Introduction
Over the past decade, significant advancements have
been made in the prognosis and management of resected
gastrointestinal stromal tumor (GIST). Risk stratification models
have been developed and are used in routine clinical practice to
provide a prognosis for patients with localized GIST. These models
serve to guide the use of adjuvant imatinib therapy following
curative surgery. The National Institutes of Health (NIH) consensus
criteria used tumor size and number of mitoses per 50 high-power
field (HPF) to stratify patients into four risk cohorts (1). Miettinen and Lasota (2) retrospectively reviewed data from the
Armed Forces Institute of Pathology, comprising the largest
reported series of more than 2000 cases of GIST, to assign specific
risks of relapse based upon size, number of mitoses and anatomic
location. In their study, Joensuu and colleagues (3) suggested an update of the NIH
consensus criteria incorporating anatomic location and presence of
tumor rupture occurring spontaneously or at the time of surgery,
following the establishment of tumor rupture as an independent
adverse risk factor for disease relapse (4).
Imatinib, a small molecule tyrosine kinase inhibitor
of the KIT oncoprotein, is of proven benefit in the adjuvant
treatment of patients with completely resected GIST. In the
randomized phase III ACOSOG Z9001 study evaluating patients with
GIST of at least 3 cm, 1 year of adjuvant imatinib improved
recurrence-free survival (5). More
recently, the SSGXVIII study enrolled 400 high-risk GIST patients
based on the modified NIH consensus criteria (3) and randomized the patients into 3
years vs. 1 year of adjuvant imatinib. Preliminary results
demonstrated that 3 years of adjuvant imatinib significantly
improved 5-year recurrence-free survival (65.6 vs. 47.9%) and
overall survival (OS) (92.0 vs. 81.7%) (6), confirming it as a new standard of
care for such patients.
The rectum is an uncommon primary site for GIST
development, representing <6% of the cases in the largest
reported series (2). Rectal tumors
pose several unique challenges to optimal management. The paucity
of space in the pelvis renders optimal oncologic surgery more
challenging compared to other bowel surgeries and proximity of
these lesions to the anal sphincter also increases the potential
morbidity of any radical surgery. In rectal adenocarcinoma, local
failure is an important factor of first treatment failure and is
associated with significant morbidity, with limited success accrued
from salvage procedures. The employment of multi-modality
peri-operative treatment with chemotherapy and radiotherapy has
resulted in ∼50% reduction of local recurrences, even in the era of
modern surgery with total mesorectal excision (7,8).
In our experience, the local control in rectal GIST
was poor and treatment for this disease subset was associated with
high morbidity. The present study aimed to evaluate the clinical
characteristics of localized, resected rectal GIST in comparison
with GIST of other primary sites, and to determine the clinical
outcomes and challenges to management of this uncommon GIST
location.
Patients and methods
Study approval
This study was approved by the Institutional Review
Board of the National Cancer Singapore (NCCS). The cases with the
diagnosis of GIST seen at NCCS between 2002 and 2011 were
identified through the institutional diagnostic records system.
Diagnoses of GIST were centrally reviewed. Only patients presenting
with localized disease and with no distant metastases, who had
undergone surgical resection were included in this study.
Patient characteristics
Clinical data were obtained from our GIST database,
patient medical charts and electronic medical records. Tumors were
classified according to the site of origin (stomach, small
intestine, colon and rectum). The type and intent of the surgery
was determined for each case based on the medical charts and
operation reports. The surgical margins of primary resection were
defined as follows: R0, microscopically-negative margins; R1,
microscopically-positive margins and R2, gross residual disease.
Tumor pathologic characteristics, including size and mitotic rate,
were recorded. Details of adjuvant or neo-adjuvant treatment were
captured. At the time of relapse, data obtained included nature of
relapse (local vs. distant). The cut-off date for reporting data
was 1 July, 2011. Survival data were determined based on medical
records and cross-referenced against the Singapore Death Registry
for patients still living in Singapore.
Statistical analysis
Comparison of the categorical characteristics by
primary sites were performed using either the Chi-square test or
Fisher’s exact test, as appropriate. The median age at the
diagnosis of rectal GIST was compared against small
intestinal/gastric GIST, using the Mann-Whitney U test.
The overall survival (OS) duration was calculated
from the date of diagnosis to the date of death from any cause.
Relapse-free survival (RFS) duration was calculated from the date
of diagnosis to the date of the first relapse or death. Patients
who did not develop any of these time-to-event endpoints were
censored at the date of the last follow up. The Kaplan-Meier method
was used to estimate survival distribution, while the log-rank test
was used to examine the differences between survival curves. The
tests were two-sided, and P<0.05 was considered to indicate a
statistically significant difference. The analyses were performed
using the SAS® 9.2 software (SAS Institute, Inc., Cary,
NC, USA).
Results
Clinical characteristics
One hundred and twelve consecutive patients with
resected localized GIST were identified based on our records. Nine
patients (8%) had rectal GIST, whereas the remaining patients had
GIST of the stomach (n=63; 56%), small intestine (n=37; 33%) and
colon (n=3; 3%). Median follow up was 46 months for the entire
cohort and 59 months for patients with rectal GIST. Due to the
small patient numbers, patients with colonic GIST were omitted from
further analyses.
The median age of patients with rectal GIST was 58
years (range, 37–69 years; 78% male). These values were not
significantly different from patients with GIST of small intestinal
or gastric origin. Of the patients with complete pathological data,
none with rectal GIST had tumors >10 cm, compared to 40% of
patients with small intestinal/gastric GIST (P=0.044). There were
no significant differences in the mitotic activity or the eventual
risk classification by the original NIH consensus criteria in
rectal and small intestinal/gastric GIST. More than 60% of patients
in each anatomic group were classified as high risk (Table I).
 | Table IClinical characteristics and
distribution of risk factors. |
Table I
Clinical characteristics and
distribution of risk factors.
| Clinical
characteristics | Rectum (n=9) | Small
intestinal/gastric (n=100) | P-value |
|---|
| Median age at
diagnosis, years (range) | 58 (37–69) | 60 (17–88) | 0.422 |
| Gender, no. (%) | | | |
| Female | 2 (22) | 38 (38) | 0.481 |
| Male | 7 (78) | 62 (62) | |
| Tumor size, no.
(%)a | | | |
| ≤2 cm | 0 | 2 (2) | 0.044 |
| >2–≤5 cm | 2 (22) | 18 (19) | |
| >5–≤10 cm | 7 (78) | 38 (39) | |
| >10 cm | 0 | 39 (40) | |
| No. of mitoses per 50
HPF, no. (%)a | | | |
| 0–5 | 2 (22) | 32 (33) | 0.422 |
| 6–10 | 0 | 14 (14) | |
| >10 | 7 (78) | 51 (53) | |
| NIH risk
classification, no. (%)a | | | |
| Very low/low | 0 | 11 (11) | 0.618 |
| Intermediate | 2 (22) | 16 (17) | |
| High | 7 (78) | 70 (72) | |
Local control and morbidity
The 9 patients with localized rectal GIST underwent
curative surgery, of whom 67% received R0 resection. This compares
unfavorably with GIST patients of small intestinal and gastric
origin, of whom 92% of evaluable patients received surgical
resection with microscopically-negative margins (P=0.054). Notably,
of the patients with rectal GIST, peri-operative morbidity was
substantial. Three patients required an abdomino-perineal resection
(APR). Of the remaining 6 patients treated with resection and bowel
anastomosis, 2 patients experienced peri-operative tumor rupture,
and 1 patient developed anastomotic wound breakdown and abscess
formation. Although not statistically significant, 22% of rectal
GIST patients experienced tumor rupture vs. only 5% of evaluable
patients with small intestinal/gastric GIST (P=0.106) (Table II).
| Table IILocal control and morbidity. |
Table II
Local control and morbidity.
| Rectum (n=9) | Small
intestinal/gastric (n=100) | P-value |
|---|
| Resection margins,
no. (%)a | | | |
| Negative | 6 (67) | 86 (91) | 0.054 |
| Positive | 3 (33) | 8 (9) | |
| Tumor rupture, no.
(%)b | | | |
| No | 7 (78) | 93 (95) | 0.106 |
| Yes | 2 (22) | 5 (5) | |
Only 2 patients with rectal GIST (22%) received
adjuvant imatinib, a proportion similar to that observed in
patients with small intestinal and gastric GIST (16 and 30%,
respectively; P=0.291). The relapse rates for rectal, small
intestinal and gastric GIST were 67, 51 and 38% respectively
(P=0.174). Five out of 6 (83%) rectal GIST patients whose disease
relapsed experienced local recurrence as a site of the first
relapse (either local recurrence only or concomitant local and
distant failure). In comparison, only 21% of first relapses in
small intestinal/gastric GIST comprised local failures
(P=0.005).
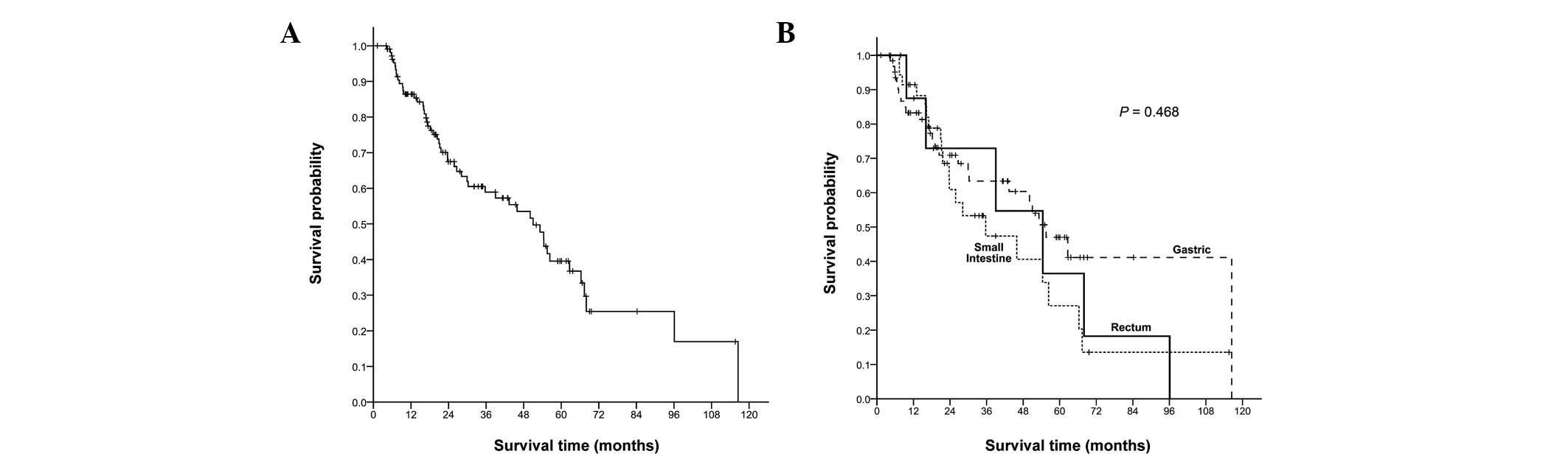
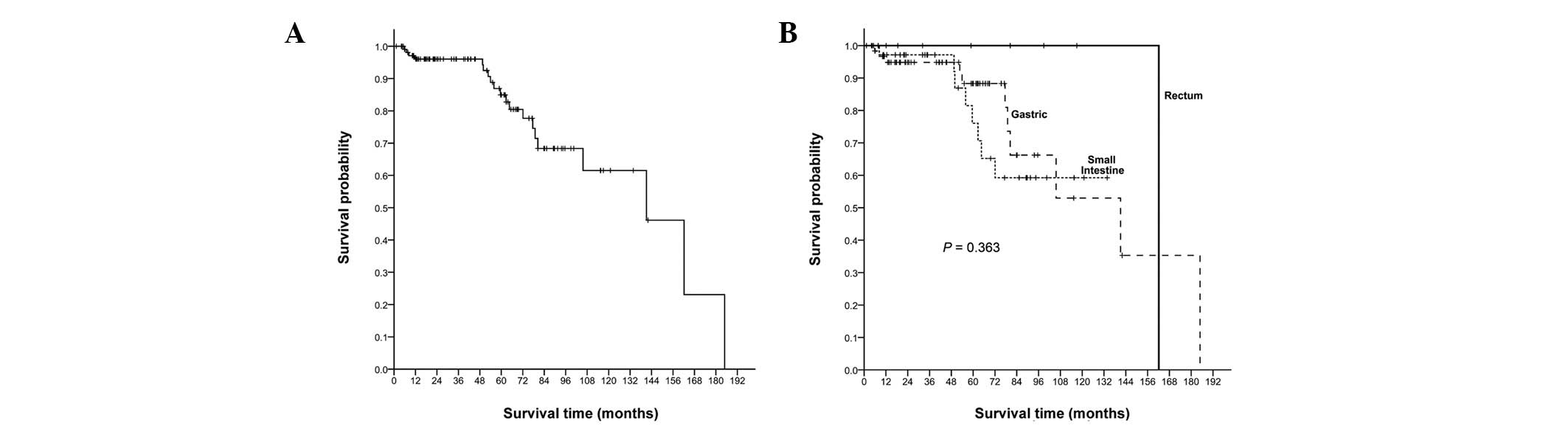
Relapse-free and overall survival
Median OS for the entire study cohort was 141
months, with no statistically significant differences between the
cohorts of patients with rectal (162 months), small intestinal (not
reached) and gastric GIST (141 months) (P= 0.363). Median RFS for
the entire cohort was 51 months, with no statistically significant
difference noted between rectal (54 months), small intestinal (36
months) and gastric GIST (56 months) (P=0.468), as shown in
Figs. 1 and 2.
Discussion
In this study, the rectum was confirmed to be an
uncommon primary site for GIST, representing only 8% of the
patients with resected localized GIST. In comparison with patients
with small intestinal and gastric GIST, there does not seem to be
any unique pattern of gender or age at presentation in rectal GIST.
Notably, rectal tumors in our series were significantly smaller
compared to small intestinal/gastric tumors. This could possibly be
correlated with the propensity for rectal masses to become
symptomatic earlier than tumors in the upper gastrointestinal
tract. The anatomic groups did not differ in terms of the other
major prognostic factor, mitotic rate, possibly accounting for the
lack of differences in NIH criteria risk categories in the
groups.
In this study, the number of patients with resected
localized GIST, who received adjuvant imatinib, was relatively low
(<30% in each anatomic group), in spite of the majority of
patients (<60% in each anatomic group) being at high risk. This
is likely due to the fact that imatinib was only recently approved
for use in this indication. In the landmark adjuvant study
conducted by the ACOSOG group prior to the SSGXVIII study, the
absence of OS benefit was likely to be another contributory factor
(5). Comparing patients regarding
primary GIST locations, no statistically significant difference was
observed in adjuvant imatinib use in rectal GIST and small
intestinal/gastric GIST patients.
Notably, although the overall relapse rates for
patients with rectal GIST was not significantly different from
those with small intestinal/gastric GIST, the patterns of relapse
differed significantly. Of the patients whose disease recurred, 83%
with rectal GIST experienced local failure at the first relapse,
compared to 21% of patients with small intestinal and gastric GIST.
This finding is probably due to the lower rates of R0 surgical
resection for rectal GIST, compared to small intestinal and gastric
GIST, a difference of almost statistically significant difference
(P=0.054). The significant challenges of complete surgical
extirpation in the tight confines of the pelvis have likely
contributed to this result. This difficulty with an optimal local
control is the most noteworthy in light of the fact that the rectal
tumors in this series were significantly smaller compared to the
non-rectal (small intestinal/gastric) tumors. The prominence of
local failure in rectal GIST has been observed by several groups.
In a review by Peralta (9) the
local recurrence rate was 75% in tumors >5 cm (regardless of the
mitotic rate), and 62% in tumors <5 cm (with >5 mitoses per
50 HPF). The failure of the local disease control has been shown to
lead to poor overall outcomes, even after secondary surgery
(10). In addition, the morbidity
associated with the local resection of rectal GIST was clearly
substantial, with 3 patients needing sphincter-compromising APRs, 2
experiencing peri-operative tumor rupture and 1 suffering from an
anastomotic breakdown/abscess formation. The proportion of patients
with rectal GIST experiencing tumor rupture was >4-fold of the
non-rectal GIST patients (22 vs. 5%; P=0.106). Although this
numerical difference did not reach statistical significance, it
might be due to the small sample size of our study population.
These findings are notable, given that the non-rectal tumors were
significantly larger compared to the rectal tumors, underlining the
prominent local morbidity associated with rectal GIST. While no
formal quality of life measures were recorded, the high rates of
local failure and the significant number of events associated with
peri-operative morbidity had a negative impact on outcomes of
patients with resected rectal GIST. In addition to an increasing
morbidity, tumor rupture has been evaluated as an independent
adverse prognostic factor by Rutkowski et al(11), for which patients would require 3
years of adjuvant imatinib with its attendant toxicities and cost,
based upon the data from the recent SSGXVIII study (6).
Thus, the significant local morbidity and high rates
of local failure associated with the surgical treatment of rectal
GIST may signal the need for novel, multi-modal therapeutic
strategies to optimize outcomes. Multi-modality peri-operative
therapy has been shown to improve outcomes and is currently the
mainstay of treatment in rectal adenocarcinoma (7,8), a
disease sharing the anatomical constraints and difficulties with
optimal local control seen in rectal GIST. Neo-adjuvant imatinib
has been shown to be safe and well-tolerated in the treatment of
locally advanced GIST. The median time to best response with
imatinib in advanced GIST has been reported to be between 3 and 4
months (12). In their study,
Blesius et al(13)
demonstrated that up to 36% of the patients with locally advanced
non-metastatic GIST deemed upfront unresectable received
neo-adjuvant imatinib and subsequently underwent surgery by the
local surgeons, who had initially advised against operation.
Neo-adjuvant imatinib has also been shown to facilitate anal
sphincter preservation without compromising optimal local control
in patients with rectal GIST initially deemed to necessitate APR
(14). These data argue strongly
for neo-adjuvant imatinib in rectal GIST, especially in patients
deemed unresectable or for whom APR is being considered. Upfront
surgical resection resulting in positive margins and/or
peri-operative tumor events is likely to exacerbate morbidity and
contribute to increased recurrences and sub-optimal outcomes.
Although the use of radiation is not traditionally
associated with the curative treatment of GIST, its role requires
further examination, particularly when combined with imatinib.
Preclinical data suggest imatinib to be a radiation-sensitizer
(15), while isolated reports have
suggested the potential efficacy of radiation in managing rectal
GIST when combined with imatinib (16).
Thus, rectal GIST is a rare subset of GIST, for
which data remain scant and outcomes are sub-optimal with surgical
resection alone. In this study, in spite of being significantly
smaller compared to GIST of other common sites, rectal GIST was
demonstrated to be associated with significantly higher rates of
positive surgical margins and local relapses attributable to the
unique anatomical location of the primary tumor. The morbidity of
upfront rectal surgery in this subset of GIST is also
substantial.
Increased local relapse and high peri-operative
morbidity render the evaluation of fresh approaches necessary to
improve outcomes in this disease. A multi-modality approach
incorporating neo-adjuvant and/or adjuvant imatinib in the
appropriate patient setting should be strongly considered. The
involvement of peri-operative radiation in rectal GIST also
deserves further clinical evaluation in a controlled, prospective
clinical trial setting.
References
|
1.
|
Fletcher CD, Berman JJ, Corless C, et al:
Diagnosis of gastrointestinal stromal tumors: a consensus approach.
Hum Pathol. 33:459–465. 2002.
|
|
2.
|
Miettinen M and Lasota J: Gastrointestinal
stromal tumors: pathology and prognosis at different sites. Semin
Diagn Pathol. 23:70–83. 2006.
|
|
3.
|
Joensuu H: Risk stratification of patients
diagnosed with gastrointestinal stromal tumor. Hum Pathol.
39:1411–1419. 2008.
|
|
4.
|
Rutkowski P, Nowecki ZI, Michej W, et al:
Risk criteria and prognostic factors for predicting recurrences
after resection of primary gastrointestinal stromal tumor. Ann Surg
Oncol. 14:2018–2027. 2007.
|
|
5.
|
Dematteo RP, Ballman KV, Antonescu CR, et
al: Adjuvant imatinib mesylate after resection of localised,
primary gastrointestinal stromal tumour: a randomised,
double-blind, placebo-controlled trial. Lancet. 373:9669–1097.
2009.
|
|
6.
|
Joensuu H, Eriksson M, Hatrmann J, et al:
Twelve versus 36 months of adjuvant imatinib as treatment of
operable GIST with a high risk of recurrence: final results of a
randomized trial (SSGXVIII/AIO) (abs. LBA1). J Clin Oncol.
29:2011.
|
|
7.
|
Van Gijn W, Marijnen CA, Nagtegaal ID, et
al: Preoperative radiotherapy combined with total mesorectal
excision for resectable rectal cancer: 12-year follow-up of the
multicentre, randomised controlled TME trial. Lancet Oncol.
12:575–582. 2011.
|
|
8.
|
Sauer R, Becker H, Hohenberger W, et al:
Preoperative versus postoperative chemoradiotherapy for rectal
cancer. N Engl J Med. 351:1731–1740. 2004.
|
|
9.
|
Peralta EA: Rare anorectal neoplasms:
gastrointestinal stromal tumor, carcinoid, and lymphoma. Clin Colon
Rectal Surg. 22:107–114. 2009.
|
|
10.
|
Dong C, Jun-Hui C, Xiao-Jun Y, Mei K, Bo
W, Chen-Fe J and Wei-Li Y: Gastrointestinal stromal tumors of the
rectum: clinical, pathologic, immunohistochemical characteristics
and prognostic analysis. Scand J Gastroenterol. 42:1221–1229.
2007.
|
|
11.
|
Rutkowski P, Bylina E, Wozniak A, et al:
Validation of the Joensuu risk criteria for primary resectable
gastrointestinal stromal tumour-the impact of tumour rupture on
patient outcomes. Eur J Surg Oncol. 37:890–896. 2011.
|
|
12.
|
Verweij J, Casali PG, Zalcberg J, et al:
Progression-free survival in gastrointestinal stromal tumours with
high-dose imatinib: randomised trial. Lancet. 364:1127–1134.
2004.
|
|
13.
|
Blesius A, Cassier PA, Bertucci F, et al:
Neoadjuvant imatinib in patients with locally advanced non
metastatic GIST in the prospective BFR14 trial. BMC Cancer.
15:722011.
|
|
14.
|
Wang JP, Wang T, Huang MJ, Wang L, Kang L
and Wu XJ: The role of neoadjuvant imatinib mesylate therapy in
sphincter-preserving procedures for anorectal gastrointestinal
stromal tumor. Am J Clin Oncol. 34:314–316. 2011.
|
|
15.
|
Choudhury A, Zhao H, Jalali F, et al:
Targeting homologous recombination using imatinib results in
enhanced tumor cell chemosensitivity and radiosensitivity. Mol
Cancer Ther. 8:203–213. 2009.
|
|
16.
|
Ciresa M, D’Angelillo RM, Ramella S, et
al: Molecularly targeted therapy and radiotherapy in the management
of localized gastrointestinal stromal tumor (GIST) of the rectum: a
case report. Tumori. 95:236–239. 2009.
|