it is possible that HE4 plays an important role in
the progression of pancreatic cancer and poor prognosis.
The association between HE4 and resistance to
anticancer drugs has been elucidated in studies on ovarian cancer.
For instance, Lee et al (57) found that HE4 enhanced drug
resistance against cisplatin and paclitaxel. Moreover, Moore et
al (58) demonstrated that
HE4, when overexpressed in SKOV-3 clones, was not so sensitive to
cisplatin and paclitaxel compared to controls in vitro.
These studies revealed that the localization of HE4 expression is
related to the active state of growth factors, such as EFG and
VEGF, which induce nuclear translocation. They also indicated that
insulin is associated with HE4 local ization; insulin does not
stimulate nuclear translocation but nucleolar translocation. From
these findings, it was inferred that EGF, VEGF, insulin and their
receptors are responsible for ovarian tumor progression and
chemoresistance (59-61). An OVCAD study assessed the
association between platinum response and HE4 concentration in
plasma and ascites and found that HE4 levels were significantly
higher in the subgroup of platinum-non-responder patients than in
that of platinum-sensitive patients (62). In addition, Ribeiro et al
(63) reported that HE4 conferred
resistance to the anticancer drugs, cisplatin and paclitaxel; HE4
overexpression promoted chemoresistance to cisplatin and
paclitaxel, which was partially reversed by the downregulation of
HE4. It has been indicated that multiple factors can facilitate
HE4-mediated chemoresistance, related to the deregulation of MAPK
signaling, which induces apoptosis, as well as alterations in
tubulin levels or stability (63).
Wang et al (64)
demonstrated that HE4 can attenuate apoptosis induced by
carboplatin by reducing the mitochondrial Bax/Bcl-2 ratio; HE4
markedly increased Bcl-2 expression, while inhibiting Bax
expression (64). Moreover,
Angioli et al (65)
proposed that evaluating the serum values of HE4 concentration may
aid in the prediction of the response to chemotherapy in epithelial
ovarian cancer. The present study demonstrated that HE4 contributed
to GEM chemoresistance based on cell viability assays of several
tumor cell lines. To the best of our knowledge, there are no
previous reports available on the role of HE4 in GEM resistance.
Based on the PDX experiment, it is possible that HE4 is also
involved in resistance to nab-paclitaxel. As nab-paclitaxel is a
nanoparticle albumin-bound form of paclitaxel, the findings of the
present study may be similar to those of previous studies that
evaluated paclitaxel resistance in ovarian cancer patients.
Although further investigations are required to determine whether
these results are applicable to pancreatic cancer, the data support
a role for HE4 in multidrug resistance.
Previous studies have demonstrated that HE4 is
upregulated in pancreatic cancer cell lines and tissues (30,31).
Moreover, Huang et al (32)
demonstrated that HE4 mRNA and protein expression increased in
pancreatic adenocarcinoma tissues and that the level of serum HE4
was elevated in patients with pancreatic adenocarcinoma. However,
to the best of our knowledge, no studies to date have reported the
involvement of HE4 in the poor prognosis and GEM resistance in
pancreatic cancer. The present study seems to be the first to
demonstrate that HE4 is associated with a poor prognosis and GEM
resistance in pancreatic cancer, thereby highlighting that HE4 may
be a candidate biomarker to predict prognosis and
chemoresistance.
Multivariate analysis indicated that high expression
levels of HE4 are a substantive prognostic factor that forecast a
poorer outcome. In addition to HE4 expression, the lack of adjuvant
chemotherapy and being male were statistically significant poor
prognostic factors. An effect of sex on pancreatic cancer was
demonstrated in the present study, although there is little
established evidence. With respect to the direct prognosis of
pancreatic cancer, several studies have demonstrated significant
differences in the sub-analysis of larger studies. Although the
studies had patient heterogeneity and included not only stage IV
(66-68), but all stages (69-72),
the male sex exhibited a poor prognosis with a significantly
reduced OS. Another study demonstrated that post-operative male
patients exhibited a reduction in disease-specific survival
(6). Liu et al (73) reported that it is more likely to
accidentally identify distant metastases in male patients with
resectable pancreatic cancer. The cause of the poor prognosis for
males has not yet been clarified. It is conceivable that females
have fewer comorbidities than males do at the same ages. Moreover,
considering that pancreatic cancer is often unresectable, there is
a possibility that sex differences may exist in the effectiveness
of chemotherapy. Hohla et al (74) reported that despite a lack of
statistical significance, OS and PFS tended to be better for
females than for males, and they demonstrated that women had better
response rates with significant differences in the FOLFIRINOX
therapy group. Women also tended to have a better prognosis after
GEM chemotherapy (75). Thus,
compared with females, males reportedly have a poorer prognosis in
pancreatic cancer, corroborating the findings of the present study.
Although serum HE4 sensitivity exhibits a sex effect, the
association with prognosis is unknown and is a topic for future
research.
The present study had certain limitations. First,
the present study could not examine the association between HE4
expression and chemotherapy in cancer patients. In the present
study, all patients did not receive chemotherapy prior to surgery,
since neoadjuvant chemotherapy has not yet been permitted in Japan.
Nevertheless, it was considered advantageous to include some
patients who had received neoadjuvant chemotherapy prior to
surgery. Second, the present study was not able to conduct
additional PDX experiments to confirm the involvement of HE4 in
chemoresistance; nonetheless, endogenous HE4 gene expression
was measured in several cell lines by RT-qPCR. Third, the absence
of western blot analysis data is another limitation. Fourth,
although cell viability assays of various cell lines were
conducted, including HUVECs and HRGECs, in response to GEM,
inherent mutations in these cell lines may be involved in
resistance to GEM. To overcome this limitation, it is necessary to
further examine the association between gene mutations in each cell
line and GEM resistance. In in vitro assays using cell
lines, HE4 gene expression in the PANC-1 cell line was
statistically significantly lower than that in the SK-N-AS, KATOIII
and ASPC-1 cell lines (Table SI).
However, following treatment with GEM, regardless of the
concentration, the viable cell number of the PANC-1 cell line was
significantly higher than that of other cell lines, including
ASPC-1, KATOIII and SK-N-AS. Due to these inconsistent results
regarding HE4 expression and GEM resistance, PANC-1 cells may
possess a different mechanism of GEM resistance. Moreover, HE4 was
highly expressed in the normal pancreatic duct cell line (H6c7).
Hence, although the present study demonstrated that HE4 expression
may be applied as a predictive marker of a poor prognosis, the
results for H6c7 cells suggested that HE4 expression was not
cancer-specific, and thus, cannot serve as a diagnostic marker for
pancreatic cancer. The regulatory mechanisms associated with a high
or low HE4 expression in this normal pancreatic cell line, and in
pancreatic cancer cell lines remain unclear, and will need to be
clarified in future investigations.
Taken together, the findings of the present study
demonstrated that HE4 induced chemoresistance. As HE4 expression
was associated with a poor prognosis and is a promising novel
prognostic marker for pancreatic cancer, HE4 as a potential
therapeutic target for pancreatic cancer is hereby proposed.
However, further studies evaluating the clinical applicability of
HE4 in the prognosis and treatment of pancreatic cancer are
essential.
Supplementary Data
Acknowledgments
Not applicable.
Funding
The present study was supported by research funds
from Noile-Immune Biotech Inc.
Availability of data and materials
The datasets used and/or analyzed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
ROh was involved in the investigative aspects of
the study, and in the methodology, validation, visualization and
writing of the original draft. EY was involved in data curation,
formal analysis, methodology, project administration and in
providing resources. SI and DK were involved in formal analysis.
YK, KH, AH, TI, YH and HA provided resources and analyzed the
general data and patient indications, as well as in the study
methodology. MS, MW, RO and KA were involved in the investigative
aspects of the study, as well as in the study methodology. JT and
KY provided resources and were involved in study methodology and
project administration. TS was involved in the study methodology.
TA and MM provided resources and were involved in study methodology
and project administration. TN, NO and MT were involved in the
investigative aspects of the study, as well as in the study
methodology. SK and TT were involved in study supervision,
methodology, project administration and reviewed and revised the
manuscript. SW was involved in the study conceptualization,
methodology, project administration, supervision and validation, as
well as in the writing, reviewing and editing of the manuscript.
All authors read and approved the final manuscript.
Ethics approval and consent to
participate
For human research, the study protocol was approved
by the Ethics Committee of the Showa University School of Medicine
(Tokyo, Japan; approval no. 2611), and all study procedures adhered
to the principles of the Declaration of Helsinki. Consent was not
obtained from the individual patients. However, the patients were
notified of the details of the study using an opt-out form and were
given the right to refuse study participation. This is a method
widely used in Japan. For animal research, all experiments
involving laboratory animals were performed in accordance with the
care and use guidelines of the Kanagawa Cancer Center Research
Institute. All protocols were approved by the ethics committee of
the Kanagawa Cancer Center Research Institute (approval no.
176).
Patient consent for publication
Not applicable.
Competing interests
The authors declare no competing interest.
Abbreviations:
|
HE4
|
human epididymis protein 4
|
|
PDX
|
patient-derived xenograft
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rahib L, Smith BD, Aizenberg R, Rosenzweig
AB, Fleshman JM and Matrisian LM: Projecting cancer incidence and
deaths to 2030: The unexpected burden of thyroid, liver, and
pancreas cancers in the United States. Cancer Res. 74:2913–2921.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kamisawa T, Wood LD, Itoi T and Takaori K:
Pancreatic cancer. Lancet. 388:73–85. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lefebvre AC, Maurel J, Boutreux S, Bouvier
V, Reimund JM, Launoy G and Arsene D: Pancreatic cancer: Incidence
treatment and survival trends-1175 cases in Calvados (France) from
1978 to 2002. Gastroenterol Clin Biol. 33:1045–1051. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sant M, Allemani C, Santaquilani M, Knijn
A, Marchesi F and Capocaccia R; EUROCARE Working Group: EUROCARE-4:
Survival of cancer patients diagnosed in 1995-1999 Results and
commentary. Eur J Cancer. 45:931–991. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Li HB, Zhou J and Zhao FQ: A prognostic
nomogram for disease-specific survival in patients with pancreatic
ductal adenocarcinoma of the head of the pancreas following
pancreatic-coduodenectomy. Med Sci Monit. 24:6313–6321. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ahrendt SA and Pitt HA: Surgical
management of pancreatic cancer. Oncology (Williston Park).
16:725–734. 2002.
|
|
8
|
Cecconi D, Palmieri M and Donadelli M:
Proteomics in pancreatic cancer research. Proteomics. 11:816–828.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Conroy T, Desseigne F, Ychou M, Bouché O,
Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de
la Fouchardière C, et al: FOLFIRINOX versus gemcitabine for
metastatic pancreatic cancer. N Engl J Med. 364:1817–1825. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Von Hoff DD, Ervin T, Arena FP, Chiorean
EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, et
al: Increased survival in pancreatic cancer with nab-paclitaxel
plus gemcitabine. N Engl J Med. 369:1691–1703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Wang Gillam A, Li CP, Bodoky G, Dean A,
Shan YS, Jameson G, Macarulla T, Lee KH, Cunningham D, Blanc JF, et
al: Nanoliposomal irinotecan with fluorouracil and folinic acid in
metastatic pancreatic cancer after previous gemcitabine based
therapy (NAPOLI-1): A global, randomised, open-label, phase 3
trial. Lancet. 387:545–557. 2016. View Article : Google Scholar
|
|
12
|
Burris HA III, Moore MJ, Andersen J, Green
MR, Rothenberg ML, Modiano MR, Cripps MC, Portenoy RK, Storniolo
AM, Tarassoff P, et al: Improvements in survival and clinical
benefit with gemcitabine as first-line therapy for patients with
advanced pancreas cancer: A randomized trial. J Clin Oncol.
15:2403–2413. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kirchhoff C, Habben I, Ivell R and Krull
N: A major human epididymis-specific cDNA encodes a protein with
sequence homology to extracellular proteinase inhibitors. Biol
Reprod. 45:350–357. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kirchhoff C: Molecular characterization of
epididymal proteins. Rev Reprod. 3:86–95. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Clauss A, Lilja H and Lundwall A: A locus
on human chromosome 20 contains several genes expressing protease
inhibitor domains with homology to whey acidic protein. Biochem J.
368:233–242. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bingle CD: Towards defining the complement
of mammalian WFDC-domain-containing proteins. Biochem Soc Trans.
39:1393–1397. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Drapkin R, von Horsten HH, Lin Y, Mok SC,
Crum CP, Welch WR and Hecht JL: Human epididymis protein 4 (HE4) is
a secreted glycoprotein that is overexpressed by serous and
endometrioid ovarian carcinomas. Cancer Res. 65:2162–2169. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hellström I, Raycraft J, Hayden-Ledbetter
M, Ledbetter JA, Schummer M, McIntosh M, Drescher C, Urban N and
Hellström KE: The HE4 (WFDC2) protein is a biomarker for ovarian
carcinoma. Cancer Res. 63:3695–3700. 2003.PubMed/NCBI
|
|
19
|
Trudel D, Têtu B, Grégoire J, Plante M,
Renaud MC, Bachvarov D, Douville P and Bairati I: Human epididymis
protein 4 (HE4) and ovarian cancer prognosis. Gynecol Oncol.
127:511–515. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bignotti E, Ragnoli M, Zanotti L, Calza S,
Falchetti M, Lonardi S, Bergamelli S, Bandiera E, Tassi RA, Romani
C, et al: Diagnostic and prognostic impact of serum HE4 detection
in endometrial carcinoma patients. Br J Cancer. 104:1418–1425.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Li X, Gao Y, Tan M, Zhuang H, Gao J, Hu Z,
Wang H, Zhu L, Liu J and Lin B: Expression of HE4 in endometrial
cancer and its clinical significance. Biomed Res Int.
2015:4374682015.PubMed/NCBI
|
|
22
|
Iwahori K, Suzuki H, Kishi Y, Fujii Y,
Uehara R, Okamoto N, Kobayashi M, Hirashima T, Kawase I and Naka T:
Serum HE4 as a diagnostic and prognostic marker for lung cancer.
Tumour Biol. 33:1141–1149. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yamashita S, Tokuishi K, Hashimoto T,
Moroga T, Kamei M, Ono K, Miyawaki M, Takeno S, Chujo M, Yamamoto S
and Kawahara K: Prognostic significance of HE4 expression in
pulmonary adenocarcinoma. Tumour Biol. 32:265–271. 2011. View Article : Google Scholar
|
|
24
|
Zhong H, Qian Y, Fang S, Yang L, Li L and
Gu W: HE4 expression in lung cancer, a meta-analysis. Clin Chim
Acta. 470:109–114. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kamei M, Yamashita S, Tokuishi K, Hashioto
T, Moroga T, Suehiro S, Ono K, Miyawaki M, Takeno S, Yamamoto S and
Kawahara K: HE4 expression can be associated with lymph node
metastases and disease-free survival in breast cancer. Anticancer
Res. 30:4779–4783. 2010.PubMed/NCBI
|
|
26
|
Guo YD, Wang JH, Lu H, Li XN, Song WW,
Zhang XD and Zhang WM: The human epididymis protein 4 acts as a
prognostic factor and promotes progression of gastric cancer.
Tumour Biol. 36:2457–2464. 2015. View Article : Google Scholar :
|
|
27
|
Kemal YN, Demirag GN, Bedir AM, Tomak L,
Derebey M, Erdem DL, Gör U and Yücel I: Serum human epididymis
protein 4 levels in colorectal cancer patients. Mol Clin Oncol.
7:481–485. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Galgano MT, Hampton GM and Frierson HF Jr:
Comprehensive analysis of HE4 expression in normal and malignant
human tissues. Mod Pathol. 19:847–853. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jiang SW, Chen H, Dowdy S, Fu A, Attewell
J, Kalogera E, Drapkin R, Podratz K, Broaddus R and Li J: HE4
transcription- and splice variants-specific expression in
endometrial cancer and correlation with patient survival. Int J Mol
Sci. 14:22655–22677. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ryu B, Jones J, Blades NJ, Parmigiani G,
Hollingsworth MA, Hruban RH and Kern SE: Relationships and
differentially expressed genes among pancreatic cancers examined by
large-scale serial analysis of gene expression. Cancer Res.
62:819–826. 2002.PubMed/NCBI
|
|
31
|
O'Neal RL, Nam KT, LaFleur BJ, Barlow B,
Nozaki K, Lee HJ, Kim WH, Yang HK, Shi C, Maitra A, et al: Human
epididymis protein 4 is up-regulated in gastric and pancreatic
adenocarcinomas. Hum Pathol. 44:734–742. 2013. View Article : Google Scholar
|
|
32
|
Huang T, Jiang SW, Qin L, Senkowski C,
Lyle C, Terry K, Brower S, Chen H, Glasgow W, Wei Y and Li J:
Expression and diagnostic value of HE4 in pancreatic
adenocarcinoma. Int J Mol Sci. 16:2956–2970. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lu Q, Chen H, Senkowski C, Wang J, Wang X,
Brower S, Glasgow W, Byck D, Jiang SW and Li J: Recombinant HE4
protein promotes proliferation of pancreatic and endometrial cancer
cell lines. Oncol Rep. 35:163–170. 2016. View Article : Google Scholar
|
|
34
|
Ohkuma R, Yada E, Ishikawa S, Komura D,
Ishizaki H, Tamada K, Kubota Y, Hamada K, Ishida H, Hirasawa Y, et
al: High expression of olfactomedin-4 is correlated with
chemoresistance and poor prognosis in pancreatic cancer. PLoS One.
15:e02267072020. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Morton CL and Houghton PJ: Establishment
of human tumor xenografts in immunodeficient mice. Nat Protoc.
2:247–250. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chijiwa T, Kawai K, Noguchi A, Sato H,
Hayashi A, Cho H, Shiozawa M, Kishida T, Morinaga S, Yokose T, et
al: Establishment of patient-derived cancer xenografts in
immune-deficient NOG mice. Int J Oncol. 47:61–70. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Langmead B, Trapnell C, Pop M and Salzberg
SL: Ultrafast and memory-efficient alignment of short DNA sequences
to the human genome. Genome Biol. 10:R252009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Komura D, Isagawa T, Kishi K, Suzuki R,
Sato R, Tanaka M, Katoh H, Yamamoto S, Tatsuno K, Fukayama M, et
al: CASTIN: A system for comprehensive analysis of cancer stromal
interactome. BMC Genomics. 17:8992016. View Article : Google Scholar
|
|
39
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expres sion data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar
|
|
40
|
Jin K, Li G, Cui B, Zhang J, Lan H, Han N,
Xie B, Cao F, He K, Wang H, et al: Assessment of a novel VEGF
targeted agent using patient-derived tumor tissue xenograft models
of colon carcinoma with lymphatic and hepatic metastases. PLoS One.
6:e283842011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yada E, Wada S, Yoshida S and Sanada T:
Use of patient-derived xenograft mouse models in cancer research
and treatment. Future Sci OA. 4:FSO2712017. View Article : Google Scholar
|
|
42
|
Hidalgo M, Amant F, Biankin AV, Budinská
E, Byrne AT, Caldas C, Clarke RB, de Jong S, Jonkers J, Mælandsmo
GM, et al: Patient derived xenograft models: An emerging platform
for translational cancer research. Cancer Discov. 4:998–1013. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cho SY, Kang W, Han JY, Min S, Kang J, Lee
A, Kwon JY, Lee C and Park H: An integrative approach to precision
cancer medi cine using patient-derived xenografts. Mol Cells.
39:77–86. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Lefford H: US Cancer Institute to overhaul
tumour cell lines. Nature. 530:3912016. View Article : Google Scholar
|
|
45
|
Fujii E, Suzuki M, Matsubara K, Watanabe
M, Chen YJ, Adachi K, Ohnishi Y, Tanigawa M, Tsuchiya M and Tamaoki
N: Establishment and characterization of in vivo human tumor models
in the NOD/SCID/gamma(c)(null) mouse. Pathol Int. 58:559–567. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Galimi F, Torti D, Sassi F, Isella C, Corà
D, Gastaldi S, Ribero D, Muratore A, Massucco P, Siatis D, et al:
Genetic and expression analysis of MET, MACC1, and HGF in
metastatic colorectal cancer: Response to met inhibition in patient
xenografts and pathologic correlations. Clin Cancer Res.
17:3146–3156. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Bertotti A, Migliardi G, Galimi F, Sassi
F, Torti D, Isella C, Corà D, Di Nicolantonio F, Buscarino M, Petti
C, et al: A molecularly annotated platform of patient-derived
xenografts ('xenopatients') identifies HER2 as an effective
therapeutic target in cetuximab-resistant colorectal cancer. Cancer
Discov. 1:508–523. 2011. View Article : Google Scholar
|
|
48
|
de Sousa Abreu R, Penalva LO, Marcotte EM
and Vogel C: Global signatures of protein and mRNA expression
levels. Mol Biosyst. 5:1512–1526. 2009.PubMed/NCBI
|
|
49
|
Schwanhäusser B, Busse D, Li N, Dittmar G,
Schuchhardt J, Wolf J, Chen W and Selbach M: Global quantification
of mammalian gene expression control. Nature. 473:337–342. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Wu L, Candille SI, Choi Y, Xie D, Jiang L,
Li-Pook-Than J, Tang H and Snyder M: Variation and genetic control
of protein abundance in humans. Nature. 499:79–82. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Zhang B, Wang J, Wang X, Zhu J, Liu Q, Shi
Z, Chambers MC, Zimmerman LJ, Shaddox KF, Kim S, et al:
Proteogenomic characterization of human colon and rectal cancer.
Nature. 513:382–387. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Zou SL, Chang XH, Ye X, Cheng HY, Cheng
YX, Tang ZJ, Zhang ZJ, Gao L, Chen XH and Cui H: Effect of human
epididymis protein 4 gene silencing on the malignant phenotype in
ovarian cancer. Chin Med J (Engl). 124:3133–3140. 2011.
|
|
53
|
Zhu YF, Gao GL, Tang SB, Zhang ZD and
Huang QS: Effect of WFDC 2 silencing on the proliferation, motility
and invasion of human serous ovarian cancer cells in vitro. Asian
Pac J Trop Med. 6:265–272. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Zhuang H, Hu Z, Tan M, Zhu L, Liu J, Liu
D, Yan L and Lin B: Overexpression of Lewis yantigen promotes human
epididymis protein 4-mediated invasion and metastasis of ovarian
cancer cells. Biochimie. 105:91–98. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Lu R, Sun X, Xiao R, Zhou L, Gao X and Guo
L: Human epididymis protein 4 (HE4) plays a key role in ovarian
cancer cell adhesion and motility. Biochem Biophys Res Commun.
419:274–280. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Li J, Chen H, Mariani A, Chen D, Klatt E,
Podratz K, Drapkin R, Broaddus R, Dowdy S and Jiang SW: HE4 (WFDC2)
promotes tumor growth in endometrial cancer cell lines. Int J Mol
Sci. 14:6026–6043. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Lee S, Choi S, Lee Y, Chung D, Hong S and
Park N: Role of human epididymis protein 4 in chemoresistance and
prognosis of epithelial ovarian cancer. J Obstet Gynaecol Res.
43:220–227. 2017. View Article : Google Scholar
|
|
58
|
Moore RG, Hill EK, Horan T, Yano N, Kim K,
MacLaughlan S, Lambert-Messerlian G, Tseng YD, Padbury JF, Miller
MC, et al: HE4 (WFDC2) gene overexpression promotes ovarian tumor
growth. Sci Rep. 4:35742014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Maihle NJ, Baron AT, Barrette BA, Boardman
CH, Christensen TA, Cora EM, Faupel-Badger JM, Greenwood T, Juneja
SC, Lafky JM, et al: EGF/ErbB receptor family in ovarian cancer.
Cancer Treat Res. 107:247–258. 2002.PubMed/NCBI
|
|
60
|
Gotlieb WH, Bruchim I, Gu J, Shi Y,
Camirand A, Blouin MJ, Zhao Y and Pollak MN: Insulin-like growth
factor receptor I targeting in epithelial ovarian cancer. Gynecol
Oncol. 100:389–396. 2006. View Article : Google Scholar
|
|
61
|
Spannuth WA, Nick AM, Jennings NB,
Armaiz-Pena GN, Mangala LS, Danes CG, Lin YG, Merritt WM, Thaker
PH, Kamat AA, et al: Functional significance of VEGFR-2 on ovarian
cancer cells. Int J Cancer. 124:1045–1053. 2009. View Article : Google Scholar :
|
|
62
|
Braicu EI, Fotopoulou C, Van Gorp T,
Richter R, Chekerov R, Hall C, Butz H, Castillo-Tong DC, Mahner S,
Zeillinger R, et al: Preoperative HE4 expression in plasma predicts
surgical outcome in primary ovarian cancer patients: Results from
the OVCAD study. Gynecol Oncol. 128:245–251. 2013. View Article : Google Scholar
|
|
63
|
Ribeiro JR, Schorl C, Yano N, Romano N,
Kim KK, Singh RK and Moore RG: HE4 promotes collateral resistance
to cisplatin and paclitaxel in ovarian cancer cells. J Ovarian Res.
9:282016. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Wang H, Zhu L, Gao J, Hu Z and Lin B:
Promotive role of recombinant HE4 protein in proliferation and
carboplatin resistance in ovarian cancer cells. Oncol Rep.
33:403–412. 2015. View Article : Google Scholar
|
|
65
|
Angioli R, Capriglione S, Aloisi A, Guzzo
F, Luvero D, Miranda A, Damiani P, Montera R, Terranova C and
Plotti F: Can HE4 predict platinum response during first-line
chemotherapy in ovarian cancer? Tumour Biol. 35:7009–7015. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Oweira H, Petrausch U, Helbling D, Schmidt
J, Mannhart M, Mehrabi A, Schöb O, Giryes A, Decker M and
Abdel-Rahman O: Prognostic value of site-specific metastases in
pancreatic adenocarcinoma: A Surveillance epidemiology and end
results database analysis. World J Gastroenterol. 23:1872–1880.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Nipp R, Tramontano AC, Kong CY,
Pandharipande P, Dowling EC, Schrag D and Hur C: Disparities in
cancer outcomes across age, sex, and race/ethnicity among patients
with pancreatic cancer. Cancer Med. 7:525–535. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Maisey NR, Norman AR, Hill A, Massey A,
Oates J and Cunningham D: CA19-9 as a prognostic factor in
inoperable pancreatic cancer: The implication for clinical trials.
Br J Cancer. 93:740–743. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Piciucchi M, Stigliano S, Archibugi L,
Zerboni G, Signoretti M, Barucca V, Valente R, Fave GD and Capurso
G: The neutrophil/lymphocyte ratio at diagnosis is significantly
associated with survival in metastatic pancreatic cancer patients.
Int J Mol Sci. 18:7302017. View Article : Google Scholar :
|
|
70
|
Luo J, Xiao L, Wu C, Zheng Y and Zhao N:
The incidence and survival rate of population-based pancreatic
cancer patients: Shanghai Cancer Registry 2004-2009. PLoS One.
8:e760522013. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Baine M, Sahak F, Lin C, Chakraborty S,
Lyden E and Batra SK: Marital status and survival in pancreatic
cancer patients: A SEER based analysis. PLoS One. 6:e210522011.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
David M, Lepage C, Jouve JL, Jooste V,
Chauvenet M, Faivre J and Bouvier AM: Management and prognosis of
pancreatic cancer over a 30-year period. Br J Cancer. 101:215–218.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Liu X, Fu Y, Chen Q, Wu J, Gao W, Jiang K,
Miao Y and Wei J: Predictors of distant metastasis on exploration
in patients with potentially resectable pancreatic cancer. BMC
Gastroenterol. 18:1682018. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Hohla F, Hopfinger G, Romeder F,
Rinnerthaler G, Bezan A, Stättner S, Hauser-Kronberger C, Ulmer H
and Greil R: Female gender may predict response to FOLFIRINOX in
patients with unresectable pancreatic cancer: A single institution
retrospective review. Int J Oncol. 44:319–326. 2014. View Article : Google Scholar
|
|
75
|
Lambert A, Jarlier M, Gourgou Bourgade S
and Conroy T: Response to FOLFIRINOX by gender in patients with
metastatic pancreatic cancer: Results from the PRODIGE 4/ACCORD 11
randomized trial. PLoS One. 12:e01832882017. View Article : Google Scholar
|