1. Introduction
Liver cancer is a common malignancy. In recent
years, the incidence rate and mortality rate of liver cancer have
been rising. Primary liver cancer was the sixth most commonly
diagnosed cancer type and the third leading cause of
cancer-associated death in the world in 2020 (1). Primary liver cancer includes
hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma,
as well as other rare types; HCC accounts for 75-85% of cases
(1). Risk factors for HCC include
chronic hepatitis B and C, alcohol addiction, metabolic liver
disease [particularly non-alcoholic fatty liver disease (NAFLD)]
and exposure to dietary toxins, such as aflatoxin and carmine acid
(2). Liver cancer is an advanced
outcome of a range of liver diseases. NAFLD and non-alcoholic
steatohepatitis (NASH) are increasingly recognized as important
underlying causes of HCC (3).
Genetic predisposition, interactions between viral and nonviral
risk factors, the cellular microenvironment and various immune
cells, as well as the severity of an underlying chronic liver
disease, among others, are at the origin of the early steps in the
malignant transformation of hepatocytes and development of HCC,
whereas an altered microenvironment is a key contributing feature
of cancer and is involved in all stages of malignant progression
(4).
Bile acids (BAs) are attracting increasing attention
from researchers and this field has developed rapidly. Hepatic
accumulation of BAs is central to the pathogenesis of
cholestasis-induced liver injury and excessive cytotoxic BAs in the
liver may lead to liver fibrosis and cirrhosis, and even liver
cancer (5). The interest in the
role of BAs in HCC has increased and there is increasing evidence
that BAs have a role in HCC. In the present review, the
biosynthesis, metabolism and transport of BAs are presented and the
mechanistic links between BAs and HCC, as well as the opportunities
of targeting BAs for the prevention or treatment of HCC are
discussed.
2. BAs
The human understanding of BAs dates back to nearly
3,000 years ago, when animal bile was widely used in Traditional
Chinese Medicine (6). Since the
19th century, BAs have become the subject of detailed research by
scientists (6). BAs, the main
lipid components of bile, are a general term for a class of
cholanic acids that are converted from cholesterol in hepatocytes
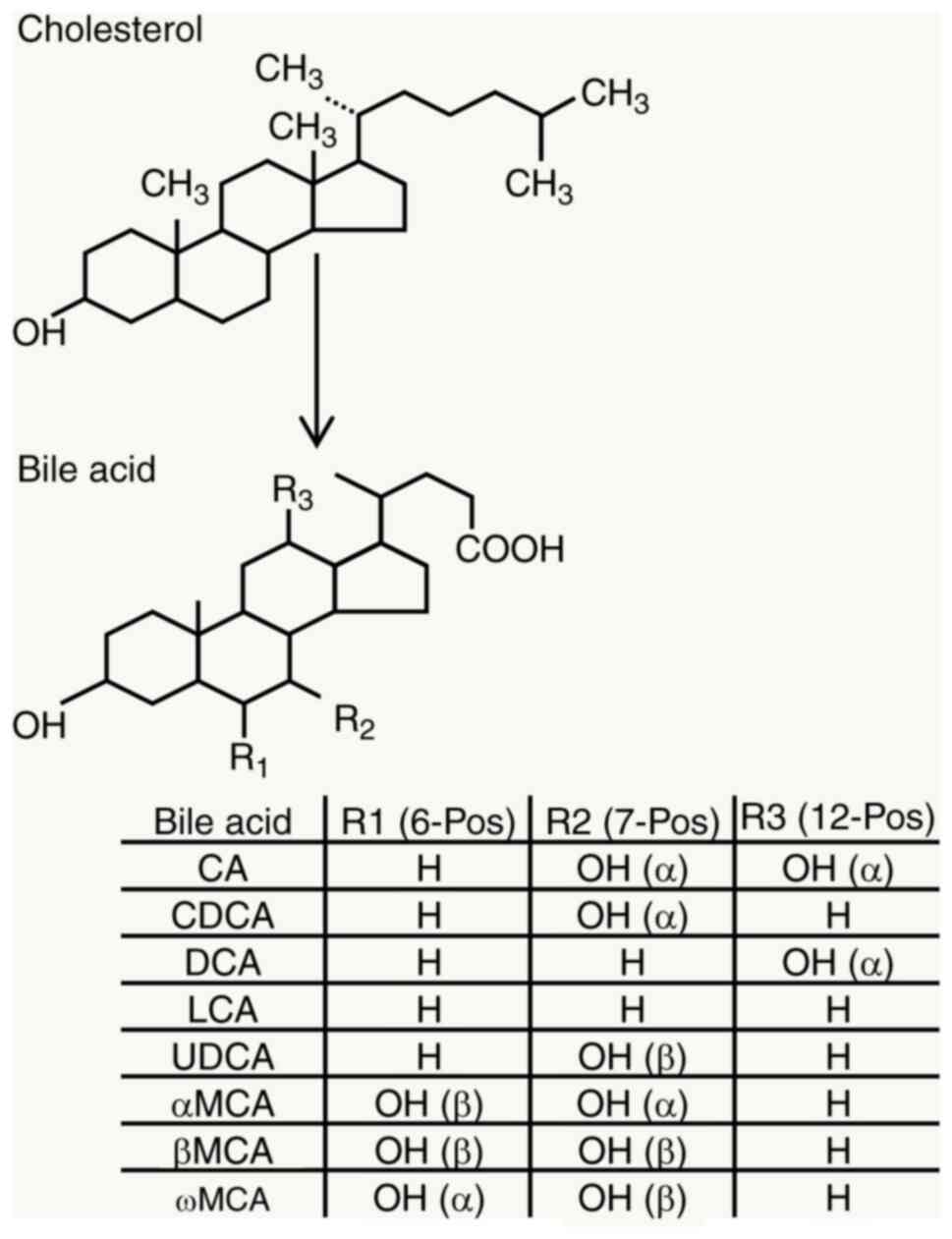
through a series of enzymatic reactions (7). In general, BAs have steroid cores and
four fused hydrocarbon rings with polar hydroxyl functional groups.
Three hydroxyl and carboxyl groups face one side of the carbon
skeleton, forming a hydrophilic surface, in contrast to a highly
hydrophobic surface (7) (Fig. 1). Thus, BAs are amphipathic
molecules with powerful detergent properties.
According to the source of BAs, they may be divided
into primary BAs and secondary BAs. In hepatocytes, BAs synthesized
directly from cholesterol are called primary BAs, which include
cholic acid (CA) and chenodeoxycholic acid (CDCA). After primary BA
synthesis, most BAs bind to glycine or taurine, changing from a
free form to a binding form; BAs form sodium salts at physiological
pH values, which increases their solubility (8). Primary BAs enter the intestine and
are converted to secondary BAs, mainly deoxycholic acid (DCA) and
trace amounts of lithocholic acid (LCA), through the enzymatic
activity of intestinal bacteria (7). These total BAs circulate in the
enterohepatic circulation of the human body, including those in the
liver (<1%), intestine (85-90%) and gallbladder (10-15%),
constituting the BA pool (9). The
human BA pool consists of CA (40%), CDCA (40%) and DCA (20%), in
which the ratio of glycine (G)-/taurine (T)-conjugated BAs is 3:1,
and the BA pool has high hydrophobicity (9). Due to the different kinds of enzymes
and metabolic pathways, the BAs in mice have other types in
addition to those mentioned above, mainly muricholic acids (MCAs)
(9).
BA synthesis
The synthesis and secretion of BAs are the main
pathways of cholesterol catabolism in the human body. Cholesterol
is eventually converted into water-soluble and easily excreted BAs.
BA formation is complex, including several reaction steps catalyzed
by at least 17 different enzymes, one or more transporters and
multiple cellular compartments, which include the cytosol,
endoplasmic reticulum (ER), mitochondria and peroxisomes (6). BA synthesis occurs in the liver,
which is the only organ that possesses all the enzymes required for
BA synthesis (9). BA synthesis is
divided into the classical and the alternative pathway, which are
initiated by the microsomal cytochrome P450 (CYP) enzymes
cholesterol 7α-hydroxylase (CYP7A1) and mitochondrial sterol
27-hydroxylase (CYP27A1), respectively (Fig. 2). In humans, the classical pathway
of BA synthesis accounts for at least 75% of total BA production
and is considered to be the main pathway of BA biosynthesis
(10). Primary BAs are
amino-conjugated at the carboxyl group, with a ratio of glycine to
taurine conjugates of approximately 3:1 (11). BAs may also bind to sulfate or
glucuronic acid to form fully ionized, negatively charged
hydrophilic polar molecules, and these bound forms of BAs
subsequently discharge into the intestine with bile. The step of
binding BAs to amino acids is markedly efficient and >98% of the
BAs secreted into bile are in taurineor glycine-conjugated forms
(6). In the intestine, the bound
form of primary BAs undergoes dissociation and dehydroxylation to
produce secondary BAs. The primary BAs synthesized in the liver of
mice also include αMCA and βMCA, and ωMCA may be produced by gut
microbial 7α/β-epimerization in the intestine of mice (10).
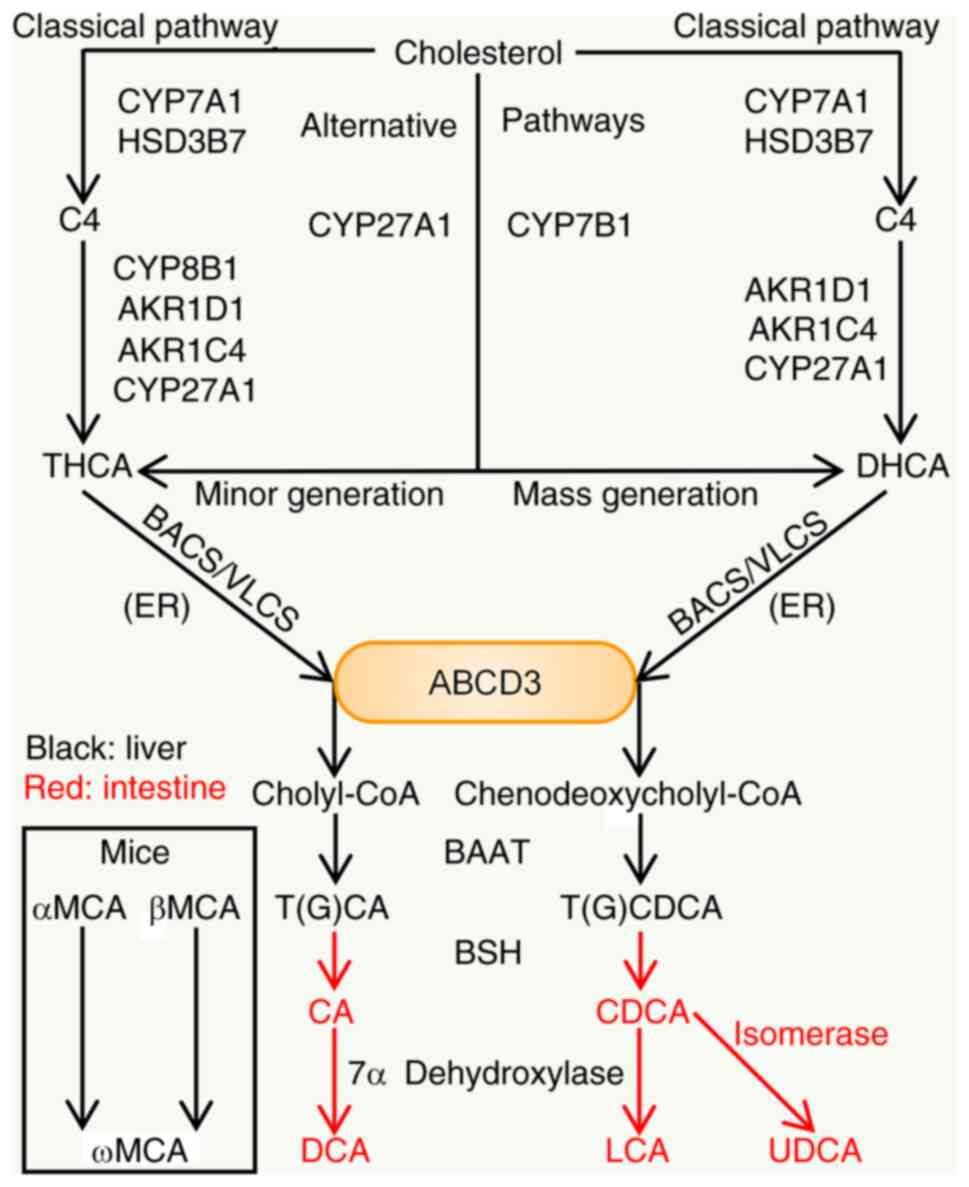 | Figure 2Processes of BA synthesis. In the
liver, the classical pathway is initiated by CYP7A1, the
rate-limiting enzyme. CYP7A1 and HSD3B7 are able to convert
cholesterol to form C4. CYP8B1 performs 12α-hydroxylation of C4.
Subsequently, under the catalysis of AKR1D1, AKR1C4 and CYP27A1,
THCA is generated. However, without 12α-hydroxylation, C4 is
converted to DHCA. BACS or VLCS in the ER then ligate Co-A to the
carboxyl groups. After transport by peroxisomal transporter ABCD3
and catalysis by a series of enzymes, THCA and DHCA synthesize
cholyl-CoA and chenodeoxycholyl-CoA. These two substances are then
conjugated to taurine or glycine by BAAT. The alternative pathway
is mainly initiated by CYP27A1. Next, through CYP7B1 and other
enzymes that belong to CYP proteins, cholesterol is being subjected
to modifications to finally generate CDCA and a small amount of CA.
Certain conjugated forms of BAs entering the intestine may be
dissociated by BSH and bacterial 7α dehydroxylase may then convert
CA and CDCA into DCA and LCA, respectively. CDCA may also be
isomerized to UDCA. In mice, the generation of MCA was observed in
addition to the above synthetic processes [Refs. (6-8,12)].
BA, bile acid; BSH, BA hydrolase; HSD3B7, 3β-hydroxy-5-C27-steroid
dehydrogenase; C4, 7α-hydroxy-4-cholesten-3-one; CYP, cytochrome
P450; CYP8B1, sterol 12α-hydroxylase; CYP7B1, nonspecific oxysterol
7α-hydroxylase; AKR1D1, aldo-keto reductase family 1 member D1;
BAAT, BA-CoA:amino acid N-acyltransferase; THCA,
3α,7α,12α-trihydroxy-5β cholestanoic acid; DHCA, 3α,7α-dihydroxy-5β
cholestanoic acid; BACS, BA-Co-A synthase; VLCS, very long-chain
Co-A synthase; ER, endoplasmic reticulum; CA, cholic acid; CDCA,
chenodeoxycholic acid; UDCA, ursodeoxycholic acid; DCA, deoxycholic
acid; LCA, lithocholic acid; MCA, muricholic acid; ABCD3, ATP
binding cassette subfamily D member 3. |
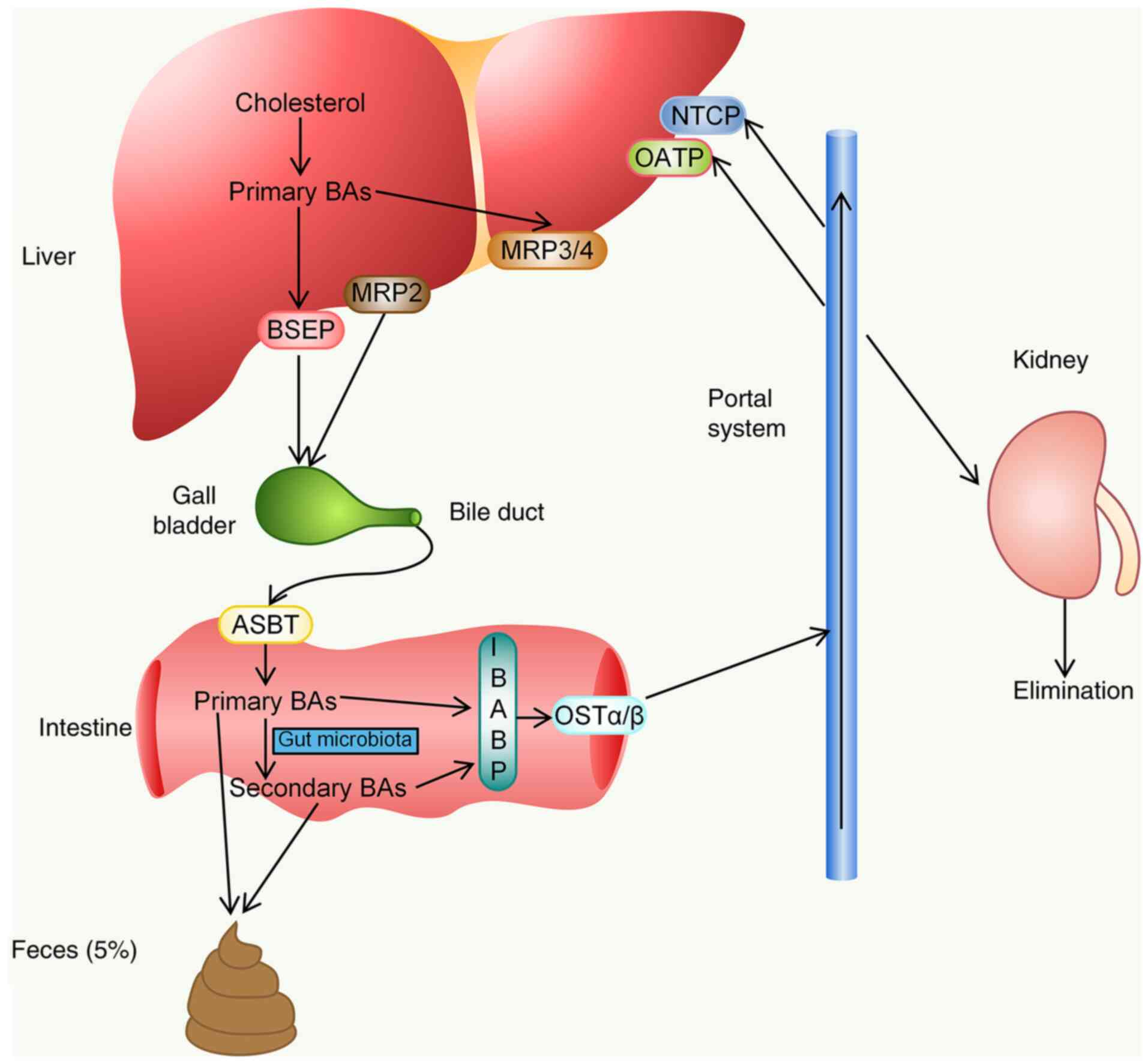
Enterohepatic circulation
The enterohepatic circulation of BAs refers to the
system in which BAs are synthesized by the liver, discharged into
the intestine with bile and then reabsorbed in the intestine and
returned to the liver via the portal vein. BAs are synthesized in
the liver and secreted by the canalicular membrane transporters, of
which the most important is the bile salt export pump [BSEP/ATP
binding cassette (ABC) subfamily B member 11] (12,13).
In addition, BAs conjugated with sulfate or glucuronic acid become
dianionic compounds and may be transported by multidrug
resistance-associated protein 2 (MRP2) on the canalicular membrane
(14). In addition, MRP3 and MRP4,
located on the basolateral side of hepatocytes, are considered
compensatory BA efflux transporters and they mainly act when bile
excretion by BSEP is impaired (15).
BAs are stored in the gallbladder and released into
the intestine after a meal. In the small intestine, a small
proportion of free BAs are reabsorbed into intestinal epithelial
cells via passive diffusion in the small intestine and colon
(16). However, the majority of
conjugated BAs can hardly be absorbed in the proximal small
intestine, and at the end of the ileum, they are mainly actively
and effectively reabsorbed into intestinal epithelial cells by the
apical sodium-dependent BA transporter [ASBT/solute carrier family
10 member 2 (SLC10A2)] of the apical membrane (16). Subsequently, BAs bind to intestinal
BA binding protein and are transported to the basement membrane for
secretion (17). Although the
absorption of BAs in the terminal ileum is effective, certain
molecules escape and reach the large intestine. BAs entering the
colon undergo modifications to produce secondary BAs. BAs in the
small and large intestine may be reabsorbed by the heterodimer
organic solute transporter α/β at the terminal lumen of the
basement membrane and transported back to the liver (18). A small number of BAs that escape
absorption may pass into the colon to be eliminated in the
feces.
The last step in the enterohepatic circulation is
the absorption of BAs from the portal vein by hepatocytes through
transporters. Sodium-taurocholate co-transporting polypeptide
(NTCP/SLC10A1) and organic anion transporting polypeptides are the
main transporters involved in this process (12). Hepatocytes reprocess BAs and
secrete them along with the bile to complete enterohepatic
circulation. BAs that are not re-ingested by hepatocytes spread to
the systemic circulation and may eventually be excreted through the
kidney (19) (Fig. 3).
The enterohepatic circulation of BAs occurs 6-8
times a day on average to maintain a constant BA pool size (~3 g)
(20,21). The enterohepatic circulation of BAs
is highly efficient, with ~95% of the BAs reabsorbed in the ileum
and only 5% of the BAs being lost in the feces (22,23).
The full elucidation of BA synthesis and transport regulators in
the enterohepatic circulation may provide potential targets for
drug treatment of cholestatic liver diseases (20).
Functions of BA
BAs have a variety of physiological roles, the most
important of which is to promote the digestion and absorption of
lipids (11). BA molecules have
hydrophilic and hydrophobic sides in their configuration, which
endows them with strong interfacial activity to reduce the surface
tension between oil and water phases and promote lipid
emulsification. At the same time, BAs enlarge the contact surface
between lipids and lipase and accelerate the digestion of lipids
(11,24). BAs may also inhibit the
precipitation of cholesterol in bile and prevent the formation of
cholesterol stones. Cholesterol is poorly soluble in water and must
be incorporated into lecithin-bile salts to be transported through
the biliary tract into the small intestine without precipitation
(25).
BAs recognize a variety of receptors and mediate
downstream signals. The main BA-mediated nuclear receptors are
farnesoid X receptor (FXR), pregnane X receptor and vitamin D
receptor. FXR, the first identified BA receptor, is essentially a
BA-binding transcription factor that functions by triggering
transcriptional changes (26). FXR
is mainly expressed in the intestine and liver, and the order of
binding potency of BAs to FXR is CDCA>LCA=DCA>CA (27,28).
Furthermore, the binding activity is different under different
physiological conditions. FXR signaling may have multiple
physiological roles, such as negatively feedback-regulating BA
synthesis, regulating BA transport and regulating energy metabolism
and immune responses (29). In
terms of cell membrane receptors, BAs mainly recognize Takeda G
protein-coupled receptor 5 (TGR5, also known as GPBAR1) (30). In addition to TGR5, BA-activated
G-protein-coupled receptors also include sphingosine-1-phosphate
receptor 2 (31). Studies have
indicated that TGR5 is highly expressed in liver cells other than
hepatocytes, including Kupffer cells and cholangiocytes, and in
gallbladder epithelial cells and immune cells (32). TGR5 is being dose-dependently
activated by BAs, with the following rank order of potency:
LCA≥DCA>CDCA>CA (30). FXR
and TGR5 are the two most important receptors for BA mediation,
whose signals provide crosstalk between the intestine and the
liver. BAs-FXR and BAs-TGR5 signals are widely involved in the
pathogenesis of HCC. Therefore, the development of FXR and TGR5
modulators may provide therapeutic interventions for HCC.
3. BAs and HCC
Relationship between alterations of BAs
and HCC
The delicate connection between BAs and HCC is
gradually being confirmed experimentally. In particular, an
imbalance between nontoxic hydrophilic BAs and toxic hydrophobic
BAs occurs when BA transporter expression is downregulated for
various reasons and the accumulation of toxic BAs drives HCC
progression (33,34). A retrospective cohort study from
2004 to 2014 including 2,262 patients with chronic hepatitis B on
conventional antiviral therapy indicated that persistent elevation
of serum total BAs was an independent risk factor for HCC (35). However, the result of another study
was that conjugated primary BAs were significantly elevated,
whereas the ratios of secondary BAs over primary BAs were
significantly lower in HCC cases than in controls (36). The doubling ratio of taurine-over
glycine-conjugated CDCA was significantly associated with a 40%
increased risk of HCC, whereas the doubling ratio of secondary over
primary BAs was associated with a 30-40% reduced risk of HCC
(36). In addition, a weighted
relative difference accumulation algorithm study suggested that
patients with hepatitis and cirrhosis had increased serum levels of
G-CDCA, G-CA and T-CA and decreased serum levels of CDCA (37). After 0.2% CA treatment,
diethylnitrosamine (DEN)-induced liver tumors in mice increased by
three-fold in number and size, and the mRNA levels of TNF-α and
IL-1β were significantly increased (38). G-CDCA promotes the survival of
HepG2 and QGY-7703 liver cancer cells by activating antiapoptotic
genes such as Bcl-2; furthermore, G-CDCA was able to reduce the
chemosensitivity of 5-fluorouracil to both cell lines (34). In addition, experiments in which
C57BL/6J mice were fed a high-fat diet for 58 weeks demonstrated
that long-term high-fat diet feeding induced liver tumors in mice,
along with the observation of significantly increased T-CDCA, T-CA
and G-CA in plasma and liver (39). T-CDCA treatment of HepG2 cells
significantly increased cell proliferation and decreased the
expression of CEBPα (CEBPα is a tumor suppressor protein) in HCC,
which suggests that BAs alone may have a tumor-promoting effect
(39). There is also an
experimental finding that metabolites related to BA biosynthesis,
such as glycochenodeoxycholic acid 3-sulfate, G-CA, G-DCA, T-CA and
T-CDCA, are downregulated in patients with HCC compared to
cirrhotic patients (40). All of
these studies indicate the possibility that BAs may be dynamically
altered all the way to the detriment of the organism in the course
of HCC progression.
The effect of BAs on HCC is complex. For instance,
in the case of CDCA, a study suggested that it promotes the growth
of a variety of tumor cell lines (39). However, another study observed
downregulation of CDCA levels in patients with HCC (40). In different experiments,
contradictory results regarding the effect of certain BAs on HCC
have been obtained, which may be due to the differences in samples,
experimental methods and measurements selected by different
research institutes. Future studies are required to have a better
design, for instance, to control a specific BA as a variable and
set up controls. It was indicated that gene knockout of key enzymes
during BA synthesis (e.g., CYP7A1, CYP27A1) in mice was able to
better qualitatively and quantitatively analyze the role of BAs in
the pathogenesis of diseases (41). This method may also be applied to
the study of HCC. However, it may be a better way to study the
signaling pathways mediated by BAs and their metabolites in HCC,
which may contribute to the future targeted treatment of BAs.
Mechanisms by which BAs mediate HCC
FXR. FXR is thought to be the most important
receptor for BAs to mediate the development of HCC. The expression
of hepatic FXR may inhibit the occurrence of HCC through the
following mechanisms: i) FXR maintains the normal liver metabolism
of BAs, glucose and lipids; ii) FXR suppresses hepatic inflammation
and promotes liver regeneration and repair after injury; iii) FXR
protects liver cells from death and enhances cell survival; and iv)
FXR may directly increase the expression of certain
tumor-suppressor genes and repress the transcription of several
oncogenes (42). Decreased FXR
signaling leads to decreased liver transporter function, resulting
in enhanced hepatic BA sequestration and persistent inflammation,
which may promote HCC development. Liver tumors are observed in 90%
of global FXR-null mice, but only 20% of liver-specific FXR-null
mice develop spontaneous HCC (43). Sirtuin 1 is a transcriptional
regulator of FXR, and under pathological conditions of cholestasis,
it is downregulated by toxic BAs such as T-DCA, T-CA and DCA,
resulting in the inhibition of FXR (44). In the course of liver injury,
signals mediated by inflammatory factors such as TNF-α and NF-κB
are also involved in the downregulation of FXR (45). FXR was indicated to bind directly
to β-catenin, leading to reduced transcriptional activity in HCC
(46). However, during HCC
progression, Wnt/β-catenin signaling is enhanced and mRNAs of its
target gene Myc are mainly found in the liver of FXR-null mice
(43). T-CA was able to increase
Myc expression in FXR-null hepatocytes and Myc has a crucial role
in HCC development due to the induction of cell proliferation and
migration (47).
Fibroblast growth factor 15/19 (FGF15/19) is also a
target gene of FXR. Activation of the FGF15/19-fibroblast growth
factor receptor 4 (FGFR4)-SRY-related high-mobility group box 18
pathway may directly promote epithelial to mesenchymal transition
of HCC cells in vitro (29,48).
FXR may also directly affect HCC cell proliferation by regulating
several tumor suppressors downstream, such as suppressor of
cytokine signaling 3 (SOCS3), N-myc downstream-regulated gene 2 and
microRNA-122 (miR-122) (29)
(Fig. 4). Therefore, when FXR is
downregulated, the body's inhibitory effect on HCC is
diminished.
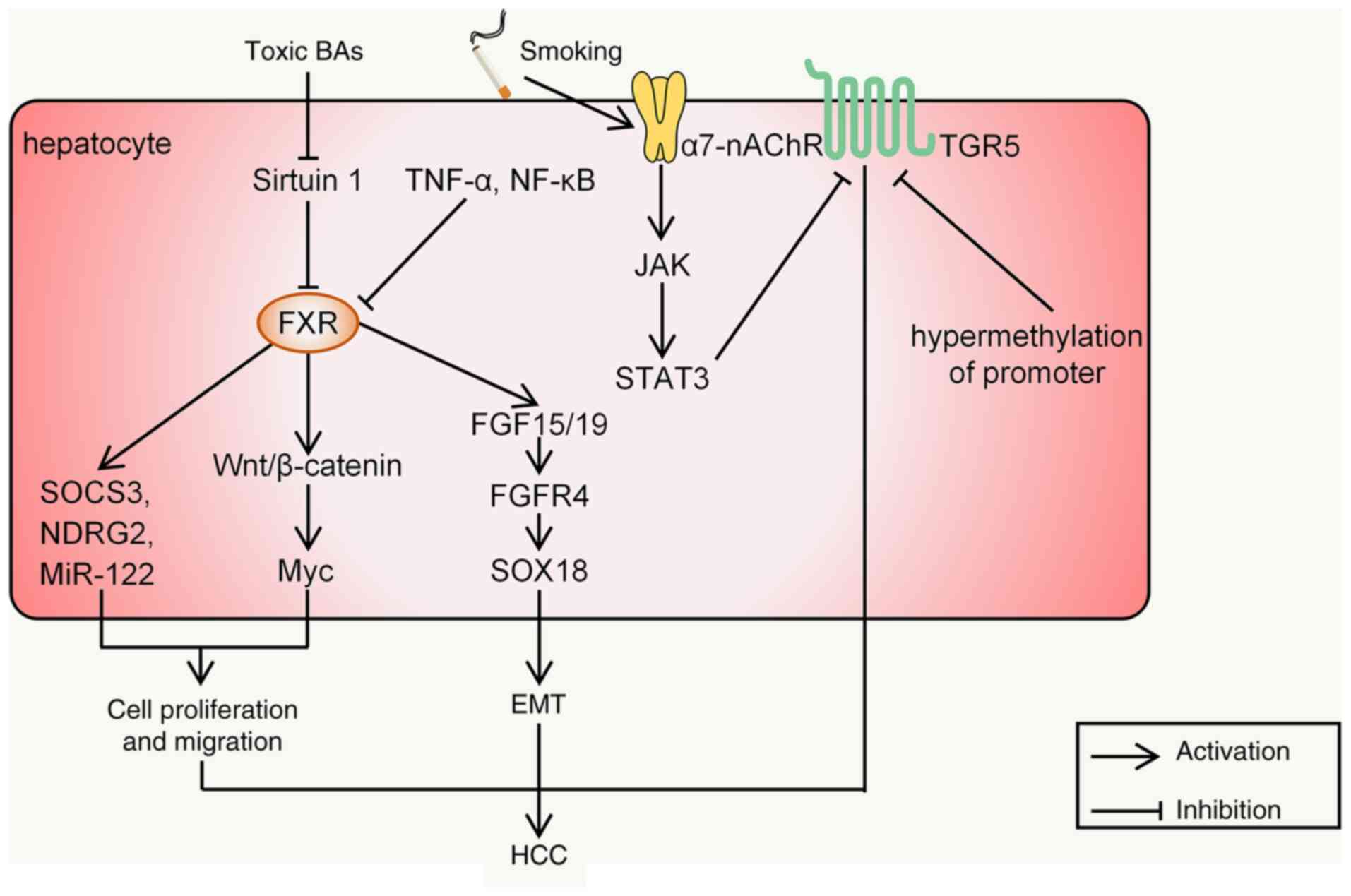 | Figure 4Intracellular signaling in HCC
mediated by FXR and TGR5. BA, bile acid; HCC, hepatocellular
carcinoma; EMT, epithelial to mesenchymal transition; FXR, FXR,
farnesoid X receptor; SOCS3, suppressor of cytokine signaling 3;
TGR5, Takeda G protein-coupled receptor 5; miR, microRNA; FGFR,
fibroblast growth factor receptor; NDRG2, N-myc
downstream-regulated gene 2; α7-nAChR, α7-nicotinic acetylcholine
receptor. |
TGR5. The secondary BAs DCA and LCA are the
most potent natural ligands for TGR5 (49). TGR5 participates in the regulation
of nutrient metabolism and energy consumption after activation. The
induction of TGR5 in intestinal endocrine cells may promote the
release of glucagon-like peptide 1 (GLP-1) (50). Certain studies have also indicated
that this process may be initiated by FXR. FXR increases the
production of LCA in the intestine, which activates TGR5 to
stimulate the secretion of GLP-1 and improve glucose and lipid
metabolism. The intestinal 'FXR-gut microbiota-TGR5-GLP-1' axis has
a key role in mediating intestinal BA receptor signal transduction
and regulating liver metabolism and homeostasis (51). The binding of BAs to TGR5 may also
activate the cyclic adenosine monophosphate-protein kinase A
signaling pathway and ultimately increase energy metabolism and
oxygen consumption (52). TGR5 is
also involved in immune regulation and inflammation. The high
expression of TGR5 in monocytes and macrophages was indicated to
decrease the phagocytic activity of these cells and inhibit the
production of numerous proinflammatory cytokines induced by
lipopolysaccharide, such as TNF-α, IL-1, IL-6 and IL-8 (53). Most studies point to TGR5-dependent
immunosuppression partly due to the suppression of the Toll-like
receptor 4/NF-κB pathway (49).
Since these inflammatory signals are closely related to HCC, the
downregulation of TGR5 may be an important factor in the
progression of HCC. A retrospective study indicated that activation
of α7-nicotinic acetylcholine receptor in smoking patients with HCC
promoted HCC metastasis and recurrence by regulating the JAK/STAT3
axis and TGR5 is down-regulated in this process (54). The abnormality of TGR5 was also
indicated to be related to HCC. Another retrospective analysis
suggested that hypermethylation of the TGR5 promoter occurred
significantly more frequently in patients with HCC (48.13%) than in
those with chronic hepatitis B (13.64%) and healthy controls
(4.44%) (55). However, there
remains a lack of in vivo and in vitro evidence on
the direct link between TGR5 and HCC. Revealing the subtle role of
TGR5 in the development of HCC may be a promising direction in the
future.
BA-mediated inflammation and injury in
hepatocytes
BAs mediate a variety of signals that lead to
inflammation and hepatocyte injury. Key factors in these pathways
include IL-6, STAT3, NF-κB, reactive oxygen species (ROS), MAF bZIP
transcription factor G (MAFG), Yes-associated protein (YAP) and
PI3K class I isoforms (p110γ).
BAs may directly damage the plasma membrane and
cause activation of protein kinase C, which activates the p38 MAPK
pathway, leading to the activation of p53 and NF-κB. When this
activation is increased, the expression of several inflammatory
factors, such as IL-6, is enhanced, ultimately leading to increased
apoptosis and inflammation (45).
Data from experiments investigating DEN-elicited-CA-induced tumors
in mice suggest that BAs may promote liver tumors by increasing
inflammatory signaling, ER stress and possibly the selective
survival of tumor-initiating stem cells (38). Apoptotic cells, as a result of BAs,
may trigger inflammation. IL-6 also activates the signal sensor and
activator of the JAK-STAT3 pathway, leading to reduced apoptosis
and progression of HCC (56).
Another study suggested that the expression level of STAT3 was
positively associated with chemoresistance of HCC cells. G-CDCA is
able to stimulate the phosphorylation of STAT3 at the Ser727 site
and mediate pSer727-STAT3 protein translocation and aggregation in
the nucleus, which is important for cell survival (57). The study suggested that G-CDCA may
activate STAT3 by phosphorylation at the Ser727 site via the
MAPK-ERK1/2 pathway, which may contribute to the progression and
chemoresistance of human liver cancer (57). Membrane perturbation by BAs may
also activate phospholipase A2, resulting in the release of
arachidonic acid from the cell membrane via cyclooxygenase and
lipoxygenase, ultimately leading to increased levels of ROS in
hepatocytes (45). ROS are
substances that jointly act on these several pathways to produce
their final effects. ROS may also directly activate NF-κB in a
feedback manner, inducing direct DNA damage in cells and the
occurrence of HCC (58).
It has been experimentally evidenced that MAFG is
induced in human HCC and its upregulation correlates with
unfavorable prognosis in HCC. It was demonstrated that LCA, through
activation of activating protein-1, NF-κB and E-box, induce MAFG
expression, and all these enhancer elements are present in the
human MAFG promoter. S-adenosylmethionine and UDCA have
complementary roles to reduce LCA-mediated changes in the
expression and DNA-binding activity of transcription factors that
bind to these elements (59).
There are also experimental results demonstrating
that BA is an upstream regulator of the Hippo pathway and its
target YAP has been identified as a key driver of liver growth and
carcinogenesis (60,61). BAs function as a tumor promoter by
driving YAP activation and the ability of BAs to activate YAP
depends on the concentration. Normal physiological or modestly
elevated BA concentrations do not lead to YAP activation; however,
chronically elevated pathological concentrations of BAs, which are
commonly seen in cholestatic patients, may activate YAP and promote
carcinogenesis (62,63).
Another study indicated that p110γ is activated by
hydrophobic, but not hydrophilic BAs. BA-induced hepatocyte
apoptosis is partly mediated via a PI3K p110γ-dependent signaling
pathway (64).
Secondary BA-induced damage to other
cells in the liver
Liver sinusoidal endothelial cells (LSECs)-natural
killer T (NKT) cells: Primary BAs (β-MCA, CDCA) may increase C-X-C
motif chemokine ligand (CXCL)16 expression, whereas secondary BAs
(ω-MCA, LCA) had the opposite effect. C-X-C motif chemokine
receptor type 6 forms the lining of liver capillaries and the first
barrier to blood from the intestine entering the liver, and its
expression on LSECs may regulate NKT cell accumulation (65). The increase of NKT cells is
beneficial to the protective effect on the liver. Thus, when NKT
cells induced by LSECs decrease, HCC progresses. In non-neoplastic
liver tissues from patients with primary liver cancer, primary BA
CDCA levels were correlated with CXCL16 expression, whereas an
inverse correlation was observed with secondary BA G-LCA (65). This suggests that the finding may
also apply to humans.
Hepatic stellate cells (HSCs): Blocking DCA
production or reducing DCA-producing gut microbes has been
indicated to prevent liver cancer development in obese mice.
Relevant studies also suggested that enterohepatic circulation of
DCA causes a related senescence-associated secretory phenotype
(SASP) in HSCs (DCA would cause DNA damage through the generation
of ROS, the key trigger of SASP), which in turn secretes various
inflammatory and tumor-promoting factors in the liver to promote
HCC development in mice after exposure to chemical carcinogens
(66,67). Furthermore, DCA-induced senescent
HSCs may also contribute to at least certain aspects of
obesity-associated HCC development via SASP in humans (68,69)
(Fig. 5).
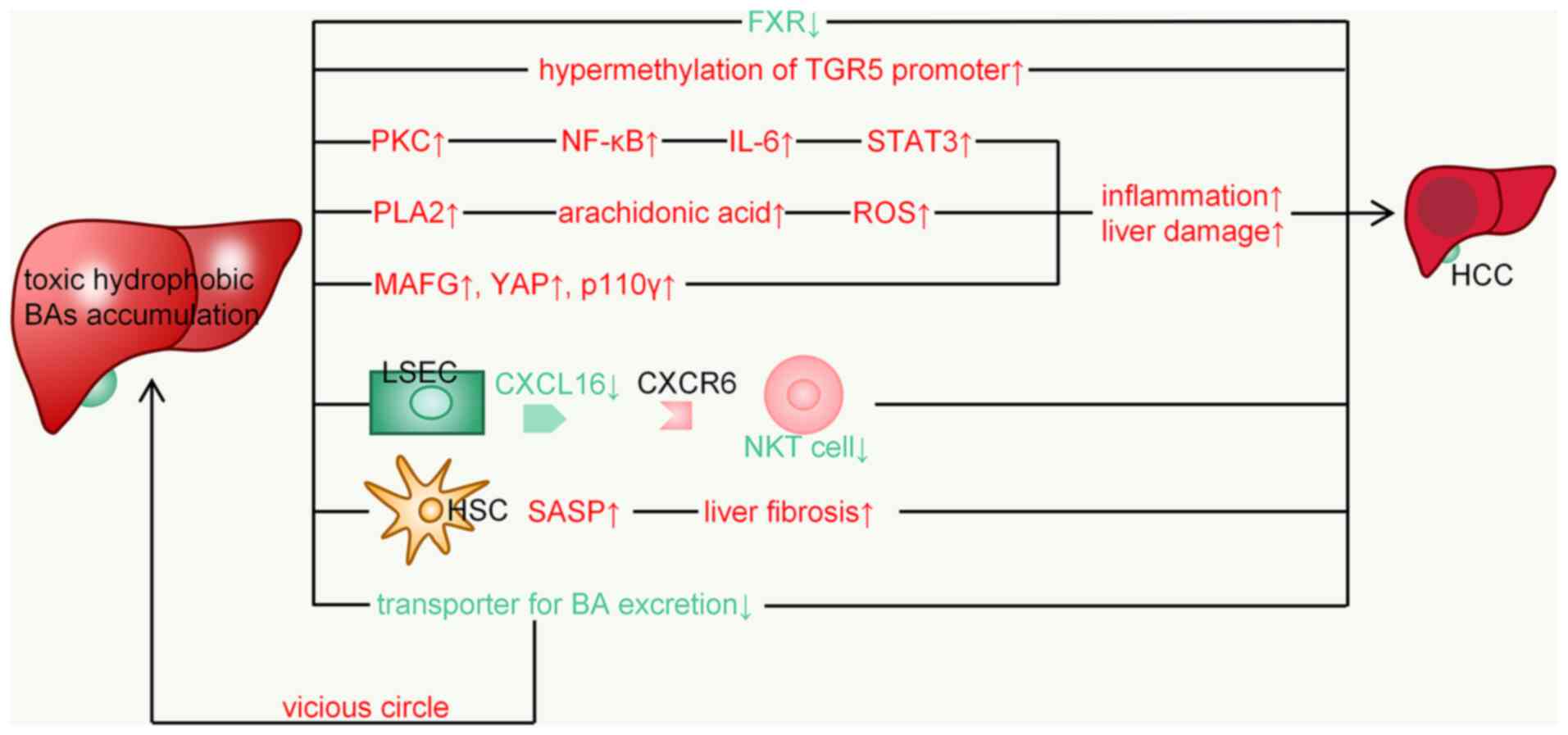 | Figure 5Mechanisms involved in BA-mediated
hepatocarcinogenesis. BA, bile acid; HCC, hepatocellular carcinoma;
FXR, FXR, farnesoid X receptor; TGR5, Takeda G protein-coupled
receptor 5; ROS, reactive oxygen species; MAFG, MAF bZIP
transcription factor G; YAP, Yes-associated protein; p110γ, PI3K
class I isoforms γ; PKC, protein kinase C; LSEC, liver sinusoidal
endothelial cell; CXCR, C-X-C motif chemokine receptor type; HSC,
hepatic stellate cell; NKT, natural killer T; SASP,
senescence-associated secretory phenotype. |
Emerging strategies for the treatment of
HCC utilizing BAs Targeting FXR: Obeticholic acid (OCA)
The semi-synthetic BA analogue
6α-ethyl-chenodeoxycholic acid, more commonly known as OCA, was
developed as the first FXR agonist to be used in humans (70). A study investigated the effect of
OCA on a NASH-associated HCC animal model induced by
diethylnitrosamine and a high-fat choline-deficient diet. The
results suggested that FXR activation by OCA is able to alleviate
the progression of NASH-associated HCC by regulating the
SOCS3/JAK2/STAT3 signaling axis (71). Small heterodimer partner, caspase-3
and p53 were upregulated in this process. Sirtuin-1, a key
regulator of FXR that controls liver regenerative response, was
also elevated after OCA treatment (71). These findings highlight the
potential role of FXR agonists in the effective treatment of
NASH-induced HCC. It is worth noting that OCA does not appear to
have a simple positive therapeutic effect on HCC, as two studies
have obtained contradictory results. An in vitro study
indicated that OCA suppresses HCC cell proliferation and metastasis
by inhibiting the IL-6/STAT3 signaling pathway, while another study
established that OCA promoted HCC cell proliferation in
vitro and xenograft tumor growth in vivo (29,59,72).
The long-term safety of OCA also requires further evaluation, as
the continuous activation of FXR may significantly change the
body's energy metabolism. More patients with NAFLD/NASH for
clinical trials should also be selected, thereby clarifying the
applicable criteria for OCA. The modification of FXR itself may
also affect the therapeutic effect. Activated HSCs may mediate
hepatic fibrosis. It was reported that activated HSCs have a
limited response to OCA and other FXR agonists due to enhanced FXR
SUMOylation (73). Therefore,
SUMOylation inhibitors rescue FXR signaling, thereby increasing the
efficacy of OCA against HSC activation and fibrosis (73). In addition to OCA, other FXR
agonists exhibiting therapeutic effects have now been discovered.
For instance, GW4064 is able to delay the progression of HCC by
blocking the STAT3 pathway through the regulation of the suppressor
of cytokine signaling 3 (70).
WAY-362450, which reduces inflammation, and INT-767 (a dual FXR and
TGR5 agonist), which has lipid-lowering effects, are also being
tested in animal experiments (74).
OCA is still the best and most important FXR agonist
for treatment. There may be a scope modify OCA to improve its
efficacy. An innovative idea is to prepare OCA as nanoparticles,
resulting in a stronger agonistic effect on FXR. Studies have
indicated that manipulation of FXR by this nanoapproach
significantly improves antitumor immune responses in murine HCC
(75). This approach undoubtedly
markedly increases the efficiency compared with oral
administration. Therefore, the improvement of OCA dosage and
administration route is a direction worth pursuing in the future.
In addition, the rise of nanotechnology will also provide an
incentive to develop novel FXR agonists. Perhaps, the replacement
of OCA as the main substance in nanoparticles with novel FXR
agonists may yield even more surprising results. Exosomes also
appear to be a better way to agonize FXR. Studies have indicated
that Lactobacillus rhamnosus GG-derived exosome-like
nanoparticles may protect against alcohol-associated liver disease
through regulation of the FXR signal in mice (76). Perhaps in the future, BAs may be
used as components of exosomes to agonize FXR with greater
precision. Alternatively, the related genes of FXR may be used as
components of exosomes to better delay the progression of HCC.
Targeting BA transporters
Targeting specific sites in the enterohepatic
circulation for regulation also appears to be a viable direction
for the treatment of HCC. Inhibition of ASBT may reduce intestinal
reabsorption of BAs and, at the same time, increase cholesterol
catabolism and BA synthesis in the liver (77). Thus, ASBT inhibitors (e.g., SC-435
and 264W94) improve lipid metabolism in obese patients and perhaps
also have efficacy against HCC due to NAFLD/NASH (74). BA sequestrants (e.g.,
cholestyramine, colesevelam), which act similarly to ASBT
inhibitors, may also reduce lipids by impairing intestinal
reabsorption of BAs, but their effects are more limited (74,77).
In addition, studies have demonstrated that DCA has a dual effect
in HCC cells and is dependent on the expression of the BA
transporter NTCP. DCA may induce apoptosis in NTCP-positive HCC
cells, particularly under hypoxic conditions, while in
NTCP-negative HCC cells, DCA markedly decreased aggressive cellular
behaviors (78). Thus, if it were
possible to examine NTCP expression and the apoptotic signaling
cascade by immunoblot analysis, hydrophobic BAs may even be a
suitable choice for the treatment of NTCP-positive HCC.
Currently, no drugs targeting BA transporters have
been approved for clinical use in patients with HCC. Despite the
ability of ASBT inhibitors to ameliorate metabolic disorders in
patients, the pathogenesis of HCC is complex. The conditions of
ASBT inhibitor application must be considered due to their
potential to have vastly different treatment outcomes for patients
with NAFLD-related HCC and those with non-NAFLD-related HCC. It is
also worth noting that blocking any site in the enterohepatic
circulation has the potential to create a disorder of BA
metabolism. Therefore, the therapeutic effects and adverse effects
must be compared and weighed when developing related drugs. Drugs
with fewer side effects, such as diarrhea and abdominal pain, would
have greater advantages on the basis of guaranteeing therapeutic
efficacy (79).
Hydrophilic BA with therapeutic
effects
UDCA. UDCA may inhibit cholestasis and has a
protective effect on CLDs (80).
T-UDCA has been indicated to exert its cytoprotective activity by
reducing ER stress and preventing apoptosis. The related mechanisms
are dependent on inhibition of the translocation of pro-apoptotic
Bax from cytosol to mitochondria, inhibition of cytochrome c
release and subsequent suppression of mitochondrial apoptosis and
reduction of the expression of cyclin D1 (81,82).
In addition, UDCA has been indicated to interfere with the
E2F-1/Mdm-2/p53 apoptotic pathway, resulting in subsequent nuclear
translocation of the BA-receptor complex and reduction of apoptosis
(81,83). UDC-dihydroartemisinin (DHA), which
is composed of a mixture of UDCA and DHA, has an inhibitory effect
on HepG2 and Huh-7 cells (84). In
conclusion, numerous studies suggest that the application of UDCA
is an effective strategy for the management of advanced
hepatobiliary diseases in the future. Based on the
anti-inflammatory, antioxidant and cytoprotective activities, UDCA
may be useful to improve treatments of advanced liver diseases,
notably in combination with other drugs such as sorafenib, to
enhance the therapeutic efficacy of targeting drugs for HCC
(49,85,86).
Furthermore, based on UDCA, monoclonal antibodies may be designed
at the key sites of these inflammatory signaling pathways to
achieve the purpose of targeted therapy. Therefore, unraveling the
signaling pathways underlying the therapeutic effects of UDCA may
provide a more definitive direction for the doses and modalities
administered, aiming to improve therapeutic outcomes for
patients.
Immunotherapy: Possible utility of
BAs
BAs have been indicated to have an immunotherapeutic
role in a variety of gastrointestinal and biliary diseases.
Immunotherapy for HCC is a more emerging strategy. At present, the
commonly used immunotherapy drugs for HCC are antiangiogenic
tyrosine kinase inhibitors (such as sorafenib), programmed death
ligand 1 (PDL1) blockade with atezolizumab and VEGF blockade with
bevacizumab (87). The question
arises whether BAs and immunotherapy for HCC have a link. As
mentioned above, primary BAs may increase hepatic NKT-cell
accumulation by upregulating CXCL16. However, abundant expression
of receptors for primary BAs across the gastrointestinal tract
overwhelms the possibility of using agonists against these
receptors for HCC control. Therefore, one study prepared an
OCA-nanoemulsion (OCA-NE) and injected it into mice. The results
suggested that OCA-NE significantly suppressed hepatic tumor growth
in a murine orthotopic H22 tumor model; furthermore, OCA-NE led to
the increase of CXCL16, IFN-γ and the number of NKT cells (88). The study made good use of the
intrinsic property of LSECs in capturing circulating nanoparticles
and a large amount of injected OCA-NE accumulated in LSECs. This
strategy for precise manipulation of LSECs should be extended. For
instance, it may be possible to design a nanoparticle of a DCA
analogue for targeted manipulation of HSCs and blocking SASP
signals inside these cells. The feasibility of this remains to be
verified by further experiments.
Immunologic agents that target BA receptors will
also be an important direction for treatments in the future. In
addition to FXR, TGR5 is also an important receptor for BAs.
Studies have indicated that nanoparticles prepared from 5β-CA may
act as antagonists of TGR5, thereby exerting a role in recruiting
immune cells and suppressing HCC (75). Dual FXR/TGR5 agonist INT-767 was
indicated to delay HCC progression and improve liver function in
mice (89). Previously, it was
mentioned that UDCA is a therapeutic BA widely used in clinics. It
may be possible to improve UDCA to prepare specific FXR
agonist/TGR5 antagonist, which is an attractive prospect. In
addition, another study suggested that UDCA may enhance anti-tumor
immunity by promoting the degradation of TGF-β (90). TGF-β is essential for tumor immune
evasion. It is also due to its effects that anti-programmed death 1
(PD1) or anti-PDL1 treatments alone do not improve the
immunosuppressive tumor microenvironment (90). UDCA is a potential TGF-β inhibitor,
which outperforms existing developed TGF-β blocking antibodies in
terms of both efficacy and safety (90). UDCA and anti-PD1/anti-PDL1
combination will also be a direction to improve the efficacy of
immune checkpoint inhibitor therapy. Combination therapy with
anti-PD1 or anti-PDL1 and UDCA may have increased efficacy in
patients with HCC.
Other emerging BA-based therapeutic
approaches
Functionalized gold nanoparticles (AuNPs) have been
widely applied due to their good biocompatibility and long drug
half-life. In one study, the researchers synthesized AuNPs capped
with ligands that possess polyethylene glycol (PEG) and LCA linked
by carboxyl groups (AuNP@MPA-PEG-LCA). The results indicated that
AuNP@MPA-PEG-LCA was more effective in promoting programmed cell
death of HCC cells due to its better cell selectivity and the
related mechanism was the activation of ROS and mediated
mitochondrial dysfunction and apoptosis (91).
Probiotics are emerging viable treatments for HCC.
Probiotics may affect BA metabolism through the modulation of the
gut microbiota. Probiotics modestly regulate the intestinal FXR
pathway to promote liver regeneration by affecting the secretion of
downstream FGF15 (92). A study
indicated that VSL#3 probiotics promote ileal BA deconjugation with
subsequent fecal BA excretion and induce hepatic BA neosynthesis
via the downregulation of the gut-liver FXR-FGF15 axis (93). VSL#3 increases the excretion of BAs
in feces, with distinct alterations in the composition of the fecal
microbiota in mice (93,94). Administration of VSL#3 for 21 days
resulted in a significantly higher abundance of Firmicutes
(51.47%) and Actinobacteria (3.31%) at the expense of
Bacteroidetes (44.22%) and Proteobacteria (1%)
(93). These findings suggest the
possibility that probiotics may be used to treat HCC by affecting
the body's BA metabolism.
4. Conclusions
The subtle relationship between BAs and HCC is
gradually being explored. FXR signaling is the most important
pathway through which BAs mediate HCC development. OCA and several
other novel FXR agonists have demonstrated promising therapeutic
effects against metabolic liver diseases and even HCC (95). In addition to FXR, BA-mediated HCC
development involves TGR5 and multiple inflammatory signals, which
implicates BAs in the immunotherapeutic process of HCC. The
hydrophilic BA UDCA also exhibits therapeutic effects on HCC by
downregulating inflammatory signaling. In addition, targeting BA
transporters, such as ASBT inhibitors, also appears to have
beneficial effects on HCC, but their efficacy requires further
experimental validation. In the future, a deeper understanding of
the mechanisms by which BAs mediate HCC is required in order to
provide further clinical treatments for HCC and to exploit the
therapeutic potential of BAs.
Availability of data and materials
Data sharing not applicable to this article, as no
datasets were generated or analyzed during the current study.
Authors' contributions
WL and SG drafted the manuscript, performed the
selection and organization of the literature and prepared the
figures. BW, YZ, JWZ, MW, JFZ and LS revised the manuscript. BC
carried out the design of this review and revised the manuscript.
All authors contributed to this manuscript and read and approved
the final manuscript. Data authentication is not applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Acknowledgments
Not applicable.
Funding
This work was supported by a grant from the Natural Science
Foundation of Guangxi (grant no. 2021GXNSFAA325001) and a grant
from the Shenyang Science and Technology Plan Fund Project (grant
no. 20-205-4-094).
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
FXR
|
farnesoid X receptor
|
|
UDCA
|
ursodeoxycholic acid
|
|
NAFLD
|
non-alcoholic fatty liver disease
|
|
NASH
|
nonalcoholic steatohepatitis
|
|
BAs
|
bile acids
|
|
CA
|
cholic acid
|
|
CDCA
|
chenodeoxycholic acid
|
|
DCA
|
deoxycholic acid
|
|
LCA
|
lithocholic acid
|
|
MCA
|
muricholic acid
|
|
ER
|
endoplasmic reticulum
|
|
CYP
|
cytochrome P450
|
|
HSD3B7
|
3β-hydroxy-5-C27-steroid
dehydrogenase
|
|
C4
|
7α-hydroxy-4-cholesten-3-one
|
|
AKR1D1
|
aldo-keto reductase family 1 member
D1
|
|
THCA
|
3α,7α,12α-trihydroxy-5β cholestanoic
acid
|
|
DHCA
|
3α,7α-dihydroxy-5β cholestanoic
acid
|
|
BACS
|
BA-Co-A synthase
|
|
VLCS
|
very long-chain Co-A synthase
|
|
BAAT
|
bile acid-CoA, amino acid
N-acyltransferase
|
|
BSH
|
bile acid hydrolase
|
|
BSEP
|
bile salt export pump
|
|
MRP2
|
multidrug resistance-associated
protein 2
|
|
ASBT
|
apical sodium-dependent bile acid
transporter
|
|
IBABP
|
intestinal bile acid binding
protein
|
|
OST
|
organic solute transporter
|
|
NTCP
|
sodium-taurocholate co-transporting
polypeptide
|
|
OATP
|
organic anion transporting
polypeptide
|
|
TGR5
|
Takeda G protein-coupled receptor
5
|
|
DEN
|
diethylnitrosamine
|
|
NF-κB
|
nuclear factor kappa-B
|
|
FGF
|
fibroblast growth factor
|
|
FGFR4
|
fibroblast growth factor receptor
4
|
|
SOX18
|
SRY-related high-mobility group box
18
|
|
EMT
|
epithelial to mesenchymal
transition
|
|
SOCS3
|
suppressor of cytokine signaling
3
|
|
NDRG2
|
N-myc downstream-regulated gene 2
|
|
miR-122
|
microRNA-122
|
|
GLP-1
|
glucagon-like peptide 1
|
|
α7-nAChR
|
α7-nicotinic acetylcholine
receptor
|
|
ROS
|
reactive oxygen species
|
|
MAFG
|
MAF bZIP transcription factor G
|
|
YAP
|
Yes-associated protein
|
|
p110γ
|
PI3K Class I isoforms γ
|
|
PKC
|
protein kinase C
|
|
COX
|
cyclooxygenase
|
|
LSECs
|
liver sinusoidal endothelial
cells
|
|
CXCR
|
C-X-C motif chemokine receptor
type
|
|
HSC
|
hepatic stellate cell
|
|
SASP
|
senescence-associated secretory
phenotype
|
|
OCA
|
obeticholic acid
|
|
DHA
|
dihydroartemisinin
|
|
AuNPs
|
gold nanoparticles
|
|
PEG
|
polyethylene glycol
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer. J Clin. 71:209–249. 2021.
|
|
2
|
Yang JD, Hainaut P, Gores GJ, Amadou A,
Plymoth A and Roberts LR: A global view of hepatocellular
carcinoma: Trends, risk, prevention and management. Nat Rev
Gastroenterol Hepatol. 16:589–604. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Foerster F, Gairing SJ, Müller L and Galle
PR: NAFLD-driven HCC: Safety and efficacy of current and emerging
treatment options. J Hepatol. 76:446–457. 2022. View Article : Google Scholar
|
|
4
|
Llovet JM, Kelley RK, Villanueva A, Singal
AG, Pikarsky E, Roayaie S, Lencioni R, Koike K, Zucman-Rossi J and
Finn RS: Hepatocellular carcinoma. Nat Rev Dis Primers. 7:62021.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Liu Y, Chen K, Li F, Gu Z, Liu Q, He L,
Shao T, Song Q, Zhu F, Zhang L, et al: Probiotic Lactobacillus
rhamnosus GG prevents liver fibrosis through inhibiting hepatic
bile acid synthesis and enhancing bile acid excretion in mice.
Hepatology. 71:2050–2066. 2020. View Article : Google Scholar
|
|
6
|
Li J and Dawson PA: Animal models to study
bile acid metabolism. Biochim Biophys Acta Mol Basis Dis.
1865:895–911. 2019. View Article : Google Scholar
|
|
7
|
Di Ciaula A, Garruti G, Lunardi Baccetto
R, Molina-Molina E, Bonfrate L, Wang DQ and Portincasa P: Bile acid
physiology. Ann Hepatol. 16(Suppl 1): s4–s14. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shulpekova Y, Shirokova E, Zharkova M,
Tkachenko P, Tikhonov I, Stepanov A, Sinitsyna A, Izotov A, Butkova
T, Shulpekova N, et al: A recent ten-year perspective: Bile acid
metabolism and signaling. Molecules. 27:19832022. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chiang JYL and Ferrell JM: Bile acid
metabolism in liver pathobiology. Gene Expr. 18:71–87. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wahlström A, Sayin SI, Marschall HU and
Bäckhed F: Intestinal crosstalk between bile acids and microbiota
and its impact on host metabolism. Cell Metab. 24:41–50. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhang B, Kuipers F, de Boer JF and
Kuivenhoven JA: Modulation of bile acid metabolism to improve
plasma lipid and lipoprotein profiles. J Clin Med. 11:42021.
View Article : Google Scholar
|
|
12
|
Perino A, Demagny H, Velazquez-Villegas L
and Schoonjans K: Molecular physiology of bile acid signaling in
health, disease, and aging. Physiol Rev. 101:683–731. 2021.
View Article : Google Scholar
|
|
13
|
Sohail MI, Dönmez-Cakil Y, Szöllősi D,
Stockner T and Chiba P: The bile salt export pump: Molecular
structure, study models and small-molecule drugs for the treatment
of inherited BSEP deficiencies. Int J Mol Sci. 22:7842021.
View Article : Google Scholar :
|
|
14
|
Jetter A and Kullak-Ublick GA: Pharmacol
Res. 154:1042342020. View Article : Google Scholar
|
|
15
|
Köck K, Ferslew BC, Netterberg I, Yang K,
Urban TJ, Swaan PW, Stewart PW and Brouwer KL: Risk factors for
development of cholestatic drug-induced liver injury: Inhibition of
hepatic basolateral bile acid transporters multidrug
resistance-associated proteins 3-4. Drug Metab Dispos. 42:665–674.
2014. View Article : Google Scholar
|
|
16
|
Xiao L and Pan G: An important intestinal
transporter that regulates the enterohepatic circulation of bile
acids and cholesterol homeostasis: The apical sodium-dependent bile
acid transporter (SLC10A2/ASBT). Clin Res Hepatol Gastroenterol.
41:509–515. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Deng F and Bae YH: Bile acid
transporter-mediated oral drug delivery. J Control Release.
327:100–116. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Suga T, Yamaguchi H, Ogura J and Mano N:
Characterization of conjugated and unconjugated bile acid transport
via human organic solute transporter α/β. Biochim Biophys Acta
Biomembr. 1861:1023–1029. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Vaz FM and Ferdinandusse S: Bile acid
analysis in human disorders of bile acid biosynthesis. Mol Aspects
Med. 56:10–24. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Trauner M, Fuchs CD, Halilbasic E and
Paumgartner G: New therapeutic concepts in bile acid transport and
signaling for management of cholestasis. Hepatology. 65:1393–1404.
2017. View Article : Google Scholar
|
|
21
|
Li T and Chiang JY: Bile acid signaling in
metabolic disease and drug therapy. Pharmacol Rev. 66:948–983.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Daruich A, Picard E, Boatright JH and
Behar-Cohen F: Review: The bile acids ursoand tauroursodeoxycholic
acid as neuroprotective therapies in retinal disease. Mol Vis.
25:610–624. 2019.
|
|
23
|
Sato R: Recent advances in regulating
cholesterol and bile acid metabolism. Biosci Biotechnol Biochem.
84:2185–2192. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ko CW, Qu J, Black DD and Tso P:
Regulation of intestinal lipid metabolism: Current concepts and
relevance to disease. Nat Rev Gastroenterol Hepatol. 17:169–183.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Blanchet M and Brunel JM: Bile acid
derivatives: From old molecules to a new potent therapeutic use: An
overview. Curr Med Chem. 25:3613–3636. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Forman BM, Goode E, Chen J, Oro AE,
Bradley DJ, Perlmann T, Noonan DJ, Burka LT, McMorris T, Lamph WW,
et al: Identification of a nuclear receptor that is activated by
farnesol metabolites. Cell. 81:687–693. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Massafra V, Pellicciari R, Gioiello A and
van Mil SWC: Progress and challenges of selective farnesoid X
receptor modulation. Pharmacol Ther. 191:162–177. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schubert K, Olde Damink SWM, von Bergen M
and Schaap FG: Interactions between bile salts, gut microbiota, and
hepatic innate immunity. Immunol Rev. 279:23–35. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sun L, Cai J and Gonzalez FJ: The role of
farnesoid X receptor in metabolic diseases, and gastrointestinal
and liver cancer. Nat Rev Gastroenterol Hepatol. 18:335–347. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Duboc H, Taché Y and Hofmann AF: The bile
acid TGR5 membrane receptor: From basic research to clinical
application. Dig Liver Dis. 46:302–312. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ticho AL, Malhotra P, Dudeja PK, Gill RK
and Alrefai WA: Bile acid receptors and gastrointestinal functions.
Liver Res. 3:31–39. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Portincasa P, Di Ciaula A, Garruti G,
Vacca M, De Angelis M and Wang DQ: Bile acids and GPBAR-1: Dynamic
interaction involving genes, environment and gut microbiome.
Nutrients. 12:37092020. View Article : Google Scholar :
|
|
33
|
Wang R, Sheps JA and Ling V: ABC
transporters, bile acids, and inflammatory stress in liver cancer.
Curr Pharm Biotechnol. 12:636–646. 2011. View Article : Google Scholar
|
|
34
|
Wang C, Yang M, Zhao J, Li X, Xiao X,
Zhang Y, Jin X and Liao M: Bile salt (glycochenodeoxycholate acid)
induces cell survival and chemoresistance in hepatocellular
carcinoma. J Cell Physiol. 234:10899–10906. 2019. View Article : Google Scholar
|
|
35
|
Wang H, Shang X, Wan X, Xiang X, Mao Q,
Deng G and Wu Y: Increased hepatocellular carcinoma risk in chronic
hepatitis B patients with persistently elevated serum total bile
acid: A retrospective cohort study. Sci Rep. 6:381802016.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Thomas CE, Luu HN, Wang R, Xie G,
Adams-Haduch J, Jin A, Koh WP, Jia W, Behari J and Yuan JM:
Association between pre-diagnostic serum bile acids and
hepatocellular carcinoma: The singapore Chinese health study.
Cancers (Basel). 13:26482021. View Article : Google Scholar
|
|
37
|
Zhang W, Zhou L, Yin P, Wang J, Lu X, Wang
X, Chen J, Lin X and Xu G: A weighted relative difference
accumulation algorithm for dynamic metabolomics data: Long-term
elevated bile acids are risk factors for hepatocellular carcinoma.
Sci Rep. 5:89842015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Sun L, Beggs K, Borude P, Edwards G,
Bhushan B, Walesky C, Roy N, Manley MW Jr, Gunewardena S, O'Neil M,
et al: Bile acids promote diethylnitrosamine-induced hepatocellular
carcinoma via increased inflammatory signaling. Am J Physiol
Gastrointest Liver Physiol. 311:G91–G104. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Xie G, Wang X, Huang F, Zhao A, Chen W,
Yan J, Zhang Y, Lei S, Ge K, Zheng X, et al: Dysregulated hepatic
bile acids collaboratively promote liver carcinogenesis. Int J
Cancer. 139:1764–1775. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ressom HW, Xiao JF, Tuli L, Varghese RS,
Zhou B, Tsai TH, Ranjbar MR, Zhao Y, Wang J, Di Poto C, et al:
Utilization of metabolomics to identify serum biomarkers for
hepatocellular carcinoma in patients with liver cirrhosis. Anal
Chim Acta. 743:90–100. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Rizzolo D, Buckley K, Kong B, Zhan L, Shen
J, Stofan M, Brinker A, Goedken M, Buckley B and Guo GL: Bile acid
homeostasis in a cholesterol 7α-hydroxylase and sterol
27-hydroxylase double knockout mouse model. Hepatology. 70:389–402.
2019.PubMed/NCBI
|
|
42
|
Huang XF, Zhao WY and Huang WD: FXR and
liver carcinogenesis. Acta Pharmacol Sin. 36:37–43. 2015.
View Article : Google Scholar :
|
|
43
|
Takahashi S, Tanaka N, Fukami T, Xie C,
Yagai T, Kim D, Velenosi TJ, Yan T, Krausz KW, Levi M and Gonzalez
FJ: Role of farnesoid X receptor and bile acids in hepatic tumor
development. Hepatol Commun. 2:1567–1582. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhao Q, Liu F, Cheng Y, Xiao XR, Hu DD,
Tang YM, Bao WM, Yang JH, Jiang T, Hu JP, et al: Celastrol protects
from cholestatic liver injury through modulation of SIRT1-FXR
signaling. Mol Cell Proteomics. 18:520–533. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Jia W, Xie G and Jia W: Bile
acid-microbiota crosstalk in gastrointestinal inflammation and
carcinogenesis. Nat Rev Gastroenterol Hepatol. 15:111–128. 2018.
View Article : Google Scholar
|
|
46
|
Liu X, Zhang X, Ji L, Gu J, Zhou M and
Chen S: Farnesoid X receptor associates with β-catenin and inhibits
its activity in hepatocellular carcinoma. Oncotarget. 6:4226–4238.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Qu A, Jiang C, Cai Y, Kim JH, Tanaka N,
Ward JM, Shah YM and Gonzalez FJ: Role of Myc in hepatocellular
proliferation and hepatocarcinogenesis. J Hepatol. 60:331–338.
2014. View Article : Google Scholar :
|
|
48
|
Chen J, Du F, Dang Y, Li X, Qian M, Feng
W, Qiao C, Fan D, Nie Y, Wu K and Xia L: Fibroblast growth factor
19-mediated up-regulation of SYR-related high-mobility group box 18
promotes hepatocellular carcinoma metastasis by transactivating
fibroblast growth factor receptor 4 and fms-related tyrosine kinase
4. Hepatology. 71:1712–1731. 2020. View Article : Google Scholar
|
|
49
|
Režen T, Rozman D, Kovács T, Kovács P,
Sipos A, Bai P and Mikó E: The role of bile acids in
carcinogenesis. Cell Mol Life Sci. 79:2432022. View Article : Google Scholar
|
|
50
|
van Nierop FS, Scheltema MJ, Eggink HM,
Pols TW, Sonne DP, Knop FK and Soeters MR: Clinical relevance of
the bile acid receptor TGR5 in metabolism. Lancet Diabetes
Endocrinol. 5:224–233. 2017. View Article : Google Scholar
|
|
51
|
Pathak P, Xie C, Nichols RG, Ferrell JM,
Boehme S, Krausz KW, Patterson AD, Gonzalez FJ and Chiang JYL:
Intestine farnesoid X receptor agonist and the gut microbiota
activate G-protein bile acid receptor-1 signaling to improve
metabolism. Hepatology. 68:1574–1588. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Fuchs CD and Trauner M: Role of bile acids
and their receptors in gastrointestinal and hepatic
pathophysiology. Nat Rev Gastroenterol Hepatol. 19:432–450. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Pols TW, Noriega LG, Nomura M, Auwerx J
and Schoonjans K: The bile acid membrane receptor TGR5 as an
emerging target in metabolism and inflammation. J Hepatol.
54:1263–1272. 2011. View Article : Google Scholar
|
|
54
|
Li CL, Lin YK, Chen HA, Huang CY, Huang MT
and Chang YJ: Smoking as an independent risk factor for
hepatocellular carcinoma due to the α7-nachr modulating the
JAK2/STAT3 signaling axis. J Clin Med. 8:13912019. View Article : Google Scholar
|
|
55
|
Han LY, Fan YC, Mu NN, Gao S, Li F, Ji XF,
Dou CY and Wang K: Aberrant DNA methylation of G-protein-coupled
bile acid receptor Gpbar1 (TGR5) is a potential biomarker for
hepatitis B virus associated hepatocellular carcinoma. Int J Med
Sci. 11:164–171. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Xu J, Lin H, Wu G, Zhu M and Li M:
IL-6/STAT3 is a promising therapeutic target for hepatocellular
carcinoma. Front Oncol. 11:7609712021. View Article : Google Scholar :
|
|
57
|
Wang J, Zhou M, Jin X, Li B, Wang C, Zhang
Q, Liao M, Hu X and Yang M: Glycochenodeoxycholate induces cell
survival and chemoresistance via phosphorylation of STAT3 at Ser727
site in HCC. J Cell Physiol. 235:2557–2568. 2020. View Article : Google Scholar
|
|
58
|
Zhang WJ, Chen SJ, Zhou SC, Wu SZ and Wang
H: Inflammasomes and fibrosis. Front Immunol. 12:6431492021.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Liu T, Yang H, Fan W, Tu J, Li TWH, Wang
J, Shen H, Yang J, Xiong T, Steggerda J, et al: Mechanisms of MAFG
dysregulation in cholestatic liver injury and development of liver
cancer. Gastroenterology. 155:557–571.e14. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Cai J, Zhang N, Zheng Y, de Wilde RF,
Maitra A and Pan D: The Hippo signaling pathway restricts the
oncogenic potential of an intestinal regeneration program. Genes
Dev. 24:2383–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Zhang S and Zhou D: Role of the
transcriptional coactivators YAP/TAZ in liver cancer. Curr Opin
Cell Biol. 61:64–71. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Anakk S, Bhosale M, Schmidt VA, Johnson
RL, Finegold MJ and Moore DD: Bile acids activate YAP to promote
liver carcinogenesis. Cell Rep. 5:1060–1069. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Russell JO and Camargo FD: Hippo
signalling in the liver: Role in development, regeneration and
disease. Nat Rev Gastroenterol Hepatol. 19:297–312. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Hohenester S, Gates A, Wimmer R, Beuers U,
Anwer MS, Rust C and Webster CR: Phosphatidylinositol-3-kinase
p110γ contributes to bile salt-induced apoptosis in primary rat
hepatocytes and human hepatoma cells. J Hepatol. 53:918–926. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ma C, Han M, Heinrich B, Fu Q, Zhang Q,
Sandhu M, Agdashian D, Terabe M, Berzofsky JA, Fako V, et al: Gut
microbiome-mediated bile acid metabolism regulates liver cancer via
NKT cells. Science. 360:eaan59312018. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Friedman SL: Hepatic stellate cells:
Protean, multifunctional, and enigmatic cells of the liver. Physiol
Rev. 88:125–172. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Matsuda M and Seki E: Hepatic stellate
cell-macrophage crosstalk in liver fibrosis and carcinogenesis.
Semin Liver Dis. 40:307–320. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Yoshimoto S, Loo TM, Atarashi K, Kanda H,
Sato S, Oyadomari S, Iwakura Y, Oshima K, Morita H, Hattori M, et
al: Obesity-induced gut microbial metabolite promotes liver cancer
through senescence secretome. Nature. 499:97–101. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Ohtani N: The roles and mechanisms of
senescence-associated secretory phenotype (SASP): Can it be
controlled by senolysis? Inflamm Regen. 42:112022. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Orabi D, Berger NA and Brown JM: Abnormal
metabolism in the progression of nonalcoholic fatty liver disease
to hepatocellular carcinoma: Mechanistic insights to
chemoprevention. Cancers (Basel). 13:34732021. View Article : Google Scholar
|
|
71
|
Attia YM, Tawfiq RA, Gibriel AA, Ali AA,
Kassem DH, Hammam OA and Elmazar MM: Activation of FXR modulates
SOCS3/Jak2/STAT3 signaling axis in a NASH-dependent hepatocellular
carcinoma animal model. Biochem Pharmacol. 186:1144972021.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Attia YM, Tawfiq RA, Ali AA and Elmazar
MM: The FXR agonist, obeticholic acid, suppresses HCC proliferation
& metastasis: Role of IL-6/STAT3 signalling pathway. Sci Rep.
7:125022017. View Article : Google Scholar :
|
|
73
|
Zhou J, Cui S, He Q, Guo Y, Pan X, Zhang
P, Huang N, Ge C, Wang G, Gonzalez FJ, et al: SUMOylation
inhibitors synergize with FXR agonists in combating liver fibrosis.
Nat Commun. 11:2402020. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Chow MD, Lee YH and Guo GL: The role of
bile acids in nonalcoholic fatty liver disease and nonalcoholic
steatohepatitis. Mol Aspects Med. 56:34–44. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Ji G, Si X, Dong S, Xu Y, Li M, Yang B,
Tang Z, Fang X, Huang L, Song W and Chen X: Manipulating liver bile
acid signaling by nanodelivery of bile acid receptor modulators for
liver cancer immunotherapy. Nano Lett. 21:6781–6791. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Jiang M, Li F, Liu Y, Gu Z, Zhang L, Lee
J, He L, Vatsalya V, Zhang HG, Deng Z, et al: Probiotic-derived
nanoparticles inhibit ALD through intestinal miR194 suppression and
subsequent FXR activation. Hepatology. Jun;112022.Epub ahead of
print.
|
|
77
|
van de Peppel IP, Verkade HJ and Jonker
JW: Metabolic consequences of ileal interruption of the
enterohepatic circulation of bile acids. Am J Physiol Gastrointest
Liver Physiol. 319:G619–G625. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Jang ES, Yoon JH, Lee SH, Lee SM, Lee JH,
Yu SJ, Kim YJ, Lee HS and Kim CY: Sodium taurocholate
cotransporting polypeptide mediates dual actions of deoxycholic
acid in human hepatocellular carcinoma cells: Enhanced apoptosis
versus growth stimulation. J Cancer Res Clin Oncol. 140:133–144.
2014. View Article : Google Scholar
|
|
79
|
Yang N, Dong YQ, Jia GX, Fan SM, Li SZ,
Yang SS and Li YB: ASBT(SLC10A2): A promising target for treatment
of diseases and drug discovery. Biomed Pharmacother.
132:1108352020. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Cabrera D, Arab JP and Arrese M: UDCA,
NorUDCA, and TUDCA in liver diseases: A review of their mechanisms
of action and clinical applications. Handb Exp Pharmacol.
256:237–264. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Kusaczuk M: Tauroursodeoxycholate-bile
acid with chaperoning activity: Molecular and cellular effects and
therapeutic perspectives. Cells. 8:14712019. View Article : Google Scholar
|
|
82
|
Castro RE, Solá S, Ma X, Ramalho RM, Kren
BT, Steer CJ and Rodrigues CM: A distinct microarray gene
expression profile in primary rat hepatocytes incubated with
ursodeoxycholic acid. J Hepatol. 42:897–906. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Solá S, Amaral JD, Castro RE, Ramalho RM,
Borralho PM, Kren BT, Tanaka H, Steer CJ and Rodrigues CM: Nuclear
translocation of UDCA by the glucocorticoid receptor is required to
reduce TGF-beta1-induced apoptosis in rat hepatocytes. Hepatology.
42:925–934. 2005. View Article : Google Scholar
|
|
84
|
Huang TE, Deng YN, Hsu JL, Leu WJ,
Marchesi E, Capobianco ML, Marchetti P, Navacchia ML, Guh JH,
Perrone D and Hsu LC: Evaluation of the anticancer activity of a
bile acid-dihydroartemisinin hybrid
ursodeoxycholic-dihydroartemisinin in hepatocellular carcinoma
cells. Front Pharmacol. 11:5990672020. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Goossens JF and Bailly C: Ursodeoxycholic
acid and cancer: From chemoprevention to chemotherapy. Pharmacol
Ther. 203:1073962019. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Lee S, Cho YY, Cho EJ, Yu SJ, Lee JH, Yoon
JH and Kim YJ: Synergistic effect of ursodeoxycholic acid on the
antitumor activity of sorafenib in hepatocellular carcinoma cells
via modulation of STAT3 and ERK. Int J Mol Med. 42:2551–2559.
2018.PubMed/NCBI
|
|
87
|
Sangro B, Sarobe P, Hervás-Stubbs S and
Melero I: Advances in immunotherapy for hepatocellular carcinoma.
Nat Rev Gastroenterol Hepatol. 18:525–543. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Ji G, Ma L, Yao H, Ma S, Si X, Wang Y, Bao
X, Ma L, Chen F, Ma C, et al: Precise delivery of obeticholic acid
via nanoapproach for triggering natural killer T cell-mediated
liver cancer immunotherapy. Acta Pharm Sin B. 10:2171–2182. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Cariello M, Peres C, Zerlotin R, Porru E,
Sabbà C, Roda A and Moschetta A: Long-term administration of
nuclear bile acid receptor FXR agonist prevents spontaneous
hepatocarcinogenesis in Abcb4-/mice. Sci Rep.
7:112032017. View Article : Google Scholar
|
|
90
|
Shen Y, Lu C, Song Z, Qiao C, Wang J, Chen
J, Zhang C, Zeng Z, Ma Z, Chen J, et al: Ursodeoxycholic acid
reduces antitumor immunosuppression by inducing CHIP-mediated TGF-β
degradation. Nat Commun. 13:34192022. View Article : Google Scholar
|
|
91
|
Zhao MX, Cai ZC, Zhu BJ and Zhang ZQ: The
apoptosis effect on liver cancer cells of gold nanoparticles
modified with lithocholic acid. Nanoscale Res Lett. 13:3042018.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Liu T, Song X, Khan S, Li Y, Guo Z, Li C,
Wang S, Dong W, Liu W, Wang B and Cao H: The gut microbiota at the
intersection of bile acids and intestinal carcinogenesis: An old
story, yet mesmerizing. Int J Cancer. 146:1780–1790. 2020.
View Article : Google Scholar
|
|
93
|
Degirolamo C, Rainaldi S, Bovenga F,
Murzilli S and Moschetta A: Microbiota modification with probiotics
induces hepatic bile acid synthesis via downregulation of the
Fxr-Fgf15 axis in mice. Cell Rep. 7:12–18. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Jones ML, Tomaro-Duchesneau C and Prakash
S: The gut microbiome, probiotics, bile acids axis, and human
health. Trends Microbiol. 22:306–308. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Polyzos SA, Kountouras J and Mantzoros CS:
Obeticholic acid for the treatment of nonalcoholic steatohepatitis:
Expectations and concerns. Metabolism. 104:1541442020. View Article : Google Scholar : PubMed/NCBI
|